
Post Penetrating Keratoplasty Ectasia: Incidence, Risk Factors, Clinical Features, and Treatment Options


Abstract
:1. Introduction
2. Clinical Features and Visual Disturbances
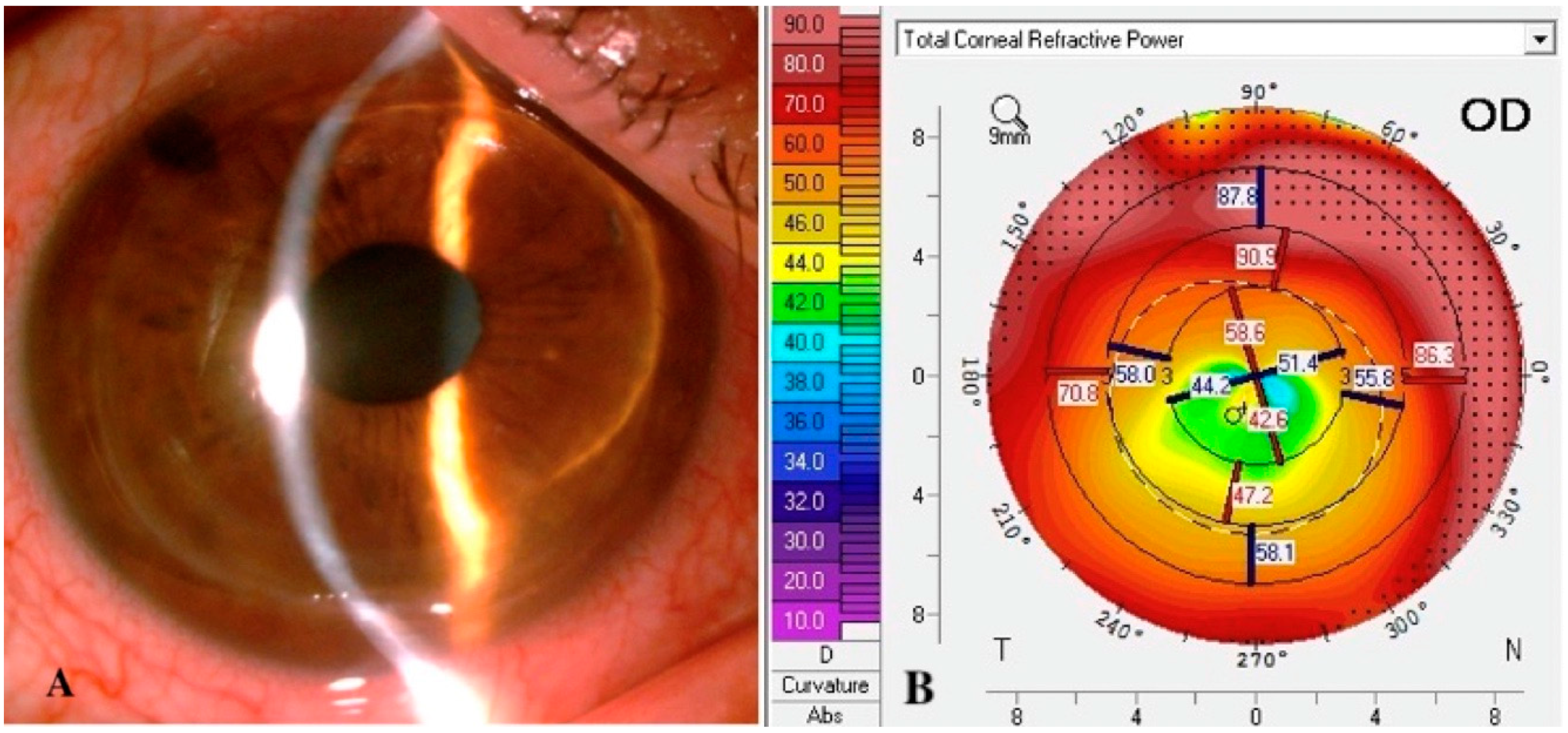
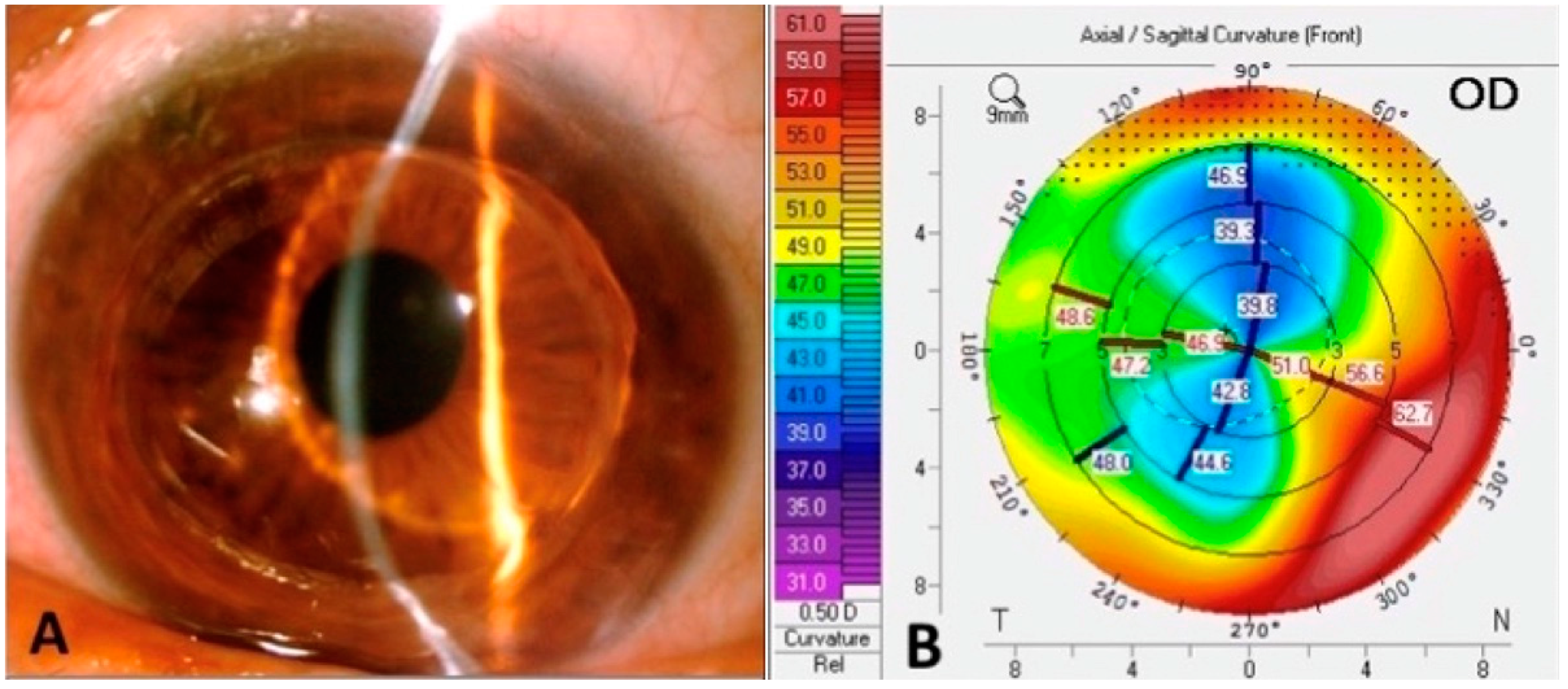
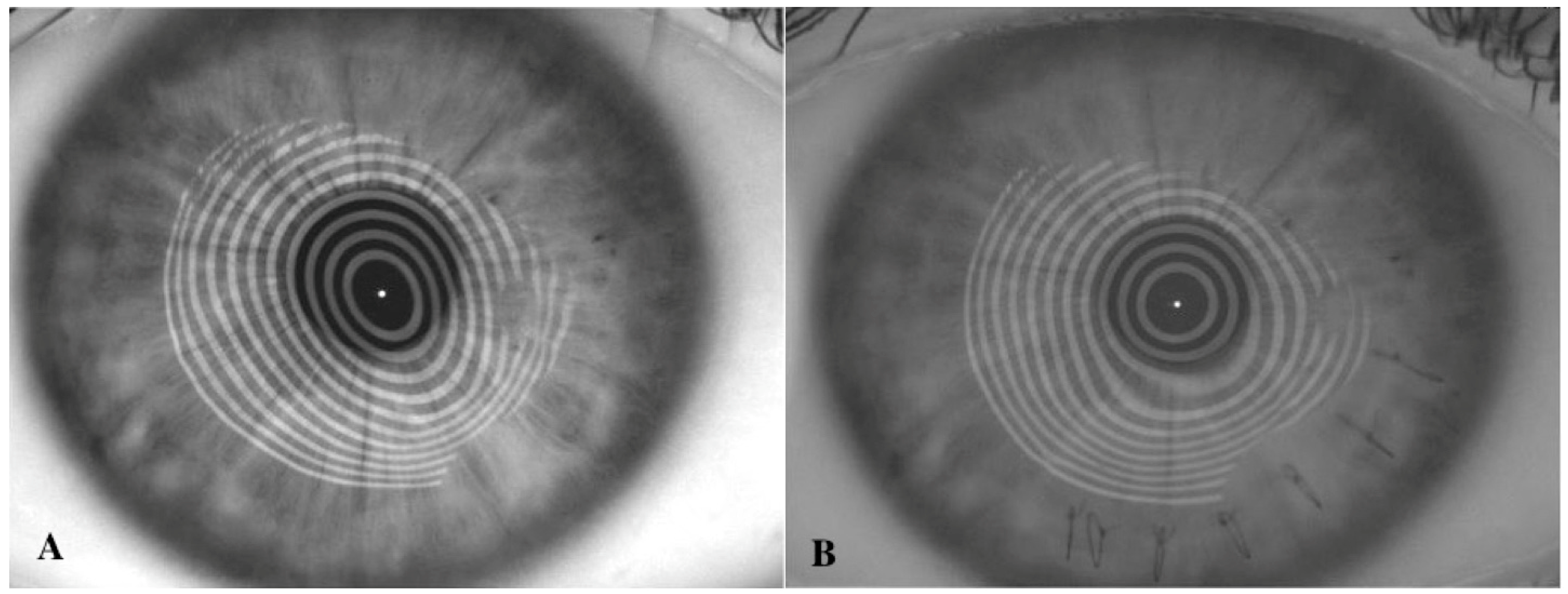
2.1. Topography
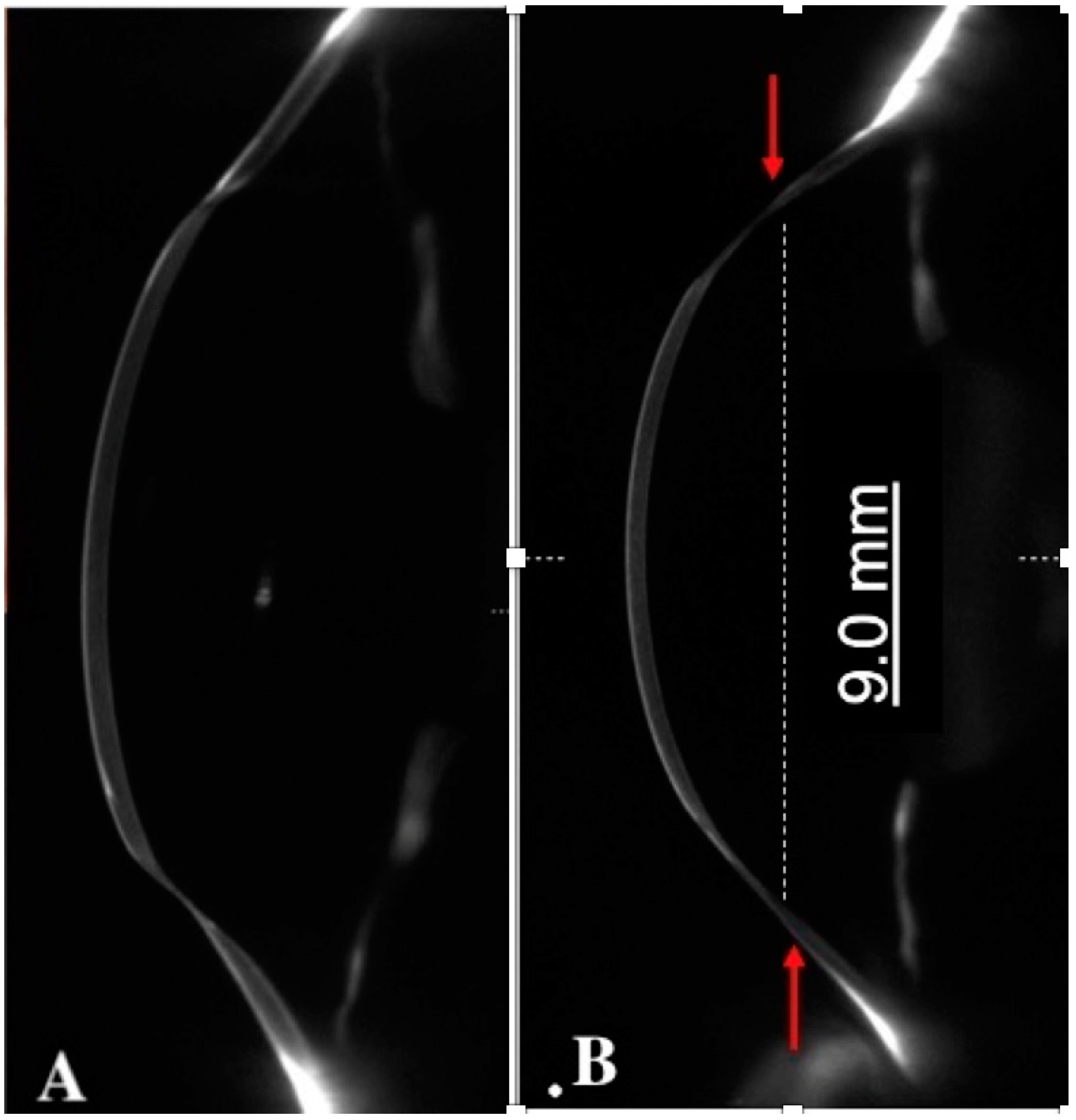
2.2. Anterior Segment OCT
3. Frequency of Corneal Ectasia after Keratoplasty
4. Mechanisms of Delayed Corneal Ectasia after Keratoplasty
5. Histological Features of Post-Keratoplasty Ectasia
6. Management
6.1. Contact Lens Fitting
6.2. Corneal Sutures
6.3. Wedge Resection
6.4. Intra Ocular Lens Implantation
6.5. Repeat Penetrating Keratoplasty
6.6. Tuck in Lamellar Keratoplasty
6.7. Peripheral Reconstructive and Annular Lamellar Keratoplasty
6.8. Overlay Deep Anterior Lamellar Keratoplasty (DALK)
7. Prevention
7.1. Crosslink (CXL)
7.2. Large DALK
8. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Romero-Jiménez, M.; Santodomingo-Rubido, J.; Wolffsohn, J.S. Keratoconus: A review. Contact Lens Anterior Eye 2010, 33, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Pramanik, S.; Musch, D.C.; Sutphin, J.E.; Farjo, A.A. Extended Long-term Outcomes of Penetrating Keratoplasty for Keratoconus. Ophthalmology 2006, 113, 1633–1638. [Google Scholar] [CrossRef] [PubMed]
- Raecker, M.E.; Erie, J.C.; Patel, S.V.; Bourne, W.M. Long-term keratometric changes after penetrating keratoplasty for keratoconus and Fuchs endothelial dystrophy. Trans. Am. Ophthalmol. Soc. 2008, 106, 187–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Ferrer, F.J.; Akpek, E.K.; Amescua, G.; Farid, M.; Lin, A.; Rhee, M.K.; Varu, D.M.; Musch, D.C.; Mah, F.S.; Dunn, S.P. Corneal Ectasia Preferred Practice Pattern®. Ophthalmology 2019, 126, 170–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sung, M.S.; Yoon, K.C. Evaluation of graft-host interface after penetrating keratoplasty using anterior segment optical coherence tomography. Jpn. J. Ophthalmol. 2014, 58, 282–289. [Google Scholar] [CrossRef]
- Brookes, N.H.; Niederer, R.L.; Hickey, D.; McGhee, C.N.J.; Sherwin, T. Recurrence of keratoconic pathology in penetrating keratoplasty buttons originally transplanted for keratoconus. Cornea 2009, 28, 688–693. [Google Scholar] [CrossRef]
- Patel, S.V.; Malta, J.B.; Banitt, M.R.; Mian, S.I.; Sugar, A.; Elner, V.M.; Tester, R.A.; Farjo, Q.A.; Soong, H.K. Recurrent ectasia in corneal grafts and outcomes of repeat keratoplasty for keratoconus. Br. J. Ophthalmol. 2009, 93, 191–197. [Google Scholar] [CrossRef]
- Maharana, P.K.; Dubey, A.; Jhanji, V.; Sharma, N.; Das, S.; Vajpayee, R.B. Management of advanced corneal ectasias. Br. J. Ophthalmol. 2016, 100, 34–40. [Google Scholar] [CrossRef] [Green Version]
- Bayramlar, H.; Karadag, R.; Cakici, O.; Ozsoy, I. Arcuate keratotomy on post-keratoplasty astigmatism is unpredictable and frequently needs repeat procedures to increase its success rate. Br. J. Ophthalmol. 2016, 100, 757–761. [Google Scholar] [CrossRef]
- Bourges, J.L.; Savoldelli, M.; Dighiero, P.; Assouline, M.; Pouliquen, Y.; BenEzra, D.; Renard, G.; Behar-Cohen, F. Recurrence of keratoconus characteristics: A clinical and histologic follow-up analysis of donor grafts. Ophthalmology 2003, 110, 1920–1925. [Google Scholar] [CrossRef]
- De Toledo, J.A.; de la Paz, M.F.; Barraquer, R.I.; Barraquer, J.; Donnenfeld, E.D. Long-term progression of astigmatism after penetrating keratoplasty for keratoconus: Evidence of late recurrence. Evid.-Based Eye Care 2003, 4, 194–195. [Google Scholar] [CrossRef]
- Ünal, M.; Yücel, I.; Akar, Y.; Akkoyunlu, G.; Gültekin, I. Recurrence of keratoconus in two corneal grafts after penetrating keratoplasty. Cornea 2007, 26, 362–364. [Google Scholar] [CrossRef] [PubMed]
- Felipe, A.F.; Hammersmith, K.M.; Nottage, J.M.; Rapuano, C.J.; Nagra, P.K.; Cohen, E.J.; Laibson, P.R. Indications, visual outcome, and ectasia in clear corneal transplants 20 years old or more. Cornea 2013, 32, 602–607. [Google Scholar] [CrossRef] [PubMed]
- Jhanji, V.; Chan, E.; Nambiar, M.; Vajpayee, R.B. Morphology of graft-host junction in cases with postkeratoplasty corneal ectasia. Cornea 2013, 32, 1031–1033. [Google Scholar] [CrossRef] [PubMed]
- Krivoy, D.; McCormick, S.; Zaidman, G.W. Postkeratoplasty keratoconus in a nonkeratoconus patient. Am. J. Ophthalmol. 2001, 131, 653–654. [Google Scholar] [CrossRef]
- Lim, L.; Pesudovs, K.; Goggin, M.; Coster, D.J. Late onset post-keratoplasty astigmatism in patients with keratoconus. Br. J. Ophthalmol. 2004, 88, 371–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buzard, K.; Febbraro, J.L.; Fundingsland, B.R. Laser in situ keratomileusis for the correction of residual ametropia after penetrating keratoplasty. J. Cataract. Refract. Surg. 2004, 30, 1006–1013. [Google Scholar] [CrossRef]
- Bergmanson, J.P.G.; Goosey, J.D.; Patel, C.K.; Mathew, J.H. Recurrence or re-emergence of keratoconus—What is the evidence telling us? Literature review and two case reports. Ocul Surf. 2014, 12, 267–272. [Google Scholar] [CrossRef]
- Feizi, S.; Zare, M. Current Approaches for Management of Postpenetrating Keratoplasty Astigmatism. J. Ophthalmol. 2011, 2011, 708736. [Google Scholar] [CrossRef] [Green Version]
- Yeniad, B.; Alparslan, N.; Akarcay, K. Eye Rubbing as an Apparent Cause of Recurrent Keratoconus. Cornea 2009, 28, 477–479. [Google Scholar] [CrossRef]
- Yoshida, J.; Murata, H.; Miyai, T.; Shirakawa, R.; Toyono, T.; Yamagami, S.; Usui, T. Characteristics and risk factors of recurrent keratoconus over the long term after penetrating keratoplasty. Graefe’s Arch. Clin. Exp. Ophthalmol. Albrecht Von Graefes Arch. Fur Klin. Und Exp. Ophthalmol. 2018, 256, 2377–2383. [Google Scholar] [CrossRef] [PubMed]
- Niziol, L.M.; Musch, D.C.; Gillespie, B.W.; Marcotte, L.M.; Sugar, A. Long-term outcomes in patients who received a corneal graft for keratoconus between 1980 and 1986. Am. J. Ophthalmol. 2013, 155, 213–219.e3. [Google Scholar] [CrossRef] [PubMed]
- Vajpayee, R.B.; Jhanji, V.; Beltz, J.; Moorthy, S. “Tuck In” Lamellar Keratoplasty for Tectonic Management of Postkeratoplasty Corneal Ectasia with Peripheral Corneal Involvement. Cornea 2011, 30, 171–174. [Google Scholar] [CrossRef] [PubMed]
- Singar, E.; Burcu, A.; Tamer-Kaderli, S.; Yalnız-Akkaya, Z.; Ozbek-Uzman, S.; Ornek, F. Resuturing after penetrating keratoplasty without trauma: Indications and results. J. Fr. Ophtalmol. 2020, 43, 18–24. [Google Scholar] [CrossRef]
- Feizi, S.; Javadi, M.A.; Khajuee-Kermani, P.; Jafari, R. Repeat Keratoplasty for Failed Deep Anterior Lamellar Keratoplasty in Keratoconus. Cornea 2017, 36, 535–540. [Google Scholar]
- Szczotka-Flynn, L.; McMahon, T.T.; Lass, J.H.; Sugar, J.; Weissman, B.A.; Stiegemeier, M.J.; Reinhart, W.J. Late-Stage Progressive Corneal Astigmatism After Penetrating Keratoplasty for Keratoconus. Eye Contact Lens Sci. Clin. Pract. 2004, 30, 105–110. [Google Scholar] [CrossRef]
- Ilari, L.; Daya, S.M. Corneal wedge resection to treat progressive keratoconus in the host cornea after penetrating keratoplasty. J. Cataract Refract. Surg. 2003, 29, 395–401. [Google Scholar] [CrossRef]
- Malbran, E.S.; Price, F.W.; Olivero, J.E.A.; Malbran, J.; Malbran, M.; Rogel, L.N.; Price, M.O.; Gordillo, C.H. Peripheral Reconstructive Lamellar Keratoplasty for Late Ectasia After Penetrating Keratoplasty in Keratoconus Eyes. Cornea 2019, 38, 1377–1381. [Google Scholar] [CrossRef]
- Bromley, J.G.; Randleman, J.B. Treatment strategies for corneal ectasia. Curr. Opin. Ophthalmol. 2010, 21, 255–258. [Google Scholar] [CrossRef] [Green Version]
- Nuijts, R.M.M.A.; Abhilakh Missier, K.A.; Nabar, V.A.; Japing, W.J. Artisan toric lens implantation for correction of postkeratoplasty astigmatism. Ophthalmology 2004, 111, 1086–1094. [Google Scholar] [CrossRef]
- Akcay, L.; Kaplan, A.T.; Kandemir, B.; Gunaydın, N.T.; Dogan, O.K. Toric intraocular Collamer lens for high myopic astigmatism after penetrating keratoplasty. J. Cataract Refract. Surg. 2009, 35, 2161–2163. [Google Scholar] [CrossRef] [PubMed]
- Fares, U.; Sarhan, A.R.S.; Dua, H.S. Management of post-keratoplasty astigmatism. J. Cataract Refract. Surg. 2012, 38, 2029–2039. [Google Scholar] [CrossRef] [PubMed]
- Severinsky, B.; Behrman, S.; Frucht-Pery, J.; Solomon, A. Scleral contact lenses for visual rehabilitation after penetrating keratoplasty: Long term outcomes. Contact Lens Anterior Eye 2014, 37, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, D.S. Update on scleral lenses. Curr. Opin. Ophthalmol. 2008, 19, 298–301. [Google Scholar] [CrossRef]
- Roper-Hall, M.J.; Atkins, A.D. Control of astigmatism after surgery and trauma: A new technique. Br. J. Ophthalmol. 1985, 69, 352–359. [Google Scholar] [CrossRef] [Green Version]
- Limberg, M.B.; Dingeldein, S.A.; Green, M.T.; Klyce, S.D.; Insler, M.S.; Kaufman, H.E. Corneal Compression Sutures for the Reduction of Astigmatism After Penetrating Keratoplasty. Am. J. Ophthalmol. 1989, 108, 36–42. [Google Scholar] [CrossRef]
- Fares, U.; Mokashi, A.A.; Al-Aqaba, M.A.; Otri, A.M.; Miri, A.; Dua, H.S. Management of postkeratoplasty astigmatism by paired arcuate incisions with compression sutures. Br. J. Ophthalmol. 2013, 97, 438–443. [Google Scholar] [CrossRef]
- Deshmukh, R.; Nair, S.; Vaddavalli, P.K.; Agrawal, T.; Rapuano, C.J.; Beltz, J.; Vajpayee, R.B. Post Penetrating Keratoplasty Astigmatism. Surv. Ophthalmol. 2021, 20, 14–28. [Google Scholar] [CrossRef]
- Mejía, L.F.; Gil, J.C.; Naranjo, S. Long-term Results of Corneal Wedge Resection for High Postkeratoplasty Astigmatism. Cornea 2020, 39, 535–539. [Google Scholar] [CrossRef]
- Tahzib, N.G.; Cheng, Y.Y.; Nuijts, R.M. Three-Year Follow-up Analysis of Artisan Toric Lens Implantation for Correction of Postkeratoplasty Ametropia in Phakic and Pseudophakic Eyes. Ophthalmology 2006, 113, 976–984. [Google Scholar] [CrossRef]
- Alfonso, J.F.; Lisa, C.; Abdelhamid, A.; Montés-Micó, R.; Poo-López, A.; Ferrer-Blasco, T. Posterior chamber phakic intraocular lenses after penetrating keratoplasty. J. Cataract Refract. Surg. 2009, 35, 1166–1173. [Google Scholar] [CrossRef] [PubMed]
- Wan, K.H.; Chang, J.S.M.; Jhanji, V.; Affiliations, F.; Kong, H. Toric Intraocular Lens for Astigmatism Correction following Keratoplasty in Phakic and Pseudophakic Eyes. 2022. Available online: http://journals.lww.com/jcrs (accessed on 8 February 2022).
- Al-Mezaine, H.; Wagoner, M.D. Repeat penetrating keratoplasty: Indications, graft survival, and visual outcome. Br. J. Ophthalmol. 2006, 90, 324–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weisbrod, D.J.; Sit, M.; Naor, J.; Slomovic, A.R. Outcomes of Repeat Penetrating Keratoplasty and Risk Factors for Graft Failure. Cornea 2003, 22, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Szentmáry, N.; Seitz, B.; Langenbucher, A.; Naumann, G.O. Repeat Keratoplasty for Correction of High or Irregular Postkeratoplasty Astigmatism in Clear Corneal Grafts. Am. J. Ophthalmol. 2005, 139, 826–830. [Google Scholar] [CrossRef] [PubMed]
- Vajpayee, R.B.; Beltz, J.; Jhanji, V.; Cassidy, D.; Chan, E. Tuck-in lamellar keratoplasty for postkeratoplasty ectasia involving the corneal periphery. Clin. Exp. Ophthalmol. 2011, 30, 171–174. [Google Scholar]
- Jiang, Y.; Li, Y.; Yang, S.; Lu, C. Tuck-in Lamellar keratoplasty with an lenticule obtained by small incision lenticule extraction for treatment of Post- LASIK Ectasia. Sci. Rep. 2017, 7, 17806. [Google Scholar] [CrossRef] [Green Version]
- Cheng, C.-L.; Theng, J.T.; Tan, D.T. Compressive C-shaped lamellar keratoplasty: A surgical alternative for the management of severe astigmatism from peripheral corneal degeneration. Ophthalmology 2005, 112, 425–430. [Google Scholar] [CrossRef]
- Fontana, L.; Parente, G.; Sincich, A.; Tassinari, G. Influence of Graft-Host Interface on the Quality of Vision After Deep Anterior Lamellar Keratoplasty in Patients with Keratoconus. Cornea 2011, 30, 497–502. [Google Scholar] [CrossRef]
- Lake, D.; Hamada, S.; Khan, S.; Daya, S.M. Deep Anterior Lamellar Keratoplasty Over Penetrating Keratoplasty for Host Rim Thinning and Ectasia. Cornea 2009, 28, 489–492. [Google Scholar] [CrossRef]
- Scorcia, V.; Beltz, J.; Busin, M. Small-Bubble Deep Anterior Lamellar Keratoplasty Technique. JAMA Ophthalmol. 2014, 132, 1369–1371. [Google Scholar] [CrossRef] [Green Version]
- Yu, A.C.; Mattioli, L.; Busin, M. Optimizing outcomes for keratoplasty in ectatic corneal disease. Curr. Opin. Ophthalmol. 2020, 31, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.K.; Scorcia, V.; Kadyan, A.; Lapenna, L.; Ponzin, D.; Busin, M. Microkeratome-Assisted Superficial Anterior Lamellar Keratoplasty for Anterior Stromal Corneal Opacities After Penetrating Keratoplasty. Cornea 2012, 31, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Gutfreund, S.; Leon, P.; Busin, M. Microkeratome-Assisted Anterior Lamellar Keratoplasty for the Correction of High-Degree Postkeratoplasty Astigmatism. Cornea 2017, 36, 880–883. [Google Scholar] [CrossRef] [PubMed]
- Sorkin, N.; Varssano, D. Corneal Collagen Crosslinking: A Systematic Review. Ophthalmologica 2014, 232, 10–27. [Google Scholar] [CrossRef] [PubMed]
- Medeiros, C.S.; Giacomin, N.T.; Bueno, R.L.; Ghanem, R.C.; Moraes, H.V.; Santhiago, M.R. Accelerated corneal collagen crosslinking: Technique, efficacy, safety, and applications. J. Cataract Refract. Surg. 2016, 42, 1826–1835. [Google Scholar] [CrossRef] [PubMed]
- Moramarco, A.; Mastrofilippo, V.; Romano, M.G.; Iannetta, D.; Braglia, L.; Fontana, L. Efficacy and Safety of Accelerated Corneal Cross-linking for Progressive Keratoconus: A 5-Year Follow-up Study. J. Refract. Surg. 2020, 36, 724–730. [Google Scholar] [CrossRef]
- Journal, O.; Ziaei, M.; Gokul, A.; Vellara, H.; Patel, D.; Mcghee, C.N. Medical Hypothesis, Discovery &Innovation Peripheral Cornea Crosslinking Before Deep Anterior Lamellar Keratoplasty. Med. Hypothesis Discov. Innov. Ophthalmol. 2020, 9, 127. [Google Scholar]
- Liu, H.; Chen, Y.; Wang, P.; Li, B.; Wang, W.; Su, Y.; Sheng, M. Efficacy and Safety of Deep Anterior Lamellar Keratoplasty vs. Penetrating Keratoplasty for Keratoconus: A Meta-Analysis. PLoS ONE 2015, 10, e0113332. [Google Scholar] [CrossRef]
- Huang, T.; Hu, Y.; Gui, M.; Zhang, H.; Wang, Y.; Hou, C. Large-diameter deep anterior lamellar keratoplasty for keratoconus: Visual and refractive outcomes. Br. J. Ophthalmol. 2015, 99, 1196–1200. [Google Scholar] [CrossRef]
- Busin, M.; Leon, P.; Nahum, Y.; Scorcia, V. Large (9 mm) Deep Anterior Lamellar Keratoplasty with Clearance of a 6-mm Optical Zone Optimizes Outcomes of Keratoconus Surgery. Ophthalmology 2017, 124, 1072–1080. [Google Scholar] [CrossRef]
- Myerscough, J.; Roberts, H.; Yu, A.C.; Elkadim, M.; Bovone, C.; Busin, M. Five-year Outcomes of Converted Mushroom Keratoplasty from Intended Deep Anterior Lamellar Keratoplasty (DALK) Mandate 9-mm Diameter DALK as the Optimal Approach to Keratoconus. Am. J. Ophthalmol. 2020, 220, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Feizi, S.; Javadi, M.-A.; Kanavi, M.R. Recurrent Keratoconus in a Corneal Graft after Deep Anterior Lamellar Keratoplasty. J. Ophthalmic Vis. Res. 2012, 7, 328–331. [Google Scholar] [PubMed]
- Romano, V.; Iovieno, A.; Parente, G.; Soldani, A.M.; Fontana, L. Long-Term Clinical Outcomes of Deep Anterior Lamellar Keratoplasty in Patients with Keratoconus. Am. J. Ophthalmol. 2015, 159, 505–511. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Procedure | Operated Eyes | Results | |
|---|---|---|---|
| Limberg et al. | Compressive suture | 5 | A 58% reduction of average cylinder in 1 week; reduction of 41% of average cylinder at 9–12 months |
| Roper-Hall and Atkins et al. | Compressive suture | 1 | 8 compression sutures to treat 10 D of refractive cylinder. |
| Kirkness et al. | Compressive suture & arcuate keratotomy | 38 | Reduction of 3.6 D–5 D in astigmatism |
| Javadi et al. | Compressive suture | 77 | A mean reduction of 3.4 D and 5.9 D in keratometric astigmatism |
| Mejia et al. | Wedge resection | 39 | Astigmatic cylinder improved from 7.99 D to 2.5 D at 12 months and remained stable thereafter |
| Ilari et al. | Wedge resection | 3 | Preoperative astigmatism decrease and corneal profile regularized |
| Nuijts et al. | IOL implantation (Artisan toric lens) | 16 | Spherical equivalent decreased from 5.50 D before surgery to 0.86 D at final follow-up |
| Tahzib et al. | IOL implantation (Artisan toric lens) | 36 | Spherical equivalent decreased from 4.31 D preoperatively to 1.20 D at the last follow-up |
| Akcay et al. | IOL implantation (Toric ICL) | 1 | Patient manifest refraction improved from −8.0/−1.75 at 170° preoperatively, to −0.75/−0.50 at 130° postoperatively |
| Alfonso et al. | IOL implantation (Posterior chamber phakic intraocular lenses) | 15 | The mean postoperative spherical equivalent was 0.95 D |
| Al Mezaine et al. | Repeat PK | 210 | 29.6% of the eyes achieved a final visual acuity greater than 20/200, while only 4.8% reached 20/40 or better |
| Daniel J. Weisbrod et al. | Repeat PK | 116 | 2 and 5-year survival rates for repeat PKP were 63.9% and 45.6%, respectively |
| Szentmàry et al. | Repeat PK | 17 | Visual acuity improved significantly from 0.2 to 0.5 |
| Vajpayee et al. | Tuck In Lamellar Keratoplasty | 12 | Kmean decreased, and the mean spherical equivalent (SEQ) refractive error decreased |
| Yang et al. | Tuck In Lamellar Keratoplasty with an lenticule | 3 | The mean min K value measured by topography preoperatively and 1 day, 1 month, 3 months and 12 months postoperative was 44.86 ± 3.92, 48.83 ± 2.38, 50.63 ± 4.24, 49.71 ± 3.26 and 50.07 ± 3.43 respectively. The max K value increased significantly after the operation and then declined gradually |
| Malbran et al. | Peripheral Reconstructive Lamellar Keratoplasty | 33 | Preoperatively, the mean keratometric measures were K1: 44.8 D and K2: 54.1 D and postoperatively K1: 47.5 D and K2: 50.8 D. |
| Cheng et al. | C-shaped lamellar keratoplasty | 3 | All eyes achieved Snellen visual acuity of 20/40 or better and stable astigmatism ranging from 0 to 2.75 diopter cylinder within 6 months |
| Lake et al. | DALK Overlay | 7 | At 12 months, mean UCVA improved from 1.157 to 0.74 Logmar. Mean BCVA improved from 0.82 to 0.37 at 12 months |
| Scorcia et al. | DALK Overlay (small bubble) | 9 | BCVA improved by at least 4 Snellen lines |
| Patel et al. | Microkeratome-Assisted Superficial Anterior Lamellar Keratoplasty | 9 |
BCVA improved in all 9 eyes at final follow-up. Refractive astigmatism also improved by an average of 0.7 diopters. |
| Gutfreund et al. | Microkeratome-Assisted Anterior Lamellar Keratoplasty (MALK) | 4 | 3 years after MALK, BCVA improved to 20/20, refractive astigmatism decreased of an average of 2.1 D (in all cases within 4.5 D), and the average surface asymmetry index decreased from 2.27 to 0.56 |
| Procedure | Indications | Advantages | Disadvantages |
|---|---|---|---|
| Contact lens fitting | First line treatment | Non-invasive, better visual acuity than spectacles | Corneal scarring, whorl keratopathy, corneal micro-trauma, epithelial and anterior stroma disruption, and chronic ocular inflammation |
| Compressive sutures | Early case of ectasia post-PK | Minimal risk of penetration into the anterior chamber | Improvement may be unpredictable and subject to loss of effect with time due to the tissue elasticity |
| Wedge resection | Ectasia of limited extension along the graft–host junction. | Prevent or delay the need for repeat PK, no risk of rejection or interface haze | Postoperative unstable astigmatism. |
| Intra ocular lens implantation | Correct post-PK astigmatism in phakic eyes or during cataract surgery | Does not alter corneal profile and transparency | Endothelial cell loss, chronic inflammation, cystoid macular edema, pigment dispersion, leading to pigmentary glaucoma, cilio-lenticular block, iris synechiae, sphincter erosion, and iris transillumination |
| Repeat penetrating keratoplasty | Extensive ectasia involving the graft-host junction | Visual acuity and astigmatism improve significantly after large PK as sutures are placed more peripherally and influence less the central graft | Increased risk of graft rejection, late endothelial failure, cataract development, and augmented risk of postoperative glaucoma and immunologic rejection |
| Tuck-in lamellar keratoplasty | Diffuse thinning of the peripheral cornea with advanced corneal ectasia involving corneal periphery and the graft-host interface | Tectonic support to the weakened peripheral cornea beyond the previous graft–host junction, no damage to the recipient’s limbal stem cells | Challenging technique to perform for both donor and host preparation |
| Peripheral reconstructive and annular lamellar keratoplasty | Diffuse thinning of the peripheral cornea with advanced corneal ectasia | Preserve the previous PK and restore normal peripheral corneal thickness, minimize forward protrusion of the cornea | Causes peripheral vascularization with early loosening of sutures. Surgically challenging to perform for both donor and host preparation |
| Overlay deep anterior lamellar keratoplasty | Extensive corneal ectasia. Aims to correct the donor and host cornea profile and thickness without replacing the PK endothelium | Preserve the globe integrity, the donor graft and peripheral host endothelium, thus reducing the risk of endothelial rejection, late graft failure, and complications related to open-sky surgery | Technically more challenging than conventional DALK, risk of perforation when dissecting across the host-graft junction |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moramarco, A.; Gardini, L.; Iannetta, D.; Versura, P.; Fontana, L. Post Penetrating Keratoplasty Ectasia: Incidence, Risk Factors, Clinical Features, and Treatment Options. J. Clin. Med. 2022, 11, 2678. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102678
Moramarco A, Gardini L, Iannetta D, Versura P, Fontana L. Post Penetrating Keratoplasty Ectasia: Incidence, Risk Factors, Clinical Features, and Treatment Options. Journal of Clinical Medicine. 2022; 11(10):2678. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102678
Chicago/Turabian StyleMoramarco, Antonio, Lorenzo Gardini, Danilo Iannetta, Piera Versura, and Luigi Fontana. 2022. "Post Penetrating Keratoplasty Ectasia: Incidence, Risk Factors, Clinical Features, and Treatment Options" Journal of Clinical Medicine 11, no. 10: 2678. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102678