
3D Printing and Virtual Surgical Planning in Oral and Maxillofacial Surgery


 ,
,
Abstract
:1. Introduction
1.1. Industrial Revolutions and the 3D Printing Era
1.2. Overview of AM Technologies
2. 3D Printing in OMFS
2.1. The 3DP Point-of-Care Concept
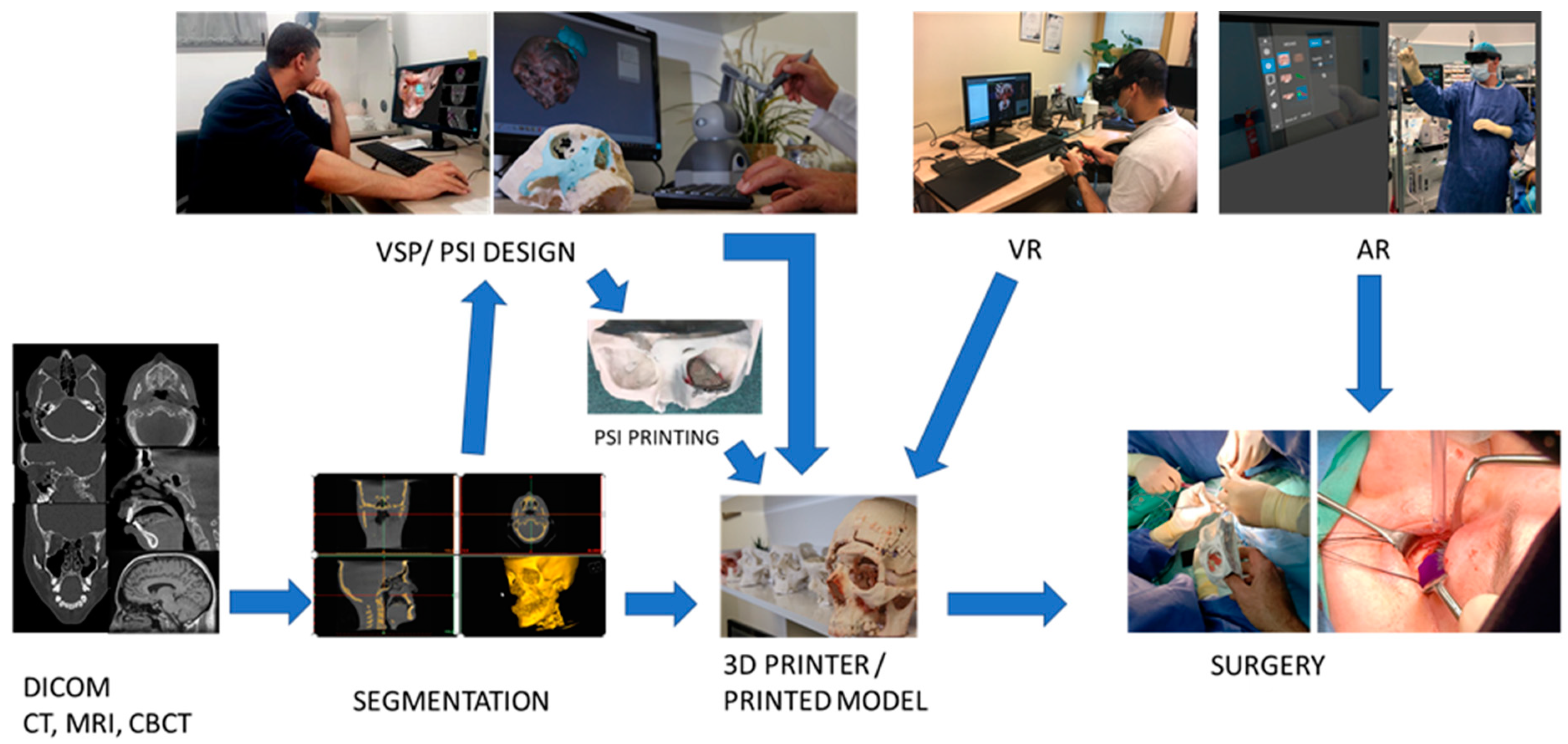
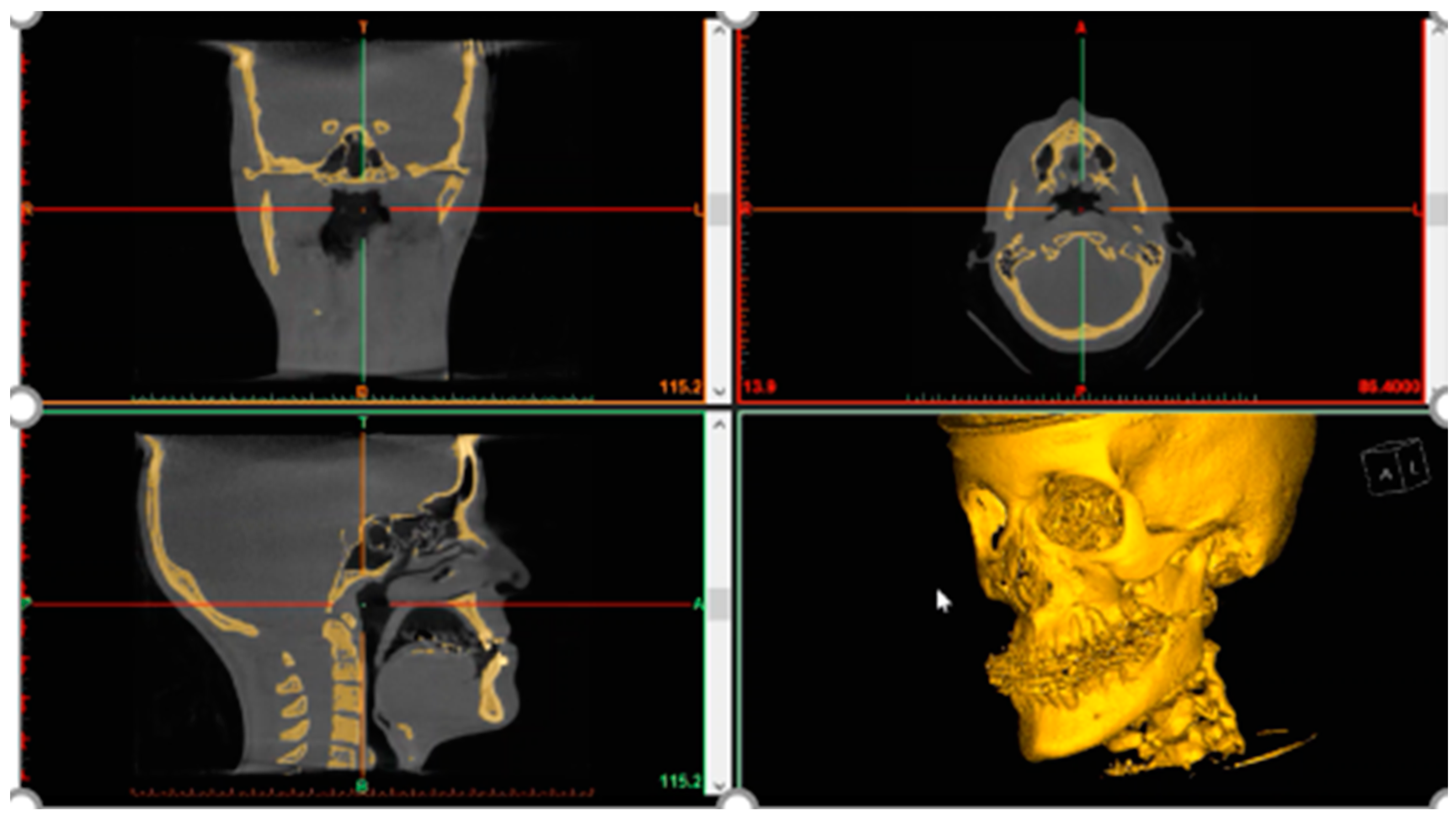
2.2. Common 3DP Point-of-Care Workflow in OMFS
3. Clinical Applications of 3D Printing in OMFS
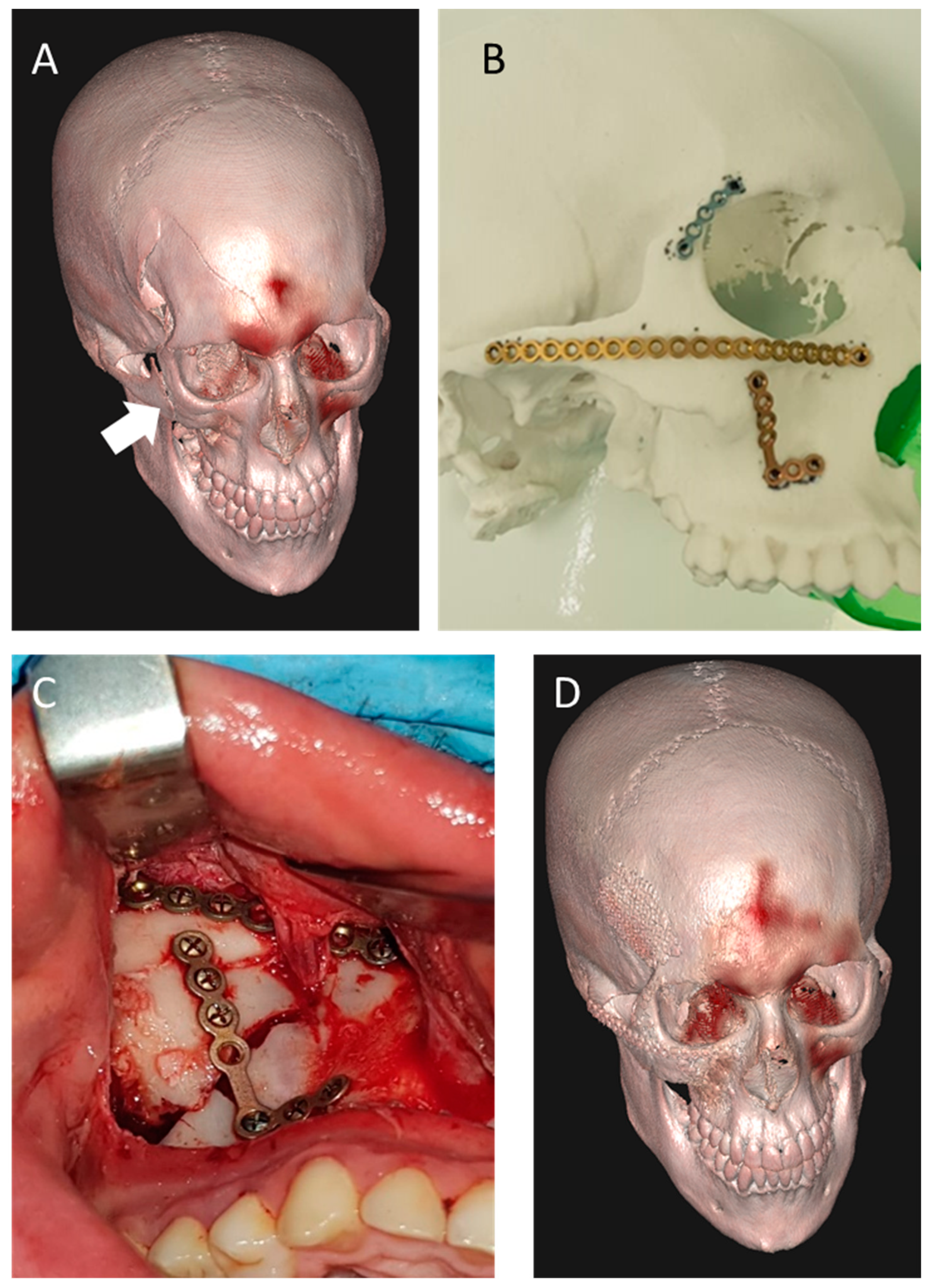
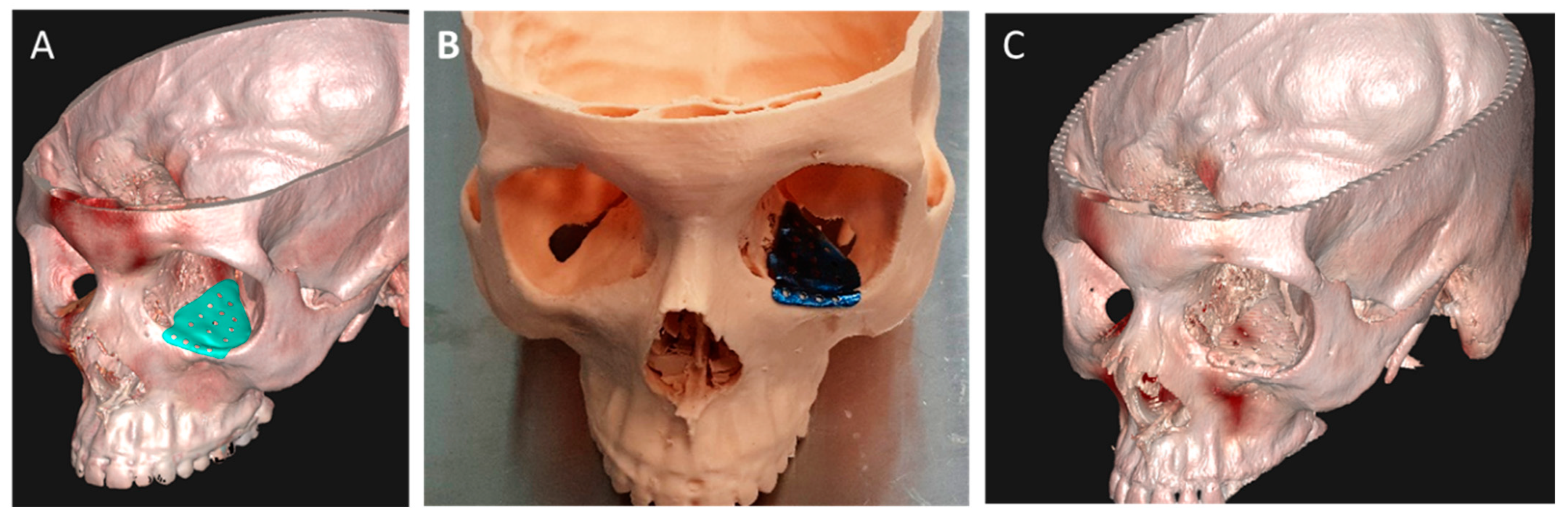
3.1. 3D Planning and Manufacturing for Management of Facial Trauma
3.2. 3D Planning and Manufacturing in Orthognathic Surgery
3.3. 3D-Based Digitization and Planning for Maxillofacial Tumor Resection and Reconstruction
3.4. Total Joint Replacement (TJR) in the Era of 3D Printing
3.5. Virtual Reality (VR) and Augmented Reality (AR) for OMFS
3.6. 3D-Based Tissue Engineering and Translational Medicine in OMFS
4. Discussion, Challenges and Future Prospects
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schwab, K. The Fourth Industrial Revolution: What It Means and How to Respond; World Economic Forum: New York, NY, USA, 2016; Available online: https://www.weforum.org/agenda/2016/01/the-fourth-industrial-revolution-what-it-means-and-how-to-respond/ (accessed on 14 February 2022).
- Ngo, T.D.; Kashani, A.; Imbalzano, G.; Nguyen, K.T.Q.; Hui, D. Additive manufacturing (3D printing): A review of materials, methods, applications and challenges. Compos. Part B Eng. 2018, 143, 172–196. [Google Scholar] [CrossRef]
- Steenhuis, H.J.; Pretorius, L. The additive manufacturing innovation: A range of implications. J. Manuf. Technol. Manag. 2017, 28, 122–143. [Google Scholar] [CrossRef]
- Barnatt, C. 3D Printing: The Next Industrial Revolution; CreateSpace: Scotts Valley, CA, USA, 2013. [Google Scholar]
- Aguado, B.A.; Grim, J.C.; Rosales, A.M.; Watson-Capps, J.J.; Anseth, K.S. Engineering precision biomaterials for personalized medicine. Sci. Transl. Med. 2018, 10, eaam8645. [Google Scholar] [CrossRef] [PubMed]
- Wohlers, T.; Caffrey, T.; Campbell, I. Wohlers Report 2016. 2016. Available online: https://wohlersassociates.com/press71.html (accessed on 18 February 2022).
- Hull, C. Apparatus for Production of Three Dimensional Objects by Stereolithography. U.S. Patent 4,575,330, 11 March 1986. [Google Scholar]
- Alexander, A.E.; Wake, N.; Chepelev, L.; Brantner, P.; Ryan, J.; Wang, K.C. A guideline for 3D printing terminology in biomedical research utilizing ISO/ASTM standards. 3D Print. Med. 2021, 7, 8. [Google Scholar] [CrossRef]
- Louvrier, A.; Marty, P.; Barrabé, A.; Euvrard, E.; Chatelain, B.; Weber, E.; Meyer, C. How useful is 3D printing in maxillofacial surgery? J. Stomatol. Oral Maxillofac. Surg. 2017, 118, 206–212. [Google Scholar] [CrossRef]
- Ziaee, M.; Crane, N.B. Binder jetting: A review of process, materials, and methods. Addit. Manuf. 2019, 28, 781–801. [Google Scholar] [CrossRef]
- Lores, A.; Azurmendi, N.; Agote, I.; Zuza, E. A review on recent developments in binder jetting metal additive manufacturing: Materials and process characteristics. Powder Metall. 2019, 62, 267–296. [Google Scholar] [CrossRef]
- Stansbury, J.W.; Idacavage, M.J. 3D printing with polymers: Challenges among expanding options and opportunities. Dent. Mater. 2016, 32, 54–64. [Google Scholar] [CrossRef]
- Anadioti, E.; Kane, B.; Soulas, E. Current and Emerging Applications of 3D Printing in Restorative Dentistry. Curr. Oral Health Rep. 2018, 5, 133–139. [Google Scholar] [CrossRef]
- Mai, H.N.; Lee, K.B.; Lee, D.H. Fit of interim crowns fabricated using photopolymer-jetting 3D printing. J. Prosthet. Dent. 2017, 118, 208–215. [Google Scholar] [CrossRef]
- Saboori, A.; Gallo, D.; Biamino, S.; Fino, P.; Lombardi, M. An overview of additive manufacturing of titanium components by directed energy deposition: Microstructure and mechanical properties. Appl. Sci. 2017, 7, 883. [Google Scholar] [CrossRef] [Green Version]
- Mazzoli, A.; Germani, M.; Raffaeli, R. Direct fabrication through electron beam melting technology of custom cranial implants designed in a PHANToM-based haptic environment. Mater. Des. 2009, 30, 3186–3192. [Google Scholar] [CrossRef]
- Ran, Q.; Yang, W.; Hu, Y.; Shen, X.; Yu, Y.; Xiang, Y.; Cai, K. Osteogenesis of 3D printed porous Ti6Al4V implants with different pore sizes. J. Mech. Behav. Biomed. Mater. 2018, 84, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Odkhuu, M.; Cho, S.; Li, J.; Park, B.Y.; Kim, J.W. 3D-printed titanium implant with pre-mounted dental implants for mandible reconstruction: A case report. Maxillofac. Plast. Reconstr. Surg. 2020, 42, 28. [Google Scholar] [CrossRef]
- Roth, G.A.; Geraci, C.L.; Stefaniak, A.; Murashov, V.; Howard, J. Potential occupational hazards of additive manufacturing. J. Occup. Environ. Hyg. 2019, 16, 321–328. [Google Scholar] [CrossRef]
- Svetlizky, D.; Das, M.; Zheng, B.; Vyatskikh, A.L.; Bose, S.; Bandyopadhyay, A.; Schoenung, J.M.; Lavernia, E.J.; Eliaz, N. Directed energy deposition (DED) additive manufacturing: Physical characteristics, defects, challenges and application. Mater. Today 2021, 49, 271–295. [Google Scholar] [CrossRef]
- Heras, E.S.; Haro, F.B.; María, J.; Del Burgo, A.; Marcos, M.E.I. Plate auto-level system for fused deposition modelling (FDM) 3D printers. Rapid Prototyp. J. 2017, 23, 401–413. [Google Scholar] [CrossRef]
- Culmone, C.; Smit, G.; Breedveld, P. Additive manufacturing of medical instruments: A state-of-the-art review. Addit. Manuf. 2019, 27, 461–473. [Google Scholar] [CrossRef]
- Fallon, J.J.; McKnight, S.H.; Bortner, M.J. Highly loaded fiber filled polymers for material extrusion: A review of current understanding. Addit. Manuf. 2019, 30, 100810. [Google Scholar] [CrossRef]
- Kessler, A.; Hickel, R.; Reymus, M. 3D printing in dentistry-state of the art. Oper. Dent. 2020, 45, 30–40. [Google Scholar] [CrossRef]
- Arnesano, A.; Kunjalukkal Padmanabhan, S.; Notarangelo, A.; Montagna, F.; Licciulli, A. Fused deposition modeling shaping of glass infiltrated alumina for dental restoration. Ceram. Int. 2020, 46, 2206–2212. [Google Scholar] [CrossRef]
- Brandt, J.; Lauer, H.C.; Peter, T.; Brandt, S. Digital process for an implant-supported fixed dental prosthesis: A clinical report. J. Prosthet. Dent. 2015, 114, 469–473. [Google Scholar] [CrossRef] [PubMed]
- Tee, Y.L.; Tran, P.; Leary, M.; Pille, P.; Brandt, M. 3D Printing of polymer composites with material jetting: Mechanical and fractographic analysis. Addit. Manuf. 2020, 36, 101558. [Google Scholar] [CrossRef]
- Väisänen, A.J.K.; Hyttinen, M.; Ylönen, S.; Alonen, L. Occupational exposure to gaseous and particulate contaminants originating from additive manufacturing of liquid, powdered, and filament plastic materials and related post-processes. J. Occup. Environ. Hyg. 2019, 16, 258–271. [Google Scholar] [CrossRef]
- Hazeveld, A.; Huddleston Slater, J.J.R.; Ren, Y. Accuracy and reproducibility of dental replica models reconstructed by different rapid prototyping techniques. Am. J. Orthod. Dentofac. Orthop. 2014, 145, 108–115. [Google Scholar] [CrossRef]
- Jain, R.; Supriya, B.S.; Gupta, K. Recent Trends of 3-D Printing in Dentistry—A review. Ann. Prosthodont. Restor. Dent. 2016, 2, 101–104. [Google Scholar]
- Sutton, A.T.; Kriewall, C.S.; Leu, M.C.; Newkirk, J.W. Powder characterisation techniques and effects of powder characteristics on part properties in powder-bed fusion processes. Virtual Phys. Prototyp. 2017, 12, 3–29. [Google Scholar] [CrossRef]
- Sun, S.; Brandt, M.; Easton, M. Powder bed fusion processes: An overview. In Laser Additive Manufacturing: Materials, Design, Technologies, and Applications; Elsevier Inc.: Amsterdam, The Netherlands, 2017; pp. 55–77. [Google Scholar] [CrossRef]
- Druzgalski, C.L.; Ashby, A.; Guss, G.; King, W.E.; Roehling, T.T.; Matthews, M.J. Process optimization of complex geometries using feed forward control for laser powder bed fusion additive manufacturing. Addit. Manuf. 2020, 34, 101169. [Google Scholar] [CrossRef]
- Olakanmi, E.O.; Cochrane, R.F.; Dalgarno, K.W. A review on selective laser sintering/melting (SLS/SLM) of aluminium alloy powders: Processing, microstructure, and properties. Prog. Mater. Sci. 2015, 74, 401–477. [Google Scholar] [CrossRef]
- Nouri, A.; Rohani Shirvan, A.; Li, Y.; Wen, C. Additive manufacturing of metallic and polymeric load-bearing biomaterials using laser powder bed fusion: A review. J. Mater. Sci. Technol. 2021, 94, 196–215. [Google Scholar] [CrossRef]
- Alageel, O.; Abdallah, M.N.; Alsheghri, A.; Song, J.; Caron, E.; Tamimi, F. Removable partial denture alloys processed by laser-sintering technique. J. Biomed. Mater. Res. Part B Appl. Biomater. 2018, 106, 1174–1185. [Google Scholar] [CrossRef] [PubMed]
- Tunchel, S.; Blay, A.; Kolerman, R.; Mijiritsky, E.; Shibli, J.A. 3D Printing/Additive Manufacturing Single Titanium Dental Implants: A Prospective Multicenter Study with 3 Years of Follow-Up. Int. J. Dent. 2016, 2016, 8590971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Xie, B.; Jin, J.; Chai, Y.; Chen, Y. 3D Printing Temporary Crown and Bridge by Temperature Controlled Mask Image Projection Stereolithography. Procedia Manuf. 2018, 26, 1023–1033. [Google Scholar] [CrossRef]
- Aly, P.; Mohsen, C. Comparison of the Accuracy of Three-Dimensional Printed Casts, Digital, and Conventional Casts: An in Vitro Study. Eur. J. Dent. 2020, 14, 189–193. [Google Scholar] [CrossRef] [Green Version]
- Dikova, T. Production of high-quality temporary crowns and bridges by stereolithography. Scr. Sci. Med. Dent. 2019, 5, 33. [Google Scholar] [CrossRef]
- Sun, Y.; Luebbers, H.T.; Agbaje, J.O.; Schepers, S.; Politis, C.; Van Slycke, S.; Vrielinck, L. Accuracy of Dental Implant Placement Using CBCT-Derived Mucosa-Supported Stereolithographic Template. Clin. Implant Dent. Relat. Res. 2015, 17, 862–870. [Google Scholar] [CrossRef]
- Kessler, A.; Reichl, F.X.; Folwaczny, M.; Högg, C. Monomer release from surgical guide resins manufactured with different 3D printing devices. Dent. Mater. 2020, 36, 1486–1492. [Google Scholar] [CrossRef]
- Coburn, J.; Di Prima, M. 3D Printing Medical Devices at Point of Care. 2019. Available online: http://www.sme.org/POC/ (accessed on 1 January 2020).
- SME Medical Additive Manufacturing/3D Printing Annual Report 2018. 2018. Available online: https://www.sme.org/smemedia/white-papers-and-reports/medical-additive-manufacturing-3d-printing-annual-report-2018/ (accessed on 24 February 2022).
- Bosc, R.; Hersant, B.; Carloni, R.; Niddam, J.; Bouhassira, J.; De Kermadec, H.; Bequignon, E.; Wojcik, T.; Julieron, M.; Meningaud, J.P. Mandibular reconstruction after cancer: An in-house approach to manufacturing cutting guides. Int. J. Oral Maxillofac. Surg. 2017, 46, 24–31. [Google Scholar] [CrossRef]
- Damecourt, A.; Nieto, N.; Galmiche, S.; Garrel, R.; de Boutray, M. In-house 3D treatment planning for mandibular reconstruction by free fibula flap in cancer: Our technique. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2020, 137, 501–505. [Google Scholar] [CrossRef]
- Naros, A.; Weise, H.; Tilsen, F.; Hoefert, S.; Naros, G.; Krimmel, M.; Reinert, S.; Polligkeit, J. Three-dimensional accuracy of mandibular reconstruction by patient-specific pre-bent reconstruction plates using an “in-house” 3D-printer. J. Cranio-Maxillofac. Surg. 2018, 46, 1645–1651. [Google Scholar] [CrossRef]
- Numajiri, T.; Morita, D.; Yamochi, R.; Nakamura, H.; Tsujiko, S.; Sowa, Y.; Toyoda, K.; Tsujikawa, T.; Arai, A.; Hirano, S. Does an in-house computer-aided design/computer-aided manufacturing approach contribute to accuracy and time shortening in mandibular reconstruction? J. Craniofac. Surg. 2020, 31, 1928–1932. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, C.A.; Lin, A.Y. A new classification of three-dimensional printing technologies: Systematic review of three-dimensional printing for patient-specific craniomaxillofacial surgery. Plast. Reconstr. Surg. 2017, 139, 1211–1220. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.F.; Alfi, D.; Alfi, J.; Huang, A.T. The Use of Patient-Specific Implants in Oral and Maxillofacial Surgery. Oral Maxillofac. Surg. Clin. N. Am. 2019, 31, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Kupfer, P.; Cheng, A.; Patel, A.; Amundson, M.; Dierks, E.J.; Bell, R.B. Virtual Surgical Planning and Intraoperative Imaging in Management of Ballistic Facial and Mandibular Condylar Injuries. Atlas Oral Maxillofac. Surg. Clin. N. Am. 2017, 25, 17–23. [Google Scholar] [CrossRef]
- Toto, J.M.; Chang, E.I.; Agag, R.; Devarajan, K.; Patel, S.A.; Topham, N.S. Improved operative efficiency of free fibula flap mandible reconstruction with patient-specific, computer-guided preoperative planning. Head Neck 2015, 37, 1660–1664. [Google Scholar] [CrossRef]
- Kokosis, G.; Davidson, E.H.; Pedreira, R.; Macmillan, A.; Dorafshar, A.H. The Use of Computer-Aided Design and Manufacturing in Acute Mandibular Trauma Reconstruction. J. Oral Maxillofac. Surg. 2018, 76, 1036–1043. [Google Scholar] [CrossRef]
- Diment, L.E.; Thompson, M.S.; Bergmann, J.H.M. Clinical efficacy and effectiveness of 3D printing: A systematic review. BMJ Open 2017, 7, e016891. [Google Scholar] [CrossRef] [Green Version]
- King, B.J.; Park, E.P.; Christensen, B.J.; Danrad, R. On-Site 3-Dimensional Printing and Preoperative Adaptation Decrease Operative Time for Mandibular Fracture Repair. J. Oral Maxillofac. Surg. 2018, 76, 1950.e1–1950.e8. [Google Scholar] [CrossRef] [Green Version]
- Costan, V.V.; Nicolau, A.; Sulea, D.; Ciofu, M.L.; Boișteanu, O.; Popescu, E. The Impact of 3D Technology in Optimizing Midface Fracture Treatment—Focus on the Zygomatic Bone. J. Oral Maxillofac. Surg. 2021, 79, 880–891. [Google Scholar] [CrossRef]
- Lassausaie, A.; Sesqué, A.; Barthélémy, I.; Depeyre, A. Virtual Surgery Planning and Three-Dimensional Printing Template for Osteotomy of the Zygoma to Correct Untreated Zygomaticomaxillary Complex Fracture. J. Craniofac. Surg. 2020, 31, 1142–1145. [Google Scholar] [CrossRef]
- Longeac, M.; Depeyre, A.; Pereira, B.; Barthelemy, I.; Pham Dang, N. Virtual surgical planning and three-dimensional printing for the treatment of comminuted zygomaticomaxillary complex fracture. J. Stomatol. Oral Maxillofac. Surg. 2021, 122, 386–390. [Google Scholar] [CrossRef] [PubMed]
- Xue, R.; Lai, Q.; Sun, S.; Lai, L.; Tang, X.; Ci, J.; Zhang, Z.; Wang, Y. Application of three-dimensional printing technology for improved orbital-maxillary-zygomatic reconstruction. J. Craniofac. Surg. 2019, 30, E127–E131. [Google Scholar] [CrossRef] [PubMed]
- Fan, B.; Chen, H.; Sun, Y.J.; Wang, B.F.; Che, L.; Liu, S.Y.; Li, G.Y. Clinical effects of 3-D printing-assisted personalized reconstructive surgery for blowout orbital fractures. Graefe’s Arch. Clin. Exp. Ophthalmol. 2017, 255, 2051–2057. [Google Scholar] [CrossRef] [PubMed]
- Weadock, W.J.; Heisel, C.J.; Kahana, A.; Kim, J. Use of 3D Printed Models to Create Molds for Shaping Implants for Surgical Repair of Orbital Fractures. Acad. Radiol. 2020, 27, 536–542. [Google Scholar] [CrossRef]
- Vehmeijer, M.; van Eijnatten, M.; Liberton, N.; Wolff, J. A Novel Method of Orbital Floor Reconstruction Using Virtual Planning, 3-Dimensional Printing, and Autologous Bone. J. Oral Maxillofac. Surg. 2016, 74, 1608–1612. [Google Scholar] [CrossRef]
- Sigron, G.R.; Rüedi, N.; Chammartin, F.; Meyer, S.; Msallem, B.; Kunz, C.; Thieringer, F.M. Three-dimensional analysis of isolated orbital floor fractures pre-and post-reconstruction with standard titanium meshes and “hybrid” patient-specific implants. J. Clin. Med. 2020, 9, 1579. [Google Scholar] [CrossRef]
- Palka, L.; Konstantinovic, V.; Pruszynski, P.; Jamroziak, K. Analysis using the finite element method of a novel modular system of additively manufactured osteofixation plates for mandibular fractures—A preclinical study. Biomed. Signal Process. Control 2021, 65, 102342. [Google Scholar] [CrossRef]
- Pavlychuk, T.; Chernogorskyi, D.; Chepurnyi, Y.; Neff, A.; Kopchak, A. Application of CAD/CAM technology for surgical treatment of condylar head fractures: A preliminary study. J. Oral Biol. Craniofac. Res. 2020, 10, 608–614. [Google Scholar] [CrossRef]
- King, C.; Shafi, A.; Burke, E. Optimising the management of concurrent symphyseal/parasymphyseal and bilateral extracapsular condylar fractures using three-dimensional printing. Oral Maxillofac. Surg. 2020, 24, 217–219. [Google Scholar] [CrossRef]
- Zhang, W.B.; Yu, Y.; Mao, C.; Wang, Y.; Guo CBin Yu, G.Y.; Peng, X. Outcomes of Zygomatic Complex Reconstruction with Patient-Specific Titanium Mesh Using Computer-Assisted Techniques. J. Oral Maxillofac. Surg. 2019, 77, 1915–1927. [Google Scholar] [CrossRef]
- Manmadhachary, A.; Aditya Mohan, A.; Haranadha Reddy, M. Manufacturing of customized implants for orbital fractures using 3D printing. Bioprinting 2021, 21, e00118. [Google Scholar]
- Uechi, J.; Okayama, M.; Shibata, T.; Muguruma, T.; Hayashi, K.; Endo, K.; Mizoguchi, I. A novel method for the 3-dimensional simulation of orthognathic surgery by using a multimodal image-fusion technique. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 786–798. [Google Scholar] [CrossRef] [PubMed]
- Nkenke, E.; Zachow, S.; Benz, M.; Maier, T.; Veit, K.; Kramer, M.; Benz, S.; Häusler, G.; Neukam, F.W.; Lell, M. Fusion of computed tomography data and optical 3D images of the dentition for streak artefact correction in the simulation of orthognathic surgery. Dentomaxillofac. Radiol. 2004, 33, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Santler, G. The Graz hemisphere splint: A new precise, non-invasive method of replacing the dental arch of 3D-models by plaster models. J. Cranio-Maxillofac. Surg. 1998, 26, 169–173. [Google Scholar] [CrossRef]
- Swennen GR, J.; Mommaerts, M.Y.; Abeloos, J.; De Clercq, C.; Lamoral, P.; Neyt, N.; Casselman, J.; Schutyser, F. A cone-beam CT based technique to augment the 3D virtual skull model with a detailed dental surface. Int. J. Oral Maxillofac. Surg. 2009, 38, 48–57. [Google Scholar] [CrossRef]
- Swennen GR, J.; Mollemans, W.; De Clercq, C.; Abeloos, J.; Lamoral, P.; Lippens, F.; Neyt, N.; Casselman, J.; Schutyser, F. A cone-beam computed tomography triple scan procedure to obtain a three-dimensional augmented virtual skull model appropriate for orthognathic surgery planning. J. Craniofac. Surg. 2009, 20, 297–307. [Google Scholar] [CrossRef]
- Kim, B.C.; Lee, C.E.; Park, W.; Kang, S.H.; Zhengguo, P.; Yi, C.K.; Lee, S.H. Integration accuracy of digital dental models and 3-dimensional computerized tomography images by sequential point- and surface-based markerless registration. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2010, 110, 370–378. [Google Scholar] [CrossRef]
- Noh, H.; Nabha, W.; Cho, J.H.; Hwang, H.S. Registration accuracy in the integration of laser-scanned dental images into maxillofacial cone-beam computed tomography images. Am. J. Orthod. Dentofac. Orthop. 2011, 140, 585–591. [Google Scholar] [CrossRef]
- Nilsson, J.; Richards, R.G.; Thor, A.; Kamer, L. Virtual bite registration using intraoral digital scanning, CT and CBCT: In vitro evaluation of a new method and its implication for orthognathic surgery. J. Cranio-Maxillofac. Surg. 2016, 44, 1194–1200. [Google Scholar] [CrossRef]
- De Waard, O.; Baan, F.; Verhamme, L.; Breuning, H.; Kuijpers-Jagtman, A.M.; Maal, T. A novel method for fusion of intra-oral scans and cone-beam computed tomography scans for orthognathic surgery planning. J. Cranio-Maxillofac. Surg. 2016, 44, 160–166. [Google Scholar] [CrossRef]
- Ho, C.T.; Lin, H.H.; Lo, L.J. Intraoral Scanning and Setting up the Digital Final Occlusion in Three-Dimensional Planning of Orthognathic Surgery: Its Comparison with the Dental Model Approach. Plast. Reconstr. Surg. 2019, 143, 1027e–1036e. [Google Scholar] [CrossRef] [PubMed]
- Zinser, M.J.; Sailer, H.F.; Ritter, L.; Braumann, B.; Maegele, M.; Zöller, J.E. A paradigm shift in orthognathic surgery? A comparison of navigation, computer-aided designed/computer-aided manufactured splints, and ‘classic’ intermaxillary splints to surgical transfer of virtual orthognathic planning. J. Oral Maxillofac. Surg. 2013, 71, 2151.e1–2151.e21. [Google Scholar] [CrossRef] [PubMed]
- Kraeima, J.; Jansma, J.; Schepers, R.H. Splintless surgery: Does patient-specific CAD-CAM osteosynthesis improve accuracy of Le Fort I osteotomy? Br. J. Oral Maxillofac. Surg. 2016, 54, 1085–1089. [Google Scholar] [CrossRef] [PubMed]
- Mascarenhas, W.; Makhoul, N. Efficient in-house 3D printing of an orthognathic splint for single-jaw cases. Int. J. Oral Maxillofac. Surg. 2021, 50, 1075–1077. [Google Scholar] [CrossRef]
- Zhang, N.; Liu, S.; Hu, Z.; Hu, J.; Zhu, S.; Li, Y. Accuracy of virtual surgical planning in two-jaw orthognathic surgery: Comparison of planned and actual results. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 122, 143–151. [Google Scholar] [CrossRef]
- Suojanen, J.; Leikola, J.; Stoor, P. The use of patient-specific implants in orthognathic surgery: A series of 32 maxillary osteotomy patients. J. Cranio-Maxillofac. Surg. 2016, 44, 1913–1916. [Google Scholar] [CrossRef] [Green Version]
- Suojanen, J.; Leikola, J.; Stoor, P. The use of patient-specific implants in orthognathic surgery: A series of 30 mandible sagittal split osteotomy patients. J. Cranio-Maxillofac. Surg. 2017, 45, 990–994. [Google Scholar] [CrossRef] [Green Version]
- Gander, T.; Bredell, M.; Eliades, T.; Rücker, M.; Essig, H. Splintless orthognathic surgery: A novel technique using patient-specific implants (PSI). J. Cranio-Maxillofac. Surg. 2015, 43, 319–322. [Google Scholar] [CrossRef]
- Rückschloß, T.; Ristow, O.; Müller, M.; Kühle, R.; Zingler, S.; Engel, M.; Hoffmann, J.; Freudlsperger, C. Accuracy of patient-specific implants and additive-manufactured surgical splints in orthognathic surgery—A three-dimensional retrospective study. J. Cranio-Maxillofac. Surg. 2019, 47, 847–853. [Google Scholar] [CrossRef]
- Heufelder, M.; Wilde, F.; Pietzka, S.; Mascha, F.; Winter, K.; Schramm, A.; Rana, M. Clinical accuracy of waferless maxillary positioning using customized surgical guides and patient specific osteosynthesis in bimaxillary orthognathic surgery. J. Cranio-Maxillofac. Surg. 2017, 45, 1578–1585. [Google Scholar] [CrossRef]
- Leiggener, C.S.; Krol, Z.; Gawelin, P.; Buitrago-Téllez, C.H.; Zeilhofer, H.F.; Hirsch, J.M. A computer-based comparative quantitative analysis of surgical outcome of mandibular reconstructions with free fibula microvascular flaps. J. Plast. Surg. Hand Surg. 2015, 49, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Okuyama, K.; Michi, Y.; Mizutani, M.; Yamashiro, M.; Kaida, A.; Harada, K. Clinical study on mandibular fracture after marginal resection of the mandible. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 121, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Melville, J.C.; Manis, C.S.; Shum, J.W.; Alsuwied, D. Single-Unit 3D-Printed Titanium Reconstruction Plate for Maxillary Reconstruction: The Evolution of Surgical Reconstruction for Maxillary Defects—A Case Report and Review of Current Techniques. J. Oral Maxillofac. Surg. 2019, 77, 874.e1–874.e13. [Google Scholar] [CrossRef] [PubMed]
- Weitz, J.; Wolff, K.D.; Kesting, M.R.; Nobis, C.P. Development of a novel resection and cutting guide for mandibular reconstruction using free fibula flap. J. Cranio-Maxillofac. Surg. 2018, 46, 1975–1978. [Google Scholar] [CrossRef]
- Azuma, M.; Yanagawa, T.; Ishibashi–Kanno, N.; Uchida, F.; Ito, T.; Yamagata, K.; Hasegawa, S.; Sasaki, K.; Adachi, K.; Tabuchi, K.; et al. Mandibular reconstruction using plates prebent to fit rapid prototyping 3-dimensional printing models ameliorates contour deformity. Head Face Med. 2014, 10, 45. [Google Scholar] [CrossRef] [Green Version]
- Bell, R.B.; Weimer, K.A.; Dierks, E.J.; Buehler, M.; Lubek, J.E. Computer planning and intraoperative navigation for palatomaxillary and mandibular reconstruction with fibular free flaps. J. Oral Maxillofac. Surg. 2011, 69, 724–732. [Google Scholar] [CrossRef]
- Bao, T.; He, J.; Yu, C.; Zhao, W.; Lin, Y.; Wang, H.; Liu, J.; Zhu, H. Utilization of a pre-bent plate-positioning surgical guide system in precise mandibular reconstruction with a free fibula flap. Oral Oncol. 2017, 75, 133–139. [Google Scholar] [CrossRef]
- Shan, X.F.; Chen, H.M.; Liang, J.; Huang, J.W.; Cai, Z.G. Surgical Reconstruction of Maxillary and Mandibular Defects Using a Printed Titanium Mesh. J. Oral Maxillofac. Surg. 2015, 73, 1437.e1–1437.e9. [Google Scholar] [CrossRef]
- Hasegawa, T.; Ushirozako, H.; Shigeto, E.; Ohba, T.; Oba, H.; Mukaiyama, K.; Shimizu, S.; Yamato, Y.; Ide, K.; Shibata, Y.; et al. The Titanium-coated PEEK Cage Maintains Better Bone Fusion with the Endplate Than the PEEK Cage 6 Months after PLIF Surgery: A Multicenter, Prospective, Randomized Study. Spine 2020, 45, E892–E902. [Google Scholar] [CrossRef]
- Järvinen, S.; Suojanen, J.; Kormi, E.; Wilkman, T.; Kiukkonen, A.; Leikola, J.; Stoor, P. The use of patient specific polyetheretherketone implants for reconstruction of maxillofacial deformities. J. Cranio-Maxillofac. Surg. 2019, 47, 1072–1076. [Google Scholar] [CrossRef] [Green Version]
- Atef, M.; Mounir, M.; Shawky, M.; Mounir, S.; Gibaly, A. Polyetheretherketone patient-specific implants (PPSI) for the reconstruction of two different mandibular contour deformities. Oral Maxillofac. Surg. 2021. [Google Scholar] [CrossRef] [PubMed]
- Mehle, K.; Eckert, A.; Gentzsch, D.; Schwan, S.; Ludtka, C.; Knoll, W. Evaluation of a New PEEK Mandibular Reconstruction Plate Design for Continuity Defect Therapy by Finite Element Analysis. Int. J. New Technol. Res. 2016, 2, 65–71. Available online: www.ijntr.org (accessed on 27 February 2022).
- De Meurechy, N.; Braem, A.; Mommaerts, M.Y. Biomaterials in temporomandibular joint replacement: Current status and future perspectives—A narrative review. Int. J. Oral Maxillofac. Surg. 2018, 47, 518–533. [Google Scholar] [CrossRef] [PubMed]
- De Meurechy, N.K.G.; Zaror, C.E.; Mommaerts, M.Y. Total Temporomandibular Joint Replacement: Stick to Stock or Optimization by Customization? Craniomaxillofac. Trauma Reconstr. 2020, 13, 59–70. [Google Scholar] [CrossRef] [PubMed]
- Wolford, L.M.; Pitta, M.C.; Reiche-Fischel, O.; Franco, P.F. TMJ concepts/techmedia custom-made TMJ total joint prosthesis: 5-year follow-up study. Int. J. Oral Maxillofac. Surg. 2003, 32, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Mercuri, L.G. Alloplastic temporomandibular joint replacement: Rationale for the use of custom devices. Int. J. Oral Maxillofac. Surg. 2012, 41, 1033–1040. [Google Scholar] [CrossRef]
- Dimitroulis, G.; Austin, S.; Sin Lee, P.V.; Ackland, D. A new three-dimensional, print-on-demand temporomandibular prosthetic total joint replacement system: Preliminary outcomes. J. Cranio-Maxillofac. Surg. 2018, 46, 1192–1198. [Google Scholar] [CrossRef]
- Johnson, N.R.; Roberts, M.J.; Doi, S.A.; Batstone, M.D. Total temporomandibular joint replacement prostheses: A systematic review and bias-adjusted meta-analysis. Int. J. Oral Maxillofac. Surg. 2017, 46, 86–92. [Google Scholar] [CrossRef]
- De Meurechy, N.; Mommaerts, M.Y. Alloplastic temporomandibular joint replacement systems: A systematic review of their history. Int. J. Oral Maxillofac. Surg. 2018, 47, 743–754. [Google Scholar] [CrossRef]
- Wolford, L.M.; Mercuri, L.G.; Schneiderman, E.D.; Movahed, R.; Allen, W. Twenty-year follow-up study on a patient-fitted temporomandibular joint prosthesis: The Techmedica/TMJ Concepts device. J. Oral Maxillofac. Surg. 2015, 73, 952–960. [Google Scholar] [CrossRef]
- Haq, J.; Patel, N.; Weimer, K.; Matthews, N.S. Single stage treatment of ankylosis of the temporomandibular joint using patient-specific total joint replacement and virtual surgical planning. Br. J. Oral Maxillofac. Surg. 2014, 52, 350–355. [Google Scholar] [CrossRef] [PubMed]
- Abel, E.W.; Hilgers, A.; McLoughlin, P.M. Finite element analysis of a condylar support prosthesis to replace the temporomandibular joint. Br. J. Oral Maxillofac. Surg. 2015, 53, 352–357. [Google Scholar] [CrossRef] [PubMed]
- Alakailly, X.; Schwartz, D.; Alwanni, N.; Demko, C.; Altay, M.; Kilinc, Y.; Baur, D.; Quereshy, F. Patient-centered quality of life measures after alloplastic temporomandibular joint replacement surgery. Int. J. Oral Maxillofac. Surg. 2016, 46, 204–207. [Google Scholar] [CrossRef] [PubMed]
- Gruber, E.; McCullough, J.; Sidebottom, A. Medium-term outcomes and complications after total replacement of the temporomandibular joint. Prospective outcome analysis after 3 and 5 years. Br. J. Oral Maxillofac. Surg. 2015, 53, 412–415. [Google Scholar] [CrossRef] [PubMed]
- Ellis, E. Complications of mandibular condyle fractures. Int. J. Oral Maxillofac. Surg. 1998, 27, 255–257. [Google Scholar] [CrossRef]
- Druelle, C.; Touzet-Roumazeille, S.; Raoul, G.; Ferri, J.; Nicot, R. How to produce pre-shaped rigid arch bars using low-cost 3D printing technology—A technical note. J. Stomatol. Oral Maxillofac. Surg. 2017, 118, 213–216. [Google Scholar] [CrossRef]
- Pang, S.S.Y.; Fang, C.; Chan, J.Y.W. Application of three-dimensional printing technology in orbital floor fracture reconstruction. Trauma Case Rep. 2018, 17, 23–28. [Google Scholar] [CrossRef]
- Hanafy, M.; Akoush, Y.; Abou-ElFetouh, A.; Mounir, R.M. Precision of orthognathic digital plan transfer using patient-specific cutting guides and osteosynthesis versus mixed analogue–digitally planned surgery: A randomized controlled clinical trial. Int. J. Oral Maxillofac. Surg. 2020, 49, 62–68. [Google Scholar] [CrossRef]
- Jain, S.; Choudhary, K.; Nagi, R.; Shukla, S.; Kaur, N.; Grover, D. New evolution of cone-beam computed tomography in dentistry: Combining digital echnologies. Imaging Sci. Dent. 2019, 49, 179–190. [Google Scholar] [CrossRef]
- Lin, H.H.; Lo, L.J. Three-dimensional computer-assisted surgical simulation and intraoperative navigation in orthognathic surgery: A literature review. J. Formos. Med. Assoc. 2015, 114, 300–307. [Google Scholar] [CrossRef] [Green Version]
- Adolphs, N.; Haberl, E.J.; Liu, W.; Keeve, E.; Menneking, H.; Hoffmeister, B. Virtual planning for craniomaxillofacial surgery—7 Years of experience. J. Cranio-Maxillofac. Surg. 2014, 42, e289–e295. [Google Scholar] [CrossRef] [PubMed]
- Zinser, M.J.; Mischkowski, R.A.; Dreiseidler, T.; Thamm, O.C.; Rothamel, D.; Zöller, J.E. Computer-assisted orthognathic surgery: Waferless maxillary positioning, versatility, and accuracy of an image-guided visualisation display. Br. J. Oral Maxillofac. Surg. 2013, 51, 827–833. [Google Scholar] [CrossRef] [PubMed]
- Alkhayer, A.; Piffkó, J.; Lippold, C.; Segatto, E. Accuracy of virtual planning in orthognathic surgery: A systematic review. Head Face Med. 2020, 16, 34. [Google Scholar] [CrossRef] [PubMed]
- Zavattero, E.; Romano, M.; Gerbino, G.; Rossi, D.S.; Giannì, A.B.; Ramieri, G.; Baj, A. Evaluation of the accuracy of virtual planning in orthognathic surgery: A morphometric study. J. Craniofac. Surg. 2019, 30, 1214–1220. [Google Scholar] [CrossRef]
- Haas, O.L.; Becker, O.E.; De Oliveira, R.B. Computer-aided planning in orthognathic surgery—Systematic review. Int. J. Oral Maxillofac. Surg. 2015, 44, 329–342. [Google Scholar] [CrossRef]
- Hsu, S.S.P.; Gateno, J.; Bell, R.B.; Hirsch, D.L.; Markiewicz, M.R.; Teichgraeber, J.F.; Zhou, X.; Xia, J.J. Accuracy of a computer-aided surgical simulation protocol for orthognathic surgery: A prospective multicenter study. J. Oral Maxillofac. Surg. 2013, 71, 128–142. [Google Scholar] [CrossRef] [Green Version]
- O’Malley, A.M.; Milosevic, A. Comparison of three facebow/semi-adjustable articulator systems for planning orthognathic surgery. Br. J. Oral Maxillofac. Surg. 2000, 38, 185–190. [Google Scholar] [CrossRef] [Green Version]
- Marko, J.V. Simple hinge and semiadjustable articulators in orthognathic surgery. Am. J. Orthod. Dentofac. Orthop. 1986, 90, 37–44. [Google Scholar] [CrossRef]
- Thurzo, A.; Urbanová, W.; Novák, B.; Waczulíková, I.; Varga, I. Utilization of a 3D Printed Orthodontic Distalizer for Tooth-Borne Hybrid Treatment in Class II Unilateral Malocclusions. Materials 2022, 15, 1740. [Google Scholar] [CrossRef]
- Thurzo, A.; Kočiš, F.; Novák, B.; Czako, L.; Varga, I. Three-Dimensional Modeling and 3D Printing of Biocompatible Orthodontic Power-Arm Design with Clinical Application. Appl. Sci. 2021, 11, 9693. [Google Scholar] [CrossRef]
- Sun, Y.; Tian, L.; Luebbers, H.T.; Politis, C. Relapse tendency after BSSO surgery differs between 2D and 3D measurements: A validation study. J. Cranio-Maxillofac. Surg. 2018, 46, 1893–1898. [Google Scholar] [CrossRef] [PubMed]
- Bengtsson, M.; Wall, G.; Greiff, L.; Rasmusson, L. Treatment outcome in orthognathic surgery—A prospective randomized blinded case-controlled comparison of planning accuracy in computer-assisted two- and three-dimensional planning techniques (part II). J. Cranio-Maxillofac. Surg. 2017, 45, 1419–1424. [Google Scholar] [CrossRef] [PubMed]
- Shaheen, E.; Shujaat, S.; Saeed, T.; Jacobs, R.; Politis, C. Three-dimensional planning accuracy and follow-up protocol in orthognathic surgery: A validation study. Int. J. Oral Maxillofac. Surg. 2019, 48, 71–76. [Google Scholar] [CrossRef] [Green Version]
- Parkin, D.M.; Bray, F.; Ferlay, J.; Pisani, P. Global Cancer Statistics, 2002. CA. Cancer J. Clin. 2005, 55, 74–108. [Google Scholar] [CrossRef] [PubMed]
- Da Silva Moro, J.; Maroneze, M.C.; Ardenghi, T.M.; Barin, L.M.; Danesi, C.C. Oral and oropharyngeal cancer: Epidemiology and survival analysis. Einstein 2018, 16, eAO4248. [Google Scholar]
- Tarsitano, A.; Ricotta, F.; Baldino, G.; Badiali, G.; Pizzigallo, A.; Ramieri, V.; Cascone, P.; Marchetti, C. Navigation-guided resection of maxillary tumours: The accuracy of computer-assisted surgery in terms of control of resection margins—A feasibility study. J. Cranio-Maxillofac. Surg. 2017, 45, 2109–2114. [Google Scholar] [CrossRef]
- Ricotta, F.; Cercenelli, L.; Battaglia, S.; Bortolani, B.; Savastio, G.; Marcelli, E.; Marchetti, C.; Tarsitano, A. Navigation-guided resection of maxillary tumors: Can a new volumetric virtual planning method improve outcomes in terms of control of resection margins? J. Cranio-Maxillofac. Surg. 2018, 46, 2240–2247. [Google Scholar] [CrossRef]
- Szewczyk, M.; Golusinski, W.; Pazdrowski, J.; Masternak, M.; Sharma, N.; Golusinski, P. Positive fresh frozen section margins as an adverse independent prognostic factor for local recurrence in oral cancer patients. Laryngoscope 2018, 128, 1093–1098. [Google Scholar] [CrossRef]
- Van Baar, G.J.C.; Forouzanfar, T.; Liberton, N.P.T.J.; Winters, H.A.H.; Leusink, F.K.J. Accuracy of computer-assisted surgery in mandibular reconstruction: A systematic review. Oral Oncol. 2018, 84, 52–60. [Google Scholar] [CrossRef]
- Kovoor, C.C.; Jayakumar, R.; George, V.V.; Padmanabhan, V.; Guild, A.J.; Viswanath, S. Vascularized fibular graft in infected tibial bone loss. Indian J. Orthop. 2011, 45, 330–335. [Google Scholar] [CrossRef]
- Steffen, C.; Sellenschloh, K.; Vollmer, M.; Morlock, M.M.; Heiland, M.; Huber, G.; Rendenbach, C. Biomechanical comparison of titanium miniplates versus a variety of CAD/CAM plates in mandibular reconstruction. J. Mech. Behav. Biomed. Mater. 2020, 111, 104007. [Google Scholar] [CrossRef] [PubMed]
- Maixner, W. Temporomandibular joint disorders. Funct. Pain Syndr. Present. Pathophysiol. 2015, 7, 1. [Google Scholar]
- McNeill, C.; Mohl, N.D.; Rugh, J.D.; Tanaka, T.T. Temporomandibular disorders: Diagnosis, management, education, and research. J. Am. Dent. Assoc. 1990, 120, 253. [Google Scholar] [CrossRef] [PubMed]
- Dimitroulis, G. Management of temporomandibular joint disorders: A surgeon’s perspective. Aust. Dent. J. 2018, 63, S79–S90. [Google Scholar] [CrossRef]
- Zou, L.; He, D.; Ellis, E. A Comparison of Clinical Follow-Up of Different Total Temporomandibular Joint Replacement Prostheses: A Systematic Review and Meta-Analysis. J. Oral Maxillofac. Surg. 2018, 76, 294–303. [Google Scholar] [CrossRef]
- Kumar, S.; Khanna, V.; Singh, B.P.; Mehrotra, D.; Patil, R.K. Impact of technology in temporomandibular joint reconstruction surgeries: A systematic review. J. Plast. Reconstr. Aesthetic Surg. 2021, 74, 1331–1345. [Google Scholar] [CrossRef]
- Kaplan, P.A.; Ruskin, J.D.; Tu, H.K.; Knibbe, M.A. Erosive arthritis of the temporomandibular joint caused by Teflon-Proplast implants: Plain film features. Am. J. Roentgenol. 1988, 151, 337–339. [Google Scholar] [CrossRef]
- Kameros, J.; Himmelfarb, R. Treatment of temporomandibular joint ankylosis with methyl methacrylate interpositional arthroplasty: Report of four cases. J. Oral Surg. 1975, 33, 282–286. [Google Scholar]
- Westermark, A.; Koppel, D.; Leiggener, C. Condylar replacement alone is not sufficient for prosthetic reconstruction of the temporomandibular joint. Int. J. Oral Maxillofac. Surg. 2006, 35, 488–492. [Google Scholar] [CrossRef]
- Elledge, R.; Mercuri, L.G.; Attard, A.; Green, J.; Speculand, B. Review of emerging temporomandibular joint total joint replacement systems. Br. J. Oral Maxillofac. Surg. 2019, 57, 722–728. [Google Scholar] [CrossRef]
- Guarda-Nardini, L.; Manfredini, D.; Ferronato, G. Temporomandibular joint total replacement prosthesis: Current knowledge and considerations for the future. Int. J. Oral Maxillofac. Surg. 2008, 37, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Mehrotra, D.; Kumar, S.; Mehrotra, P.; Khanna, R.; Khanna, V.; Eggbeer, D.; Evans, P. Patient specific total temporomandibular joint reconstruction: A review of biomaterial, designs, fabrication and outcomes. J. Oral Biol. Craniofac. Res. 2021, 11, 334–343. [Google Scholar] [CrossRef] [PubMed]
- Giannakopoulos, H.E.; Sinn, D.P.; Quinn, P.D. Biomet microfixation temporomandibular joint replacement system: A 3-year follow-up study of patients treated during 1995 to 2005. J. Oral Maxillofac. Surg. 2012, 70, 787–794. [Google Scholar] [CrossRef] [PubMed]
- Lungu, A.J.; Swinkels, W.; Claesen, L.; Tu, P.; Egger, J.; Chen, X. A review on the applications of virtual reality, augmented reality and mixed reality in surgical simulation: An extension to different kinds of surgery. Expert Rev. Med Devices 2021, 18, 47–62. [Google Scholar] [CrossRef] [PubMed]
- Bartella, A.K.; Kamal, M.; Scholl, I.; Schiffer, S.; Steegmann, J.; Ketelsen, D.; Hölzle, F.; Lethaus, B. Virtual reality in preoperative imaging in maxillofacial surgery: Implementation of “the next level”? Br. J. Oral Maxillofac. Surg. 2019, 57, 644–648. [Google Scholar] [CrossRef]
- Zaragoza-Siqueiros, J.; Medellin-Castillo, H.I.; de la Garza-Camargo, H.; Lim, T.; Ritchie, J.M. An integrated haptic-enabled virtual reality system for orthognathic surgery planning. Comput. Methods Biomech. Biomed. Eng. 2019, 22, 499–517. [Google Scholar] [CrossRef]
- Kim, H.-J.; Jo, Y.-J.; Choi, J.-S.; Kim, H.-J.; Park, I.-S.; You, J.-S.; Oh, J.-S.; Moon, S.-Y. Virtual Reality Simulation and Augmented Reality-Guided Surgery for Total Maxillectomy: A Case Report. Appl. Sci. 2020, 10, 6288. [Google Scholar] [CrossRef]
- Chang, H.-W.; Lin, H.-H.; Chortrakarnkij, P.; Kim, S.G.; Lo, L.-J. Intraoperative navigation for single-splint two-jaw orthognathic surgery: From model to actual surgery. J. Cranio-Maxillofac. Surg. 2015, 43, 1119–1126. [Google Scholar] [CrossRef]
- De Paolis, L.T.; De Luca, V. Augmented visualization with depth perception cues to improve the surgeon’s performance in minimally invasive surgery. Med Biol. Eng. Comput. 2018, 57, 995–1013. [Google Scholar] [CrossRef]
- Meola, A.; Cutolo, F.; Carbone, M.; Cagnazzo, F.; Ferrari, M.; Ferrari, V. Augmented reality in neurosurgery: A systematic review. Neurosurg. Rev. 2016, 40, 537–548. [Google Scholar] [CrossRef]
- Mischkowski, R.A.; Zinser, M.J.; Kübler, A.C.; Krug, B.; Seifert, U.; Zöller, J.E. Application of an augmented reality tool for maxillary positioning in orthognathic surgery—A feasibility study. J. Cranio-Maxillofac. Surg. 2006, 34, 478–483. [Google Scholar] [CrossRef] [PubMed]
- Fushima, K.; Kobayashi, M. Mixed-reality simulation for orthognathic surgery. Maxillofac. Plast. Reconstr. Surg. 2016, 38, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woo, T.; Kraeima, J.; Kim, Y.O.; Kim, Y.S.; Roh, T.S.; Lew, D.H.; Yun, I.S. Mandible Reconstruction with 3D Virtual Planning. J. Int. Soc. Simul. Surg. 2015, 2, 90–93. [Google Scholar] [CrossRef] [Green Version]
- Olsson, P.; Nysjö, F.; Hirsch, J.-M.; Carlbom, I.B. A haptics-assisted cranio-maxillofacial surgery planning system for restoring skeletal anatomy in complex trauma cases. Int. J. Comput. Assist. Radiol. Surg. 2013, 8, 887–894. [Google Scholar] [CrossRef]
- Qu, M.; Hou, Y.; Xu, Y.; Shen, C.; Zhu, M.; Xie, L.; Wang, H.; Zhang, Y.; Chai, G. Precise positioning of an intraoral distractor using augmented reality in patients with hemifacial microsomia. J. Cranio-Maxillofac. Surg. 2015, 43, 106–112. [Google Scholar] [CrossRef]
- Gao, Y.; Liu, K.; Lin, L.; Wang, X.; Xie, L. The Use of Augmented Reality Navigation to Optimize the Surgical Management of Craniofacial Fibrous Dysplasia. Br. J. Oral Maxillofac. Surg. 2021. [Google Scholar] [CrossRef]
- Roncari, A.; Bianchi, A.; Taddei, F.; Marchetti, C.; Schileo, E.; Badiali, G. Navigation in Orthognathic Surgery: 3D Accuracy. Facial Plast. Surg. 2015, 31, 463–473. [Google Scholar] [CrossRef]
- Cercenelli, L.; Carbone, M.; Condino, S.; Cutolo, F.; Marcelli, E.; Tarsitano, A.; Marchetti, C.; Ferrari, V.; Badiali, G. The Wearable VOSTARS System for Augmented Reality-Guided Surgery: Preclinical Phantom Evaluation for High-Precision Maxillofacial Tasks. J. Clin. Med. 2020, 9, 3562. [Google Scholar] [CrossRef]
- Wu, H.-K.; Lee, S.W.-Y.; Chang, H.-Y.; Liang, J.-C. Current status, opportunities and challenges of augmented reality in education. Comput. Educ. 2013, 62, 41–49. [Google Scholar] [CrossRef]
- Küçük, S.; Kapakin, S.; Göktaş, Y. Learning anatomy via mobile augmented reality: Effects on achievement and cognitive load. Anat. Sci. Educ. 2016, 9, 411–421. [Google Scholar] [CrossRef]
- Langer, R.; Vacanti, J.P. Tissue engineering. Science 1993, 260, 920–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levenberg, S.; Langer, R. Advances in Tissue Engineering. Curr. Top. Dev. Biol. 2004, 61, 113–134. [Google Scholar] [PubMed]
- Dvir, T.; Timko, B.P.; Kohane, D.S.; Langer, R. Nanotechnological strategies for engineering complex tissues. Nat. Nanotechnol. 2011, 6, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Gimble, J.; Guilak, F. Adipose-derived adult stem cells: Isolation, characterization, and differentiation potential. Cytotherapy 2003, 5, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Caplan, A.I. Mesenchymal stem cells: Cell-based reconstructive therapy in orthopedics. Tissue Eng. 2005, 11, 1198–1211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Legemate, K.; Tarafder, S.; Jun, Y.; Lee, C. Engineering Human TMJ Discs with Protein-Releasing 3D-Printed Scaffolds. J. Dent. Res. 2016, 95, 800–807. [Google Scholar] [CrossRef]
- Donahue, R.P.; Hu, J.C.; Athanasiou, K.A. Remaining Hurdles for Tissue-Engineering the Temporomandibular Joint Disc. Trends Mol. Med. 2019, 25, 241–256. [Google Scholar] [CrossRef] [Green Version]
- Bhumiratana, S.; Bernhard, J.C.; Alfi, D.M.; Yeager, K.; Eton, R.E.; Bova, J.; Shah, F.; Gimble, J.M.; Lopez, M.J.; Eisig, S.B.; et al. Tissue-engineered autologous grafts for facial bone reconstruction. Sci. Transl. Med. 2016, 8, 343ra83. [Google Scholar] [CrossRef] [Green Version]
- Chen, D.; Wu, J.Y.; Kennedy, K.M.; Yeager, K.; Bernhard, J.C.; Ng, J.J.; Zimmerman, B.K.; Robinson, S.; Durney, K.M.; Shaeffer, C.; et al. Tissue engineered autologous cartilage-bone grafts for temporomandibular joint regeneration. Sci. Transl. Med. 2020, 12, 6683. [Google Scholar] [CrossRef]
- Kang, H.-W.; Lee, S.J.; Ko, I.K.; Kengla, C.; Yoo, J.J.; Atala, A. A 3D bioprinting system to produce human-scale tissue constructs with structural integrity. Nat. Biotechnol. 2016, 34, 312–319. [Google Scholar] [CrossRef]
- Korn, P.; Ahlfeld, T.; Lahmeyer, F.; Kilian, D.; Sembdner, P.; Stelzer, R.; Pradel, W.; Franke, A.; Rauner, M.; Range, U.; et al. 3D Printing of Bone Grafts for Cleft Alveolar Osteoplasty—In vivo Evaluation in a Preclinical Model. Front. Bioeng. Biotechnol. 2020, 8, 217. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Starly, B.; Daly, A.C.; Burdick, J.A.; Groll, J.; Skeldon, G.; Shu, W.; Sakai, Y.; Shinohara, M.; Nishikawa, M.; et al. The bioprinting roadmap. Biofabrication 2020, 12, 022002. [Google Scholar] [CrossRef] [PubMed]
- Datta, P.; Ozbolat, V.; Ayan, B.; Dhawan, A.; Ozbolat, I.T. Bone tissue bioprinting for craniofacial reconstruction. Biotechnol. Bioeng. 2017, 114, 2424–2431. [Google Scholar] [CrossRef] [PubMed]
- Lawlor, K.T.; Vanslambrouck, J.M.; Higgins, J.W.; Chambon, A.; Bishard, K.; Arndt, D.; Er, P.X.; Wilson, S.B.; Howden, S.E.; Tan, K.S.; et al. Cellular extrusion bioprinting improves kidney organoid reproducibility and conformation. Nat. Mater. 2021, 20, 260–271. [Google Scholar] [CrossRef] [PubMed]
- Szklanny, A.A.; Machour, M.; Redenski, I.; Chochola, V.; Goldfracht, I.; Kaplan, B.; Epshtein, M.; Yameen, H.S.; Merdler, U.; Feinberg, A.; et al. 3D Bioprinting of Engineered Tissue Flaps with Hierarchical Vessel Networks (VesselNet) for Direct Host-To-Implant Perfusion. Adv. Mater. 2021, 33, 2102661. [Google Scholar] [CrossRef]
- Lee, A.; Hudson, A.R.; Shiwarski, D.J.; Tashman, J.W.; Hinton, T.J.; Yerneni, S.; Bliley, J.M.; Campbell, P.G.; Feinberg, A.W. 3D bioprinting of collagen to rebuild components of the human heart. Science 2019, 365, 482–487. [Google Scholar] [CrossRef]
- Romanazzo, S.; Molley, T.G.; Nemec, S.; Lin, K.; Sheikh, R.; Gooding, J.J.; Wan, B.; Li, Q.; Kilian, K.A.; Roohani, I. Synthetic Bone-Like Structures Through Omnidirectional Ceramic Bioprinting in Cell Suspensions. Adv. Funct. Mater. 2021, 31, 2008216. [Google Scholar] [CrossRef]
- Singh, S.; Choudhury, D.; Yu, F.; Mironov, V.; Naing, M.W. In situ bioprinting—Bioprinting from benchside to bedside? Acta Biomater. 2019, 101, 14–25. [Google Scholar] [CrossRef]
- Albanna, M.; Binder, K.W.; Murphy, S.V.; Kim, J.; Qasem, S.A.; Zhao, W.; Tan, J.; El-Amin, I.B.; Dice, D.D.; Marco, J.; et al. In Situ Bioprinting of Autologous Skin Cells Accelerates Wound Healing of Extensive Excisional Full-Thickness Wounds. Sci. Rep. 2019, 9, 1856. [Google Scholar] [CrossRef] [Green Version]
- Amler, A.-K.; Thomas, A.; Tüzüner, S.; Lam, T.; Geiger, M.-A.; Kreuder, A.-E.; Palmer, C.; Nahles, S.; Lauster, R.; Kloke, L. 3D bioprinting of tissue-specific osteoblasts and endothelial cells to model the human jawbone. Sci. Rep. 2021, 11, 4876. [Google Scholar] [CrossRef]
- Korn, P.; Ahlfeld, T.; Pradel, W.; Lode, A.; Franke, A.; Rauner, M.; Range, U.; Stadlinger, B.; Lauer, G.; Gelinsky, M. 3D-bioprinting of bone grafts for alveolar defects—A preclinical pilot study. Int. J. Oral Maxillofac. Surg. 2019, 48, 273. [Google Scholar] [CrossRef]
- Okuyama, K.; Sakamoto, Y.; Naruse, T.; Kawakita, A.; Yanamoto, S.; Furukawa, K.; Umeda, M. Intraoral extraction of an ectopic mandibular third molar detected in the subcondylar region without a pathological cause: A case report and literature review. CRANIO 2016, 35, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Rana, M.; Gellrich, N. Increasing the accuracy of orbital reconstruction with selective laser melted patient-specific implants combined with intraoperative navigation. Br. J. Oral Maxillofac. Surg. 2015, 53, e125. [Google Scholar] [CrossRef]
- Jansen, J.; Schreurs, R.; Dubois, L.; Maal, T.J.; Gooris, P.J.; Becking, A.G. The advantages of advanced computer-assisted diagnostics and three-dimensional preoperative planning on implant position in orbital reconstruction. J. Cranio-Maxillofac. Surg. 2018, 46, 715–721. [Google Scholar] [CrossRef] [PubMed]
- Essig, H.; Dressel, L.; Rana, M.; Rana, M.; Kokemueller, H.; Ruecker, M.; Gellrich, N.-C. Precision of posttraumatic primary orbital reconstruction using individually bent titanium mesh with and without navigation: A retrospective study. Head Face Med. 2013, 9, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, H.H.; Lonic, D.; Lo, L.J. 3D printing in orthognathic surgery—A literature review. J. Formos. Med. Assoc. 2018, 117, 547–558. [Google Scholar] [CrossRef] [PubMed]
- Ettinger, K.S.; Alexander, A.E.; Morris, J.M.; Arce, K. Novel Geometry of an Extended Length Chimeric Scapular Free Flap for Hemimandibular Reconstruction: Nuances of the Technique Streamlined by In-House Virtual Surgical Planning and 3D Printing for a Severely Vessel-Depleted Neck. J. Oral Maxillofac. Surg. 2020, 78, 823–834. [Google Scholar] [CrossRef]
- Ren, W.; Gao, L.; Li, S.; Chen, C.; Li, F.; Wang, Q.; Zhi, Y.; Song, J.; Dou, Z.; Xue, L.; et al. Virtual planning and 3D printing modeling for mandibular reconstruction with fibula free flap. Med. Oral Patol. Oral Cir. Bucal 2018, 23, e359–e366. [Google Scholar] [CrossRef]
- Nawaz, F.; Wall, B.M. Drug Rash With Eosinophilia and Systemic Symptoms (DRESS) Syndrome: Suspected Association With Titanium Bioprosthesis. Am. J. Med Sci. 2007, 334, 215–218. [Google Scholar] [CrossRef]
- United States Food and Drug Administration. Guidance for Industry: #3 General Principles for Evaluating the Human Food Safety of New Animal Drugs Used in Food-Producing Animals Guidance for Industry. 2018. Available online: https://www.regulations.gov/ (accessed on 22 December 2020).
- Makvandi, P.; Corcione, C.E.; Paladini, F.; Gallo, A.L.; Montagna, F.; Jamaledin, R.; Pollini, M.; Maffezzoli, A. Antimicrobial modified hydroxyapatite composite dental bite by stereolithography. Polym. Adv. Technol. 2018, 29, 364–371. [Google Scholar] [CrossRef]
- Corduas, F.; Mathew, E.; McGlynn, R.; Mariotti, D.; Lamprou, D.A.; Mancuso, E. Melt-extrusion 3D printing of resorbable levofloxacin-loaded meshes: Emerging strategy for urogynaecological applications. Mater. Sci. Eng. C 2021, 131, 112523. [Google Scholar] [CrossRef] [PubMed]
- Tappa, K.; Jammalamadaka, U.; Weisman, J.A.; Ballard, D.H.; Wolford, D.D.; Pascual-Garrido, C.; Wolford, L.M.; Woodard, P.K.; Mills, D.K. 3D Printing Custom Bioactive and Absorbable Surgical Screws, Pins, and Bone Plates for Localized Drug Delivery. J. Funct. Biomater. 2019, 10, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palka, L.; Mazurek-Popczyk, J.; Arkusz, K.; Baldy-Chudzik, K. Susceptibility to biofilm formation on 3D-printed titanium fixation plates used in the mandible: A preliminary study. J. Oral Microbiol. 2020, 12, 1838164. [Google Scholar] [CrossRef] [PubMed]
- Bandyopadhyay, A.; Mitra, I.; Shivaram, A.; Dasgupta, N.; Bose, S. Direct comparison of additively manufactured porous titanium and tantalum implants towards in vivo osseointegration. Addit. Manuf. 2019, 28, 259–266. [Google Scholar] [CrossRef]
- Song, P.; Hu, C.; Pei, X.; Sun, J.; Sun, H.; Wu, L.; Jiang, Q.; Fan, H.; Yang, B.; Zhou, C.; et al. Dual modulation of crystallinity and macro-/microstructures of 3D printed porous titanium implants to enhance stability and osseointegration. J. Mater. Chem. B 2019, 7, 2865–2877. [Google Scholar] [CrossRef]
- Pobloth, A.-M.; Checa, S.; Razi, H.; Petersen, A.; Weaver, J.C.; Schmidt-Bleek, K.; Windolf, M.; Tatai, A.Á.; Roth, C.P.; Schaser, K.-D.; et al. Mechanobiologically optimized 3D titanium-mesh scaffolds enhance bone regeneration in critical segmental defects in sheep. Sci. Transl. Med. 2018, 10, eaam8828. [Google Scholar] [CrossRef] [Green Version]
- Lucas, R.; Federico, M.; Edmund, C. (Eds.) Computer-Assisted Musculoskeletal Surgery; Springer: Cham, Switzerland, 2016. [Google Scholar]
- Pierrakakis, K.; Kandias, M.; Gritzali, C.D.; Gritzalis, D. 3D Printing and its Regulation Dynamics: The World in Front of a Paradigm Shift. In Proceedings of the 6th International Conference on Information Law and Ethics, Thessaloniki, Greece, 30–31 May 2014. [Google Scholar]
- Gupta, D.K.; Ali, M.H.; Ali, A.; Jain, P.; Anwer, K.; Iqbal, Z.; Mirza, M.A. 3D printing technology in healthcare: Applications, regulatory understanding, IP repository and clinical trial status. J. Drug Target. 2021, 30, 131–150. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Application | References | |
|---|---|---|
| 3D planning and manufacturing for management of facial trauma | pre-bending of fixation plates on anatomical models | Mandible—[55] Midface—[56,57,58] Orbit—[59,60,61,62,63] |
| production of custom plating based on VSP | Mandible—[53,64,65,66] Midface—[56,67] Orbit—[68] | |
| 3D Planning and Manufacturing in Orthognathic Surgery | Composite models based on fiducial markers | [69,70,71] |
| Composite models based on repeated CBCT scans and data obtained using oral scanners | [72,73,74,75,76,77,78] | |
| VSP-based splints and cutting guides | [79,80,81,82,83,84] | |
| VSP design for Splintless\waferless surgery | [80,85,86,87] | |
| 3D-Based Digitization and Planning for Maxillofacial Tumor Resection and Reconstruction | 3D study models of resection sites | [88,89] |
| Osteotomy guides | [45,90,91] | |
| Pre-bending of Reconstruction plates | [92,93,94] | |
| VSP-based PSIs | [90,95,96,97,98,99] | |
| Total Joint Replacement (TJR) in the Era of 3D Printing | Design of cutting guides for TJR | [100,101,102,103] |
| Custom and VSP-based TJR implants | [100,104,105,106,107,108,109,110,111] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zoabi, A.; Redenski, I.; Oren, D.; Kasem, A.; Zigron, A.; Daoud, S.; Moskovich, L.; Kablan, F.; Srouji, S. 3D Printing and Virtual Surgical Planning in Oral and Maxillofacial Surgery. J. Clin. Med. 2022, 11, 2385. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11092385
Zoabi A, Redenski I, Oren D, Kasem A, Zigron A, Daoud S, Moskovich L, Kablan F, Srouji S. 3D Printing and Virtual Surgical Planning in Oral and Maxillofacial Surgery. Journal of Clinical Medicine. 2022; 11(9):2385. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11092385
Chicago/Turabian StyleZoabi, Adeeb, Idan Redenski, Daniel Oren, Adi Kasem, Asaf Zigron, Shadi Daoud, Liad Moskovich, Fares Kablan, and Samer Srouji. 2022. "3D Printing and Virtual Surgical Planning in Oral and Maxillofacial Surgery" Journal of Clinical Medicine 11, no. 9: 2385. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11092385