
Exercise Training in Post-COVID-19 Patients: The Need for a Multifactorial Protocol for a Multifactorial Pathophysiology

Abstract
:1. Introduction
2. COVID-19
- Is it a chronic disease? At the end of the viral and inflammation phase causing the active disease, most patient are discharged without breathlessness at rest, yet often with poor exercise tolerance associated with persistency of COVID-19 signs at RX or CT pre-discharge evaluation (i.e., long-COVID-19 syndrome). Elevated levels of inflammatory cytokines could persist at follow up, causing vascular remodelling and endothelial dysfunction, possibly leading to pulmonary hypertension [3].
- Is it a multifactorial disease? To date, there is paucity of data about the precise mechanisms underpinning COVID-19 and no single interpretation may unify the pathophysiological mechanisms underlying the disease and its consequences, which conceivably are multifactorial. Alterations associated with COVID-19, especially in patients requiring ICU care, involve respiratory function (impairment of alveolar air exchange, decrease in pulmonary ventilation, respiratory muscle dysfunction and, probably, pulmonary fibrosis in the long run), cardiac function (reduced systolic function in some cases and possible persistent myocardial damage in the long run), pulmonary vessels (pulmonary hypertension in some cases due to pulmonary embolism and/or thrombosis), peripheral muscle function (due to deconditioning and decreased lean body mass, fatigue and the effects of hypokalaemia) [4,5], and, likely, liver, kidney, and brain and nervous and immune systems [6]. Finally, decreased exercise capacity is the most common dysfunction (61,4% of discharged mild patients) mainly due to the long-term immobilization or to the muscle invasion by the virus [7].
3. Inflammation and Exercise Training
4. Exercise Training in Post-COVID-19 Patients
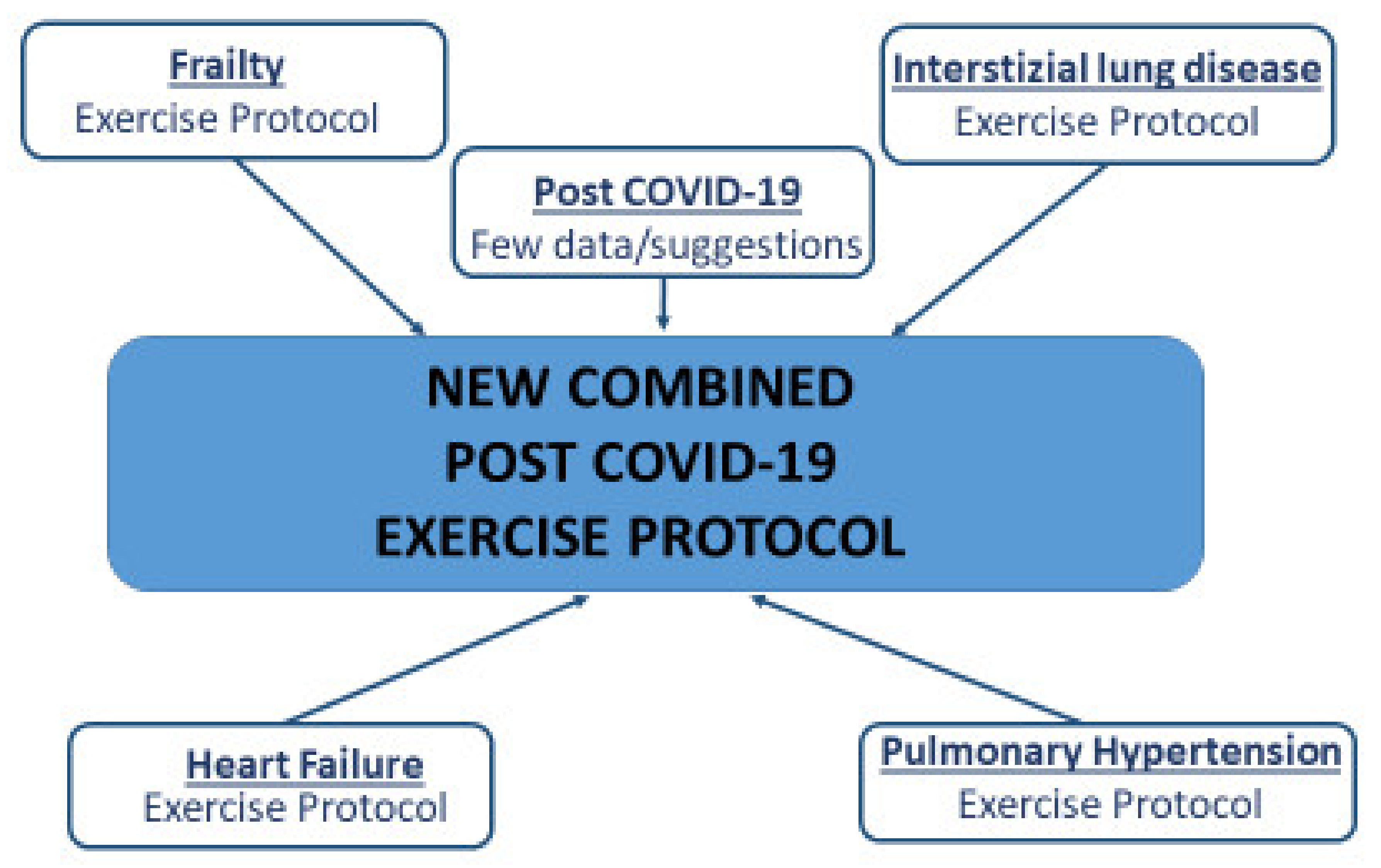
5. The “New Combined Post-COVID-19 Exercise Protocol”
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Achilleos, S.; Quattrocchi, A.; Gabel, J.; Heraclides, A.; Kolokotroni, O.; Constantinou, C.; Ugarte, M.P.; Nicolaou, N.; Rodriguez-Llanes, J.M.; Bennett, C.M.; et al. Excess all-cause mortality and COVID-19-related mortality: A temporal analysis in 22 countries, from January until August 2020. Int. J. Epidemiol. 2022, 51, 35–53. [Google Scholar] [CrossRef] [PubMed]
- Jimeno-Almazán, A.; Pallarés, J.G.; Buendía-Romero, Á.; Martínez-Cava, A.; Franco-López, F.; Sanchez-Alcaraz Martínez, B.J.; Bernal-Morel, E.; Courel-Ibáñez, J. Post-COVID-19 Syndrome and the Potential Benefits of Exercise. Int. J. Environ. Res. Public Health 2021, 18, 5329. [Google Scholar] [CrossRef] [PubMed]
- Brugliera, L.; Spina, A.; Castellazzi, P.; Cimino, P.; Arcuri, P.; Deriu, M.G.; Zanetta, C.; Angelone, S.M.; Capitanio, J.F.; Alemanno, F.; et al. Rehabilitative of COVID-19 patients with acute lower extremity Ischemia and amputation. J. Rehabil. Med. 2020, 2, 52. [Google Scholar] [CrossRef] [PubMed]
- Barker-Davies, R.M.; O’Sullivan, O.; Senaratne, K.P.P.; Baker, P.; Cranley, M.; Dharm-Datta, S.; Ellis, H.; Goodall, D.; Gough, M.; Lewis, S.; et al. The Stanford Hall consensus statement for post-COVID-19 rehabilitation. Br. J. Sports Med. 2020, 54, 949–959. [Google Scholar] [CrossRef]
- Zhang, Y.; Coats, A.J.S.; Zheng, Z.; Adamo, M.; Ambrosio, G.; Anker, S.D.; Butler, J.; Xu, D.; Mao, J.; Khan, M.S.; et al. Management of heart failure patients with COVID-19: A joint position paper of the Chinese Heart Failure Association & National Heart Failure Committee and the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2020, 22, 941–956. [Google Scholar] [CrossRef]
- Li, J. Rehabilitation management of patients with COVID-19: Lessons learned from the first experiences in China. Eur. J. Phys. Rehabil. Med. 2020, 56, 335–338. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Nigro, E.; Polito, R.; Alferi, A.; Mancini, A.; Imperlini, E.; Elce, A.; Krustrup, P.; Orrù, S.; Buono, P.; Daniele, A. Molecular mechanisms involved in the positivie effects of physical activity on copinc with COVID-19. Eur. J. Appl. Physiol. 2020, 120, 2569–2582. [Google Scholar] [CrossRef]
- Rahmati-Ahmadabad, S.; Hossein, F. Exercise against SARS-Cov-2 (COVID 19): Does workout intensity matter? Obes. Med. 2020, 19, 100245. [Google Scholar] [CrossRef]
- Heffernan, K.S.; Jae, S.Y. Exercise as a medicine for COVID-19: An ACE in the hole? Med. Hypotheses 2020, 142, 109835. [Google Scholar] [CrossRef]
- Kenyon, C. The Forrest Gump approach to preventing severe COVID-19–Reverse the predisposing pro-inflammatory state with exercise. Microbes Infect. 2020, 22, 151–153. [Google Scholar] [CrossRef]
- Rice, H.; Harrold, M.; Fowler, R.; Watson, C.; Waterer, G.; Hill, K. Exercise training for adults hospitalized with an acute respiratory condition: A systematic scoping review. Clin. Rehabil. 2020, 34, 45–55. [Google Scholar] [CrossRef]
- Task Force for the Management of COVID-19 of the European Society of Cardiology. ESC guidance for the diagnosis and management of cardiovascular disease during the COVID-19 pandemic: Part 2—Care pathways, treatment, and follow-up. Eur. Heart J. 2021, 43, 1059–1103. [Google Scholar] [CrossRef]
- Borg, K.; StamBorg, H. COVID-19 and physical and rehabilitation medicine. J. Rehabil. Med. 2020, 52, jrm00045. [Google Scholar] [CrossRef]
- Mureddu, G.F.; Ambrosetti, M.; Venturini, E.; la Rovere, M.T.; Mazza, A.; Pedretti, R.; Sarullo, F.; Fattirolli, F.; Faggiano, P.; Giallauria, F.; et al. Cardiac rehabilitation activities during the COVID-19 pandemic in Italy. Position Paper of the AICPR. Monaldi Arch. Chest Dis. 2020, 90, 1439. [Google Scholar] [CrossRef]
- Sheehy, L.M. Considerations for Postacute Rehabilitation for Survivors of COVID-19. JMIR Public Health Surveill. 2020, 6, e19462. [Google Scholar] [CrossRef]
- Yang, L.-L.; Yang, T. Pulmonary rehabilitation for patients with coronavirus disease 2019 (COVID-19). Chronic Dis. Transl. Med. 2020, 6, 79–86. [Google Scholar] [CrossRef]
- Zeng, B.; Chen, D.; Qiu, Z.; Zhang, M. Expert consensus on protocol of rehabilitation for COVID-19 patients using framework and approaches of WHO International Family Clasifications. Aging Med. 2020, 3, 82–94. [Google Scholar] [CrossRef]
- Chen, H.; Shi, H.; Liu, X.; Sun, T.; Wu, J.; Liu, Z. Effect of pulmonary rehabilitation for patients with post-COVID-19: A systemic review and meta-analysis. Front. Med. 2022, 9, 837420. [Google Scholar] [CrossRef]
- McNarry, M.A.; Berg, R.M.; Shelley, J.; Hudson, J.; Saynor, Z.L.; Duckers, J.; Lewis, K.; Davies, G.A.; Mackintosh, K.A. Inspiratory muscle training enhamces recovery post COVID-19: A randomized controlled trial. Eur. Respir. J. 2022; in press. [Google Scholar] [CrossRef]
- Ahmadi Hekmatikar, A.H.; Ferreira, J.B.; Shahrbanian, S. Functional and psychological changes after exercise training in post-COVID-19 patients discharged from the hospital: A PRISMA-compliant systemic review. Int. J. Environ. Res. Public Health 2022, 19, 2290. [Google Scholar] [CrossRef]
- Angulo, J.; El Assar, A.; Álvarez-Bustosc, A.; Rodríguez-Mañas, L. Physical activity and exercise: Strategies to manage frailty. Redox Biol. 2020, 35, 101513. [Google Scholar] [CrossRef]
- Afilalo, J. Evaluating and Treating Frailty in Cardiac Rehabilitation. Clin. Geriatr. Med. 2019, 35, 445–457. [Google Scholar] [CrossRef]
- Zhao, H.; Yu-Xiao, X.; Chen, W. Recommendations for respiratory rehabilitation in adults with COVID-19. Chin. Med J. 2020, 133, 1595–1602. [Google Scholar] [CrossRef]
- Liu, K.; Zhang, W.; Yang, Y.; Zhang, J.; Li, Y.; Chen, Y. Respiratory rehabilitation in elderly patients with COVID-19: A randomized controlled study. Complement. Ther. Clin. Pract. 2020, 39, 101166. [Google Scholar] [CrossRef]
- Severin, R.; Arena, R.; Lavie, C.J.; Bond, S.; Phillips, S.A. Respiratory Muscle Performance Screening for Infectious Disease Management Following COVID-19: A Highly Pressurized Situation. Am. J. Med. 2020, 133, 1025–1032. [Google Scholar] [CrossRef]
- Yang, F.; Liu, N.; Hu, J.Y.; Wu, L.L.; Su, G.S.; Zhong, N.S.; Zheng, Z.G. Pulmonary rehabilitation guidelines in the principle of 4S for patients infected with 2019 novel coronavirus (2019-nCoV). Zhonghua Jie He He Hu Xi Za Zhi 2020, 43, 180. [Google Scholar]
- Lau, H.M.; Yin-Fat, G.; Yee-Men Jones, A.; Lee, E.W.; Siu, E.H.; Hui, D.S. A randomized controlled trial of the effectiveness of an exercise training program in patients recovering from severe acute respiratory syndrome. Aust. J. Physiother. 2005, 51, 213–219. [Google Scholar] [CrossRef] [Green Version]
- Spruit, M.A.; Singh, S.J.; Garvey, C.; ZuWallack, R.; Nici, L.; Rochester, C.; Hill, K.; Holland, A.E.; Lareau, S.C.; Man, W.D.C.; et al. An official American thoracic society/European respiratory society statement: Key concepts and advances in pulmonary rehabilitation. Am. I Resp. Crit. Care Med. 2013, 188, e13–e64. [Google Scholar] [CrossRef]
- Vainshelboim, B.; Oliveira, J.; Yehoshua, L.; Weiss, I.; Fox, B.D.; Fruchter, O.; Kramer, M.R. Exercise Training-Based Pulmonary Rehabilitation Program Is Clinically Beneficial for Idiopathic Pulmonary Fibrosis. Respiration 2014, 88, 378–388. [Google Scholar] [CrossRef]
- Curtis, K.; Hopkinson, N.S. Exercise training in interstitial lung disease: Lumping or splitting? Thorax 2017, 72, 589–590. [Google Scholar] [CrossRef] [PubMed]
- Garvey, B.; Paternostro, M.; Larry, F.; Hill, K.; Holland, A.; Limberg, T.; Spruit, M. Pulmonary rehabilitation exercise prescription in chronic obstructive pulmonary disease: Review of selected guidelines. J. Cardiopulm. Rehab. Prev. 2016, 36, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Ehlken, N.; Lichtblau, M.; Klose, H.; Weidenhammer, J.; Fischer, C.; Nechwatal, R.; Uiker, S.; Halank, M.; Olsson, K.; Seeger, W.; et al. Exercise training improves peak oxygen consumption and haemodynamics in patients with severe pulmonary arterial hypertension and inoperable chronic thrombo-embolic pulmonary hypertension: A prospective, randomized, controlled trial. Eur. Heart J. 2016, 37, 35–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grünig, E.; Eichstaedt, C.; Barberà, J.-A.; Benjamin, N.; Blanco, I.; Bossone, E.; Cittadini, A.; Coghlan, G.; Corris, P.; D’Alto, M.; et al. ERS statement on exercise training and rehabilitation in patients with severe chronic pulmonary hypertension. Eur. Respir. J. 2019, 53, 1800332. [Google Scholar] [CrossRef] [Green Version]
- Piepoli, M.F.; Conraads, V.; Corrà, U.; Dickstein, K.; Francis, D.P.; Jaarsma, T.; Mcmurray, J.; Pieske, B.; Piotrowicz, E.; Schmid, J.-P.; et al. Exercise training in heart failure: From theory to practice. A consensus document of the Heart Failure Association and the European Association for Cardiovascular Prevention and Rehabilitation. Eur. J. Heart Fail. 2011, 13, 347–357. [Google Scholar] [CrossRef]
- Cattadori, G.; Segurini, C.; Picozzi, A.; Padeletti, L.; Anzà, C. Exercise and heart failure: An update. ESC Heart Fail. 2018, 5, 222–232. [Google Scholar] [CrossRef]
- Arena, R. Exercise Training in Group 2 Pulmonary Hypertension: Which Intensity and What Modality. Prog. Cardiovasc. Dis. 2011, 13, 454–463. [Google Scholar] [CrossRef]
- Mereles, A.; Ehlken, N.; Kreuscher, S.; Ghofrani, S.; Hoeper, M.H.; Halank, M.; Meyer, F.J.; Karger, G.; Buss, J.; Juenger, J.; et al. Exercise and Respiratory Training Improve Exercise Capacity and Quality of Life in Patients with Severe Chronic Pulmonary Hypertension. Circulation 2006, 114, 1482–1489. [Google Scholar] [CrossRef] [Green Version]
- Bussotti, M.; Gremigni, P.; Pedretti, R.F.E.; Kransinska, P.; Di Marco, S.; Corbo, P.; Marchese, G.; Totaro, P.; Sommaruga, M. Effects of an Outpatient Service Rehabilitation Programme in Patients Affected by Pulmonary Arterial Hypertension: An Observational Study. Cardiovasc. Hematol. Disord. Drug. Targets 2017, 17, 3–10. [Google Scholar] [CrossRef]
- Raj, S.R.; Arnold, A.C.; Barboi, A.; Claydon, V.E.; Limber, J.K.; Lucci, V.M.; Numan, M.; Peltier, A.; Snapper, H.; Vermino, S.; et al. Long-COVID postural tachycardia syndrome: An American Autonomic Society Statement. Clin. Auton. Res. 2021, 31, 365–368. [Google Scholar] [CrossRef]
- Bouwstra, H.; Smit, E.B.; Wattel, E.M.; van der Wouden, J.C.; Hertogh, C.M.P.M.; Terluin, B.; Terwee, C.B. Index Measurement Properties of the Barthel Index in Geriatric Rehabilitation. J. Am. Med. Dir. Assoc. 2019, 20, 420–425. [Google Scholar] [CrossRef]
- Kojima, G. Quick and Simple FRAIL Scale Predicts Incident Activities of Daily Living (ADL) and Instrumental ADL (IADL) Disabilities: A Systematic Review and Meta-analysis. J. Am. Med Dir. Assoc. 2018, 19, 1063–1068. [Google Scholar] [CrossRef]
- Guralnik, J.M.; Ferrucci, L.; Simonsick, E.M.; Salive, M.E.; Wallace, R.B. Lower-extremity Function in Persons Over the Age of 70 Years as a Predictor of Subsequent Disability. N. Engl. J. Med. 1995, 332, 556–561. [Google Scholar] [CrossRef] [Green Version]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older study: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005, 173, 489–495. [Google Scholar] [CrossRef] [Green Version]
- Afilalo, J.; Mottillo, S.; Xue, X.; Colacone, A.; Morais, J.A.; Delaney, J.S.; Afilalo, M. Frailty and adverse outcomes in older adults being discharged from the emergency department: A prospective cohort study. Can. J. Emerg. Med. 2020, 22, 65–73. [Google Scholar] [CrossRef]
- Robles, P.G.; Mathur, S.; Janaudis-Fereira, T.; Dolmage, T.E.; Goldstein, R.S.; Brooks, D. Measurement of peripheral muscle strength in individuals with chronic obstructive pulmonary disease: A systematic review. J. Cardiopulm. Rehabil. Prev. 2011, 31, 11–24. [Google Scholar] [CrossRef]
- Puente-Maestu, L.; Palange, P.; Casaburi, R.; Laveneziana, P.; Maltais, F.; Neder, J.A.; O’Donnell Dem Onorati, P.; Porszasz, J.; Rabinovich, R.; Rossiter, H.; et al. Use of exercise testing in the evaluation of interventional efficacy: An official ERS statement. Eur. Respir. J. 2016, 47, 429–460. [Google Scholar] [CrossRef]
- Downs, S.; Marquez, J.; Chiarelli, P. The Berg Balance Scale has high intra- and inter-rater reliability but absolute reliability varies across the scale: A systematic review. J. Physiother. 2013, 59, 93–99. [Google Scholar] [CrossRef] [Green Version]
- Lee, P.H.; Macfarlane, D.J.; Lam, T.H.; Stewart, S.M. Validity of the International Activity Questionnaire Short form: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 115. [Google Scholar] [CrossRef] [Green Version]
- Sattler, M.C.; Jaunig, J.; Tösch, C.; Watson, E.D.; Mokkink, L.B.; Dietz, P.; van Poppel, M. Current Evidence of Measurement Properties of Physical Activity Questionnaires for Older Adults: An Updated Systematic Review. Sports Med. 2020, 50, 1271–1315. [Google Scholar] [CrossRef] [Green Version]
- Green, C.P.; Porter, C.B.; Bresnahan, D.R.; Spertus, J.A. Development and evaluation of the Kansas City Cardiomyopathy Questionnaire: A new health status measure for heart failure. J. Am. Coll. Cardiol. 2000, 35, 1245–1255. [Google Scholar] [CrossRef] [Green Version]
- Jones, P.W.; Quirk, F.H.; Baveystock, C.M. The St. George’s Respiratory Questionnaire. Resp. Med. 1991, 85 (Suppl. SB), 2531. [Google Scholar] [CrossRef]
- Dermot Phelan Jonathan, H.; Kim Eugene, H. Chung. A game plan for the resumption of sport and exercise after coronavirus disease 2019 (COVID-19) infection. JAMA Cardiol. 2020, 5, 1085–1086. [Google Scholar]
- Jimesez-Pavon, D.; Carbonell-Baeza, A. Physical exercise as therapy to fight against the mental and physical consequences of COVID-19 quarantine: Special focus in older people. Prog. Cardiovasc. Dis. 2020, 63, 386–388. [Google Scholar] [CrossRef]
- Kiekens, C.; Boldrini, C.; Andreoli, A.; Avesani, R.; Gamna, F.; Grandi, M.; Lombardi, F.; Lusuardi, M.; Molteni, F.; Perboni, A.; et al. Rehabilitation and respiratory management in the acute and early post-acute phase. “Instant paper from the field” on rehabilitation answers to the COVID-19 emergency. Eur. J. Phys. Rehabil. Med. 2020, 56, 323–326. [Google Scholar] [CrossRef]


{kind=link}
| COVID-19 Patients Training |
|---|
|
| COVID-19 Pathophysiology Features [4,5,6,7,40] | Related Landmark Diseases [22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39] |
|---|---|
| Respiratory distress with impairment of alveolar air exchange, decrease in pulmonary ventilation and, probably, pulmonary fibrosis in the long run | SARS |
| Interstitial lung disease | |
| Idiopathic pulmonary fibrosis | |
| Pulmonary vessels dysfunction with pulmonary hypertension in some cases due to pulmonary embolism and/or thrombosis | Pulmonary Hypertension |
| Interstitial lung disease | |
| Idiopathic pulmonary fibrosis | |
| Decreased exercise capacity and musculoskeletal deterioration due to the long-term immobilization or to the muscle invasion by the virus, leading to a “frail” post-COVID-19 population | Frailty |
| Symptomatic high heart rate | Heart Failure |
| Interstitial lung disease | |
| Idiopathic pulmonary fibrosis | |
| Pulmonary Hypertension | |
| Cardiac dysfunction: reduced systolic function in some cases and possible persistent myocardial damage in the long run | Heart Failure |
| Training | General Description | COVID-19 Related Diseases Trial Data | COVID-19 Trial/Expert Consensus Data |
|---|---|---|---|
| Continuous Aerobic training | Characterized by continuous, dynamic, rhythmic activities involving major muscle groups (i.e., walking, treadmill, cycle ergometer, stair climbing, rower, elliptical trainers) Typically performed at submaximal intensity with the main purpose of progressively moving the anaerobic threshold Heart rate or oxygen consumption measurement to set training intensity. | SARS-CoV-1 | COVID-19 trial Expert Consensus |
| Frailty | |||
| Interstitial lung disease | |||
| Idiopathic pulmonary fibrosis | |||
| Heart Failure Pulmonary Hypertension | |||
| Interval Training | High/Low intensity: intermittent periods of high/low intensity exercise separated by periods of low intensity/recovery Heart rate or oxygen consumption measurement to set training intensity. | Heart Failure | COVID-19 trial |
| Resistance Training | Primarily anaerobic physical exercises designed to promote muscles force against external weights. 1RM (one-repetition maximum), the maximum amount of weight that a person can possibly lift for one repetition, used to set training intensity. It promotes less pronounced cardiorespiratory responses when compared to aerobic exercise | SARS-CoV-1 | COVID-19 trial Expert Consensus |
| Frailty | |||
| Interstitial lung disease | |||
| Idiopathic pulmonary fibrosis | |||
| Heart Failure | |||
| Pulmonary Hypertension | |||
| Inspiratory muscles training | Inspiration using a commercial hand-held resistance | SARS-CoV-1 | COVID-19 trial Expert Consensus |
| Heart Failure | |||
| Pulmonary Hypertension | |||
| Cough Exercise | Sets of active cough under the guidance of a rehabilitation therapist | COVID-19 trial Expert Consensus | |
| Diaphragm Training | Maximal voluntary diaphragmatic contractions in the supine position, placing a medium weight (1–3 kg) on the anterior abdominal wall to resist diaphragmatic descent | COVID-19 trial Expert Consensus | |
| Stretching Exercise | The respiratory muscles stretched under the guidance of a rehabilitation therapist; the patient placed in the supine or lateral decubitus position with the knees bent to correct the lumbar curve; patients ordered to move their arms in flexion, horizontal extension, abduction and external | Idiopathic pulmonary fibrosis | COVID-19 trials Expert Consensus |
| Flexibility Exercise | Static and dynamic stretching leading to progressive increase in range of motion | Frailty | |
| Idiopathic pulmonary fibrosis | |||
| Balance Exercise | Leg stances, semi-tandem and tandem stance, toe walking, heel walking, tandem gait, walking on a balance board, eye–hand and eye–leg coordination | Frailty | Expert Consensus |
| Deep/ slow breath sessions | Special form of training skilfully mastered by patients through a series of choreographed action routines and with the help of words, pictures, videos or other communication methods. During breathing training, it is necessary to pay attention to the coordination of diaphragm movement with trunk and limb movement so that diaphragm-function training, breathing-mode training and body and joint training can be carried out at the same time. | Idiopathic pulmonary fibrosis Heart Failure Pulmonary Hypertension | Expert Consensus |
| Evaluation | Scales or Tests |
|---|---|
| Disability | BARTHEL Index [41] Activities of Daily Living scale (ADL) [42] Short Physical Performance Battery (SPPB) [43] |
| Frailty | Fried’s Frailty Phenotype [44] Frailty Index of Accumulative Deficits [45] 5 m Gait Speed [46] SPPB [43] |
| Strength | Hand Grip Test [47] |
| Endurance | Cardiopulmonary Exercise Test (if available) [48] 6 Minute Walking Test (SpO2 + respiratory rate + Borg scale before/after) [48] |
| Balance | Berg Balance Scale [49] SPPB [43] |
| Respiratory Function | Rest/nocturnal SpO2 [32] Spirometry [32] Diffusion capacity [32] Maximal Inspiratory/Expiratory Pressure (MIP/MEP) [29] |
| Cardiovascular Function | Transthoracic echocardiogram [48] |
| Questionnaire | International Physical Activity Questionnaire-Short Form (IPAQ-SF) [50] Physical Activity Scale for the Elderly (PASE) [51] Kansas City Cardiomyopathy Questionnaire (KCCQ) [52] St. George’s Respiratory Questionnaire (SGRQ) [53] |
| Training | Modality | Frequency | Intensity | Duration |
|---|---|---|---|---|
| Aerobic continuous training | Walking or cycling | 2→5 days/week; 150–300 min/week | Walking 80% of peak walking speed achieved on the 6 MWt; Cycling at 50–60%→70% WR max or 60–75%-->80–85% HR max estimated from 6 MWt or Borg 4–6→10; between AT and RC estimated from CPET | 20–30 min→65 min per session; 8–12 weeks long |
| Interval training | Walking or cycling | Short bouts (10–30 s) of moderate–high intensity at 50–100% peak exercise capacity and a longer recovery (80–60 s) | 30 min aerobic interval training (5 min bout + 1 min rest repeated 5 times) | |
| Resistance/ Strength training | Upper and lower body strength | 2–3→5 times/week | 10–15→40→80% of 1 RM; 3–5 on Borg scale; wall push-ups, chair squat, dumbbells shoulder press, dumbbells biceps curls, dumbbells arm extension and abdominal curl-ups | 8–12→15 repetitions with 1 min of rest between steps for 1–3→4–6 times; 10→45 min for each session |
| Inspiratory muscles training | Using a commercial hand-held resistance | 2 times/day; 2 sessions/week | 60% of maximal expiratory mouth pressure | 3 sets with 10 breaths in each set with a rest period of 1 min |
| Cough Exercise | Under the guidance of a rehabilitation therapist | 2 sessions/week | 3 sets of 10 active coughs | |
| Diaphragmatic muscle training | Supine position | 2 sessions/week | placing a medium weight (1–3 kg) on the anterior abdominal wall to resist diaphragmatic descent | 30 maximal voluntary diaphragmatic contractions |
| Stretching Exercise | Supine or lateral decubitus with the knees bent to correct the lumbar curve, moving their arms in flexion, horizontal extension, abduction and external rotation | Titrate to symptoms | One set of 4–5 stretching exercises for 15–30 s | |
| Balance Exercise | Leg stances, semi-tandem and tandem stance, toe walking, heel walking, tandem gait, walking on a balance board, eye–hand and eye–leg coordination; under the guidance of a rehabilitation therapist | 2–3 days/week | Among the different training days | |
| Flexibility Exercise | Static and dynamic stretching leading to progressive increase in range of motion; dynamic stretching in warm-up, whereas static stretching exercise at the end in the cool-down phase; under the guidance of a rehabilitation therapist | 2–3→5 days/week | 5 min long | |
| Slow breathing Sessions | The patient connected to a device providing rhythmic sounds for the progressive lowering of the respiratory rate | 6 b/min 30′ daily | 20–30 min for every daily session |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cattadori, G.; Di Marco, S.; Baravelli, M.; Picozzi, A.; Ambrosio, G. Exercise Training in Post-COVID-19 Patients: The Need for a Multifactorial Protocol for a Multifactorial Pathophysiology. J. Clin. Med. 2022, 11, 2228. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11082228
Cattadori G, Di Marco S, Baravelli M, Picozzi A, Ambrosio G. Exercise Training in Post-COVID-19 Patients: The Need for a Multifactorial Protocol for a Multifactorial Pathophysiology. Journal of Clinical Medicine. 2022; 11(8):2228. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11082228
Chicago/Turabian StyleCattadori, Gaia, Silvia Di Marco, Massimo Baravelli, Anna Picozzi, and Giuseppe Ambrosio. 2022. "Exercise Training in Post-COVID-19 Patients: The Need for a Multifactorial Protocol for a Multifactorial Pathophysiology" Journal of Clinical Medicine 11, no. 8: 2228. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11082228