
Myopia Control Effect Is Influenced by Baseline Relative Peripheral Refraction in Children Wearing Defocus Incorporated Multiple Segments (DIMS) Spectacle Lenses

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Measurements
- Age at enrolment: 8–13 years
- Central spherical equivalent refraction (SE): −1.00 to −5.00 D
- Astigmatism: up to 1.50 D
- Anisometropia: up to 1.25 D
- Strabismus and binocular vision abnormalities
- Ocular and systemic abnormalities
- Prior experience with myopia control
- SE = S + C/2
- J0 = −(C/2) cos (2θ)
- J45 = −(C/2) sin (2θ)
2.2. Data Analysis
3. Results
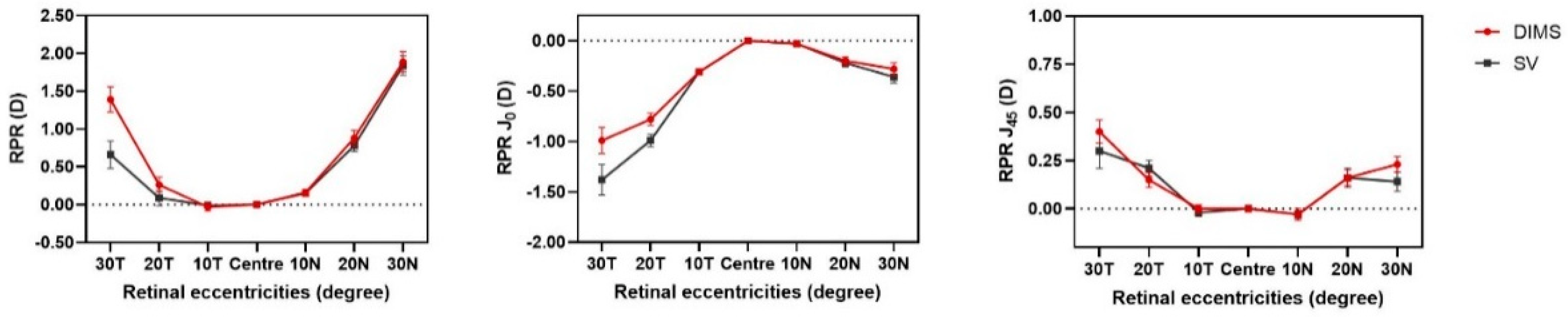
3.1. RPR SE
3.2. RPR J0, J45
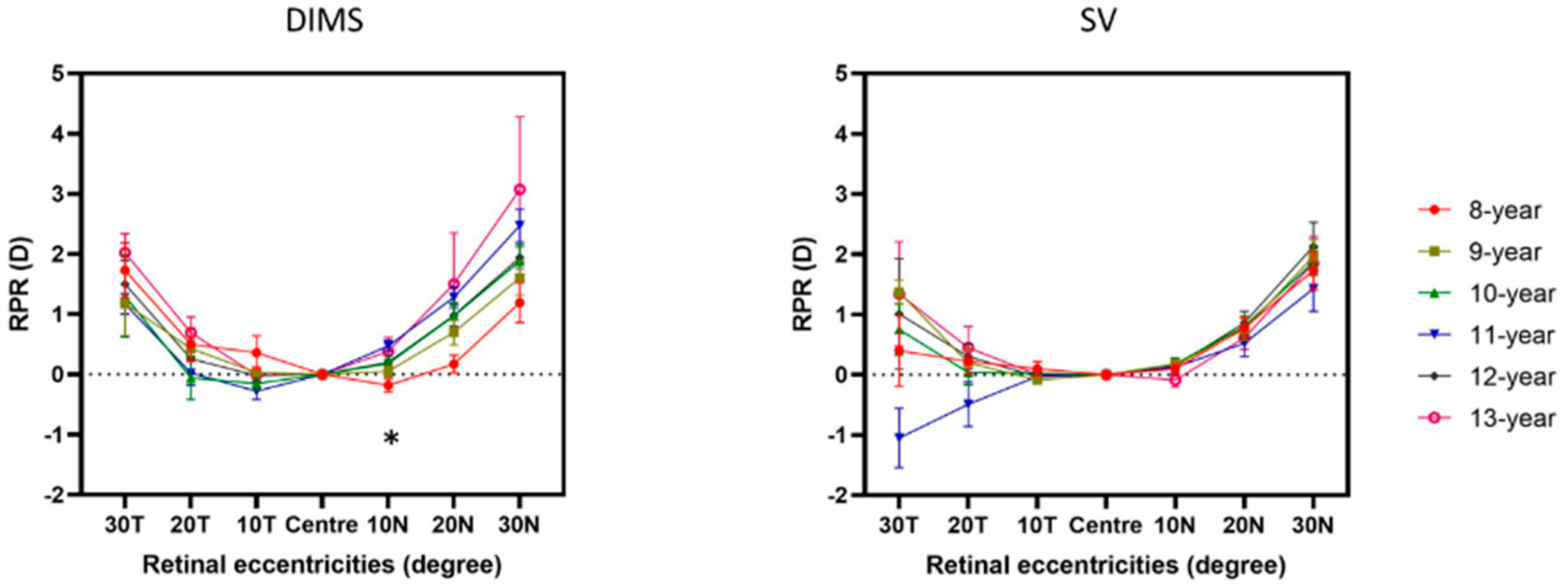
3.3. RPR and Age
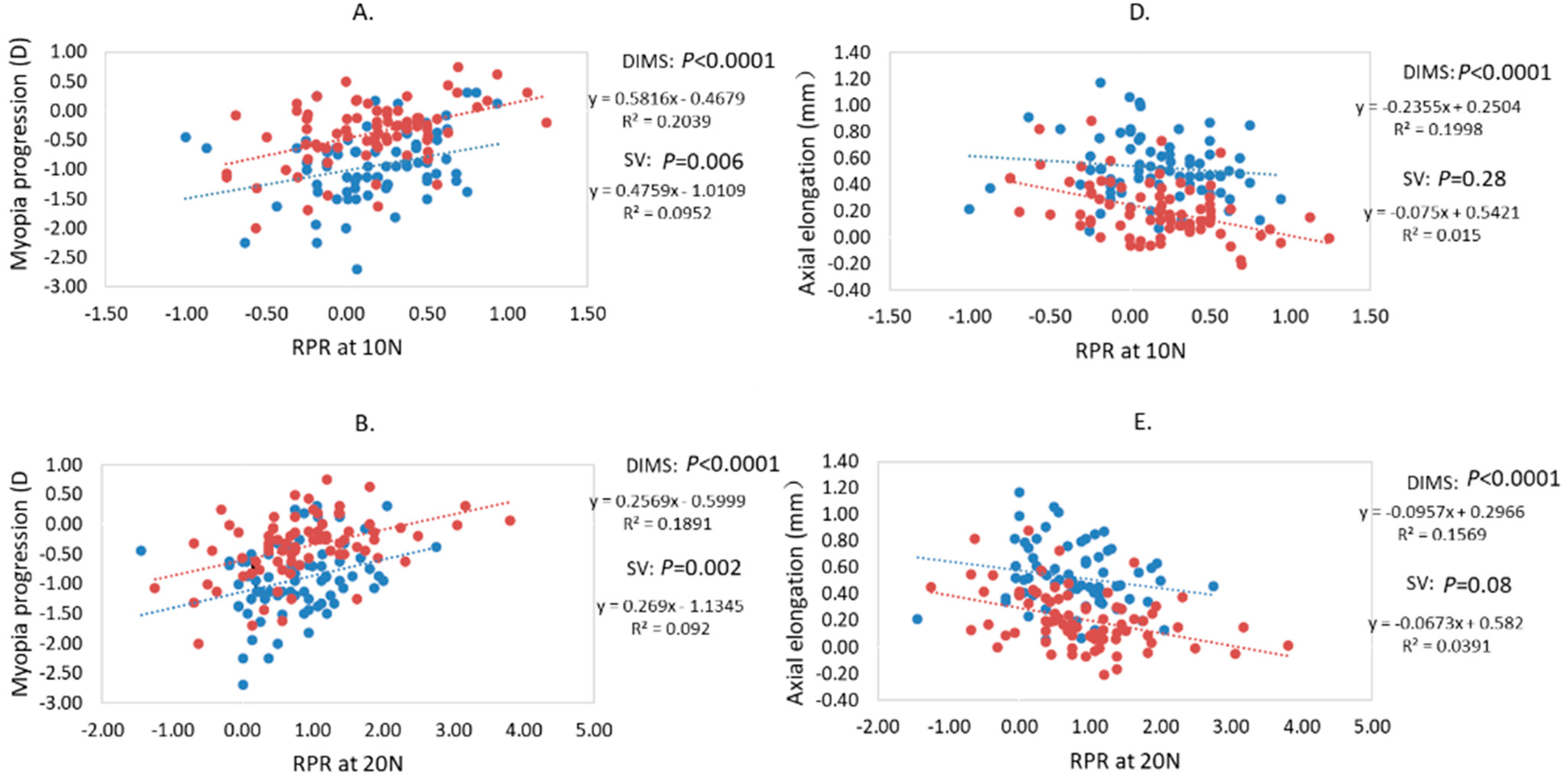
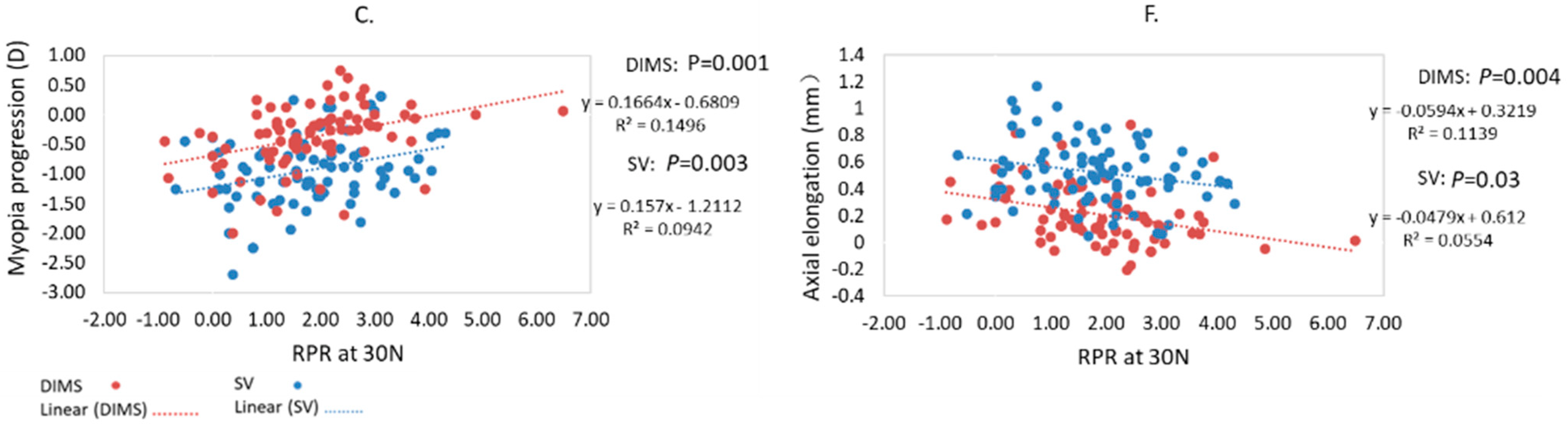
3.4. Relationship between Baseline RPR and Myopia Progression and Axial Elongation
3.5. Comparison between Baseline Myopic RPR and Hyperopic RPR at 10 N and 20 N Subgroups
4. Discussion
4.1. RPR in Young Children
4.2. RPR in Relation with Myopia Progression and Axial Elongation
4.3. RPR in Myopia Control Using Myopic Defocus
4.4. The Effective Range of Myopic Defocus in Myopia Control
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Villarreal, M.G.; Ohlsson, J.; Abrahamsson, M.; Sjöström, A.; Sjöstrand, J. Myopisation: The refractive tendency in teenagers. Prevalence of myopia among young teenagers in Sweden. Acta Ophthalmol. 2000, 78, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.W.; Ramamurthy, D.; Saw, S.M. Worldwide prevalence and risk factors for myopia. Ophthalmic Physiol. Opt. 2012, 32, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.W.; Dirani, M.; Cheng, C.Y.; Wong, T.Y.; Saw, S.M. The age-specific prevalence of myopia in Asia: A meta-analysis. Optom. Vis. Sci. 2015, 92, 258–266. [Google Scholar] [CrossRef] [PubMed]
- Saw, S.M.; Gazzard, G.; Shih-Yen, E.C.; Chua, W.H. Myopia and associated pathological complications. Ophthalmic Physiol. Opt. 2005, 25, 381–391. [Google Scholar] [CrossRef] [PubMed]
- Marcus, M.W.; de Vries, M.M.; Junoy Montolio, F.G.; Jansonius, N.M. Myopia as a risk factor for open-angle glaucoma: A systematic review and meta-analysis. Ophthalmology 2011, 118, 1989–1994.e2. [Google Scholar] [CrossRef]
- Smith, E.L., 3rd; Hung, L.F.; Huang, J. Relative peripheral hyperopic defocus alters central refractive development in infant monkeys. Vis. Res. 2009, 49, 2386–2392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, E.L., 3rd; Kee, C.S.; Ramamirtham, R.; Qiao-Grider, Y.; Hung, L.F. Peripheral vision can influence eye growth and refractive development in infant monkeys. Investig. Ophthalmol. Vis. Sci. 2005, 46, 3965–3972. [Google Scholar] [CrossRef] [PubMed]
- Morgan, I.G.; Ambadeniya, M.P. Imposed Peripheral Myopic Defocus Can Prevent the Development of Lens–Induced Myopia. Investig. Ophthalmol. Vis. Sci. 2006, 47, 3328. [Google Scholar]
- Smith, E.L., 3rd; Hung, L.F.; Huang, J.; Arumugam, B. Effects of local myopic defocus on refractive development in monkeys. Optom. Vis. Sci. 2013, 90, 1176–1186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, Z.; Martinez, A.; Chen, X.; Li, L.; Sankaridurg, P.; Holden, B.A.; Ge, J. Peripheral defocus with single-vision spectacle lenses in myopic children. Optom. Vis. Sci. 2010, 87, 4–9. [Google Scholar] [CrossRef]
- Backhouse, S.; Fox, S.; Ibrahim, B.; Phillips, J.R. Peripheral refraction in myopia corrected with spectacles versus contact lenses. Ophthalmic Physiol. Opt. 2012, 32, 294–303. [Google Scholar] [CrossRef] [Green Version]
- Lam, C.S.; Tang, W.C.; Tse, D.Y.; Tang, Y.Y.; To, C.H. Defocus Incorporated Soft Contact (DISC) lens slows myopia progression in Hong Kong Chinese schoolchildren: A 2-year randomised clinical trial. Br. J. Ophthalmol. 2014, 98, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Lam, C.S.Y.; Tang, W.C.; Tse, D.Y.; Lee, R.P.K.; Chun, R.K.M.; Hasegawa, K.; Qi, H.; Hatanaka, T.; To, C.H. Defocus Incorporated Multiple Segments (DIMS) spectacle lenses slow myopia progression: A 2-year randomised clinical trial. Br. J. Ophthalmol. 2020, 104, 363–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chamberlain, P.; Peixoto-de-Matos, S.C.; Logan, N.S.; Ngo, C.; Jones, D.; Young, G. A 3-year Randomized Clinical Trial of MiSight Lenses for Myopia Control. Optom. Vis. Sci. 2019, 96, 556–567. [Google Scholar] [CrossRef] [Green Version]
- Sng, C.C.; Lin, X.Y.; Gazzard, G.; Chang, B.; Dirani, M.; Chia, A.; Selvaraj, P.; Ian, K.; Drobe, B.; Wong, T.Y.; et al. Peripheral refraction and refractive error in singapore chinese children. Investig. Ophthalmol. Vis. Sci. 2011, 52, 1181–1190. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Sankaridurg, P.; Donovan, L.; Lin, Z.; Li, L.; Martinez, A.; Holden, B.; Ge, J. Characteristics of peripheral refractive errors of myopic and non-myopic Chinese eyes. Vis. Res. 2010, 50, 31–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, S.M.; Li, S.Y.; Liu, L.R.; Zhou, Y.H.; Yang, Z.; Kang, M.T.; Li, H.; Yang, X.Y.; Wang, Y.P.; Zhan, S.Y.; et al. Peripheral refraction in 7- and 14-year-old children in central China: The Anyang Childhood Eye Study. Br. J. Ophthalmol. 2015, 99, 674–679. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.T.; Cho, P. Relative peripheral refraction in children: Twelve-month changes in eyes with different ametropias. Ophthalmic Physiol. Opt. 2013, 33, 283–293. [Google Scholar] [CrossRef] [PubMed]
- Seidemann, A.; Schaeffel, F.; Guirao, A.; Lopez-Gil, N.; Artal, P. Peripheral refractive errors in myopic, emmetropic, and hyperopic young subjects. J. Opt. Soc. Am. A Opt. Image Sci. Vis. 2002, 19, 2363–2373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sng, C.C.; Lin, X.Y.; Gazzard, G.; Chang, B.; Dirani, M.; Lim, L.; Selvaraj, P.; Ian, K.; Drobe, B.; Wong, T.Y.; et al. Change in peripheral refraction over time in Singapore Chinese children. Investig. Ophthalmol. Vis. Sci. 2011, 52, 7880–7887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lam, C.S.Y.; Tang, W.C.; Qi, H.; Radhakrishnan, H.; Hasegawa, K.; To, C.H.; Charman, W.N. Effect of Defocus Incorporated Multiple Segments Spectacle Lens Wear on Visual Function in Myopic Chinese Children. Transl. Vis. Sci. Technol. 2020, 9, 11. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.Y.; Lam, C.S.Y.; Tang, W.C.; Leung, M.; To, C.H. Defocus Incorporated Multiple Segments Spectacle Lenses Changed the Relative Peripheral Refraction: A 2-Year Randomized Clinical Trial. Investig. Ophthalmol. Vis. Sci. 2020, 61, 53. [Google Scholar] [CrossRef]
- Hartwig, A.; Charman, W.N.; Radhakrishnan, H. Baseline peripheral refractive error and changes in axial refraction during one year in a young adult population. J. Optom. 2016, 9, 32–39. [Google Scholar] [CrossRef]
- Thibos, L.N.; Wheeler, W.; Horner, D. Power vectors: An application of Fourier analysis to the description and statistical analysis of refractive error. Optom. Vis. Sci. 1997, 74, 367–375. [Google Scholar] [CrossRef] [PubMed]
- Atchison, D.A.; Pritchard, N.; Schmid, K.L. Peripheral refraction along the horizontal and vertical visual fields in myopia. Vis. Res. 2006, 46, 1450–1458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atchison, D.A.; Pritchard, N.; White, S.D.; Griffiths, A.M. Influence of age on peripheral refraction. Vis. Res. 2005, 45, 715–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atchison, D.A.; Li, S.M.; Li, H.; Li, S.Y.; Liu, L.R.; Kang, M.T.; Meng, B.; Sun, Y.Y.; Zhan, S.Y.; Mitchell, P.; et al. Relative Peripheral Hyperopia Does Not Predict Development and Progression of Myopia in Children. Investig. Ophthalmol. Vis. Sci. 2015, 56, 6162–6170. [Google Scholar] [CrossRef] [PubMed]
- Hoogerheide, J.; Rempt, F.; Hoogenboom, W. Acquired myopia in young pilots. Ophthalmologica 1971, 163, 209–215. [Google Scholar] [CrossRef]
- Mutti, D.O.; Hayes, J.R.; Mitchell, G.L.; Jones, L.A.; Moeschberger, M.L.; Cotter, S.A.; Kleinstein, R.N.; Manny, R.E.; Twelker, J.D.; Zadnik, K.; et al. Refractive error, axial length, and relative peripheral refractive error before and after the onset of myopia. Investig. Ophthalmol. Vis. Sci. 2007, 48, 2510–2519. [Google Scholar] [CrossRef] [PubMed]
- Logan, N.S.; Radhakrishnan, H.; Cruickshank, F.E.; Allen, P.M.; Bandela, P.K.; Davies, L.N.; Hasebe, S.; Khanal, S.; Schmid, K.L.; Vera-Diaz, F.A.; et al. IMI Accommodation and Binocular Vision in Myopia Development and Progression. Investig. Ophthalmol. Vis. Sci. 2021, 62, 4. [Google Scholar] [CrossRef]
- Walline, J.J.; Walker, M.K.; Mutti, D.O.; Jones-Jordan, L.A.; Sinnott, L.T.; Giannoni, A.G.; Bickle, K.M.; Schulle, K.L.; Nixon, A.; Pierce, G.E.; et al. Effect of High Add Power, Medium Add Power, or Single-Vision Contact Lenses on Myopia Progression in Children: The BLINK Randomized Clinical Trial. JAMA 2020, 324, 571–580. [Google Scholar] [CrossRef] [PubMed]
- Lam, C.S.Y.; Tang, W.C.; Lee, P.H.; Zhang, H.Y.; Qi, H.; Hasegawa, K.; To, C.H. Myopia control effect of defocus incorporated multiple segments (DIMS) spectacle lens in Chinese children: Results of a 3-year follow-up study. Br. J. Ophthalmol. 2021, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Irving, E.L.; Sivak, J.G.; Callender, M.G. Refractive plasticity of the developing chick eye. Ophthalmic Physiol. Opt. 1992, 12, 448–456. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Kurihara, T.; Kunimi, H.; Miyauchi, M.; Ikeda, S.I.; Mori, K.; Tsubota, K.; Torii, H.; Tsubota, K. A highly efficient murine model of experimental myopia. Sci. Rep. 2018, 8, 2026. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.L., 3rd; Hung, L.-F. The role of optical defocus in regulating refractive development in infant monkeys. Vis. Res. 1999, 39, 1415–1435. [Google Scholar] [CrossRef] [Green Version]
- Garcia Garcia, M.; Wahl, S.; Pusti, D.; Artal, P.; Ohlendorf, A. 2-D Peripheral image quality metrics with different types of multifocal contact lenses. Sci. Rep. 2019, 9, 18487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Troilo, D.; Smith, E.L., 3rd; Nickla, D.L.; Ashby, R.; Tkatchenko, A.V.; Ostrin, L.A.; Gawne, T.J.; Pardue, M.T.; Summers, J.A.; Kee, C.S.; et al. IMI—Report on Experimental Models of Emmetropization and Myopia. Investig. Ophthalmol. Vis. Sci. 2019, 60, M31–M88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowrey, H.E.; Zeng, G.; Tse, D.Y.; Leotta, A.J.; Wu, Y.; To, C.H.; Wildsoet, C.F.; McFadden, S.A. The Effect of Spectacle Lenses Containing Peripheral Defocus on Refractive Error and Horizontal Eye Shape in the Guinea Pig. Investig. Ophthalmol. Vis. Sci. 2017, 58, 2705–2714. [Google Scholar] [CrossRef] [Green Version]
- Berntsen, D.A.; Barr, C.D.; Mutti, D.O.; Zadnik, K. Peripheral defocus and myopia progression in myopic children randomly assigned to wear single vision and progressive addition lenses. Investig. Ophthalmol. Vis. Sci. 2013, 54, 5761–5770. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Ciuffreda, K.J. Depth-of-focus of the human eye in the near retinal periphery. Vis. Res. 2004, 44, 1115–1125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.Z.; Thibos, L.N.; Bradley, A. Effects of refractive error on detection acuity and resolution acuity in peripheral vision. Investig. Ophthalmol. Vis. Sci. 1997, 38, 2134–2143. [Google Scholar]
- Faria-Ribeiro, M.; Queirós, A.; Lopes-Ferreira, D.; Jorge, J.; González-Méijome, J.M. Peripheral refraction and retinal contour in stable and progressive myopia. Optom. Vis. Sci. 2013, 90, 9–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, E.L., 3rd; Arumugam, B.; Hung, L.F.; She, Z.; Beach, K.; Sankaridurg, P. Eccentricity-dependent effects of simultaneous competing defocus on emmetropization in infant rhesus monkeys. Vis. Res. 2020, 177, 32–40. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Relative Peripheral Refraction at Baseline | Myopia Progression | Axial Elongation | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Regression Coefficient | 95% CI for B | p† | Regression Coefficient | 95% CI for B | p† | ||||
| B | Lower Bound | Upper Bound | B | Lower Bound | Upper Bound | ||||
| Adjusting for Age, Gender and Initial Refractive Error | Adjusting for Age, Gender and Initial Axial Length | ||||||||
| DIMS group | |||||||||
| 10 T | 0.00 | −0.24 | 0.24 | 0.99 | 0.03 | −0.08 | 0.11 | 0.74 | |
| 20 T | −0.08 | −0.17 | 0.08 | 0.45 | 0.03 | −0.04 | 0.05 | 0.77 | |
| 30 T | 0.03 | −0.08 | 0.10 | 0.81 | −0.08 | −0.05 | 0.02 | 0.53 | |
| 10 N | 0.36 | 0.19 | 0.74 | 0.001 | −0.35 | −0.29 | −0.08 | 0.001 | |
| 20 N | 0.35 | 0.08 | 0.33 | 0.001 | −0.30 | −0.12 | −0.02 | 0.004 | |
| 30 N | 0.25 | 0.01 | 0.20 | 0.03 | −0.22 | −0.08 | −0.002 | 0.05 | |
| SV group | |||||||||
| 10 T | 0.06 | −0.28 | 0.48 | 0.59 | 0.03 | −0.12 | 0.15 | 0.77 | |
| 20 T | −0.06 | −0.18 | 0.11 | 0.62 | 0.11 | −0.02 | 0.08 | 0.29 | |
| 30 T | −0.07 | −0.13 | 0.08 | 0.65 | 0.14 | −0.02 | 0.06 | 0.29 | |
| 10 N | 0.37 | 0.23 | 0.90 | 0.001 | −0.15 | −0.22 | 0.03 | 0.13 | |
| 20 N | 0.36 | 0.12 | 0.49 | 0.001 | −0.23 | −0.14 | −0.01 | 0.02 | |
| 30 N | 0.35 | 0.07 | 0.29 | 0.002 | −0.24 | −0.09 | 0.009 | 0.02 | |
| Myopic RPR at 10 N | Hyperopic RPR at 10 N | Mean Difference | †p Value | |||
|---|---|---|---|---|---|---|
| Mean ± SD | n | Mean ± SD | n | |||
| DIMS group | ||||||
| Myopia progression (D) | −0.61 ± 0.60 | 27 | −0.25 ± 0.44 | 52 | −0.36 ± 0.14 | 0.009 |
| Axial elongation (mm) | 0.32 ± 0.24 | 27 | 0.16 ± 0.18 | 52 | 0.16 ± 0.05 | 0.001 |
| SV group | ||||||
| Myopia progression (D) | −1.10 ± 0.58 | 27 | −0.84 ± 0.59 | 54 | 0.26 ± 0.14 | 0.06 |
| Axial elongation (mm) | 0.55 ± 0.27 | 27 | 0.51 ± 0.22 | 54 | 0.04 ± 0.05 | 0.48 |
| Myopic RPR at 20 N | Hyperopic RPR at 20 N | Mean Difference | †p Value | |||
|---|---|---|---|---|---|---|
| Mean ± SD | n | Mean ± SD | n | |||
| DIMS group | ||||||
| Myopia progression (D) | −0.72 ± 0.64 | 12 | −0.31 ± 0.48 | 67 | −0.40 ± 0.16 | 0.01 |
| Axial elongation (mm) | 0.34 ± 0.24 | 12 | 0.19 ± 0.20 | 67 | 0.15 ± 0.07 | 0.02 |
| SV group | ||||||
| Myopia progression (D) | −1.14 ± 0.53 | 11 | −0.89 ± 0.60 | 70 | −0.25 ± 0.20 | 0.19 |
| Axial elongation (mm) | 0.60 ± 0.28 | 11 | 0.51 ± 0.23 | 70 | 0.08 ± 0.08 | 0.27 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, H.; Lam, C.S.Y.; Tang, W.-C.; Leung, M.; Qi, H.; Lee, P.H.; To, C.-H. Myopia Control Effect Is Influenced by Baseline Relative Peripheral Refraction in Children Wearing Defocus Incorporated Multiple Segments (DIMS) Spectacle Lenses. J. Clin. Med. 2022, 11, 2294. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11092294
Zhang H, Lam CSY, Tang W-C, Leung M, Qi H, Lee PH, To C-H. Myopia Control Effect Is Influenced by Baseline Relative Peripheral Refraction in Children Wearing Defocus Incorporated Multiple Segments (DIMS) Spectacle Lenses. Journal of Clinical Medicine. 2022; 11(9):2294. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11092294
Chicago/Turabian StyleZhang, Hanyu, Carly S. Y. Lam, Wing-Chun Tang, Myra Leung, Hua Qi, Paul H. Lee, and Chi-Ho To. 2022. "Myopia Control Effect Is Influenced by Baseline Relative Peripheral Refraction in Children Wearing Defocus Incorporated Multiple Segments (DIMS) Spectacle Lenses" Journal of Clinical Medicine 11, no. 9: 2294. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11092294