
Clinical, Microbiological, and Biochemical Impact of the Surgical Treatment of Peri-Implantitis—A Prospective Case Series

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study design
- Presence of at least one implant with peri-implantitis, defined as: radiographic evidence of bone loss >2 mm, inflammation of the peri-implant mucosa as defined by positive BoP and/or suppuration, and at least one site with PD ≥ 5 mm.
- Based on the radiographic examination, the affected implant should not have a vertical peri-implant defect. Positive selection was based on the presence of peri-implant lesions wider than 4 mm, with an angle greater than 35°.
- In patients with a history of periodontitis, periodontal therapy should have been provided at least 6 months prior to the initiation of the study.
- Presence of relevant medical conditions and/or systemic medications that would contraindicate the surgical procedure or modify the tissue response after therapy.
- Patients requiring antibiotic prophylaxis.
- Heavy smokers (>10 cigarettes/day).
- Pregnant or lactating women.
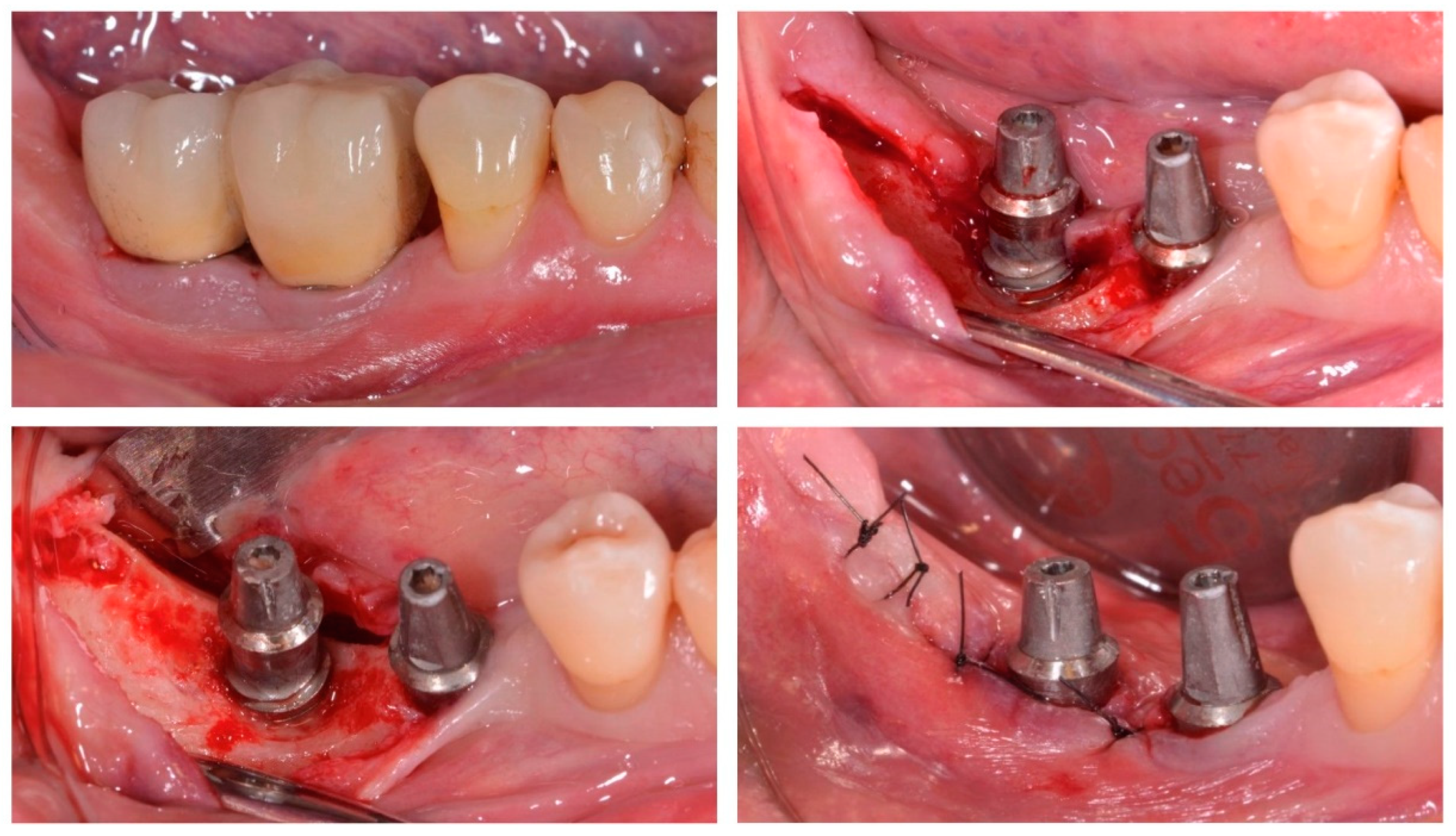
2.2. Interventions
2.3. Outcome Variables
2.4. Data Analysis
3. Results
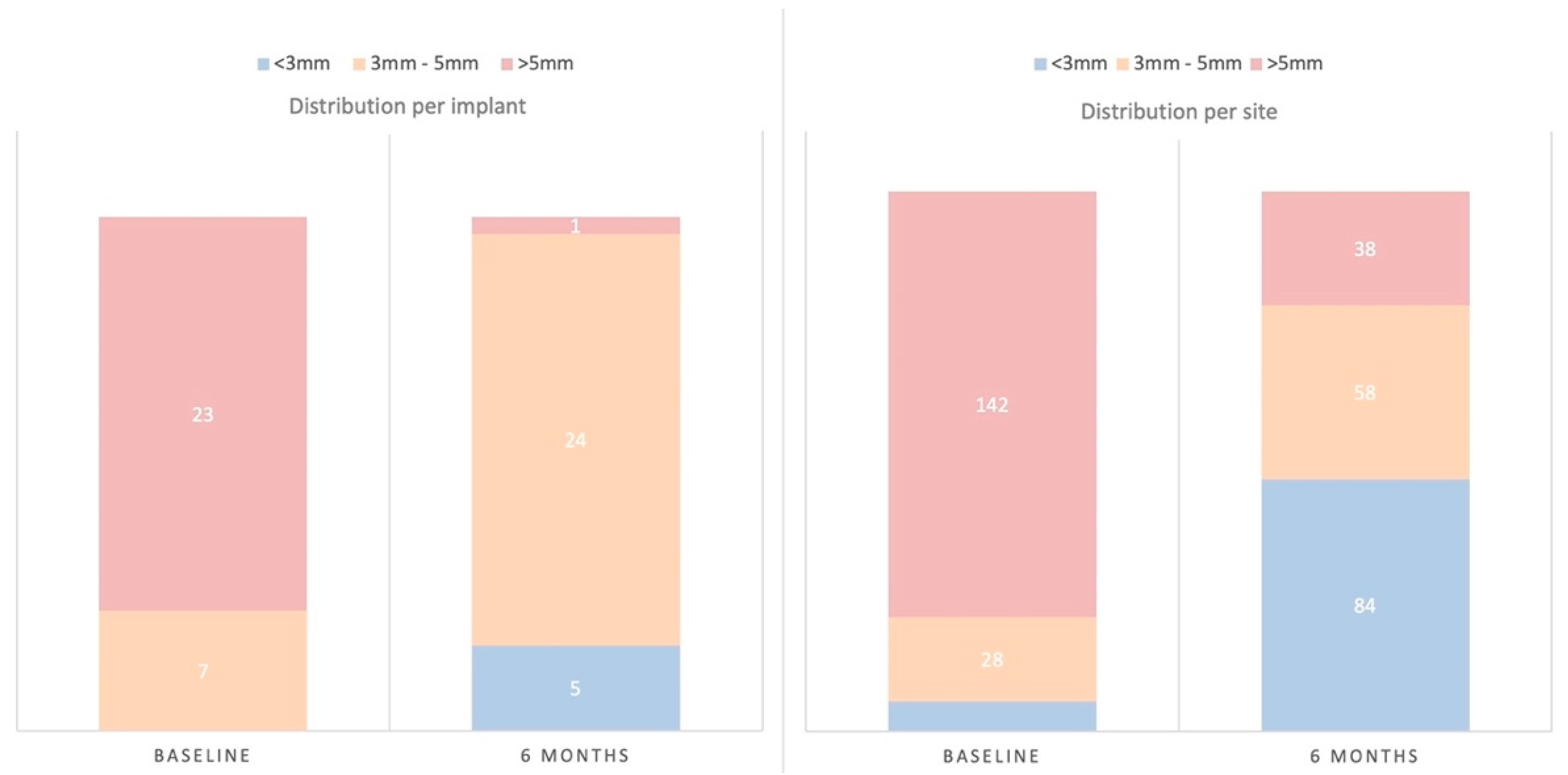
- Clinical outcome variables: PD showed, at 6 months post-surgery, a significant mean reduction of 2.14 mm (SD = 1.07) (p < 0.001), with a significant concomitant mean increase in REC of 1.00 mm (SD = 0.77) (p < 0.001) (Table 1). Implant sites with PD >5 mm at baseline showed PD of 3 mm or less, at 6 months post-surgery, in 76.67% of the cases; only one implant (3%) maintained sites >5 mm after therapy (Figure 2). Implant sites with PD between 3–5 mm at baseline were maintained within this category in 57.14% of the cases, while in 42.86%, it was reduced to <3 mm.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Probing Depth | Recession | Bleeding on Probing | Suppuration | Plaque | Radiographic Bone Loss | |
|---|---|---|---|---|---|---|
| Baseline | 5.80 ± 1.17 | 0.09 ± 0.17 | 90.00% ± 17.29 | 7.78% ± 18.94 | 72.22% ± 34.56 | 3.79 ± 1.15 |
| 6 months | 3.66 ± 0.69 | 1.09 ± 0.74 | 27.78% ± 17.69 | 0.00% ± 0.00 | 31.67% ± 27.80 | 3.76 ± 1.27 |
| Change | −2.14 ± 1.07 | 1.00 ± 0.77 | −62.22% ± 24.34 | −7.78% ± 18.94 | −40.56% ± 26.51 | −0.03 ± 0.61 |
| p-value | p < 0.001 * | p < 0.001 * | p < 0.001 * | p = 0.039 * | p < 0.001 * | p = 0.789 |
- Microbiological outcome variables: Counts, proportions, and frequencies of detection of the targeted bacterial species did not show statistically significant changes (Table 4) except for the reduction in the proportions of P. micra (p = 0.023).
- Changes in biomarkers in GCF: The measured inflammatory biomarkers demonstrated reductions in their quantitative levels (expressed in pg.) although these changes were only statistically significant for IL-8 (p = 0.010) (Table 5).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45 (Suppl. 20), 286–291. [Google Scholar] [CrossRef] [PubMed]
- Derks, J.; Tomasi, C. Peri-implant health and disease. A systematic review of current epidemiology. J. Clin. Periodontol. 2015, 42 (Suppl. 16), S158–S171. [Google Scholar] [CrossRef]
- Lindhe, J.; Meyle, J.; Group D of European Workshop on Periodontology. Peri-implant diseases: Consensus Report of the Sixth European Workshop on Periodontology. J. Clin. Periodontol. 2008, 35 (Suppl. 8), 282–285. [Google Scholar] [CrossRef] [PubMed]
- Rakic, M.; Galindo-Moreno, P.; Monje, A.; Radovanovic, S.; Wang, H.L.; Cochran, D.; Sculean, A.; Canullo, L. How frequent does peri-implantitis occur? A systematic review and meta-analysis. Clin. Oral. Investig. 2018, 22, 1805–1816. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo, D.; Sanz-Sanchez, I.; Figuero, E.; Llodra, J.C.; Bravo, M.; Caffesse, R.G.; Vallcorba, N.; Guerrero, A.; Herrera, D. Prevalence and risk indicators of peri-implant diseases in Spain. J. Clin. Periodontol. 2018, 45, 1510–1520. [Google Scholar] [CrossRef] [PubMed]
- Romandini, M.; Lima, C.; Pedrinaci, I.; Araoz, A.; Soldini, M.C.; Sanz, M. Prevalence and risk/protective indicators of peri-implant diseases: A university-representative cross-sectional study. Clin. Oral Implant. Res. 2021, 32, 112–122. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Chapple, I.L.; Jepsen, S.; Sanz, M. Primary and secondary prevention of periodontal and peri-implant diseases: Introduction to, and objectives of the 11th European Workshop on Periodontology consensus conference. J. Clin. Periodontol. 2015, 42 (Suppl. 16), S1–S4. [Google Scholar] [CrossRef] [PubMed]
- Renvert, S.; Persson, G.R.; Pirih, F.Q.; Camargo, P.M. Peri-implant health, peri-implant mucositis, and peri-implantitis: Case definitions and diagnostic considerations. J. Clin. Periodontol. 2018, 45 (Suppl. 20), S278–S285. [Google Scholar] [CrossRef]
- Charalampakis, G.; Leonhardt, A.; Rabe, P.; Dahlen, G. Clinical and microbiological characteristics of peri-implantitis cases: A retrospective multicentre study. Clin. Oral Implant. Res. 2012, 23, 1045–1054. [Google Scholar] [CrossRef]
- Mombelli, A.; Muller, N.; Cionca, N. The epidemiology of peri-implantitis. Clin. Oral Implant. Res. 2012, 23 (Suppl. 6), 67–76. [Google Scholar] [CrossRef] [PubMed]
- Leonhardt, A.; Dahlen, G.; Renvert, S. Five-year clinical, microbiological, and radiological outcome following treatment of peri-implantitis in man. J. Periodontol. 2003, 74, 1415–1422. [Google Scholar] [CrossRef]
- Quirynen, M.; De Soete, M.; van Steenberghe, D. Infectious risks for oral implants: A review of the literature. Clin. Oral Implant. Res. 2002, 13, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Alassy, H.; Parachuru, P.; Wolff, L. Peri-Implantitis Diagnosis and Prognosis Using Biomarkers in Peri-Implant Crevicular Fluid: A Narrative Review. Diagnostics 2019, 9, 214. [Google Scholar] [CrossRef]
- Severino, V.O.; Beghini, M.; de Araujo, M.F.; de Melo, M.L.R.; Miguel, C.B.; Rodrigues, W.F.; de Lima Pereira, S.A. Expression of IL-6, IL-10, IL-17 and IL-33 in the peri-implant crevicular fluid of patients with peri-implant mucositis and peri-implantitis. Arch. Oral Biol. 2016, 72, 194–199. [Google Scholar] [CrossRef]
- Duarte, P.M.; Serrao, C.R.; Miranda, T.S.; Zanatta, L.C.; Bastos, M.F.; Faveri, M.; Figueiredo, L.C.; Feres, M. Could cytokine levels in the peri-implant crevicular fluid be used to distinguish between healthy implants and implants with peri-implantitis? A systematic review. J. Periodontal. Res. 2016, 51, 689–698. [Google Scholar] [CrossRef] [PubMed]
- Renvert, S.; Widen, C.; Persson, G.R. Cytokine expression in peri-implant crevicular fluid in relation to bacterial presence. J. Clin Periodontol. 2015, 42, 697–702. [Google Scholar] [CrossRef]
- Renvert, S.; Widen, C.; Persson, R.G. Cytokine and microbial profiles in relation to the clinical outcome following treatment of peri-implantitis. Clin. Oral Implant. Res. 2017, 28, 1127–1132. [Google Scholar] [CrossRef]
- Ramanauskaite, A.; Fretwurst, T.; Schwarz, F. Efficacy of alternative or adjunctive measures to conventional non-surgical and surgical treatment of peri-implant mucositis and peri-implantitis: A systematic review and meta-analysis. Int. J. Implant. Dent. 2021, 7, 112. [Google Scholar] [CrossRef]
- Khoury, F.; Keeve, P.L.; Ramanauskaite, A.; Schwarz, F.; Koo, K.T.; Sculean, A.; Romanos, G. Surgical treatment of peri-implantitis—Consensus report of working group 4. Int. Dent. J. 2019, 69 (Suppl. 2), 18–22. [Google Scholar] [CrossRef] [PubMed]
- Figuero, E.; Graziani, F.; Sanz, I.; Herrera, D.; Sanz, M. Management of peri-implant mucositis and peri-implantitis. Periodontology 2000 2014, 66, 255–273. [Google Scholar] [CrossRef] [PubMed]
- Ramanauskaite, A.; Daugela, P.; Faria de Almeida, R.; Saulacic, N. Surgical Non-Regenerative Treatments for Peri-Implantitis: A Systematic Review. J. Oral Maxillofac. Res. 2016, 7, e14. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; Chapple, I.L.; Working Group 4 of the VIII European Workshop on Periodontology. Clinical research on peri-implant diseases: Consensus report of Working Group 4. J. Clin. Periodontol. 2012, 39 (Suppl. 12), 202–206. [Google Scholar] [CrossRef] [PubMed]
- Suarez-Lopez Del Amo, F.; Yu, S.H.; Wang, H.L. Non-Surgical Therapy for Peri-Implant Diseases: A Systematic Review. J. Oral Maxillofac. Res. 2016, 7, e13. [Google Scholar] [CrossRef]
- Schwarz, F.; Schmucker, A.; Becker, J. Efficacy of alternative or adjunctive measures to conventional treatment of peri-implant mucositis and peri-implantitis: A systematic review and meta-analysis. Int. J. Implant. Dent. 2015, 1, 22. [Google Scholar] [CrossRef] [PubMed]
- Faggion, C.M., Jr.; Listl, S.; Fruhauf, N.; Chang, H.J.; Tu, Y.K. A systematic review and Bayesian network meta-analysis of randomized clinical trials on non-surgical treatments for peri-implantitis. J. Clin. Periodontol. 2014, 41, 1015–1025. [Google Scholar] [CrossRef] [PubMed]
- Muthukuru, M.; Zainvi, A.; Esplugues, E.O.; Flemmig, T.F. Non-surgical therapy for the management of peri-implantitis: A systematic review. Clin. Oral Implant. Res. 2012, 23 (Suppl. 6), 77–83. [Google Scholar] [CrossRef] [PubMed]
- Nart, J.; Pons, R.; Valles, C.; Esmatges, A.; Sanz-Martin, I.; Monje, A. Non-surgical therapeutic outcomes of peri-implantitis: 12-month results. Clin. Oral Investig. 2020, 24, 675–682. [Google Scholar] [CrossRef]
- Linares, A.; Pico, A.; Blanco, C.; Blanco, J. Adjunctive Systemic Metronidazole to Nonsurgical Therapy of Peri-implantitis with Intrabony Defects: A Retrospective Case Series Study. Int. J. Oral Maxillofac. Implant. 2019, 34, 1237–1245. [Google Scholar] [CrossRef]
- Estefania-Fresco, R.; Garcia-de-la-Fuente, A.M.; Egana-Fernandez-Valderrama, A.; Bravo, M.; Aguirre-Zorzano, L.A. One-year results of a nonsurgical treatment protocol for peri-implantitis. A retrospective case series. Clin. Oral Implant. Res. 2019, 30, 702–712. [Google Scholar] [CrossRef]
- Renvert, S.; Polyzois, I.; Claffey, N. Surgical therapy for the control of peri-implantitis. Clin. Oral Implant. Res. 2012, 23 (Suppl. 6), 84–94. [Google Scholar] [CrossRef] [PubMed]
- Roccuzzo, A.; Stahli, A.; Monje, A.; Sculean, A.; Salvi, G.E. Peri-Implantitis: A Clinical Update on Prevalence and Surgical Treatment Outcomes. J. Clin. Med. 2021, 10, 1107. [Google Scholar] [CrossRef] [PubMed]
- Lasserre, J.F.; Brecx, M.C.; Toma, S. Implantoplasty Versus Glycine Air Abrasion for the Surgical Treatment of Peri-implantitis: A Randomized Clinical Trial. Int. J. Oral Maxillofac. Implant. 2020, 35, 197–206. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.A.; Salvi, G.E.; Mombelli, A.; Loup, P.J.; Heitz, F.; Kruger, E.; Lang, N.P. Supportive peri-implant therapy following anti-infective surgical peri-implantitis treatment: 5-year survival and success. Clin. Oral Implant. Res. 2018, 29, 1–6. [Google Scholar] [CrossRef]
- Toma, S.; Brecx, M.C.; Lasserre, J.F. Clinical Evaluation of Three Surgical Modalities in the Treatment of Peri-Implantitis: A Randomized Controlled Clinical Trial. J. Clin. Med. 2019, 8, 966. [Google Scholar] [CrossRef] [PubMed]
- Berglundh, T.; Wennstrom, J.L.; Lindhe, J. Long-term outcome of surgical treatment of peri-implantitis. A 2–11-year retrospective study. Clin. Oral Implant. Res. 2018, 29, 404–410. [Google Scholar] [CrossRef] [PubMed]
- Carcuac, O.; Derks, J.; Abrahamsson, I.; Wennstrom, J.L.; Petzold, M.; Berglundh, T. Surgical treatment of peri-implantitis: 3-year results from a randomized controlled clinical trial. J. Clin. Periodontol. 2017, 44, 1294–1303. [Google Scholar] [CrossRef] [PubMed]
- Sahm, N.; Becker, J.; Santel, T.; Schwarz, F. Non-surgical treatment of peri-implantitis using an air-abrasive device or mechanical debridement and local application of chlorhexidine: A prospective, randomized, controlled clinical study. J. Clin. Periodontol. 2011, 38, 872–878. [Google Scholar] [CrossRef] [PubMed]
- Keim, D.; Nickles, K.; Dannewitz, B.; Ratka, C.; Eickholz, P.; Petsos, H. In vitro efficacy of three different implant surface decontamination methods in three different defect configurations. Clin. Oral Implant. Res. 2019, 30, 550–558. [Google Scholar] [CrossRef]
- Cha, J.K.; Paeng, K.; Jung, U.W.; Choi, S.H.; Sanz, M.; Sanz-Martin, I. The effect of five mechanical instrumentation protocols on implant surface topography and roughness: A scanning electron microscope and confocal laser scanning microscope analysis. Clin. Oral Implant. Res. 2019, 30, 578–587. [Google Scholar] [CrossRef] [PubMed]
- Ronay, V.; Merlini, A.; Attin, T.; Schmidlin, P.R.; Sahrmann, P. In vitro cleaning potential of three implant debridement methods. Simulation of the non-surgical approach. Clin. Oral Implant. Res. 2017, 28, 151–155. [Google Scholar] [CrossRef]
- Sahrmann, P.; Ronay, V.; Hofer, D.; Attin, T.; Jung, R.E.; Schmidlin, P.R. In vitro cleaning potential of three different implant debridement methods. Clin. Oral Implant. Res. 2015, 26, 314–319. [Google Scholar] [CrossRef]
- Renvert, S.; Polyzois, I. Treatment of pathologic peri-implant pockets. Periodontology 2000 2018, 76, 180–190. [Google Scholar] [CrossRef] [PubMed]
- Cha, J.K.; Lee, J.S.; Kim, C.S. Surgical Therapy of Peri-Implantitis with Local Minocycline: A 6-Month Randomized Controlled Clinical Trial. J. Dent. Res. 2019, 98, 288–295. [Google Scholar] [CrossRef]
- Carcuac, O.; Derks, J.; Charalampakis, G.; Abrahamsson, I.; Wennstrom, J.; Berglundh, T. Adjunctive Systemic and Local Antimicrobial Therapy in the Surgical Treatment of Peri-implantitis: A Randomized Controlled Clinical Trial. J. Dent. Res. 2016, 95, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Syed, S.A.; Loesche, W.J. Survival of human dental plaque flora in various transport media. Appl. Microbiol. 1972, 24, 638–644. [Google Scholar] [CrossRef]
- Alsina, M.; Olle, E.; Frias, J. Improved, low-cost selective culture medium for Actinobacillus actinomycetemcomitans. J. Clin. Microbiol. 2001, 39, 509–513. [Google Scholar] [CrossRef] [PubMed]
- Serino, G.; Turri, A. Outcome of surgical treatment of peri-implantitis: Results from a 2-year prospective clinical study in humans. Clin. Oral Implant. Res. 2011, 22, 1214–1220. [Google Scholar] [CrossRef] [PubMed]
- Serino, G.; Turri, A.; Lang, N.P. Probing at implants with peri-implantitis and its relation to clinical peri-implant bone loss. Clin. Oral Implant. Res. 2013, 24, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulos, C.A.; Vouros, I.; Menexes, G.; Konstantinidis, A. The utilization of a diode laser in the surgical treatment of peri-implantitis. A randomized clinical trial. Clin. Oral Investig. 2015, 19, 1851–1860. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.; Salvi, G.E.; Mombelli, A.; Faddy, M.; Lang, N.P.; On behalf of the Implant Complication Research Group Anti-infective surgical therapy of peri-implantitis. A 12-month prospective clinical study. Clin. Oral Implant. Res. 2012, 23, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Hallstrom, H.; Persson, G.R.; Lindgren, S.; Renvert, S. Open flap debridement of peri-implantitis with or without adjunctive systemic antibiotics: A randomized clinical trial. J. Clin. Periodontol. 2017, 44, 1285–1293. [Google Scholar] [CrossRef] [PubMed]
- Roos-Jansaker, A.M.; Persson, G.R.; Lindahl, C.; Renvert, S. Surgical treatment of peri-implantitis using a bone substitute with or without a resorbable membrane: A 5-year follow-up. J. Clin. Periodontol. 2014, 41, 1108–1114. [Google Scholar] [CrossRef] [PubMed]
- Roos-Jansaker, A.M.; Renvert, H.; Lindahl, C.; Renvert, S. Surgical treatment of peri-implantitis using a bone substitute with or without a resorbable membrane: A prospective cohort study. J. Clin. Periodontol. 2007, 34, 625–632. [Google Scholar] [CrossRef] [PubMed]
- De Waal, Y.C.M.; Vangsted, T.E.; Van Winkelhoff, A.J. Systemic antibiotic therapy as an adjunct to non-surgical peri-implantitis treatment: A single-blind RCT. J. Clin. Periodontol. 2021, 48, 996–1006. [Google Scholar] [CrossRef] [PubMed]
- Polymeri, A.; van der Horst, J.; Anssari Moin, D.; Wismeijer, D.; Loos, B.G.; Laine, M.L. Non-surgical peri-implantitis treatment with or without systemic antibiotics: A randomized controlled clinical trial. Clin. Oral Implant. Res. 2022, 33, 548–557. [Google Scholar] [CrossRef]
- Oen, M.; Leknes, K.N.; Lund, B.; Bunaes, D.F. The efficacy of systemic antibiotics as an adjunct to surgical treatment of peri-implantitis: A systematic review. BMC Oral Health 2021, 21, 666. [Google Scholar] [CrossRef] [PubMed]
- Monje, A.; Mesquita, P.F. Clinical considerations in the surgical management of peri-implantitis lesions in the esthetic zone. J. Esthet. Restor. Dent. 2022. Online ahead of print. [Google Scholar] [CrossRef]
- Serino, G.; Turri, A.; Lang, N.P. Maintenance therapy in patients following the surgical treatment of peri-implantitis: A 5-year follow-up study. Clin. Oral Implant. Res. 2015, 26, 950–956. [Google Scholar] [CrossRef] [PubMed]
- Lagervall, M.; Jansson, L.E. Treatment outcome in patients with peri-implantitis in a periodontal clinic: A retrospective study. J. Periodontol. 2013, 84, 1365–1373. [Google Scholar] [CrossRef]
- Roccuzzo, M.; Layton, D.M.; Roccuzzo, A.; Heitz-Mayfield, L.J. Clinical outcomes of peri-implantitis treatment and supportive care: A systematic review. Clin. Oral Implant. Res. 2018, 29 (Suppl. 16), 331–350. [Google Scholar] [CrossRef] [PubMed]
- Heitz-Mayfield, L.J. Peri-implant diseases: Diagnosis and risk indicators. J. Clin. Periodontol. 2008, 35, 292–304. [Google Scholar] [CrossRef]
- Schwarz, F.; Derks, J.; Monje, A.; Wang, H.L. Peri-implantitis. J. Clin. Periodontol. 2018, 45 (Suppl. 20), 246–266. [Google Scholar] [CrossRef] [PubMed]
- Serino, G.; Strom, C. Peri-implantitis in partially edentulous patients: Association with inadequate plaque control. Clin. Oral Implant. Res. 2009, 20, 169–174. [Google Scholar] [CrossRef]
- de Tapia, B.; Mozas, C.; Valles, C.; Nart, J.; Sanz, M.; Herrera, D. Adjunctive effect of modifying the implant-supported prosthesis in the treatment of peri-implant mucositis. J. Clin. Periodontol. 2019, 46, 1050–1060. [Google Scholar] [CrossRef] [PubMed]
- Dalago, H.R.; Schuldt Filho, G.; Rodrigues, M.A.; Renvert, S.; Bianchini, M.A. Risk indicators for Peri-implantitis. A cross-sectional study with 916 implants. Clin. Oral Implant. Res. 2017, 28, 144–150. [Google Scholar] [CrossRef]
- Renvert, S.; Quirynen, M. Risk indicators for peri-implantitis. A narrative review. Clin. Oral Implant. Res. 2015, 26 (Suppl. 11), 15–44. [Google Scholar] [CrossRef]
- Blanco, J.; Pico, A.; Caneiro, L.; Novoa, L.; Batalla, P.; Martin-Lancharro, P. Effect of abutment height on interproximal implant bone level in the early healing: A randomized clinical trial. Clin. Oral Implant. Res. 2018, 29, 108–117. [Google Scholar] [CrossRef] [PubMed]
- Molina, A.; Sanz-Sanchez, I.; Martin, C.; Blanco, J.; Sanz, M. The effect of one-time abutment placement on interproximal bone levels and peri-implant soft tissues: A prospective randomized clinical trial. Clin. Oral Implant. Res. 2017, 28, 443–452. [Google Scholar] [CrossRef] [PubMed]
- Galindo-Moreno, P.; Leon-Cano, A.; Ortega-Oller, I.; Monje, A.; Suarez, F.; F, O.V.; Spinato, S.; Catena, A. Prosthetic Abutment Height is a Key Factor in Peri-implant Marginal Bone Loss. J. Dent. Res. 2014, 93 (Suppl. 7), 80–85. [Google Scholar] [CrossRef]
- Axelsson, P.; Paulander, J.; Lindhe, J. Relationship between smoking and dental status in 35-, 50-, 65-, and 75-year-old individuals. J. Clin. Periodontol. 1998, 25, 297–305. [Google Scholar] [CrossRef]
- Tomar, S.L.; Asma, S. Smoking-attributable periodontitis in the United States: Findings from NHANES III. National Health and Nutrition Examination Survey. J. Periodontol. 2000, 71, 743–751. [Google Scholar] [CrossRef] [PubMed]
- Bergstrom, J. Periodontitis and smoking: An evidence-based appraisal. J. Evid. Based Dent. Pract. 2006, 6, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.S.; Mason, M.R.; Brooker, M.R.; O’Brien, K. Pyrosequencing reveals unique microbial signatures associated with healthy and failing dental implants. J. Clin. Periodontol. 2012, 39, 425–433. [Google Scholar] [CrossRef]
- Javed, F.; Al-Hezaimi, K.; Salameh, Z.; Almas, K.; Romanos, G.E. Proinflammatory cytokines in the crevicular fluid of patients with peri-implantitis. Cytokine 2011, 53, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.L.; Garaicoa-Pazmino, C.; Collins, A.; Ong, H.S.; Chudri, R.; Giannobile, W.V. Protein biomarkers and microbial profiles in peri-implantitis. Clin. Oral Implant. Res. 2016, 27, 1129–1136. [Google Scholar] [CrossRef] [PubMed]
- Panagakos, F.S.; Aboyoussef, H.; Dondero, R.; Jandinski, J.J. Detection and measurement of inflammatory cytokines in implant crevicular fluid: A pilot study. Int. J. Oral Maxillofac. Implant. 1996, 11, 794–799. [Google Scholar]
- Ataoglu, H.; Alptekin, N.O.; Haliloglu, S.; Gursel, M.; Ataoglu, T.; Serpek, B.; Durmus, E. Interleukin-1beta, tumor necrosis factor-alpha levels and neutrophil elastase activity in peri-implant crevicular fluid. Clin. Oral Implant. Res. 2002, 13, 470–476. [Google Scholar] [CrossRef]
- Duarte, P.M.; Reis, A.F.; de Freitas, P.M.; Ota-Tsuzuki, C. Bacterial adhesion on smooth and rough titanium surfaces after treatment with different instruments. J. Periodontol. 2009, 80, 1824–1832. [Google Scholar] [CrossRef]



| Component | n (%) |
|---|---|
| Probing depth (PD) < 5 mm | 29 (97%) |
| No bleeding on probing (BoP) | 17 (56.67%) |
| No additional bone loss (<0.5 mm change) | 27 (90.0%) |
| Combinations | n (%) |
| PD < 5 mm and no BoP | 17 (56.67%) |
| PD < 5 mm and no bone loss (<0.5 mm) | 26 (86.67%) |
| No BoP and no bone loss (<0.5 mm) | 17 (56.67%) |
| PD < 5 mm, no BoP, no bone loss (<0.5 mm) | 17 (56.67%) |
| Patient-Related Factors | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gender | Smoker | Additional Implants with Peri-implantitis | Compliance with Supportive Care | |||||||||
| Male | Female | Non-smoker | Smoker | Former Smoker | No | Yes | Full Compliance | Occasionally/Not Attended | ||||
| n/N (%) | 12/12 (100%) | 11/18 (61.1%) | 13/16 (81.3%) | 7/11 (63.6%) | 3/3 (100%) | 10/12 (83.3%) | 13/18 (72.2%) | 20/20 (100%) | 3/10 (30%) | |||
| p | 0.014 * | 0.342 | 0.481 | <0.001 * | ||||||||
| Implant-related Factors | ||||||||||||
| Platform switching connection | Mechanized collar neck | Presence of microthread | Implant design | Connection type | ||||||||
| No | Yes | No | Yes | No | Yes | 1-piece implant | 2-piece implant | External connection | Internal connection | |||
| n/N (%) | 18/24 (75.0%) | 5/6 (83.3%) | 17/22 (77.3%) | 6/8 (75.0%) | 19/24 (79.2%) | 4/6 (66.7%) | 3/3 (100%) | 20/27 (74.1%) | 11/14 (78.6%) | 12/16 (75.0%) | ||
| p | 0.666 | 0.896 | 0.517 | 0.314 | 0.818 | |||||||
| Prosthetic-related Factors | ||||||||||||
| Restoration size | Prosthesis material | Implant connection misfit | Prosthesis retention | Transepithelial abutment height | ||||||||
| Single crown | Bridge | Overdenture | Metal–ceramic | Metal–resin | No | Yes | Screw-retained | Cement-retained | 1 mm | 2 mm | 3 mm | |
| n/N (%) | 3/4 (75.0%) | 16/21 (76.2%) | 4/5 (80.0%) | 19/25 (76.0%) | 4/5 (80.0%) | 12/16 (75.0%) | 11/14 (78.6%) | 20/24 (83.3%) | 3/6 (50.0%) | 4/5 (80.0%) | 2/2 (100%) | ½ (50%) |
| p | 0.980 | 0.847 | 0.818 | 0.084 | 0.697 | |||||||
| Outcome | Total Anaerobic Counts | Aggregatibacter Actinomycetemcomitans | Porphyromonas Gingivalis | Prevotella Intermedia | Tannerella Forsythia | Parvimonas Micra | Fusobacterium Nucleatum | Campylobacter Rectus | |
|---|---|---|---|---|---|---|---|---|---|
| Baseline | Counts | 6.14 ± 0.92 | 0.31 ± 1.17 | 3.62 ± 2.72 | 2.76 ± 2.46 | 1.12 ± 2.08 | 1.90 ± 2.41 | 2.80 ± 2.24 | 0.29 ± 1.12 |
| Proportions | 0.06% ± 0.25 | 10.63% ± 15.97 | 3.40% ± 6.89 | 0.46% ± 0.95 | 5.14% ± 10.79 | 1.36% ± 2.10 | 0.14% ± 0.59 | ||
| Frequency | 6.70% | 66.70% | 60.00% | 23.30% | 40.00% | 63.30% | 6.70% | ||
| Detection (n) | 2 | 20 | 18 | 7 | 12 | 19 | 2 | ||
| 6 Months | Counts | 6.15 ± 0.76 | 0.14 ± 0.75 | 3.17 ± 2.76 | 2.31 ± 2.31 | 0.99 ± 2.02 | 0.92 ± 1.89 | 3.67 ± 1.82 | 0.23 ± 0.90 |
| Proportions | 0.05% ± 0.29 | 12.37% ± 21.78 | 1.68% ± 4.25 | 0.46% ± 1.21 | 0.62% ± 1.32 | 2.22% ± 2.25 | 0.16% ± 0.83 | ||
| Frequency | 3.30% | 60.00% | 53.30% | 20.00% | 20.00% | 83.30% | 6.70% | ||
| Detection (n) | 1 | 18 | 16 | 6 | 6 | 25 | 2 | ||
| Changes | Counts | 0.01 ± 1.13 | −0.17 ± 0.83 | −0.45 ± 3.31 | −0.45 ± 3.24 | −0.13 ± 2.67 | −0.98 ± 2.92 | 0.86 ± 2.63 | −0.06 ± 1.48 |
| p-value | 0.766 | 0.180 | 0.475 | 0.449 | 0.929 | 0.088 | 0.084 | 0.715 | |
| Proportions | −0.01% ± 0.32 | 1.74% ± 28.83 | −1.72% ± 8.18 | 0.01% ± 1.49 | 4.52% ± 10.98 | 0.86% ± 2.87 | 0.02% ± 1.04 | ||
| p-value | 0.655 | 0.732 | 0.317 | 0.656 | 0.023 * | 0.088 | 1.000 | ||
| Frequency | −3.4% | −6.7% | −6.7% | −3.3% | −20.0% | 20.00% | 0.00% | ||
| p-value | 1.000 | 0.754 | 0.791 | 1.000 | 0.146 | 0.146 | 1.000 |
| Interleukin 1β | Interleukin 6 | Interleukin 8 | Tumor Necrosis Factor α | |
|---|---|---|---|---|
| Baseline | 17.96 ± 30.98 | 0.70 ± 2.10 | 180.51 ± 240.99 | 0.65 ± 0.75 |
| 6 months | 12.42 ± 30.10 | 0.52 ± 1.07 | 57.09 ± 51.70 | 0.49 ± 0.90 |
| Change (%) | −5.54 ± 41.86 (−30.85%) | −0.18 ± 2.42 (−25.71%) | −123.42 ± 245.89 (−68.37%) | −0.16 ± 1.29 (−24.62%) |
| p-value | 0.474 | 0.692 | 0.010 * | 0.490 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luengo, F.; Solonko, M.; Sanz-Esporrín, J.; Sanz-Sánchez, I.; Herrera, D.; Sanz, M. Clinical, Microbiological, and Biochemical Impact of the Surgical Treatment of Peri-Implantitis—A Prospective Case Series. J. Clin. Med. 2022, 11, 4699. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11164699
Luengo F, Solonko M, Sanz-Esporrín J, Sanz-Sánchez I, Herrera D, Sanz M. Clinical, Microbiological, and Biochemical Impact of the Surgical Treatment of Peri-Implantitis—A Prospective Case Series. Journal of Clinical Medicine. 2022; 11(16):4699. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11164699
Chicago/Turabian StyleLuengo, Fernando, Myroslav Solonko, Javier Sanz-Esporrín, Ignacio Sanz-Sánchez, David Herrera, and Mariano Sanz. 2022. "Clinical, Microbiological, and Biochemical Impact of the Surgical Treatment of Peri-Implantitis—A Prospective Case Series" Journal of Clinical Medicine 11, no. 16: 4699. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11164699