
Meibomian Gland Density: An Effective Evaluation Index of Meibomian Gland Dysfunction Based on Deep Learning and Transfer Learning

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Materials
2.2. Methods
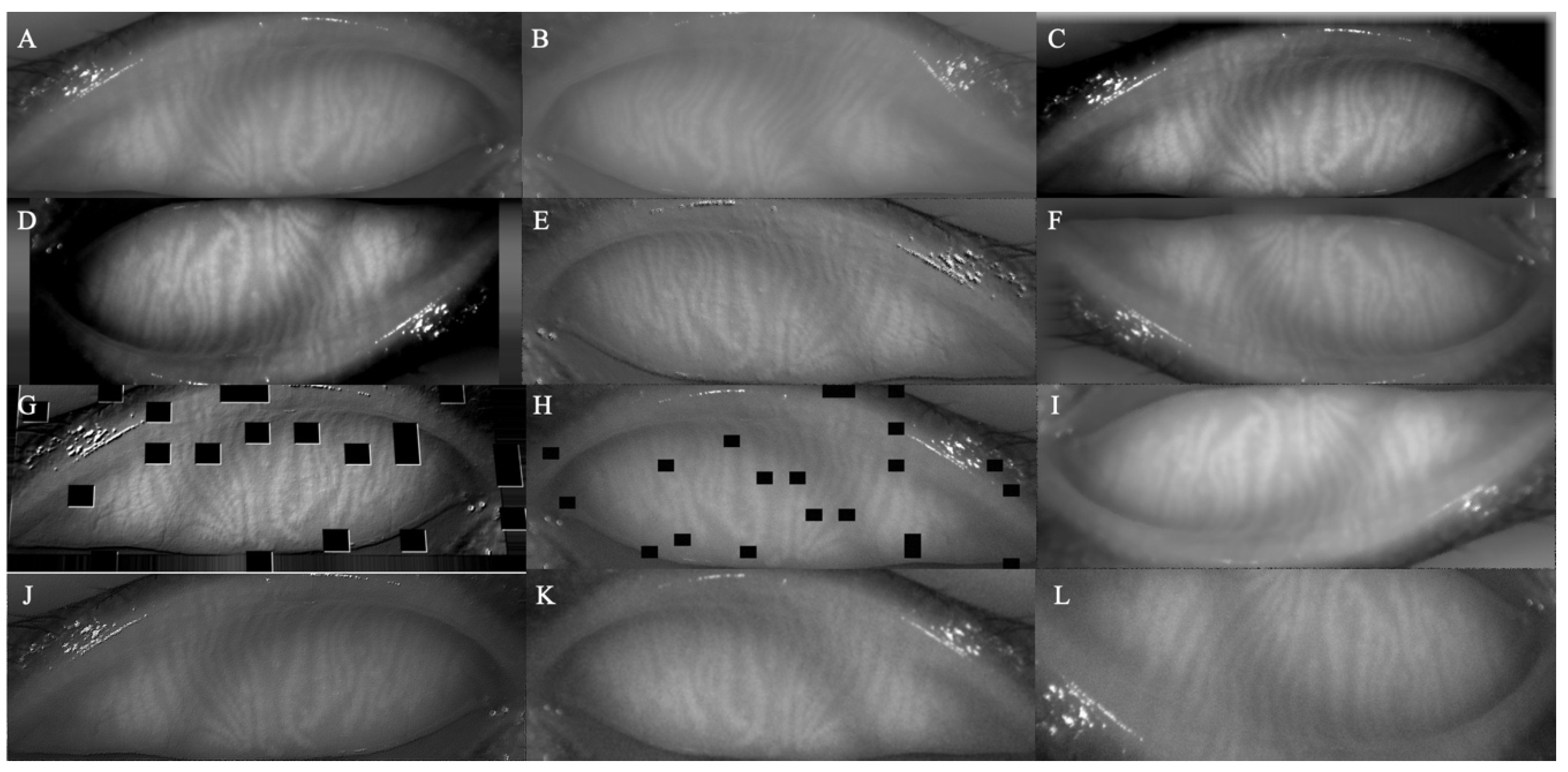
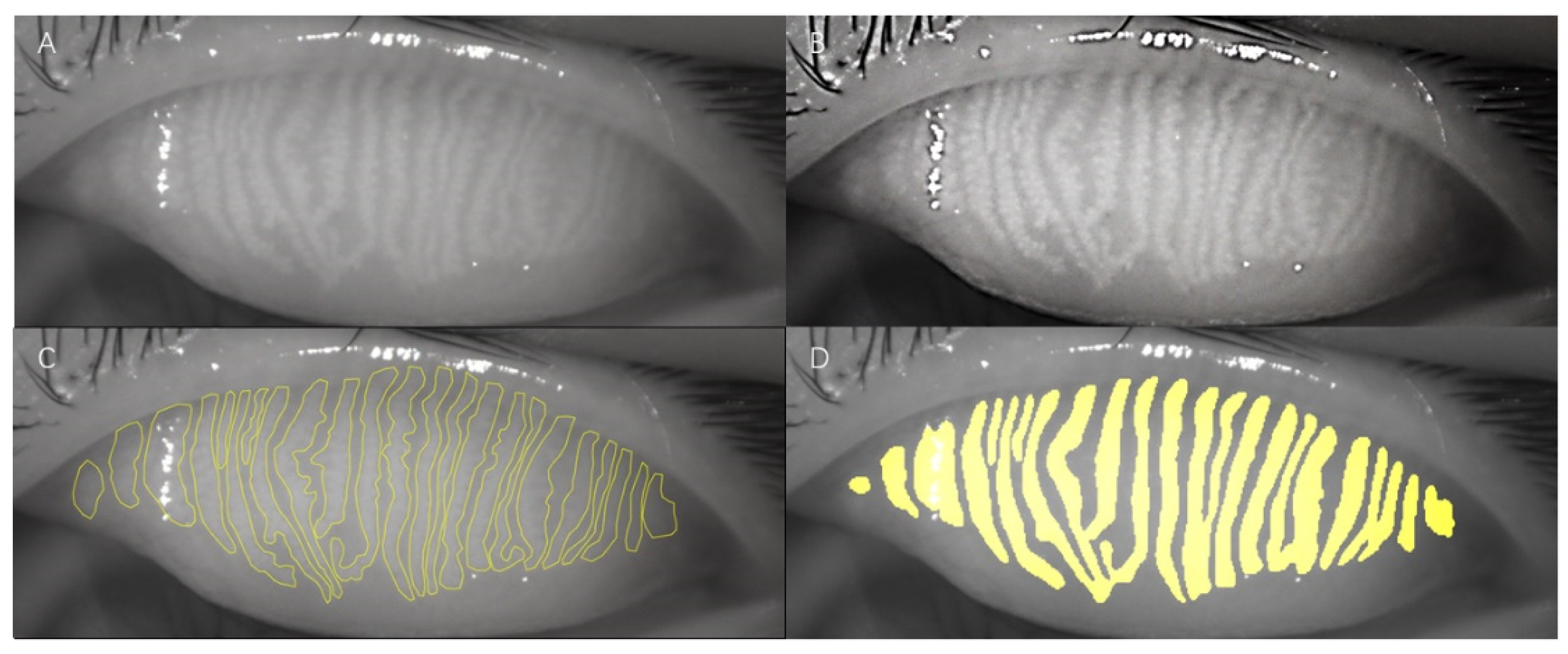
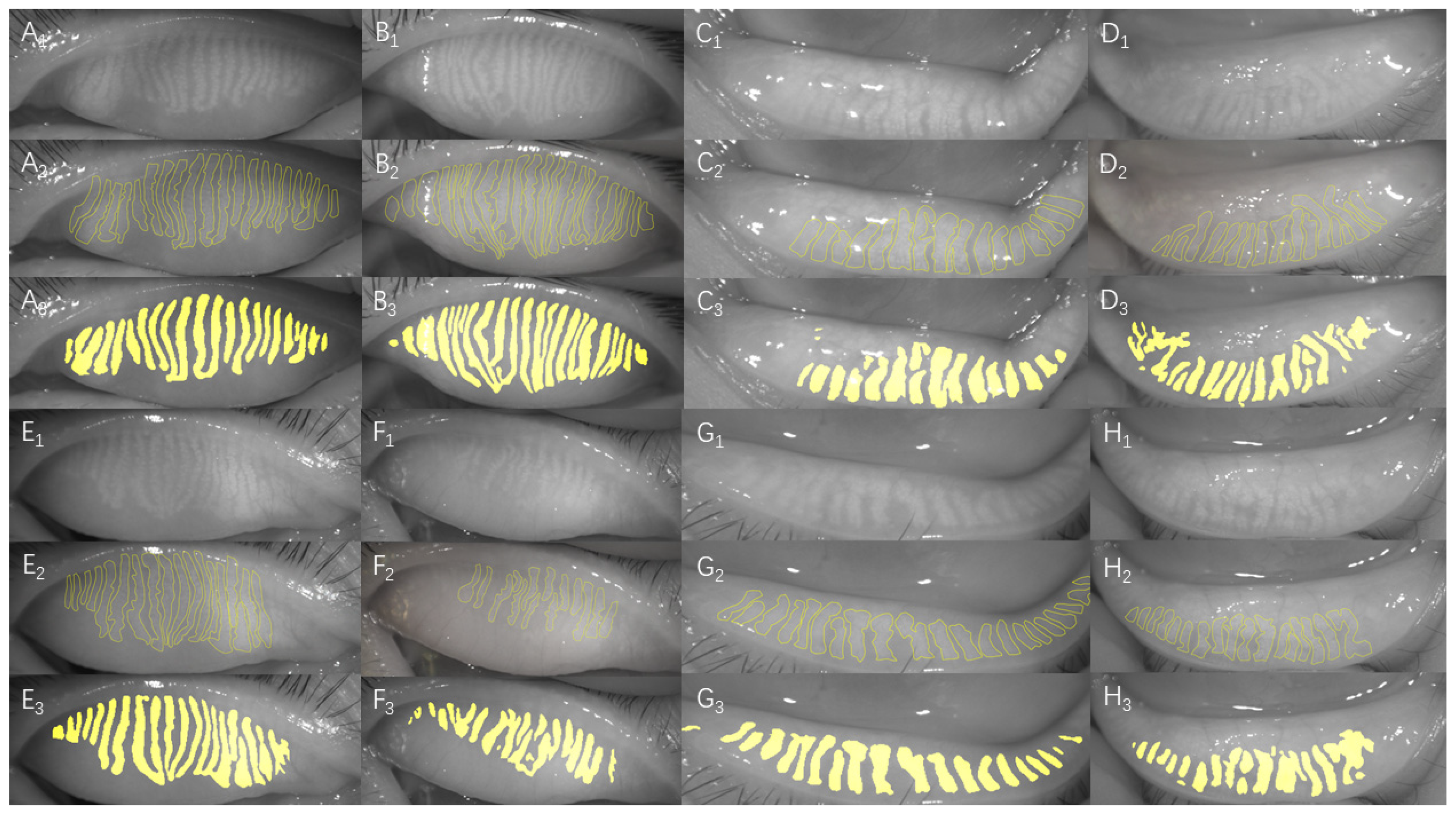
2.2.1. Data Collection and Processing of Samples
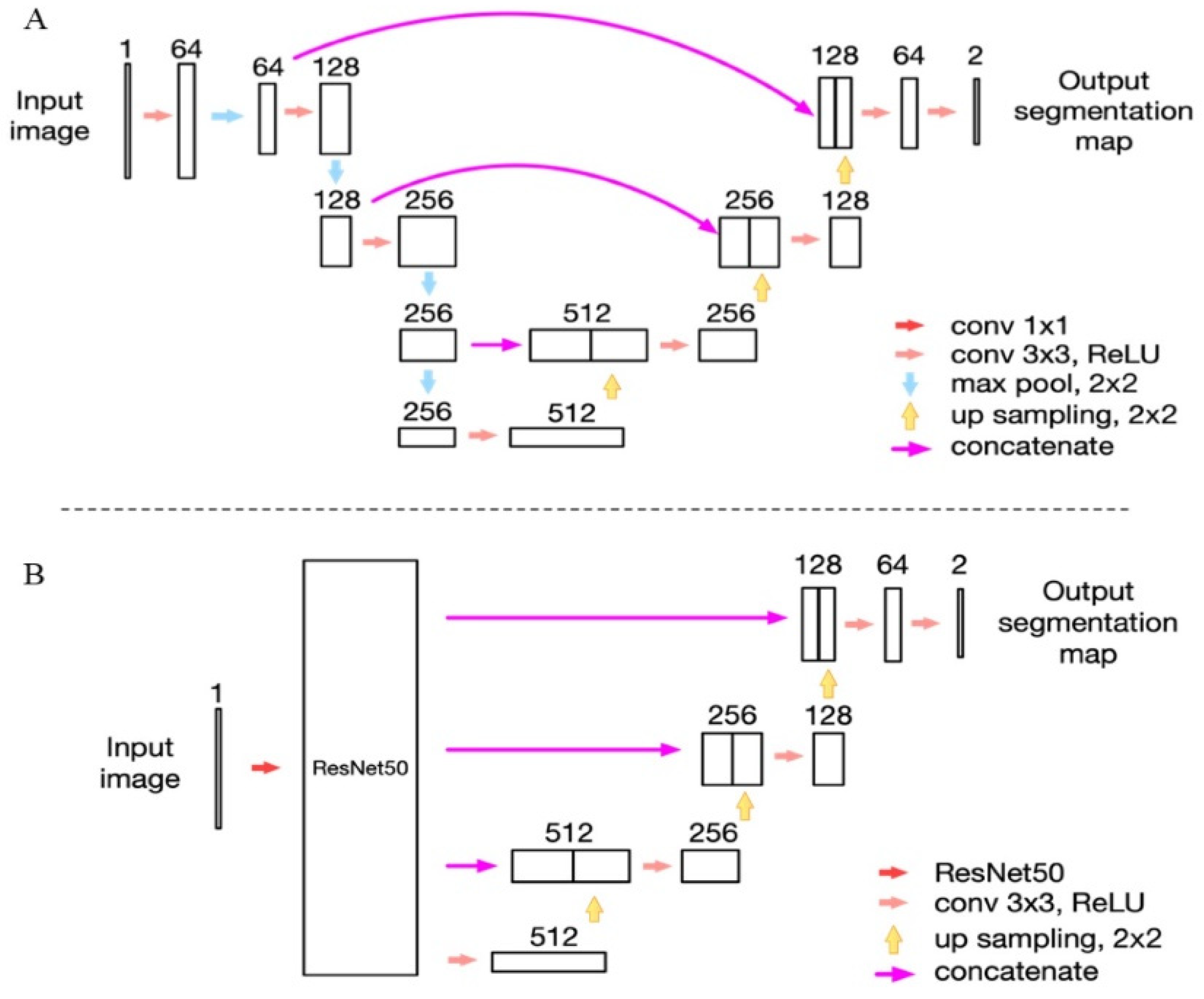
2.2.2. Network Structure and AI Training
2.2.3. Clinical Parameters
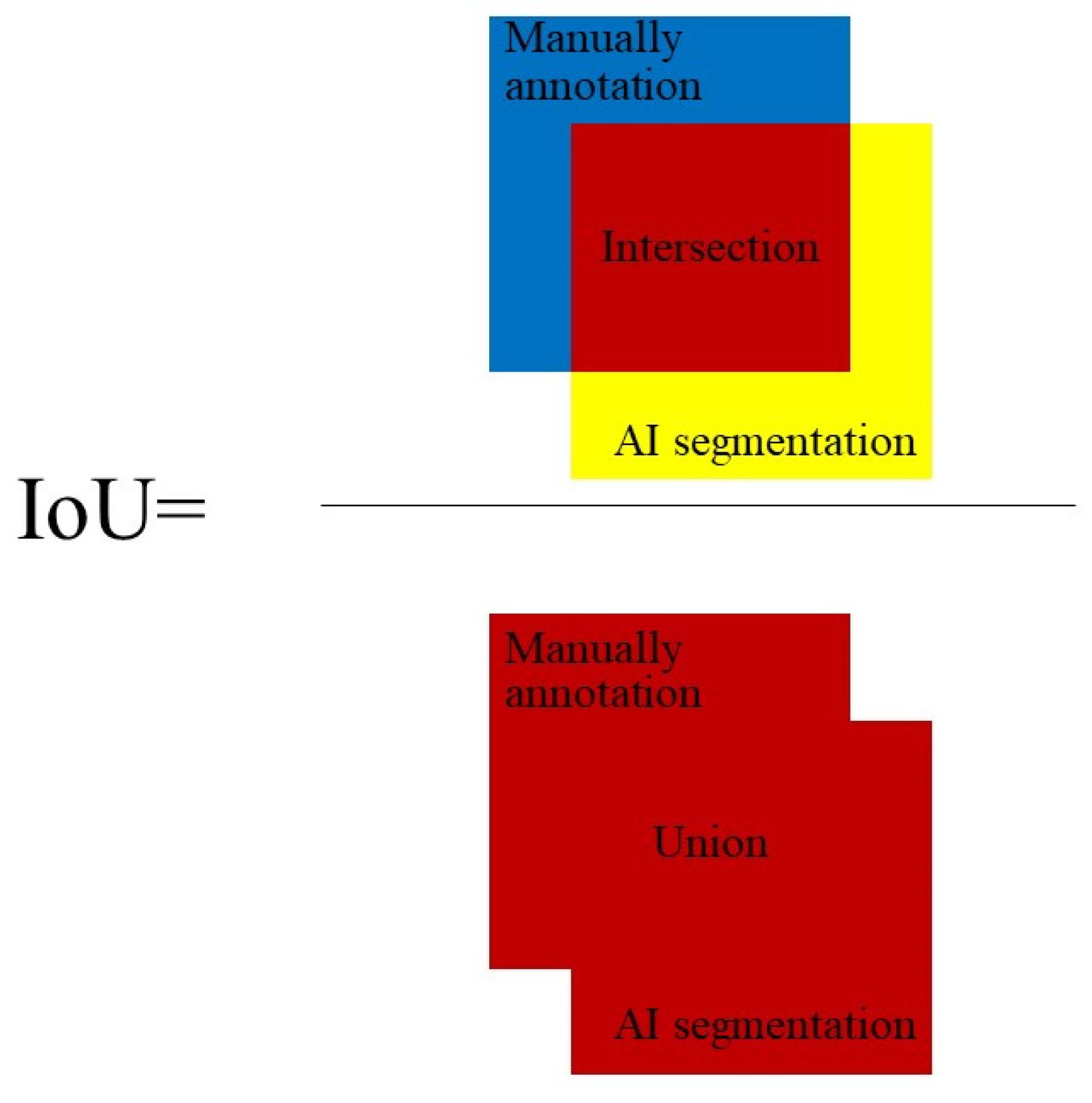
2.2.4. MG Indices
2.2.5. Statistical Analysis
3. Results
3.1. AI Training and Testing
3.2. Characteristics
3.3. MG Density and Functions
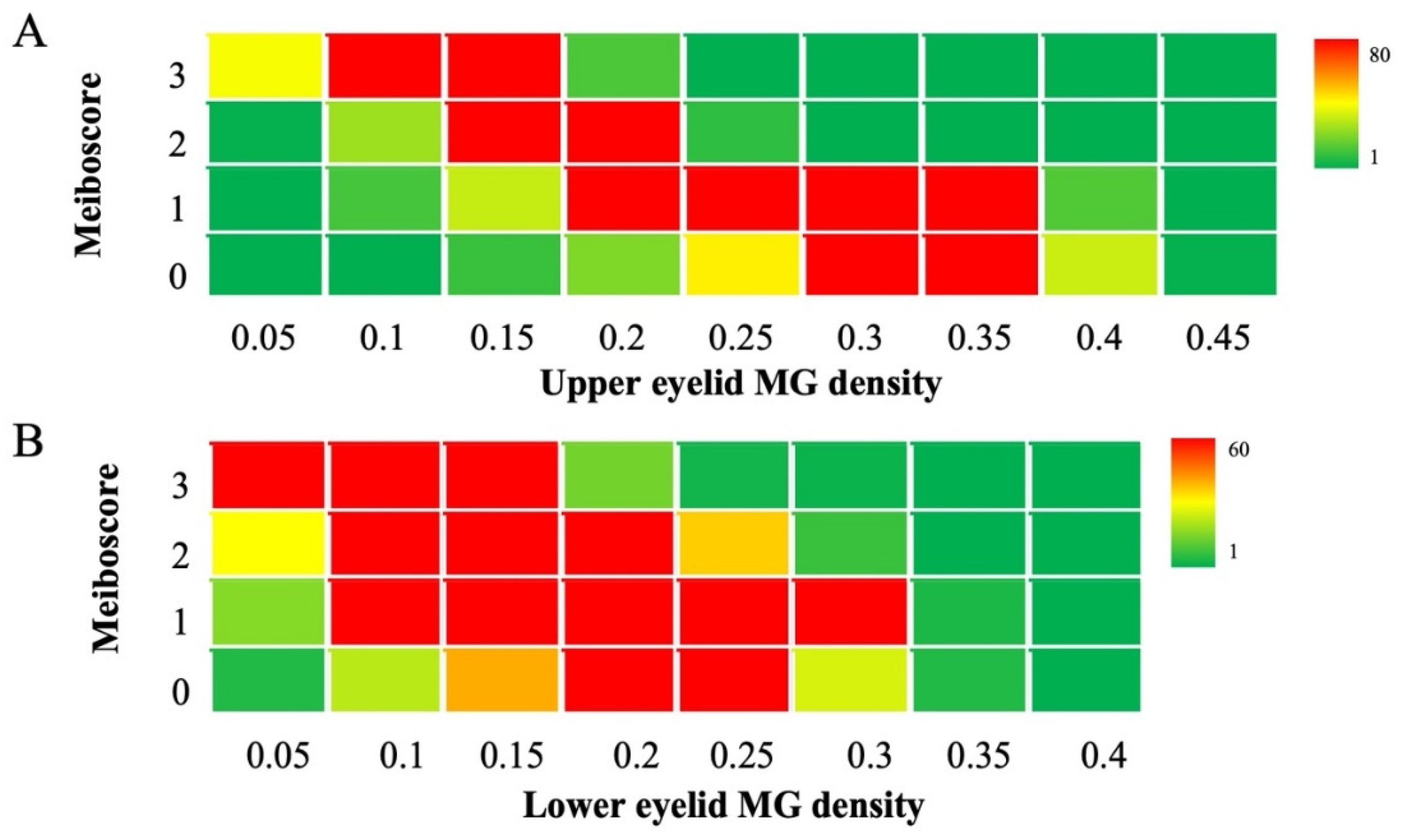
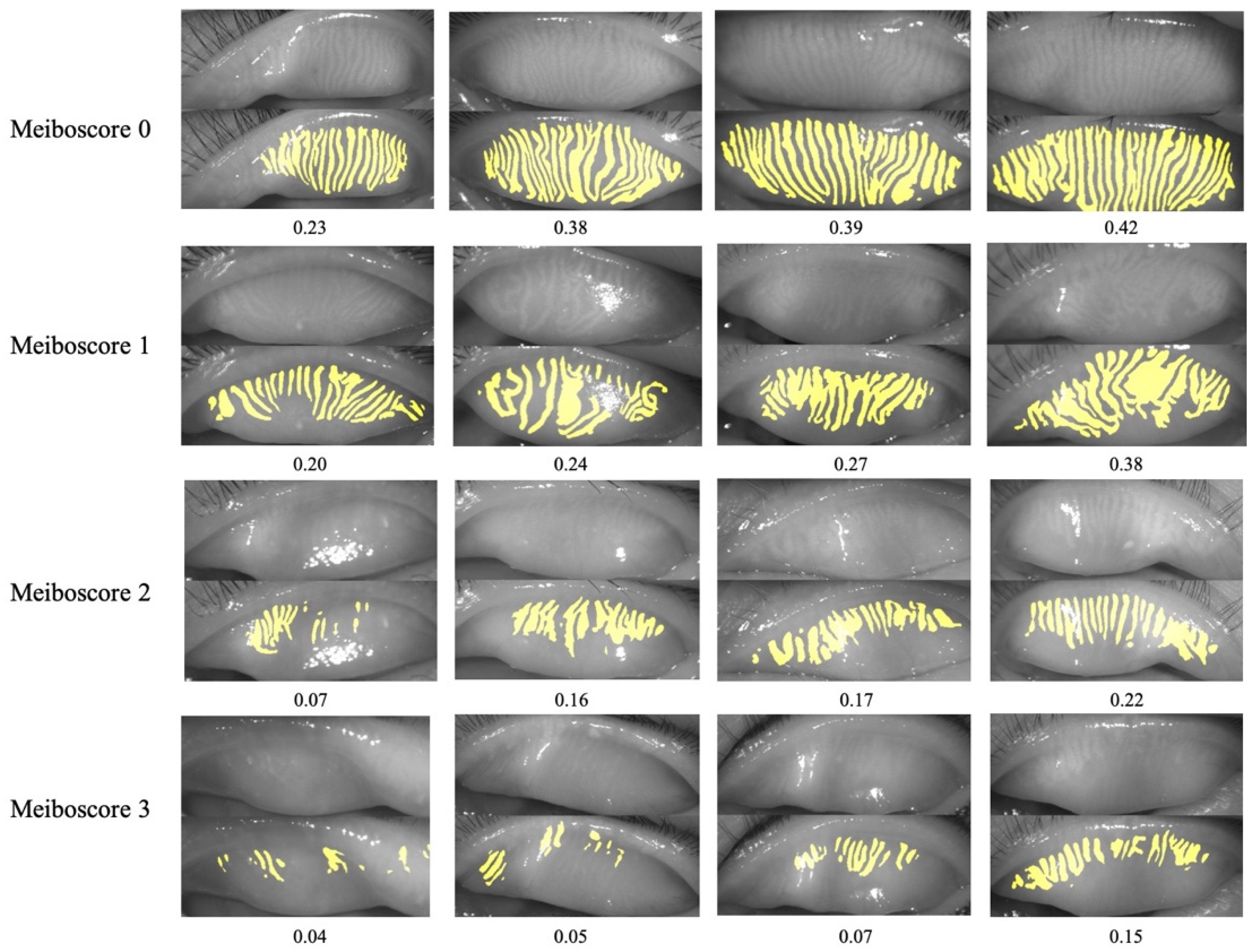
3.4. MG Density with Meiboscore
3.5. MG Density to Meiboscore
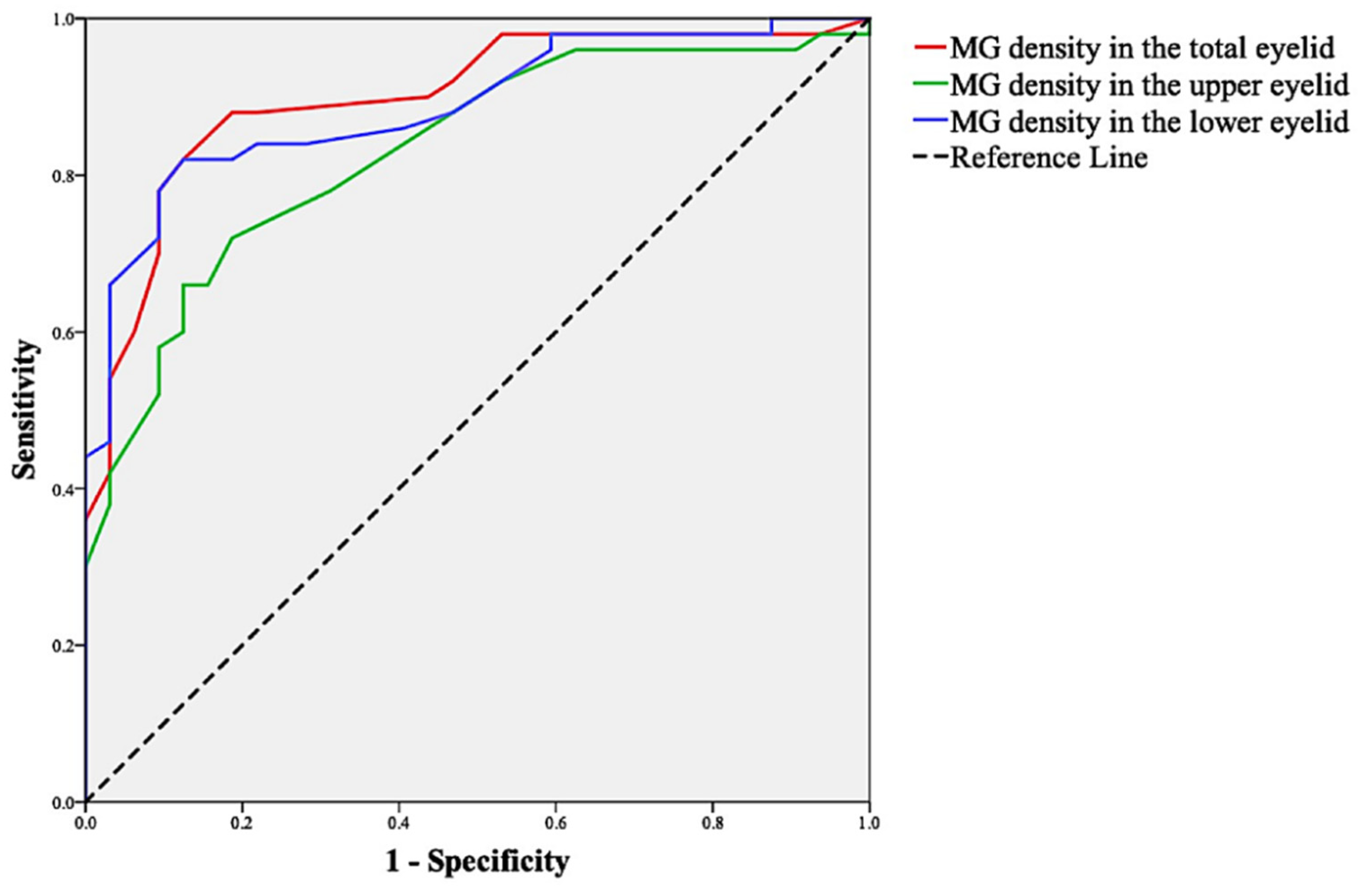
3.6. Sensitivity and Specificity of MG Density
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nichols, K.K.; Foulks, G.N.; Bron, A.J.; Glasgow, B.J.; Dogru, M.; Tsubota, K.; Lemp, M.A.; Sullivan, D.A. The international workshop on meibomian gland dysfunction: Executive summary. Investig. Ophthalmol. Vis. Sci. 2011, 52, 1922–1929. [Google Scholar] [CrossRef] [Green Version]
- Craig, J.P.; Nichols, K.K.; Akpek, E.K.; Caffery, B.; Dua, H.S.; Joo, C.K.; Liu, Z.; Nelson, J.D.; Nichols, J.J.; Tsubota, K.; et al. TFOS DEWS II Definition and Classification Report. Ocul. Surf. 2017, 15, 276–283. [Google Scholar] [CrossRef]
- Giannaccare, G.; Vigo, L.; Pellegrini, M.; Sebastiani, S.; Carones, F. Ocular Surface Workup With Automated Noninvasive Measurements for the Diagnosis of Meibomian Gland Dysfunction. Cornea 2018, 37, 740–745. [Google Scholar] [CrossRef]
- Ban, Y.; Shimazaki-Den, S.; Tsubota, K.; Shimazaki, J. Morphological evaluation of meibomian glands using noncontact infrared meibography. Ocul. Surf. 2013, 11, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Pult, H.; Riede-Pult, B.H.; Nichols, J.J. Relation between upper and lower lids’ meibomian gland morphology, tear film, and dry eye. Optom. Vis. Sci. 2012, 89, E310–E315. [Google Scholar] [CrossRef]
- Yin, Y.; Gong, L. Uneven Meibomian Gland Dropout Over the Tarsal Plate and its Correlation With Meibomian Gland Dysfunction. Cornea 2015, 34, 1200–1205. [Google Scholar] [CrossRef]
- Pult, H.; Nichols, J.J. A review of meibography. Optom. Vis. Sci. 2012, 89, E760–E769. [Google Scholar] [CrossRef] [Green Version]
- Srinivasan, S.; Menzies, K.; Sorbara, L.; Jones, L. Infrared imaging of meibomian gland structure using a novel keratograph. Optom. Vis. Sci. 2012, 89, E788–E794. [Google Scholar] [CrossRef]
- Arita, R.; Itoh, K.; Inoue, K.; Amano, S. Noncontact infrared meibography to document age-related changes of the meibomian glands in a normal population. Ophthalmology 2008, 115, 911–915. [Google Scholar] [CrossRef]
- Engel, L.A.; Wittig, S.; Bock, F.; Sauerbier, L.; Scheid, C.; Holtick, U.; Chemnitz, J.M.; Hallek, M.; Cursiefen, C.; Steven, P. Meibography and meibomian gland measurements in ocular graft-versus-host disease. Bone Marrow Transplant. 2015, 50, 961–967. [Google Scholar] [CrossRef] [Green Version]
- Arita, R.; Suehiro, J.; Haraguchi, T.; Shirakawa, R.; Tokoro, H.; Amano, S. Objective image analysis of the meibomian gland area. Br. J. Ophthalmol. 2014, 98, 746–755. [Google Scholar] [CrossRef] [Green Version]
- Xiao, P.; Luo, Z.; Deng, Y.; Wang, G.; Yuan, J. An automated and multiparametric algorithm for objective analysis of meibography images. Quant. Imaging Med. Surg. 2021, 11, 1586–1599. [Google Scholar] [CrossRef]
- Llorens-Quintana, C.; Rico-Del-Viejo, L.; Syga, P.; Madrid-Costa, D.; Iskander, D.R. A Novel Automated Approach for Infrared-Based Assessment of Meibomian Gland Morphology. Transl. Vis. Sci. Technol. 2019, 8, 17. [Google Scholar] [CrossRef] [Green Version]
- Ciężar, K.; Pochylski, M. 2D fourier transform for global analysis and classification of meibomian gland images. Ocul. Surf. 2020, 18, 865–870. [Google Scholar] [CrossRef]
- Yeh, C.H.; Yu, S.X.; Lin, M.C. Meibography Phenotyping and Classification From Unsupervised Discriminative Feature Learning. Transl. Vis. Sci. Technol. 2021, 10, 4. [Google Scholar] [CrossRef]
- Koh, Y.W.; Celik, T.; Lee, H.K.; Petznick, A.; Tong, L. Detection of meibomian glands and classification of meibography images. J. Biomed. Opt. 2012, 17, 086008. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Yeh, T.N.; Chakraborty, R.; Yu, S.X.; Lin, M.C. A Deep Learning Approach for Meibomian Gland Atrophy Evaluation in Meibography Images. Transl. Vis. Sci. Technol. 2019, 8, 37. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.W.; Yu, Y.; Zhou, Y.B.; Tan, Y.J.; Wu, L.L.; Xing, Y.Q.; Yang, Y.N. An advanced imaging method for measuring and assessing meibomian glands based on deep learning. Zhonghua Yan Ke Za Zhi 2020, 56, 774–779. [Google Scholar]
- Maruoka, S.; Tabuchi, H.; Nagasato, D.; Masumoto, H.; Chikama, T.; Kawai, A.; Oishi, N.; Maruyama, T.; Kato, Y.; Hayashi, T.; et al. Deep Neural Network-Based Method for Detecting Obstructive Meibomian Gland Dysfunction with In Vivo Laser Confocal Microscopy. Cornea 2020, 39, 720–725. [Google Scholar] [CrossRef]
- Dai, Q.; Liu, X.; Lin, X.; Fu, Y.; Chen, C.; Yu, X.; Zhang, Z.; Li, T.; Liu, M.; Yang, W.; et al. A Novel Meibomian Gland Morphology Analytic System Based on a Convolutional Neural Network. IEEE Access 2021, 9, 23083–23094. [Google Scholar] [CrossRef]
- Arita, R.; Itoh, K.; Maeda, S.; Maeda, K.; Furuta, A.; Fukuoka, S.; Tomidokoro, A.; Amano, S. Proposed diagnostic criteria for obstructive meibomian gland dysfunction. Ophthalmology 2009, 116, 2058–2063.e1. [Google Scholar] [CrossRef]
- He, K.; Gkioxari, G.; Dollar, P.; Girshick, R. Mask R-CNN. IEEE Trans. Pattern. Anal. Mach. Intell. 2020, 42, 386–397. [Google Scholar] [CrossRef]
- Deng, J.; Dong, W.; Socher, R.; Li, L.; Kai, L.; Li, F. Imagenet: A large-scale hierarchical image database. In Proceedings of the 2009 IEEE Conference on Computer Vision and Pattern Recognition, Miami, FL, USA, 20–25 June 2009; pp. 248–255. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Markoulli, M.; Duong, T.B.; Lin, M.; Papas, E. Imaging the Tear Film: A Comparison Between the Subjective Keeler Tearscope-Plus™ and the Objective Oculus® Keratograph 5M and LipiView® Interferometer. Curr. Eye Res. 2018, 43, 155–162. [Google Scholar] [CrossRef]
- De Paiva, C.S.; Pflugfelder, S.C. Corneal epitheliopathy of dry eye induces hyperesthesia to mechanical air jet stimulation. Am. J. Ophthalmol. 2004, 137, 109–115. [Google Scholar] [CrossRef]
- Cochener, B.; Cassan, A.; Omiel, L. Prevalence of meibomian gland dysfunction at the time of cataract surgery. J. Cataract. Refract. Surg. 2018, 44, 144–148. [Google Scholar] [CrossRef]
- Lin, X.; Fu, Y.; Li, L.; Chen, C.; Chen, X.; Mao, Y.; Lian, H.; Yang, W.; Dai, Q. A Novel Quantitative Index of Meibomian Gland Dysfunction, the Meibomian Gland Tortuosity. Transl. Vis. Sci. Technol. 2020, 9, 34. [Google Scholar] [CrossRef]
- García-Marqués, J.V.; García-Lázaro, S.; Talens-Estarelles, C.; Martínez-Albert, N.; Cerviño, A. Diagnostic Capability of a New Objective Method to Assess Meibomian Gland Visibility. Optom. Vis. Sci. 2021, 98, 1045–1055. [Google Scholar] [CrossRef]
- Russakovsky, O.; Deng, J.; Su, H.; Krause, J.; Satheesh, S.; Ma, S.; Huang, Z.; Karpathy, A.; Khosla, A.; Bernstein, M.; et al. Imagenet large scale visual recognition challenge. Int. J. Comput. Vis. 2015, 115, 211–252. [Google Scholar] [CrossRef] [Green Version]
- Burlina, P.; Pacheco, K.D.; Joshi, N.; Freund, D.E.; Bressler, N.M. Comparing humans and deep learning performance for grading AMD: A study in using universal deep features and transfer learning for automated AMD analysis. Comput. Biol. Med. 2017, 82, 80–86. [Google Scholar] [CrossRef] [Green Version]
- Asaoka, R.; Murata, H.; Hirasawa, K.; Fujino, Y.; Matsuura, M.; Miki, A.; Kanamoto, T.; Ikeda, Y.; Mori, K.; Iwase, A.; et al. Using Deep Learning and Transfer Learning to Accurately Diagnose Early-Onset Glaucoma From Macular Optical Coherence Tomography Images. Am. J. Ophthalmol. 2019, 198, 136–145. [Google Scholar] [CrossRef]
- Green-Church, K.B.; Butovich, I.; Willcox, M.; Borchman, D.; Paulsen, F.; Barabino, S.; Glasgow, B.J. The international workshop on meibomian gland dysfunction: Report of the subcommittee on tear film lipids and lipid-protein interactions in health and disease. Investig. Ophthalmol. Vis. Sci. 2011, 52, 1979–1993. [Google Scholar] [CrossRef] [Green Version]
- Nelson, J.D.; Shimazaki, J.; Benitez-del-Castillo, J.M.; Craig, J.P.; McCulley, J.P.; Den, S.; Foulks, G.N. The international workshop on meibomian gland dysfunction: Report of the definition and classification subcommittee. Investig. Ophthalmol. Vis. Sci. 2011, 52, 1930–1937. [Google Scholar] [CrossRef] [Green Version]
- Pflugfelder, S.C.; Tseng, S.C.; Sanabria, O.; Kell, H.; Garcia, C.G.; Felix, C.; Feuer, W.; Reis, B.L. Evaluation of subjective assessments and objective diagnostic tests for diagnosing tear-film disorders known to cause ocular irritation. Cornea 1998, 17, 38–56. [Google Scholar] [CrossRef]
- Nichols, J.J.; Berntsen, D.A.; Mitchell, G.L.; Nichols, K.K. An assessment of grading scales for meibography images. Cornea 2005, 24, 382–388. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Normal (n = 32) | MGD (n = 53) | p | p * |
|---|---|---|---|---|
| Age (years), Median (IQR) | 25.00 (16.25–32.75) | 35.00 (30.00–50.00) | <0.001 | - |
| Sex (n, male/female) | 13/19 | 20/33 | 0.794 | - |
| OSDI (0–100), Median (IQR) | 4.47 (0.30–12.35) | 25.00 (13.24–37.80) | <0.001 | <0.001 |
| Symptom score (0–14), Median (IQR) | 2.00 (0–4.00) | 7.00 (5.00–8.00) | <0.001 | <0.001 |
| TBUT (s), Median (IQR) | 5.00 (5.00–7.75) | 2.50 (1.33–3.67) | <0.001 | <0.001 |
| CFS (0–20), Median (IQR) | 0 (0–0) | 0 (0–0) | 0.058 | 0.021 |
| TMH (mm), Median (IQR) | 0.19 (0.16–0.23) | 0.20 (0.17–0.24) | 0.461 | 0.871 |
| Lid margin score (0–4), Median (IQR) | 0 (0–1.00) | 2.00 (1.00–2.00) | <0.001 | <0.001 |
| Meiboscore (0–6), Median (IQR) | 2.00 (1.00–2.00) | 3.00 (2.00–4.50) | <0.001 | <0.001 |
| Meibum expressibility score (0–45), Median (IQR) | 38.50 (30.00–45.00) | 18.00 (5.50–34.50) | <0.001 | <0.001 |
| OSDI | TBUT | CFS | TMH | Lid Margin Score | Meiboscore | Meibum Expressibility Score | ||
|---|---|---|---|---|---|---|---|---|
| MG density | Upper eyelid | −0.320 † | 0.484 ‡ | −0.162 | −0.059 | −0.350 † | −0.749 ‡ | 0.425 ‡ |
| Lower eyelid | −0.420 ‡ | 0.598 ‡ | −0.177 | −0.058 | −0.396 ‡ | −0.720 ‡ | 0.438 ‡ | |
| Total eyelid | −0.404 ‡ | 0.601 ‡ | −0.166 | −0.070 | −0.416 ‡ | −0.805 ‡ | 0.480 ‡ | |
| MG Density | ||||||
|---|---|---|---|---|---|---|
| Upper Eyelid (1620) | Lower Eyelid (2386) | |||||
| Median (IQR) | H-Value | p | Median (IQR) | H-Value | p | |
| Meiboscore 0 | 0.30 (0.25–0.33) | 882.932 | <0.001 | 0.19 (0.14–0.23) | 596.815 | <0.001 |
| Meiboscore 1 | 0.25 (0.21–0.29) | 0.17 (0.13–0.21) | ||||
| Meiboscore 2 | 0.15 (0.12–0.18) | 0.13 (0.10–0.17) | ||||
| Meiboscore 3 | 0.10 (0.06–0.12) | 0.07 (0.04–0.11) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Z.; Lin, X.; Yu, X.; Fu, Y.; Chen, X.; Yang, W.; Dai, Q. Meibomian Gland Density: An Effective Evaluation Index of Meibomian Gland Dysfunction Based on Deep Learning and Transfer Learning. J. Clin. Med. 2022, 11, 2396. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11092396
Zhang Z, Lin X, Yu X, Fu Y, Chen X, Yang W, Dai Q. Meibomian Gland Density: An Effective Evaluation Index of Meibomian Gland Dysfunction Based on Deep Learning and Transfer Learning. Journal of Clinical Medicine. 2022; 11(9):2396. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11092396
Chicago/Turabian StyleZhang, Zuhui, Xiaolei Lin, Xinxin Yu, Yana Fu, Xiaoyu Chen, Weihua Yang, and Qi Dai. 2022. "Meibomian Gland Density: An Effective Evaluation Index of Meibomian Gland Dysfunction Based on Deep Learning and Transfer Learning" Journal of Clinical Medicine 11, no. 9: 2396. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11092396