
What Role Does PDGFA Gene Polymorphisms Play in Treating Tennis Elbow with PRP? A Prospective Cohort Study

 ,
,  , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. PRP Separation and Injection Procedure
2.4. Whole Blood and PRP Analyses
2.5. Follow-Up, Outcomes, Measures of Effectiveness
2.6. Genetic Analyses
2.7. Statistical Analyses
3. Results
3.1. General Characteristics of the Study Group
3.2. Factors Influencing Platelets and PDGF-AB Concentration
3.3. Factors Influencing PROMs Values
3.4. PDGFA Gene Polymorphisms and Patients Characteristics
3.5. PDGFA Gene Polymorphisms and Platelet Parameters
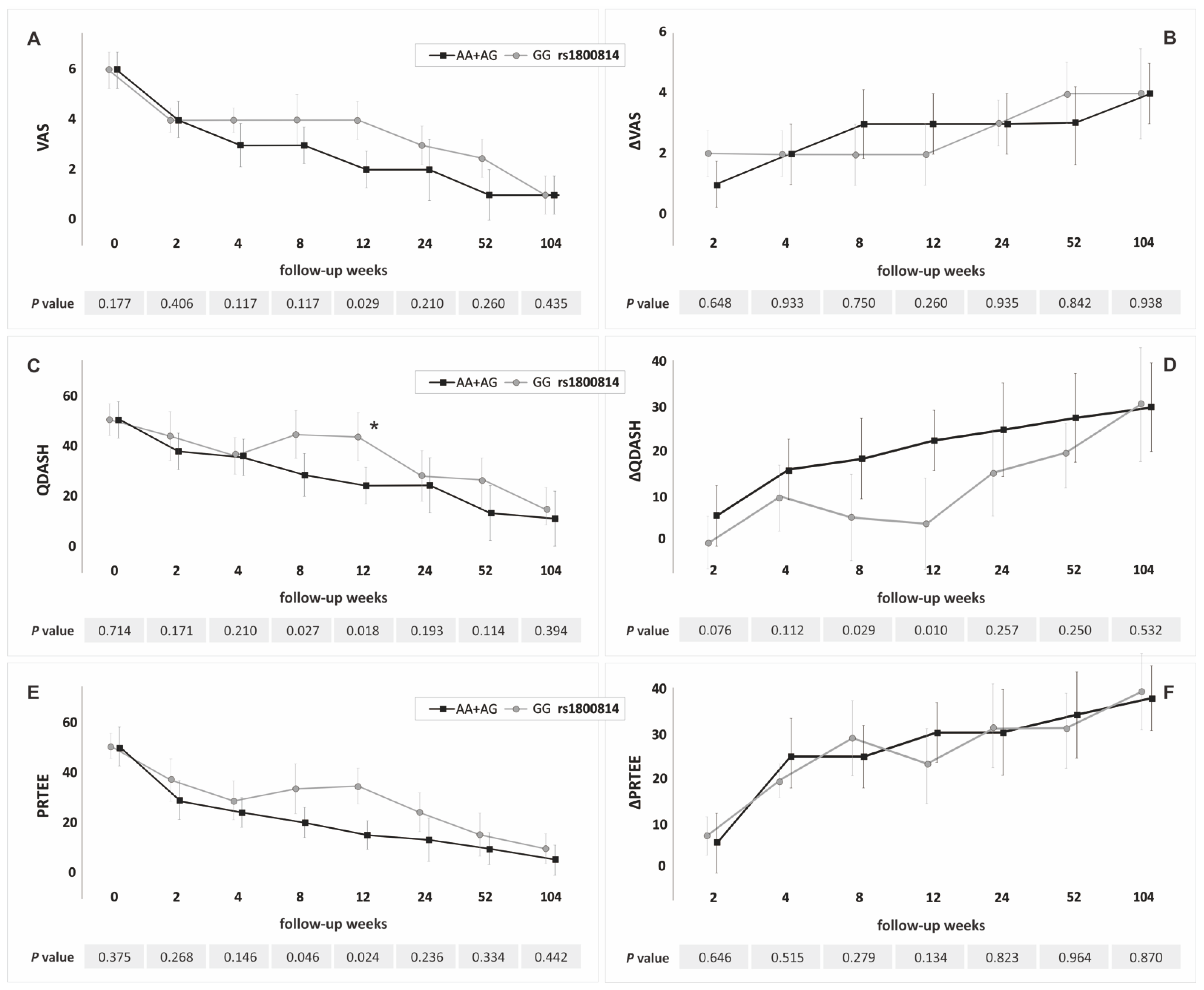
3.6. PDGFA Gene Polymorphisms and PROMs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vaquero-Picado, A.; Barco, R.; Antuña, S.A. Lateral epicondylitis of the elbow. EFORT Open Rev. 2017, 1, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Popescu, M.N.; Iliescu, M.G.; Beiu, C.; Popa, L.G.; Mihai, M.M.; Berteanu, M.; Ionescu, A.M. Autologous Platelet-Rich Plasma Efficacy in the Field of Regenerative Medicine: Product and Quality Control. Biomed. Res. Int. 2021, 2021, 4672959. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, J.; Bulsara, M.; Zheng, M.H. The Effectiveness of Platelet-Rich Plasma in the Treatment of Tendinopathy: A Meta-analysis of Randomized Controlled Clinical Trials. Am. J. Sports Med. 2017, 45, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Niemiec, P.; Szyluk, K.; Jarosz, A.; Iwanicki, T.; Balcerzyk, A. Effectiveness of Platelet-Rich Plasma for Lateral Epicondylitis. A Systematic Review and Meta-analysis Based on Achievement of Minimal Clinically Important Difference. Orthop. J. Sports Med. 2022, 10. [Google Scholar] [CrossRef]
- Lenoir, H.; Mares, O.; Carlier, Y. Management of lateral epicondylitis. Orthop. Traumatol. Surg. Res. 2019, 105, S241–S246. [Google Scholar] [CrossRef]
- Popescu, M.B.; Carp, M.; Tevanov, I.; Nahoi, C.A.; Stratila, M.A.; Haram, O.M.; Ulici, A. Isolated Meniscus Tears in Adolescent Patients Treated with Platelet-Rich Plasma Intra-articular Injections: 3-Month Clinical Outcome. Biomed. Res. Int. 2020, 2020. [Google Scholar] [CrossRef] [PubMed]
- Eisinger, F.; Patzelt, J.; Langer, H.F. The Platelet Response to Tissue Injury. Front. Med. 2018, 5, 317. [Google Scholar] [CrossRef] [Green Version]
- Kohler, N.; Lipton, A. Platelets as a source of fibroblast growth-promoting activity. Exp. Cell Res. 1974, 87, 297–301. [Google Scholar] [CrossRef]
- Wu, D.; Wang, M.; Wang, X.; Zhang, Y.B.; Song, T.; Yin, N.; Zhao, Z. Interaction between interferon regulatory factor 6 and glycine receptor beta shows a protective effect on developing non-syndromic cleft lip with or without cleft palate in the Han Chinese population. Eur. J. Oral Sci. 2019, 127, 27–32. [Google Scholar] [CrossRef]
- Fredriksson, L.; Li, H.; Eriksson, U. The PDGF family: Four gene products form five dimeric isoforms. Cytokine Growth Factor Rev. 2004, 15, 197–204. [Google Scholar] [CrossRef]
- Gupta, A.; El-Amin, S.F., 3rd; Levy, H.J.; Sze-Tu, R.; Ibim, S.E.; Maffulli, N. Umbilical cord-derived Wharton’s jelly for regenerative medicine applications. J. Orthop. Surg. Res. 2020, 15, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, A.; Xia, X.; Yeh, J.; Kua, H.; Liu, H.; Mishina, Y.; Hao, A.; Li, B. PDGF-AA promotes osteogenic differentiation and migration of mesenchymal stem cells by down-regulating PDGFRα and derepressing BMP-Smad1/5/8 signaling. PLoS ONE 2014, 9, e113785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niemiec, P.; Szyluk, K.; Balcerzyk, A.; Kalita, M.; Jarosz, A.; Iwanicka, J.; Iwanicki, T.; Nowak, T.; Negru, M.; Francuz, T.; et al. Why PRP works only on certain patients with tennis elbow? Is PDGFB gene a key for PRP therapy effectiveness? A prospective cohort study. BMC Musculoskelet. Disord. 2021, 22, 710. [Google Scholar] [CrossRef] [PubMed]
- Hao, Q.; Devji, T.; Zeraatkar, D.; Wang, Y.; Qasim, A.; Siemieniuk, R.A.C.; Vandvik, P.O.; Lähdeoja, T.; Carrasco-Labra, A.; Agoritsas, T.; et al. Minimal important differences for improvement in shoulder condition patient-reported outcomes: A systematic review to inform a BMJ Rapid Recommendation. BMJ Open 2019, 9, e028777. [Google Scholar] [CrossRef] [Green Version]
- Smith-Forbes, E.V.; Howell, D.M.; Willoughby, J.; Pitts, D.G.; Uhl, T.L. Specificity of the minimal clinically important difference of the quick Disabilities of the Arm Shoulder and Hand (QDASH) for distal upper extremity conditions. J. Hand Ther. 2016, 29, 81–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poltawski, L.; Watson, T. Measuring clinically important change with the Patient-rated Tennis Elbow Evaluation. Hand Ther. 2011, 16, 52–57. [Google Scholar] [CrossRef] [Green Version]
- National Library of Medicine (US): National Center for Biotechnology Information. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/snp/ (accessed on 5 March 2022).
- Zeckey, C.; Hildebrand, F.; Glaubitz, L.M.; Jürgens, S.; Ludwig, T.; Andruszkow, H.; Hüfner, T.; Krettek, C.; Stuhrmann, M. Are polymorphisms of molecules involved in bone healing correlated to aseptic femoral and tibial shaft non-unions? J. Orthop. Res. 2011, 29, 1724–1731. [Google Scholar] [CrossRef]
- Andrae, J.; Gallini, R.; Betsholtz, C. Role of platelet-derived growth factors in physiology and medicine. Genes Dev. 2008, 22, 1276–1312. [Google Scholar] [CrossRef] [Green Version]
- Shah, P.; Keppler, L.; Rutkowski, J. A review of platelet-derived growth factor playing pivotal role in bone regeneration. J. Oral Implantol. 2014, 40, 330–340. [Google Scholar] [CrossRef]
- Deptuła, M.; Karpowicz, P.; Wardowska, A.; Sass, P.; Sosnowski, P.; Mieczkowska, A.; Filipowicz, N.; Dzierżyńska, M.; Sawicka, J.; Nowicka, E.; et al. Development of a Peptide Derived from Platelet-Derived Growth Factor (PDGF-BB) into a Potential Drug Candidate for the Treatment of Wounds. Adv. Wound Care 2020, 9, 657–675. [Google Scholar] [CrossRef]
- Liang, T.; Zhu, L.; Gao, W.; Gong, M.; Ren, J.; Yao, H.; Wang, K.; Shi, D. Coculture of endothelial progenitor cells and mesenchymal stem cells enhanced their proliferation and angiogenesis through PDGF and Notch signaling. FEBS Open Bio. 2017, 7, 1722–1736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casati, L.; Celotti, F.; Negri-Cesi, P.; Sacchi, M.C.; Castano, P.; Colciago, A. Platelet derived growth factor (PDGF) contained in Platelet Rich Plasma (PRP) stimulates migration of osteoblasts by reorganizing actin cytoskeleton. Cell Adhes. Migr. 2014, 8, 595–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evrova, O.; Buschmann, J. In vitro and in vivo effects of PDGF-BB delivery strategies on tendon healing: A review. Eur. Cell Mater. 2017, 34, 15–39. [Google Scholar] [CrossRef] [PubMed]
- Manoranjan, S.J.; Faizuddin, M.; Hemalatha, M.; Ranganath, V. The effect of platelet derived growth factor-AB on periodontal ligament fibroblasts: An in vitro study. J. Indian Soc. Periodontol. 2012, 16, 49–53. [Google Scholar] [CrossRef]
- Salini, V.; Vanni, D.; Pantalone, A.; Abate, M. Platelet Rich Plasma Therapy in Non-insertional Achilles Tendinopathy: The Efficacy is Reduced in 60-years Old People Compared to Young and Middle-Age Individuals. Front. Aging Neurosci. 2015, 7, 228. [Google Scholar] [CrossRef] [Green Version]
- Evanson, J.R.; Guyton, M.K.; Oliver, D.L.; Hire, J.M.; Topolski, R.L.; Zumbrun, S.D.; McPherson, J.C.; Bojescul, J.A. Gender and age differences in growth factor concentrations from platelet-rich plasma in adults. Mil. Med. 2014, 179, 799–805. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, B.; Tol, J.L.; Knez, W.; Chalabi, H. Exercise and the platelet activator calcium chloride both influence the growth factor content of platelet-rich plasma (PRP): Overlooked biochemical factors that could influence PRP treatment. Br. J. Sports Med. 2015, 49, 957–960. [Google Scholar] [CrossRef]
- Mannava, S.; Whitney, K.E.; Kennedy, M.I.; King, J.; Dornan, G.J.; Klett, K.; Chahla, J.; Evans, T.A.; Huard, J.; LaPrade, R.F. The Influence of Naproxen on Biological Factors in Leukocyte-Rich Platelet-Rich Plasma: A Prospective Comparative Study. Arthroscopy 2019, 35, 201–210. [Google Scholar] [CrossRef]
- Sundman, E.A.; Cole, B.J.; Fortier, L.A. Growth factor and catabolic cytokine concentrations are influenced by the cellular composition of platelet-rich plasma. Am. J. Sports Med. 2011, 39, 2135–2140. [Google Scholar] [CrossRef]
- Lim, W.; Park, S.H.; Kim, B.; Kang, S.W.; Lee, J.W.; Moon, Y.L. Relationship of cytokine levels and clinical effect on platelet-rich plasma-treated lateral epicondylitis. J. Orthop. Res. 2018, 36, 913–920. [Google Scholar] [CrossRef]
- De Melo Viveiros, M.E.; Viveiros, M.M.H.; da Silva, M.G.; Rainho, C.A.; Schellini, S.A. In vitro effect of triamcinolone and platelet-rich plasma on cytokine levels of elbow lateral epicondylitis-derived cells. J. Orthop. Surg. Res. 2022, 17, 94. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Li, H.; Chen, K.; Wu, B.; Liu, H. Association of polymorphisms rs1800012 in COL1A1 with sports-related tendon and ligament injuries: A meta-analysis. Oncotarget 2017, 8, 27627–27634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lv, Z.T.; Gao, S.T.; Cheng, P.; Liang, S.; Yu, S.Y.; Yang, Q.; Chen, A.M. Association between polymorphism rs12722 in COL5A1 and musculoskeletal soft tissue injuries: A systematic review and meta-analysis. Oncotarget 2017, 9, 15365–15374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, R.; Aizezi, A.; Fan, Y.; Ji, Z.; Li, W.; Li, Y.; Wang, Z.; Ning, K. Association between matrix metalloproteinase-3 gene polymorphisms and tendon-ligament injuries: Evidence from a meta-analysis. BMC Sports Sci. Med. Rehabil. 2022, 14, 26. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | |||
|---|---|---|---|
| Subjects | Number of subjects, n (%) | 107 | (100.0) |
| Single tennis elbow, n (%) | 82 | (76.6) | |
| Bilateral tennis elbow, n (%) | 25 | (23.4) | |
| Elbows | Number of elbows, n (%) | 132 | (100.0) |
| Tennis elbow in the dominant hand, n (%) | 86 | (65.2) | |
| Tennis elbow in the non-dominant hand, n (%) | 46 | (34.8) | |
| Demographics | Females, n (%) | 77 | (58.3) |
| Age, median ± QD | 46.00 | 5.50 | |
| BMI | BMI, median ± QD | 25.65 | 2.00 |
| BMI ≥ 25, n (%) | 86 | (65.2) | |
| Cigarette smoking | Current smoking, n (%) | 22 | (16.6) |
| Former smoking, n (%) | 48 | (36.4) | |
| Main comorbidities | Diabetes mellitus, n (%) | 4 | (3.0) |
| Gout, n (%) | 8 | (6.1) | |
| Thyroid diseases, n (%) | 15 | (11.4) | |
| Hypercholesterolemia, n (%) | 7 | (5.3) | |
| Hypertension, n (%) | 18 | (13.6) | |
| Variables | PLT WB, 109/L | PLT PRP, 109/L | PDGF-AB, ng/mL | Age | BMI | Cigarettes/Day | Alcohol Units/Week |
|---|---|---|---|---|---|---|---|
| PLT WB, 109/L | - | 0.57 * | 0.45 * | −0.08 | 0.10 | 0.11 | −0.31 * |
| PLT PRP, 109/L | 0.57 * | - | 0.71 * | −0.12 | 0.32 * | 0.19 * | −0.04 |
| PDGF-AB, ng/mL | 0.45 * | 0.71 * | - | −0.23 * | 0.16 | 0.26 * | −0.05 |
| Age | −0.08 | −0,12 | −0.23 * | - | 0.20 * | −0.05 | −0.06 |
| BMI | 0.10 | 0.32 * | 0.16 | 0.20 * | - | 0.00 | 0.10 |
| Cigarettes/day | 0.11 | 0.19 * | 0.26 * | −0.05 | 0.00 | - | −0.03 |
| Alcohol units/week | −0.31 * | −0.04 | −0.05 | −0.06 | 0.10 | −0.03 | - |
| SNP | Genotypes | n (%) | Alleles | n (%) |
|---|---|---|---|---|
| rs1800814 | AA | 37 (28.0) | A | 134 (50.8) |
| AG | 60 (45.5) | G | 130 (49.2) | |
| GG | 35 (26.5) | |||
| AA + AG | 97 (73.5) | |||
| GG + AG | 95 (72.0) | |||
| rs2070958 | CC | 23 (17.4) | C | 102 (38.6) |
| CT | 56 (42.4) | T | 162 (61.4) | |
| TT | 53 (40.2) | |||
| CC + CT | 79 (59.8) | |||
| TT + CT | 109 (82.6) | |||
| rs62433334 | CC | 65 (49.2) | C | 187 (70.8) |
| CG | 57 (43.2) | G | 77 (29.2) | |
| GG | 10 (7.6) | |||
| CC + CG | 122 (92.4) | |||
| GG + CG | 67 (50.8) |
| PROM | Week | Median ± QD in Respective Genotypes | p-Value | |||||
|---|---|---|---|---|---|---|---|---|
| rs1800814 | Kruskal–Wallis | AA vs. AG | AA vs. GG | AG vs. GG | ||||
| AA | AG | GG | ||||||
| QDASH | 8 | 25.00 ± 18.18 | 29.55 ± 15.34 | 45.45 ± 18.18 | 0.049 | 0.892 | 0.047 | 0.294 |
| ΔQDASH | 8 | 18.18 ± 19.87 | 22.73 ± 14.38 | 4.54 ± 20.46 | 0.035 | 1.000 | 0.125 | 0.040 |
| VAS | 12 | 3.00 ± 1.50 | 2.00 ± 1.50 | 4.00 ± 1.50 | 0.039 | 0.582 | 0.816 | 0.038 |
| rs2070958 | Kruskal–Wallis | CC vs. CT | CC vs. TT | CT vs. TT | ||||
| CC | CT | TT | ||||||
| ΔQDASH | 4 | 4.54 ± 13.63 | 14.77 ± 15.34 | 15.90 ± 18.18 | 0.017 | 0.123 | 0.013 | 0.836 |
| QDASH | 8 | 52.27 ± 15.91 | 29.55 ± 14.77 | 29.54 ± 20.45 | 0.014 | 0.026 | 0.018 | 1.000 |
| ΔQDASH | 8 | 2.27 ± 14.77 | 17.04 ± 16.60 | 18.18 ± 18.18 | 0.012 | 0.118 | 0.009 | 0.677 |
| PRTEE | 8 | 33.00 ± 17.25 | 21.75 ± 16 | 19.50 ± 13.50 | 0.042 | 0.105 | 0.043 | 1.000 |
| VAS | 12 | 4.00 ± 1.50 | 2.00 ± 1.50 | 2.00 ± 1.50 | 0.028 | 0.030 | 0.071 | 1.000 |
| QDASH | 12 | 43.18 ± 18.18 | 27.27 ± 13.07 | 25.00 ± 20.45 | 0.008 | 0.008 | 0.020 | 1.000 |
| ΔQDASH | 12 | 0.00 ± 12.50 | 22.72 ± 14.21 | 23.64 ± 19.20 | 0.004 | 0.013 | 0.004 | 1.000 |
| PRTEE | 12 | 36.50 ± 17.50 | 15.75 ± 11.50 | 18.00 ± 13.25 | 0.007 | 0.007 | 0.017 | 1.000 |
| rs62433334 | Kruskal–Wallis | CC vs. CG | CC vs. GG | CG vs. GG | ||||
| CC | CG | GG | ||||||
| ΔQDASH | 104 | 34.09 ± 21.59 | 27.27 ± 22.27 | 52.27 ± 9.09 | 0.031 | 0.295 | 0.369 | 0.044 |
| ΔPRTEE | 104 | 38.50 ± 15.75 | 33.50 ± 15.50 | 55.25 ± 11.25 | 0.035 | 0.650 | 0.189 | 0.034 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jarosz, A.; Szyluk, K.; Iwanicka, J.; Balcerzyk, A.; Nowak, T.; Iwanicki, T.; Negru, M.; Kalita, M.; Francuz, T.; Garczorz, W.; et al. What Role Does PDGFA Gene Polymorphisms Play in Treating Tennis Elbow with PRP? A Prospective Cohort Study. J. Clin. Med. 2022, 11, 3504. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11123504
Jarosz A, Szyluk K, Iwanicka J, Balcerzyk A, Nowak T, Iwanicki T, Negru M, Kalita M, Francuz T, Garczorz W, et al. What Role Does PDGFA Gene Polymorphisms Play in Treating Tennis Elbow with PRP? A Prospective Cohort Study. Journal of Clinical Medicine. 2022; 11(12):3504. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11123504
Chicago/Turabian StyleJarosz, Alicja, Karol Szyluk, Joanna Iwanicka, Anna Balcerzyk, Tomasz Nowak, Tomasz Iwanicki, Marius Negru, Marcin Kalita, Tomasz Francuz, Wojciech Garczorz, and et al. 2022. "What Role Does PDGFA Gene Polymorphisms Play in Treating Tennis Elbow with PRP? A Prospective Cohort Study" Journal of Clinical Medicine 11, no. 12: 3504. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11123504