
Comparison in Short-Term Safety and Efficacy between New-Generation WATCHMAN FLX and Conventional WATCHMAN 2.5 for Percutaneous Left Atrial Appendage Closure

 , , and
, , and
Abstract
:1. Background
2. Methods
2.1. Patient Selection
2.2. Procedures
2.3. Post-Procedure Management
2.4. Study Outcome
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
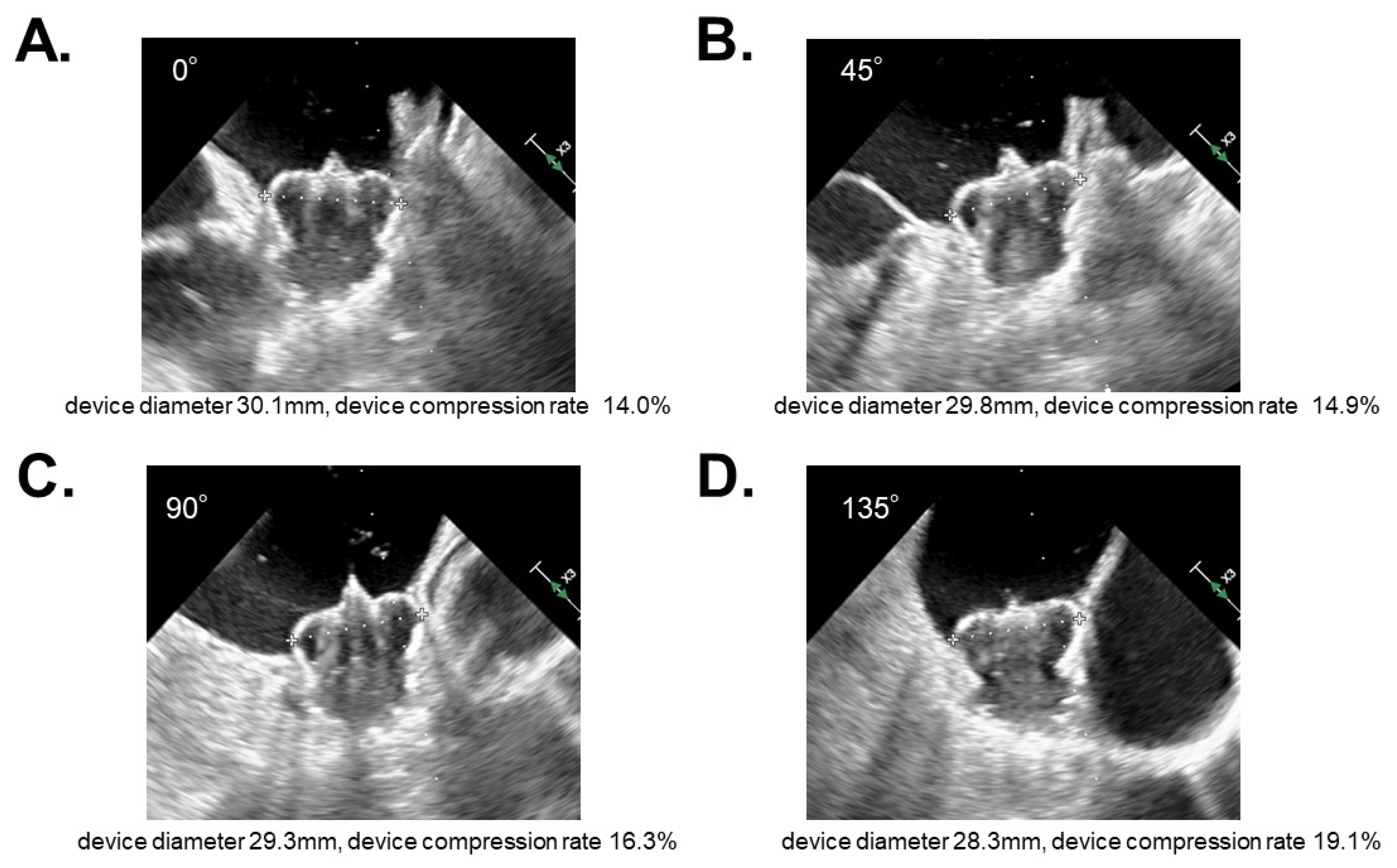
3.2. Procedure Data
3.3. Echocardiographic Follow-Up Data
3.4. Clinical Events
4. Discussion
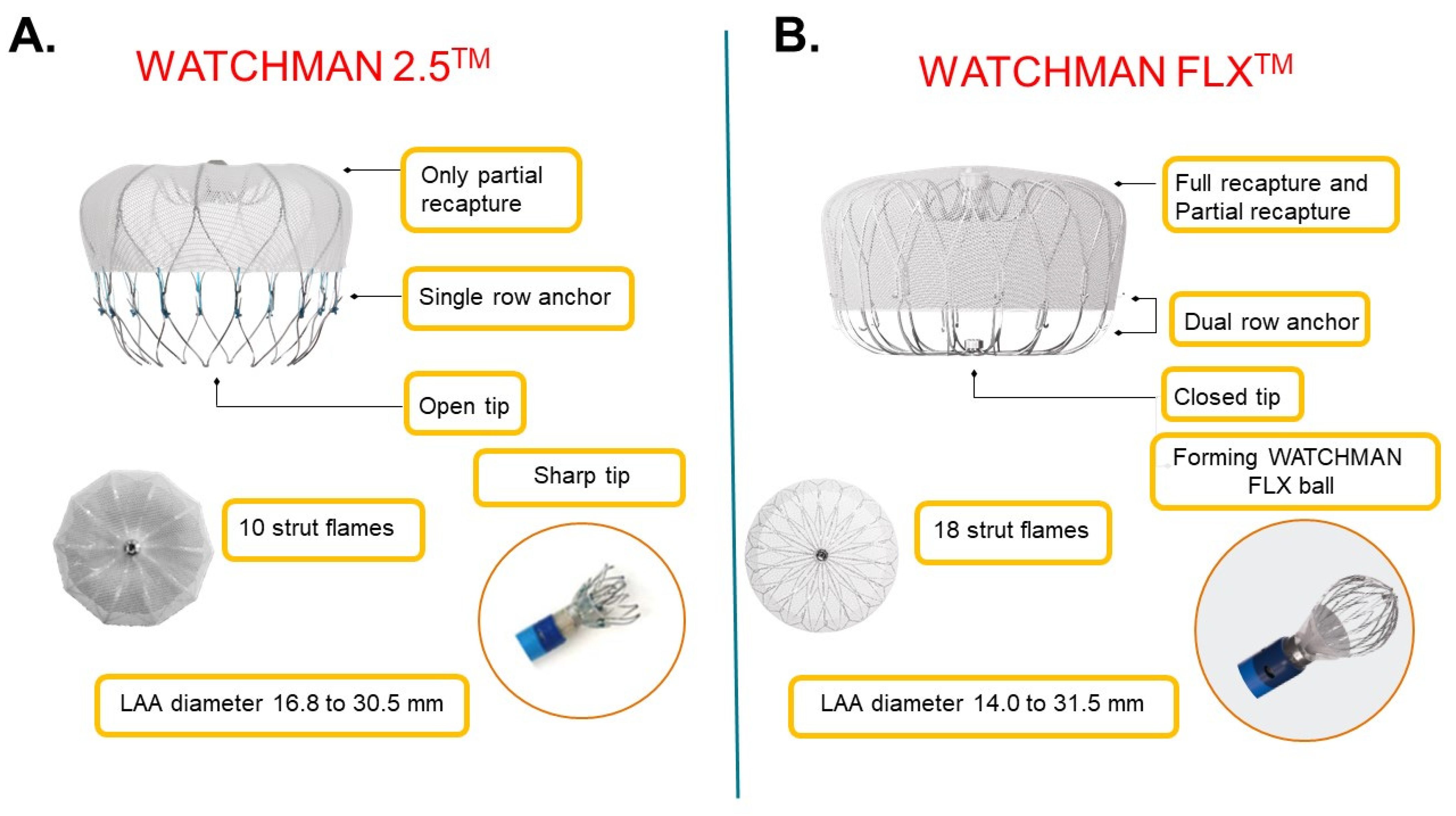
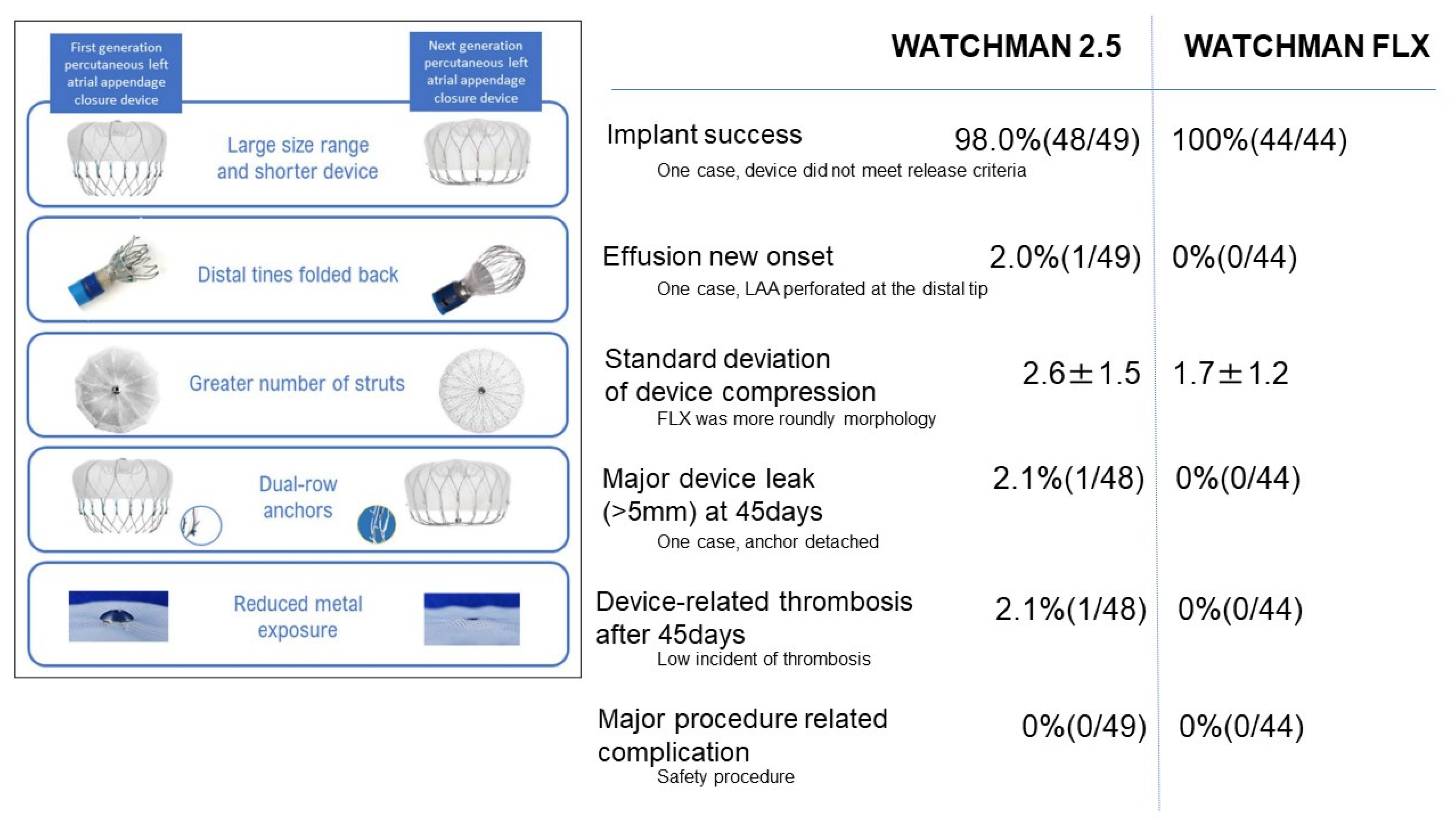
4.1. Innovation of New-Generation WATCHMAN FLX
4.2. Procedure-Related Complication
4.3. Short-Term Outcomes
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wolf, P.A.; Abbott, R.D.; Kannel, W.B. Atrial fibrillation as an independent risk factor for stroke: The Framingham Study. Stroke 1991, 22, 983–988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blackshear, J.L.; Odell, J.A. Appendage obliteration to reduce stroke in cardiac surgical patients with atrial fibrillation. Ann. Thorac. Surg. 1996, 61, 755–759. [Google Scholar] [CrossRef]
- January, C.T.; Wann, L.S.; Calkins, H.; Chen, L.Y.; Cigarroa, J.E.; Cleveland, J.C., Jr.; Ellinor, P.T., Jr.; Ezekowitz, M.D.; Field, M.E.; Furie, K.L.; et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients with Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in Collaboration with the Society of Thoracic Surgeons. Circulation 2019, 140, e125–e151. [Google Scholar] [CrossRef] [PubMed]
- Hart, R.G.; Pearce, L.; Aguilar, M.I. Meta-analysis: Antithrombotic Therapy to Prevent Stroke in Patients Who Have Nonvalvular Atrial Fibrillation. Ann. Intern. Med. 2007, 146, 857–867. [Google Scholar] [CrossRef] [PubMed]
- Holmes, D.R., Jr.; Kar, S.; Price, M.J.; Whisenant, B.; Sievert, H.; Doshi, S.K.; Huber, K.; Reddy, V.Y. Prospective randomized evaluation of the Watchman Left Atrial Appendage Closure device in patients with atrial fibrillation versus long-term warfarin therapy: The PREVAIL trial. J. Am. Coll. Cardiol. 2014, 64, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holmes, D.R.; Reddy, V.; Turi, Z.G.; Doshi, S.K.; Sievert, H.; Buchbinder, M.; Mullin, C.M.; Sick, P. Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fibrillation: A randomised non-inferiority trial. Lancet 2009, 374, 534–542. [Google Scholar] [CrossRef]
- Osmancik, P.; Herman, D.; Neuzil, P.; Hala, P.; Taborsky, M.; Kala, P.; Poloczek, M.; Stasek, J.; Haman, L.; Branny, M.; et al. Left Atrial Appendage Closure Versus Direct Oral Anticoagulants in High-Risk Patients with Atrial Fibrillation. J. Am. Coll. Cardiol. 2020, 75, 3122–3135. [Google Scholar] [CrossRef] [PubMed]
- Reddy, V.Y.; Holmes, D.; Doshi, S.K.; Neuzil, P.; Kar, S. Safety of percutaneous left atrial appendage closure: Results from the watchman left atrial appendage system for embolic protection in patients with AF (PROTECT AF) clinical trial and the continued access registry. Circulation 2011, 123, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Holmes, D.R.; Doshi, S.K.; Kar, S.; Price, M.J.; Sanchez, J.M.; Sievert, H.; Valderrabano, M.; Reddy, V.Y. Left Atrial Appendage Closure as an Alternative to Warfarin for Stroke Prevention in Atrial Fibrillation: A Patient-Level Meta-Analysis. J. Am. Coll. Cardiol. 2015, 65, 2614–2623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boersma, L.V.; Ince, H.; Kische, S.; Pokushalov, E.; Schmitz, T.; Schmidt, B.; Gori, T.; Meincke, F.; Protopopov, A.; Betts, T.; et al. Efficacy and safety of left atrial appendage closure with WATCHMAN in patients with or without contraindication to oral anticoagulation: 1-Year follow-up outcome data of the EWOLUTION trial. Heart Rhythm 2017, 14, 1302–1308. [Google Scholar] [CrossRef] [Green Version]
- Aonuma, K.; Yamasaki, H.; Nakamura, M.; Matsumoto, T.; Takayama, M.; Ando, K.; Hirao, K.; Goya, M.; Morino, Y.; Hayashida, K.; et al. Efficacy and Safety of Left Atrial Appendage Closure with WATCHMAN in Japanese Nonvalvular Atrial Fibrillation Patients―Final 2-Year Follow-Up Outcome Data from the SALUTE Trial. Circ. J. 2020, 84, 1237–1243. [Google Scholar] [CrossRef] [PubMed]
- Kar, S.; Doshi, S.K.; Sadhu, A.; Horton, R.; Osorio, J.; Ellis, C.; Stone, J., Jr.; Shah, M.; Dukkipati, S.R.; Adler, S.; et al. Primary outcome evaluation of a next generation left atrial appendage closure device: Results from the PINNACLE FLX trial. Circulation 2021, 143, 1754–1762. [Google Scholar] [CrossRef] [PubMed]
- Nogami, A.; Kurita, T.; Kusano, K.; Goya, M.; Shoda, M.; Tada, H.; Naito, S.; Yamane, T.; Kimura, M.; Shiga, T.; et al. JCS/JHRS 2021 Guideline Focused Update on Non-Pharmacotherapy of Cardiac Arrhythmias. Circ. J. 2022, 86, 337–363. [Google Scholar] [CrossRef] [PubMed]
- Ono, K.; Iwasaki, Y.; Shimizu, W.; Akao, M.; Ikeda, T.; Ishii, K.; Inden, Y.; Kusano, K.; Kobayashi, Y.; Koretsune, Y. JCS/JHRS 2020 Guideline on Pharmacotherapy of Cardiac Arrhythmias. Circ. J. 2022. [Google Scholar] [CrossRef]
- Cruz-González, I.; Korsholm, K.; Trejo-Velasco, B.; Thambo, J.B.; Mazzone, P.; Rioufol, G.; Grygier, M.; Möbius-Winkler, S.; Betts, T.; Meincke, F.; et al. Procedural and Short-Term Results with the New Watchman FLX left atrial appendage occlusion device. J. Am. Coll. Cardiol. Interv. 2020, 13, 2732–2741. [Google Scholar] [CrossRef] [PubMed]
- Korsholm, K.; Samaras, A.; Andersen, A.; Møller Jensen, J.; Nielsen-Kudsk, J.E. The Watchman FLX Device: First European Experience and Feasibility of Intracardiac Echocardiography to Guide Implantation. J. Am. Coll. Cardiol. 2020, 6, 1633–1642. [Google Scholar]
- Cruz-González, I.; Torres Saura, F.; Trejo-Velasco, B.; Antonio Fernández Díaz, J.; Fajardo Molina, R.; Del Valle-Fernández, R.; Moreno Terribas, G.; Martí Sánchez, D.; López-Mínguez, J.R.; Gomez-Blazquez, I.; et al. Impact of operators experience on peri-procedural outcomes with Watchman FLX: Insights from the FLX-SPA registry. Int. J. Cardiol. Heart Vasc. 2022, 38, 100941. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 93) | WATCHMAN 2.5 (n = 49) | WATCHMAN FLX (n = 44) | p Value | |
|---|---|---|---|---|
| Demographics | ||||
| Sex, male | 63 (68) | 36 (74) | 27 (61) | 0.21 |
| Age (years) | 73.0 ± 7.3 | 76.4 ± 7.4 | 80.8 ± 6.6 | <0.01 * |
| Body mass index (kg/m2) | 23.3 ± 3.5 | 24.0 ± 3.2 | 22.5 ± 3.8 | 0.049 * |
| Body surface area (m2) | 1.58 ± 0.17 | 1.62 ± 0.17 | 1.54 ± 0.16 | 0.035 * |
| Comorbidity | ||||
| Heart failure | 56 (60) | 28 (57) | 28 (64) | 0.53 |
| New York Heart Association class II-IV | 49 (53) | 22 (45) | 27 (61) | 0.12 |
| Hypertension | 75 (81) | 40 (82) | 35 (80) | 0.82 |
| Diabetes mellitus | 28 (30) | 17 (35) | 11 (25) | 0.31 |
| Prior stroke or transient ischemia attach | 49 (53) | 29 (59) | 20 (45) | 0.19 |
| Prior ischemic stroke | 35 (38) | 20 (41) | 15 (34) | 0.51 |
| Prior hemorrhagic stroke | 13 (14) | 9 (18) | 4 (9) | 0.20 |
| Prior transient ischemic attack | 5 (5) | 4 (8) | 1 (2) | 0.20 |
| Prior thromboembolic events | 20 (22) | 13 (27) | 7 (16) | 0.22 |
| Hyperlipidemia | 45 (48) | 23 (46) | 22 (50) | 0.77 |
| Coronary artery disease | 30 (32) | 17 (35) | 13 (30) | 0.60 |
| Chronic obstructive pulmonary disease | 2 (2) | 0 (0) | 2 (5) | 0.16 |
| Peripheral arterial disease | 9 (10) | 8 (16) | 1 (2) | 0.018 * |
| Chronic dialysis | 22 (24) | 17 (34) | 5 (11) | <0.01 * |
| Paroxysmal atrial fibrillation | 34 (37) | 20 (41) | 14 (32) | 0.37 |
| Prior intervention | ||||
| Prior myocardial infarction | 8 (9) | 6 (12) | 2 (5) | 0.19 |
| Prior percutaneous coronary intervention | 29 (31) | 17 (35) | 12 (27) | 0.45 |
| Prior coronary artery bypass grafting | 6 (7) | 5 (10) | 1 (2) | 0.12 |
| Scores | ||||
| CHADS2 score | 3.3 ± 1.4 | 3.2 ± 1.4 | 3.4 ± 1.4 | 0.54 |
| CHA2DS2-VASc score | 4.9 ± 1.5 | 4.9 ± 1.6 | 4.9 ± 1.4 | 0.76 |
| HAS-BLED score | 3.0 ± 0.9 | 3.2 ± 1.0 | 2.8 ± 0.8 | <0.01 * |
| History of relevant bleeding | ||||
| Total | 44 (47) | 29 (59) | 15 (34) | <0.01 * |
| Intracranial | 21 (22) | 11 (22) | 10 (22) | 0.98 |
| Gastrointestinal | 18 (19) | 13 (27) | 5 (11) | 0.06 |
| Hematuria | 3 (3) | 1 (2) | 2 (4) | 0.35 |
| Respiratory | 2 (2) | 2 (4) | 0 (0) | 0.16 |
| Epistaxis | 2 (2) | 2 (4) | 0 (0) | 0.16 |
| Transthoracic echocardiography | ||||
| Left atrial diameter (mm) | 43.7 ± 8.5 | 47.4 ± 9.2 | 46.5 ± 7.7 | 0.58 |
| Left atrial volume index (ml/m2) | 59.0 ± 23.4 | 63.3 ± 26.5 | 54.3 ± 18.8 | 0.07 |
| Left ventricular end-diastolic diameter (mm) | 47.9 ± 7.6 | 48.6 ± 8.1 | 47.2 ± 6.8 | 0.40 |
| Left ventricular ejection fraction (%) | 58.9 ± 13.5 | 56.6 ± 12.2 | 61.4 ± 14.6 | 0.09 |
| Anti-platelet/anti-coagulant therapy at baseline | ||||
| None | 1 (1) | 0 (0) | 1 (2) | 0.32 |
| Any SAPT | 3 (3) | 0 (0) | 3 (7) | 0.08 |
| Any DAPT | 3 (3) | 1 (2) | 2 (5) | 0.50 |
| Any single anti-coagulant therapy | 55 (59) | 28 (57) | 27 (61) | 0.68 |
| Warfarin | 11 (12) | 9 (18) | 2 (5) | 0.035 * |
| DOAC | 44 (47) | 19 (39) | 25 (57) | 0.08 |
| Any SAPT and anti-coagulant therapy | 31 (33) | 20 (41) | 11 (25) | 0.11 |
| Any SAPT and Warfarin | 13 (14) | 12 (24) | 1 (2) | <0.01 * |
| Any SAPT and DOAC | 18 (19) | 8 (16) | 10 (23) | 0.44 |
| Any DAPT and anti-coagulant (triple therapy) | 0 (0) | 0 (0) | 0 (0) | - |
| WATCHMAN 2.5 (n = 49) | WATCHMAN FLX (n = 44) | p Value | |
|---|---|---|---|
| General procedure data | |||
| Procedure success | 48 (98) | 44 (100) | 0.25 |
| General anesthesia | 49 (100) | 44 (100) | 1.0 |
| Transesophageal echocardiography | 49 (100) | 44 (100) | 1.0 |
| Concomitant procedure | 10 (20) | 6 (14) | 0.66 |
| Procedure-related data | |||
| Anesthesia time (min) | 127 ± 31 | 127 ± 39 | 0.91 |
| Fluoroscopy duration (min) | 18 ± 10 | 17 ± 12 | 0.82 |
| Procedure time (min) | 63 ± 18 | 55 ± 20 | 0.047 * |
| Contrast volume (ml) | 69 ± 23 | 76 ± 38 | 0.32 |
| Left atrial appendage ostium diameter | |||
| 0 degree (mm) | 20.9 ± 3.8 | 21.3 ± 4.0 | 0.60 |
| 45 degrees (mm) | 19.4 ± 3.5 | 20.6 ± 3.9 | 0.13 |
| 90 degrees (mm) | 20.1 ± 3.7 | 21.5 ± 4.0 | 0.09 |
| 135 degrees (mm) | 23.0 ± 4.0 | 23.0 ± 3.9 | 0.98 |
| Device size | |||
| WATCHMAN 2.5 21/24/27/30/33 mm | 2/1/11/11/23 | - | - |
| WATCHMAN FLX 20/24/27/31/35 mm | - | 2/4/12/14/11 | - |
| Device compression rate | |||
| 0 degree (%) | 16.8 ± 7.0 | 15.2 ± 5.2 | 0.22 |
| 45 degrees (%) | 18.6 ± 5.8 | 15.4 ± 5.5 | <0.01 * |
| 90 degrees (%) | 17.3 ± 6.7 | 14.3 ± 4.7 | 0.018 * |
| 135 degrees (%) | 14.4 ± 5.8 | 14.8 ± 5.7 | 0.72 |
| Standard deviation of device compression at 4 angles | 2.6 ± 1.5 | 1.7 ± 1.2 | <0.01 * |
| Peri-device leak | |||
| <3 mm | 0 (0) | 0 (0) | - |
| 3–5 mm | 0 (0) | 0 (0) | - |
| >5 mm | 0 (0) | 0 (0) | - |
| Medications at index discharge | |||
| None | 0 (0) | 0 (0) | - |
| Any SAPT | 0 (0) | 0 (0) | - |
| Any DAPT | 0 (0) | 0 (0) | - |
| Any single anti-coagulant therapy | 8 (16) | 9 (20) | 0.6 |
| Warfarin | 1 (2) | 0 (0) | 0.35 |
| DOAC | 7 (15) | 9 (20) | 0.44 |
| Any SAPT and anti-coagulant therapy | 41 (85) | 35 (80) | 0.41 |
| Any SAPT and Warfarin | 22 (46) | 3 (6) | <0.01 * |
| Any SAPT and DOAC | 19 (40) | 32 (72) | <0.01 * |
| Any DAPT and anti-coagulant (triple therapy) | 0 (0) | 0 (0) | - |
| WATCHMAN 2.5 (n = 48) | WATCHMAN FLX (n = 43) | p Value | |
|---|---|---|---|
| Transesophageal echocardiography | |||
| Procedure completion | 45 (93) | 39 (91) | 0.61 |
| Device compression rate | |||
| 0 degree (%) | 13.2 ± 6.6 | 12.4 ± 5.4 | 0.56 |
| 45 degrees (%) | 15.1 ± 6.5 | 13.7 ± 6.7 | 0.36 |
| 90 degrees (%) | 14.9 ± 6.2 | 12.1 ± 5.5 | 0.05 |
| 135 degrees (%) | 12.7 ± 5.9 | 13.0 ± 5.9 | 0.80 |
| Standard deviation of device compression at 4 angles | 2.8 ± 1.1 | 2.9 ± 1.3 | 0.60 |
| Peri-device leak | |||
| <3 mm | 8 (18) | 6 (15) | 0.77 |
| 3–5 mm | 1 (2) | 0 (0) | 0.36 |
| >5 mm | 1 (2) | 0 (0) | 0.36 |
| Device-related thrombosis | 1 (2) | 0 (0) | 0.36 |
| Medications | |||
| None | 0 (0) | 0 (0) | - |
| Any SAPT | 5 (10) | 6 (14) | 0.61 |
| Any DAPT | 36 (75) | 32 (74) | 0.95 |
| Any single anti-coagulant therapy | 6 (13) | 3 (7) | 0.38 |
| Warfarin | 0 (0) | 0 (0) | - |
| DOAC | 6 (13) | 3 (7) | 0.38 |
| Any SAPT and anti-coagulant therapy | 1 (2) | 2 (5) | 0.50 |
| Any SAPT and Warfarin | 1 (2) | 0 (0) | 0.35 |
| Any SAPT and DOAC | 0 (0) | 2 (5) | 0.16 |
| Any DAPT and anti-coagulant (triple therapy) | 0 (0) | 0 (0) | - |
| WATCHMAN 2.5 (n = 49) | WATCHMAN FLX (n = 44) | p Value | |
|---|---|---|---|
| Procedure related events | 1 (2) | 0 (0) | 0.35 |
| Major procedure related complication | 0 (0) | 0 (0) | - |
| Death | 0 (0) | 0 (0) | - |
| Cerebrovascular events | 0 (0) | 0 (0) | - |
| Systemic embolism | 0 (0) | 0 (0) | - |
| Air embolism | 0 (0) | 0 (0) | - |
| Any bleeding | 0 (0) | 0 (0) | - |
| Minor bleeding BARC 1–2 | 0 (0) | 0 (0) | - |
| Major bleeding BARC 3–5 | 0 (0) | 0 (0) | - |
| Pericardial effusion new onset | 1 (2) | 0 (0) | 0.35 |
| Clinically non-relevant | 1 (2) | 0 (0) | 0.35 |
| Clinically relevant | 0 (0) | 0 (0) | - |
| Vascular access site complication | 0 (0) | 0 (0) | - |
| Acute kidney injury | 0 (0) | 0 (0) | - |
| Non procedure related events | |||
| Death | 0 (0) | 0 (0) | - |
| Cardiovascular death | 0 (0) | 0 (0) | - |
| Cardiovascular event | 0 (0) | 0 (0) | - |
| Systemic embolism | 0 (0) | 0 (0) | - |
| Any bleeding | 1 (2) | 0 (0) | 0.35 |
| Minor bleeding BARC 1–2 | 0 (0) | 0 (0) | - |
| Major bleeding BARC 3–5 | 1 (2) | 0 (0) | 0.35 |
| All clinical events at 45-day follow-up | |||
| Death | 0 (0) | 1 (2) | 0.32 |
| Cardiovascular death | 0 (0) | 1 (2) | 0.32 |
| Cerebrovascular event | 0 (0) | 0 (0) | - |
| Stroke | 0 (0) | 0 (0) | - |
| Ischemic stroke | 0 (0) | 0 (0) | - |
| Hemorrhagic stroke | 0 (0) | 0 (0) | - |
| Transient ischemic attack | 0 (0) | 0 (0) | - |
| Systemic embolism | 0 (0) | 0 (0) | |
| Myocardial infarction | 0 (0) | 1 (2) | 0.32 |
| Any bleeding | 3 (6) | 2 (5) | 0.74 |
| Minor bleeding BARC 1–2 | 0 (0) | 1 (2) | 0.32 |
| Major bleeding BARC 3–5 | 3 (6) | 1 (2) | 0.37 |
| Pericardial effusion new onset | 0 (0) | 0 (0) | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fukuda, N.; Imamura, T.; Tanaka, S.; Kataoka, N.; Ushijima, R.; Ueno, H.; Kinugawa, K. Comparison in Short-Term Safety and Efficacy between New-Generation WATCHMAN FLX and Conventional WATCHMAN 2.5 for Percutaneous Left Atrial Appendage Closure. J. Clin. Med. 2022, 11, 1618. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11061618
Fukuda N, Imamura T, Tanaka S, Kataoka N, Ushijima R, Ueno H, Kinugawa K. Comparison in Short-Term Safety and Efficacy between New-Generation WATCHMAN FLX and Conventional WATCHMAN 2.5 for Percutaneous Left Atrial Appendage Closure. Journal of Clinical Medicine. 2022; 11(6):1618. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11061618
Chicago/Turabian StyleFukuda, Nobuyuki, Teruhiko Imamura, Shuhei Tanaka, Naoya Kataoka, Ryuichi Ushijima, Hiroshi Ueno, and Koichiro Kinugawa. 2022. "Comparison in Short-Term Safety and Efficacy between New-Generation WATCHMAN FLX and Conventional WATCHMAN 2.5 for Percutaneous Left Atrial Appendage Closure" Journal of Clinical Medicine 11, no. 6: 1618. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11061618