
Clinical Outcome and Comparison of Regenerative and Apexification Intervention in Young Immature Necrotic Teeth—A Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Study Quality Assessment
3. Results
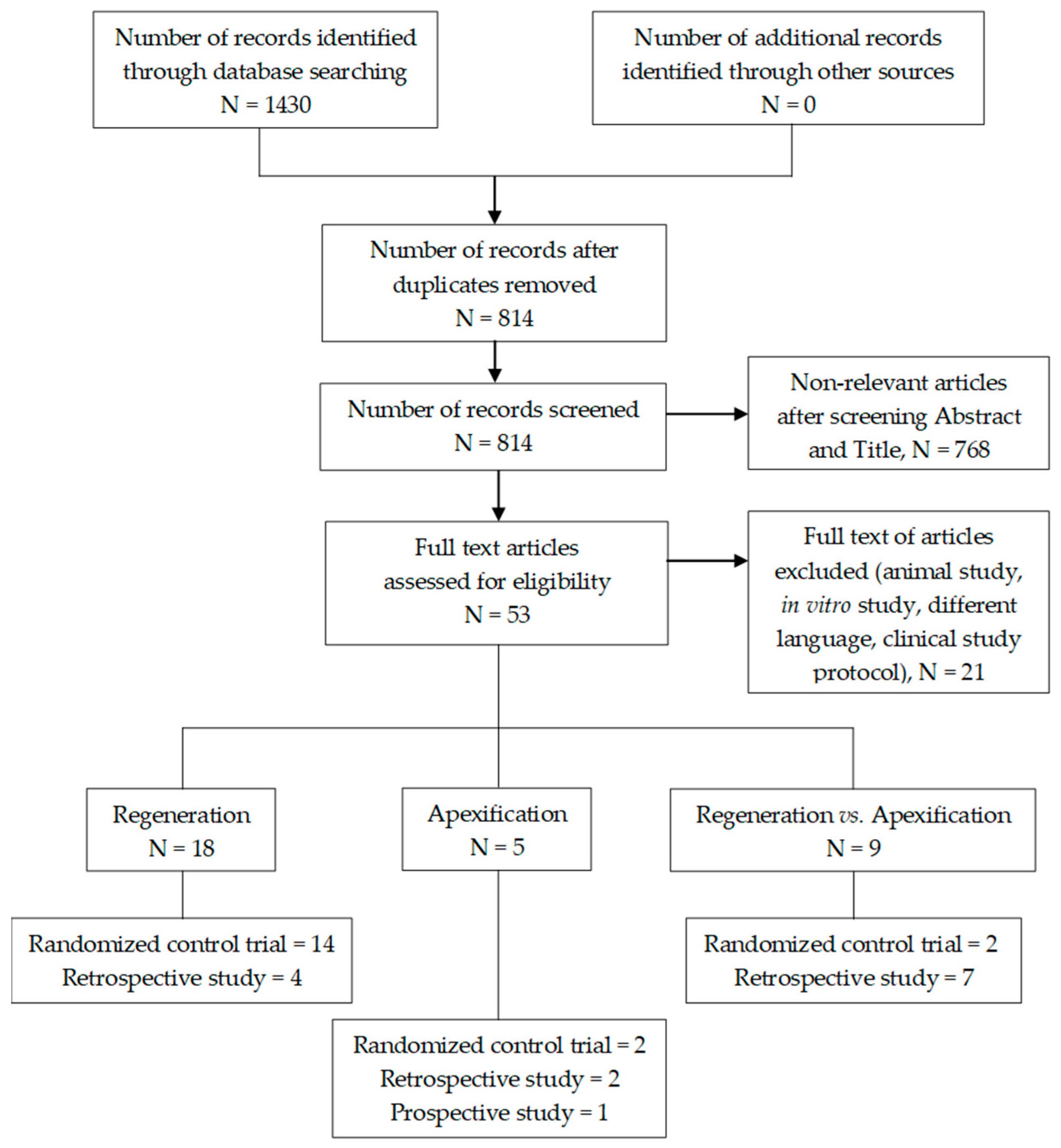
3.1. Selection of Studies
3.2. Characteristics of Studies
3.2.1. Design
3.2.2. Participants
3.2.3. Intervention
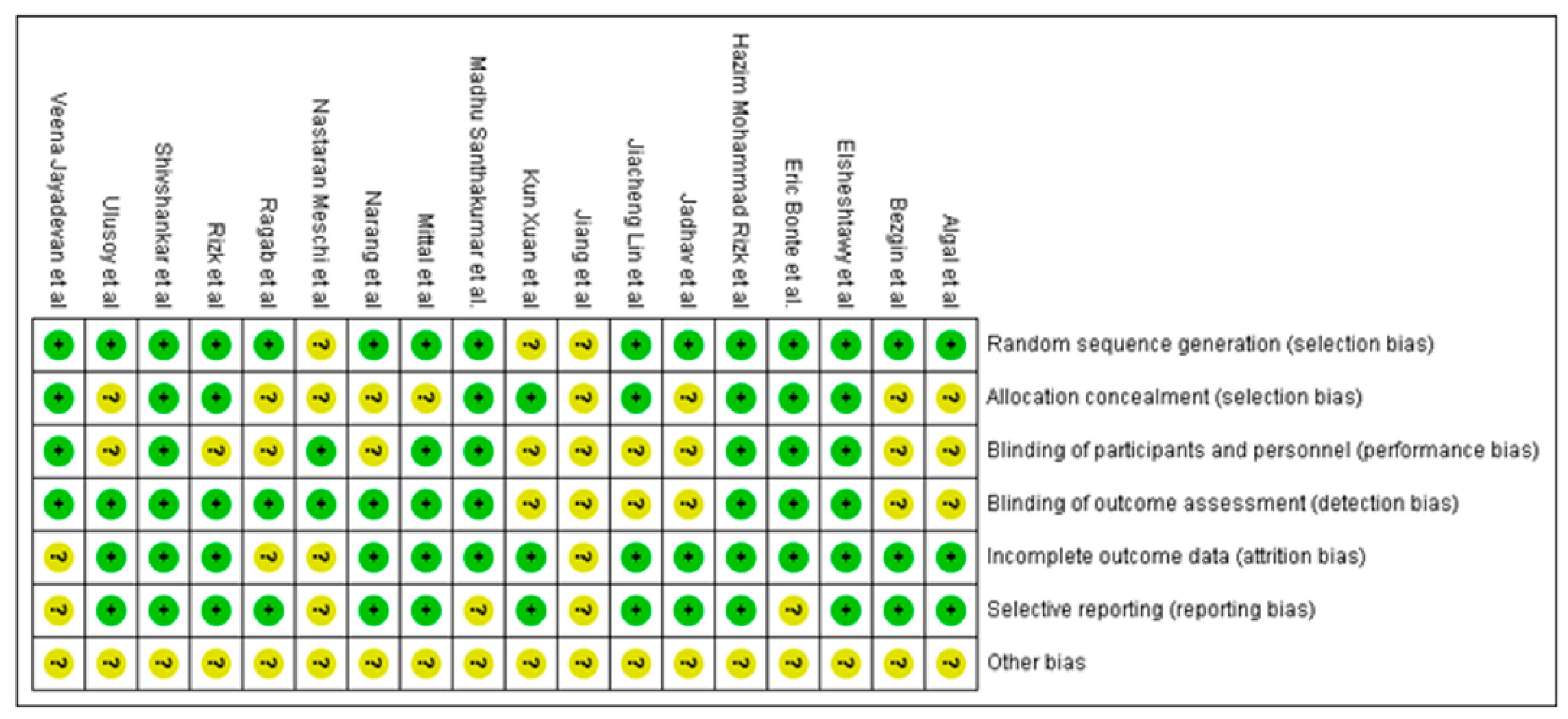
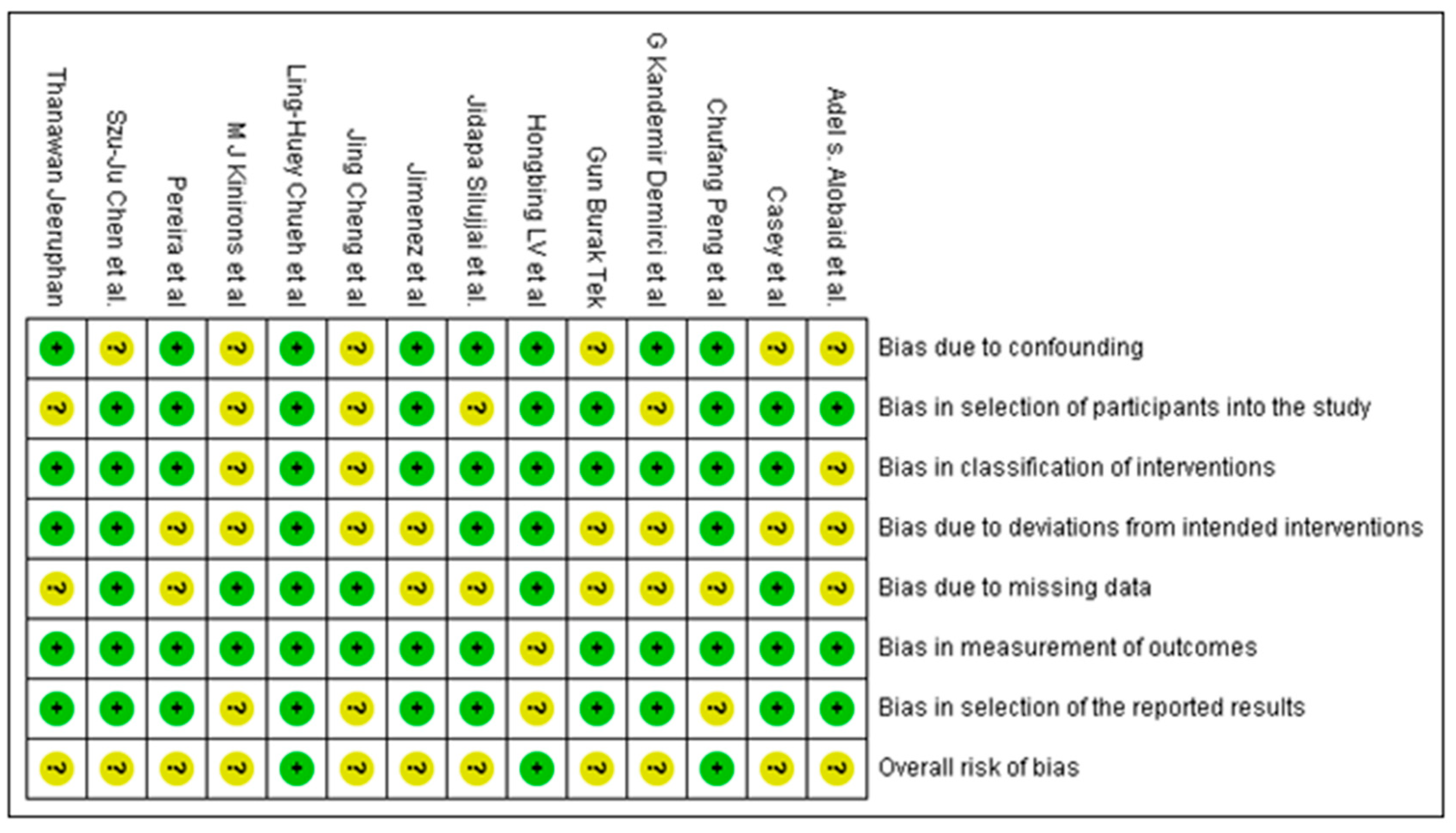
3.3. Analysis of Quality of the Studies
3.4. Synthesis of Results
3.4.1. DWT in REP with APC Compared to BC in Young Immature Permanent Teeth
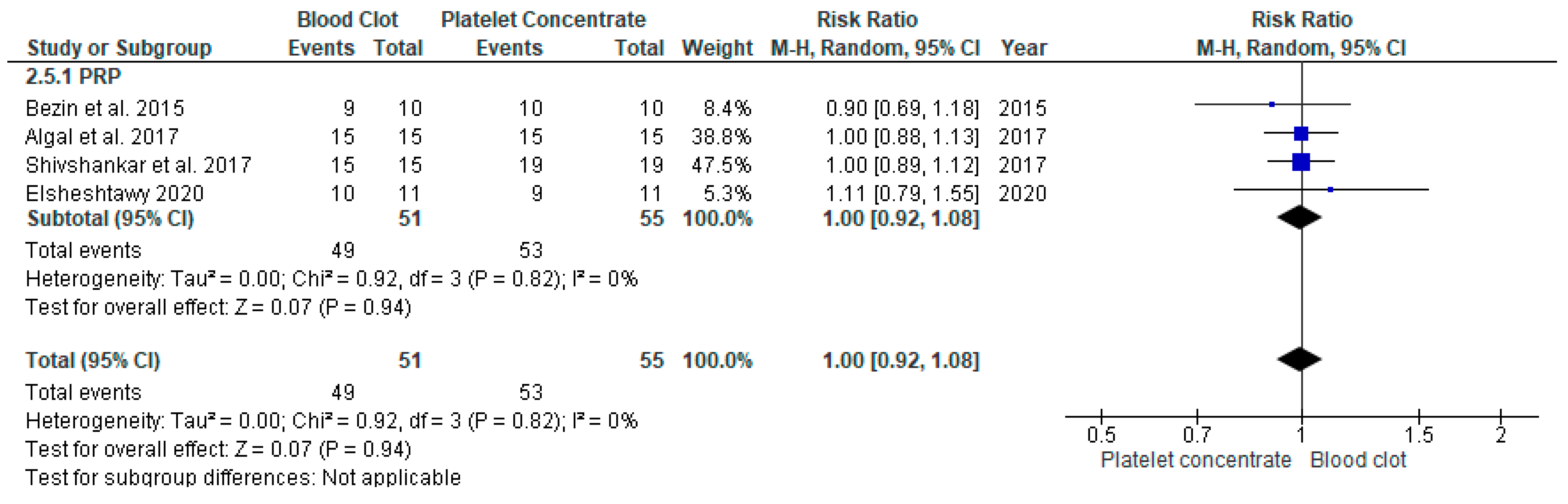
3.4.2. Increased Root Length in REP with APC Compared to BC in Young Immature Permanent Teeth
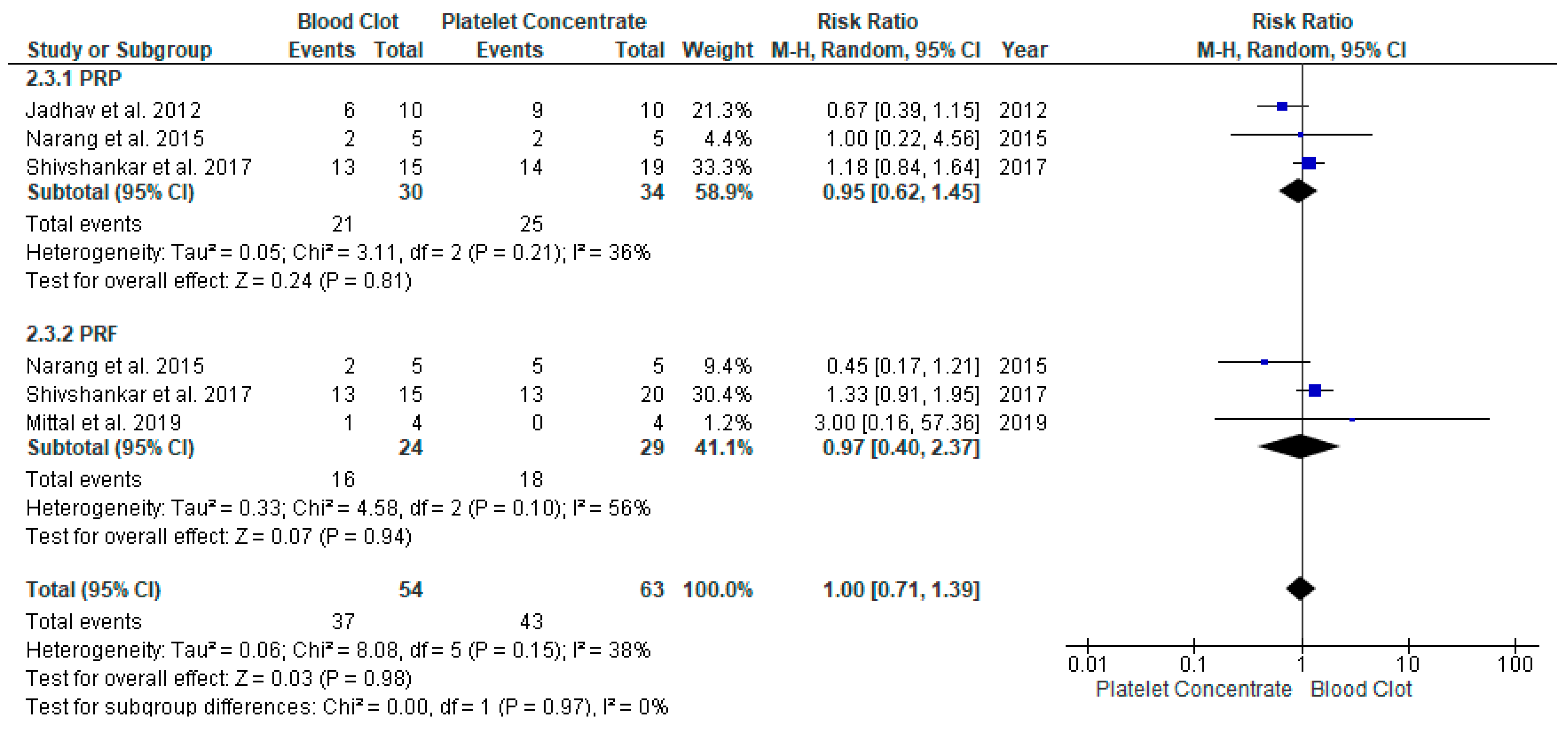
3.4.3. Apical Closure Formation in REP with APC Compared to BC in Young Immature Permanent Teeth
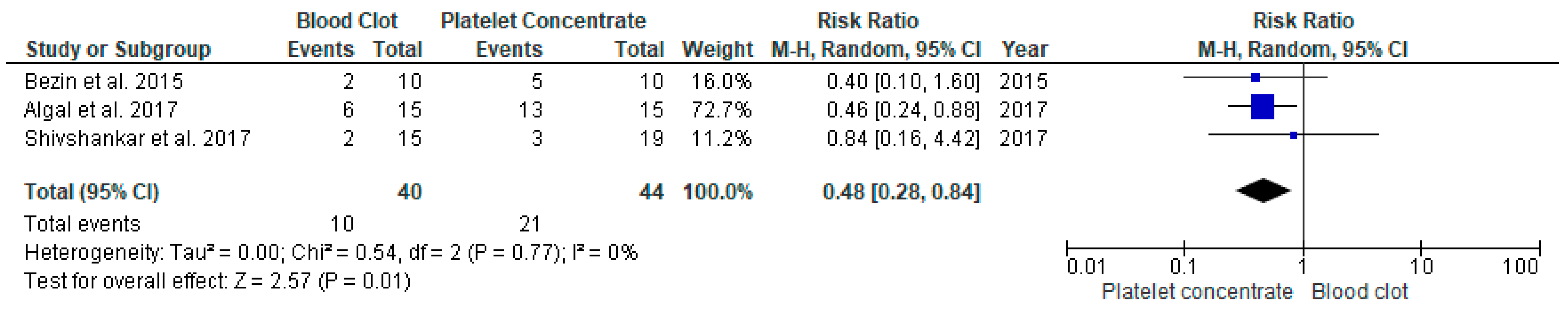
3.4.4. Vitality Response in REP with APC Compared to BC in Young Immature Permanent Teeth
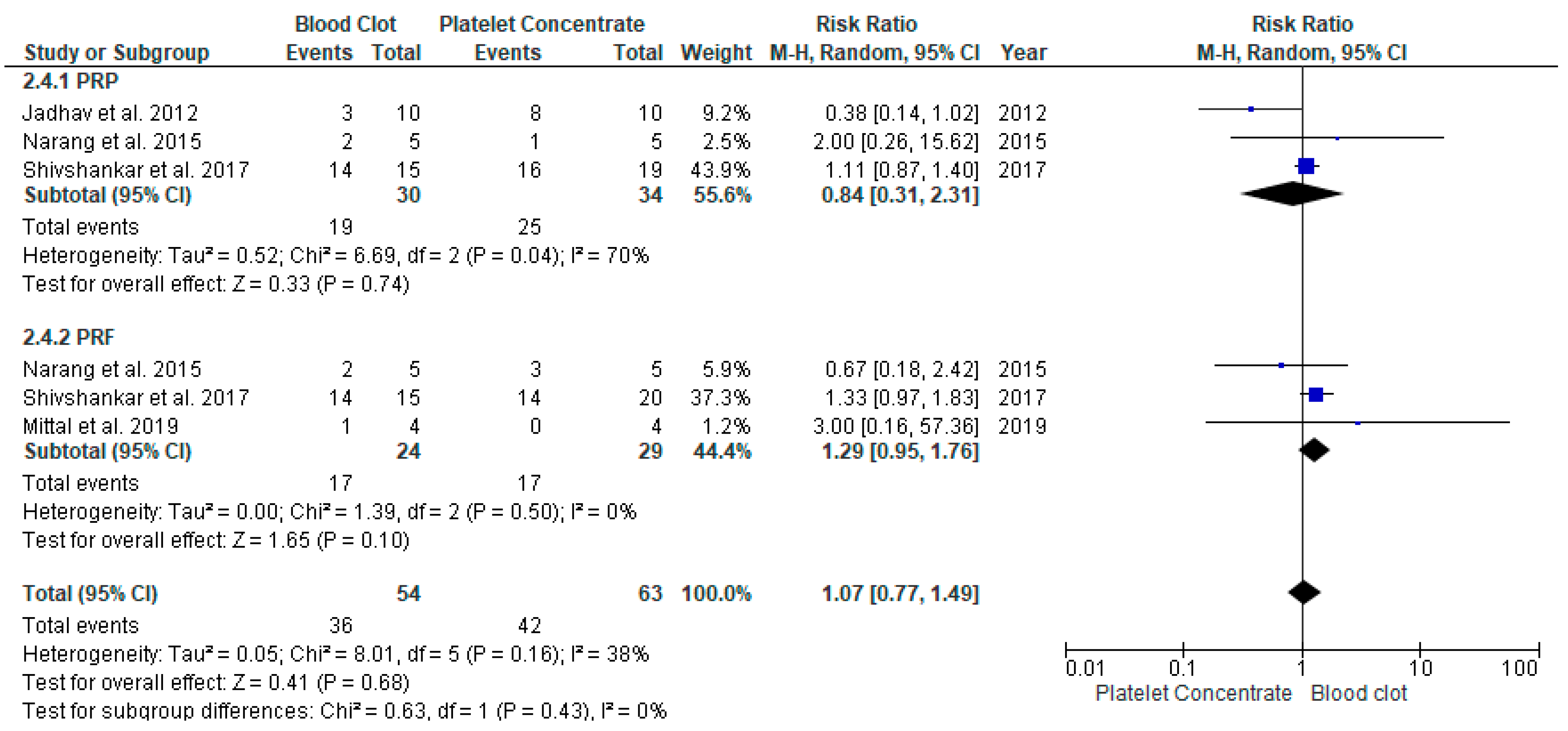
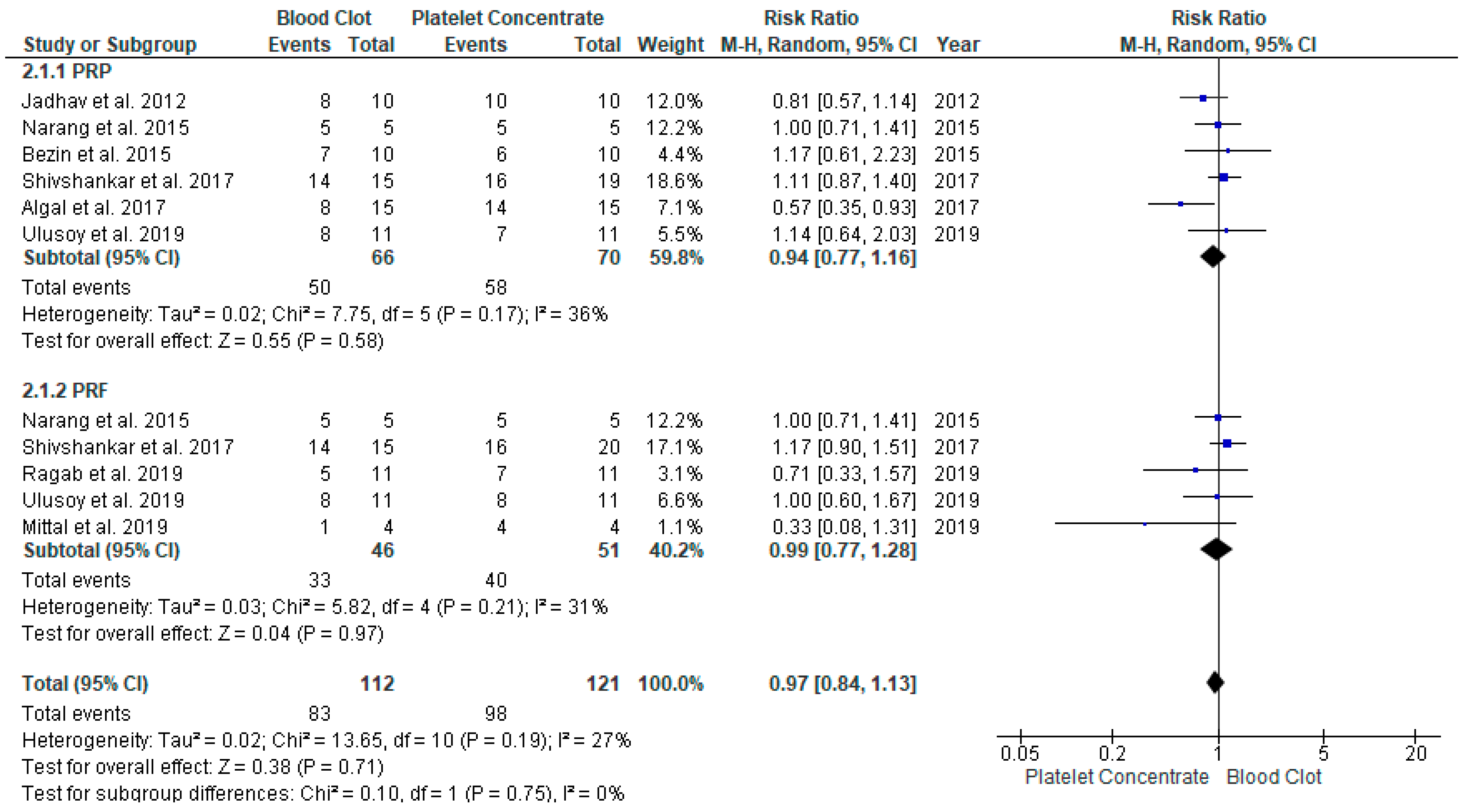
3.4.5. Success Rate of REP with APC Compared to BC in Young Immature Permanent Teeth
3.4.6. Survival Assessment in Young Immature Permanent Teeth Undergone either REP or Apexification Procedure in Young Immature Permanent Teeth
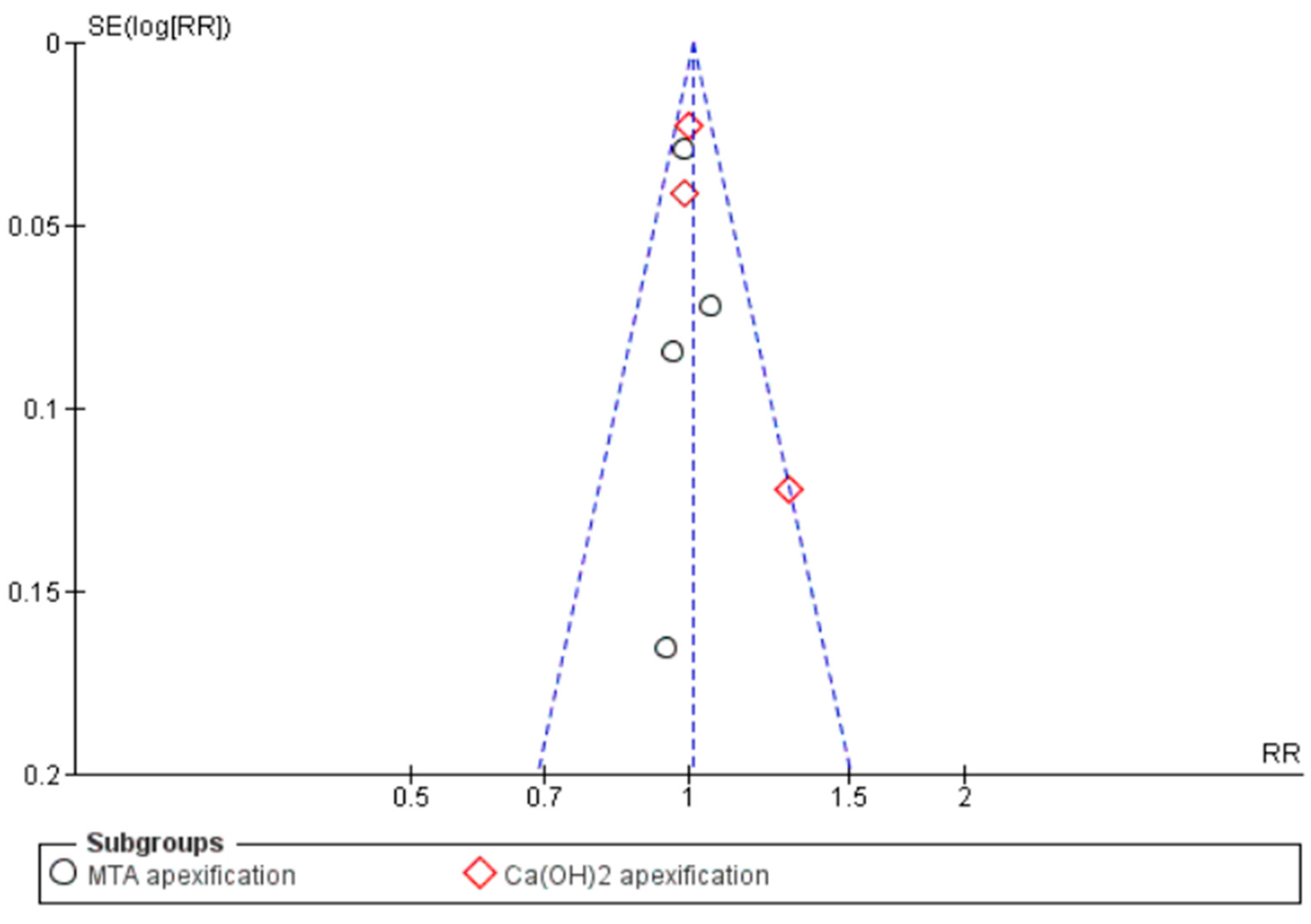
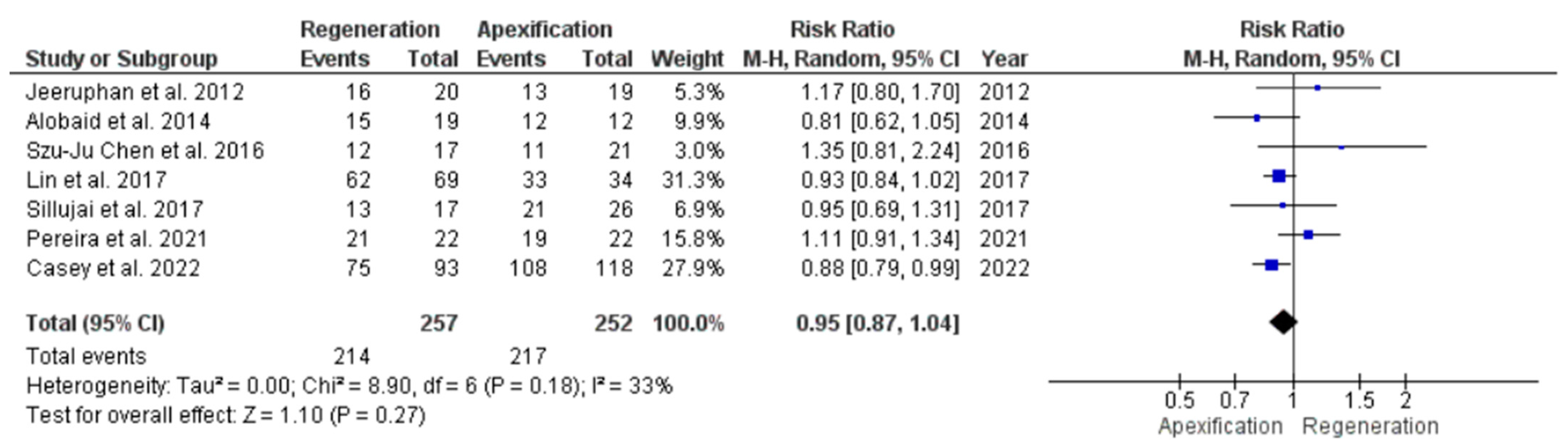
3.4.7. Comparison of Success Rate in Young Immature Permanent Teeth Treated with REP or Apexification Procedure
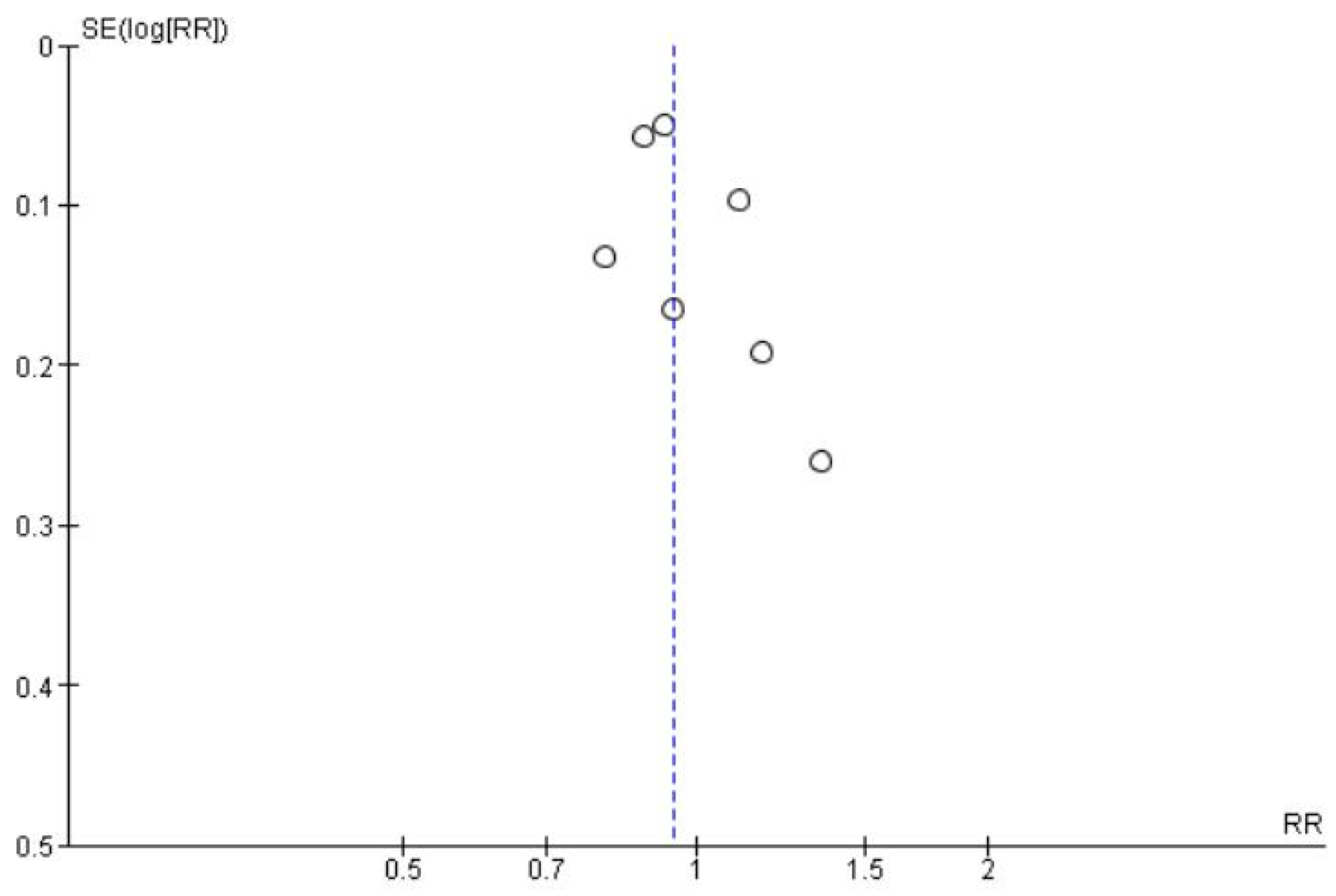
3.4.8. Comparison of Increase in Root Length in Young Immature Permanent Teeth Treated with REP or Apexification Procedure
3.4.9. Comparison of Decrease in Apical Foramen Width in Young Immature Permanent Teeth Treated with REP Or AEP
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Reason for Exclusion |
|---|---|
| Alhaddad Alhamoui et al., 2014 [88] | In vitro study |
| Alkaisi et al., 2013 [89] | Animal study |
| El Arshy et al., 2016 [90] | Animal study |
| El-Tayeb et al., 2019 [91] | Animal study |
| Huang et al., 2013 [92] | Animal study |
| Peng et al., 2017 [93] | Chinese language |
| Jamshidi et al., 2018 [94] | In vitro study |
| Moradi et al., 2016 [95] | Animal study |
| Ok et al., 2015 [96] | In vitro study |
| Pagliarin et al., 2016 [97] | Animal study |
| Rafaei et al., 2020 [98] | In vitro study |
| Ritter AL et al., 2004 [99] | Animal study |
| Sogukpinar et al., 2020 [100] | In vitro study |
| Thibodeau et al., 2007 [101] | In vitro study |
| Valera et al., 2015 [102] | Animal study |
| Yang et al., 2018 [103] | Animal study |
| Yoo et al., 2014 [104] | Animal study |
| Zhang et al., 2014 [105] | Animal study |
| Zuong et al., 2010 [106] | Animal study |
| Beslot-Neveu et al., 2011 [107] | Study protocol |
| Bukhari et al., 2016 [108] | Case series |
References
- Wikström, A.; Brundin, M.; Lopes, M.F.; El Sayed, M.; Tsilingaridis, G. What is the best long-term treatment modality for immature permanent teeth with pulp necrosis and apical periodontitis? Eur. Arch. Paediatr. Dent. 2021, 22, 311–340. [Google Scholar] [CrossRef] [PubMed]
- Locker, D. Self-reported dental and oral injuries in a population of adults aged 18–50 years. Dent. Traumatol. 2007, 23, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Petti, S.; Glendor, U.; Andersson, L. World traumatic dental injury prevalence and incidence, a meta-analysis-One billion living people have had traumatic dental injuries. Off. Publ. Int. Assoc. Dent. Traumatol. Dent. Traumatol. 2018, 34, 71–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hecova, H.; Tzigkounakis, V.; Merglova, V.; Netolický, J. A retrospective study of 889 injured permanent teeth. Dent. Traumatol. 2010, 26, 466–475. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.G.; Malek, M.; Sigurdsson, A.; Lin, L.M.; Kahler, B. Regenerative endodontics: A comprehensive review. Int. Endod. J. 2018, 51, 1367–1388. [Google Scholar] [CrossRef] [PubMed]
- Cvek, M. Prognosis of luxated non-vital maxillary incisors treated with calcium hydroxide and filled with gutta-percha. A retrospective clinical study. Endod. Dent. Traumatol. 1992, 8, 45–55. [Google Scholar] [CrossRef]
- Trope, M. Treatment of the Immature Tooth with a Non–Vital Pulp and Apical Periodontitis. Dent. Clin. N. Am. 2010, 54, 313–324. [Google Scholar] [CrossRef]
- Duggal, M.; Tong, H.J.; Alansary, M.; Twati, W.; Day, P.F.; Nazzal, H. Interventions for the endodontic management of non-vital traumatised immature permanent anterior teeth in children and adolescents: A systematic review of the evidence and guidelines of the European Academy of Paediatric Dentistry. Eur. Arch. Paediatr. Dent. 2017, 18, 139–151. [Google Scholar] [CrossRef]
- Lee, B.-N.; Moon, J.-W.; Chang, H.-S.; Hwang, I.-N.; Oh, W.-M.; Hwang, Y.-C. A review of the regenerative endodontic treatment procedure. Restor. Dent. Endod. 2015, 40, 179–187. [Google Scholar] [CrossRef]
- Rafter, M. Apexification: A review. Dent. Traumatol. 2005, 21, 1–8. [Google Scholar] [CrossRef]
- Murray, P.E.; Garcia-Godoy, F.; Hargreaves, K.M. Regenerative Endodontics: A Review of Current Status and a Call for Action. J. Endod. 2007, 33, 377–390. [Google Scholar] [CrossRef]
- Finucane, D.; Kinirons, M.J. Non-vital immature permanent incisors: Factors that may infIuence treatment outcome. Dent. Traumatol. 1999, 15, 273–277. [Google Scholar] [CrossRef]
- Mackie, I.C.; Bentley, E.M.; Worthington, H.V. The closure of open apices in non-vital immature incisor teeth. Br. Dent. J. 1988, 165, 169–173. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Alagl, A.; Bedi, S.; Hassan, K.; AlHumaid, J. Use of platelet-rich plasma for regeneration in non-vital immature permanent teeth: Clinical and cone-beam computed tomography evaluation. J. Int. Med. Res. 2017, 45, 583–593. [Google Scholar] [CrossRef] [PubMed]
- Bezgin, T.; Yilmaz, A.D.; Celik, B.N.; Kolsuz, M.E.; Sonmez, H. Efficacy of Platelet-rich Plasma as a Scaffold in Regenerative Endodontic Treatment. J. Endod. 2015, 41, 36–44. [Google Scholar] [CrossRef] [PubMed]
- ElSheshtawy, A.S.; Nazzal, H.; El Shahawy, O.I.; El Baz, A.A.; Ismail, S.M.; Kang, J.; Ezzat, K.M. The effect of platelet-rich plasma as a scaffold in regeneration/revitalization endodontics of immature permanent teeth assessed using 2-dimensional radiographs and cone beam computed tomography: A randomized controlled trial. Int. Endod. J. 2020, 53, 905–921. [Google Scholar] [CrossRef] [PubMed]
- Jadhav, G.; Shah, N.; Logani, A. Revascularization with and without Platelet-rich Plasma in Nonvital, Immature, Anterior Teeth: A Pilot Clinical Study. J. Endod. 2012, 38, 1581–1587. [Google Scholar] [CrossRef]
- Rizk, H.M.; Al-Deen, M.S.S.; Emam, A.A. Regenerative Endodontic Treatment of Bilateral Necrotic Immature Permanent Maxillary Central Incisors with Platelet-rich Plasma versus Blood Clot: A Split Mouth Double-blinded Randomized Controlled Trial. Int. J. Clin. Pediatr. Dent. 2019, 12, 332–339. [Google Scholar] [CrossRef]
- Ragab, R.A.; El Lattif, A.E.A.; Dokky, N.A.E.W.E. Comparative Study between Revitalization of Necrotic Immature Permanent Anterior Teeth with and without Platelet Rich Fibrin: A Randomized Controlled Trial. J. Clin. Pediatr. Dent. 2019, 43, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Mittal, N.; Parashar, V. Regenerative Evaluation of Immature Roots Using PRF and Artificial Scaffolds in Necrotic Perma-nent Teeth: A Clinical Study. J. Contemp. Dent. Pract. 2019, 20, 720–726. [Google Scholar] [CrossRef] [PubMed]
- Shivashankar, V.Y.; Johns, D.A.; Maroli, R.K.; Sekar, M.; Chandrasekaran, R.; Karthikeyan, S.; Renganathan, S.K. Comparison of the Effect of PRP, PRF and Induced Bleeding in the Revascularization of Teeth with Necrotic Pulp and Open Apex: A Triple Blind Randomized Clinical Trial. J. Clin. Diagn. Res. 2017, 11, ZC34–ZC39. [Google Scholar] [CrossRef]
- Rizk, H.M.; Al-Deen, M.S.M.S.; Emam, A.A. Comparative evaluation of Platelet Rich Plasma (PRP) versus Platelet Rich Fibrin (PRF) scaffolds in regenerative endodontic treatment of immature necrotic permanent maxillary central incisors: A double blinded randomized controlled trial. Saudi Dent. J. 2020, 32, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Liu, H.; Peng, C. Clinical and Radiographic Assessment of the Efficacy of a Collagen Membrane in Regenerative Endodontics: A Randomized, Controlled Clinical Trial. J. Endod. 2017, 43, 1465–1471. [Google Scholar] [CrossRef]
- Narang, I.; Mittal, N.; Mishra, N. A comparative evaluation of the blood clot, platelet-rich plasma, and platelet-rich fibrin in regeneration of necrotic immature permanent teeth: A clinical study. Contemp. Clin. Dent. 2015, 6, 63–68. [Google Scholar] [CrossRef]
- Meschi, N.; EzEldeen, M.; Garcia, A.E.T.; Lahoud, P.; Van Gorp, G.; Coucke, W.; Jacobs, R.; Vandamme, K.; Teughels, W.; Lambrechts, P. Regenerative Endodontic Procedure of Immature Permanent Teeth with Leukocyte and Platelet-rich Fibrin: A Multicenter Controlled Clinical Trial. J. Endod. 2021, 47, 1729–1750. [Google Scholar] [CrossRef]
- Ulusoy, A.T.; Turedi, I.; Cimen, M.; Cehreli, Z.C. Evaluation of Blood Clot, Platelet-rich Plasma, Platelet-rich Fibrin, and Platelet Pellet as Scaffolds in Regenerative Endodontic Treatment: A Prospective Randomized Trial. J. Endod. 2019, 45, 560–566. [Google Scholar] [CrossRef]
- Peng, C.; Yang, Y.; Zhao, Y.; Liu, H.; Xu, Z.; Zhao, D.; Qin, M. Long-term treatment outcomes in immature permanent teeth by revascularisation using MTA and GIC as canal-sealing materials: A retrospective study. Int. J. Paediatr. Dent. 2017, 27, 454–462. [Google Scholar] [CrossRef]
- Lv, H.; Chen, Y.; Cai, Z.; Lei, L.; Zhang, M.; Zhou, R.; Huang, X. The efficacy of platelet-rich fibrin as a scaffold in regenerative endodontic treatment: A retrospective controlled cohort study. BMC Oral Health 2018, 18, 139. [Google Scholar] [CrossRef]
- Cheng, J.; Yang, F.; Li, J.; Hua, F.; He, M.; Song, G. Treatment Outcomes of Regenerative Endodontic Procedures in Traumatized Immature Permanent Necrotic Teeth: A Retrospective Study. J. Endod. 2022. epub ahead of print. [Google Scholar] [CrossRef]
- Chueh, L.-H.; Ho, Y.-C.; Kuo, T.-C.; Lai, W.-H.; Chen, Y.-H.M.; Chiang, C.-P. Regenerative Endodontic Treatment for Necrotic Immature Permanent Teeth. J. Endod. 2009, 35, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Jayadevan, V.; Gehlot, P.-M.; Manjunath, V.; Madhunapantula, S.V.; Lakshmikanth, J.-S. A comparative evaluation of Advanced Platelet-Rich Fibrin (A-PRF) and Platelet-Rich Fibrin (PRF) as a Scaffold in Regenerative Endodontic Treatment of Traumatized Immature Non-vital permanent anterior teeth: A Prospective clinical study. J. Clin. Exp. Dent. 2021, 13, e463–e472. [Google Scholar] [CrossRef] [PubMed]
- Bonte, E.; Beslot, A.; Boukpessi, T.; Lasfargues, J.-J. MTA versus Ca(OH)2 in apexification of non-vital immature permanent teeth: A randomized clinical trial comparison. Clin. Oral Investig. 2015, 19, 1381–1388. [Google Scholar] [CrossRef] [PubMed]
- Santhakumar, M.; Yayathi, S.; Retnakumari, N. A clinicoradiographic comparison of the effects of platelet-rich fibrin gel and platelet-rich fibrin membrane as scaffolds in the apexification treatment of young permanent teeth. J. Indian Soc. Pedod. Prev. Dent. 2018, 36, 65–70. [Google Scholar]
- Demirci, G.K.; Kaval, M.E.; Güneri, P.; Çalışkan, M.K. Treatment of immature teeth with nonvital pulps in adults: A prospective comparative clinical study comparing MTA with Ca(OH)2. Int. Endod. J. 2020, 53, 5–18. [Google Scholar] [CrossRef] [PubMed]
- Tek, G.B.; Keskin, G. Use of Mineral Trioxide Aggregate with or without a Collagen Sponge as an Apical Plug in Teeth with Immature Apices. J. Clin. Pediatr. Dent. 2021, 45, 165–170. [Google Scholar] [CrossRef]
- Kinirons, M.J.; Srinivasan, V.; Welbury, R.R.; Finucane, D. A study in two centres of variations in the time of apical barrier detection and barrier position in nonvital immature permanent incisors. Int. J. Paediatr. Dent. 2001, 11, 447–451. [Google Scholar] [CrossRef]
- Lin, J.; Zeng, Q.; Wei, X.; Zhao, W.; Cui, M.; Gu, J.; Lu, J.; Yang, M.; Ling, J. Regenerative Endodontics Versus Apexification in Immature Permanent Teeth with Apical Periodontitis: A Prospective Randomized Controlled Study. J. Endod. 2017, 43, 1821–1827. [Google Scholar] [CrossRef]
- Xuan, K.; Li, B.; Guo, H.; Sun, W.; Kou, X.; He, X.; Zhang, Y.; Sun, J.; Liu, A.; Liao, L.; et al. Deciduous autologous tooth stem cells regenerate dental pulp after implantation into injured teeth. Sci. Transl. Med. 2018, 10, eaaf3227. [Google Scholar] [CrossRef] [Green Version]
- Alobaid, A.S.; Cortes, L.M.; Lo, J.; Nguyen, T.T.; Albert, J.; Abu-Melha, A.S.; Lin, L.M.; Gibbs, J.L. Radiographic and Clinical Outcomes of the Treatment of Immature Permanent Teeth by Revascularization or Apexification: A Pilot Retrospective Cohort Study. J. Endod. 2014, 40, 1063–1070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casey, S.M.; Fox, D.; Duong, W.; Bui, N.; Latifi, N.; Ramesh, V.; Podborits, E.; Flake, N.M.; Khan, A.A.; Gibbs, J.L. Patient Centered Outcomes among a Cohort Receiving Regenerative Endodontic Procedures or Apexification Treatments. J. Endod. 2022, 48, 345–354. [Google Scholar] [CrossRef] [PubMed]
- Caleza-Jiménez, C.; Ribas-Pérez, D.; Biedma-Perea, M.; Solano-Mendoza, B.; Mendoza-Mendoza, A. Radiographic differences observed following apexification vs revascularization in necrotic immature molars and incisors: A follow-up study of 18 teeth. Eur. Arch. Paediatr. Dent. Off. J. Eur. Acad. Paediatr. Dent. 2022, 23, 381–389. [Google Scholar] [CrossRef] [PubMed]
- Pereira, A.C.; Oliveira, M.L.; Cerqueira-Neto, A.C.C.L.; Vargas-Neto, J.; Nagata, J.Y.; Gomes, B.P.; Ferraz, C.C.R.; de Almeida, J.F.A.; De-Jesus-Soares, A. Outcomes of traumatised immature teeth treated with apexification or regenerative endodontic procedure: A retrospective study. Aust. Endod. J. 2020, 47, 178–187. [Google Scholar] [CrossRef]
- Jeeruphan, T.; Jantarat, J.; Yanpiset, K.; Suwannapan, L.; Khewsawai, P.; Hargreaves, K.M. Mahidol Study 1: Comparison of Radiographic and Survival Outcomes of Immature Teeth Treated with Either Regenerative Endodontic or Apexification Methods: A Retrospective Study. J. Endod. 2012, 38, 1330–1336. [Google Scholar] [CrossRef]
- Silujjai, J.; Linsuwanont, P. Treatment Outcomes of Apexification or Revascularization in Nonvital Immature Permanent Teeth: A Retrospective Study. J. Endod. 2017, 43, 238–245. [Google Scholar] [CrossRef]
- Chen, S.-J.; Chen, L.-P. Radiographic outcome of necrotic immature teeth treated with two endodontic techniques: A retrospective analysis. Biomed. J. 2016, 39, 366–371. [Google Scholar] [CrossRef] [Green Version]
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.J.; Mouhyi, J.; Gogly, B. Platelet-rich fibrin (PRF): A second generation platelet concentrate—part I: Technological concepts and evolution. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, e37–e44. [Google Scholar] [CrossRef]
- Dohan, D.M.; Choukroun, J. PRP, cPRP, PRF, PRG, PRGF, FC … How to find your way in the jungle of platelet concentrates? Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 103, 305–306. [Google Scholar] [CrossRef]
- Choukroun, J.; Diss, A.; Simonpieri, A.; Girard, M.O.; Schoeffler, C.; Dohan, S.L.; Dohan, A.J.; Mouhyi, J.; Dohan, D.M. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part V: Histologic evaluations of PRF effects on bone allograft maturation in sinus lift. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, 299–303. [Google Scholar]
- Saber, S.E.-D.M. Tissue engineering in endodontics. J. Oral Sci. 2009, 51, 495–507. [Google Scholar] [CrossRef] [Green Version]
- Taweewattanapaisan, P.; Jantarat, J.; Ounjai, P.; Janebodin, K. The Effects of EDTA on Blood Clot in Regenerative Endodontic Procedures. J. Endod. 2019, 45, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Metlerska, J.; Fagogeni, I.; Nowicka, A. Efficacy of Autologous Platelet Concentrates in Regenerative Endodontic Treatment: A Systematic Review of Human Studies. J. Endod. 2019, 45, 20–30.e1. [Google Scholar] [CrossRef] [PubMed]
- Del Fabbro, M.; Lolato, A.; Bucchi, C.; Taschieri, S.; Weinstein, R.L. Autologous Platelet Concentrates for Pulp and Dentin Regeneration: A Literature Review of Animal Studies. J. Endod. 2016, 42, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Ezzatt, O.M. Autologous Platelet Concentrate Preparations in Dentistry. Biomed. J. Sci. Tech. Res. 2018, 8. [Google Scholar] [CrossRef]
- Giannini, S.; Cielo, A.; Bonanome, L.; Rastelli, C.; Derla, C.; Corpaci, F.; Falisi, G. Comparison between PRP, PRGF and PRF: Lights and shadows in three similar but different protocols. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 927–930. [Google Scholar]
- Goel, D.S.; Sinha, D.D.J.; Singh, D.U.P.; Jaiswal, D.N. Advancements in Regenerative Endodontics: Platelet-Rich Plasma (PRP) And Platelet-Rich Fibrin (PRF). Int. J. Curr. Res. 2019, 11, 5. [Google Scholar]
- Koç, S.; Del Fabbro, M. Does the Etiology of Pulp Necrosis Affect Regenerative Endodontic Treatment Outcomes? A Systematic Review and Meta-analyses. J. Évid. Based Dent. Pract. 2020, 20, 101400. [Google Scholar] [CrossRef]
- Tong, H.J.; Rajan, S.; Bhujel, N.; Kang, J.; Duggal, M.; Nazzal, H. Regenerative Endodontic Therapy in the Management of Nonvital Immature Permanent Teeth: A Systematic Review—Outcome Evaluation and Meta-analysis. J. Endod. 2017, 43, 1453–1464. [Google Scholar] [CrossRef]
- Regenerative Endodontics Clinical Newsletter—AAE. Am. Assoc. Endodontists. Available online: https://www.aae.org/specialty/newsletter/regenerative-endodontics/ (accessed on 26 July 2021).
- Martin, D.E.; De Almeida, J.F.A.; Henry, M.A.; Khaing, Z.Z.; Schmidt, C.E.; Teixeira, F.B.; Diogenes, A. Concentration-dependent Effect of Sodium Hypochlorite on Stem Cells of Apical Papilla Survival and Differentiation. J. Endod. 2014, 40, 51–55. [Google Scholar] [CrossRef]
- Galler, K.M.; Widbiller, M.; Buchalla, W.; Eidt, A.; Hiller, K.-A.; Hoffer, P.C.; Schmalz, G. EDTA conditioning of dentine promotes adhesion, migration and differentiation of dental pulp stem cells. Int. Endod. J. 2016, 49, 581–590. [Google Scholar] [CrossRef] [PubMed]
- Pai, A.V.; Pai, S.; Thomas, M.S.; Bhat, V. Effect of calcium hydroxide and triple antibiotic paste as intracanal medicaments on the incidence of inter-appointment flare-up in diabetic patients: An in vivo study. J. Conserv. Dent. 2014, 17, 208–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahhal, J.G.; Rovai, E.D.S.; Holzhausen, M.; Caldeira, C.L.; Dos Santos, C.F.; Sipert, C.R. Root canal dressings for revascularization influence in vitro mineralization of apical papilla cells. J. Appl. Oral Sci. Rev. FOB 2019, 27, e20180396. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-H.; Kim, Y.; Shin, S.-J.; Park, J.-W.; Jung, I.Y. Tooth Discoloration of Immature Permanent Incisor Associated with Triple Antibiotic Therapy: A Case Report. J. Endod. 2010, 36, 1086–1091. [Google Scholar] [CrossRef]
- Panda, S.; Mishra, L.; Arbildo-Vega, H.I.; Lapinska, B.; Lukomska-Szymanska, M.; Khijmatgar, S.; Parolia, A.; Bucchi, C.; Del Fabbro, M. Effectiveness of Autologous Platelet Concentrates in Management of Young Immature Necrotic Permanent Teeth—A Systematic Review and Meta-Analysis. Cells 2020, 9, 2241. [Google Scholar] [CrossRef]
- Management of Non-Vital Permanent Teeth with Incomplete Root Formation. Available online: https://ukdiss.com/examples/non-vital-permanent-teeth-incomplete-root.php (accessed on 26 July 2021).
- Kleier, D.J.; Barr, E.S. A study of endodontically apexified teeth. Dent. Traumatol. 1991, 7, 112–117. [Google Scholar] [CrossRef]
- Hargreaves, K.M.; Diogenes, A.; Teixeira, F.B. Treatment options: Biological basis of regenerative endodontic procedures. Pediatr. Dent. 2013, 35, 129–140. [Google Scholar] [CrossRef] [Green Version]
- Banchs, F.; Trope, M. Revascularization of Immature Permanent Teeth with Apical Periodontitis: New Treatment Protocol? J. Endod. 2004, 30, 196–200. [Google Scholar] [CrossRef]
- Iwaya, S.-I.; Ikawa, M.; Kubota, M. Revascularization of an immature permanent tooth with periradicular abscess after luxation. Dent. Traumatol. 2011, 27, 55–58. [Google Scholar] [CrossRef]
- Tong, H.J.; Sim, Y.F.; Berdouses, E.; Al-Jundi, S.; El Shahawy, O.; Nazzal, H. Regenerative endodontic therapy (RET) for managing immature non-vital teeth: Experiences and opinions of paediatric dental practitioners in the European and Arabian regions. Eur. Arch. Paediatr. Dent. 2021, 22, 145–155. [Google Scholar] [CrossRef]
- Kobayashi, E.; Flückiger, L.; Fujioka-Kobayashi, M.; Sawada, K.; Sculean, A.; Schaller, B.; Miron, R.J. Comparative release of growth factors from PRP, PRF, and advanced-PRF. Clin. Oral Investig. 2016, 20, 2353–2360. [Google Scholar] [CrossRef] [PubMed]
- Savović, J.; Turner, R.M.; Mawdsley, D.; Jones, H.E.; Beynon, R.; Higgins, J.P.T.; Sterne, J.A.C. Association between Risk-of-Bias Assessments and Results of Randomized Trials in Cochrane Reviews: The ROBES Meta-Epidemiologic Study. Am. J. Epidemiol. 2018, 187, 1113–1122. [Google Scholar] [CrossRef] [PubMed]
- Vidal, K.; Martin, G.; Lozano, O.; Salas, M.; Trigueros, J.; Aguilar, G. Apical Closure in Apexification: A Review and Case Report of Apexification Treatment of an Immature Permanent Tooth with Biodentine. J. Endod. 2016, 42, 730–734. [Google Scholar] [CrossRef] [PubMed]
- Shabahang, S. Treatment options: Apexogenesis and apexification. Pediatr. Dent. 2013, 35, 125–128. [Google Scholar] [CrossRef]
- Holden, D.T.; Schwartz, S.A.; Kirkpatrick, T.C.; Schindler, W.G. Clinical Outcomes of Artificial Root-end Barriers with Mineral Trioxide Aggregate in Teeth with Immature Apices. J. Endod. 2008, 34, 812–817. [Google Scholar] [CrossRef]
- Apexification—An Overview | ScienceDirect Topics. Available online: https://0-www-sciencedirect-com.brum.beds.ac.uk/topics/medicine-and-dentistry/apexification (accessed on 21 June 2021).
- Guerrero, F.; Mendoza, A.; Ribas, D.; Aspiazu, K. Apexification: A systematic review. J. Conserv. Dent. 2018, 21, 462–465. [Google Scholar] [CrossRef]
- Mohammadi, Z.; Dummer, P.M.H. Properties and applications of calcium hydroxide in endodontics and dental traumatology. Int. Endod. J. 2011, 44, 697–730. [Google Scholar] [CrossRef]
- Kunert, M.; Lukomska-Szymanska, M. Bio-Inductive Materials in Direct and Indirect Pulp Capping—A Review Article. Materials 2020, 13, 1204. [Google Scholar] [CrossRef] [Green Version]
- Sood, R.; Hans, M.K.; Shetty, S. Apical barrier technique with mineral trioxide aggregate using internal matrix: A case report. Compend. Contin. Educ. Dent. 2012, 33, e88–e90. [Google Scholar]
- Shokouhinejad, N.; Khoshkhounejad, M.; Alikhasi, M.; Bagheri, P.; Camilleri, J. Prevention of coronal discoloration induced by regenerative endodontic treatment in an ex vivo model. Clin. Oral Investig. 2018, 22, 1725–1731. [Google Scholar] [CrossRef] [Green Version]
- Sharma, V.; Srinivasan, A.; Nikolajeff, F.; Kumar, S. Biomineralization process in hard tissues: The interaction complexity within protein and inorganic counterparts. Acta Biomater. 2021, 120, 20–37. [Google Scholar] [CrossRef] [PubMed]
- Nicoloso, G.F.; Goldenfum, G.M.; Pizzol, T.D.S.D.; Scarparo, R.K.; Montagner, F.; Rodrigues, J.D.A.; Casagrande, L. Pulp Revascularization or Apexification for the Treatment of Immature Necrotic Permanent Teeth: Systematic Review and Meta-Analysis. J. Clin. Pediatr. Dent. 2019, 43, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Becerra, P.; Ricucci, D.; Loghin, S.; Gibbs, J.L.; Lin, L.M. Histologic Study of a Human Immature Permanent Premolar with Chronic Apical Abscess after Revascularization/Revitalization. J. Endod. 2014, 40, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.Y.-H.; Chen, K.-L.; Chen, C.-A.; Tayebaty, F.; Rosenberg, P.A.; Lin, L.M. Responses of immature permanent teeth with infected necrotic pulp tissue and apical periodontitis/abscess to revascularization procedures. Int. Endod. J. 2012, 45, 294–305. [Google Scholar] [CrossRef] [PubMed]
- Alhamoui, F.A.; Steffen, H.; Splieth, C.H. The sealing ability of ProRoot MTA when placed as an apical barrier using three different techniques: An in-vitro apexification model. Quintessence Int. Berl. Ger. 1985, 45, 821–827. [Google Scholar] [CrossRef]
- Alkaisi, A.; Ismail, A.R.; Mutum, S.S.; Ahmad, Z.A.R.; Masudi, S.; Razak, N.H.A. Transplantation of Human Dental Pulp Stem Cells: Enhance Bone Consolidation in Mandibular Distraction Osteogenesis. J. Oral Maxillofac. Surg. 2013, 71, 1758.e1–1758.e13. [Google Scholar] [CrossRef]
- El Ashry, S.H.; Abu-Seida, A.M.; Bayoumi, A.A.; Hashem, A.A. Regenerative potential of immature permanent non-vital teeth following different dentin surface treatments. Exp. Toxicol. Pathol. 2016, 68, 181–190. [Google Scholar] [CrossRef]
- El-Tayeb, M.M.; Abu-Seida, A.M.; El Ashry, S.; El-Hady, S.A. Evaluation of antibacterial activity of propolis on regenerative potential of necrotic immature permanent teeth in dogs. BMC Oral Health 2019, 19, 174. [Google Scholar] [CrossRef] [Green Version]
- Huang, R.; Liu, P.; Xiao, M.; Zhou, Z. A comparative study on apexification using different kinds of materials in dogs. Hua Xi Kou Qiang Yi Xue Za Zhi = Huaxi Kouqiang Yixue Zazhi = WNort. China J. Stomatol. 2013, 31, 377–388. [Google Scholar]
- Peng, C.F.; Zhao, Y.M.; Yang, Y.; Liu, H.; Qin, M. Retrospective analysis of pulp revascularization in immature permanent teeth with diffuse pulpitis. Zhonghua Kou Qiang Yi Xue Za Zhi = Zhonghua Kouqiang Yixue Zazhi = Chin. J. Stomatol. 2017, 52, 10–15. [Google Scholar]
- Jamshidi, D.; Homayouni, H.; Majd, N.M.; Shahabi, S.; Arvin, A.; Ranjbaromidi, B. Impact and Fracture Strength of Simulated Immature Teeth Treated with Mineral Trioxide Aggregate Apical Plug and Fiber Post Versus Revascularization. J. Endod. 2018, 44, 1878–1882. [Google Scholar] [CrossRef] [PubMed]
- Moradi, S.; Talati, A.; Forghani, M.; Jafarian, A.H.; Naseri, M.; Shojaeian, S. Immunohistological Evaluation of Revascularized Immature Permanent Necrotic Teeth Treated by Platelet-Rich Plasma: An Animal Investigation. Cell J. 2016, 18, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Ok, E.; Altunsoy, M.; Tanriver, M.; Çapar, I.D. Effectiveness of different irrigation protocols on calcium hydroxide removal from simulated immature teeth after apexification. Acta Biomater. Odontol. Scand. 2015, 1, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagliarin, C.M.L.; Londero, C.D.L.D.; Felippe, M.C.S.; Felippe, W.T.; Danesi, C.C.; Barletta, F.B. Tissue characterization following revascularization of immature dog teeth using different disinfection pastes. Braz. Oral Res. 2016, 30. [Google Scholar] [CrossRef]
- Jahromi, M.Z.; Refaei, P.; Moughari, A.A.K. Comparison of the microleakage of mineral trioxide aggregate, calcium-enriched mixture cement, and Biodentine orthograde apical plug. Dent. Res. J. 2020, 17, 66. [Google Scholar] [CrossRef]
- Ritter, A.L.D.S.; Ritter, A.V.; Murrah, V.; Sigurdsson, A.; Trope, M. Pulp revascularization of replanted immature dog teeth after treatment with minocycline and doxycycline assessed by laser Doppler flowmetry, radiography, and histology. Dent. Traumatol. 2004, 20, 75–84. [Google Scholar] [CrossRef]
- Sogukpinar, A.; Arikan, V. Comparative evaluation of four endodontic biomaterials and calcium hydroxide regarding their effect on fracture resistance of simulated immature teeth. Huaxi Kouqiang Yixue Zazhi W. Chin. J. Stomatol. 2020, 21, 23–28. [Google Scholar] [CrossRef]
- Thibodeau, B.; Teixeira, F.; Yamauchi, M.; Caplan, D.J.; Trope, M. Pulp Revascularization of Immature Dog Teeth with Apical Periodontitis. J. Endod. 2007, 33, 680–689. [Google Scholar] [CrossRef] [Green Version]
- Valera, M.C.; Albuquerque, M.T.P.; Yamasaki, M.C.; Vassallo, F.N.S.; da Silva, D.; Nagata, J.Y. Fracture resistance of weakened bovine teeth after long-term use of calcium hydroxide. Dent. Traumatol. 2015, 31, 385–389. [Google Scholar] [CrossRef]
- Yang, J.; Wang, W.J.; Jia, W.Q.; Zhao, Y.M.; Ge, L.H. Effect of exogenous stem cells from apical papillae in the pulp re-vascularization treatment for the immature permanent tooth with periapical periodontitis. Zhonghua Kou Qiang Yi Xue Za Zhi = Zhonghua Kouqiang Yixue Zazhi = Chin. J. Stomatol. 2018, 53, 459–465. [Google Scholar] [CrossRef]
- Yoo, Y.-J.; Lee, W.; Cho, Y.-A.; Park, J.-C.; Shon, W.-J.; Baek, S.-H. Effect of Conditioned Medium from Preameloblasts on Regenerative Cellular Differentiation of the Immature Teeth with Necrotic Pulp and Apical Periodontitis. J. Endod. 2014, 40, 1355–1361. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.-D.; Chen, X.; Bao, Z.-F.; Chen, M.; Ding, Z.-J.; Zhong, M. Histologic Comparison between Platelet-rich Plasma and Blood Clot in Regenerative Endodontic Treatment: An Animal Study. J. Endod. 2014, 40, 1388–1393. [Google Scholar] [CrossRef] [PubMed]
- Zuong, X.-Y.; Yang, Y.-P.; Chen, W.-X.; Zhang, Y.-J.; Wen, C.-M. [Pulp revascularization of immature anterior teeth with apical periodontitis]. Hua Xi Kou Qiang Yi Xue Za Zhi = Huaxi Kouqiang Yixue Zazhi = W. Chin. J. Stomatol. 2010, 28, 672–674. [Google Scholar]
- Beslot-Neveu, A.; Bonte, E.; Baune, B.; Serreau, R.; Aissat, F.; Quinquis, L.; Grabar, S.; Lasfargues, J.-J. Mineral trioxyde aggregate versus calcium hydroxide in apexification of non vital immature teeth: Study protocol for a randomized controlled trial. Trials 2011, 12, 174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bukhari, S.; Kohli, M.R.; Setzer, F.; Karabucak, B. Outcome of Revascularization Procedure: A Retrospective Case Series. J. Endod. 2016, 42, 1752–1759. [Google Scholar] [CrossRef] [PubMed]














| Search Strategy |
|---|
| #1 immature teeth/immature tooth/immature permanent tooth/immature permanent teeth/young permanent tooth/young permanent dentition |
| #2 pulp revascularization/pulp regeneration/pulp revitalization/PRF/PRP/blood clot |
| #3 apexification/calcific barrier/apical closure/root end closure/root apex closure/root end formation/root apex closure/apical plug/MTA plug |
| #4 survival rate/dentinal thickness/pulp vitality/root completion/successful rate/periapical healing/decrease in apical foramen width |
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Study design: Randomized controlled trials, clinical studies, observational studies (Retrospective study) | Case reports, comments, conference proceedings |
| Patients with immature necrotic permanent teeth | Studies experimenting on vital teeth |
| Studies in which either one of the interventions or both are compared | Animal studies, case reports, in vitro studies, laboratory studies |
| Articles published in English language |
| Author | Etiology of Pulp Necrosis | Presence of Periapical Lesion | Instrumentation | Irrigation Method | Intracanal Medication | Recall Time (in Weeks) | Preparation Protocol of APC | Access Restoration |
|---|---|---|---|---|---|---|---|---|
| Alagl et al., 2017 [16] | Secondary to trauma/caries | Yes | No | 2.5% NaOCl (20 mL), sterile saline (20 mL), and 0.12% CHX (10 mL), followed by 17% EDTA after 3 weeks | TAP | 3 | PRP was prepared according to the description by Dohan et al. [48]. PRP was combined with equal volumes of sterile solution containing 10% calcium chloride and sterile bovine thrombin (100 U/mL) to achieve coagulation. | NR |
| Bezgin et al., 2015 [17] | Secondary to trauma/caries | Yes | No | 2.5% NaOCl (20 mL), sterile saline (20 mL), and 0.12% CHX (10 mL), followed by 5% EDTA (20 mL) after 3 weeks | TAP | 3 | PRP was prepared according to the description by Dohan et al. [48]. PRP was combined with equal volumes of sterile solution containing 10% calcium chloride and sterile bovine thrombin (100 U/mL) to achieve coagulation. | Final restoration was completed with white MTA (Angelus, Londrina, Brazil), reinforced GI cement (Ketac Molar Easymix; 3M ESPE, Seefeld, Germany) and composite resin (Filtek Supreme XT; 3M ESPE, St Paul, MN, USA) |
| Elsheshtawy et al., 2020 [18] | Secondary to trauma and Dens invaginatus | Yes | No | 20 mL of 5.25% NaOCl. At recall, 20 mL of 2.5% NaOCl, followed by 20 mL sterile saline and 10 mL of 17% EDTA solution | TAP | NR | PRP was prepared according to Dohan et al. [48], after which concentrated platelet-rich plasma (cPRP) was prepared and introduced inside dry root canals using a sterile 30 G syringe. The canal was then backfilled with cPRP to a level just beneath the CEJ and left to clot for 10 min | MTA, using a layer of reinforced GI (Riva self-cure, SDI limited, Bayswater, Victoria, Australia), followed by resin composite (Filtek Z250 universal restorative, 3 mol L, 3M ESPE, St. Paul, MN, USA) |
| Jadhav et al., 2012 [19] | Secondary to trauma/caries | No | Minimal (#60H file) | 2.5% NaOCl (copious irrigation) | TAP | NR | PRP: 8 mL of blood drawn by venipuncture of the antecubital vein was collected in a 10 mL sterile glass tube coated with an anticoagulant (acid citrate dextrose) and centrifuged at 2400 rpm for 10 min to separate PRP and platelet-poor plasma (PPP) from the red blood cell fraction. The topmost layer (PRP + PPP) was transferred to another tube and again centrifuged at 3600 rpm for 15 min to separate the PRP to precipitate at the bottom of the glass tube. This was mixed with 1 mL 10% calcium chloride to activate the platelets and to neutralize the acidity of acid citrate dextrose. | Resin-modified GI cement (Photac-Fill; 3M ESPE, St Paul, MN, USA) |
| Rizk et al., 2019 [20] | Secondary to trauma | Yes | No | 20 mL 2% NaOCl for 5 min, followed by 20 mL 17% EDTA. | TAP | 3 | PRP was prepared according to the description by Dohan et al. [48]. PRP was combined with equal volumes of sterile solution containing 10% calcium chloride and sterile bovine thrombin (100 U/mL) to achieve coagulation. PRF: 10 mL blood was collected in a sterile tube without anticoagulant and centrifuged immediately for 10 min at a speed of 3000 rpm. | An MTA orifice plug extending 2–3 mm in the canal was used to seal the canal orifice then GI (GC America, Alsip, IL, USA) and composite (Z250, 3M ESPE) were applied to give an effective and durable seal |
| Ragab et al., 2019 [21] | Secondary to trauma | Yes | No | 20 mL of 5.25% NaOCl followed by 20 mL sterile saline. | DAP | 3 | PRF was prepared by drawing 12 mL sample of whole blood intravenously from the patient’s right antecubital vein and centrifuged at 3000 rpm for 12 min. | MTA plus Light Cure GI cement |
| Mittal et al., 2019 [22] | Secondary to trauma/caries | Yes | Minimal (#30k file) | 2.5% NaOCl (copious irrigation). | DAP | 4 | PRF was prepared by drawing 5 mL of venous blood from the patient, collected in a dried glass test tube, and centrifuged at 2700 rpm for 12 min. | GI cement followed by composite resin |
| Shivashankar et al., 2017 [23] | Secondary to trauma/caries | No | Minimal | 5.25% NaOCl (copious irrigation). | TAP | 3 | NR | NR |
| Hazim Rizk et al., 2020 [24] | Trauma, Caries | Yes | No | 20 mL of 2.5% NaOCl followed by 20 mL of 17% EDTA. At recall 20 mL sterile saline followed by 20 mL 17% EDTA solution | TAP | 3 | PRP and PRF was prepared according to Dohan and Choukroun (2007) [49] method. | MTA, using a layer of GI (GC America, Alsip, IL, USA) followed by composite (Z 250, 3 M ESPE) |
| Jiang et al., 2017 [25] | Trauma, Broken central cusp | Yes | NO | 20 mL 1.25% NaOCl. At recall, 20 mL 17% EDTA. | Ca(OH)2 paste | 2 | NR | A layer of Filtek Z250 composite resin (3M ESPE, Irvine, CA; 3–4 mm) was placed over the capping material for the final restoration. |
| Narang et al., 2015 [26] | Secondary to trauma/caries | Yes | Minimal | 2.5% NaOCl (copious irrigation) | TAP | 4 | NR | Resin-modified GI cement was placed extending 3–4 mm in the canal. Access cavity was sealed with composite (Clearfil Majesty, Kuraray Medical Inc., Tokyo, Japan). |
| Meschi et al., 2021 [27] | Trauma, Caries, Anatomic anomaly (dens invaginatus) | Yes | No | 20 mL 1.5% NaOCl and subsequently with 20 mL saline. At recall, 30 mL EDTA 17% 1 mm short of the working length. | DAP | 2 | Blood samples were centrifuged. Fibrin clots were collected after centrifugation, and 2 of them were transformed into membranes after 5 min of pressure under a sterile glass plate. | Tooth was sealed by means of a GI lining and composite restoration. |
| Ulusoy et al., 2019 [28] | Secondary to trauma | Yes | No | 20 mL 1.25% NaOCl. At recall, 2% CHX, saline and 1 mL 17% EDTA. | TAP | 4 | PRP: Citrated blood was centrifuged in a standard laboratory centrifuge PK 130 (ALC International; ColognoMonzese, Italy) for 15 min at 1250 rpm to obtain PRP without erythrocytes and leukocytes. PRF: 10 mL blood was collected in a sterile tube without anticoagulant and centrifuged immediately for 10 min at a speed of 3000 rpm (Andreas Hettich Group, Ltd., Tuttlingen, Germany). | MTA coronal barrier was sealed with a thin GI base, and final coronal restorations were placed at the same visit using acid etch composite resin. |
| Jayadevan et al., 2021 [33] | Trauma | No | Minimal (#80–120K file) | 1.5% NaOCl solution (20 mL) followed by saline and 17% EDTA. Recall session, copious and gentle irrigation with saline and 20 mL of 17% EDTA. | TAP | 4 | A-PRF or PRF was freshly prepared using a centrifuge (R-8C Laboratory centrifuge, Remi Lab, Mumbai, India). For PRF, 10 mL of intravenous blood was drawn into a tube without anticoagulant and centrifuged at 2700 rpm for 12 min. For A-PRF, 10 mL of intravenous blood was drawn into a tube without anticoagulant and centrifuged at 1500 rpm for 14 min. | GI cement (GC, Fuji IX, GC India) was placed gently in a thickness of about 3–4 mm over the Biodentine and the access was temporized with Cavit. Post regenerative treatment consisted of non-vital bleaching or composite restoration. These procedures were performed after a period of one week. |
| Peng et al., 2017 [29] | Anatomic, Caries, Trauma | Yes | Minimal (#30K file) | 5.25% NaOCl solution (20 mL) | TAP | 1–4 | NR | Conventional GI cement (Fuji IX, Fuji Corporation, Osaka, Japan) was placed over the blood clot at the level of CEJ, followed by phosphoric acid etching for 30 s, a single-bond adhesive agent, and placement of Filtek Z250 composite resin (3M ESPE, Irvine, CA, USA). Instead of GI cement, mixture of ProRoot MTA (Dentsply Tulsa Dental, Johnson City, TN, USA) with 3 mm thickness was placed at the level of the CEJ. |
| Lv et al., 2018 [30] | Dens evaginatus, Tooth fracture | Yes | Minimal (35 K-file) | 20 mL of 1% NaOCl followed by 10 mL of 17% EDTA solution | TAP | 4 | PRF was prepared as described by Choukroun et al. [50]. Immediately before surgery, 5 mL of whole blood was drawn into 10 mL test tubes without anticoagulant reagent and was centrifuged at 400× g for 10 min. The PRF layer was separated using sterile scissors, and PRF clots were pressed into a membranous film with sterile dry gauze. | A 3-mm-thick layer of MTA was placed followed by a moist cotton pellet and Cavit. One week later, the Cavit was removed and replaced with a bonded resin restoration (Filtek Z350 XT: 3M ESPE Dental Products, St Paul, MN, USA). |
| Cheng et al., 2022 [31] | Secondary to trauma | No | Minimal or No | 0.5–1.5% NaOCl and saline or NaOCl in combination with saline and 17% EDTA | TAP | 2 | CGF was prepared from the patient’s intravenous blood. After immediate differential centrifugation of blood, CGF was represented as the buffy coat in the middle layer. Then the CGF layer was separated using sterile scissors. | Teeth were restored with a bio-ceramic material [i.e., MTA (Dentsply Sirona, Ballaigues, Switzerland) or iRoot BP Plus (Innovative Bioceramix Inc, Vancouver, BC, Canada)] followed by various restorative materials. |
| Chueh et al., 2009 [32] | Trauma | Yes | No | 2.5% NaOCl | Ca(OH)2 paste | 1–2 | NR | The access was sealed with temporary filling materials or resin. |
| Bonte et al., 2014 [34] | Trauma | Yes | No | Active 3% NaOCl | - | - | - | Composite resin |
| Santhakumar et al., 2018 [35] | Trauma and Dental caries | Yes | No | 3% NaOCl followed by saline | TAP | 3 | A 5 mL blood sample was taken from the patient’s anticubital vein. The blood was centrifuged without anticoagulant at 3000 rpm for 10 min, and PRF gel was obtained at the bottom of the test tube and was removed with a sterile tweezer. After obtaining PRF gel, it was squeezed using especially designed PRF compression device to remove the excess fluid. The membrane obtained was cut linearly in the shape of root canal space for ease of placement. | Triple sealed with MTA (ProRoot MTA), type II GI cement (Fugi 2) and composite material (3M ESPE). |
| Kandemir Demirci et al., 2019 [36] | Trauma, Dens invaginatus, Caries | Yes | No | 2.5% NaOCl solution. At recall, 2.5% NaOCl, 17% EDTA followed by 2% CHX | Ca(OH)2 powder mixed with saline | 1 | - | Bonded composite resin |
| Tek et al. 2021 [37] | Trauma | Yes | Yes | 2.5% NaOCl solution. Recall 2.5% NaOCl solution followed by distilled water | Ca(OH)2 paste | 1 | - | Resin composite (3M ESPE Filtek Ultimate Seefeld, Germany) |
| Kinirons et al., 2001 [38] | Trauma | NR | No | NR | - | - | - | NR |
| Lin et al., 2017 [39] | Secondary to trauma/Dens evaginatus | Yes | Minimal (#25 K file) | 20 mL 1.5% NaOCl, 0.9% physiological saline, 20 mL 17% EDTA | TAP | 3 | - | GI cement followed by composite resin |
| Xuan et al., 2018 [40] | Secondary to trauma | Yes | No | NR | NR | 4 | The pulp tissue for hDPSC isolation was harvested using standard sterile techniques. Autologous hDPSCs were obtained from the patient’s maxillary deciduous canine tooth. | NR |
| Alobaid et al., 2014 [41] | Secondary to Trauma | Yes | No | 20 mL 17% EDTA | TAP | 3 | PRP and PRF were prepared according to the method of Dohan and Choukroun (2007) [49]. | An MTA orifice plug extending 2–3 mm in the canal was used to seal the canal orifice then GI (GC America, Alsip, IL, USA) and composite (Z 250, 3 M ESPE) to give an effective and durable seal. |
| Casey et al., 2022 [42] | Secondary to trauma | Yes | Minimal | Varying concentrations of NaOCl, CHX, and/or EDTA | TAP | 2 | NR | Resin bonded restoration |
| Caleza-Jimenez et al., 2022 [43] | Trauma, Caries | Yes | No | 1.5–2.5% NaOCl and 17% EDTA | TAP | 2 | NR | Composite restoration |
| Pereira et al., 2021 [44] | Trauma | No | Minimal | 6% NaOCl, 2% CHX, saline solution, and EDTA 17% or Ca(OH)2 and 2% CHX gel | TAP | 3 | NR | Resin bonded restoration |
| Jeeruphan et al., 2012 [45] | Secondary to trauma/Caries | No | Minimal | 5.25% NaOCl | TAP | 3 | NR | NR |
| Silujjai et al., 2017 [46] | Secondary to trauma/Caries/Dens evaginatus | Yes | No | 1.5–2.5% NaOCl followed by 17% EDTA | Ca(OH)2 or TAP | NR | NR | MTA plus bonded restoration |
| Chen et al., 2016 [47] | Dens evaginatus | Yes | Minimal (#25 K file) | Copious 2.5% NaOCl | NR | NR | NR | NR |
| Author | Intervention | Type of Study | Comparative Group | Sample Size | Follow Up Time (in Months) | RA | Parameters to Assess Clinical Evaluation | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| DWT | IRL | AFW | AC | VR | PAH | BD | |||||||
| Alagl et al., 2017 [16] | REP | RCT | BC | 15 | 12 | CBCT | - | 11.80 ± 3.28 mm | - | 53.33% | 53.33% | - | 445.44 ± 153.54 HU |
| PRP | 15 | - | 12.14 ± 3.32 mm | - | 93.33% | 86.66% | - | 485.88 ± 154.15 HU | |||||
| Bezgin et al., 2015 [17] | REP | RCT | BC | 10 | 18 | IOPAR | - | 12.6% | - | 60% | 20% | - | - |
| PRP | 10 | - | 9.86% | - | 70% | 50% | - | - | |||||
| Elsheshtawy et al., 2020 [18] | REP | RCT | BC | 11 | 12 | CBCT | ICC = 1 | ICC = 0.998 | ICC = 1 | - | - | - | - |
| PRP | 11 | ICC = 0.997 | ICC = 0.999 | ICC = 0.998 | - | - | - | - | |||||
| Jadhav et al., 2012 [19] | REP | RCT | BC | 10 | 12 | IOPAR | S = 70% G = 30% | S = 40% G = 60% | - | S = 50% G = 30 E = 20% | - | S = 30%, G = 70% | - |
| PRP | 10 | S = 20%, G = 50%, E = 30% | S = 10% G = 50% E = 40% | - | G = 30%, E = 70% | - | S = 10% G = 40% E = 50% | - | |||||
| Rizk et al., 2019 [20] | REP | RCT | BC | 13 | 12 | IOPAR | - | 0.68 ± 0.44 mm | 2.2 ± 3.97 mm | - | - | - | 58.96 ± 19.95 Grey |
| PRP | 13 | - | 1.48 ± 0.37 mm | 2.49 ± 3.93 mm | - | - | - | 65.08 ± 30.043 Grey | |||||
| Ragab et al., 2019 [21] | REP | RCT | BC | 11 | 12 | IOPAR | - | 14.8% | - | 45.4% | - | 80.5% | - |
| PRF | 11 | - | 12.8% | - | 63.6% | - | 70.2% | - | |||||
| Mittal et al., 2019 [22] | REP | RCT | BC | 4 | 12 | IOPAR | 100% | 25% | - | 25% | - | 75% | - |
| PRF | 4 | 100% | 0 | - | 100% | - | 75% | - | |||||
| Shivashankar et al., 2017 [23] | REP | RCT | BC | 15 | 12 | IOPAR | 93.3% | 86.7% | - | - | 13.30% | 2.07 ± 0.594 mm | - |
| PRP | 19 | 84.2% | 73.7% | - | - | 15.8% | 1.32 ± 0.478 mm | - | |||||
| PRF | 20 | 70% | 65% | - | - | 15% | 1.85 ± 1.040 mm | - | |||||
| Hazim Rizk et al., 2020 [24] | REP | RCT | PRP | 13 | 12 | IOPAR | - | 1.48 ± 0.37 mm | 0.97 ± 0.75 mm | - | - | - | 65.08 ± 30.043 Grey |
| PRF | 12 | - | 1.24 ± 0.54 mm | 1.003 ± 0.392 mm | - | - | - | 53.44 ± 22.165 Grey | |||||
| Jiang et al., 2017 [25] | REP | RCT | Without Bio-Gide | 22 | 6 | IOPAR | 21.2 ± 19.5% | 15.4 ± 13.6% | −55 ± 34% | - | 18% | - | - |
| With Bio-Gide | 21 | 21.5 ± 22.5% | 16.4 ± 13.6% | −65 ± 34% | - | 33% | - | - | |||||
| Narang et al., 2015 [26] | REP | RCT | MTA | 5 | 18 | IOPAR | 0% | 0% | - | 0% | - | 58% | - |
| BC | 5 | 50% | 40% | - | 66.67% | - | 60% | - | |||||
| PRP | 5 | 60% | 99% | - | 40% | - | 98% | - | |||||
| PRF | 5 | 20% | 40% | - | 60% | - | 80% | - | |||||
| Meschi et al., 2021 [27] | REP | RCT | REP-LPRF | 13 | 36 | CBCT | 30% | 0% | - | - | - | 100% | - |
| REP + LPRF | 6 | 10% | 10% | - | - | - | 100% | - | |||||
| Ulusoy et al., 2019 [28] | REP | RCT | BC | 21 | Until complete healing 10–49 | IOPAR | 14.91 ± 3.38 mm | 7.15 ±1.39 mm | - | - | - | - | - |
| PRP | 18 | 19.01 ± 4.20 mm | 4.74 ± 0.91 mm | - | - | - | - | - | |||||
| PRF | 17 | 9.80 ± 3.03 mm | 6.00 ± 1.57 mm | - | - | - | - | - | |||||
| PP | 17 | 8.55 ± 3.55 mm | 4.17 ± 1.33 mm | - | - | - | - | - | |||||
| Jayadevan et al., 2021 [33] | REP | RCT | PRF | 10 | 12 | IOPAR | 50% | 80% | 45.5% | ||||
| APRF | 11 | 91% | 72% | 40% | |||||||||
| Peng et al., 2017 [29] | REP | NRCT | Conventional GIC | 32 | 12 | IOPAR | 26.3% | 10.5% | - | - | - | - | - |
| ProRoot MTA | 28 | 30.7% | 11.0% | - | - | - | - | - | |||||
| Lv et al., 2018 [30] | REP | NRCT | BC | 5 | 12 | IOPAR | 80% | 80% | - | 80% | 100% | 100% | - |
| PRF | 5 | 80% | 80% | - | 80% | 100% | 100% | - | |||||
| Cheng et al., 2022 [31] | REP | NRCT | BC | 32 | 16 | IOPAR | F = 17.4 ± 16.4% L = 52.5 ± 24.8% Ci = 26.0 ± 37.3% A = 37.0% | F = 8.3 ± 11.7% L = 23.8 ± 18.1% Ci = 10.3 ± 16.6% A = 12.0% | F = 76.4 ± 30.9% L = 69.3 ± 43.9% Ci = 45.0 ± 37.7% A = 100.0% | ||||
| CGF | 30 | ||||||||||||
| Chueh et al., 2009 [32] | REP | NRCT | MTA | 8 | 6–108 | IOPAR | - | 87.5% | 87.5% | - | - | - | - |
| MTA + GP/GP/ Amalgam | 15 | - | 93.33% | 80% | - | - | - | - | |||||
| Bonte et al., 2014 [34] | APP | RCT | MTA | 15 | 12 | IOPAR | - | - | 76.5% | - | - | 82.4% | - |
| CH | 15 | - | - | 50% | - | - | 75.0% | - | |||||
| Santhakumar et al., 2018 [35] | APP | RCT | PRF Gel | 19 | 18 | IOPAR | - | 94.73% | - | - | 100% | - | - |
| PRF Membrane | 19 | - | 89.47% | - | - | 100% | - | - | |||||
| Kandemir Demirci et al., 2019 [36] | APP | NRCT | MTA | 39 | 12 | IOPAR | - | - | 74% | - | - | 92% | - |
| CH | 34 | - | - | 79% | - | - | 91% | - | |||||
| Tek et al., 2021 [37] | APP | NRCT | Apical plug with MTA | 10 | 12 | IOPAR | - | - | - | - | - | 50% | - |
| Collagen sponge + apical plug with MTA | 10 | - | - | - | - | - | 62.5% | - | |||||
| Kinirons et al., 2001 [38] | APP | NRCT | CH in Newcastle | 43 | 3 | IOPAR | - | - | 100% | - | - | - | - |
| CH in Belfast | 64 | - | - | 100% | - | - | - | - | |||||
| Lin et al., 2017 [39] | REP vs. APP | RCT | BC | 69 | 12 | CBCT | 82.60% | 81.16% | - | 65.21% | - | 100% | - |
| Vitapex paste | 34 | 0% | 26.47% | - | 82.35% | - | 100% | - | |||||
| Xuan et al., 2018 [40] | REP vs. APP | RCT | hDPSC | 20 | 12 | CBCT | - | 5.24 ± 0.92 mm | 2.64 ± 0.73 mm | - | 43.43 ± 0.86 mm | - | - |
| CH | 10 | - | 0.88 ± 0.67 mm | 0.62 ± 0.22 mm | - | 0.17 ± 0.16 mm | - | - | |||||
| Alobaid et al., 2014 [41] | REP vs. APP | NRCT | BC | 19 | 15–22 | IOPAR | - | 20% | 10.2 ± −4.0% | - | - | - | - |
| CH & MTA | 12 | - | 12.5% | 1.4 ± −3.2% | - | - | - | - | |||||
| Casey et al., 2022 [42] | REP vs. APP | NRCT | BC | 93 | 31–33 | IOPAR | - | - | - | - | 19% | - | - |
| CH & MTA | 118 | - | - | - | - | 0 | - | - | |||||
| Caleza-Jimenez et al., 2022 [43] | REP vs. APP | NRCT | BC | 9 | 6–66 | IOPAR | 12.76% | 34.57 ± 16.62% | |||||
| MTA | 9 | 0.29% | −3.36 ± 4.13% | ||||||||||
| Pereira et al., 2021 [44] | REP vs. APP | NRCT | BC | 22 | 12–30 | IOPAR | 0.21 ± 0.35 mm | 1.42 ± 1.25 mm | 0.88 ± 0.77 mm | - | - | 95.45% | - |
| MTA | 22 | 0.03 ± 0.07 mm | 0.88 ± 0.7 mm | 0.6 ± 0.51 mm | - | - | 86.36% | - | |||||
| Jeeruphan et al., 2012 [45] | REP vs. APP | NRCT | BC | 20 | 24 | IOPAR | - | 14.9% | 28.2% | - | - | 80% | - |
| MTA | 19 | - | 6.1% | 0.00% | - | - | 68% | - | |||||
| CH | 22 | - | 0.4% | 1.52% | - | - | 77% | - | |||||
| Silujjai et al., 2017 [46] | REP vs. APP | NRCT | BC | 17 | 12–96 | IOPAR | - | 9.51 ± 18.14% | 13.75 ± 19.91% | - | - | - | - |
| MTA | 26 | - | 8.55 ± 8.97% | −3.30 ± 14.14% | - | - | - | - | |||||
| Chen et al., 2016 [47] | REP vs. APP | NRCT | CH, BC, MTA | 17 | 12 | IOPAR | - | 94.12% | - | - | - | - | - |
| CH, MTA | 21 | - | 85.71% | - | - | - | - | - | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Panda, P.; Mishra, L.; Govind, S.; Panda, S.; Lapinska, B. Clinical Outcome and Comparison of Regenerative and Apexification Intervention in Young Immature Necrotic Teeth—A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 3909. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11133909
Panda P, Mishra L, Govind S, Panda S, Lapinska B. Clinical Outcome and Comparison of Regenerative and Apexification Intervention in Young Immature Necrotic Teeth—A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(13):3909. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11133909
Chicago/Turabian StylePanda, Pratima, Lora Mishra, Shashirekha Govind, Saurav Panda, and Barbara Lapinska. 2022. "Clinical Outcome and Comparison of Regenerative and Apexification Intervention in Young Immature Necrotic Teeth—A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 13: 3909. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11133909