
Impact of COVID-19 on Subclinical Placental Thrombosis and Maternal Thrombotic Factors

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Approval and Registration
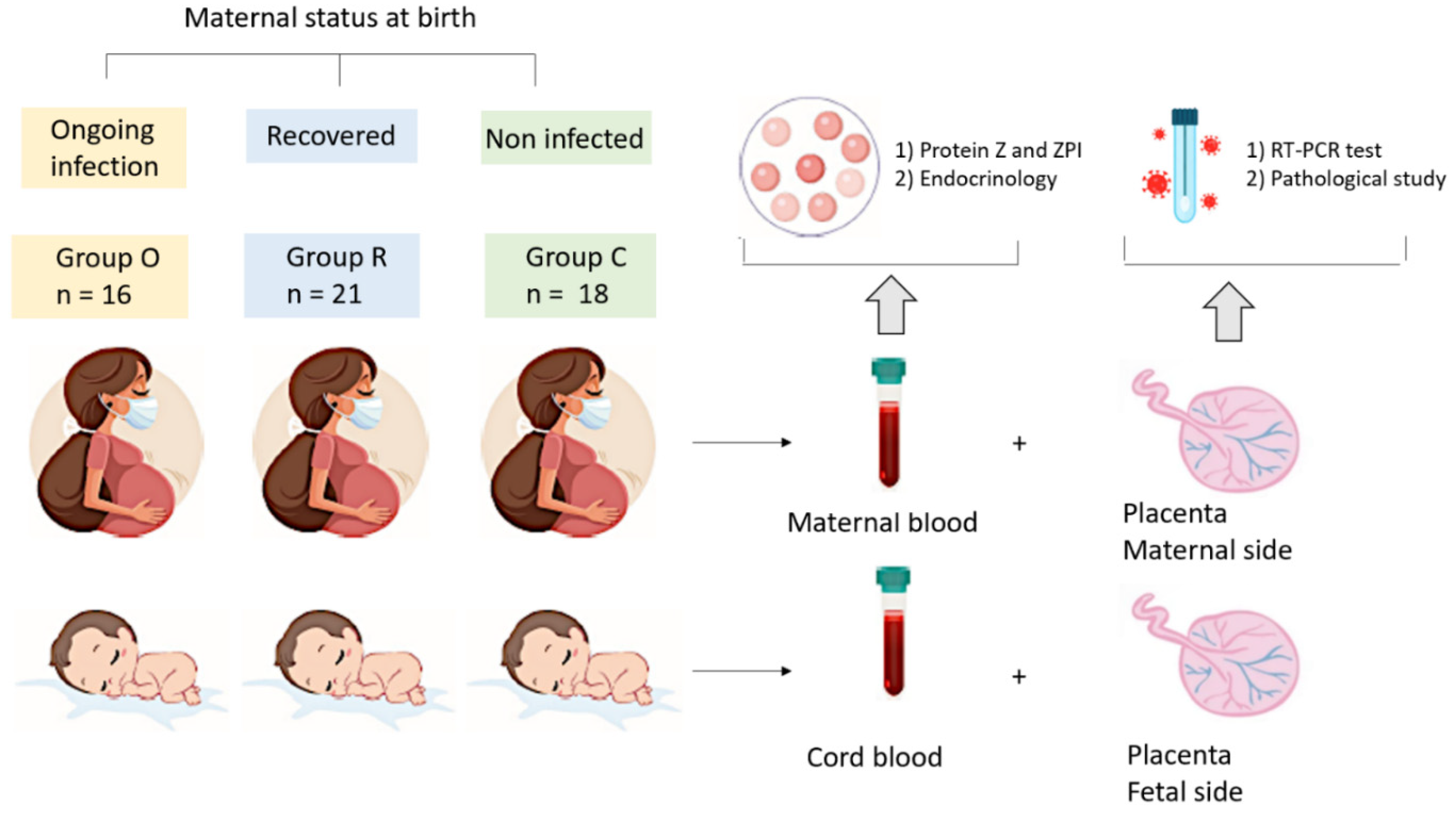
2.2. Participants and Data Collection
2.3. Biological and Placenta Analysis
2.4. Statistical Analysis
3. Results
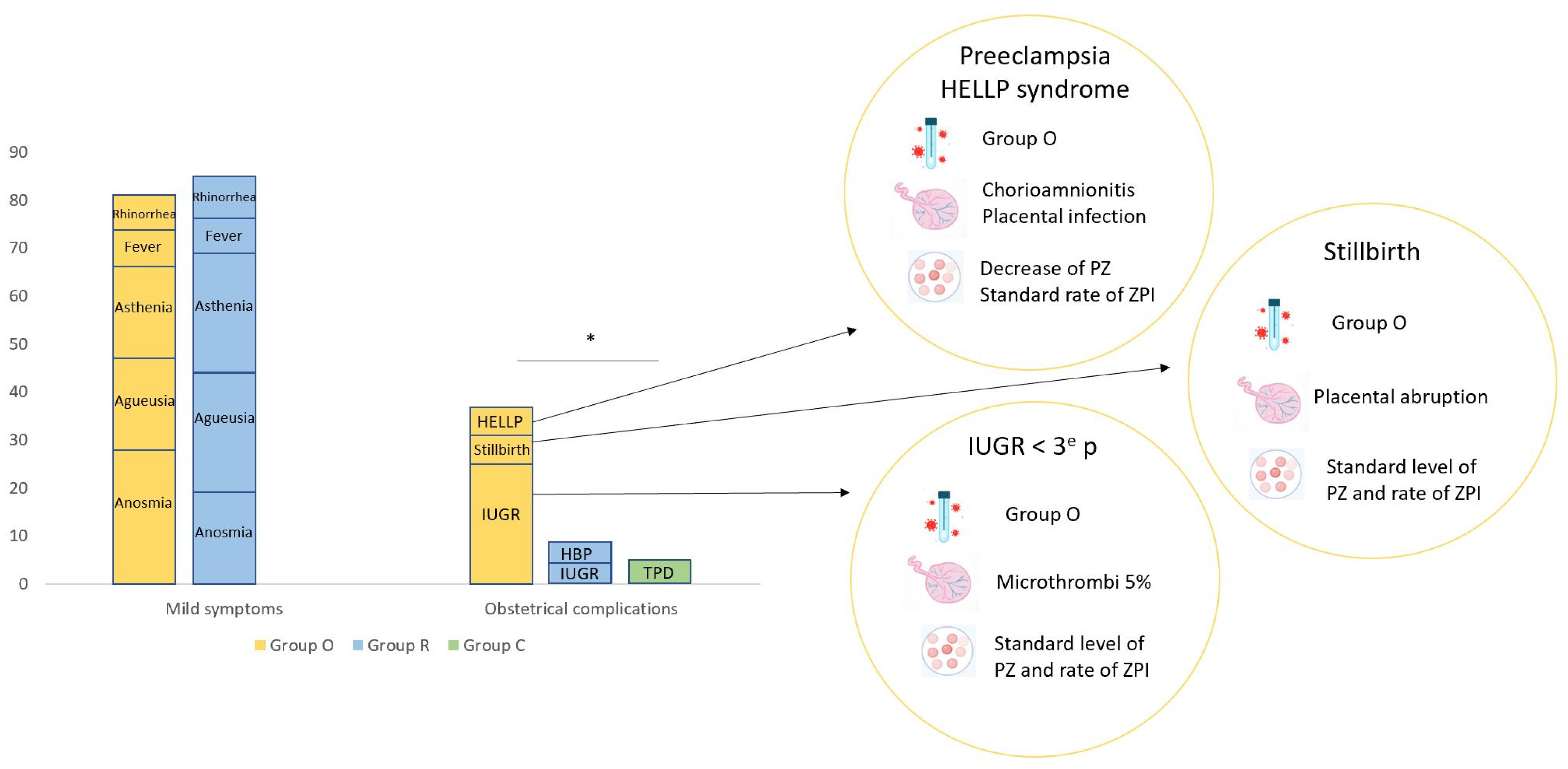
3.1. Demographic and Clinical Features of Study Groups
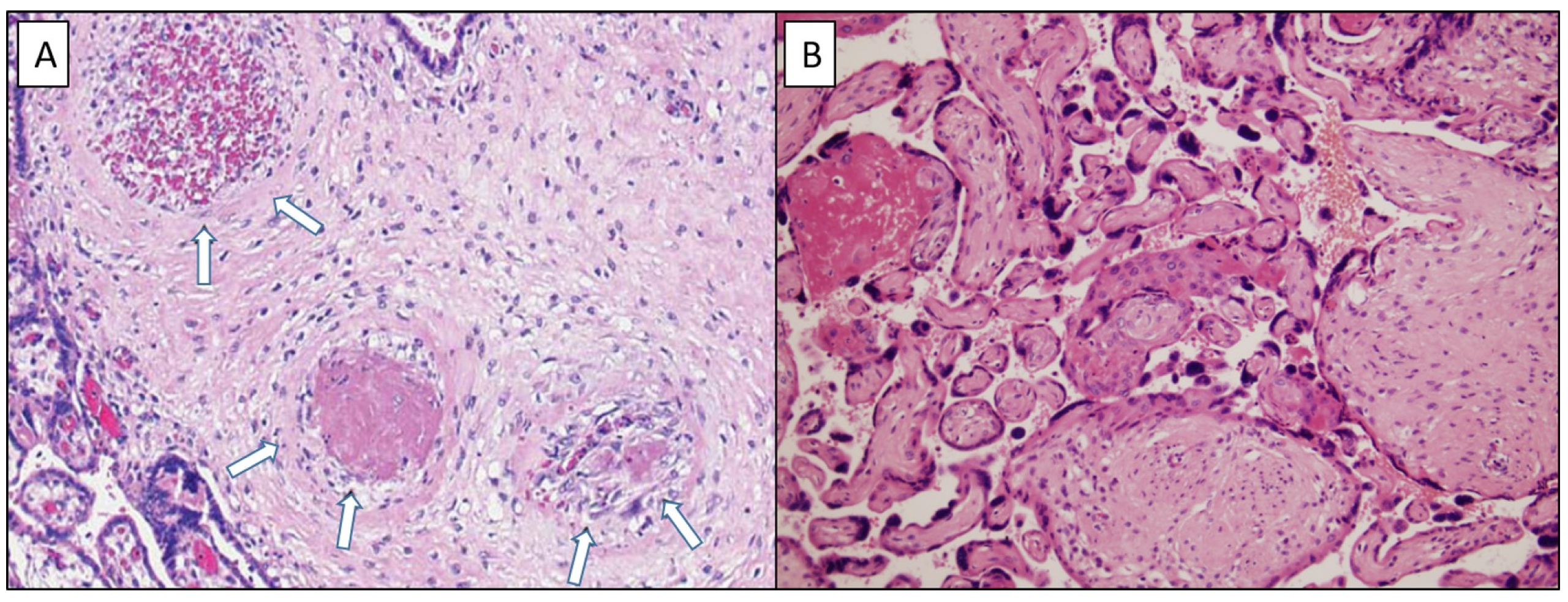
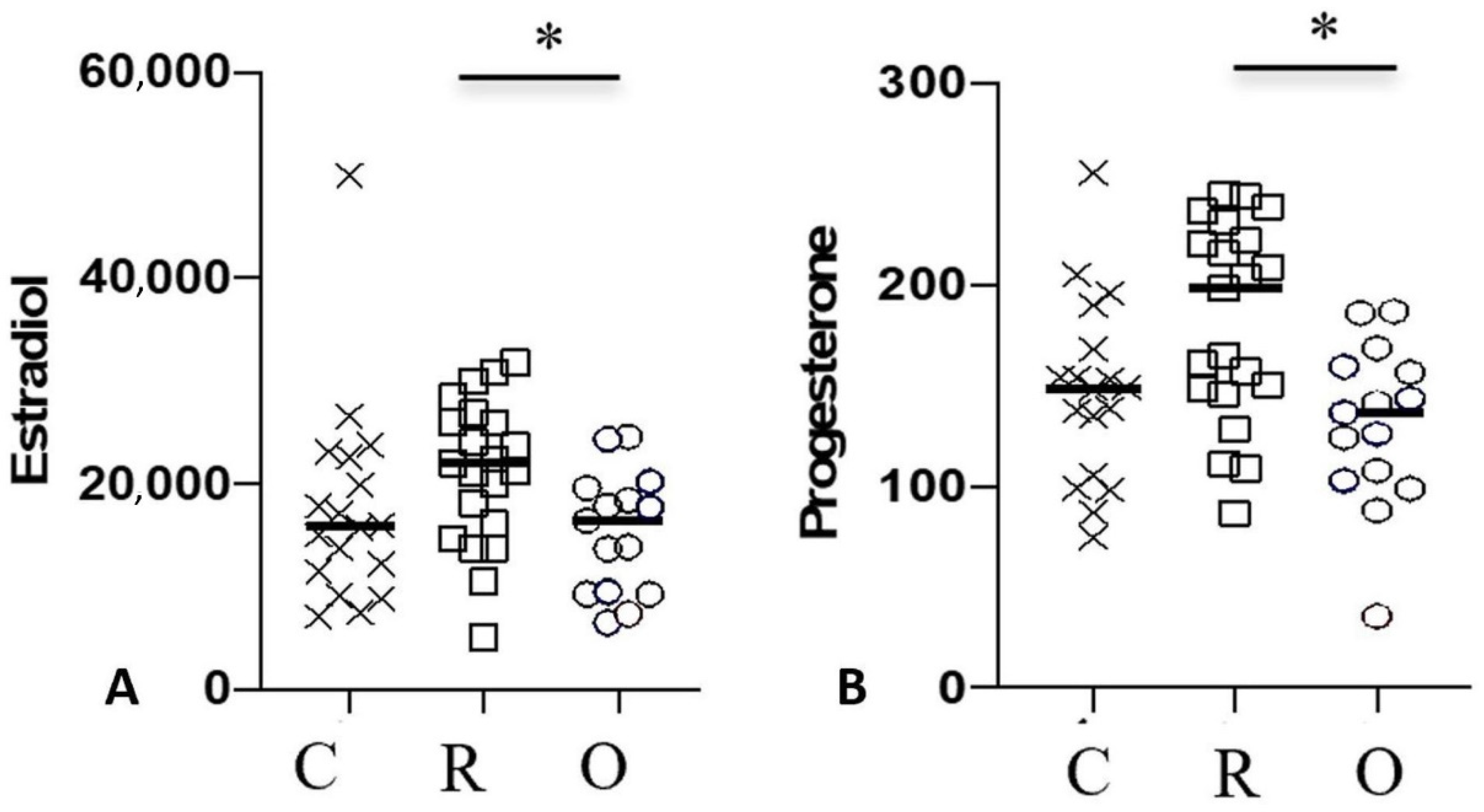
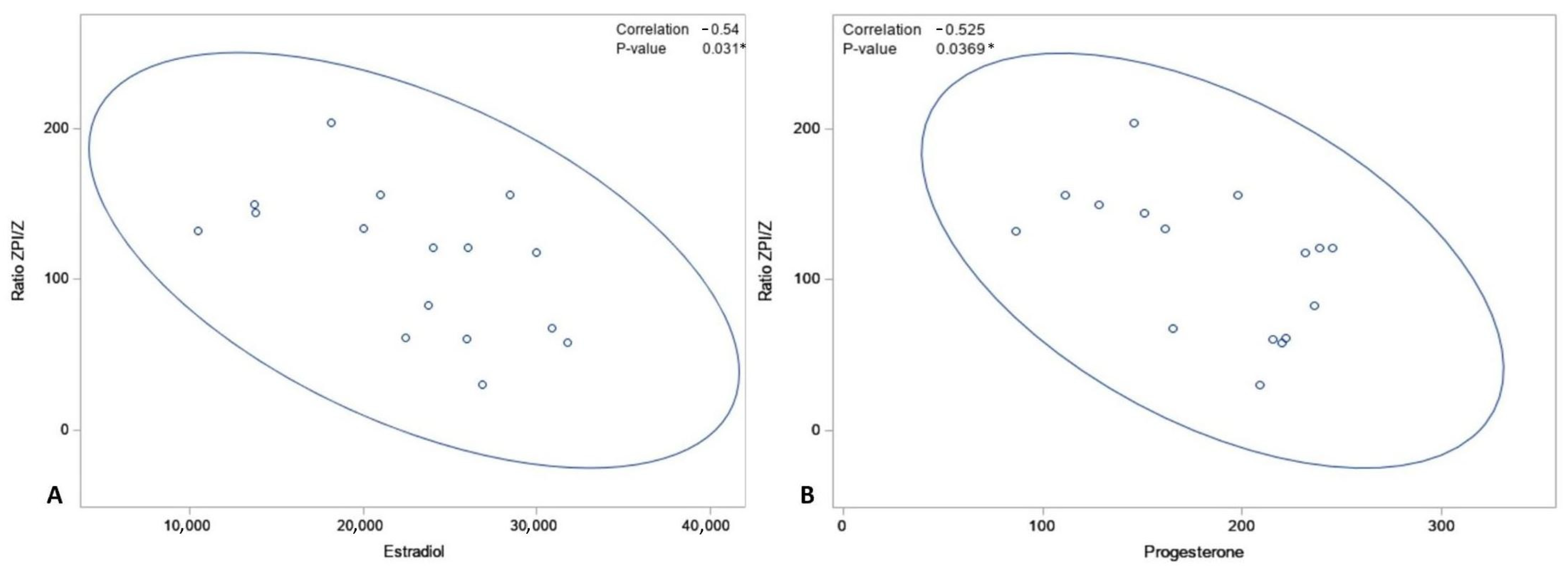
3.2. Placenta and Protein Z and ZPI Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Coronavirus (COVID-19) Dashboard [Internet]. Available online: https://covid19.who.int (accessed on 16 December 2021).
- Xie, Y.; Wang, Z.; Liao, H.; Marley, G.; Wu, D.; Tang, W. Epidemiologic, clinical, and laboratory findings of the COVID-19 in the current pandemic: Systematic review and meta-analysis. BMC Infect. Dis. 2020, 20, 640. [Google Scholar] [CrossRef] [PubMed]
- Cui, S.; Chen, S.; Li, X.; Liu, S.; Wang, F. Prevalence of venous thromboembolism in patients with severe novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 1421–1424. [Google Scholar] [CrossRef] [PubMed]
- Benhamou, D.; Keita, H.; Ducloy-Bouthors, A.S.; Bonnet, M.P.; Bonnin, M.; Bouthors, A.S.; Bouvet, L.; Castel, A.; Chassard, D.; Dewandre, P.Y.; et al. Coagulation changes and thromboembolic risk in COVID-19 obstetric patients. Anaesth. Crit. Care Pain Med. 2020, 39, 351–353. [Google Scholar] [CrossRef]
- Jafari, M.; Pormohammad, A.; Sheikh Neshin, S.A.; Ghorbani, S.; Bose, D.; Alimohammadi, S.; Basirjafari, S.; Mohammadi, M.; Rasmussen-Ivey, C.; Razizadeh, M.H.; et al. Clinical characteristics and outcomes of pregnant women with COVID-19 and comparison with control patients: A systematic review and meta-analysis. Rev. Med. Virol. 2021, 31, 1–16. [Google Scholar] [CrossRef]
- Conde-Agudelo, A.; Romero, R. SARS-CoV-2 infection during pregnancy and risk of preeclampsia: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2022, 226, 68–89.e3. [Google Scholar] [CrossRef]
- Male, V. SARS-CoV-2 infection and COVID-19 vaccination in pregnancy. Nat. Rev. Immunol. 2022, 22, 277–282. [Google Scholar] [CrossRef]
- Mastrolia, S.A.; Mazor, M.; Loverro, G.; Klaitman, V.; Erez, O. Placental vascular pathology and increased thrombin generation as mechanisms of disease in obstetrical syndromes. PeerJ 2014, 2, e653. [Google Scholar] [CrossRef] [Green Version]
- Huang, X.; Swanson, R.; Kroh, H.K.; Bock, P.E. Protein Z-dependent protease inhibitor (ZPI) is a physiologically significant inhibitor of prothrombinase function. J. Biol. Chem. 2019, 294, 7644–7657. [Google Scholar] [CrossRef]
- Bretelle, F.; Arnoux, D.; Shojai, R.; D’Ercole, C.; Sampol, J.; Dignat, F.; Camoin-Jau, L. Protein Z in patients with pregnancy complications. Am. J. Obstet. Gynecol. 2005, 193, 1698–1702. [Google Scholar] [CrossRef]
- Zhang, P.; Li, Y.C.; Li, L.; Lu, Y. Plasma concentration of protein Z-dependent protease inhibitor and ZPI exon 3 mutations in preeclampsia. J. Obstet. Gynaecol. 2021, 41, 1053–1056. [Google Scholar] [CrossRef]
- Almawi, W.Y.; Al-Shaikh, F.S.; Melemedjian, O.K.; Almawi AWProtein, Z. An anticoagulant protein with expanding role in reproductive biology. Reproduction 2013, 146, R73–R80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, C.; Huang, Y.; Guo, X.; Gu, C.; Guo, J.; Luo, X. Expression and diagnostic value of serum protein Z and protein Z-dependent protease inhibitor in fetal growth restriction. Ginekol. Pol. 2022; Online ahead of print. [Google Scholar]
- Razanakolona, M.; Adam, F.; Bianchini, E.; Saller, F.; Carvalho, A.; de Diehl, J.L.; Denis, C.V.; Meziani, F.; Borgel, D.; Helms, J.; et al. Anti-inflammatory Activity of the Protein Z-Dependent Protease Inhibitor. TH Open 2021, 5, e220–e229. [Google Scholar] [CrossRef] [PubMed]
- Redline, R.W.; Heller, D.; Keating, S.; Kingdom, J. Placental diagnostic criteria and clinical correlation—A workshop report. Placenta 2005, 26 (Suppl. A), S114–S117. [Google Scholar] [CrossRef] [PubMed]
- Cromi, A.; Ghezzi, F.; Dürig, P.; Di Naro, E.; Raio, L. Sonographic umbilical cord morphometry and coiling patterns in twin-twin transfusion syndrome. Prenat Diagn. 2005, 25, 851–855. [Google Scholar] [CrossRef]
- Shanes, E.D.; Mithal, L.B.; Otero, S.; Azad, H.A.; Miller, E.S.; Goldstein, J.A. Placental Pathology in COVID-19. Am. J. Clin. Pathol. 2020, 154, 23–32. [Google Scholar] [CrossRef]
- Flores-Pliego, A.; Miranda, J.; Vega-Torreblanca, S.; Valdespino-Vázquez, Y.; Helguera-Repetto, C.; Espejel-Nuñez, A.; Borboa-Olivares, H.; Espino y Sosa, S.; Mateu-Rogell, P.; León-Juárez, M.; et al. Molecular Insights into the Thrombotic and Microvascular Injury in Placental Endothelium of Women with Mild or Severe COVID-19. Cells 2021, 10, 364. [Google Scholar] [CrossRef]
- Jaiswal, N.; Puri, M.; Agarwal, K.; Singh, S.; Yadav, R.; Tiwary, N.; Tayal, P.; Vats, B. COVID-19 as an independent risk factor for subclinical placental dysfunction. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 259, 7–11. [Google Scholar] [CrossRef]
- Hecht, J.L.; Quade, B.; Deshpande, V.; Mino-Kenudson, M.; Ting, D.T.; Desai, N.; Dygulska, B.; Heyman, T.; Salafia, C.; Shen, D.; et al. SARS-CoV-2 can infect the placenta and is not associated with specific placental histopathology: A series of 19 placentas from COVID-19-positive mothers. Mod. Pathol. 2020, 33, 2092–2103. [Google Scholar] [CrossRef]
- Penfield, C.A.; Brubaker, S.G.; Limaye, M.A.; Lighter, J.; Ratner, A.J.; Thomas, K.M.; Meyer, J.A.; Roman, A.S. Detection of severe acute respiratory syndrome coronavirus 2 in placental and fetal membrane samples. Am. J. Obstet. Gynecol. MFM 2020, 2, 100133. [Google Scholar] [CrossRef]
- Sofi, F.; Cesari, F.; Abbate, R.; Gensini, G.F.; Broze, G.; Fedi, S. A meta-analysis of potential risks of low levels of protein Z for diseases related to vascular thrombosis. Thromb. Haemost. 2010, 103, 749–756. [Google Scholar]
- Girard, T.J.; Lasky, N.M.; Tuley, E.A.; Broze GJProtein, Z. protein Z-dependent protease inhibitor (serpinA10), and the acute-phase response. J. Thromb. Haemost. 2013, 11, 375–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khong, T.Y.; Mooney, E.E.; Ariel, I.; Balmus, N.C.M.; Boyd, T.K.; Brundler, M.A.; Derricott, H.; Evans, M.J.; Faye-Petersen, O.M.; Gillan, J.E.; et al. Sampling and Definitions of Placental Lesions: Amsterdam Placental Workshop Group Consensus Statement. Arch. Pathol. Lab. Med. 2016, 140, 698–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villar, J.; Ariff, S.; Gunier, R.B.; Thiruvengadam, R.; Rauch, S.; Kholin, A.; Roggero, P.; Prefumo, F.; Vale, M.S.D.; Cardona-Perez, J.A.; et al. Maternal and Neonatal Morbidity and Mortality Among Pregnant Women with and Without COVID-19 Infection: The INTERCOVID Multinational Cohort Study. JAMA Pediatr. 2021, 175, 817–826. [Google Scholar] [CrossRef] [PubMed]
- DeSisto, C.L.; Wallace, B.; Simeone, R.M.; Polen, K.; Ko, J.Y.; Meaney-Delman, D.; Ellington, S.R. Risk for Stillbirth Among Women with and Without COVID-19 at Delivery Hospitalization—United States, March 2020-September 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1640–1645. [Google Scholar] [CrossRef] [PubMed]
- Peyronnet, V.; Sibiude, J.; Huissoud, C.; Lescure, F.X.; Lucet, J.C.; Mandelbrot, L.; Nisand, I.; Belaish-Allart, J.; Vayssière, C.; Yazpandanah, Y.; et al. Infection with SARS-CoV-2 in pregnancy. Update of Information and proposed care. CNGOF. Gynecol. Obstet. Fertil. Senol. 2020, 48, 858–870. [Google Scholar]
- Daclin, C.; Carbonnel, M.; Rossignol, M.; Abbou, H.; Trabelsi, H.; Cimmino, A.; Delmas, J.; Rifai, A.-S.; Coiquaud, L.-A.; Tiberon, A.; et al. Impact of COVID-19 infection in pregnancy and neonates: A case control study. J. Gynecol. Obstet. Hum. Reprod. 2022, 51, 102366. [Google Scholar] [CrossRef] [PubMed]
- Vivanti, A.J.; Mattern, J.; Vauloup-Fellous, C.; Jani, J.; Rigonnot, L.; Hachem, L.E.; Le Gouez, A.; Desconclois, C.; Ben M’Barek, I.; Sibiude, J.; et al. Retrospective Description of Pregnant Women Infected with Severe Acute Respiratory Syndrome Coronavirus 2, France—Volume 26, Number 9—September 2020—Emerging Infectious Diseases Journal—CDC. Available online: https://wwwnc.cdc.gov/eid/article/26/9/20-2144_article (accessed on 22 December 2021).
- Wong, Y.P.; Khong, T.Y.; Tan, G.C. The Effects of COVID-19 on Placenta and Pregnancy: What Do We Know So Far? Diagnostics 2021, 11, 94. [Google Scholar] [CrossRef]
- Mavedatnia, D.; Tran, J.; Oltean, I.; Bijelić, V.; Moretti, F.; Lawrence, S.; El Demellawy, D. Impact of Co-Existing Placental Pathologies in Pregnancies Complicated by Placental Abruption and Acute Neonatal Outcomes. J. Clin. Med. 2021, 10, 5693. [Google Scholar] [CrossRef]
- Suhren, J.T.; Meinardus, A.; Hussein, K.; Schaumann, N. Meta-analysis on COVID-19-pregnancy-related placental pathologies shows no specific pattern. Placenta 2022, 117, 72–77. [Google Scholar] [CrossRef]
- Campello, E.; Radu, C.M.; Simion, C.; Spiezia, L.; Bulato, C.; Gavasso, S.; Tormene, D.; Perin, N.; Turatti, G.; Simioni, P. Longitudinal Trend of Plasma Concentrations of Extracellular Vesicles in Patients Hospitalized for COVID-19. Front. Cell. Dev. Biol. 2021, 9, 770463. [Google Scholar] [CrossRef]
- Campello, E.; Spiezia, L.; Radu, C.M.; Dhima, S.; Visentin, S.; Valle, F.D.; Tormene, D.; Woodhams, B.; Cosmi, E.; Simioni, P. Circulating microparticles in umbilical cord blood in normal pregnancy and pregnancy with preeclampsia. Thromb. Res. 2015, 136, 427–431. [Google Scholar] [CrossRef] [PubMed]
- Kotlyar, A.M.; Grechukhina, O.; Chen, A.; Popkhadze, S.; Grimshaw, A.; Tal, O.; Taylor, H.S.; Tal, R. Vertical transmission of coronavirus disease 2019: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2021, 224, 35–53.e3. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, R.; Malhamé, I.; Teshler, L.; Acharya, G.; Hunt, B.J.; McLintock, C. A critical review of the pathophysiology of thrombotic complications and clinical practice recommendations for thromboprophylaxis in pregnant patients with COVID-19. Acta Obstet. Gynecol. Scand. 2020, 99, 1110–1120. [Google Scholar] [CrossRef] [PubMed]
- Mauvais-Jarvis, F.; Klein, S.L.; Levin, E.R. Estradiol, Progesterone, Immunomodulation, and COVID-19 Outcomes. Endocrinology 2020, 161, bqaa127. [Google Scholar] [CrossRef]
- Zafari Zangeneh, F.; Sarmast Shoushtari, M. Estradiol and COVID-19: Does 17-Estradiol Have an Immune-Protective Function in Women Against Coronavirus? J. Fam. Reprod. Health 2021, 15, 150–159. [Google Scholar] [CrossRef]
- Murtada, R.; Carbonnel, M.; Revaux, A.; Favre-Inhofer, A.; Ayoubi, J.M. Managing a Department of Obstetrics and Gynecology in Times of COVID-19 Outbreak: The Foch Hospital Experience. Front. Surg. 2021, 8, 564145. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Maternal SARS-CoV-2 Status | Group O | Group R | Group C | p Value |
|---|---|---|---|---|
| Maternal Characteristics (n) | n = 16 | n = 21 | n = 18 | |
| Median age, years (min–max) | 34.0 (21–40) | 31.0 (24–43) | 32.5 (26–44) | 0.52 |
| Median BMI (min–max) | 28.4 (21–36) | 25.5 (19–31) | 27.0 (22–34) | 0.09 |
| BMI > 30 kg/m2 | 4 (25%) | 2 (9.5%) | 4 (22%) | 0.29 |
| Gravidity, mean (min–max) | 1.0 (1–3) | 1.5 (1–7) | 1.0 (1–3) | 0.65 |
| Parity, mean (min–max) | 0 (0–2) | 1.0 (0–3) | 1.0 (0–3) | 0.08 |
| Asthma | 0 | 2 (10%) | 2 (11%) | 0.54 |
| High blood pressure | 0 | 0 | 0 | NA |
| History of Preeclampsia | 1 (6%) | 0 | 0 | 0.29 |
| Diabetes | 0 | 0 | 0 | NA |
| Gestational age of COVID-19 infection Median (min–max) | 38 (30–41) | 27 (8–37) | NA | <0.001 |
| Days between positive SARS-CoV-2+ status (nasopharyngeal swab) and birth, median (min–max) | 7 (0–56) | 84 (21–225) | NA | <0.001 |
| Positive IgG serology at inclusion | 8 (50%) | 15 (71%) | 0 | <0.001 |
| COVID-19 symptoms | 13 (87%) | 18 (86%) | NA | 1 |
| Fever | 4 (25%) | 5 (24%) | NA | 1 |
| Cough | 6 (37%) | 9 (43%) | NA | 0.74 |
| Asthenia | 5 (31%) | 11 (52%) | NA | 0.20 |
| Anosmia | 7 (44%) | 10 (48%) | NA | 0.81 |
| Ageusia | 5 (31%) | 11 (52%) | NA | 0.20 |
| Rhinorrhea | 3 (19%) | 7 (33%) | NA | 0.46 |
| Asymptomatic | 3 (14%) | 2 (13%) | NA | 1 |
| Severity signs | 2 (12%) | 1 (5%) | NA | 0.56 |
| Hospitalization | 3 (19%) | 0 | 3 (17%) | 0.09 |
| Hospitalization for COVID-19 | 1 (6%) | 0 | 0 | 0.29 |
| Total number of obstetrical complications | 6 (37%) | 2 (10%) | 1 (6%) | 0.03 |
| Stillbirth | 1 (6%) | 0 | 0 | 0.29 |
| High Blood Pressure | 0 | 1 (5%) | 0 | 1 |
| Preeclampsia | 1 (6%) | 0 | 0 | 0.29 |
| Threat of premature delivery | 1 (6%) | 0 | 1 (6%) | 0.52 |
| IUGR | 4 (25%) | 1 (5%) | 0 | 0.10 |
| Term at birth median (min–max) | 39 (29–41) | 40 (37–41) | 39.5 (37–41) | 0.68 |
| Pyrexia during labor | 1 (6%) | 0 | 0 | 0.29 |
| Neonatal characteristics (n) | n = 16 | n = 21 | n = 18 | |
| Cesarean section (mode of delivery) | 3 (19%) | 4 (19%) | 1 (6%) | 0.45 |
| Weight median (g) (min–max) | 3100 (1484–4140) | 3320 (2760–4270) | 3515 (2660–4198) | 0.13 |
| pH median (min–max) | 7.25 (7.20–7.35) | 7.24 (7.08–7.43) | 7.23 (7.09–7.45) | 0.26 |
| Transfer to ICU | 2 (13%) | 0 | 0 | 0.07 |
| Respiratory distress | 1 (6%) | 1 (5%) | 0 | 0.75 |
| Group O n = 16 | Group R n = 19 | Group C n = 18 | p Value | |
|---|---|---|---|---|
| Vascular malperfusion | 9 (56%) | 8 (42%) | 8 (44%) | 0.68 |
| Maternal side | ||||
| Villous infarct | 5 (31%) | 4 (21%) | 6 (33%) | 0.68 |
| Volume (%) | 3 (2–4) | 3 (1–5) | 2 (2–5) | 0.67 |
| Microthrombi | 6 (37%) | 6 (32%) | 4 (22%) | 0.62 |
| Affected vessels (%) | 5 (2–5) | 5 (2–5) | 2 (2–5) | 0.19 |
| Deciduous arteriopathy | 0 | 0 | 0 | - |
| Retroplacental hemorrhage | 1 (6%) | 0 | 0 | 1 |
| Fetal side | ||||
| Subchorionic thrombosis | 3 (19%) | 3 (16%) | 0 | 0.11 |
| Surface (%) | 5 (2–20) | 2 (1–2) | - | 0.16 |
| Chorionic thrombosis | 0 | 0 | 0 | - |
| Acute chorioamnionitis | 3 (19%) | 1 (5%) | 0 | 0.10 |
| Group O | Group R | Group C | p Value | |
|---|---|---|---|---|
| Maternal blood | n = 14 | n = 16 | n = 18 | |
| PZ | 2.7 (0.6–4.4) | 2.3 (0.9–4.4) | 2.1 (1.2–4.6) | 0.49 |
| ZPI | 173.5 (63.0–247.0) | 187.5 (89.0–288.0) | 164.5 (81.0–276.0) | 0.51 |
| Ratio ZPI/Z | 64.4 (44.8–216.7) | 66.7 (42.7–145.0) | 69.9 (38.5–130.7) | 0.87 |
| Fetal cord blood | n = 14 | n = 17 | n = 17 | |
| PZ | 0.4 (0.1–2.3) | 0.4 (0.2–0.7) | 0.5 (0.02–0.7) | 0.49 |
| ZPI | 34.0 (17.0–194.0) | 45.0 (17.0–92.0) | 35.0 (15.0–55.0) | 0.3 |
| Ratio ZPI/Z | 82.6 (41.3–743.6) | 120.7 (29.8–203.5) | 66.8 (28.2–2043.5) | 0.04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carbonnel, M.; Daclin, C.; Tourne, M.; Roux, E.; Le-Marchand, M.; Racowsky, C.; Kennel, T.; Farfour, E.; Vasse, M.; Ayoubi, J.-M. Impact of COVID-19 on Subclinical Placental Thrombosis and Maternal Thrombotic Factors. J. Clin. Med. 2022, 11, 4067. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11144067
Carbonnel M, Daclin C, Tourne M, Roux E, Le-Marchand M, Racowsky C, Kennel T, Farfour E, Vasse M, Ayoubi J-M. Impact of COVID-19 on Subclinical Placental Thrombosis and Maternal Thrombotic Factors. Journal of Clinical Medicine. 2022; 11(14):4067. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11144067
Chicago/Turabian StyleCarbonnel, Marie, Camille Daclin, Morgan Tourne, Emmanuel Roux, Mathilde Le-Marchand, Catherine Racowsky, Titouan Kennel, Eric Farfour, Marc Vasse, and Jean-Marc Ayoubi. 2022. "Impact of COVID-19 on Subclinical Placental Thrombosis and Maternal Thrombotic Factors" Journal of Clinical Medicine 11, no. 14: 4067. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11144067