
Oncofertility and Reproductive Counseling in Patients with Breast Cancer: A Retrospective Study

 , , ,
, , ,  , , , , and
, , , , and
Abstract
:1. Introduction
1.1. Histological and Molecular Classification
- Primary tumor (T), wherein the local extension of the tumor is examined;
- Regional lymph nodes (N), wherein the impairment of the draining lymph nodes are assessed. In the case of the breast, the axillary lymph nodes are of primary interest;
- Distant metastasis (M), werein the presence or absence of systemic metastases is studied.
- Luminal A, neoplasms with the expression of hormone receptors for estrogen and progesterone, associated with HER2 negativity and low Ki67 levels [13];
- Luminal B, neoplasms that express hormone receptors, like Luminal A, which are associated with high values of proliferative activity. These, in turn, are divided according to the expression of HER2 into HER2 negative and HER2 positive, in which the levels of Ki67 are not relevant, the strong replicative activity is at the basis of a high risk of recidivism [14];
- HER2-positive, highly expressed HER2 (3+ in immunohistochemical reactions) with an absence of estrogen receptors [15];
Treatment of Breast Cancer
1.2. Antineoplastic Treatments and Infertility
- Direct damage due to destruction of primary follicles that cannot be replaced, resulting in premature ovarian exhaustion (POF) as the ovarian reserve has been significantly reduced by the treatment;
- Indirect damage that can result either from the involvement of granulosa cells with hormone production deficiency and, therefore, the development of temporary hypoestrogenic hypergonadotropic amenorrhea lasting about 2 months with the recovery determined by the entry of new follicles in the cyclic phase or due to the compromise of the vascular network and of the ovarian stroma with ischemic suffering of the primordial follicles, which causes the apoptosis of the latter [33,34].
- High risk (>80%): cyclophosphamide, adjuvant therapy for breast cancer in combination with methotrexate, fluorouracil, doxorubicin, epirubicin in patients >40 years;
- Intermediate risk (20–80%): taxani, adjuvant therapy for breast cancer in combination with methotrexate, fluorouracil, doxorubicin, epirubicin in patients 30–39 years;
- Low risk (<20%) vinblastine, bleomycin, dactinomycin, 6-mercapto-purine, adjuvant therapy for breast cancer in combination with methotrexate, fluorouracil, doxorubicin, epirubicin in patients >30 years;
- Very low/absent risk: vincristine, 5-fluorouracil, methotrexate;
1.3. Oncofertility
Preservation of Fertility in Breast Cancer
- Induction of multiple follicular growth: this entails an ovarian stimulation phase, obtained through the daily subcutaneous injection of gonadotropins, associated with the subcutaneous injection of a similar luteinizing hormone-releasing hormone (LHRH) to avoid early spontaneous ovulation. The duration of the stimulation can vary between 9 and 15 days, causing a delay in the start of chemotherapy;
- Ultrasound-guided egg retrieval: this consists of a short-term invasive procedure, which can be performed under general or local anesthesia. Complications are rare;
1.4. Rules Governing Oncofertility
- They should be placed within public health facilities that meet the multidisciplinary criteria and the criteria of structural compliance with the Guidelines;
- They ought to be capable of guaranteeing a dedicated and consistent service and be adequately staffed (gynecologists, endocrinologists-andrologists, biologists-oncologists, psychologists and nurses);
- OCs need to rely on an effective booking system with availability for specialist-patient consultation within 24–48 h on an informative website;
- OCs need to be able to provide adequate counseling on cryopreservation, on any subsequent MAP options and techniques with adequate information material, and create a standardized informed consent form and digital archiving, preferably on a national basis.
1.5. Reproductive Counseling in Cancer Patients
- Recommendation 1: cancer patients are to be considered interested in discussing the preservation of their fertility. It is, therefore, the duty of the doctor and in general of any health professional to talk about the risk of infertility as early as possible before treatment;
- Recommendation 2: healthcare professionals should refer patients who express an interest in preserving fertility (and those who are undecided) to a reproductive specialist;
- Recommendation 3: in order to keep all options open, fertility preservation ought to be discussed as early as possible before the start of therapies.
2. Experimental Study
2.1. Objectives of the Study
- Investigate adherence to good clinical practice, as dictated by the guidelines, within the Breast Unit of the Policlinico Umberto I in Rome, evaluating the number of patients with whom reproductive counseling took place;
- Analyze the relationship between the diagnosis and the fertility preservation proposal;
- Investigate the discrepancy between the counseling proposal and adherence to fertility preservation practices;
- Investigate the ways in which reproductive counseling is conducted and the patient’s satisfaction in this regard;
- Analyze the impact of the SARS COVID-19 pandemic on the issue of oncofertility;
- Raise awareness and inform doctors on the topic of “oncofertility” and on the importance of reproductive counseling in the multidisciplinary management of cancer patients of childbearing age for the fundamental purpose of promoting adherence to national guidelines for the preservation of fertility in cancer patients, in compliance with the legal and ethical duties of the doctor.
2.2. Materials and Methods
2.2.1. Study Design
2.2.2. Procedure and Methods of Data Collection
2.2.3. Characteristics of the Sample
2.2.4. Data Processing
3. Results
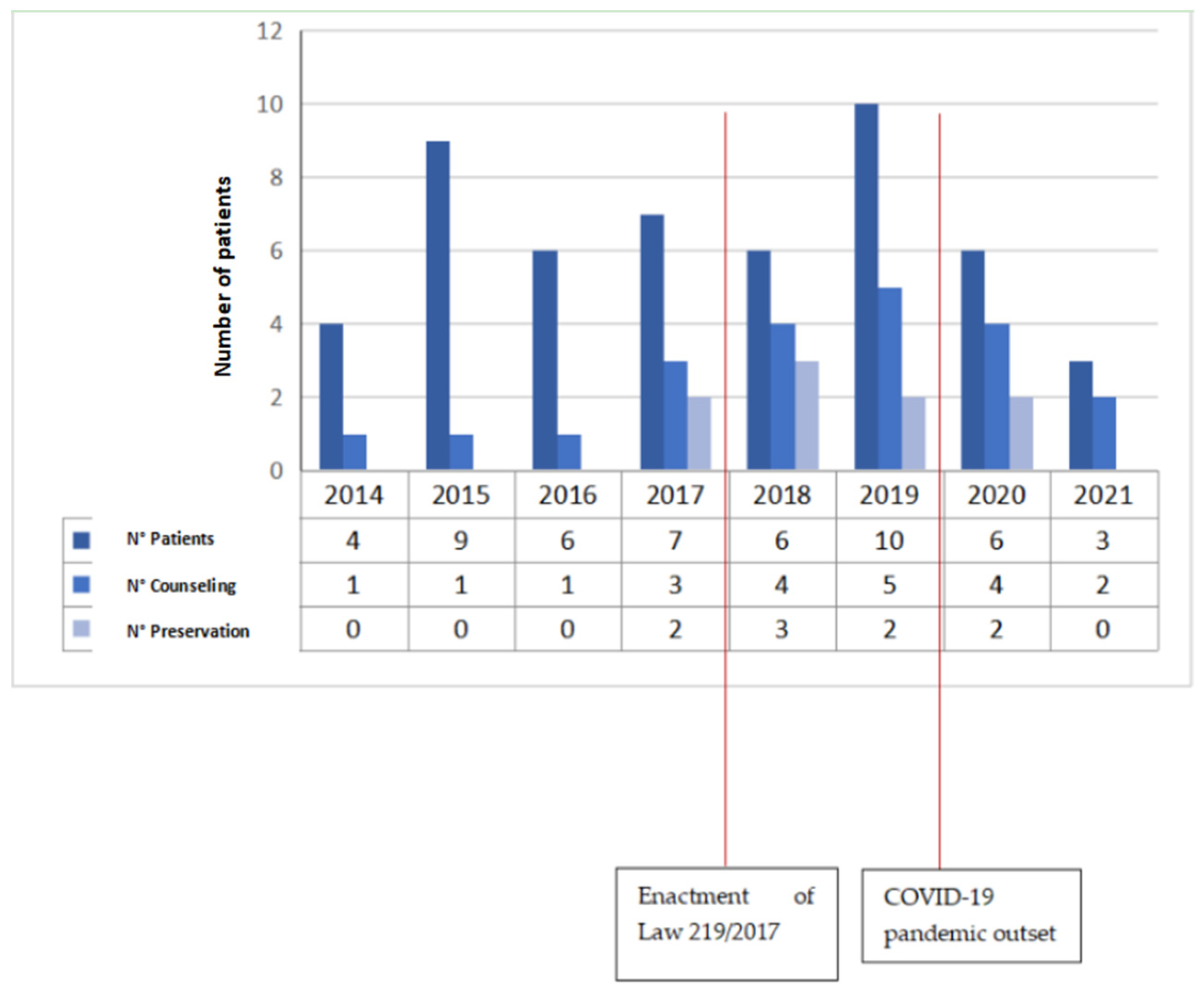
- Item 1: the first data collected are the year of diagnosis: in 2014, 4 patients were selected, in 2015, 9 patients were selected, in 2016, 6 patients were selected, 7 patients were selected in 2017, 6 in 2018, 10 in 2019, 6 in 2020, and 3 in 2021 (Figure 1). As is apparent, new and extraordinary obstacles to cancer care and oncofertility counseling have been caused by the COVID-19 pandemic [88]. Such challenges have affected access to fertility preservation procedures as well: elective procedures relying on ART have been discontinued or procrastinated, which are reflected in the study’s findings as well. The difficulties faced by patients as a result of the ongoing pandemic range from essential aspects such as gaining access to tertiary facilities performing both cancer treatments and fertility preservation interventions to the major concerns arising from the fear of possibly getting infected during fertility preservation procedures, which of course entail additional risks stemming from more hospital stays and surgical interventions. Hence, pandemic-related disruptions may even become a disincentivizing factor due to the sense of anxiety that some patients may experience out of fear of getting infected, which could even cause some patients to decide against fertility preservation despite their wish to start a family after cancer treatment. It is therefore of utmost importance for thorough oncofertility counseling to address the additional concerns and emotional distress experienced by many patients because of the ongoing pandemic while striving to outline and put in place additional targeted safety protocols in order to face the dangers and set the patients’ minds at ease [89].
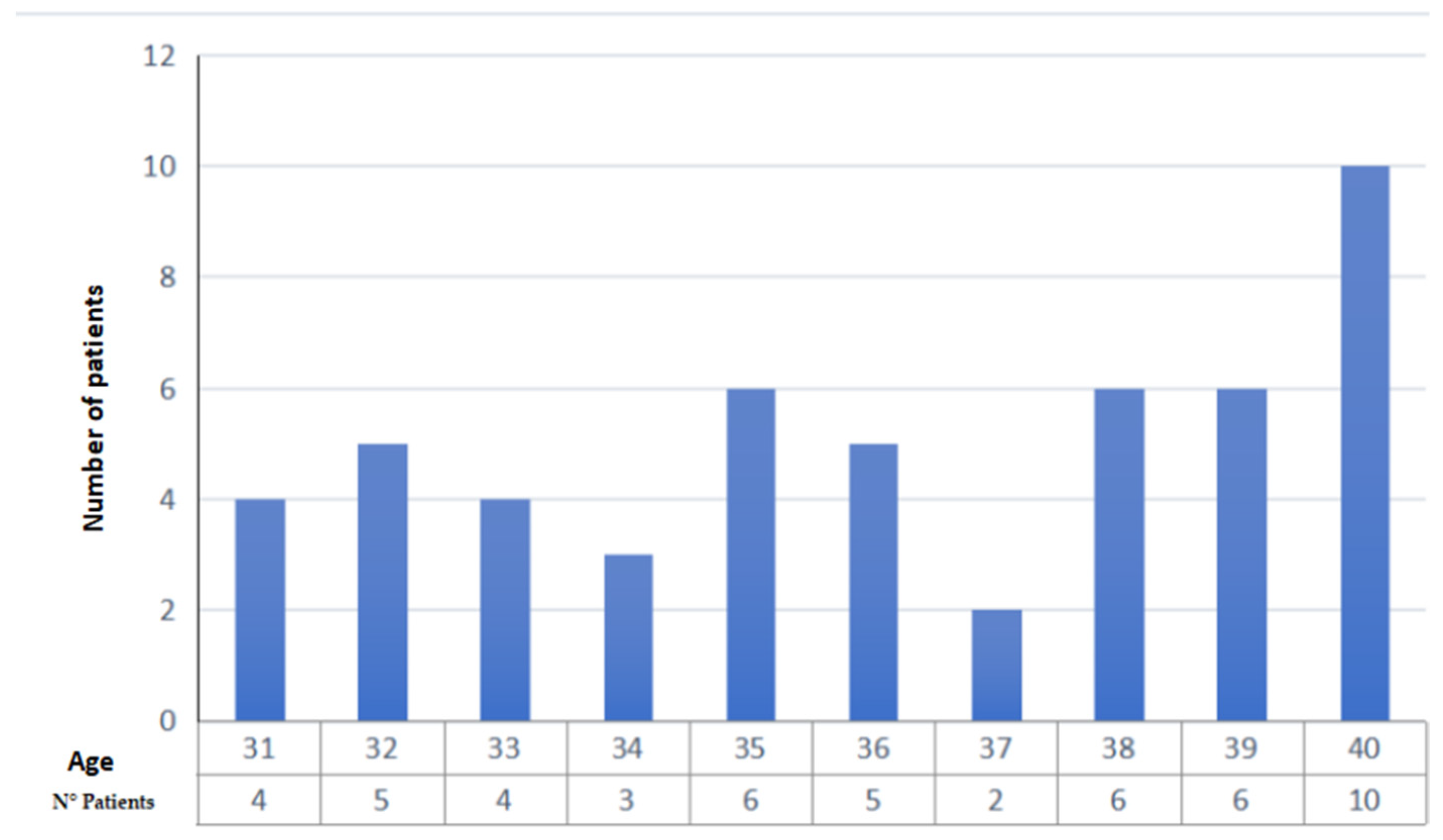
- Item 2: the second parameter taken into consideration is the age of the patient, a primary inclusion criterion. Our study collected patients in the age group 31–40 years (mean age 36.15 years, standard deviation 3.0) (Figure 2);
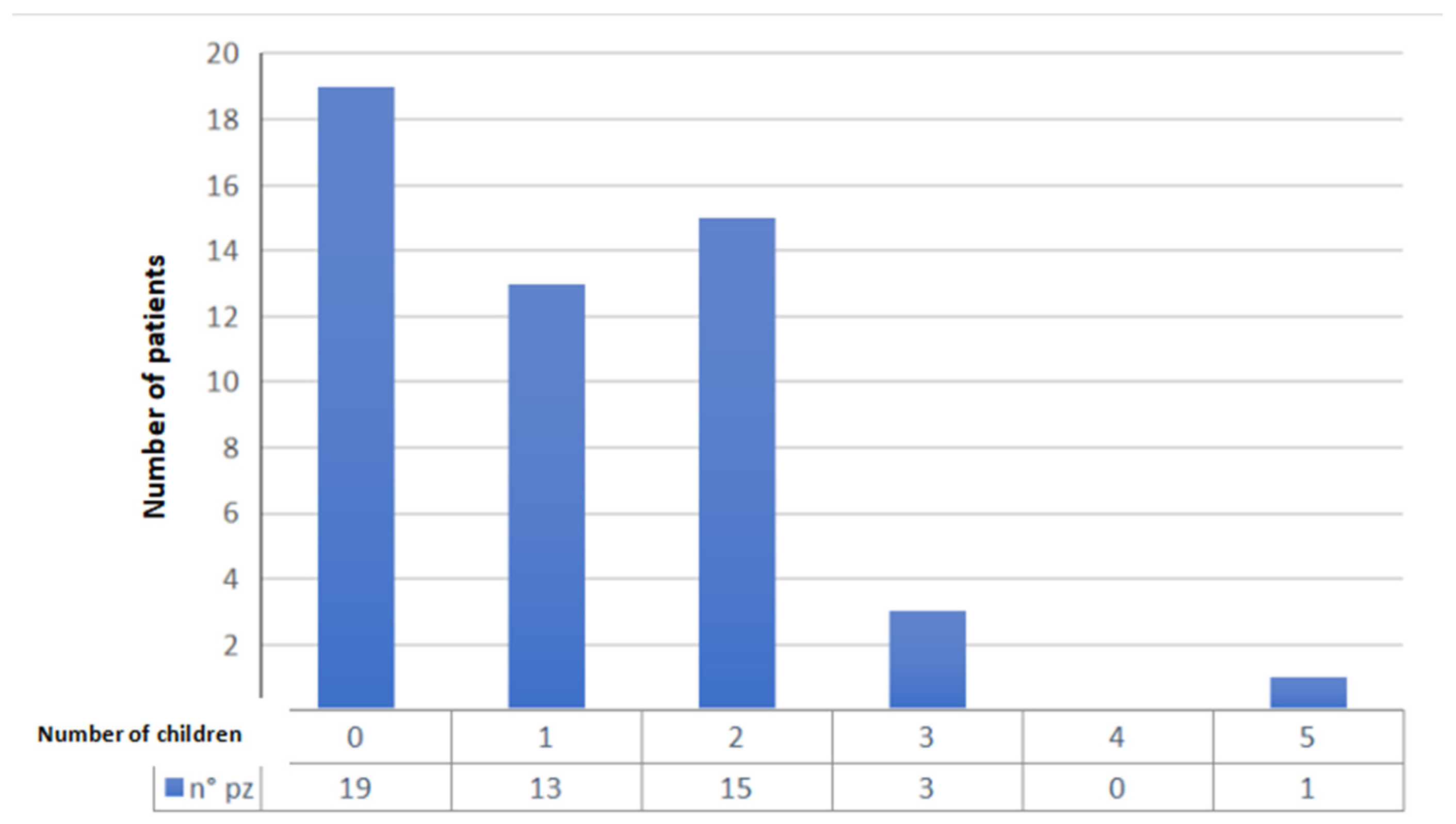
- Item 3: the third data collected is the number of children at the time of diagnosis. A total of 19 patients had no children (37%), 13 had only 1 child (25%), 15 had 2 children (29%), 3 patients had 3 children (6%) and one patient had 5 children (2%) (Figure 3);
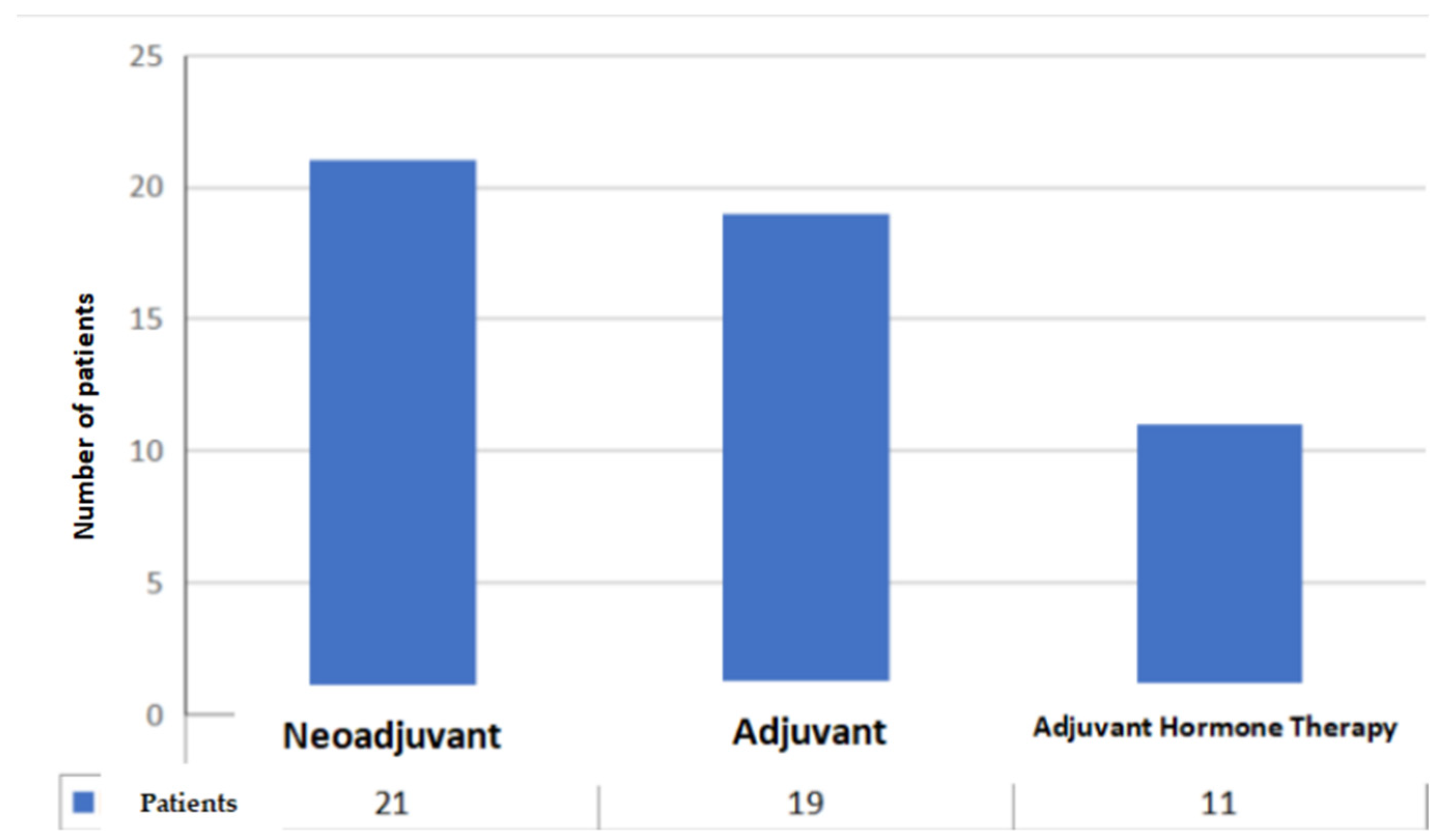
- Item 4: from the data collected regarding the therapy performed by the patients, it emerged that 21 patients (41%) underwent cycles of neoadjuvant chemotherapy, 19 patients (37%) underwent cycles of adjuvant chemotherapy and, for 11 patients (22%), adjuvant hormone therapy was prescribed (Figure 4);
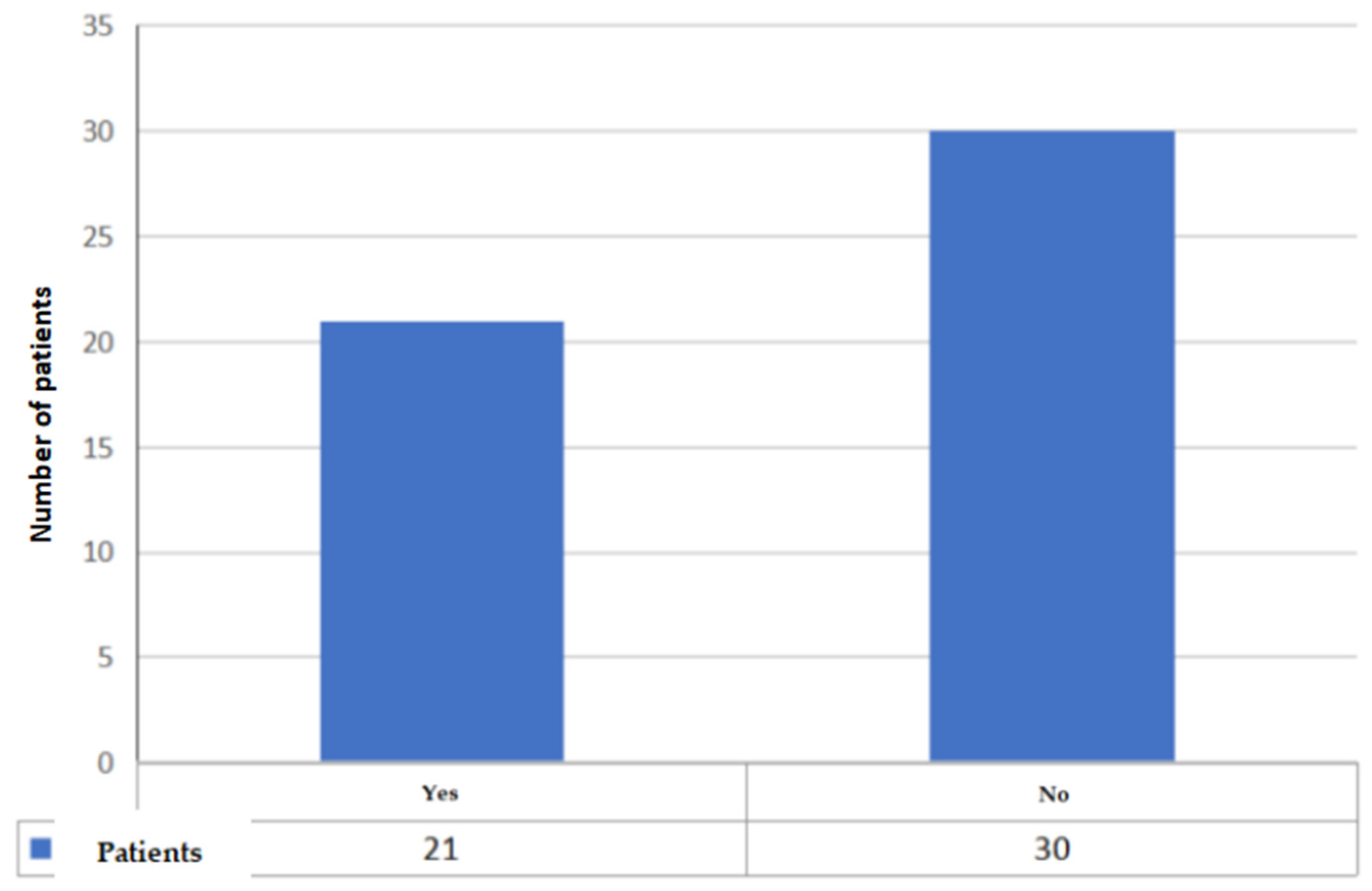
- Items 5 to 8: relate to reproductive counseling and adherence to fertility preservation programs. Reproductive counseling was offered to 21 patients (41%); in the only cases reported (11), it was done through an interview (Figure 5).






4. Discussion
- Question 1 is, in turn, made up of 4 questions for the collection of general information on the patient at the time of diagnosis and at present;
- Question 2 asks for the diagnosis received;
- Questions 3 and 4 investigate the patient’s knowledge of the topic “oncofertility”;
- Questions 5 to 10 investigate the implementation of reproductive counseling, the methods of carrying out such counseling and the outcomes;
- Questions 11 and 12 are asked to find out whether the patient has had full-term pregnancies after recovery. If the patient answers affirmatively, they are asked if these pregnancies were natural or through MAP;
- Question 13 is addressed to patients who have not embarked on a fertility preservation process following reproductive counseling to investigate the causes;
- Question 14 is asked to patients who have not received counseling in order to know the patient’s interest in the possibility of preserving their fertility.
4.1. Medical-Legal Remarks
- Informed, hence based on exhaustive information which must be clear, appropriate to the educational level, age and cognitive functions of each patient, so that they are able to understand the diagnosis, the methods of intervention, the possible alternative therapies, the prognosis, the probabilities of success, the consequences and side effects of the treatment and the strategies to counter the latter;
- Granted in awareness, i.e., expressed by patients who, after having received thorough information, are enabled to understand and make informed decisions;
- Unequivocal, so as not to raise doubts or uncertainty as to the consent or refusal of the proposed treatment;
- Specific, i.e., strictly related to a specific treatment;
- Revocable at any time, even in proximity of the therapeutic act, as long as it is technically possible to refuse it. The withdrawal of consent must be recorded in the medical record in the same manner in which consent to the treatment was acquired;
- Free, i.e., not extorted by deception or duress, since only consent granted without undue external pressure can be considered valid;
- Personal, that is, it must come from patients in possession of their ability to act and to dispose of their bodies, or in any case from a guardian or legal representative holding power of attorney;
- Free of charge, since it cannot be granted in exchange for money or services of any kind.
4.2. Characteristics of the Study, Limitations and Future Prospects
- The need for more information to patients, both oral and, above all, written, through documents and printed resources;
- The need for greater psychological support and assistance to the patient in the decision to preserve fertility;
- The need for greater training of health personnel in this area;
- A positive trend has emerged in recent years with respect to oncofertility information provision to patients.
5. Conclusions
- Create a multi-specialist team within each operating unit for the diagnosis and treatment of neoplastic diseases, which should include oncologists, surgeons, endocrinologists, gynecologists, psychologists and reproductive medicine specialists. The fundamental purpose and priority of the health care team is to fully cover and address all the various complexities and distinctive traits inherent in the oncofertility blueprint and to effectively address women’s psychosocial distress. The team must be able to provide reproductive counseling at the time of diagnosis or soon after the diagnostic-therapeutic process, since fertility, far from being a mere biological parameter, often constitutes a cornerstone of femininity for society and patients themselves;
- Outline and implement a single and standardized reproductive counseling protocol, laid out and agreed on by highly qualified specialists, documented in medical records with informed consent value, based on what has been determined by legal regulations and medical ethics provisions.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ghoncheh, M.; Pournamdar, Z.; Salehiniya, H. Incidence and Mortality and Epidemiology of Breast Cancer in the World. Asian Pac. J. Cancer Prev. 2016, 17, 43–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Fact Sheets. Breast Cancer. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/breast-cancer (accessed on 28 November 2021).
- AIOM-AIRTUM. Cancer Data in Italy. 2019 Edition. Available online: https://www.registri-tumori.it/cms/sites/default/files/pubblicazioni/I%20numeri%20del%20cancro%20in%20Italia%20-%20versione%20per%20operatori.pdf (accessed on 30 November 2021).
- AIOM Guidelines. Breast Neoplasms. Edizione 2019. Available online: https://aiom.it/wp-content/uploads/2019/10/2019_LG_AIOM_Mammella.pdf (accessed on 30 November 2021).
- Akram, M.; Iqbal, M.; Daniyal, M.; Khan, A.U. Awareness and Current Knowledge of Breast Cancer. Biol. Res. 2017, 50, 33. [Google Scholar] [CrossRef] [Green Version]
- Lebeau, A. Updated WHO classification of tumors of the breast. Der Pathol. 2021, 42 (Suppl. S2), 155–159. [Google Scholar] [CrossRef]
- Tan, P.H.; Ellis, I.; Allison, K.; Brogi, E.; Fox, S.B.; Lakhani, S.; Lazar, A.J.; Morris, E.A.; Sahin, A.; Salgado, R.; et al. The 2019 World Health Organization Classification of Tumours of the Breast. Histopathology 2020, 77, 181–185. [Google Scholar] [CrossRef]
- Van de Vijver, M.J.; He, Y.D.; van’t Veer, L.J.; Dai, H.; Hart, A.A.M.; Voskuil, D.W.; Schreiber, G.J.; Peterse, J.L.; Roberts, C.; Marton, M.J.; et al. A Gene-Expression Signature as a Predictor of Survival in Breast Cancer. N. Engl. J. Med. 2002, 347, 1999–2009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piergentili, R.; Zaami, S.; Cavaliere, A.F.; Signore, F.; Scambia, G.; Mattei, A.; Marinelli, E.; Gulia, C.; Perelli, F. Non-Coding RNAs as Prognostic Markers for Endometrial Cancer. Int. J. Mol. Sci. 2021, 22, 3151. [Google Scholar] [CrossRef]
- Mei, J.; Hao, L.; Wang, H.; Xu, R.; Liu, Y.; Zhu, Y.; Liu, C. Systematic Characterization of Non-Coding RNAs in Triple-Negative Breast Cancer. Cell. Prolif. 2020, 53, e12801. [Google Scholar] [CrossRef] [Green Version]
- Vallone, C.; Rigon, G.; Gulia, C.; Baffa, A.; Votino, R.; Morosetti, G.; Zaami, S.; Briganti, V.; Catania, F.; Gaffi, M.; et al. Non-Coding RNAs and Endometrial Cancer. Genes 2018, 9, 187. [Google Scholar] [CrossRef] [Green Version]
- Filipits, M.; Rudas, M.; Jakesz, R.; Dubsky, P.; Fitzal, F.; Singer, C.F.; Dietze, O.; Greil, R.; Jelen, A.; Sevelda, P.; et al. A New Molecular Predictor of Distant Recurrence in ER-Positive, HER2-Negative Breast Cancer Adds Independent Information to Conventional Clinical Risk Factors. Clin. Cancer Res. 2011, 17, 6012–6020. [Google Scholar] [CrossRef] [Green Version]
- Filipits, M.; Dubsky, P.; Rudas, M.; Greil, R.; Balic, M.; Bago-Horvath, Z.; Singer, C.F.; Hlauschek, D.; Brown, K.; Bernhisel, R.; et al. Prediction of Distant Recurrence Using EndoPredict Among Women with ER+, HER2- Node-Positive and Node-Negative Breast Cancer Treated with Endocrine Therapy Only. Clin. Cancer Res. 2019, 25, 3865–3872. [Google Scholar] [CrossRef] [Green Version]
- Naoi, Y.; Tsunashima, R.; Shimazu, K.; Noguchi, S. The Multigene Classifiers 95GC/42GC/155GC for Precision Medicine in ER-Positive HER2-Negative Early Breast Cancer. Cancer Sci. 2021, 112, 1369–1375. [Google Scholar] [CrossRef]
- Vyberg, M.; Nielsen, S.; Røge, R.; Sheppard, B.; Ranger-Moore, J.; Walk, E.; Gartemann, J.; Rohr, U.-P.; Teichgräber, V. Immunohistochemical Expression of HER2 in Breast Cancer: Socioeconomic Impact of Inaccurate Tests. BMC Health Serv. Res. 2015, 15, 352. [Google Scholar] [CrossRef] [PubMed]
- Alluri, P.; Newman, L.A. Basal-like and Triple-Negative Breast Cancers: Searching for Positives among Many Negatives. Surg. Oncol. Clin. N. Am. 2014, 23, 567–577. [Google Scholar] [CrossRef] [Green Version]
- Rakha, E.A.; Ellis, I.O. Triple-Negative/Basal-like Breast Cancer: Review. Pathology 2009, 41, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Buonomo, O.C.; Caredda, E.; Portarena, I.; Vanni, G.; Orlandi, A.; Bagni, C.; Petrella, G.; Palombi, L.; Orsaria, P. New Insights into the Metastatic Behavior after Breast Cancer Surgery, According to Well-Established Clinicopathological Variables and Molecular Subtypes. PLoS ONE 2017, 12, e0184680. [Google Scholar] [CrossRef] [Green Version]
- Van Uden, D.J.P.; van Maaren, M.C.; Strobbe, L.J.A.; Bult, P.; van der Hoeven, J.J.; Siesling, S.; de Wilt, J.H.W.; Blanken-Peeters, C.F.J.M. Metastatic Behavior and Overall Survival According to Breast Cancer Subtypes in Stage IV Inflammatory Breast Cancer. Breast Cancer Res. 2019, 21, 113. [Google Scholar] [CrossRef] [PubMed]
- Plesca, M.; Bordea, C.; El Houcheimi, B.; Ichim, E.; Blidaru, A. Evolution of radical mastectomy for breast cancer. J. Med. Life 2016, 9, 183–186. [Google Scholar]
- Karmakar, M.K.; Samy, W.; Lee, A.; Li, J.W.; Chan, W.C.; Chen, P.P.; Tsui, B.C. Survival Analysis of Patients with Breast Cancer Undergoing a Modified Radical Mastectomy with or without a Thoracic Paravertebral Block: A 5-Year Follow-up of a Randomized Controlled Trial. Anticancer. Res. 2017, 37, 5813–5820. [Google Scholar] [CrossRef]
- Salvatorelli, L.; Puzzo, L.; Vecchio, G.M.; Caltabiano, R.; Virzì, V.; Magro, G. Ductal Carcinoma In Situ of the Breast: An Update with Emphasis on Radiological and Morphological Features as Predictive Prognostic Factors. Cancers 2020, 12, 609. [Google Scholar] [CrossRef] [Green Version]
- Dereere, E.; Papadimitriou, K.; Tjalma, W.; Altintas, S. Ductal Carcinoma in Situ: A Disease Entity That Merits More Recognition. Minerva Chir. 2015, 70, 231–239. [Google Scholar]
- Altomare, V.; Guerriero, G.; Giacomelli, L.; Battista, C.; Carino, R.; Montesano, M.; Vaccaro, D.; Rabitti, C. Management of nonpalpable breast lesions in a modern functional breast unit. Breast Cancer Res. Treat. 2005, 93, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Subhedar, P.; Olcese, C.; Patil, S.; Morrow, M.; Van Zee, K.J. Decreasing Recurrence Rates for Ductal Carcinoma In Situ: Analysis of 2996 Women Treated with Breast-Conserving Surgery Over 30 Years. Ann. Surg. Oncol. 2015, 22, 3273–3281. [Google Scholar] [CrossRef] [Green Version]
- Choi, Y.J.; Shin, Y.D.; Song, Y.J. Comparison of Ipsilateral Breast Tumor Recurrence after Breast-Conserving Surgery between Ductal Carcinoma in Situ and Invasive Breast Cancer. World J. Surg. Oncol. 2016, 14, 126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Llarena, N.C.; Estevez, S.L.; Tucker, S.L.; Jeruss, J.S. Impact of Fertility Concerns on Tamoxifen Initiation and Persistence. J. Natl. Cancer Inst. 2015, 107, djv202. [Google Scholar] [CrossRef] [Green Version]
- Sella, T.; Poorvu, P.D.; Ruddy, K.J.; Gelber, S.I.; Tamimi, R.M.; Peppercorn, J.M.; Schapira, L.; Borges, V.F.; Come, S.E.; Partridge, A.H.; et al. Impact of Fertility Concerns on Endocrine Therapy Decisions in Young Breast Cancer Survivors. Cancer 2021, 127, 2888–2894. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to Build a Bridge from a Population-Based to a More “Personalized” Approach to Cancer Staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef] [PubMed]
- De Maeyer, L.; Van Limbergen, E.; De Nys, K.; Moerman, P.; Pochet, N.; Hendrickx, W.; Wildiers, H.; Paridaens, R.; Smeets, A.; Christiaens, M.-R.; et al. Does Estrogen Receptor Negative/Progesterone Receptor Positive Breast Carcinoma Exist? J. Clin. Oncol. 2008, 26, 335–336, author reply 336–338. [Google Scholar] [CrossRef] [PubMed]
- Klein, C.A. Cancer Progression and the Invisible Phase of Metastatic Colonization. Nat. Rev. Cancer 2020, 20, 681–694. [Google Scholar] [CrossRef]
- Dillekås, H.; Rogers, M.S.; Straume, O. Are 90% of Deaths from Cancer Caused by Metastases? Cancer Med. 2019, 8, 5574–5576. [Google Scholar] [CrossRef] [Green Version]
- Bedoschi, G.; Navarro, P.A.; Oktay, K. Chemotherapy-Induced Damage to Ovary: Mechanisms and Clinical Impact. Future Oncol. 2016, 12, 2333–2344. [Google Scholar] [CrossRef] [Green Version]
- Bedoschi, G.M.; Navarro, P.A.; Oktay, K.H. Novel Insights into the Pathophysiology of Chemotherapy-Induced Damage to the Ovary. Panminerva Med. 2019, 61, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Lambertini, M.; Del Mastro, L.; Pescio, M.C.; Andersen, C.Y.; Azim, H.A.; Peccatori, F.A.; Costa, M.; Revelli, A.; Salvagno, F.; Gennari, A.; et al. Cancer and Fertility Preservation: International Recommendations from an Expert Meeting. BMC Med. 2016, 14, 1. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Schover, L.R.; Partridge, A.H.; Patrizio, P.; Wallace, W.H.; Hagerty, K.; Beck, L.N.; Brennan, L.V.; Oktay, K.; American Society of Clinical Oncology. American Society of Clinical Oncology Recommendations on Fertility Preservation in Cancer Patients. J. Clin. Oncol. 2006, 24, 2917–2931. [Google Scholar] [CrossRef] [PubMed]
- Oktay, K.; Harvey, B.E.; Partridge, A.H.; Quinn, G.P.; Reinecke, J.; Taylor, H.S.; Wallace, W.H.; Wang, E.T.; Loren, A.W. Fertility Preservation in Patients with Cancer: ASCO Clinical Practice Guideline Update. J. Clin. Oncol. 2018, 36, 1994–2001. [Google Scholar] [CrossRef] [PubMed]
- Van Houten, E.L.A.F.; Themmen, A.P.N.; Visser, J.A. Anti-Müllerian Hormone (AMH): Regulator and Marker of Ovarian Function. Ann. Endocrinol. 2010, 71, 191–197. [Google Scholar] [CrossRef]
- Shrikhande, L.; Shrikhande, B.; Shrikhande, A. AMH and Its Clinical Implications. J. Obstet. Gynaecol. India 2020, 70, 337–341. [Google Scholar] [CrossRef]
- Wang, S.Y.; Wang, S. Anti-Müllerian hormone as a new marker of the ovarian reserve function preservation by goserelin during (neo)adjuvant chemotherapy for young breast cancer patients. J. Peking Univ. Health Sci. 2019, 51, 536–541. [Google Scholar] [CrossRef]
- Meirow, D.; Biederman, H.; Anderson, R.A.; Wallace, W.H.B. Toxicity of Chemotherapy and Radiation on Female Reproduction. Clin. Obstet. Gynecol. 2010, 53, 727–739. [Google Scholar] [CrossRef]
- Spears, N.; Lopes, F.; Stefansdottir, A.; Rossi, V.; De Felici, M.; Anderson, R.A.; Klinger, F.G. Ovarian Damage from Chemotherapy and Current Approaches to Its Protection. Hum. Reprod. Update 2019, 25, 673–693. [Google Scholar] [CrossRef]
- Mgboji, G.E.; Cordeiro Mitchell, C.N.; Bedrick, B.S.; Vaidya, D.; Tao, X.; Liu, Y.; Maher, J.Y.; Christianson, M.S. Predictive Factors for Fertility Preservation in Pediatric and Adolescent Girls with Planned Gonadotoxic Treatment. J. Assist. Reprod. Genet. 2021, 38, 2713–2721. [Google Scholar] [CrossRef]
- Kim, H.; Han, W.; Ku, S.Y.; Suh, C.S.; Kim, S.H.; Choi, Y.M. Feature of Amenorrhea in Postoperative Tamoxifen Users with Breast Cancer. J. Gynecol. Oncol. 2017, 28, e10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.; Kim, S.K.; Lee, J.R.; Hwang, K.J.; Suh, C.S.; Kim, S.H. Fertility Preservation for Patients with Breast Cancer: The Korean Society for Fertility Preservation Clinical Guidelines. Clin. Exp. Reprod. Med. 2017, 44, 181–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagani, O.; Partridge, A.; Peccatori, F.; Azim, H.; Colleoni, M.; Saura, C.; Kroep, J.; Warner, E.; Gombos, A.; Sætersdal, A.; et al. POSITIVE: A Study Evaluating Pregnancy, Disease Outcome and Safety of Interrupting Endocrine Therapy for Premenopausal Women with Endocrine ResponsIVE Breast Cancer Who Desire Pregnancy (IBCSG 48-14/BIG 8-13). Cancer Res. 2019, 79 (Suppl. S4), OT1-01-06. [Google Scholar]
- Pagani, O.; Ruggeri, M.; Manunta, S.; Saunders, C.; Peccatori, F.; Cardoso, F.; Kaufman, B.; Paluch-Shimon, S.; Gewefel, H.; Gallerani, E.; et al. Pregnancy after Breast Cancer: Are Young Patients Willing to Participate in Clinical Studies? Breast 2015, 24, 201–207. [Google Scholar] [CrossRef]
- Lambertini, M.; Campbell, C.; Bines, J.; Korde, L.A.; Izquierdo, M.; Fumagalli, D.; Del Mastro, L.; Ignatiadis, M.; Pritchard, K.; Wolff, A.C.; et al. Adjuvant Anti-HER2 Therapy, Treatment-Related Amenorrhea, and Survival in Premenopausal HER2-Positive Early Breast Cancer Patients. J. Natl. Cancer Inst. 2019, 111, 86–94. [Google Scholar] [CrossRef] [PubMed]
- La Rosa, V.L.; Garzon, S.; Gullo, G.; Fichera, M.; Sisti, G.; Gallo, P.; Riemma, G.; Schiattarella, A. Fertility preservation in women affected by gynaecological cancer: The importance of an integrated gynaecological and psychological approach. Ecancermedicalscience 2020, 14, 1035. [Google Scholar] [CrossRef]
- Mattiuzzi, C.; Lippi, G. Current Cancer Epidemiology. J. Epidemiol. Glob. Health 2019, 9, 217–222. [Google Scholar] [CrossRef] [Green Version]
- Yeomanson, D.J.; Morgan, S.; Pacey, A.A. Discussing Fertility Preservation at the Time of Cancer Diagnosis: Dissatisfaction of Young Females. Pediatr. Blood Cancer 2013, 60, 1996–2000. [Google Scholar] [CrossRef]
- Bedoschi, G.; Oktay, K. Current Approach to Fertility Preservation by Embryo Cryopreservation. Fertil. Steril. 2013, 99, 1496–1502. [Google Scholar] [CrossRef] [Green Version]
- Brezina, P.R.; Kutteh, W.H.; Bailey, A.P.; Ding, J.; Ke, R.W.; Klosky, J.L. Fertility Preservation in the Age of Assisted Reproductive Technologies. Obstet. Gynecol. Clin. N. Am. 2015, 42, 39–54. [Google Scholar] [CrossRef]
- Practice Committee of the American Society for Reproductive Medicine; Practice Committee of the Society for Assisted Reproductive Technology. Mature Oocyte Cryopreservation: A Guideline. Fertil. Steril. 2013, 99, 37–43. [Google Scholar] [CrossRef] [PubMed]
- ACOG. Committee Opinion No. 584: Oocyte Cryopreservation. Obstet. Gynecol. 2014, 123, 221–222. [Google Scholar] [CrossRef] [PubMed]
- Papatheodorou, A.; Vanderzwalmen, P.; Panagiotidis, Y.; Petousis, S.; Gullo, G.; Kasapi, E.; Goudakou, M.; Prapas, N.; Zikopoulos, K.; Georgiou, I.; et al. How Does Closed System Vitrification of Human Oocytes Affect the Clinical Outcome? A Prospective, Observational, Cohort, Noninferiority Trial in an Oocyte Donation Program. Fertil. Steril. 2016, 106, 1348–1355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doyle, J.O.; Richter, K.S.; Lim, J.; Stillman, R.J.; Graham, J.R.; Tucker, M.J. Successful Elective and Medically Indicated Oocyte Vitrification and Warming for Autologous in Vitro Fertilization, with Predicted Birth Probabilities for Fertility Preservation According to Number of Cryopreserved Oocytes and Age at Retrieval. Fertil. Steril. 2016, 105, 459–466.e2. [Google Scholar] [CrossRef] [Green Version]
- Gullo, G.; Petousis, S.; Papatheodorou, A.; Panagiotidis, Y.; Margioula-Siarkou, C.; Prapas, N.; D’Anna, R.; Perino, A.; Cucinella, G.; Prapas, Y. Closed vs. Open Oocyte Vitrification Methods Are Equally Effective for Blastocyst Embryo Transfers: Prospective Study from a Sibling Oocyte Donation Program. Gynecol. Obstet. Investig. 2020, 85, 206–212. [Google Scholar] [CrossRef]
- Practice Committee of the American Society for Reproductive Medicine. Evidence-Based Outcomes after Oocyte Cryopreservation for Donor Oocyte in Vitro Fertilization and Planned Oocyte Cryopreservation: A Guideline. Fertil. Steril. 2021, 116, 36–47. [Google Scholar] [CrossRef]
- Ladanyi, C.; Mor, A.; Christianson, M.S.; Dhillon, N.; Segars, J.H. Recent Advances in the Field of Ovarian Tissue Cryopreservation and Opportunities for Research. J. Assist. Reprod. Genet. 2017, 34, 709–722. [Google Scholar] [CrossRef]
- Lambertini, M.; Anserini, P.; Fontana, V.; Poggio, F.; Iacono, G.; Abate, A.; Levaggi, A.; Miglietta, L.; Bighin, C.; Giraudi, S.; et al. The PREgnancy and FERtility (PREFER) Study: An Italian Multicenter Prospective Cohort Study on Fertility Preservation and Pregnancy Issues in Young Breast Cancer Patients. BMC Cancer 2017, 17, 346. [Google Scholar] [CrossRef]
- Ives, A.; Saunders, C.; Bulsara, M.; Semmens, J. Pregnancy after Breast Cancer: Population Based Study. BMJ 2007, 334, 194. [Google Scholar] [CrossRef] [Green Version]
- Universal Declaration of Human Rights. Proclaimed by the United Nations General Assembly in Paris on 10 December 1948 (General Assembly resolution 217 A). Available online: https://www.un.org/en/about-us/universal-declaration-of-human-rights (accessed on 22 November 2021).
- European Convention on Human Rights. Signed on 4th November 1950. Effective since 3rd September 1953. Available online: https://www.echr.coe.int/Documents/Convention_ENG.pdf (accessed on 30 November 2021).
- International Conference on Human Rights. Teheran, 22 April–13 May 1968. Available online: https://undocs.org/A/CONF.32/41 (accessed on 30 November 2021).
- International Conference on Population and Development Held on 5–13 September 1994, Cairo, Egypt. Available online: https://undocs.org/en/A/CONF.171/13/Rev.1 (accessed on 30 November 2021).
- Woodruff, T.K. Oncofertility: A Grand Collaboration between Reproductive Medicine and Oncology. Reproduction 2015, 150, S1–S10. [Google Scholar] [CrossRef] [Green Version]
- AIOM-SIE-SIGU. Oncofertility Recommendations. Issued on 12 July 2016. Available online: http://www.societaitalianadiendocrinologia.it/html/pag/sie-aiom-sigo-oncofertilita.asp (accessed on 30 November 2021).
- Italian Ministry of Health. Terapie Oncologiche e Fertilità. Last Updated on 17 September 2021. Available online: https://www.salute.gov.it/portale/fertility/dettaglioContenutiFertility.jsp?id=4571&area=fertilita&menu=tutela (accessed on 30 November 2021).
- Martínez, F.; Devesa, M.; Coroleu, B.; Tur, R.; González, C.; Boada, M.; Solé, M.; Veiga, A.; Barri, P.N. Cancer and Fertility Preservation: Barcelona Consensus Meeting. Gynecol. Endocrinol. 2013, 29, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Arecco, L.; Perachino, M.; Damassi, A.; Latocca, M.M.; Soldato, D.; Vallome, G.; Parisi, F.; Razeti, M.G.; Solinas, C.; Tagliamento, M.; et al. Burning Questions in the Oncofertility Counseling of Young Breast Cancer Patients. Breast Cancer 2020, 14, 1178223420954179. [Google Scholar] [CrossRef] [PubMed]
- Zaami, S.; Montanari Vergallo, G.; Moscatelli, M.; Napoletano, S.; Sernia, S.; La Torre, G. Oncofertility: The importance of counseling for fertility preservation in cancer patients. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 6874–6880. [Google Scholar] [CrossRef] [PubMed]
- Runco, D.V.; Taylor, J.F.; Helft, P.R. Ethical Barriers in Adolescent Oncofertility Counseling. J. Pediatr. Hematol. Oncol. 2017, 39, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Schover, L.R.; Rybicki, L.A.; Martin, B.A.; Bringelsen, K.A. Having Children after Cancer. A Pilot Survey of Survivors’ Attitudes and Experiences. Cancer 1999, 86, 697–709. [Google Scholar] [CrossRef]
- Campbell, J.E.; Assanasen, C.; Robinson, R.D.; Knudtson, J.F. Fertility Preservation Counseling for Pediatric and Adolescent Cancer Patients. J. Adolesc. Young Adult Oncol. 2016, 5, 58–63. [Google Scholar] [CrossRef]
- Jungheim, E.S.; Carson, K.R.; Brown, D. Counseling and Consenting Women with Cancer on Their Oncofertility Options: A Clinical Perspective. Cancer Treat. Res. 2010, 156, 403–412. [Google Scholar] [CrossRef] [Green Version]
- Dolmans, M.-M. Recent Advances in Fertility Preservation and Counseling for Female Cancer Patients. Expert Rev. Anticancer Ther. 2018, 18, 115–120. [Google Scholar] [CrossRef]
- Smith, K.L.; Gracia, C.; Sokalska, A.; Moore, H. Advances in Fertility Preservation for Young Women with Cancer. Am. Soc. Clin. Oncol. Educ. Book 2018, 38, 27–37. [Google Scholar] [CrossRef]
- Hohmann, C.; Borgmann-Staudt, A.; Rendtorff, R.; Reinmuth, S.; Holzhausen, S.; Willich, S.N.; Henze, G.; Goldbeck, L.; Keil, T. Patient Counselling on the Risk of Infertility and Its Impact on Childhood Cancer Survivors: Results from a National Survey. J. Psychosoc. Oncol. 2011, 29, 274–285. [Google Scholar] [CrossRef]
- Del-Pozo-Lérida, S.; Salvador, C.; Martínez-Soler, F.; Tortosa, A.; Perucho, M.; Giménez-Bonafé, P. Preservation of Fertility in Patients with Cancer (Review). Oncol. Rep. 2019, 41, 2607–2614. [Google Scholar] [CrossRef] [PubMed]
- Logan, S.; Anazodo, A. The Psychological Importance of Fertility Preservation Counseling and Support for Cancer Patients. Acta Obstet. Gynecol. Scand. 2019, 98, 583–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hill, K.A.; Nadler, T.; Mandel, R.; Burlein-Hall, S.; Librach, C.; Glass, K.; Warner, E. Experience of Young Women Diagnosed with Breast Cancer Who Undergo Fertility Preservation Consultation. Clin. Breast Cancer 2012, 12, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Biglia, N.; Torrisi, R.; D’Alonzo, M.; Codacci Pisanelli, G.; Rota, S.; Peccatori, F.A. Attitudes on Fertility Issues in Breast Cancer Patients: An Italian Survey. Gynecol. Endocrinol. 2015, 31, 458–464. [Google Scholar] [CrossRef]
- Abe, A.; Kuwahara, A.; Iwasa, T.; Nishimura, M.; Irahara, M. A Survey on Fertility Management in Young Women of Reproductive Age Treated with Chemotherapy. Int. J. Clin. Oncol. 2016, 21, 1183–1190. [Google Scholar] [CrossRef]
- Benedict, C.; Shuk, E.; Ford, J.S. Fertility Issues in Adolescent and Young Adult Cancer Survivors. J. Adolesc. Young Adult Oncol. 2016, 5, 48–57. [Google Scholar] [CrossRef] [Green Version]
- Schüring, A.N.; Fehm, T.; Behringer, K.; Goeckenjan, M.; Wimberger, P.; Henes, M.; Henes, J.; Fey, M.F.; von Wolff, M. Practical Recommendations for Fertility Preservation in Women by the FertiPROTEKT Network. Part I: Indications for Fertility Preservation. Arch. Gynecol. Obstet. 2018, 297, 241–255. [Google Scholar] [CrossRef] [Green Version]
- Von Wolff, M.; Germeyer, A.; Liebenthron, J.; Korell, M.; Nawroth, F. Practical Recommendations for Fertility Preservation in Women by the FertiPROTEKT Network. Part II: Fertility Preservation Techniques. Arch. Gynecol. Obstet. 2018, 297, 257–267. [Google Scholar] [CrossRef] [Green Version]
- Ueda, M.; Martins, R.; Hendrie, P.C.; McDonnell, T.; Crews, J.R.; Wong, T.L.; McCreery, B.; Jagels, B.; Crane, A.; Byrd, D.R.; et al. Managing Cancer Care During the COVID-19 Pandemic: Agility and Collaboration Toward a Common Goal. J. Natl. Compr. Canc. Netw. 2020, 18, 366–369. [Google Scholar] [CrossRef] [Green Version]
- Sirohi, B.; Rohatgi, T.B.; Lambertini, M. Oncofertility and COVID-19-Cancer Does Not Wait. Ecancermedicalscience 2020, 14, ed101. [Google Scholar] [CrossRef]
- ESMO/ASCO Task Force on Global Curriculum in Medical Oncology; Hansen, H.H.; Bajorin, D.F.; Muss, H.B.; Purkalne, G.; Schrijvers, D.; Stahel, R. Recommendations for a Global Core Curriculum in Medical Oncology. JCO 2004, 22, 4616–4625. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, N. Clinical Practice Guidelines for Fertility Preservation in Pediatric, Adolescent, and Young Adults with Cancer. Int. J. Clin. Oncol. 2019, 24, 20–27. [Google Scholar] [CrossRef] [PubMed]
- La Rosa, V.L.; Valenti, G.; Sapia, F.; Gullo, G.; Rapisarda, A.M.C. Psychological impact of gynecological diseases: The importance of a multidisciplinary approach. Ital. J. Gynaecol. Obstet. 2018, 30, 23–26. [Google Scholar]
- Wang, Y.; Logan, S.; Stern, K.; Wakefield, C.E.; Cohn, R.J.; Agresta, F.; Jayasinghe, Y.; Deans, R.; Segelov, E.; McLachlan, R.I.; et al. Supportive Oncofertility Care, Psychological Health and Reproductive Concerns: A Qualitative Study. Support Care Cancer 2020, 28, 809–817. [Google Scholar] [CrossRef] [PubMed]
- Legislative Decree 101/2018 Which Adapts Legislative Decree 196/2003 to the Provisions of Regulation (EU) 2016/679-GDPR. Available online: https://www.gazzettaufficiale.it/eli/id/2018/09/04/18G00129/SG (accessed on 29 November 2021).
- Fabi, A.; Lanzetta, G.; Vizza, E.; Corsi, D.; Moscetti, L.; Spinelli, G.; Mentuccia, L.; Lalle, M.; Perrone, M.; Baiocco, L.; et al. The Unmet Need for Oncofertility Preservation in Women: Results of a Survey by Different Oncological Specialists in Lazio, Italy. Curr. Probl. Cancer 2019, 43, 100479. [Google Scholar] [CrossRef] [PubMed]
- Italian National Committee for Bioethics. Information and Consent to Medical Procedures. 1992. Available online: http://www.dentistimadonnabianca.it/documents/03bis.InformazioneConsenso.CNB1992.pdf (accessed on 21 November 2021).
- Law n. 219 “Norme in Materia di Consenso Informato e di Disposizioni Anticipate di Trattamento” (Norms Governing Informed Consent and Advance Health Care Directives). Enacted by the Italian Parliament on 22 December 2017. Available online: https://www.trovanorme.salute.gov.it/norme/dettaglioAtto?id=62663 (accessed on 22 November 2021).
- Constitution of the Italian Republic. Passed on 27 December 1947. Available online: https://www.senato.it/documenti/repository/istituzione/costituzione_inglese.pdf (accessed on 22 November 2021).
- Italian Medical Code of Ethics. Last Updated 15 December 2017. Available online: https://portale.fnomceo.it/wp-content/uploads/2018/03/CODICE-DEONTOLOGIA-MEDICA-2014.pdf (accessed on 22 November 2021).
- Zaami, S.; Montanari Vergallo, G.; Napoletano, S.; Signore, F.; Marinelli, E. The issue of delivery room infections in the Italian law. A brief comparative study with English and French jurisprudence. J. Matern. Fetal Neonatal. Med. 2018, 31, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Satyanarayana Rao, K.H. Informed Consent: An Ethical Obligation or Legal Compulsion? J. Cutan. Aesthet. Surg. 2008, 1, 33–35. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Sample Characteristics | |
|---|---|
| Inclusion Criteria | Exclusion Criteria |
| Age ≤ 40 (ultimate average age was 36.15; standard deviation: 3.0) | Previous diagnosis of malignancy, breast or otherwise |
| Diagnosed between 2014 and 2021 | Previous diagnosis of metastatic disease [86,87] |
| History of neoadjuvant or adjuvant chemotherapy or hormone therapy | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaami, S.; Melcarne, R.; Patrone, R.; Gullo, G.; Negro, F.; Napoletano, G.; Monti, M.; Aceti, V.; Panarese, A.; Borcea, M.C.; et al. Oncofertility and Reproductive Counseling in Patients with Breast Cancer: A Retrospective Study. J. Clin. Med. 2022, 11, 1311. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11051311
Zaami S, Melcarne R, Patrone R, Gullo G, Negro F, Napoletano G, Monti M, Aceti V, Panarese A, Borcea MC, et al. Oncofertility and Reproductive Counseling in Patients with Breast Cancer: A Retrospective Study. Journal of Clinical Medicine. 2022; 11(5):1311. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11051311
Chicago/Turabian StyleZaami, Simona, Rossella Melcarne, Renato Patrone, Giuseppe Gullo, Francesca Negro, Gabriele Napoletano, Marco Monti, Valerio Aceti, Alessandra Panarese, Maria Carola Borcea, and et al. 2022. "Oncofertility and Reproductive Counseling in Patients with Breast Cancer: A Retrospective Study" Journal of Clinical Medicine 11, no. 5: 1311. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11051311