1. Introduction
At the beginning of 2021, the successful vaccine campaign against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) started, offering protection against hospitalization and death from coronavirus disease 2019 (COVID-19) for most patient groups, irrespective of emerging variants [
1]. Despite this success in the general population, solid organ transplant (SOT) recipients had a poor response to vaccination and a limited benefit from the initially recommended two vaccinations [
2]. At the same time, the mortality of SOT recipients acquiring COVID-19 is unacceptably high, with rates up to 20% reported in registries [
3,
4]. Recent data from the United Kingdom collected between September 2020 and August 2021 show an unadjusted COVID-19 case fatality rate of 9.8% in SOT. The vaccination with two doses did not prevent infections in SOT recipients and increased 28-day survival in COVID-19 infected SOTs only marginally from 88.8% to 91.8%. This is equivalent to a 20% reduction in risk of death in vaccinated SOT recipients, as compared to a 68-fold reduction of death in the general population [
5].
Early in 2021, it was recognized that SOT, and especially kidney transplant recipients (KTR), show a diminished serological response compared to healthy individuals and hemodialysis patients [
6,
7,
8]. Subsequent studies revealed that the level of antibodies correlates with protection from disease [
9,
10], arguing for serological response controls in SOT recipients.
After three vaccinations, which were early recommended for SOT recipients and later for the general population, serological vaccine response was inadequately low in at least 40% [
11]. T cell response over time only changes at a functional level, never reaching the level of healthy individuals [
12,
13]. In summary, the poor T cell response in combination with an impaired humoral response offered only a limited protection from infection and a severe course of COVID-19 [
14]. Consistent with the observation that mycophenolic acid treatment impairs B-cell proliferation and plasmablast proliferation, experimental data have suggested that a short-term MPA pause can improve serological response to the fourth dose of the SARS-CoV-2 vaccination [
13].
The question therefore arises about optimal management of non-responding patients, and, in particular, whether repeated vaccinations increase cumulative serological response rates. In the current study, we provide the first systematic investigation analyzing the serological response to up to five repeated vaccinations against SARS-CoV-2 in non-responding COVID-19-naïve KTR. In particular, we report the response rates of KTR after basic immunization, three, four, and five vaccinations, and the predictors of serological response after three and four vaccinations as well as the effects of different immunosuppressive reduction regimes on the serological response.
3. Outcome
The primary outcome was serological response to immunization, defined as the maximum serological response after a minimum of 14 days after each immunization, i.e., after basic immunization, three, four, and five doses of SARS-CoV-2 vaccines.
We used an anti-SARS-CoV-2 enzyme-linked immunosorbent assays (ELISA) for the detection of IgG antibodies against the S1 domain of the SARS-CoV-2 spike (S) protein in serum according to the instructions of the manufacturer (Anti-SARS-CoV-2-ELISA (IgG), EUROIMMUN Medizinische Labordiagnostika AG, Lübeck, Germany) [
15,
16]. Processing and measurement were done using the fully automated “Immunomat” (Institut Virion\Serion GmbH, Würzburg, Germany). Results were determined by comparing the obtained signals of the patient samples with the previously obtained cut-off value of the calibrator. As suggested by the manufacturer, samples with a cut-off index ≥ 1.1 were considered to be positive. Alternatively, the electrochemiluminescence immunoassay (ECLIA, Elecsys, Anti-SARS-CoV-2, Roche Diagnostics GmbH, Mannheim, Germany) was used either alone or in parallel detecting human immunoglobulins, including IgG, IgA, and IgM against the spike receptor binding (RBD) domain protein. Results were determined by comparing the obtained signals of the patient samples with the previously obtained cut-off value of the calibrator. As suggested by the manufacturer, samples with a cut-off index ≥ 264 U/mL were considered to be positive as recommended by Caillard et al. [
17].
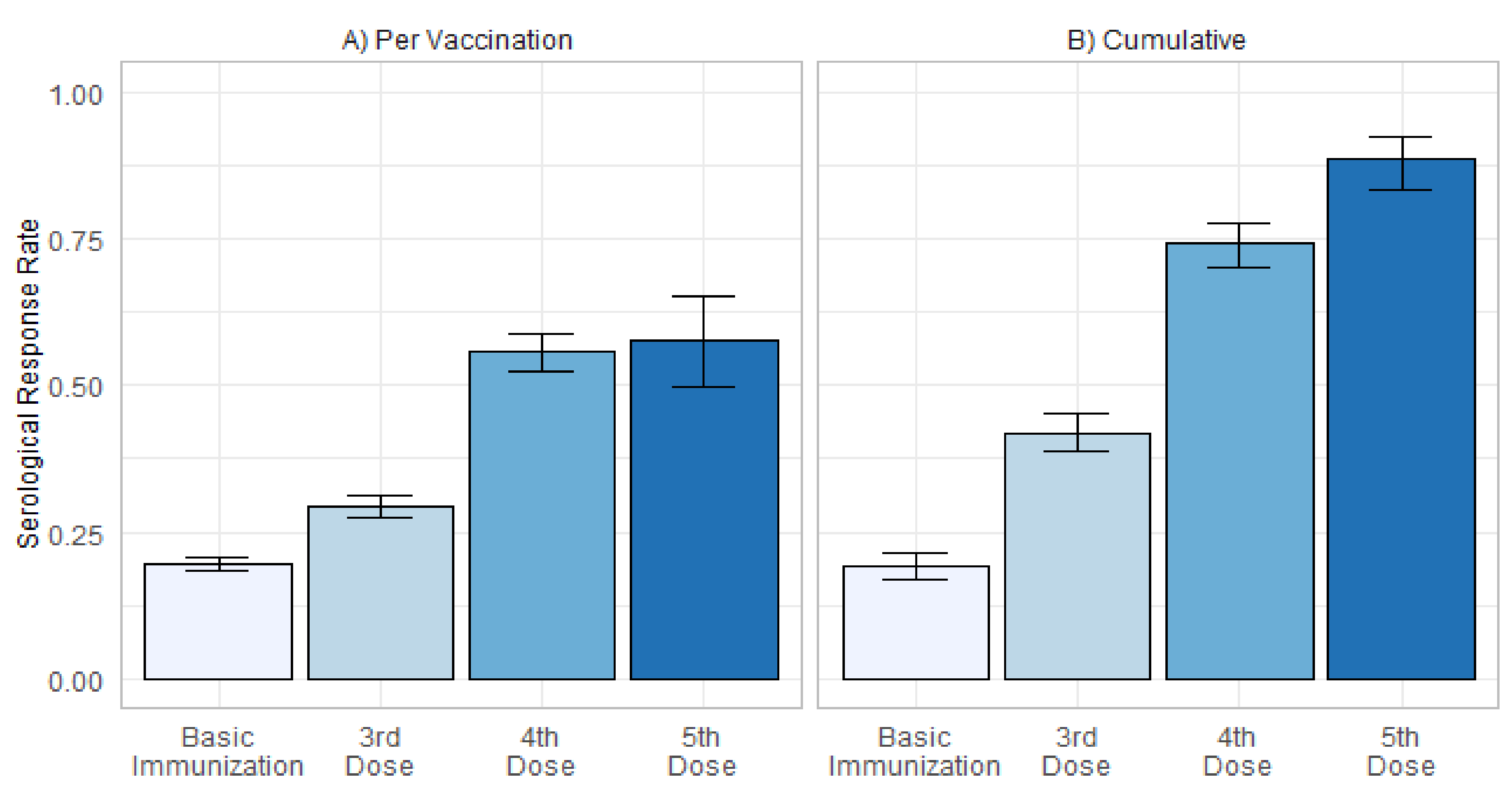
Any non-negative titer below the cut-off in each test was defined as low-positive. Accordingly, response to immunization was categorized as a sufficient serological response (responders) in the case of a positive SARS-CoV-2 antibody titer or as an insufficient serological response (non-responders) in case of a negative or low-positive SARS-CoV-2 antibody titer. The serological response rate was calculated as the rate of responders after each basic immunization, three, four, and five doses.
In order to exclude patients with a history of COVID-19, we simultaneously measured antibodies against the nucleocapsid (N) protein with an electrochemiluminescence immunoassay (ECLIA, Elecsys Anti-SARS-CoV-2, Roche Diagnostics GmbH). As before, results were determined by comparing the obtained signals of the patient samples with the previously obtained cut-off value of the calibrator. As suggested by the manufacturer, samples with a cut-off index ≥ 1.0 were considered to be positive.
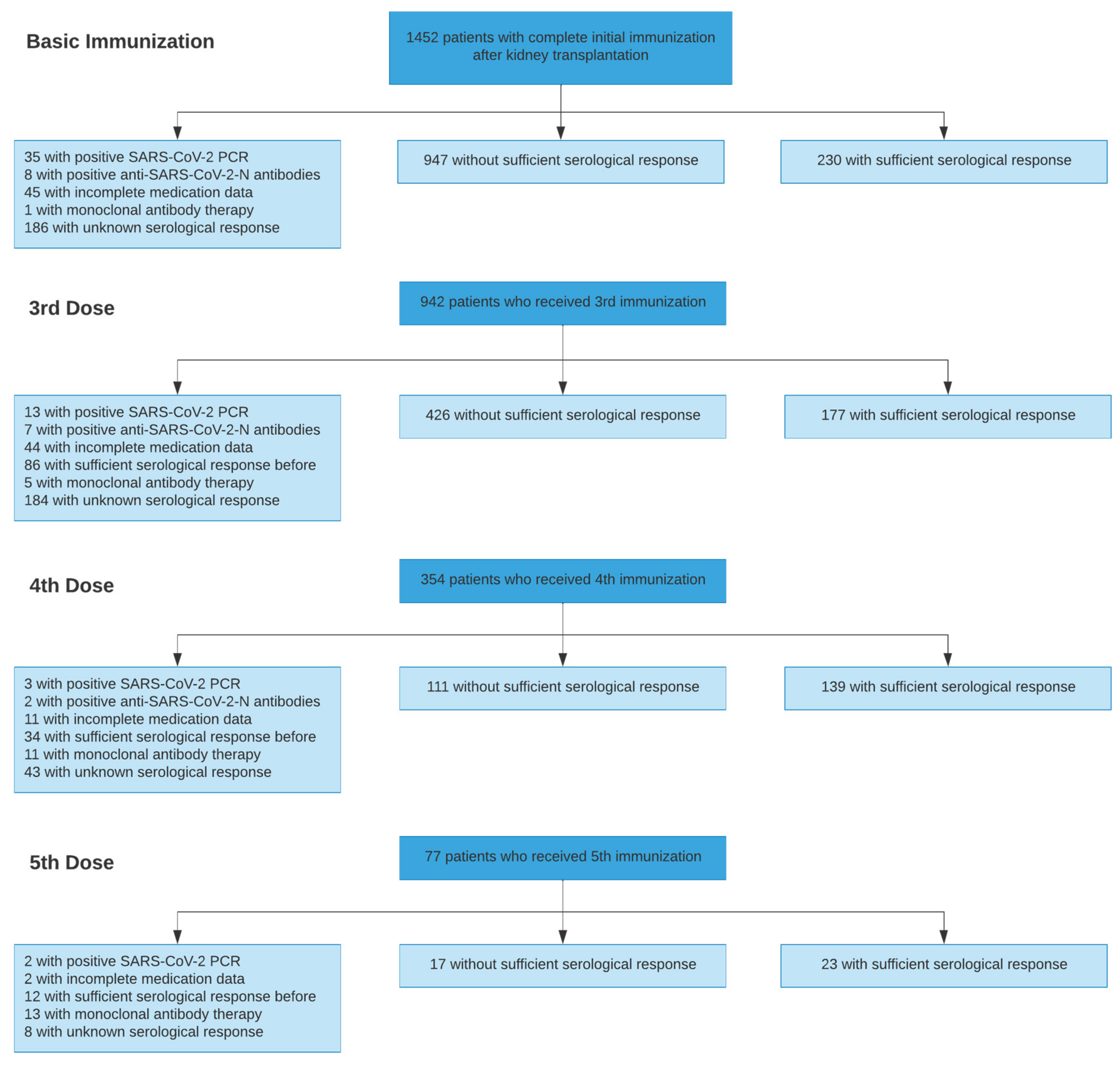
We included immunization from all adult KTR at our institution within the study period. Immunizations were excluded from analysis when they occurred before transplantation, when no medication data were available, or in case of ineligible serological data (see
Table 1). The latter occurred if patients received additional vaccination doses without the assessment of the SARS-CoV-2 IgG titer before and after, mostly when performed outside the transplant center.
The cumulative serological response was calculated using the Kaplan–Meier method with the number of vaccinations as the time variable and the first positive serological response as the event of interest. Patients, who remained sustained non-responders after their last vaccination, were treated as censored at this point [
18].
3.1. Multivariable Analysis of Predictors of Serological Response
The influence of 8 variables on the primary outcome after the third vaccination dose and the influence of 5 variables on the primary outcome after the fourth vaccination dose were examined in two separate multivariable analyses using logistic regression. Candidate variables included basic patient demographics, transplantation data, vaccination characteristics, the latest immunosuppressive medication, and routine laboratory parameters (detailed variable definition provided in
Table S1). Immunizations with missing candidate variable data were excluded from multivariable analysis. No imputation methods were used. Adjusted p-values according to Holm’s correction for multiple comparisons are reported.
Since not all patients received calcineurin inhibitors (CNI), the influence on CNI through levels on serological response rate was studied in two separate multivariable analyses, which included % deviance from the target CNI-through level (6 ng/mL for tacrolimus, and 80 ng/mL for cyclosporine) as an additional predictor variable [
19].
3.2. Comparison of Mycophenolic Acid (MPA) Dose Adjustment Regimens
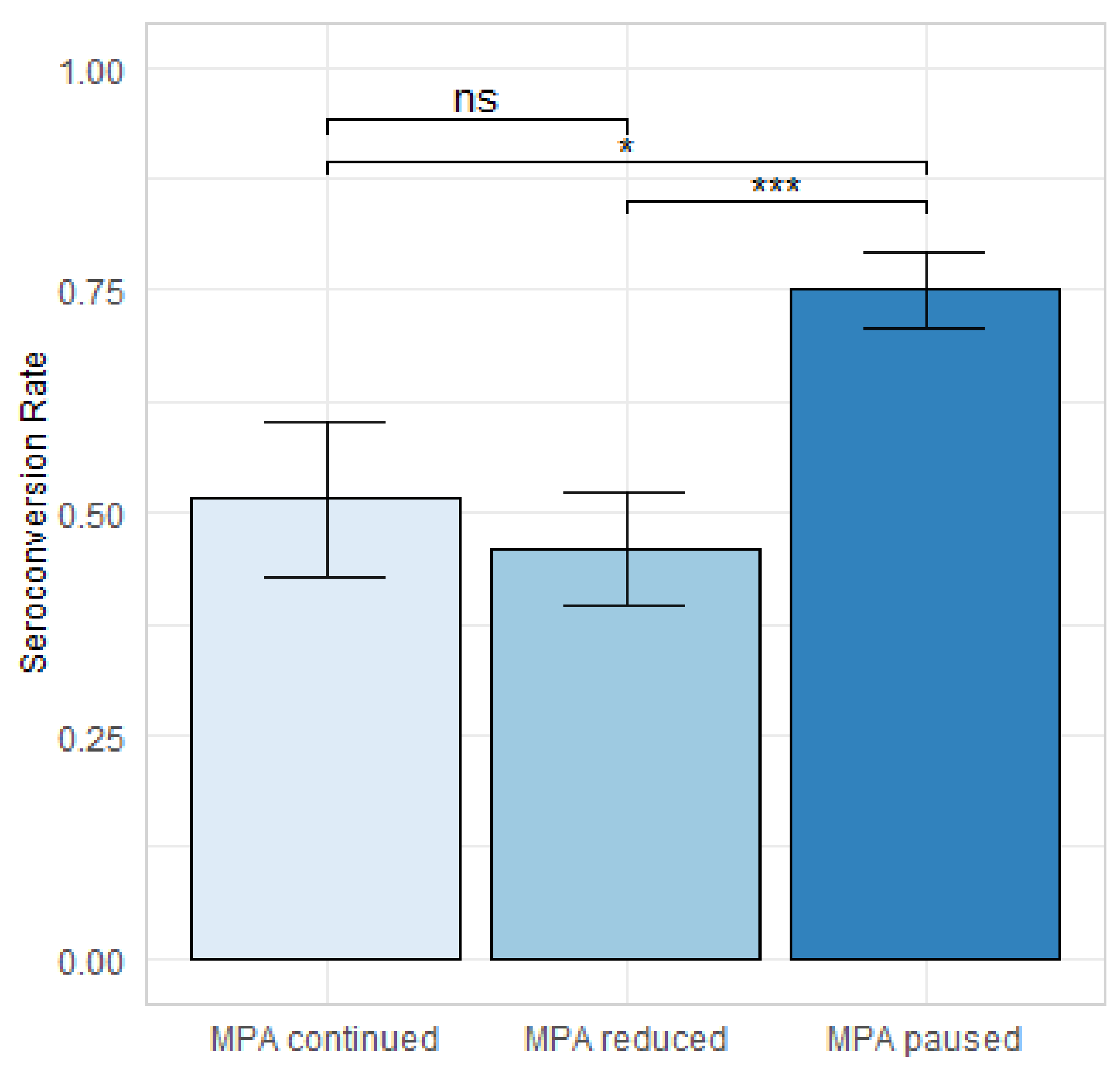
Due to the important role of MPA with regard to the response to immunization, different approaches for MPA dose adjustment before fourth SARS-CoV-2 immunization were followed at our institution according to the patients’ individual risk factors, such as previous rejection episodes, anti-HLA antibodies, previous response to SARS-CoV-2 immunization, and based on the physicians’ and patients’ shared-decision making. In CNI-treated patients, MPA was reduced (reduction of 25–50% compared to the maintenance dose) or paused from one week before immunization until four weeks after immunization. Steroids were maintained at 5 mg prednisolone equivalent. In case of steroid-free treatment, 5 mg prednisolone equivalent was added for the time of MPA reduction, which was discontinued after restart of MPA.
To examine MPA related effects, patients on CNI-based immunosuppression receiving a fourth dose of a SARS-CoV-2 vaccine were assigned to three groups according to their change in MPA dose in relation to the MPA dose before their third SARS-CoV-2 vaccination: (1) steady MPA dose, (2) reduced MPA dose, and (3) paused MPA. Serological response rates between the 3 groups were compared using the Kruskal–Wallis test, and pairwise comparisons were performed using Mann–Whitey U test with Holm’s correction for multiple comparisons.
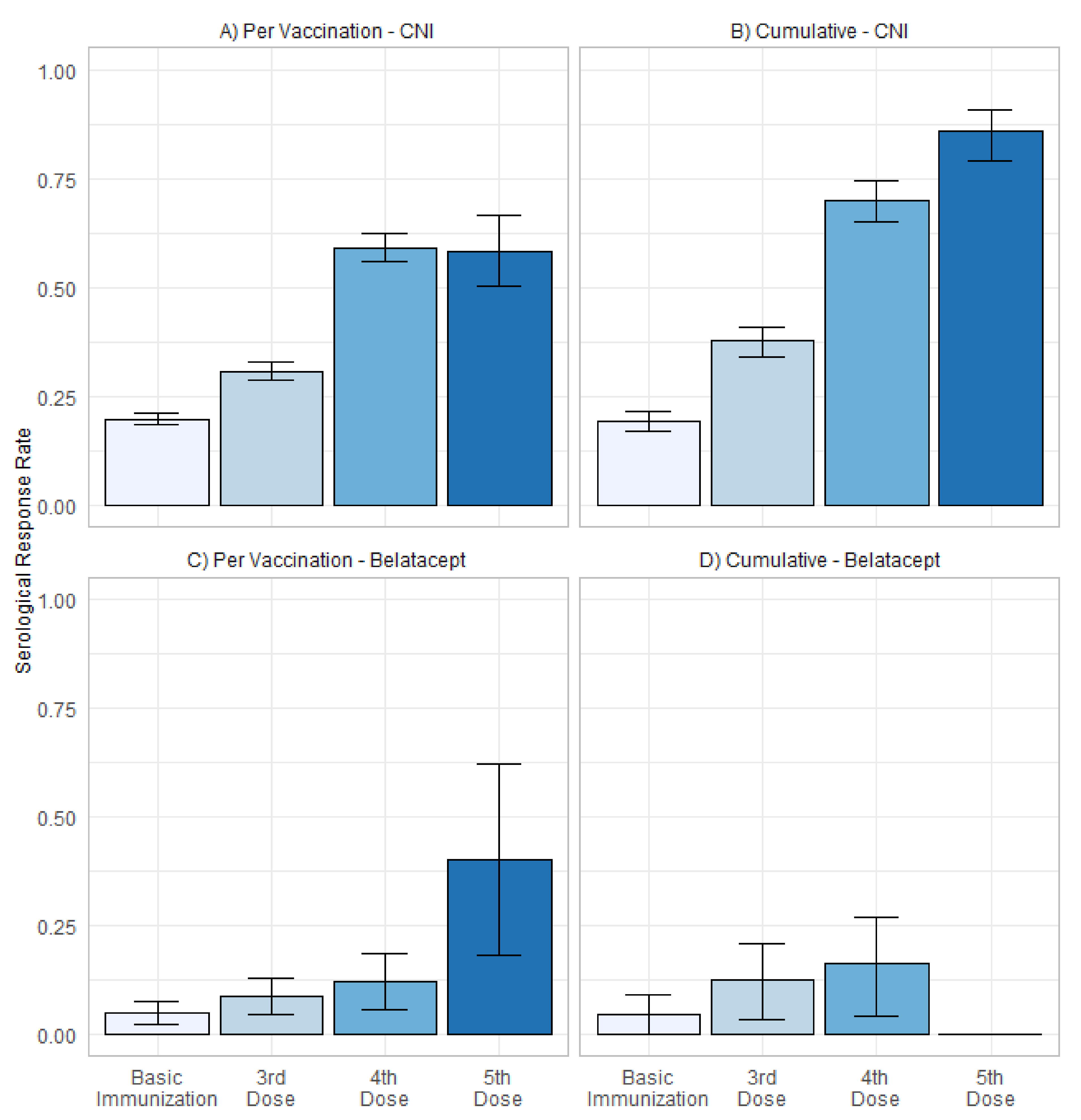
3.3. Serological Response in Patients with CNI and Belatacept Maintenance Immunosuppression
The serological response rate in patients on CNI-based as well as belatacept-based immunosuppression was calculated separately. Additionally, the cumulative serological response rate was described as stated above. For patients with belatacept-based immunosuppression, no cumulative serological response rate is shown after 5 vaccinations, due to the low patient count in this group. Serological responders receiving belatacept-based immunosuppression were further analyzed on the patient-level.
Statistical analysis was performed using R studio v.1.2.5042 (Boston, MA, USA) and R version 4.0.2 (Vienna, Austria) (22 June 2020).
5. Discussion
We provide the first systematic investigation analyzing the serological response to up to five repeated vaccinations against SARS-CoV-2 in a closely monitored cohort of adult KTR. This includes the largest reported cohort of KTR receiving four doses as well as the first reported cohort of KTR receiving five doses of a SARS-CoV-2 vaccine.
Our data indicate that repeated vaccination of up to five times is safe and induces sufficient serological response in patients who did not respond after two or three vaccinations and achieves satisfactory antibody titers in most patients.
Contrary to other previously reported case series that supported the administration of a fourth dose of vaccine [
20,
21], we were able to also compare different approaches to the reduction of immunosuppression and their effects on serological response. In CNI-treated non-responders after three vaccinations, serological response was improved by pausing MPA and adding 5 mg prednisolone equivalent for 4 to 8 weeks at the time of fourth vaccination. A mere partial reduction of MPA, however, did not lead to an improved response rate.
In patients treated with belatacept, additional immunizations have only a limited effect on a serological response, in particular, if treated with full-dose MPA—a result that complements previous descriptions of poor serological response to three doses of vaccine in KTR under belatacept immunosuppression [
22,
23]. It is obvious that these patients require different approaches.
We were able to show that several factors reported to affect the response to basic immunization against SARS-CoV-2 are also predictors of serological response after three and four doses of the vaccine [
24,
25]. Multivariable analysis revealed that MPA dose and belatacept treatment are the most important modifiable risk factors of impaired serological response, while non-modifiable factors include younger age, higher BMI, and years after transplantation. These observations are consistent with the concept that increased immunosenescence in elderly individuals leads to a diminished vaccine response in general [
26,
27,
28], and especially in KTR [
24,
25,
26,
27,
28,
29]. A longer time after transplantation goes along with a general reduction of immunosuppression from waning steroids over a reduction in CNI levels [
30]. Conflicting data exist concerning the BMI of patients. On the one hand, it has been shown that convalescent plasma donors with higher BMI had higher and more stable antibody titers [
31], while a direct impact of BMI on serological response has not been constantly reported [
32,
33].
We believe that this analysis has several important implications. First, the observation that patients with CNI and MPA based maintenance immunosuppression are likely to develop a serological response after four or five SARS-CoV-2 vaccines suggests that repeated vaccination is an alternative immunization strategy to the administration of monoclonal antibodies in non-responders after 3 vaccinations, with the latter being performed by several transplant centers. Second, serological response can be improved by pausing MPA and adding 5 mg prednisolone equivalent 1 week before until 4 weeks after vaccination without increased short-term risk of rejection.
Still, anti-HLA antibody development may occur with time delay in a low percentage and has to be weighed against the benefit of protection from a potentially life-threatening disease. As a consequence, we recommend close monitoring after temporary change of immunosuppression.
Third, patients receiving belatacept are likely to be sustained non-responders even after five vaccinations. For these patients, the optimal strategy to prevent severe COVID-19 has to be defined. We advocate for pre-exposure prophylaxis with monoclonal anti-S-protein antibodies for non-responders after three vaccines who receive belatacept treatment. Switching from belatacept to a CNI-based regimen is another option, but the effect of belatacept lasts two to three months after cessation. Since some patients receive belatacept as a rescue therapy in case of poor graft function (e.g., due to CNI toxicity or thrombotic microangiopathy), the optimal strategy for belatacept-treated patients remains a challenge. Other concepts might include a pill-in-the-pocket concept using nirmatrelvir/ritonavir for early treatment after exposure. This needs to be performed under dose adaption or pause of CNI and close monitoring of CNI levels. Alternatively, early treatment with remdesevir or post-exposure prophylaxis with monoclonal antibodies are more widely available alternatives.
Limitations arise from the study’s retrospective design, which in combination with the large cohort size, did not enable complete follow-up for every patient. Hence, patients with incomplete medication data were excluded from all analyses, since these patients are not regularly followed up at our transplant center, and their records are prone to incomplete and erroneous data, including that about vaccination and serological outcome. While serological measurements were routinely performed at our institution, there was a considerable number of vaccinations that were not preceded or followed by serological measurements (
Figure 1). Consequently, a patient-based approach was discarded in favor of a vaccination-based evaluation, introducing a risk of selection bias. However, our approach allows us to account for the incompleteness of the data and to optimize the number of examinable vaccinations. Intraindividual changes of titers between or after vaccinations were not represented with this approach, whereas protection after vaccination will evolve and might effectively decrease over time.
With regard to the effects of MPA dose adjustment around the fourth vaccination, the retrospective assignment to treatment groups limits the validity of the results because the groups were not fully matched and confounding factors could have influenced the group assignment. Nevertheless, comparison of the major potential influencing factors was provided to account for these risks.
Finally, while this study focuses on vaccine-induced humoral response as correlate of protection from disease, there are other contributors to immunity, such as T cell response, that may influence the degree of protection.
In conclusion, repeated vaccination against SARS-CoV-2 of up to five times effectively induces humoral serological response in kidney transplant recipients. Serological response can be enhanced by pausing MPA at the time of vaccination without increased short-term risk of acute rejection. Patients with belatacept immunosuppression and full-dose MPA are unlikely to achieve a sufficient serological response, thus requiring a different approach to ensure protection for this population at-risk.


 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}