
The Impact of Resistance Training Program on Static Balance in Multiple Sclerosis Population: A Randomized Controlled Trial Study

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Testing Procedure
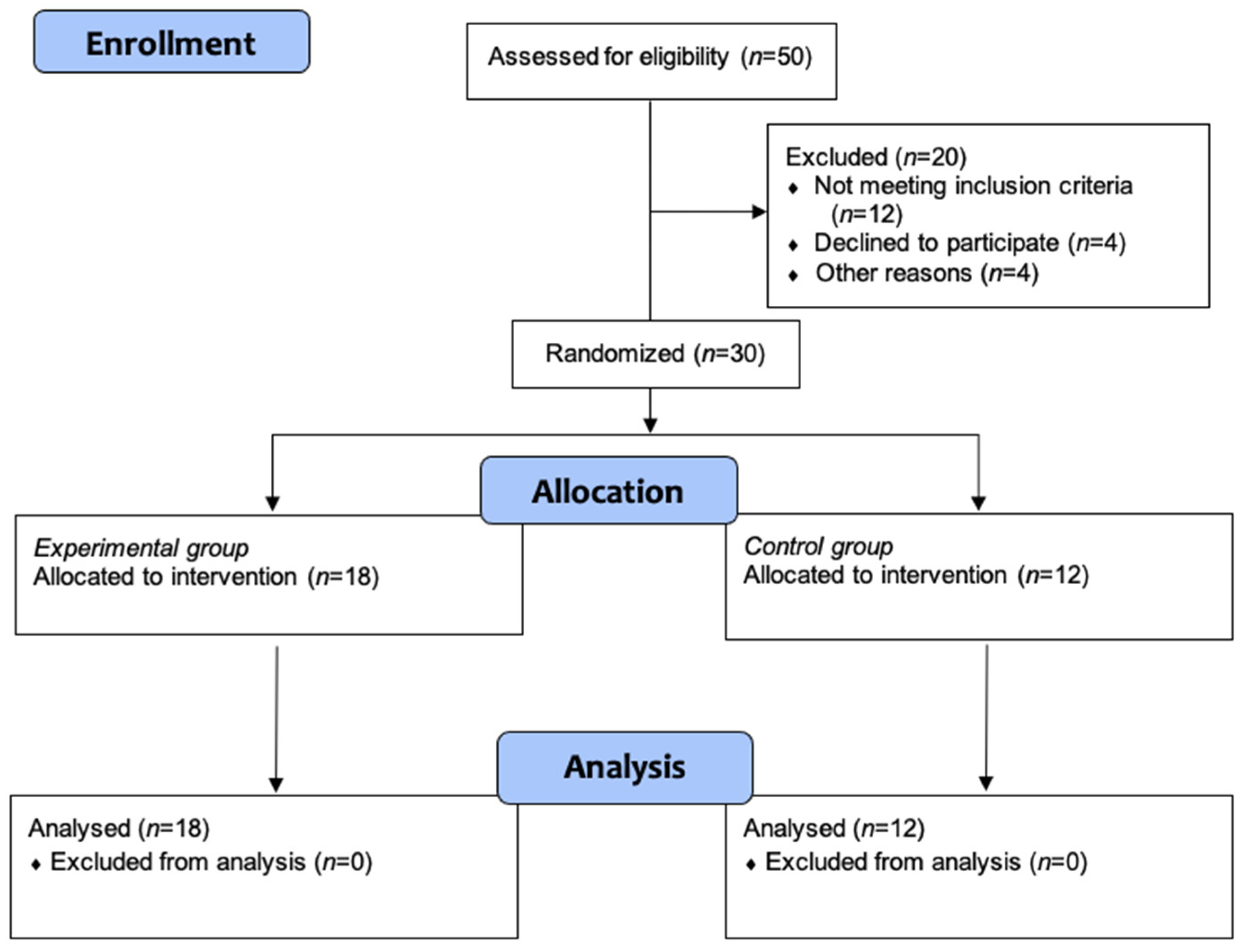
2.2. Participants
2.3. Procedures
2.4. Outcomes Measures
2.5. Testing Procedures
2.6. Balance
2.7. Statistical Analyses
3. Results
4. Discussion
Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chiaravalloti, N.D.; DeLuca, J. Cognitive impairment in multiple sclerosis. Lancet Neurol. 2008, 7, 1139–1151. [Google Scholar] [CrossRef]
- Jørgensen, M.L.K.; Dalgas, U.; Wens, I.; Hvid, L.G. Muscle strength and power in persons with multiple sclerosis—A systematic review and meta-analysis. J. Neurol. Sci. 2017, 376, 225–241. [Google Scholar] [CrossRef] [PubMed]
- Hickman, S.J.; Raoof, N.; McLean, R.J.; Gottlob, I. Vision and multiple sclerosis. Mult. Scler. Relat. Disord. 2014, 3, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.L.; Phillips, B.A.; Kilpatrick, T.J.; Butzkueven, H.; Tubridy, N.; McDonald, E.; Galea, M.P. Gait and balance impairment in early multiple sclerosis in the absence of clinical disability. Mult. Scler. 2006, 12, 620–628. [Google Scholar] [CrossRef] [PubMed]
- Sosnoff, J.J.; Socie, M.J.; Boes, M.K.; Sandroff, B.M.; Pula, J.H.; Suh, Y.; Weikert, M.; Balantrapu, S.; Morrison, S.; Motl, R.W. Mobility, balance and falls in persons with multiple sclerosis. PLoS ONE 2011, 6, e28021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasser, S.L.; Jacobs, J.V.; Foley, J.T.; Cardinal, B.J.; Maddalozzo, G.F. A prospective evaluation of balance, gait, and strength to predict falling in women with multiple sclerosis. Arch. Phys. Med. Rehabil. 2011, 92, 1840–1846. [Google Scholar] [CrossRef]
- Prosperini, L.; Fortuna, D.; Giannì, C.; Leonardi, L.; Pozzilli, C. The diagnostic accuracy of static posturography in predicting accidental falls in people with multiple sclerosis. Neurorehabil. Neural Repair 2013, 27, 45–52. [Google Scholar] [CrossRef]
- Prosperini, L.; Kouleridou, A.; Petsas, N.; Leonardi, L.; Tona, F.; Pantano, P.; Pozzilli, C. The relationship between infratentorial lesions, balance deficit and accidental falls in multiple sclerosis. J. Neurol. Sci. 2011, 304, 55–60. [Google Scholar] [CrossRef]
- Houdijk, H.; Fickert, R.; van Velzen, J.; van Bennekom, C. The energy cost for balance control during upright standing. Gait Posture 2009, 30, 150–154. [Google Scholar] [CrossRef]
- Andreu-Caravaca, L.; Ramos-Campo, D.J.; Chung, L.H.; Rubio-Arias, J.Á. Dosage and effectiveness of aerobic training on cardiorespiratory fitness, functional capacity, balance, and fatigue in people with Multiple Sclerosis: A systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2021, 102, 1826–1839. [Google Scholar] [CrossRef]
- Cruickshank, T.M.; Reyes, A.R.; Ziman, M.R. A Systematic Review and Meta-Analysis of Strength Training in Individuals with Multiple Sclerosis or Parkinson Disease. Medicine 2015, 94, e411. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Lastra, M.A.; Martínez-Aldao, D.; Molina, A.J.; Ayán, C. Pilates for people with multiple sclerosis: A systematic review and meta-analysis. Mult. Scler. Relat. Disord. 2019, 28, 199–212. [Google Scholar] [CrossRef] [PubMed]
- Callesen, J.; Cattaneo, D.; Brincks, J.; Kjeldgaard Jørgensen, M.L.; Dalgas, U. How do resistance training and balance and motor control training affect gait performance and fatigue impact in people with multiple sclerosis? A randomized controlled multi-center study. Mult. Scler. J. 2020, 26, 1420–1432. [Google Scholar] [CrossRef]
- Aidar, F.J.; Carneiro, A.L.; Costa Moreira, O.; Patrocínio De Oliveira, C.E.; Garrido, N.D.; Machado Reis, V.; Raineh, I.; Vhaça, J.M.; Gama De Matos, D. Effects of resistance training on the physical condition of people with multiple sclerosis. J. Sports Med. Phys. Fitness 2018, 58, 1127–1134. [Google Scholar] [CrossRef] [PubMed]
- Blazevich, A.J.; Wilson, C.J.; Alcaraz, P.E.; Rubio-Arias, J.A. Effects of Resistance Training Movement Pattern and Velocity on Isometric Muscular Rate of Force Development: A Systematic Review with Meta-analysis and Meta-regression. Sport. Med. 2020, 50, 943–963. [Google Scholar] [CrossRef] [PubMed]
- Karpatkin, H.I.; Cohen, E.T.; Klein, S.; Park, D.; Wright, C.; Zervas, M. The Effect of Maximal Strength Training on Strength, Walking, and Balance in People with Multiple Sclerosis: A Pilot Study. Mult. Scler. Int. 2016, 2016, 5235971. [Google Scholar] [CrossRef]
- Association, W.M. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Kjølhede, T.; Vissing, K.; Dalgas, U. Multiple sclerosis and progressive resistance training: A systematic review. Mult. Scler. J. 2012, 18, 1215–1228. [Google Scholar] [CrossRef]
- Dohoney, P.; Chromiak, J.A.; Lemire, D.; Abadie, B.R.; Kovacs, C. Prediction of one repetition maximum (1-RM) strength from a 4-6 RM and a7-10 RM submaximal strength test in healthy young adult males. J. Exerc. Physiol. Online 2002, 20, 584–592. [Google Scholar]
- Abdalla, P.P.; Carvalho, A.D.S.; Dos Santos, A.P.; Venturini, A.C.R.; Alves, T.C.; Mota, J.; MacHado, D.R.L. One-repetition submaximal protocol to measure knee extensor muscle strength among older adults with and without sarcopenia: A validation study. BMC Sports Sci. Med. Rehabil. 2020, 12, 29. [Google Scholar] [CrossRef] [PubMed]
- ACSM. ACSM’s Guidelines for Exercise Testing and Prescripstion; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2009; ISBN 978-0-7817-6903-7. [Google Scholar]
- Kantner, R.M.; Rubin, A.M.; Armstrong, C.W.; Cummings, V. Stabilometry in balance assessment of dizzy and normal subjects. Am. J. Otolaryngol. Neck Med. Surg. 1991, 12, 196–204. [Google Scholar] [CrossRef]
- Cattaneo, D.; Regola, A.; Meotti, M. Validity of six balance disorders scales in persons with multiple sclerosis. Disabil. Rehabil. 2006, 28, 789–795. [Google Scholar] [CrossRef]
- Prosperini, L.; Pozzilli, C. The Clinical Relevance of Force Platform Measures in Multiple Sclerosis: A Review. Mult. Scler. Int. 2013, 2013, 756564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeBolt, L.S.; McCubbin, J.A. The Effects of Home-Based Resistance Exercise on Balance, Power, and Mobility in Adults with Multiple Sclerosis. Arch. Phys. Med. Rehabil. 2004, 85, 290–297. [Google Scholar] [CrossRef]
- Widener, G.L.; Allen, D.D.; Gibson-Horn, C. Randomized clinical trial of balance-based torso weighting for improving upright mobility in people with multiple sclerosis. Neurorehabil. Neural Repair 2009, 23, 784–791. [Google Scholar] [CrossRef]
- Schuhfried, O.; Mittermaier, C.; Jovanovic, T.; Pieber, K.; Paternostro-Sluga, T. Effects of whole-body vibration in patients with multiple sclerosis: A pilot study. Clin. Rehabil. 2005, 19, 834–842. [Google Scholar] [CrossRef] [Green Version]
- Missaoui, B.; Thoumie, P. How far do patients with sensory ataxia benefit from so-called “proprioceptive rehabilitation”? Neurophysiol. Clin. 2009, 39, 229–233. [Google Scholar] [CrossRef]
- Coote, S.; Hughes, L.; Rainsford, G.; Minogue, C.; Donnelly, A. Pilot Randomized Trial of Progressive Resistance Exercise Augmented by Neuromuscular Electrical Stimulation for People with Multiple Sclerosis Who Use Walking Aids. Arch. Phys. Med. Rehabil. 2015, 96, 197–204. [Google Scholar] [CrossRef]
- Hayes, H.A.; Gappmaier, E.; Lastayo, P.C. Effects of high-intensity resistance training on strength, mobility, balance, and fatigue in individuals with multiple sclerosis: A randomized controlled trial. J. Neurol. Phys. Ther. 2011, 35, 2–10. [Google Scholar] [CrossRef]
- Hogan, N.; Kehoe, M.; Larkin, A.; Coote, S. The Effect of Community Exercise Interventions for People with MS Who Use Bilateral Support for Gait. Mult. Scler. Int. 2014, 2014, 109142. [Google Scholar] [CrossRef] [PubMed]
- Jonsdottir, J.; Gervasoni, E.; Bowman, T.; Bertoni, R.; Tavazzi, E.; Rovaris, M.; Cattaneo, D. Intensive multimodal training to improve gait resistance, mobility, balance and cognitive function in persons with multiple sclerosis: A pilot randomized controlled trial. Front. Neurol. 2018, 9, 800. [Google Scholar] [CrossRef] [PubMed]
- Frevel, D.; Mäurer, M. Internet-based home training is capable to improve balance in multiple sclerosis: A randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2015, 51, 23–30. [Google Scholar] [PubMed]
- Keser, I.; Meric, A.; Kirdi, N.; Kurne, A.; Karabudak, R. Comparing routine neurorehabilitation programme with callisthenic exercises in multiple sclerosis. NeuroRehabilitation 2011, 29, 91–98. [Google Scholar] [CrossRef]
- van Hooren, B.; Bosch, F.; Meijer, K. Can Resistance Training Enhance the Rapid Force Development in Unloaded Dynamic Isoinertial Multi-Joint Movements? A Systematic Review. J. Strength Cond. Res. 2017, 31, 2324–2337. [Google Scholar] [CrossRef] [Green Version]
- Gandolfi, M.; Munari, D.; Geroin, C.; Gajofatto, A.; Benedetti, M.D.; Midiri, A.; Carla, F.; Picelli, A.; Waldner, A.; Smania, N. Sensory integration balance training in patients with multiple sclerosis: A randomized, controlled trial. Mult. Scler. J. 2015, 21, 1453–1462. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | All (n = 30) | RTG (n = 18) | CG (n = 12) | p |
|---|---|---|---|---|
| Age (years) | 46.21 ± 10.43 | 44.89 ± 10.62 | 48.36 ± 10.23 | 0.394 |
| Sex (men/women) | 15:15 | 10:8 | 5:7 | |
| MS phenotype (RR/SP) | 27:3 | 16:2 | 11:1 | |
| EDSS | 3.21 (1.00–6.00) | 3.17 (1.00–6.00) | 3.27 (1.50–5.50) | |
| Weight (kg) | 68.51 ± 11.55 | 67.19 ± 10.63 | 70.67 ± 13.17 | 0.442 |
| Height (cm) | 166.86 ± 6.95 | 166.44 ± 7.32 | 167.54 ± 6.58 | 0.687 |
| BMI (kg⋅m−2) | 24.56 ± 3.29 | 24.26 ± 3.12 | 25.06 ± 3.64 | 0.534 |
| Fat mass (%) | 26.47 ± 8.72 | 25.92 ± 8.28 | 27.34 ± 9.69 | 0.680 |
| Outcomes | All (n = 30) | RTG (n = 18) | CG (n = 12) | p |
|---|---|---|---|---|
| SA (mm2) | 5.35 ± 4.11 | 5.00 ± 3.93 | 5.49 ± 3.76 | 0.731 |
| TSD (mm) | 917.00 ± 183.00 | 914.00 ± 191.00 | 870.00 ± 149.00 | 0.493 |
| MAPD (mm) | 2.24 ± 1.06 | 2.04 ± 1.10 | 2.54 ± 1.21 | 0.264 |
| MMLD (mm) | 4.20 ± 1.80 | 4.39 ± 2.00 | 4.15 ± 1.67 | 0.729 |
| SDAAP (mm) | 5.23 ± 2.20 | 5.38 ± 2.27 | 5.16 ± 2.06 | 0.785 |
| SDAML (mm) | 2.85 ± 1.31 | 3.22 ± 1.46 | 2.64 ± 1.43 | 0.299 |
| SDVAP (mm/s) | 22.57 ± 5.91 | 21.90 ± 4.17 | 22.40 ± 6.86 | 0.834 |
| SDVML (mm/s) | 26.45 ± 6.40 | 26.9 ± 6.84 | 24.30 ± 5.30 | 0.259 |
| PPPAP (a.u.) | 23.32 ± 6.03 | 22.8 ± 4.40 | 23.10 ± 6.94 | 0.876 |
| PPPML (a.u.) | 26.77 ± 6.42 | 27.20 ± 6.83 | 24.60 ± 5.30 | 0.275 |
| PPPAP-ML (a.u.) | 36.06 ± 7.30 | 35.80 ± 7.26 | 34.50 ± 6.48 | 0.629 |
| MTV (mm/s) | 30.59 ± 6.12 | 30.50 ± 6.38 | 29.00 ± 4.93 | 0.504 |
| Outcomes | All (n = 30) | RTG (n = 18) | CG (n = 12) | p |
|---|---|---|---|---|
| SA (mm2) | 6.68 ± 5.49 | 5.25 ± 5.08 | 6.34 ± 3.71 | 0.552 |
| TSD (mm) | 1105.00 ± 285.00 | 1085.00 ± 270.00 | 992.00 ± 85.80 | 0.316 |
| MAPD (mm) | 2.47 ± 1.68 | 2.14 ± 0.89 | 2.22 ± 1.68 | 0.893 |
| MMLD (mm) | 5.82 ± 3.05 | 5.16 ± 3.03 | 6.22 ± 2.72 | 0.339 |
| SDAAP (mm) | 7.16 ± 3.58 | 6.20 ± 3.48 | 7.65 ± 3.26 | 0.270 |
| SDAML (mm) | 3.14 ± 2.07 | 2.80 ± 2.07 | 2.79 ± 1.20 | 0.985 |
| SDVAP (mm/s) | 28.61 ± 9.21 | 26.70 ± 7.62 | 28.30 ± 7.65 | 0.600 |
| SDVML (mm/s) | 28.13 ± 6.27 | 28.10 ± 6.19 | 26.30 ± 4.47 | 0.389 |
| PPPAP (a.u.) | 29.55 ± 9.49 | 27.70 ± 8.03 | 29.40 ± 7.89 | 0.598 |
| PPPML (a.u.) | 28.44 ± 6.27 | 28.30 ± 6.19 | 26.70 ± 4.69 | 0.456 |
| PPPAP-ML (a.u.) | 42.47 ± 10.12 | 41.30 ± 9.96 | 41.10 ± 6.93 | 0.947 |
| MTV (mm/s) | 35.95 ± 8.26 | 35.30 ± 8.45 | 34.60 ± 5.53 | 0.811 |
| Outcomes | RTG | CG | BF | t Test | p |
|---|---|---|---|---|---|
| SA (mm2) | 5.12 ± 4.25 | 6.10 ± 4.86 | 0.398 | −0.59 | 0.55 |
| TSD (mm) | 893.00 ± 204.00 | 1006.00 ± 163.00 | 0.894 | −1.65 | 0.11 |
| MAPD (mm) | 1.99 ± 0.77 | 2.59 ± 1.16 | 0.993 | −1.57 | 0.13 |
| MMLD (mm) | 3.94 ± 1.68 | 4.34 ± 1.98 | 0.398 | −0.60 | 0.55 |
| SDAAP (mm) | 5.54 ± 2.52 | 4.91 ± 2.13 | 0.429 | −0.74 | 0.456 |
| SDAML (mm) | 2.50 ± 0.99 | 3.28 ± 1.32 | 1.192 | −1.73 | 0.097 |
| SDVAP (mm/s) | 21.20 ± 5.85 | 25.80 ± 6.81 | 1.377 | −1.88 | 0.074 |
| SDVML (mm/s) | 26.00 ± 6.42 | 28.50 ± 6.79 | 0.504 | −0.97 | 0.341 |
| PPPAP (a.u.) | 22.00 ± 6.01 | 26.40 ± 6.84 | 1.278 | −1.84 | 0.080 |
| PPPML (a.u.) | 26.30 ± 6.52 | 29.00 ± 6.67 | 0.553 | −1.10 | 0.284 |
| PPPAP-ML (a.u.) | 34.90 ± 8.01 | 39.70 ± 6.66 | 1.040 | −1.78 | 0.087 |
| MTV (mm/s) | 29.80 ± 6.81 | 33.50 ± 5.49 | 0.861 | −1.62 | 0.117 |
| Outcomes | RTG | CG | BF | t Test | p |
|---|---|---|---|---|---|
| SA (mm2) | 6.84 ± 5.81 | 9.16 ± 6.85 | 0.506 | −0.94 | 0.347 |
| TSD (mm) | 1123 ± 372 | 1134.00 ± 208.00 | 0.373 | −0.08 | 0.937 |
| MAPD (mm) | 2.64 ± 1.99 | 2.94 ± 1.77 | 0.387 | −0.41 | 0.68 |
| MMLD (mm) | 5.82 ± 3.19 | 6.48 ± 3.38 | 0.395 | −0.52 | 0.61 |
| SDAAP (mm) | 7.30 ± 3.89 | 8.01 ± 3.65 | 0.390 | −0.50 | 0.624 |
| SDAML (mm) | 3.35 ± 2.44 | 3.70 ± 2.16 | 0.390 | −0.38 | 0.705 |
| SDVAP (mm/s) | 28.60 ± 11.1 | 32.10 ± 9.79 | 0.471 | −0.83 | 0.406 |
| SDVML (mm/s) | 27.50 ± 6.74 | 31.00 ± 7.00 | 0.679 | −1.30 | 0.207 |
| PPPAP (a.u.) | 29.70 ± 11.4 | 32.70 ± 10.2 | 0.433 | −0.68 | 0.496 |
| PPPML (a.u.) | 27.70 ± 6.70 | 31.50 ± 6.88 | 0.744 | −1.40 | 0.176 |
| PPPAP-ML (a.u.) | 42.00 ± 12.10 | 46.70 ± 9.67 | 0.554 | −1.13 | 0.271 |
| MTV (mm/s) | 35.60 ± 9.66 | 39.10 ± 8.02 | 0.519 | −1.02 | 0.317 |
| ANOVA | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Time Effect | Group Effect | Time × Group Effect | |||||||||||||||
| Outcome | Group | Pre | Post | F | p | eta | F | p | eta | F | p | eta | Post Intr Padj | Post Intr ES (d) | Post M | Post Intr Pad | Post Intr ES (d) |
| SA (mm2) | CG | 5.49 ± 3.76 | 6.10 ± 4.86 | 0.579 | 0.453 | 0.002 | 0.244 | 0.625 | 0.008 | 0.273 | 0.605 | 0.001 | 0.99 | 0.14 | Pre | 1.00 | 0.22 |
| RTG | 5.00 ± 3.93 | 5.12 ± 4.25 | 1.00 | 0.03 | Post | 1.00 | 0.13 | ||||||||||
| TSD (mm) | CG | 870 ± 149 | 1006 ± 163 | 1.608 | 0.216 | 0.025 | 0.450 | 0.508 | 0.009 | 3.012 | 0.094 | 0.046 | 0.14 | 0.87 | Pre | 0.25 | 0.60 |
| RTG | 914 ± 191 | 893 ± 204 | 1.00 | 0.11 | Post | 1.00 | 0.25 | ||||||||||
| MAPD (mm) | CG | 2.54 ± 1.21 | 2.59 ± 1.16 | 0.000 | 0.995 | 0.000 | 2.163 | 0.153 | 0.007 | 0.145 | 0.707 | 0.000 | 1.00 | 0.04 | Pre | 0.51 | 0.63 |
| RTG | 2.04 ± 1.10 | 1.99 ± 0.77 | 1.00 | 0.05 | Post | 0.21 | 0.44 | ||||||||||
| MMLD (mm) | CG | 4.15 ± 1.67 | 4.34 ± 1.98 | 0.334 | 0.568 | 0.001 | 0.015 | 0.903 | 0.000 | 2.084 | 0.160 | 0.008 | 0.96 | 0.10 | Pre | 1.00 | 0.22 |
| RTG | 4.39 ± 2.00 | 3.94 ± 1.68 | 0.35 | 0.24 | Post | 1.00 | 0.13 | ||||||||||
| SDAAP (mm) | CG | 5.16 ± 2.06 | 5.54 ± 2.52 | 0.035 | 0.853 | 0.001 | 0.066 | 0.799 | 0.002 | 3.004 | 0.094 | 0.009 | 0.31 | 0.19 | Pre | 0.54 | 0.17 |
| RTG | 5.38 ± 2.27 | 4.91 ± 2.13 | 0.16 | 0.21 | Pos | 0.67 | 0.24 | ||||||||||
| SDAML (mm) | CG | 2.64 ± 1.43 | 3.28 ± 1.32 | 0.068 | 0.797 | 0.000 | 2.156 | 0.154 | 0.067 | 0.433 | 0.516 | 0.002 | 0.77 | 0.04 | Pre | 0.30 | 0.69 |
| RTG | 3.22 ± 1.46 | 2.50 ± 0.99 | 1.00 | 0.12 | Post | 0.08 | 0.40 | ||||||||||
| SDVAP (mm/s) | CG | 22.40 ± 6.86 | 25.80 ± 6.81 | 1.704 | 0.202 | 0.013 | 1.692 | 0.204 | 0.045 | 3.898 | 0.058 | 0.030 | 0.05 | 0.49 | Pre | 0.82 | 0.72 |
| RTG | 21.90 ± 4.17 | 21.20 ± 5.85 | 1.00 | 0.13 | Post | 0.06 | 0.09 | ||||||||||
| SDVML (mm/s) | CG | 24.30 ± 5.30 | 28.50 ± 6.79 | 1.291 | 0.266 | 0.016 | 0.002 | 0.966 | 0.000 | 3.217 | 0.084 | 0.039 | 0.17 | 0.68 | Pre | 0.56 | 0.37 |
| RTG | 26.90 ± 6.84 | 26.00 ± 6.42 | 1.00 | 0.14 | Post | 0.67 | 0.42 | ||||||||||
| PPPAP (a.u.) | CG | 23.10 ± 6.94 | 26.40 ± 6.84 | 1.557 | 0.222 | 0.011 | 1.475 | 0.235 | 0.040 | 4.23 | 0.049 | 0.030 | 0.04 | 0.48 | Pre | 1.00 | 0.70 |
| RTG | 22.8 ± 4.40 | 22.00 ± 6.01 | 1.00 | 0.15 | Post | 0.14 | 0.06 | ||||||||||
| PPPML (a.u.) | CG | 24.60 ± 5.30 | 29.00 ± 6.67 | 1.574 | 0.220 | 0.019 | 0.003 | 0.957 | 0.000 | 3.528 | 0.071 | 0.004 | 0.14 | 0.73 | Pre | 0.59 | 0.42 |
| RTG | 27.20 ± 6.83 | 26.30 ± 6.52 | 1.00 | 0.13 | Post | 0.56 | 0.40 | ||||||||||
| PPPAP-ML (a.u.) | CG | 34.50 ± 6.48 | 39.70 ± 6.66 | 1.725 | 0.200 | 0.023 | 0.685 | 0.415 | 0.016 | 3.482 | 0.073 | 0.045 | 0.12 | 0.79 | Pre | 1.00 | 0.65 |
| RTG | 35.80 ± 7.26 | 34.90 ± 8.01 | 1.00 | 0.12 | Post | 0.19 | 0.18 | ||||||||||
| MTV (mm/s) | CG | 29.00 ± 4.93 | 33.50 ± 5.49 | 1.520 | 0.228 | 0.024 | 0.438 | 0.514 | 0.009 | 2.893 | 0.100 | 0.044 | 0.15 | 0.85 | Pre | 1.00 | 0.59 |
| RTG | 30.50 ± 6.38 | 29.80 ± 6.81 | 1.00 | 0.11 | Post | 0.26 | 0.24 | ||||||||||
| ANOVA | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Time Effect | Group Effect | Time × Group Effect | |||||||||||||||
| Outcome | Group | Pre | Post | F | p | eta | F | p | eta | F | p | eta | Post Intr Padj | Post Intr ES (d) | Post M | Post Intr Pad | Post Intr ES (d) |
| SA (mm2) | CG | 6.34 ± 3.71 | 9.16 ± 6.85 | 7.106 | 0.013 | 0.039 | 0.710 | 0.407 | 0.024 | 0.559 | 0.462 | 0.003 | 0.10 | 0.51 | Pre | 1.00 | 0.23 |
| RTG | 5.25 ± 5.08 | 6.84 ± 5.81 | 0.29 | 0.29 | Post | 0.71 | 0.38 | ||||||||||
| TSD (mm) | CG | 992 ± 85.8 | 1134 ± 208 | 3.118 | 0.090 | 0.024 | 0.161 | 0.691 | 0.005 | 1.034 | 0.319 | 0.008 | 0.25 | 0.89 | Pre | 0.65 | 0.41 |
| RTG | 1085 ± 270 | 1123 ± 372 | 1.00 | 0.12 | Post | 1.00 | 0.03 | ||||||||||
| MAPD (mm) | CG | 2.22 ± 1.68 | 2.94 ± 1.77 | 6.786 | 0.015 | 0.031 | 0.033 | 0.857 | 0.001 | 0.662 | 0.423 | 0.003 | 0.15 | 0.57 | Pre | 1.00 | 0.05 |
| RTG | 2.14 ± 0.89 | 2.64 ± 1.99 | 0.28 | 0.23 | Post | 1.00 | 0.16 | ||||||||||
| MMLD (mm) | CG | 6.22 ± 2.72 | 4.34 ± 1.98 | 1.559 | 0.223 | 0.006 | 0.582 | 0.452 | 0.019 | 0.304 | 0.586 | 0.001 | 0.95 | 0.08 | Pre | 0.70 | 0.36 |
| RTG | 5.16 ± 3.03 | 3.94 ± 1.68 | 0.46 | 0.21 | Post | 1.00 | 0.20 | ||||||||||
| SDVML (mm/s) | CG | 26.30 ± 4.47 | 31.00 ± 7.00 | 2.669 | 0.115 | 0.027 | 0.167 | 0.687 | 0.005 | 4.524 | 0.043 | 0.045 | 0.17 | 0.80 | Pre | 0.83 | 0.51 |
| RTG | 28.10 ± 6.19 | 27.50 ± 6.74 | 1.00 | 0.10 | Post | 0.40 | 0.32 | ||||||||||
| PPPAP (a.u.) | CG | 29.40 ± 7.89 | 32.70 ± 10.2 | 5.823 | 0.023 | 0.019 | 0.402 | 0.532 | 0.015 | 0.316 | 0.579 | 0.001 | 0.02 | 0.37 | Pre | 1.00 | 0.21 |
| RTG | 27.70 ± 8.03 | 29.70 ± 11.4 | 0.42 | 0.21 | Post | 1.00 | 0.27 | ||||||||||
| PPPML (a.u.) | CG | 26.70 ± 4.69 | 31.50 ± 6.88 | 2.961 | 0.098 | 0.030 | 0.261 | 0.614 | 0.008 | 4.559 | 0.043 | 0.045 | 0.16 | 0.82 | Pre | 0.96 | 0.28 |
| RTG | 28.30 ± 6.19 | 27.70 ± 6.70 | 1.00 | 0.08 | Post | 0.34 | 0.55 | ||||||||||
| PPPAP-ML (a.u.) | CG | 41.10 ± 6.93 | 46.70 ± 9.67 | 3.120 | 0.090 | 0.024 | 0.390 | 0.538 | 0.012 | 1.961 | 0.174 | 0.015 | 0.17 | 0.67 | Pre | 1.00 | 0.02 |
| RTG | 41.30 ± 9.96 | 42.00 ± 12.1 | 1.00 | 0.06 | Post | 0.60 | 0.42 | ||||||||||
| MTV (mm/s) | CG | 34.60 ± 5.53 | 39.10 ± 8.02 | 2.490 | 0.127 | 0.020 | 0.227 | 0.638 | 0.007 | 1.988 | 0.171 | 0.016 | 0.21 | 0.65 | Pre | 1.00 | 0.09 |
| RTG | 35.30 ± 8.45 | 35.60 ± 9.66 | 1.00 | 0.03 | Post | 0.68 | 0.39 | ||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andreu-Caravaca, L.; Ramos-Campo, D.J.; Manonelles, P.; Chung, L.H.; Ramallo, S.; Rubio-Arias, J.Á. The Impact of Resistance Training Program on Static Balance in Multiple Sclerosis Population: A Randomized Controlled Trial Study. J. Clin. Med. 2022, 11, 2405. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11092405
Andreu-Caravaca L, Ramos-Campo DJ, Manonelles P, Chung LH, Ramallo S, Rubio-Arias JÁ. The Impact of Resistance Training Program on Static Balance in Multiple Sclerosis Population: A Randomized Controlled Trial Study. Journal of Clinical Medicine. 2022; 11(9):2405. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11092405
Chicago/Turabian StyleAndreu-Caravaca, Luis, Domingo J. Ramos-Campo, Pedro Manonelles, Linda H. Chung, Salvador Ramallo, and Jacobo Á. Rubio-Arias. 2022. "The Impact of Resistance Training Program on Static Balance in Multiple Sclerosis Population: A Randomized Controlled Trial Study" Journal of Clinical Medicine 11, no. 9: 2405. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11092405