
Association between Lung Fluid Levels Estimated by Remote Dielectric Sensing Values and Invasive Hemodynamic Measurements

 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Participant Selection
2.2. Study Protocol
2.3. ReDS System
2.4. Statistical Procedures
3. Results
3.1. Baseline Characteristics
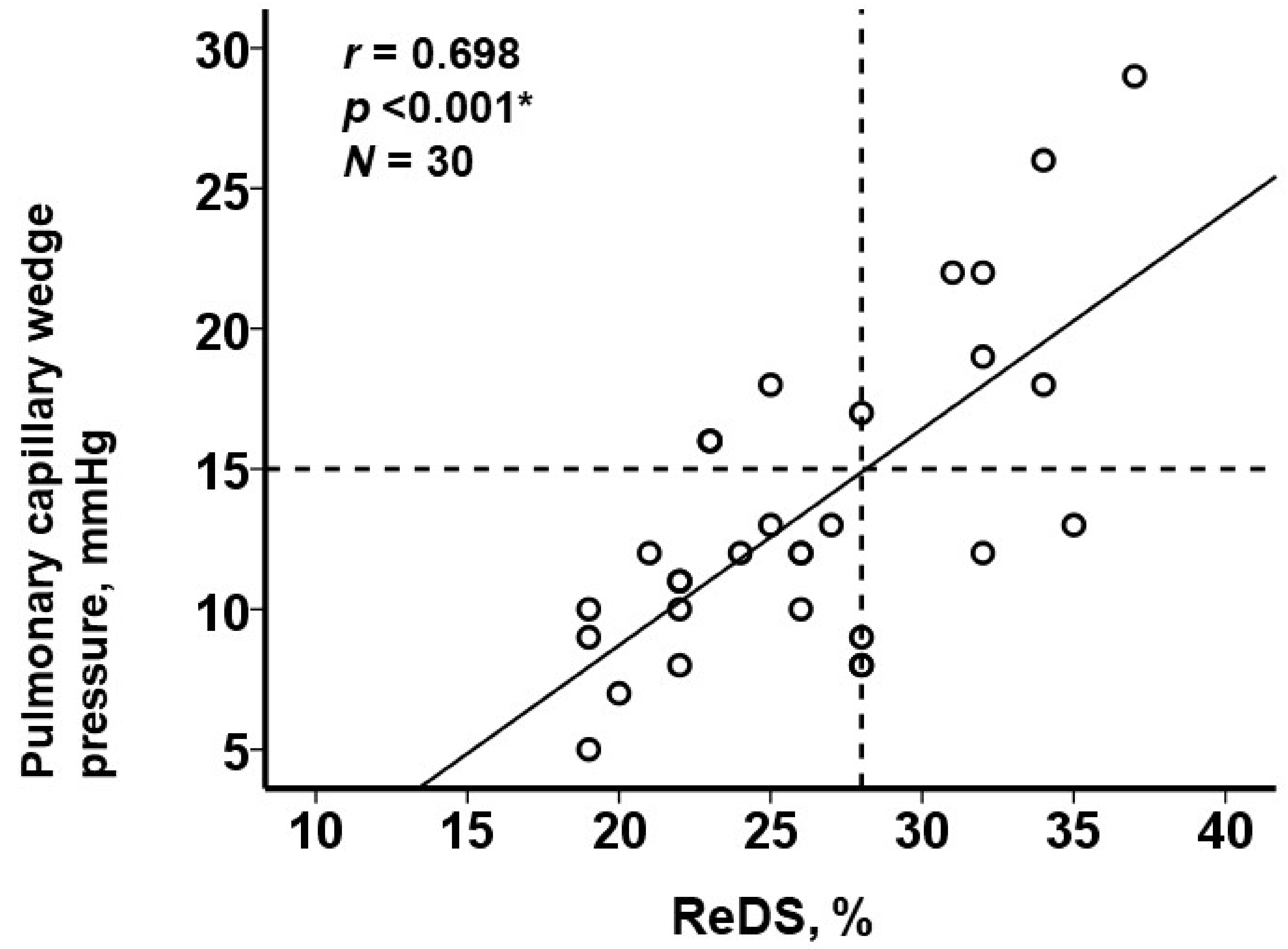
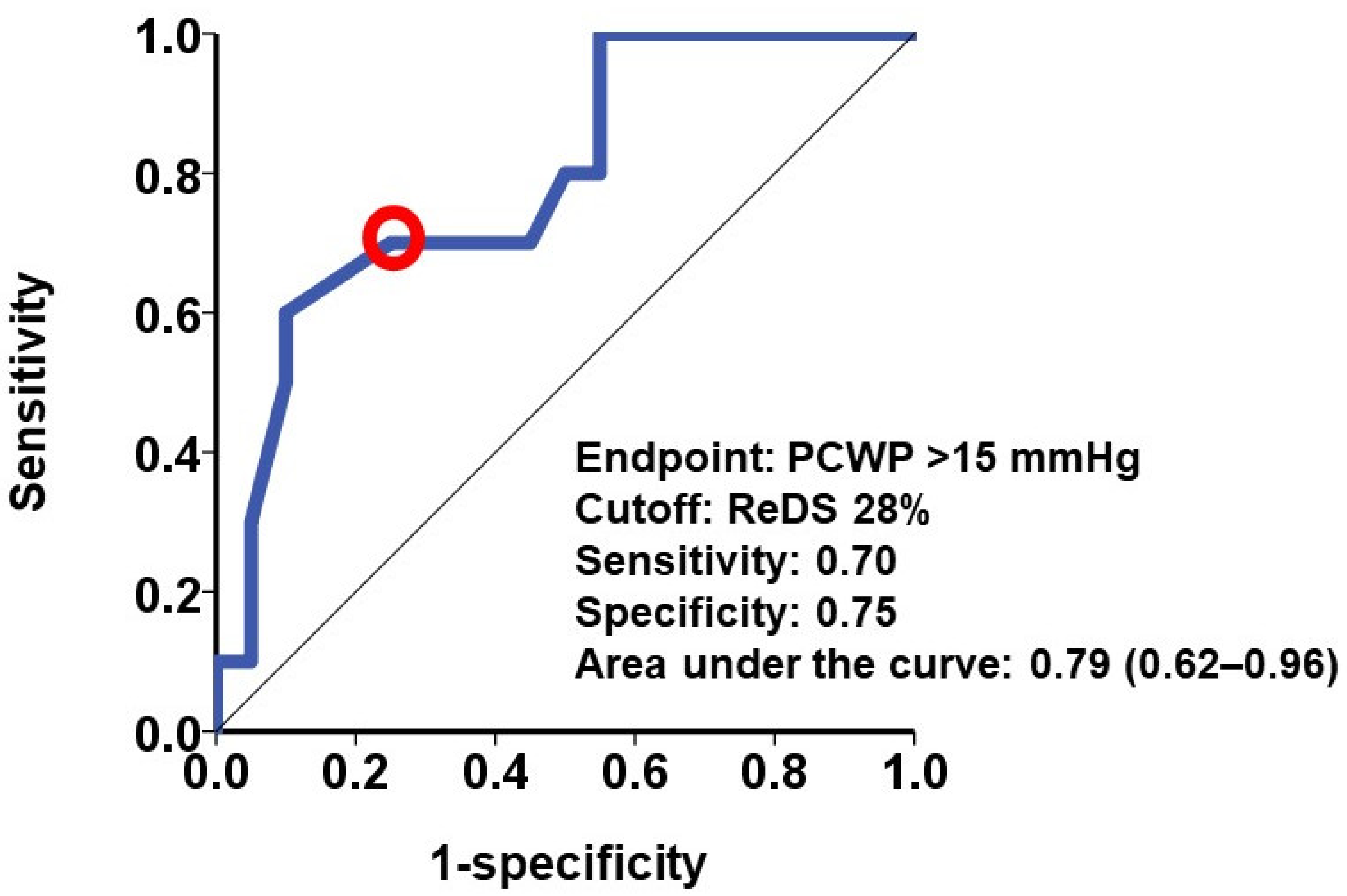
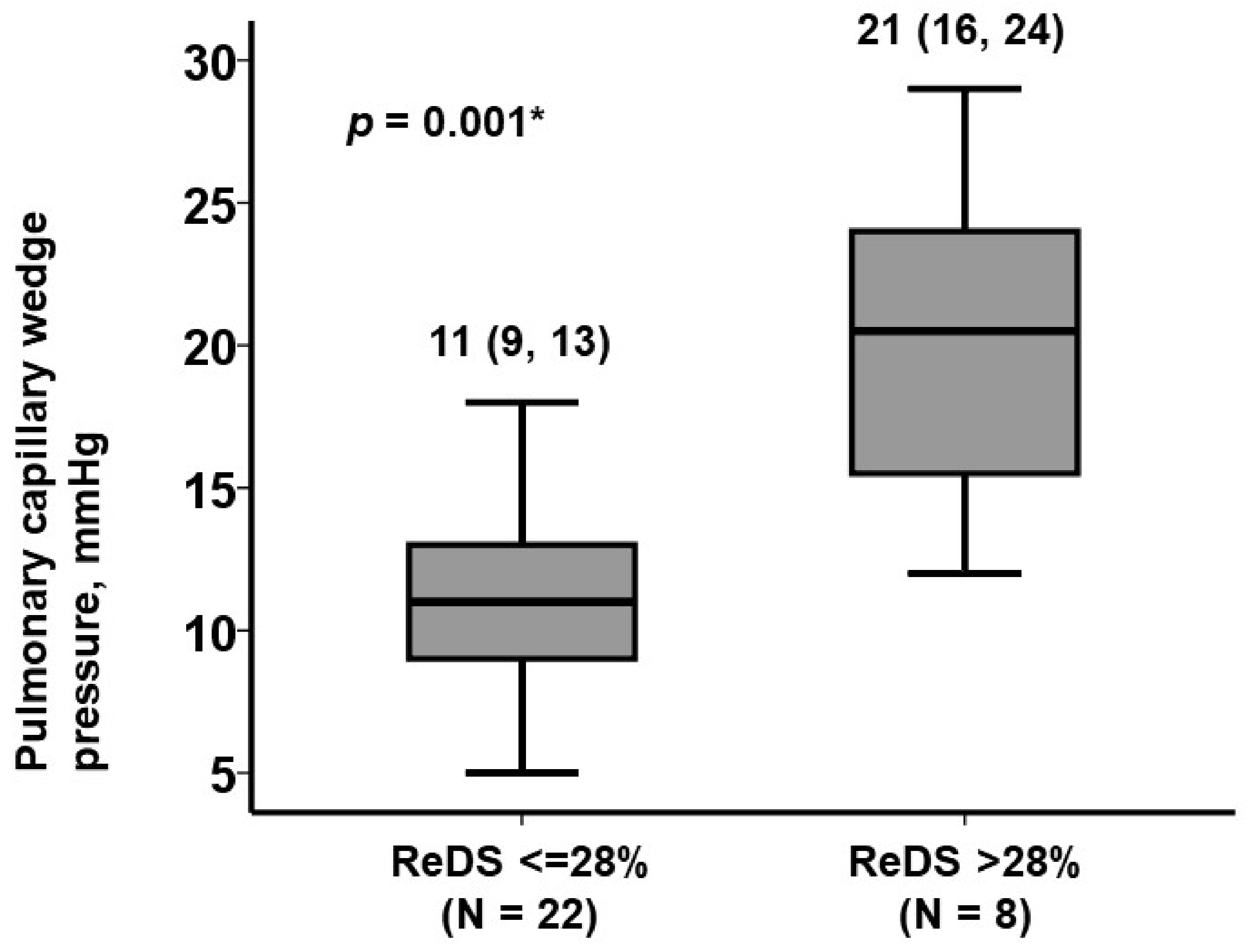
3.2. Association between ReDS Values and PCWP
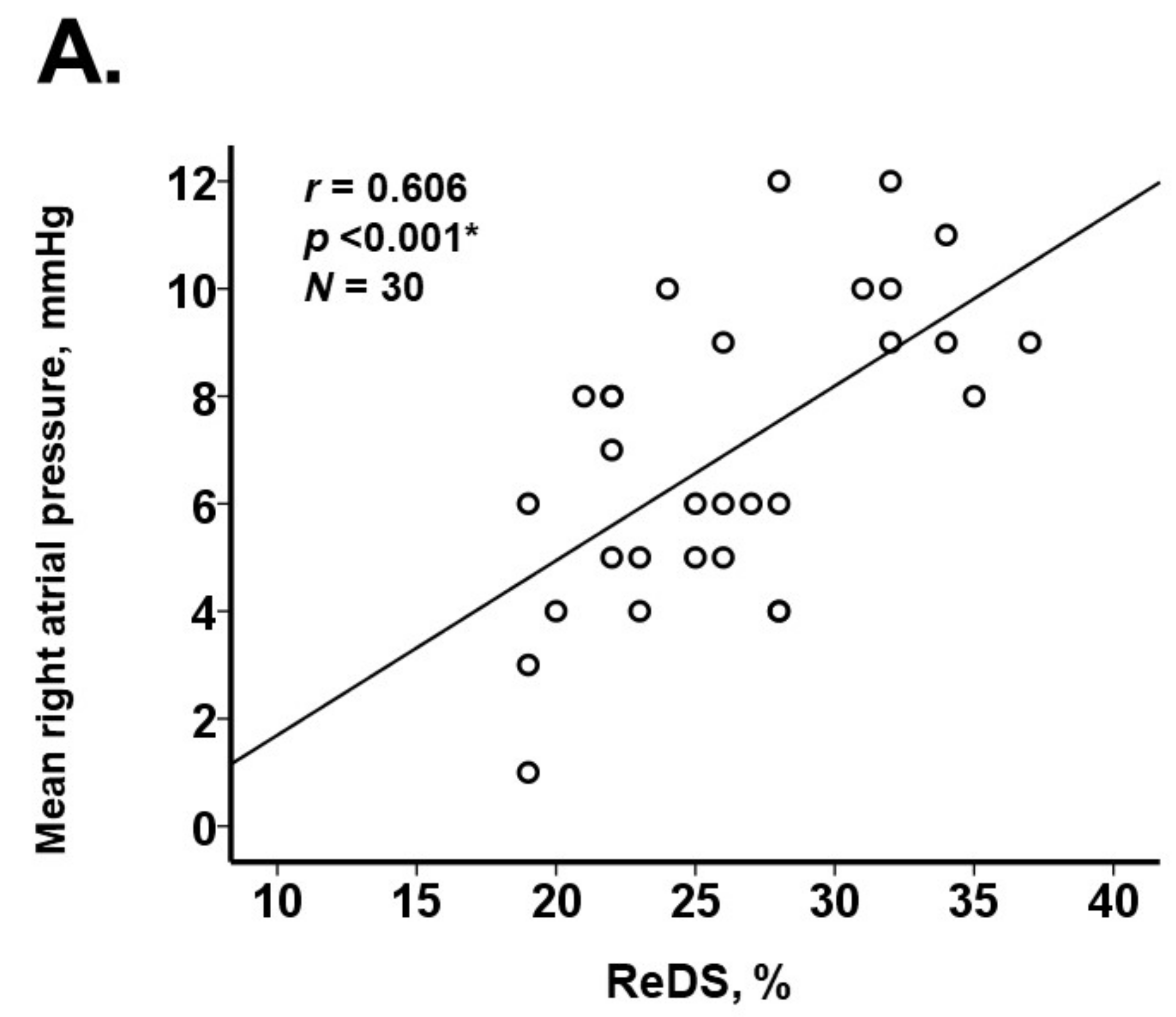
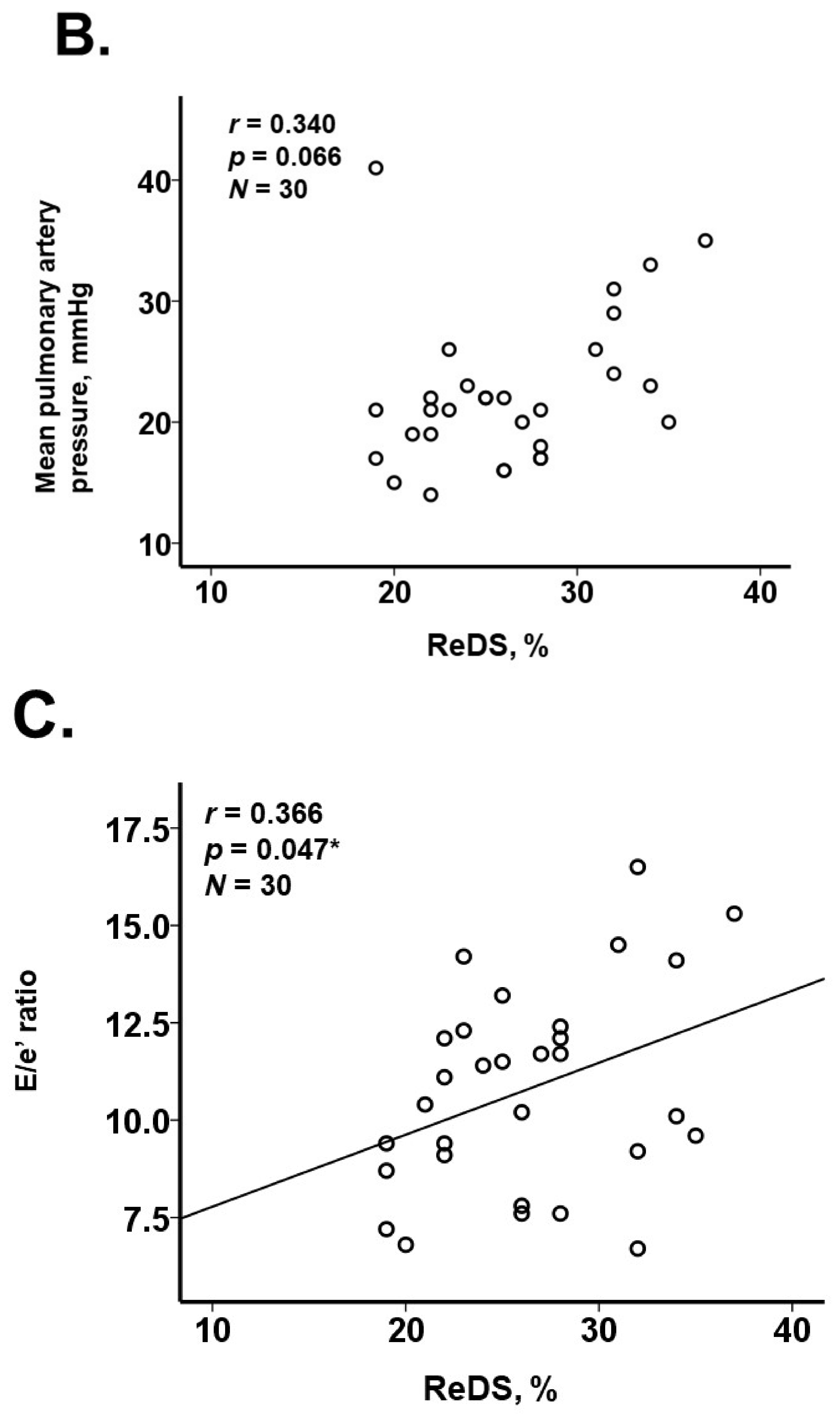
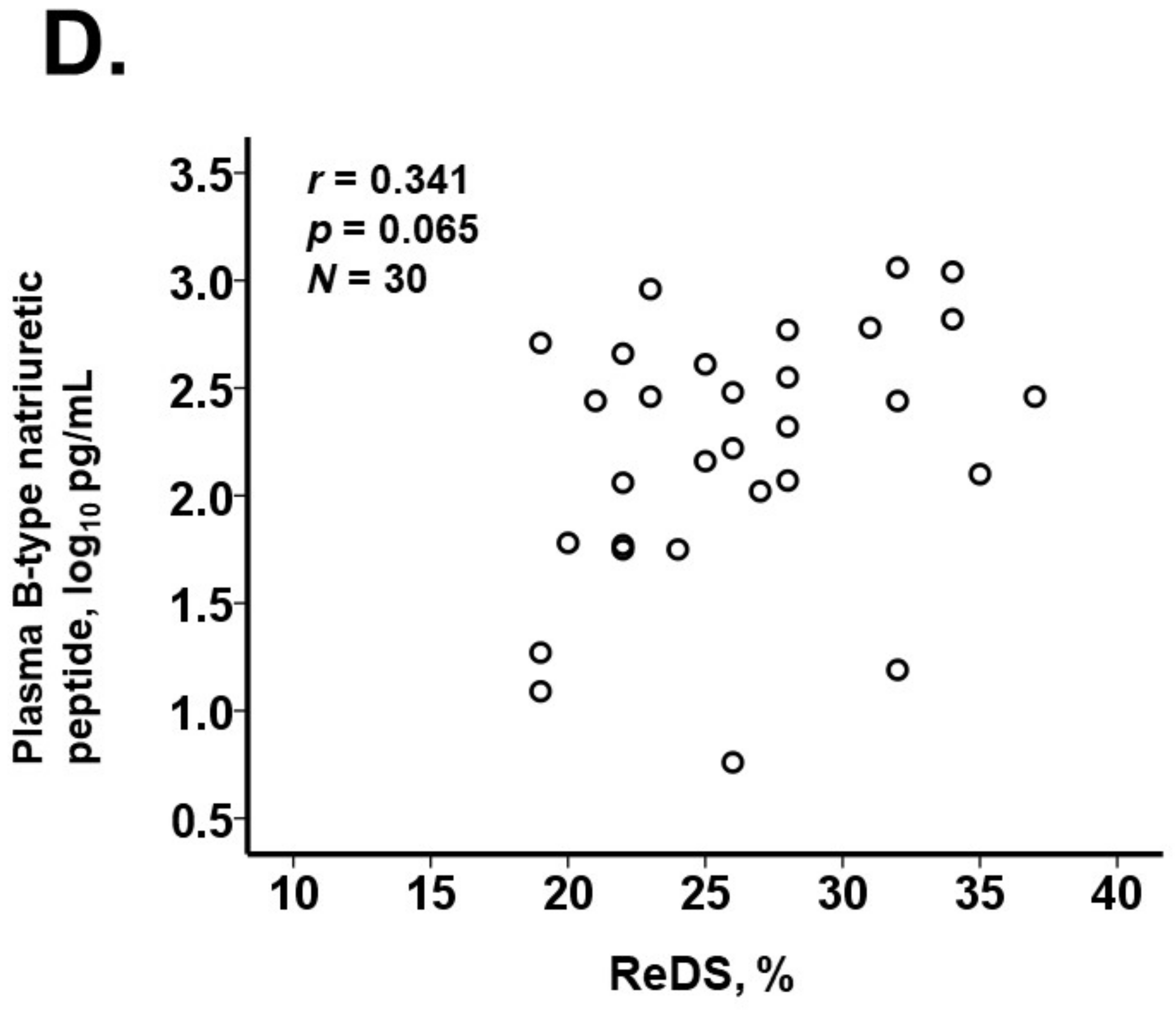
3.3. Association between ReDS Values and Other Parameters
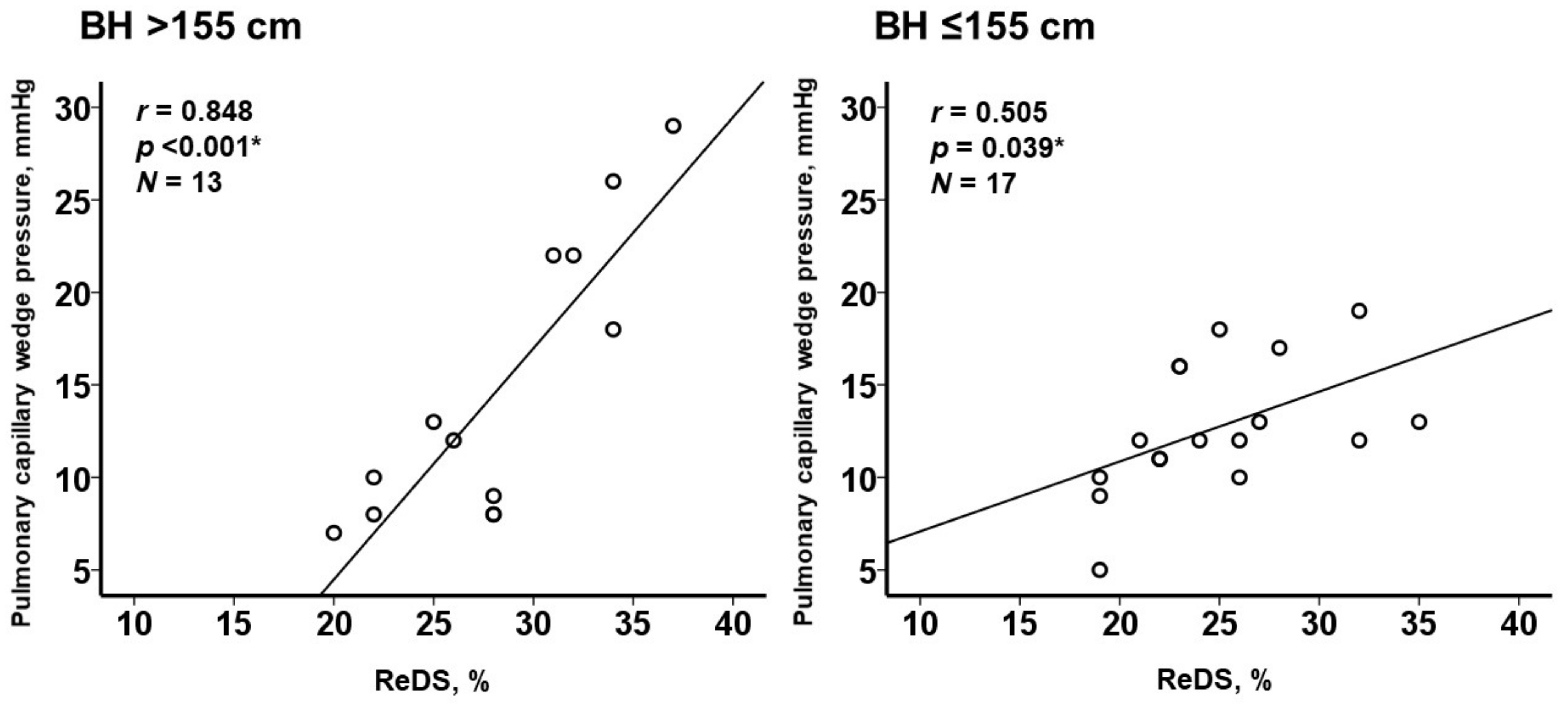
3.4. Sub-Group Analyses According to the Body Height
4. Discussion
4.1. ReDS Engineering
4.2. ReDS Values and PCWP Values
4.3. Prior Analyses
4.4. Body Size
4.5. ReDS System and Right Heart Catheterization
4.6. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abraham, W.T.; Perl, L. Implantable Hemodynamic Monitoring for Heart Failure Patients. J. Am. Coll. Cardiol. 2017, 70, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Amir, O.; Rappaport, D.; Zafrir, B.; Abraham, W.T. A novel approach to monitoring pulmonary congestion in heart failure: Initial animal and clinical experiences using remote dielectric sensing technology. Congest. Heart Fail. 2013, 19, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Amir, O.; Azzam, Z.S.; Gaspar, T.; Faranesh-Abboud, S.; Andria, N.; Burkhoff, D.; Abbo, A.; Abraham, W.T. Validation of remote dielectric sensing (ReDS) technology for quantification of lung fluid status: Comparison to high resolution chest computed tomography in patients with and without acute heart failure. Int. J. Cardiol. 2016, 221, 841–846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amir, O.; Ben-Gal, T.; Weinstein, J.M.; Schliamser, J.; Burkhoff, D.; Abbo, A.; Abraham, W.T. Evaluation of remote dielectric sensing (ReDS) technology-guided therapy for decreasing heart failure re-hospitalizations. Int. J. Cardiol. 2017, 240, 279–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lala, A.; Barghash, M.H.; Giustino, G.; Alvarez-Garcia, J.; Konje, S.; Parikh, A.; Ullman, J.; Keith, B.; Donehey, J.; Mitter, S.S.; et al. Early use of remote dielectric sensing after hospitalization to reduce heart failure readmissions. ESC Heart Fail. 2021, 8, 1047–1054. [Google Scholar] [CrossRef] [PubMed]
- Uriel, N.; Sayer, G.; Imamura, T.; Rodgers, D.; Kim, G.; Raikhelkar, J.; Sarswat, N.; Kalantari, S.; Chung, B.; Nguyen, A.; et al. Relationship Between Noninvasive Assessment of Lung Fluid Volume and Invasively Measured Cardiac Hemodynamics. J. Am. Heart Assoc. 2018, 7, e009175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pirrotta, F.; Mazza, B.; Gennari, L.; Palazzuoli, A. Pulmonary Congestion Assessment in Heart Failure: Traditional and New Tools. Diagnostics 2021, 11, 1306. [Google Scholar] [CrossRef] [PubMed]
- Thibodeau, J.T.; Drazner, M.H. The Role of the Clinical Examination in Patients With Heart Failure. JACC Heart Fail. 2018, 6, 543–551. [Google Scholar] [CrossRef] [PubMed]
- Galiè, N.; Humbert, M.; Vachiery, J.L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Vonk Noordegraaf, A.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur. Respir. J. 2015, 46, 903–975. [Google Scholar] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N = 30 | |
|---|---|
| Demographics | |
| Age, years | 79 (73, 84) |
| Men | 13 (43%) |
| Body height, cm | 153 (149, 163) |
| Body height < 155 cm | 17 (57%) |
| Body weight, kg | 55.0 (50.1, 61.1) |
| Body mass index | 22.9 (20.0, 24.5) |
| Comorbidity | |
| Hypertension | 22 (73%) |
| Dyslipidemia | 13 (43%) |
| Diabetes mellitus | 8 (27%) |
| Atrial fibrillation | 12 (40%) |
| Chronic kidney disease | 18 (60%) |
| History of stroke | 2 (7%) |
| History of coronary intervention | 2 (7%) |
| Valvular disease | 14 (47%) |
| Echocardiography | |
| Left ventricular end-diastolic diameter, mm | 48 (44, 54) |
| Left ventricular ejection fraction, % | 54 (42, 66) |
| Left atrial diameter, mm | 45 (40, 51) |
| E/e’ ratio | 10.8 (9.1, 12.3) |
| Hemodynamics | |
| Heart rate, bpm | 70 (64, 82) |
| Mean right atrial pressure, mmHg | 7 (6, 9) |
| Mean pulmonary artery pressure, mmHg | 21 (19, 23) |
| Pulmonary capillary wedge pressure, mmHg | 12 (10, 17) |
| Cardiac index, L/min/m2 | 2.1 (1.9, 2.3) |
| Medications | |
| Beta-blocker | 16 (53%) |
| Angiotensin converting enzyme inhibitor | 22 (73%) |
| Mineralocorticoid receptor antagonist | 11 (37%) |
| Loop diuretics | 15 (50%) |
| Plasma B-type natriuretic peptide, log10 pg/mL | 2.22 (1.90, 2.47) |
| Remote dielectric sensing, % | 26 (22, 28) |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| Beta Value (95% CI) | p Value | Beta Value (95% CI) | p Value | |
| Age, years | 0.06 (−0.17–0.30) | 0.58 | −0.004 (−0.22–0.21) | 0.98 |
| Body mass index | −0.21 (−0.78–0.35) | 0.44 | −0.22 (−0.79–0.13) | 0.15 |
| Chronic kidney disease | −3.58 (−0.78–0.63) | 0.092 | 0.04 (−4.10–5.10) | 0.82 |
| Left ventricular ejection fraction, % | −0.08 (−0.20–0.04) | 0.17 | −0.02 (−0.11–0.11) | 0.99 |
| Remote dielectric sensing, % | 0.77 (0.47–1.08) | <0.001 * | 0.74 (0.38–1.26) | 0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imamura, T.; Hori, M.; Ueno, Y.; Narang, N.; Onoda, H.; Tanaka, S.; Nakamura, M.; Kataoka, N.; Sobajima, M.; Fukuda, N.; et al. Association between Lung Fluid Levels Estimated by Remote Dielectric Sensing Values and Invasive Hemodynamic Measurements. J. Clin. Med. 2022, 11, 1208. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11051208
Imamura T, Hori M, Ueno Y, Narang N, Onoda H, Tanaka S, Nakamura M, Kataoka N, Sobajima M, Fukuda N, et al. Association between Lung Fluid Levels Estimated by Remote Dielectric Sensing Values and Invasive Hemodynamic Measurements. Journal of Clinical Medicine. 2022; 11(5):1208. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11051208
Chicago/Turabian StyleImamura, Teruhiko, Masakazu Hori, Yohei Ueno, Nikhil Narang, Hiroshi Onoda, Shuhei Tanaka, Makiko Nakamura, Naoya Kataoka, Mitsuo Sobajima, Nobuyuki Fukuda, and et al. 2022. "Association between Lung Fluid Levels Estimated by Remote Dielectric Sensing Values and Invasive Hemodynamic Measurements" Journal of Clinical Medicine 11, no. 5: 1208. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11051208