
Suppression Head Impulse Test (SHIMP) versus Head Impulse Test (HIMP) When Diagnosing Bilateral Vestibulopathy

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Population
Study Design
2.2. Experimental Setup
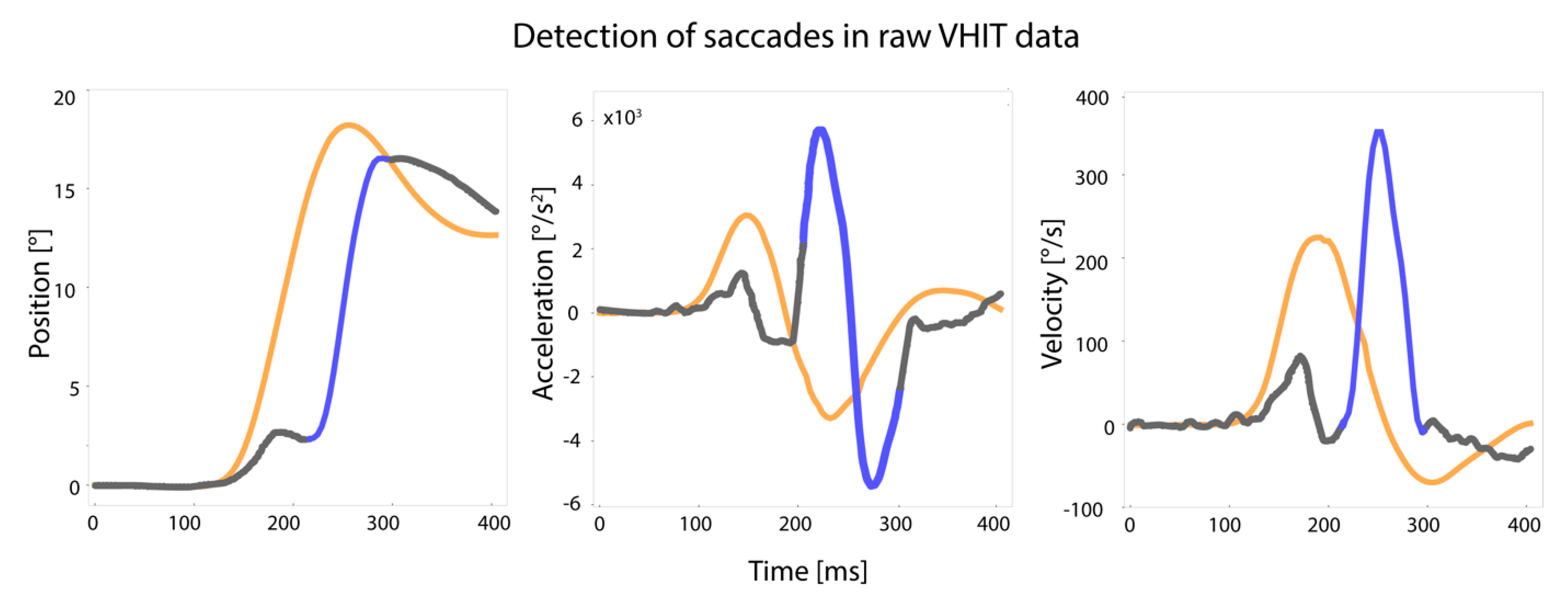
2.3. Saccades
2.3.1. Saccade Detection
2.3.2. Presence of Covert Saccades
2.3.3. Latency of Saccades
2.4. VOR Gain
2.5. Statistical Analysis
2.5.1. Statistical Analysis of Saccades
Covert Saccades
Latency of First Saccade (Covert and/or Overt)
2.5.2. Statistical Analysis of VOR Gain
2.5.3. Statistical Analysis of Peak Head Velocity
2.5.4. Analysis of Agreement between HIMP and SHIMP Regarding BV Diagnosis
2.6. Ethical Considerations
3. Results
3.1. Patient Characteristics
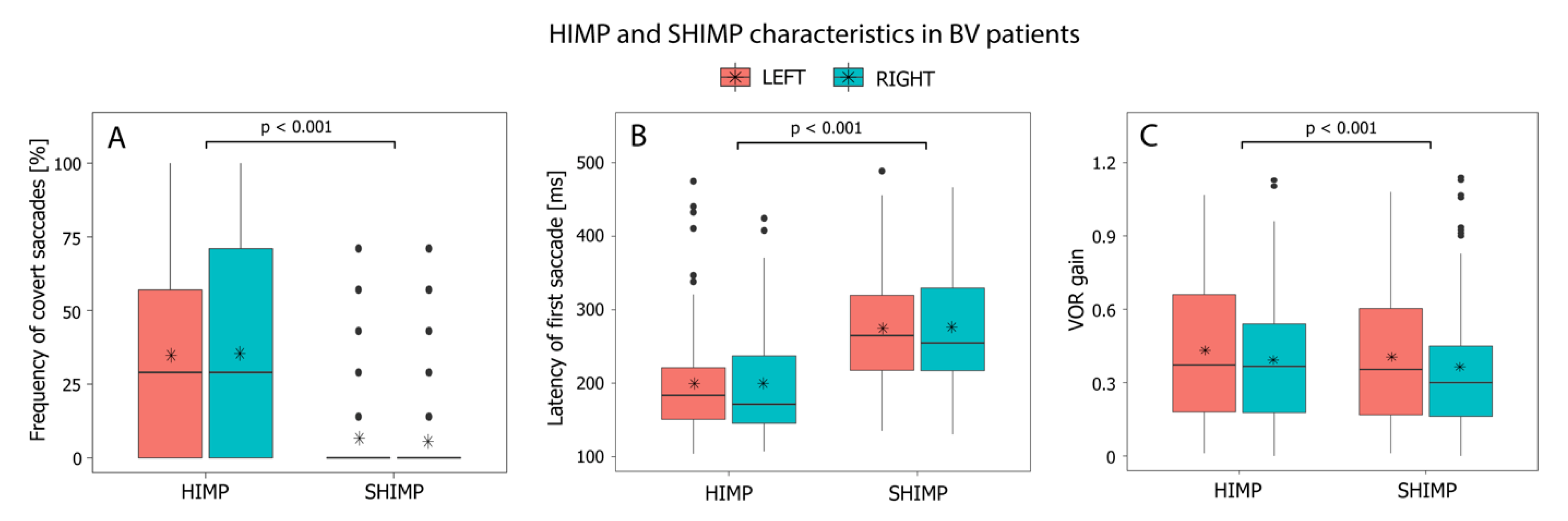
3.2. HIMP versus SHIMP: Presence of Covert Saccades
3.3. HIMP versus SHIMP: Latency of the First Saccade (Covert and/or Overt)
3.4. HIMP versus SHIMP: VOR Gain Differences

3.5. HIMP versus SHIMP: Peak Head Velocity
3.6. Analysis of Agreement between HIMP and SHIMP Regarding BV Diagnosis
4. Discussion
4.1. HIMP versus SHIMP: Covert Saccades
4.2. HIMP versus SHIMP: VOR Gain
4.3. HIMP versus SHIMP: Agreement on the Diagnosis of BV
4.4. HIMP versus SHIMP: The Daily Practice
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Halmagyi, G.M.; Curthoys, I.S. A clinical sign of canal paresis. Arch. Neurol. 1988, 45, 737–739. [Google Scholar] [CrossRef] [PubMed]
- van de Berg, R.; Rosengren, S.; Kingma, H. Laboratory examinations for the vestibular system. Curr. Opin. Neurol. 2018, 31, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Halmagyi, G.M.; Chen, L.; MacDougall, H.G.; Weber, K.P.; McGarvie, L.A.; Curthoys, I.S. The Video Head Impulse Test. Front. Neurol. 2017, 8, 258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strupp, M.; Kim, J.-S.; Murofushi, T.; Straumann, D.; Jen, J.C.; Rosengren, S.M.; Della Santina, C.C.; Kingma, H. Bilateral vestibulopathy: Diagnostic criteria Consensus document of the Classification Committee of the Barany Society. J. Vestib. Res. 2017, 27, 177–189. [Google Scholar] [CrossRef] [Green Version]
- van de Berg, R.; van Tilburg, M.; Kingma, H. Bilateral Vestibular Hypofunction: Challenges in Establishing the Diagnosis in Adults. ORL J. Otorhinolaryngol. Relat. Spec. 2015, 77, 197–218. [Google Scholar] [CrossRef]
- Macdougall, H.G.; McGarvie, L.A.; Halmagyi, G.M.; Curthoys, I.S.; Weber, K.P. The video Head Impulse Test (vHIT) detects vertical semicircular canal dysfunction. PLoS ONE 2013, 8, e61488. [Google Scholar] [CrossRef]
- MacDougall, H.G.; McGarvie, L.A.; Halmagyi, G.M.; Rogers, S.J.; Manzari, L.; Burgess, A.M.; Curthoys, I.S.; Weber, K.P. A new saccadic indicator of peripheral vestibular function based on the video head impulse test. Neurology 2016, 87, 410–418. [Google Scholar] [CrossRef] [Green Version]
- Starkov, D.; Vermorken, B.; Van Dooren, T.S.; Van Stiphout, L.; Janssen, M.; Pleshkov, M.; Guinand, N.; Fornos, A.P.; Van Rompaey, V.; Kingma, H.; et al. The Effect of Different Head Movement Paradigms on Vestibulo-Ocular Reflex Gain and Saccadic Eye Responses in the Suppression Head Impulse Test in Healthy Adult Volunteers. Front. Neurol. 2021, 12, 729081. [Google Scholar] [CrossRef]
- Rey-Martinez, J.; Thomas, I.; Espinosa-Sanchez, J.M.; Caletrio, A.B.; Trinidad-Ruiz, G.; Matiño-Soler, E.; Perez-Fernandez, N. Vestibulo-ocular reflex gain values in the suppression head impulse test of healthy subjects. Laryngoscope 2018, 128, 2383–2389. [Google Scholar] [CrossRef]
- Crane, B.T.; Demer, J.L. Latency of voluntary cancellation of the human vestibulo-ocular reflex during transient yaw rotation. Exp. Brain Res. 1999, 127, 67–74. [Google Scholar] [CrossRef]
- van Dooren, T.S.; Lucieer, F.; Janssen, A.; Kingma, H.; van de Berg, R. The Video Head Impulse Test and the Influence of Daily Use of Spectacles to Correct a Refractive Error. Front. Neurol. 2018, 9, 125. [Google Scholar] [CrossRef] [Green Version]
- Mantokoudis, G.; Tehrani, A.S.S.; Kattah, J.C.; Eibenberger, K.; Guede, C.I.; Zee, D.S.; Newman-Toker, D.E. Quantifying the vestibulo-ocular reflex with video-oculography: Nature and frequency of artifacts. Audiol. Neurootol. 2015, 20, 39–50. [Google Scholar] [CrossRef] [Green Version]
- Castro, P.; Esteves, S.S.; Lerchundi, F.; Buckwell, D.; Gresty, M.A.; Bronstein, A.M.; Arshad, Q. Viewing Target Distance Influences the Vestibulo-Ocular Reflex Gain when Assessed Using the Video Head Impulse Test. Audiol. Neurootol. 2018, 23, 285–289. [Google Scholar] [CrossRef]
- Rey-Martinez, J.; Yanes, J.; Esteban, J.; Sanz, R.; Martin-Sanz, E. The Role of Predictability in Saccadic Eye Responses in the Suppression Head Impulse Test of Horizontal Semicircular Canal Function. Front. Neurol. 2017, 8, 536. [Google Scholar] [CrossRef] [Green Version]
- Mantokoudis, G.; Tehrani, A.S.S.; Schubert, M.C.; Wong, A.; Agrawal, Y.; Xie, L.; Newman-Toker, D.E. Compensatory saccades benefit from prediction during head impulse testing in early recovery from vestibular deafferentation. Eur. Arch. Otorhinolaryngol. 2016, 273, 1379–1385. [Google Scholar] [CrossRef]
- van Dooren, T.S.; Starkov, D.; Lucieer, F.M.P.; Vermorken, B.; Janssen, A.M.L.; Guinand, N.; Pérez-Fornos, A.; Van Rompaey, V.; Kingma, H.; van de Berg, R. Comparison of three video head impulse test systems for the diagnosis of bilateral vestibulopathy. J. Neurol. 2020, 267 (Suppl. 1), 256–264. [Google Scholar] [CrossRef]
- Cleworth, T.W.; Carpenter, M.G.; Honegger, F.; Allum, J.H. Differences in head impulse test results due to analysis techniques. J. Vestib. Res. 2017, 27, 163–172. [Google Scholar] [CrossRef]
- Wenzel, A.; Hülse, R.; Thunsdorff, C.; Rotter, N.; Curthoys, I. Reducing the number of impulses in video head impulse testing—It’s the quality not the numbers. Int. J. Pediatr. Otorhinolaryngol. 2019, 125, 206–211. [Google Scholar] [CrossRef]
- Park, J.S.; Lee, J.-Y.; Nam, W.; Noh, S.; Chang, S.O.; Kim, M.-B. Comparing the Suppression Head Impulse Paradigm and the Head Impulse Paradigm in Vestibular Neuritis. Otol. Neurotol. 2020, 41, e76–e82. [Google Scholar] [CrossRef]
- Devantier, L.; Hoskison, E.; Ovesen, T.; Henriksen, J.-J.M. Suppression head impulse paradigm in healthy adolescents—A novel variant of the head impulse test. J. Vestib. Res. 2018, 28, 311–317. [Google Scholar] [CrossRef]
- Maheu, M.; Behtani, L.; Nooristani, M.; Delcenserie, A.; Champoux, F. Enhanced vestibulo-ocular reflex suppression in dancers during passive high-velocity head impulses. Exp. Brain Res. 2019, 237, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.S.; Lim, H.W.; Yang, C.J.; Kim, Y.H.; Choi, W.R.; Kim, Y.R.; Park, J.W.; Kang, B.C.; Park, H.J. Changes of video head impulse test results in lateral semicircular canal plane by different peak head velocities in patients with vestibular neuritis. Acta Otolaryngol. 2018, 138, 785–789. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.K.; Hougaard, D.D. Suppression head impulse testing is recommended for vestibular testing of patients with untreated unilateral vestibular schwannoma. Eur. Arch. Otorhinolaryngol. 2021, 279, 91–99. [Google Scholar] [CrossRef] [PubMed]
- van de Berg, R.; Ramos, A.; Van Rompaey, V.; Bisdorff, A.; Perez-Fornos, A.; Rubinstein, J.T.; Phillips, J.O.; Strupp, M.; Della Santina, C.C.; Guinand, N. The vestibular implant: Opinion statement on implantation criteria for research. J. Vestib. Res. 2020, 30, 213–223. [Google Scholar] [CrossRef]
- D’Albora, R.; Noboa, R.; Gutman, M.C.; Fuentes, S.F.; Palazón, C.V.A.; Silveira, L.; Moreno, C.A.F.; Monaco, M.J.; Zalazar, G.J.; Carmona, S. Clinical Testing of Head Impulse Paradigm and Suppression Head Impulse Paradigm Using a Diagnostic Headband: Combined Clinical Sign for Improved Performance. Otol. Neurotol. 2021, 43, e268–e273. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| 1a. Diagnosis According to VHIT Results (n = 92) | HIMP (Cut-Off < 0.6) | SHIMP (Cut-Off < 0.6) | SHIMP (Cut-Off < 0.5) |
|---|---|---|---|
| Bilateral vestibulopathy | |||
| VOR gain <0.6 on both sides | 64 | 70 | 65 |
| No bilateral vestibulopathy | |||
| VOR gain >0.6 on both sides | 10 | 9 | 14 |
| VOR gain >0.6 on one side | 18 | 13 | 13 |
| 1b. Agreement on the Diagnosis of BV between HIMP and SHIMP | |||
| HIMP (cut-off < 0.6) and SHIMP (cut-off < 0.6) | 93% | ||
| HIMP (cut-off < 0.6) and SHIMP (cut-off < 0.5) | 97% | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Dooren, T.; Starkov, D.; Lucieer, F.; Dobbels, B.; Janssen, M.; Guinand, N.; Pérez Fornos, A.; Kingma, H.; Van Rompaey, V.; van de Berg, R. Suppression Head Impulse Test (SHIMP) versus Head Impulse Test (HIMP) When Diagnosing Bilateral Vestibulopathy. J. Clin. Med. 2022, 11, 2444. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11092444
van Dooren T, Starkov D, Lucieer F, Dobbels B, Janssen M, Guinand N, Pérez Fornos A, Kingma H, Van Rompaey V, van de Berg R. Suppression Head Impulse Test (SHIMP) versus Head Impulse Test (HIMP) When Diagnosing Bilateral Vestibulopathy. Journal of Clinical Medicine. 2022; 11(9):2444. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11092444
Chicago/Turabian Stylevan Dooren, Tessa, Dmitrii Starkov, Florence Lucieer, Bieke Dobbels, Miranda Janssen, Nils Guinand, Angelica Pérez Fornos, Herman Kingma, Vincent Van Rompaey, and Raymond van de Berg. 2022. "Suppression Head Impulse Test (SHIMP) versus Head Impulse Test (HIMP) When Diagnosing Bilateral Vestibulopathy" Journal of Clinical Medicine 11, no. 9: 2444. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11092444