
Hepatitis B Core-Related Antigen Is Useful for Predicting Phase and Prognosis of Hepatitis B e Antigen-Positive Patients


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Definition of the CHB Phase
2.3. Clinical Evaluation and Follow-Up
2.4. Liver Biopsy
2.5. Laboratory Assays
2.6. Outcomes
2.7. Statistical Analysis
3. Results
3.1. Patient Characteristics
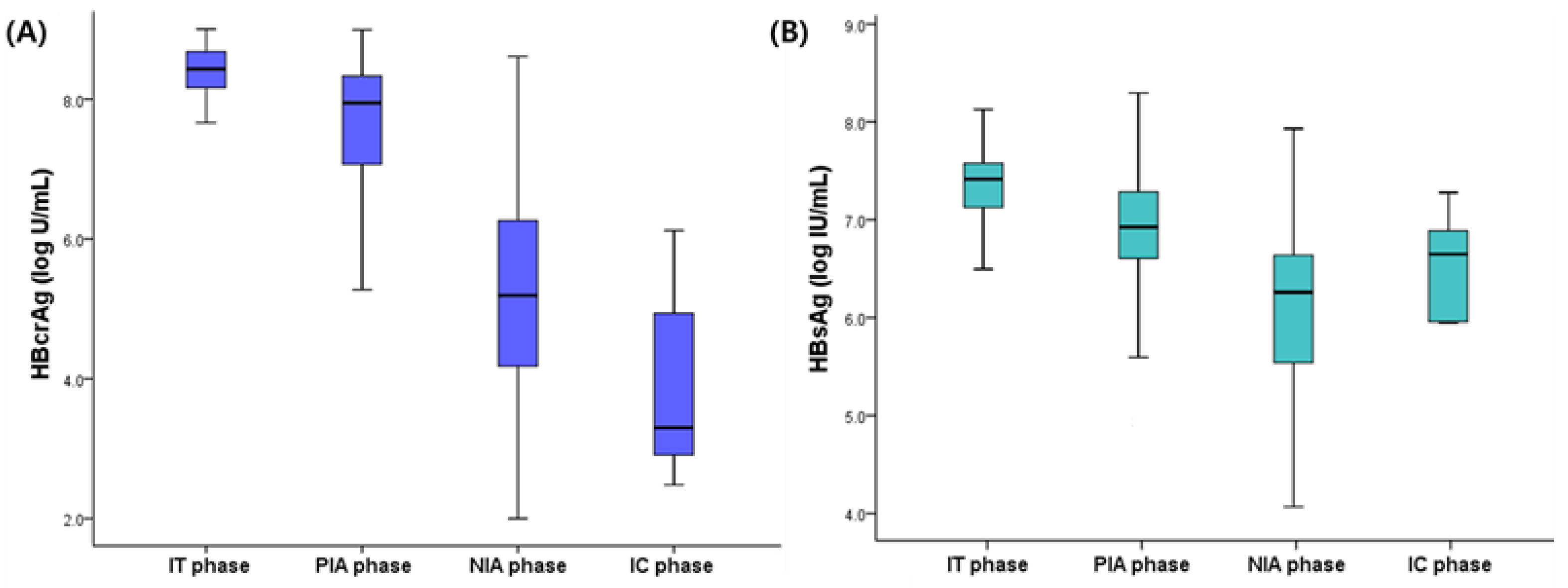
3.2. Hepatitis B e Antigen-Positive Patients
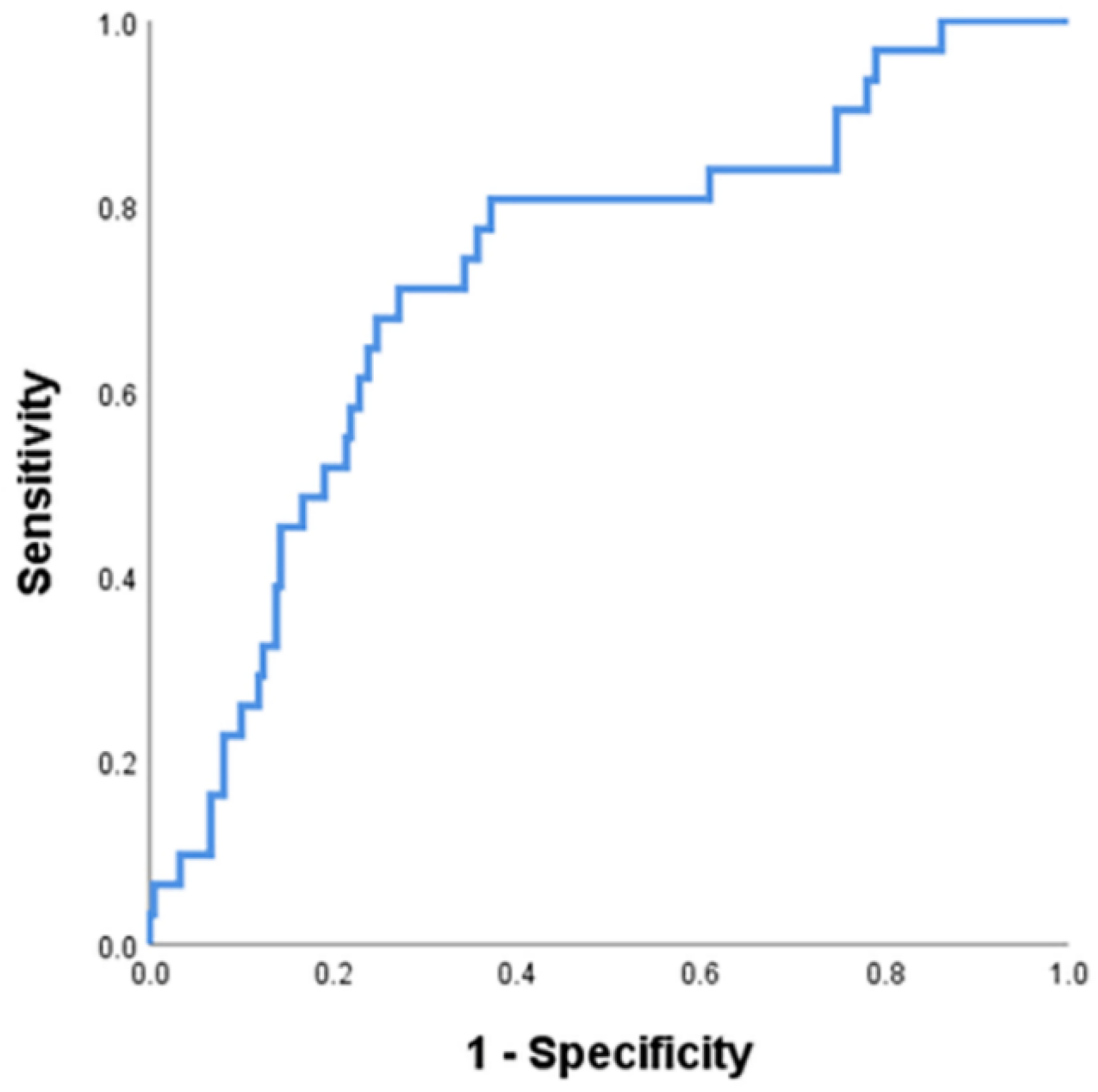
3.3. Predictors of the Immune-Tolerant Phase
3.4. Predictors of the Hepatitis B e Antigen Seroconversion after Antiviral Therapy
3.5. Hepatitis B e Antigen-Negative Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schweitzer, A.; Horn, J.; Mikolajczyk, R.T.; Krause, G.; Ott, J.J. Estimations of worldwide prevalence of chronic hepatitis B virus infection: A systematic review of data published between 1965 and 2013. Lancet 2015, 386, 1546–1555. [Google Scholar] [CrossRef]
- Chen, C.J.; Yang, H.I.; Su, J.; Jen, C.-L.; You, S.-L.; Lu, S.-N.; Huang, G.-T.; Iloeje, U.H.; REVEAL-HBV Study Group. Risk of hepatocellular carcinoma across a biological gradient of serum hepatitis B virus DNA level. JAMA 2006, 295, 65–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.A.; Lee, H.W.; Kim, S.U.; Sinn, D.I.; Yu, J.H.; Seo, Y.S.; Um, S.H.; Lee, J.I.; Lee, K.S.; Lee, C.H.; et al. Extremely low risk of hepatocellular carcinoma development in patients with chronic hepatitis B in immune-tolerant phase. Alim. Pharmacol. Ther. 2020, 52, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Terrault, N.A.; Lok, A.S.F.; McMahon, B.J.; Chang, K.-M.; Hwang, J.P.; Jonas, M.M.; Brown, R.S., Jr.; Bzowej, N.H.; Wong, J.B. Update on Prevention, Diagnosis, and Treatment of Chronic Hepatitis B: AASLD 2018 Hepatitis B Guidance. Clin. Liver Dis. 2018, 12, 33–34. [Google Scholar] [CrossRef] [PubMed]
- Bonacci, M.; Lens, S.; Mariño, Z.; London, M.-C.; Rodriguez-Tajes, S.; Mas, A.; Garcia-Lopez, M.; Perez-del-Pulgar, S.; Sanchez-Tapias, J.M.; Forns, X. Anti-viral therapy can be delayed or avoided in a significant proportion of HBeAg-negative Caucasian patients in the Grey Zone. Alim. Pharmacol. Ther. 2018, 47, 1397–1408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inoue, T.; Tanaka, Y. Novel biomarkers for the management of chronic hepatitis B. Clin. Mol. Hepatol. 2020, 26, 261–279. [Google Scholar] [CrossRef] [PubMed]
- Seto, W.-K.; Wong, D.K.-H.; Fung, J.; Huang, F.-Y.; Liu, K.S.-H.; Lai, C.-L.; Yuen, M.-F. Linearized hepatitis B surface antigen and hepatitis B core-related antigen in the natural history of chronic hepatitis B. Clin. Microbiol. Infect. 2014, 20, 1173–1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chuaypen, N.; Posuwan, N.; Payungporn, S.; Tanaka, Y.; Shinkai, N.; Poovorowan, Y.; Tangkijvanich, P. Serum hepatitis B core-related antigen as a treatment predictor of pegylated interferon in patients with HBeAg-positive chronic hepatitis B. Liver Int. 2016, 36, 827–836. [Google Scholar] [CrossRef] [PubMed]
- Kumada, T.; Toyoda, H.; Tada, T.; Kiriyama, S.; Tanikawa, M.; Hisanaga, Y.; Kanamori, A.; Niinomi, T.; Yasuda, S.; Andou, Y.; et al. Effect of nucleos(t)ide analogue therapy on hepatocarcinogenesis in chronic hepatitis B patients: A propensity score analysis. J. Hepatol. 2013, 58, 427–433. [Google Scholar] [CrossRef]
- Tada, T.; Kumada, T.; Toyoda, H.; Kiriyama, S.; Tanikawa, M.; Hisanaga, Y.; Kanamori, A.; Kitabatake, S.; Yama, T.; Tanaka, J. HBcrAg predicts hepatocellular carcinoma development: An analysis using time-dependent receiver operating characteristics. J. Hepatol. 2016, 65, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Brunetto, M.R.; Carey, I.; Maasoumy, B.; Marcos-Fosch, C.; Boonstra, A.; Caviglia, G.A.; Loglio, A.; Cavallone, D.; Scholtes, C.; Ricco, C.; et al. Incremental value of HBcrAg to classify 1582 HBeAg-negative individuals in chronic infection without liver disease or hepatitis. Alim. Pharmacol. Ther. 2021, 53, 733–744. [Google Scholar]
- Chan, H.L.Y.; Yasuda, S.; Wong, G.L.H.; Tada, T.; Chan, C.K.M.; Kumada, T.; Tse, Y.K.; Wong, V.W.S.; Toyoda, H. Use of hepatitis B virus core-related antigen to evaluate natural history of chronic hepatitis B. J. Gastroenterol. Hepatol. 2020, 35, 2202–2209. [Google Scholar] [CrossRef] [PubMed]
- Colloredo, G.; Guido, M.; Sonzogni, A.; Leandro, G. Impact of liver biopsy size on histological evaluation of chronic viral hepatitis: The smaller the sample, the milder the disease. J. Hepatol. 2003, 39, 239–244. [Google Scholar] [CrossRef]
- Knodell, R.G.; Ishak, K.G.; Black, W.C.; Chen, T.S.; Craig, R.; Kaplowitz, N.; Kiernan, T.W.; Wollman, J. Formulation and application of a numerical scoring system for assessing histological activity in asymptomatic chronic active hepatitis. Hepatology 1981, 1, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Ishak, K.; Baptista, A.; Bianchi, L.; Callea, F.; De Groote, J.; Gudat, F.; Denk, H.; Desmet, V.; Korb, G.; Macsween, R.N.; et al. Histological grading and staging of chronic hepatitis. J. Hepatol. 1995, 22, 696–699. [Google Scholar] [CrossRef]
- Yim, H.J.; Kim, J.H.; Yoon, E.L.; Park, H.; Kwon, J.Y.; Sinn, D.Y.; Lee, S.H.; Lee, J.-H.; Lee, H.W. Comparison of clinical practice guidelines for the management of chronic hepatitis B: When to start, when to change, and when to stop. Clin. Mol. Hepatol. 2020, 26, 411–429. [Google Scholar] [CrossRef]
- Chen, C.F.; Lee, W.-C.; Yang, H.I.; Chang, H.C.; Jen, C.L.; Iloeje, U.H.; Su, J.; Hsiao, C.K.; Wang, L.Y.; You, S.-L.; et al. Changes in Serum Levels of HBV DNA and Alanine Aminotransferase Determine Risk for Hepatocellular Carcinoma. Gastroenterology 2011, 141, 1240–1248.e2. [Google Scholar] [CrossRef]
- Duarte-Rojo, A.; Heathcote, E.J. Review: Efficacy and safety of tenofovir disoproxil fumarate in patients with chronic hepatitis B. Ther. Adv. Gastroenterol. 2010, 3, 107–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hui, C.K.; Leung, N.; Yuen, S.T.; Zhang, H.Y.; Leung, K.-W.; Lei, L.; Cheung, S.F.K.; Wong, W.-M.; Lau, J.K.; Hong Kong Liver Fibrosis Study Group. Natural history and disease progression in Chinese chronic hepatitis B patients in im-mune-tolerant phase. Hepatology 2007, 46, 395–401. [Google Scholar] [CrossRef]
- Sarin, S.K.; Kumar, M.P.; Lau, G.K.; Abbas, Z.; Chan, H.L.Y.; Chen, C.J.; Chen, D.-S.; Chen, H.L.; Chien, R.N.; Dokmeci, A.; et al. Asian-Pacific clinical practice guidelines on the management of hepatitis B: A 2015 update. Hepatol. Int. 2016, 10, 1–98. [Google Scholar] [CrossRef] [PubMed]
- M’Kada, H.; Munteanu, M.; Perazzo, H.; Ngo, Y.; Ramanujam, N.; Imbert-Bismut, F.; Ratziu, V.; Bonnefont-Rousselot, D.; Souberbielle, B.; Schuppe-Koistinen, I.; et al. What are the best reference values for a normal serum alanine transaminase activity (ALT)? Impact on the presumed prevalence of drug induced liver injury (DILI). Regul. Toxicol. Pharmacol. 2011, 60, 290–295. [Google Scholar] [CrossRef]
- Lee, Y.B.; Ha, Y.; Chon, Y.E.; Kim, M.N.; Lee, J.H.; Park, H.; Kim, K.-I.; Kim, S.-H.; Rim, S.K.; Hwang, S.H. Association between hepatic steatosis and the development of hepatocellular carcinoma in pa-tients with chronic hepatitis B. Clin. Mol. Hepatol. 2019, 25, 52–64. [Google Scholar] [CrossRef] [PubMed]
- Karra, V.K.; Chowdhury, S.J.; Ruttala, R.; Polipalli, S.K.; Kar, P. Clinical Significance of Quantitative HBsAg Titres and its Correlation With HBV DNA Levels in the Natural History of Hepatitis B Virus Infection. J. Clin. Exp. Hepatol. 2016, 6, 209–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, T.; Thompson, A.J.; Bowden, S.; Croagh, C.; Bell, S.; Desmond, P.V.; Levy, M.; Locarnini, S.A. Hepatitis B surface antigen levels during the natural history of chronic hepatitis B: A perspective on Asia. J. Hepatol. 2010, 52, 508–513. [Google Scholar] [CrossRef] [PubMed]
- Caviglia, G.; Armandi, A.; Rosso, C.; Ribaldone, D.; Pellicano, R.; Fagoonee, S. Hepatitis B Core-Related Antigen as Surrogate Biomarker of Intrahepatic Hepatitis B Virus Covalently-Closed-Circular DNA in Patients with Chronic Hepatitis B: A Meta-Analysis. Diagnostics 2021, 11, 187. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Carey, I.; Bruce, M.; Montague, S.; Dusheiko, G.; Agarwal, K. HBsAg and HBcrAg as predictors of HBeAg seroconversion in HBeAg-positive patients treated with nucleos(t)ide analogues. J. Viral Hepat. 2018, 25, 886–893. [Google Scholar] [CrossRef] [PubMed]
- Seto, W.K.; Tanaka, Y.; Wong, D.K.; Lai, C.-L.; Shinkai, N.; Yuen, J.C.-H.; Tong, T.; Fung, J.; Hung, I.F.N.; Yuen, M.-F. Evidence of serologic activity in chronic hepatitis B after surface antigen (HBsAg) sero-clearance documented by conventional HBsAg assay. Hepatol. Int. 2012, 7, 98–105. [Google Scholar] [CrossRef] [Green Version]
- Sonneveld, M.J.; van Oord, G.W.; van Campenhout, M.J.; De Man, R.A.; Janssen, H.L.A.; de Knegt, R.J.; Boonstra, A.; van der Eijk, A.A. Relationship between hepatitis B core-related antigen levels and sustained HBeAg seroconversion in patients treated with nucleo(s)tide analogues. J. Viral. Hepat. 2019, 26, 828–834. [Google Scholar] [CrossRef]
- zu Siederdissen, C.H.; Maasoumy, B.; Deterding, K.; Port, K.; Manns, M.; Wedemeyer, H.; Cornberg, M. Clinical significance of drug-drug interactions during HCV therapy with sofosbuvir and simeprevir in comparison to first wave protease inhibitors. Z. Gastroenterol. 2015, 53, A5_14. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | IT Patients (n = 32, 11.9%) | PIA Patients (n = 211, 86.8%) | p Value | NIA Patients (n = 125, 86.8%) | IC Patients (n = 19, 13.2%) | p Value |
|---|---|---|---|---|---|---|
| Age, years | 31.8 ± 11.0 | 38.5 ± 12.4 | 0.004 | 46.5 ± 10.1 | 43.0 ± 11.2 | 0.172 |
| Male, n (%) | 32 (100) | 128 (60.7) | <0.001 | 86 (68.8) | 14 (73.7) | 0.667 |
| Diabetes, n (%) | 1 (3.1) | 9 (4.3) | 0.762 | 11 (8.8) | 2 (10.5) | 0.807 |
| Platelet count, ×109/L | 210.6 ± 41.1 | 184.4 ± 58.5 | 0.015 | 163.0 ± 47.0 | 194.6 ± 49.7 | 0.007 |
| PT INR | 1.03 ± 0.65 | 1.06 ± 0.09 | 0.117 | 1.08 ± 1.00 | 1.06 ± 0.11 | 0.376 |
| ALT, IU/L | 80.5 ± 53.8 | 212.4 ± 242.2 | <0.001 | 161.9 ± 259.3 | 77.3 ± 92.5 | 0.009 |
| Bilirubin, mg/dL | 0.77 ± 0.49 | 0.77 ± 0.48 | 0.987 | 0.97 ± 2.13 | 0.68 ± 0.34 | 0.555 |
| Albumin, g/dL | 4.07 ± 1.15 | 4.0 ± 0.6 | 0.787 | 4.0 ± 0.4 | 4.4 ± 0.4 | <0.001 |
| AFP, ng/mL | 2.6 ± 1.2 | 17.7 ± 58.1 | <0.001 | 11.6 ± 31.9 | 2.9 ± 1.3 | 0.253 |
| HBV DNA, log IU/mL | 7.3 ± 1.5 | 7.3 ± 1.1 | 0.990 | 5.5 ± 1.8 | 3.3 ± 1.9 | <0.001 |
| HBsAg, log IU/mL | 7.4 ± 0.6 | 6.9 ± 0.6 | 0.002 | 5.2 ± 2.6 | 5.3 ± 2.8 | 0.859 |
| HBcrAg, log U/mL | 8.2 ± 0.7 | 7.6 ± 1.1 | <0.001 | 5.3 ± 1.4 | 4.0 ± 1.6 | <0.001 |
| Variables | Rating | Univariate | Multivariate | ||
|---|---|---|---|---|---|
| p Value | Odds Ratio | 95% CI | p Value | ||
| Age | years | 0.005 | 0.949 | 0.906–0.993 | 0.025 |
| Male sex | 0 = no; 1 = yes | 0.996 | |||
| Diabetes | 0 = no; 1 = yes | 0.763 | |||
| Platelet count | ×109/L | 0.020 | 1.003 | 0.994–1.013 | 0.505 |
| PT INR | 0.117 | ||||
| ALT | IU/L | 0.005 | 0.988 | 0.980–0.996 | 0.002 |
| Bilirubin | mg/dL | 0.986 | |||
| Albumin | g/dL | 0.660 | |||
| HBV DNA | log IU/mL | 0.987 | |||
| HBsAg | log IU/mL | 0.001 | 2.076 | 0.717–6.014 | 0.178 |
| HBcrAg | log U/mL | 0.003 | 2.745 | 1.157–6.514 | 0.022 |
| Variables | Rating | Univariate | ||
|---|---|---|---|---|
| Hazard Ratio | 95% CI | p Value | ||
| Age | years | 0.981 | 0.955–1.007 | 0.150 |
| Male sex | 0 = no; 1 = yes | 0.736 | 0.440–1.233 | 0.245 |
| Diabetes | 0 = no; 1 = yes | 0.534 | 0.162–1.760 | 0.303 |
| Platelet count | ×109/L | 1.000 | 0.996–1.004 | 0.904 |
| PT INR | 1.785 | 0.267–11.933 | 0.550 | |
| ALT | IU/L | 1.001 | 0.999–1.002 | 0.395 |
| Bilirubin | mg/dL | 1.108 | 0.666–1.844 | 0.694 |
| Albumin | g/dL | 1.374 | 0.980–1.926 | 0.065 |
| HBV DNA | log IU/mL | 0.924 | 0.663–1.288 | 0.641 |
| HBsAg | log IU/mL | 1.056 | 0.574–1.942 | 0.861 |
| HBcrAg | log U/mL | 1.285 | 1.027–1.609 | 0.028 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.A.; Lee, H.W.; Park, Y.; Kim, H.-S.; Seo, Y.S. Hepatitis B Core-Related Antigen Is Useful for Predicting Phase and Prognosis of Hepatitis B e Antigen-Positive Patients. J. Clin. Med. 2022, 11, 1729. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11061729
Lee HA, Lee HW, Park Y, Kim H-S, Seo YS. Hepatitis B Core-Related Antigen Is Useful for Predicting Phase and Prognosis of Hepatitis B e Antigen-Positive Patients. Journal of Clinical Medicine. 2022; 11(6):1729. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11061729
Chicago/Turabian StyleLee, Han Ah, Hyun Woong Lee, Younhee Park, Hyon-Suk Kim, and Yeon Seok Seo. 2022. "Hepatitis B Core-Related Antigen Is Useful for Predicting Phase and Prognosis of Hepatitis B e Antigen-Positive Patients" Journal of Clinical Medicine 11, no. 6: 1729. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11061729