
The Effects of Active Video Game Exercise Based on Self-Determination Theory on Physical Fitness and Cognitive Function in Older Adults

 ,
,  , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
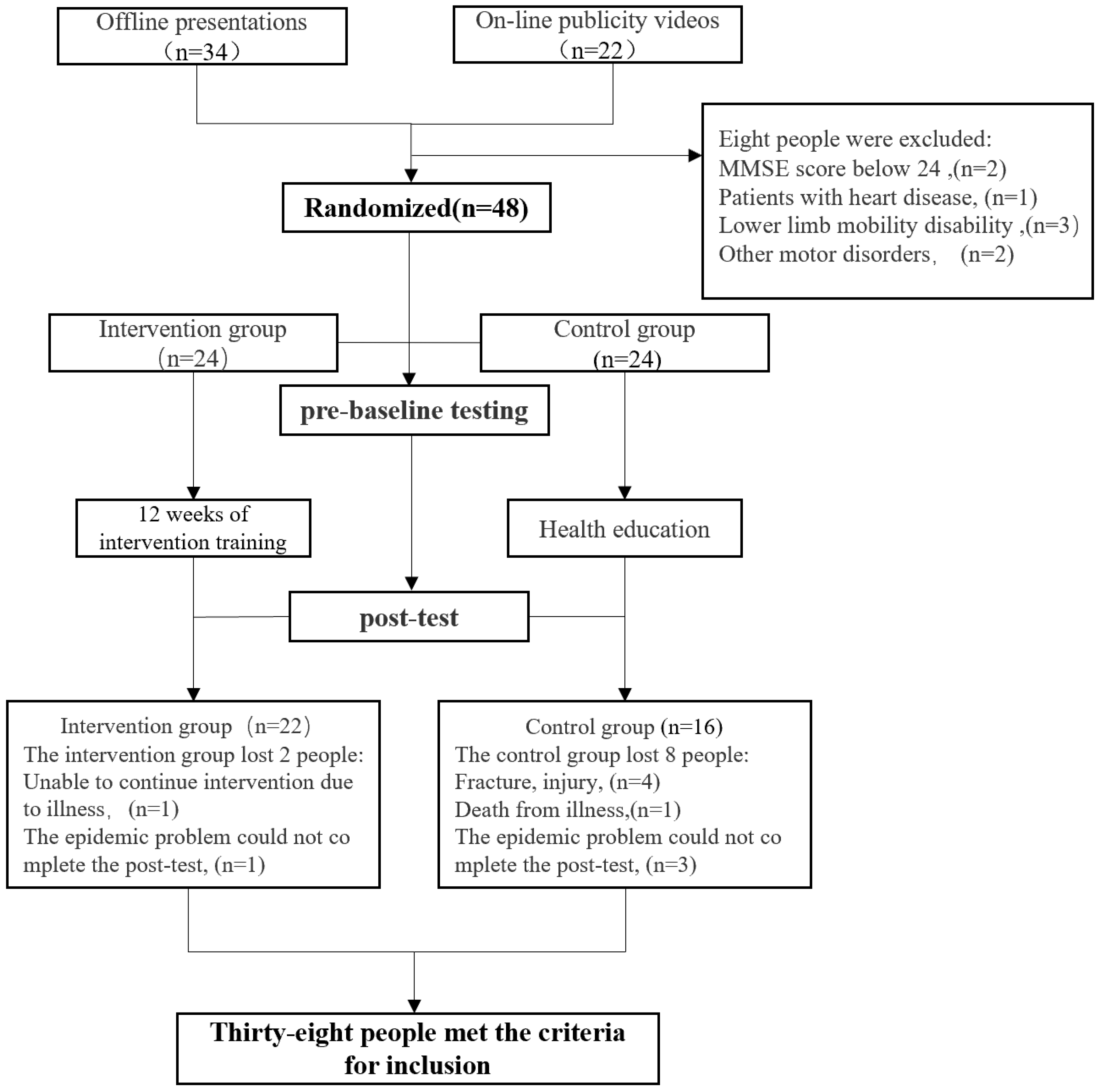
2.1. Participants
2.2. Study Design and Procedure
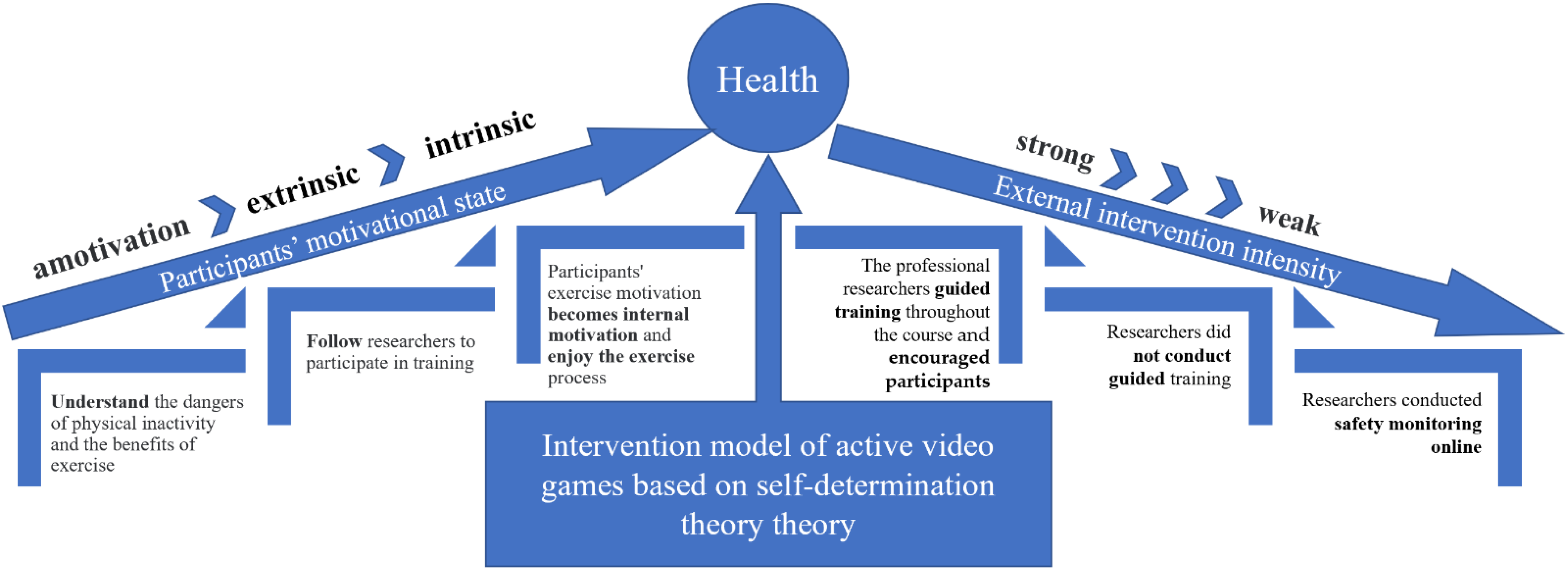
2.3. Intervention
- (1)
- Competence: Speak to the participants about the risks of low physical activity and the benefits of regular exercise; there are also professional researchers for professional training monitoring and guidance;
- (2)
- Autonomy: Visually demonstrate more and less intense exercise varieties to allow participants to choose which version to perform based on their level of physical fitness;
- (3)
- Relatedness: Conduct group scoring ranking and establish a reward system for persistence exercise.
- (1)
- The professional researchers conducted guided training throughout the course. The researchers instructed the participants in movements and techniques, at the same time leading the participants to exercise and encouraging them to increase their sense of achievement and enjoyment.
- (2)
- Participants were divided into groups and competed for scores between groups. These researchers were responsible for the monitoring game scores and establishing a scoring system and did not conduct the guided training.
- (3)
- Participants performed online video exercises at home, and the researchers conducted safety monitoring online. (The original plan of the study was that participants would train autonomously according to routine, with noninterference from researchers except for safety monitoring and start-up hardware devices. However, due to the local coronavirus virus outbreak, the local policy required residents to observe home quarantine to prevent the spread of the virus, so offline training was changed to online training at home. Online training did not violate the principles of the experimental design; that is, participants were allowed to train independently without interference).
- (1)
- Zumba@ Fitness: Zumba Fitness is a dance game that consists of different music styles. For this study, each song was selected according to its intensity, rhythm, and acceptability to the participants. Each song lasted for 4 min, and there was a 1-min break after every 2 songs.
- (2)
- Fitboxing2 Aerobic boxing: This is a boxing virtual game. Participants held the handle to control their player. When the block entered the area, participants tried to punch toward the screen with the handle using different techniques such as hook, jab, dodge, dive dodge, U-bend, and step.
- (3)
- Mario Tennis Ace: This is a tennis virtual game that adopted the swing mode for this intervention. Participants held the handle as a racket and swung left or right to control the player to hit the ball. In the swing mode, the game provides an auxiliary movement function in which the player will semi-automatically move to the position of hitting, and two participants fight each other.
2.4. Outcome Measures
2.4.1. Physical Activity Questionnaire
2.4.2. Physical Fitness Test
2.4.3. Cognitive Testing
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- He, W.; Goodkind, D.K.P. An Aging World: 2015. International Publication Reports; U.S. Census Bureau: Suitland-Silver Hill, MD, USA, 2016. [Google Scholar]
- Bulletin of the Seventh National Census. Available online: http://www.stats.gov.cn/xxgk/sjfb/zxfb2020/202105/t20210511_1817200.html (accessed on 15 May 2022).
- Harada, C.N.; Love, M.C.N.; Triebel, K.L. Normal Cognitive Aging Mild Cognitive Impairment Dementia Aging Cognition. Clin. Geriatr. Med. 2013, 29, 737–752. [Google Scholar] [CrossRef] [Green Version]
- Lang, P.O.; Michel, J.P.; Zekry, D. Frailty Syndrome: A Transitional State in a Dynamic Process. Gerontology 2009, 55, 539–549. [Google Scholar] [CrossRef]
- Lei, Y.L.; Xin, J.G.; Yang, C.S.; Zhou, K.; Zhao, L.; Ma, X. Association between Sedentary Behavior and Multiple Chronic Diseases in Adults. Mod. Prev. Med. 2020, 47, 3158–3162. [Google Scholar]
- Hang, Y.; Zhang, X.; Wang, J.-H. Self-Paid Direct Medical Expense and Economic Risk among Hospitalized Chronic Disease Patients in China: 2013. Chin. J. Public Health 2021, 37, 618–622. [Google Scholar] [CrossRef]
- Castelli, L.; Galasso, L.; Mulè, A.; Bruno, E.; Shokohyar, S.; Esposito, F.; Montaruli, A.; Roveda, E. Physical Activity, Chronotype and Sleep in a Sample of Italian Elderly Population. Sport Sci. Health 2019, 16, 55–64. [Google Scholar] [CrossRef]
- McPhee, J.S.; French, D.P.; Jackson, D.; Nazroo, J.; Pendleton, N.; Degens, H. Physical Activity in Older Age: Perspectives for Healthy Ageing and Frailty. Biogerontology 2016, 17, 567–580. [Google Scholar] [CrossRef] [PubMed]
- Falck, R.S.; Davis, J.C.; Best, J.R.; Crockett, R.A.; Liu-Ambrose, T. Impact of Exercise Training on Physical and Cognitive Function among Older Adults: A Systematic Review and Meta-Analysis. Neurobiol. Aging 2019, 79, 119–130. [Google Scholar] [CrossRef]
- Jurak, G.; Morrison, S.A.; Leskošek, B.; Kovač, M.; Hadžić, V.; Vodičar, J.; Truden, P.; Starc, G. Physical Activity Recommendations during the Coronavirus Disease-2019 Virus Outbreak. J. Sport Health Sci. 2020, 9, 325–327. [Google Scholar] [CrossRef]
- Chen, P.; Mao, L.; Nassis, G.P.; Harmer, P.; Ainsworth, B.E.; Li, F. Coronavirus Disease (COVID-19): The Need to Maintain Regular Physical Activity While Taking Precautions. J. Sport Health Sci. 2020, 9, 103–104. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Self-Determination Theory and the Facilitation of Intrinsic Motivation, Social Development, and Well-Being. J. Sports Med. 2000, 55, 68–78. [Google Scholar] [CrossRef]
- McDonough, D.J.; Helgeson, M.A.; Liu, W.; Gao, Z. Effects of a Remote, YouTube-Delivered Exercise Intervention on Young Adults’ Physical Activity, Sedentary Behavior, and Sleep during the COVID-19 Pandemic: Randomized Controlled Trial. J. Sport Health Sci. 2022, 11, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Brötz, D. Exercise, Physical Activity, and Self-Determination Theory: A Systematic Review. Physioscience 2013, 9, 78. [Google Scholar] [CrossRef]
- Meekes, W.; Stanmore, E.K. Motivational Determinants of Exergame Participation for Older People in Assisted Living Facilities: Mixed-Methods Study. J. Med. Internet Res. 2017, 19, e238. [Google Scholar] [CrossRef] [PubMed]
- Graves, L.E.F.; Ridgers, N.D.; Williams, K.; Stratton, G.; Atkinson, G.; Cable, N.T. The Physiological Cost and Enjoyment of Wii Fit in Adolescents, Young Adults, and Older Adults. J. Phys. Act. Health 2010, 7, 393–401. [Google Scholar] [CrossRef]
- Perron, R.M.; Graham, C.A.; Hall, E.E. Comparison of Physiological and Psychological Responses to Exergaming and Treadmill Walking in Healthy Adults. Games Health J. 2012, 1, 411–415. [Google Scholar] [CrossRef]
- Viana, R.B.; De Lira, C.A.B. Exergames as Coping Strategies for Anxiety Disorders during the COVID-19 Quarantine Period. Games Health J. 2020, 9, 147–149. [Google Scholar] [CrossRef]
- Fang, Q.; Ghanouni, P.; Anderson, S.E.; Touchett, H.; Shirley, R.; Fang, F.; Fang, C. Effects of Exergaming on Balance of Healthy Older Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Games Health J. 2020, 9, 11–23. [Google Scholar] [CrossRef] [Green Version]
- Stojan, R.; Voelcker-Rehage, C. A Systematic Review on the Cognitive Benefits and Neurophysiological Correlates of Exergaming in Healthy Older Adults. J. Clin. Med. 2019, 8, 734. [Google Scholar] [CrossRef] [Green Version]
- Chao, Y.Y.; Scherer, Y.K.; Montgomery, C.A. Effects of Using Nintendo WiiTM Exergames in Older Adults: A Review of the Literature. J. Aging Health 2015, 27, 379–402. [Google Scholar] [CrossRef]
- Yu, T.C.; Chiang, C.H.; Wu, P.T.; Wu, W.L.; Chu, I.H. Effects of Exergames on Physical Fitness in Middle-Aged and Older Adults in Taiwan. Int. J. Environ. Res. Public Health 2020, 17, 2565. [Google Scholar] [CrossRef] [Green Version]
- Kari, T. Can Exergaming Promote Physical Fitness and Physical Activity? A Systematic Review of Systematic Reviews. Int. J. Gaming Comput.-Mediat. Simul. 2014, 6, 59–77. [Google Scholar] [CrossRef] [Green Version]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”: A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Society, C. Physical Activity Readiness Questionnaire. In ACSM’s Guidelines for Exercise Testing and Prescription; ACSM: Indianapolis, IN, USA, 2002; Volume 26. [Google Scholar]
- Sherrington, C.; Tiedemann, A.; Fairhall, N.; Close, J.C.T.; Lord, S.R. Exercise to Prevent Falls in Older Adults: An Updated Meta-Analysis and Best Practice Recommendations. NSW Public Health Bull. 2011, 22, 78–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brach, M.; Hauer, K.; Rotter, L.; Werres, C.; Korn, O.; Konrad, R.; Göbel, S. Modern Principles of Training in Exergames for Sedentary Seniors: Requirements and Approaches for Sport and Exercise Sciences. Int. J. Comput. Sci. Sport 2012, 11, 86–99. [Google Scholar] [CrossRef]
- Tian, Y.; Lu, Y.; Zhao, J.X.; Wang, Z.X.; Xu, G.; An, J.H.; Tian, J.M. Physical Fitness Guidelines for Chinese People. China Sport Sci. 2010, 30, 3–10. [Google Scholar] [CrossRef]
- Jones, C.; Hammig, B. Case Report: Injuries Associated with Interactive Game Consoles: Preliminary Data. Physician Sportsmed. 2009, 37, 138–140. [Google Scholar] [CrossRef]
- Chen, X.; Su, D.; Chen, X.; Chen, Y. What Intensity of Exercise Is Most Suitable for the Elderly in China? A Propensity Score Matching Analysis. BMC Public Health 2021, 21, 1396. [Google Scholar] [CrossRef]
- Macfarlane, D.J.; Lee, C.C.Y.; Ho, E.Y.K.; Chan, K.L.; Chan, D.T.S. Reliability and Validity of the Chinese Version of IPAQ (Short, Last 7 Days). J. Sci. Med. Sport 2007, 10, 45–51. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Li, D.M.; Liu, C.; Li, G.Y. The Construction Of ‘Basic Cognitive Capacity Test’And Its Standardization. Acta Psychol. Sin. 2014, 7, 107–115. [Google Scholar]
- Lebrasseur, A.; Fortin-Bédard, N.; Lettre, J.; Bussières, E.L.; Best, K.; Boucher, N.; Hotton, M.; Beaulieu-Bonneau, S.; Mercier, C.; Lamontagne, M.E.; et al. Impact of COVID-19 on People with Physical Disabilities: A Rapid Review. Disabil. Health J. 2021, 14, 101014. [Google Scholar] [CrossRef] [PubMed]
- Jones, G.R.; Brandon, C.; Gill, D.P. Physical Activity Levels of Community-Dwelling Older Adults Are Influenced by Winter Weather Variables. Arch. Gerontol. Geriatr. 2017, 71, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Jang, D.; Kim, I.; Kwon, S. Motivation and Intention Toward Physical Activity During the COVID-19 Pandemic: Perspectives from Integrated Model of Self-Determination and Planned Behavior Theories. Front. Psychol. 2021, 12, 714865. [Google Scholar] [CrossRef]
- Irandoust, K.; Taheri, M.; H’Mida, C.; Neto, G.R.; Trabelsi, K.; Ammar, A.; Souissi, N.; Chtourou, H.; Nikolaidis, P.T.; Rosemann, T.; et al. Exergaming and Aquatic Exercises Affect Lung Function and Weight Loss in Obese Children. Int. J. Sports Med. 2021, 42, 566–572. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.B. The Effect of Tai Chi Exercise on the Human Respiratory System. J. Shanxi Financ. Econ. Univ. 2011, s4, 205. [Google Scholar] [CrossRef]
- Hang, L.I. Effect of Long-Term Aerobic Exercise on the Respiratory and Metabolic Function of Female University Student. J. Guangzhou Sport Univ. 2010, 30, 5–7. [Google Scholar] [CrossRef]
- Shenggui, P.A.N.; Ye, L.I.N.; Shasha, Z.; People, F. Effects of Resistance Breathing Training Combined with Aerobic Exercise on Cardiopulmonary Function and Exercise Tolerance in Patients with Chronic Obstructive Pulmonary Disease. Clin. Med. Res. Pract. 2020, 5, 79–80. [Google Scholar] [CrossRef]
- Yu, J.; Kim, J. Effects of a Physical Activity Program Using Exergame with Elderly Women. J. Korean Acad. Nurs. 2015, 45, 84–96. [Google Scholar] [CrossRef]
- Donath, L.; Rössler, R.; Faude, O. Effects of Virtual Reality Training (Exergaming) Compared to Alternative Exercise Training and Passive Control on Standing Balance and Functional Mobility in Healthy Community-Dwelling Seniors: A Meta-Analytical Review. Sports Med. 2016, 46, 1293–1309. [Google Scholar] [CrossRef]
- Sato, K.; Kuroki, K.; Saiki, S.; Nagatomi, R. Improving Walking, Muscle Strength, and Balance in the Elderly with an Exergame Using Kinect: A Randomized Controlled Trial. Games Health J. 2015, 4, 161–167. [Google Scholar] [CrossRef]
- Huang, H.C.; Wong, M.K.; Lu, J.; Huang, W.F.; Teng, C.I. Can Using Exergames Improve Physical Fitness? A 12-Week Randomized Controlled Trial. Comput. Hum. Behav. 2017, 70, 310–316. [Google Scholar] [CrossRef]
- Nasrullah, D.; Aisyah, S.; Fitri, A. Proposing a Healthy Environment for Elderly People with Hypertension: Taichi Gymnastic against Blood Pressure. IOP Conf. Ser. Earth Environ. Sci. 2020, 469, 012083. [Google Scholar] [CrossRef]
- Cheng, X.D.; Fan, Y.; Ge, L.; Zang, D.; Li, J.; Li, J.; Wu, H. Effects of Tai Chi Softball Exercises on Physical Fitness Level and Cardiovascular Health-Related Factors among Older Females. J. Healthc. Eng. 2021, 2021, 7671596. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.W.K.; Chair, S.Y.; Lee, D.T.F.; Leung, D.Y.P.; Sit, J.W.H.; Cheng, H.Y.; Taylor-Piliae, R.E. Tai Chi Exercise Is More Effective than Brisk Walking in Reducing Cardiovascular Disease Risk Factors among Adults with Hypertension: A Randomised Controlled Trial. Int. J. Nurs. Stud. 2018, 88, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Stanmore, E.; Stubbs, B.; Vancampfort, D.; de Bruin, E.D.; Firth, J. The Effect of Active Video Games on Cognitive Functioning in Clinical and Non-Clinical Populations: A Meta-Analysis of Randomized Controlled Trials. Neurosci. Biobehav. Rev. 2017, 78, 34–43. [Google Scholar] [CrossRef]
- Maillot, P.; Perrot, A.; Hartley, A. Effects of Interactive Physical-Activity Video-Game Training on Physical and Cognitive Function in Older Adults. Psychol. Aging 2012, 27, 589–600. [Google Scholar] [CrossRef] [Green Version]
- Guimarães, A.V.; Barbosa, A.R.; Meneghini, V. Active Videogame-Based Physical Activity vs. Aerobic Exercise and Cognitive Performance in Older Adults: A Randomized Controlled Trial. J. Phys. Educ. Sport 2018, 18, 203–209. [Google Scholar] [CrossRef]
- King, A.C.; Haskell, W.L.; Young, D.R.; Oka, R.K.; Stefanick, M.L. Long-Term Effects of Varying Intensities and Formats of Physical Activity on Participation Rates, Fitness, and Lipoproteins in Men and Women Aged 50 to 65 Years. Circulation 1995, 91, 2596–2604. [Google Scholar] [CrossRef]
- Farinatti, P.; Monteiro, W.D.; Oliveira, R.B. Long Term Home-Based Exercise Is Effective to Reduce Blood Pressure in Low Income Brazilian Hypertensive Patients: A Controlled Trial. High Blood Press. Cardiovasc. Prev. 2016, 23, 395–404. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Index | IG | CG | Total | t/χ2 | p | |
|---|---|---|---|---|---|---|
| Number of people | 22 | 16 | 38 | |||
| Age, M (SD) | 65.64 (4.2) | 65.75 (3.24) | 65.68 (3.78) | −0.90 | 0.929 | |
| Female (%) | 14 (63.6) | 10 (62.5) | 24 (63.20) | 0.01 | 0.943 | |
| Mini mental screener examination, M (SD) | 29 (1) | 28.69 (1.1) | 28.87 (1.07) | 0.89 | 0.381 | |
| Education (%) | 5.80 | 0.215 | ||||
| Primary school | 1 (4.5) | 1 (16.3) | 2 (5.3) | |||
| Junior high school | 8 (36.4) | 2 (12.5) | 10 (26.3) | |||
| High school | 5 (22.7) | 7 (43.8) | 12 (31.6) | |||
| college | 6 (27.3) | 2 (12.5) | 8 (21.1) | |||
| Undergraduate course | 2 (9.1) | 5 (25) | 6 (15.8) | |||
| Smoking (%) | 1 (4.5) | 1 (6.3) | 2 (5.3) | 0.05 | 0.816 | |
| Alcohol consumption (%) | 4 (18.2) | 1 (6.3) | 5 (13.2) | 1.15 | 0.283 | |
| Industry engaged (%) | 1.72 | 0.887 | ||||
| professional | 6 (27.3) | 4 (25) | 10 (26.3) | |||
| industrial | 1 (4.5) | 2 (12.5) | 3 (7.9) | |||
| administrative | 2 (9.1) | 1 (06.3) | 3 (7.9) | |||
| Agriculture | 2 (9.1) | 1 (06.3) | 3 (7.9) | |||
| general | 1 (4.5) | 0 (00.0) | 1 (2.6) | |||
| other | 10 (45.5) | 8 (50.0) | 18 (47.4) | |||
| Sports injury (%) | 6.00 | 0.199 | ||||
| knee | 3 (13.6) | 7 (43.8) | 10 (26.3) | |||
| vertebral | 5 (22.7) | 1 (6.3) | 6 (15.8) | |||
| diverse | 1 (4.5) | 0 | 1 (2.6) | |||
| other | 3 (13.6) | 1 (6.3) | 4 (10.5) | |||
| without | 10 (45.5) | 7 (43.8) | 17 (44.7) | |||
| Medication (%) | 11 (50) | 5 (31.3) | 16 (42.1) | 1.34 | 0.248 | |
| Chronic diseases (%) | 0.48 | 0.923 | ||||
| One of the three tenors | 4 (18.2) | 4 (25.0) | 8 (21.1) | |||
| diverse | 4 (18.3) | 2 (12.5) | 6 (15.8) | |||
| other | 5 (22.7) | 3 (18.8) | 8 (21.1) | |||
| without | 9 (40.9) | 7 (43.8) | 16 (42.1) | |||
| Vision and hearing problems (%) | 8.60 | 0.072 | ||||
| myopia | 4 (18.2) | 0 | 4 (10.5) | |||
| presbyopia | 2 (9.1) | 4 (25.5) | 6 (15.8) | |||
| diverse | 0 | 2 (12.5) | 2 (5.3) | |||
| other | 2 (9.1) | 0 | 2 (5.3) | |||
| without | 14 (63.6) | 10 (62.5) | 24 (63.2) | |||
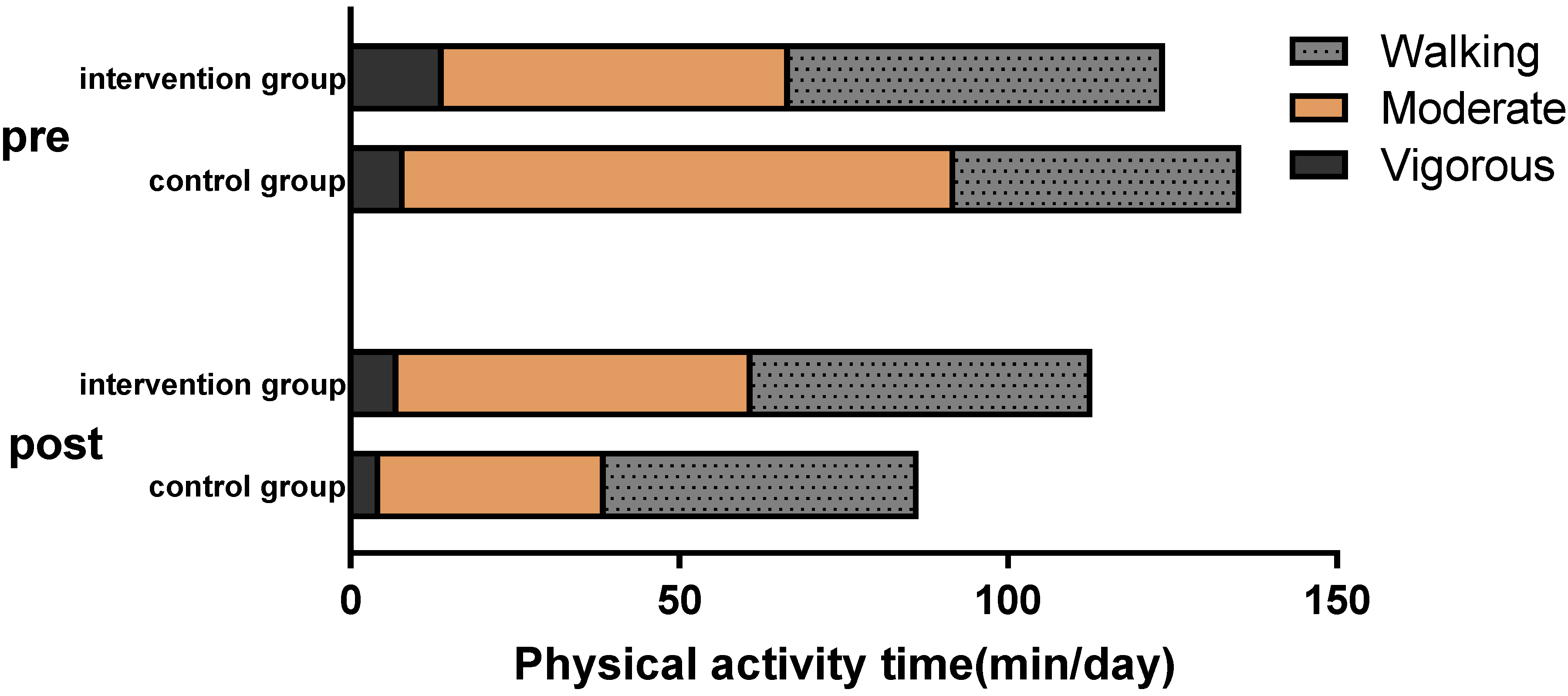
| Walking (min/day) | 57.0 (44.4) | 43.5 (41.1) | 51.3 (43.0) | 0.95 | 0.347 | |
| Moderate physical activity (min/day) | 52.6 (88.9) | 83.7 (83.9) | 65.8 (87.1) | −1.09 | 0.283 | |
| Vigorous physical activity (min/day) | 14.2 (31.7) | 8.2 (16.7) | 11.7 (26.3) | 0.68 | 0.499 | |
| Total physical activity (min/day) | 123.8 (97.2) | 135.5 (103.1) | 128.7 (98.5) | −0.36 | 0.724 |
| IG (n = 22), Mean (SD) | CG (n = 16), Mean (SD) | 0 Weeks vs. 12 Weeks | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Index | 0 Weeks | 12 Weeks | 0 Weeks | 12 Weeks | F | p | d | Effect Size | ||||
| Physical fitness | ||||||||||||
| BMI, kg/m2 | 23.84 | (2.8) | 23.33 | (2.58) | 23.65 | (3.69) | 23.86 | (3.54) | 9.814 | 0.004 * | −0.93 | L |
| Body fat rate, % | 24.78 | (8.57) | 25.95 | (7.16) | 25.13 | (6.75) | 26.14 | (6.78) | 0.070 | 0.793 | 0.03 | - |
| Systolic blood pressure, mmhg | 126.18 | (15.13) | 127.23 | (16.14) | 122.30 | (12.90) | 132.10 | (8.90) | 5.280 | 0.028 * | −0.68 | M |
| Diastolic blood pressure, mmhg | 75.68 | (8.81) | 74.91 | (6.89) | 70.80 | (10.40) | 77.30 | (8.20) | 6.418 | 0.016 * | −0.86 | L |
| Vital capacity, mL | 2570.82 | (785.61) | 2762.18 | (991.1) | 2646.60 | (736.4) | 2556.70 | (844.9) | 4.708 | 0.038 * | 0.67 | M |
| Grip strength, kg | 28.31 | (8.20) | 27.76 | (9.04) | 30.30 | (9.1) | 28.70 | (9.0) | 0.647 | 0.427 | 0.39 | S |
| Sitting forward, cm | 5.68 | (11.94) | 5.96 | (11.13) | 5.20 | (11.0) | 6.90 | (10.5) | 0.932 | 0.342 | −0.32 | S |
| Reaction time, s | 0.56 | (0.09) | 0.58 | (0.07) | 0.60 | (0.1) | 0.60 | (0.1) | 0.099 | 0.756 | 0.25 | S |
| Static balance | ||||||||||||
| Total length of the swing, mm (open Eyes) | 209.83 | (51.81) | 205.12 | (60.44) | 213.42 | (47.65) | 226.12 | (49.62) | 1.237 | 0.274 | −0.22 | S |
| Total velocity of the swing, mm/s (open Eyes) | 10.49 | (2.59) | 10.26 | (3.02) | 10.67 | (2.38) | 11.31 | (2.48) | 1.231 | 0.275 | −0.25 | S |
| Total area of swing, mm × s (open Eyes) | 212.90 | (124.10) | 181.63 | (105.58) | 194.34 | (65.61) | 202.78 | (69.23) | 1.097 | 0.303 | −0.33 | S |
| Total length of the swing, mm (Closed Eyes) | 271.48 | (82.40) | 230.85 | (74.57) | 257.31 | (80.44) | 288.58 | (95.86) | 3.728 | 0.062 | −0.62 | M |
| Total velocity of the swing, mm/s (Closed Eyes) | 13.57 | (4.12) | 11.55 | (3.73) | 12.87 | (4.02) | 14.43 | (4.77) | 3.740 | 0.062 | −0.62 | M |
| Total area of swing, mm × s (Closed Eyes) | 271.18 | (141.13) | 203.92 | (116.03) | 216.80 | (93.30) | 269.10 | (142.60) | 2.920 | 0.097 | −0.70 | M |
| Blood biochemical tests | ||||||||||||
| Total bilirubin, μmol/L | 16.87 | (3.54) | 13.42 | (2.22) | 16.29 | (3.73) | 13.82 | (3.54) | 0.666 | 0.421 | −0.31 | S |
| Direct bilirubin, μmol/L | 7.02 | (1.52) | 3.94 | (1.12) | 6.84 | (1.25) | 4.30 | (1.56) | 1.632 | 0.211 | −0.36 | S |
| Indirect bilirubin, μmol/L | 10.17 | (2.63) | 9.55 | (1.88) | 9.47 | (2.66) | 9.53 | (2.26) | 0.182 | 0.673 | −0.30 | S |
| Glutamic-pyruvic transaminase, μ/L | 24.41 | (18.86) | 25.79 | (13.25) | 27.78 | (33.88) | 26.00 | (12.78) | 0.261 | 0.613 | 0.16 | - |
| Glutamic oxalacetic transaminase, μ/L | 22.85 | (11.48) | 21.96 | (5.65) | 19.47 | (4.82) | 22.22 | (5.02) | 0.075 | 0.786 | −0.37 | S |
| Glucose, mmol/L | 4.80 | (0.75) | 5.15 | (0.85) | 4.87 | (0.60) | 5.14 | (0.94) | 0.500 | 0.485 | 0.14 | - |
| Urea, mmol/L | 5.33 | (1.28) | 6.74 | (1.58) | 5.55 | (1.24) | 6.38 | (1.27) | 2.780 | 0.105 | 0.51 | M |
| Creatinine, μmol/L | 69.92 | (14.95) | 73.36 | (12.61) | 72.80 | (10.84) | 73.56 | (11.46) | 1.062 | 0.310 | 0.33 | S |
| Uric acid, μmol/L | 331.86 | (97.26) | 279.55 | (73.84) | 346.83 | (80.59) | 309.19 | (69.49) | 1.691 | 0.203 | −0.29 | S |
| Total cholesterol, mmol/L | 5.50 | (0.96) | 5.40 | (0.97) | 5.30 | (1.17) | 4.94 | (0.91) | 7.020 | 0.012 | 0.37 | S |
| Triglyceride, mmol/L | 1.39 | (0.58) | 1.49 | (0.73) | 1.43 | (0.68) | 1.56 | (0.81) | 0.082 | 0.777 | −0.05 | - |
| High density cholesterol, mmol/L | 1.59 | (0.38) | 1.51 | (0.38) | 1.62 | (0.34) | 1.43 | (0.35) | 1.964 | 0.171 | 0.40 | S |
| Low density cholesterol, mmol/L | 3.35 | (0.73) | 3.23 | (0.78) | 3.10 | (0.79) | 2.78 | (0.53) | 9.469 | 0.004 | 0.34 | S |
| Insulin, μ/mL | 6.69 | (3.51) | 5.87 | (2.93) | 6.68 | (2.37) | 6.19 | (2.12) | 0.001 | 0.977 | −0.14 | - |
| IG (n = 22), Mean (SD) | CG (n = 16), Mean (SD) | 0 Weeks vs. 12 Weeks | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Index | 0 Weeks | 12 Weeks | 0 Weeks | 12 Weeks | F | p | d | Effect Size | ||||
| Symbol search | 29.14 | (6.33) | 29.91 | (7.00) | 30.10 | (7.30) | 30.00 | (7.20) | 0.103 | 0.751 | 0.19 | - |
| Operations span | 3.49 | (2.00) | 4.09 | (4.09) | 5.10 | (3.20) | 5.10 | (3.10) | 0.050 | 0.825 | 0.25 | S |
| Portrait memory | 19.50 | (6.06) | 19.59 | (7.58) | 20.70 | (9.20) | 18.20 | (8.80) | 1.413 | 0.243 | 0.38 | S |
| Spatial cognition | 5.00 | (3.04) | 5.86 | (2.80) | 4.90 | (2.30) | 3.90 | (2.90) | 8.261 | 0.007 * | 0.72 | M |
| Similar tests | 33.41 | (12.09) | 32.91 | (14.31) | 31.40 | (14.50) | 36.00 | (11.70) | 0.847 | 0.364 | −0.46 | S |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, C.; Zhao, C.; Li, Y.; Zhao, M.; Wang, L.; Guo, J.; Zhang, L.; Sun, Y.; Ye, X.; Zhu, W. The Effects of Active Video Game Exercise Based on Self-Determination Theory on Physical Fitness and Cognitive Function in Older Adults. J. Clin. Med. 2022, 11, 3984. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11143984
Zhao C, Zhao C, Li Y, Zhao M, Wang L, Guo J, Zhang L, Sun Y, Ye X, Zhu W. The Effects of Active Video Game Exercise Based on Self-Determination Theory on Physical Fitness and Cognitive Function in Older Adults. Journal of Clinical Medicine. 2022; 11(14):3984. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11143984
Chicago/Turabian StyleZhao, Chenglei, Chenxi Zhao, Yunfeng Li, Minmin Zhao, Lin Wang, Jiawei Guo, Longhai Zhang, Yuliang Sun, Xintong Ye, and Wenfei Zhu. 2022. "The Effects of Active Video Game Exercise Based on Self-Determination Theory on Physical Fitness and Cognitive Function in Older Adults" Journal of Clinical Medicine 11, no. 14: 3984. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11143984