
Can Leukotriene Receptor Antagonist Therapy Improve the Control of Patients with Severe Asthma on Biological Therapy and Coexisting Bronchiectasis? A Pilot Study

 , , ,
, , ,  , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Study Design
- Need of inhaled reliever medication, adherence to therapy.
- Time of asthmatic disease expressed in years.
- Skin prick test (SPT) was performed in accordance with the guidelines [13].
- In accordance with the guidelines [14], flow/volume (F/V) spirometry and plethysmography were performed. We measured and recorded the forced vital capacity (FVC) and the forced expiratory volume during the first second of the forced breath (FEV1) from the F/V Spirometry and the residual volume (RV) from the plethysmography. The best of three reproducible measurements was selected and expressed as a percentage of the predicted value.
- A venous blood sample was taken, and white blood cell (WBC) values were recorded: WBCs, eosinophilia (EOS) and total immunoglobulin E (IgE).
- The number of courses of oral corticosteroid (OCS)/year, which is defined as the annual number of OCS prescriptions. The mean dose of OCS prescribed is reported as prednisone-equivalent dosages.
- The number of antibiotic courses/year, which is defined as the annual number of antibiotic prescriptions
- The number of bronchial exacerbations/year, which is defined as the presence of symptoms related to either an asthma exacerbation or a bronchiectasis exacerbation. Asthma exacerbations are defined as acute worsening in symptoms and lung function from the patient’s usual status [4]. Bronchiectasis exacerbations are defined by an increase in daily respiratory symptoms such as cough, sputum production, malaise, fatigue and breathlessness [5].
- The number of unscheduled specialist visits/year: number of urgent and unscheduled pulmonary visits without subsequent hospitalization in the last year.
- The number of hospitalizations/year: number of hospitalizations due to bronchial exacerbations caused by asthma and/or bronchiectasis in the last year.
2.3. Skin Prick Test
2.4. Lung Function
2.5. FeNO Measurement
2.6. Data Analysis
3. Results
3.1. Demographics and Baseline Characteristics
3.2. Comparison between Group
3.2.1. Comparison within the Entire Population between T0 and T1
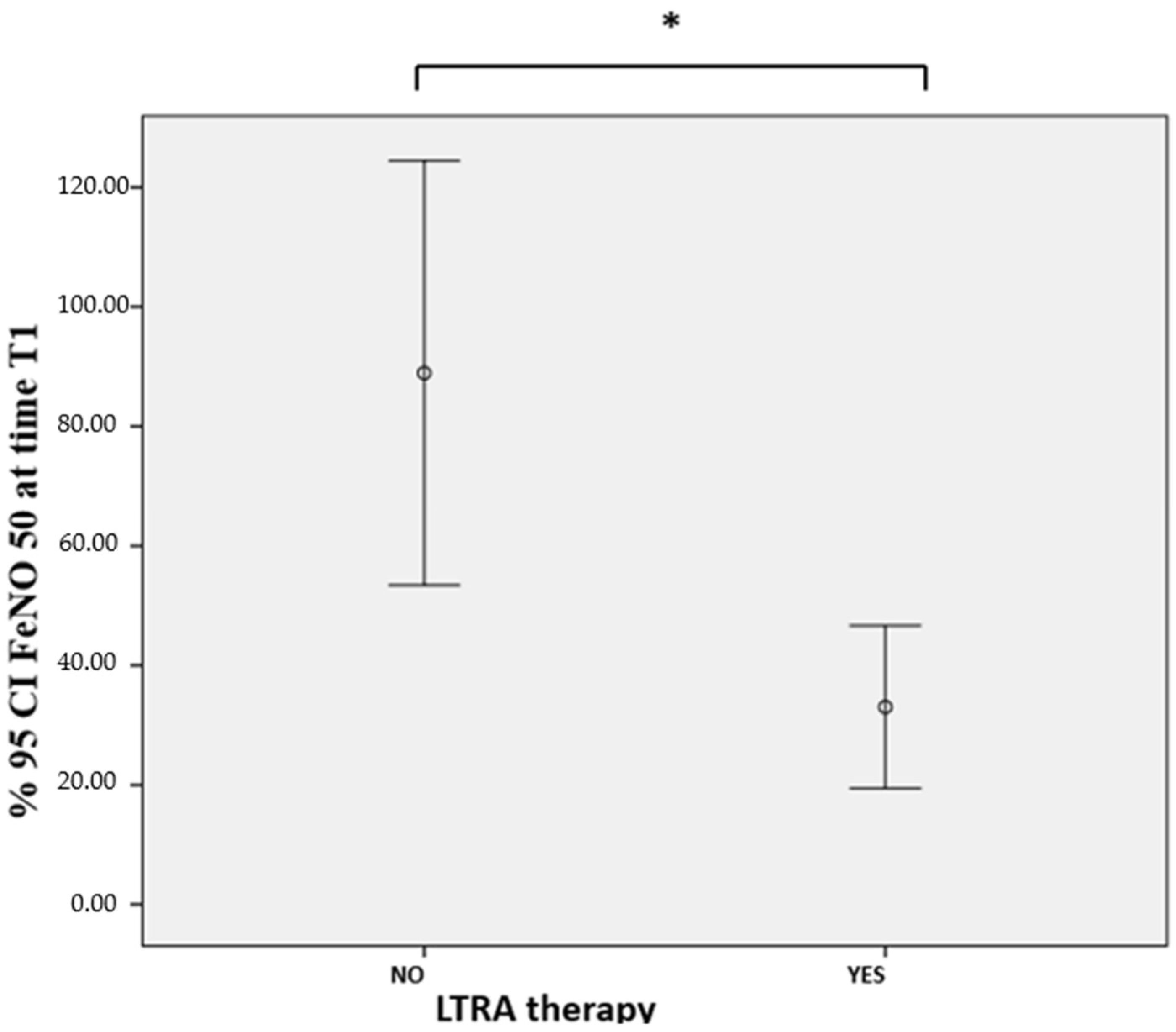
3.2.2. Comparison of Subgroups Based on LTRA Therapy (LTRA–No LTRA)
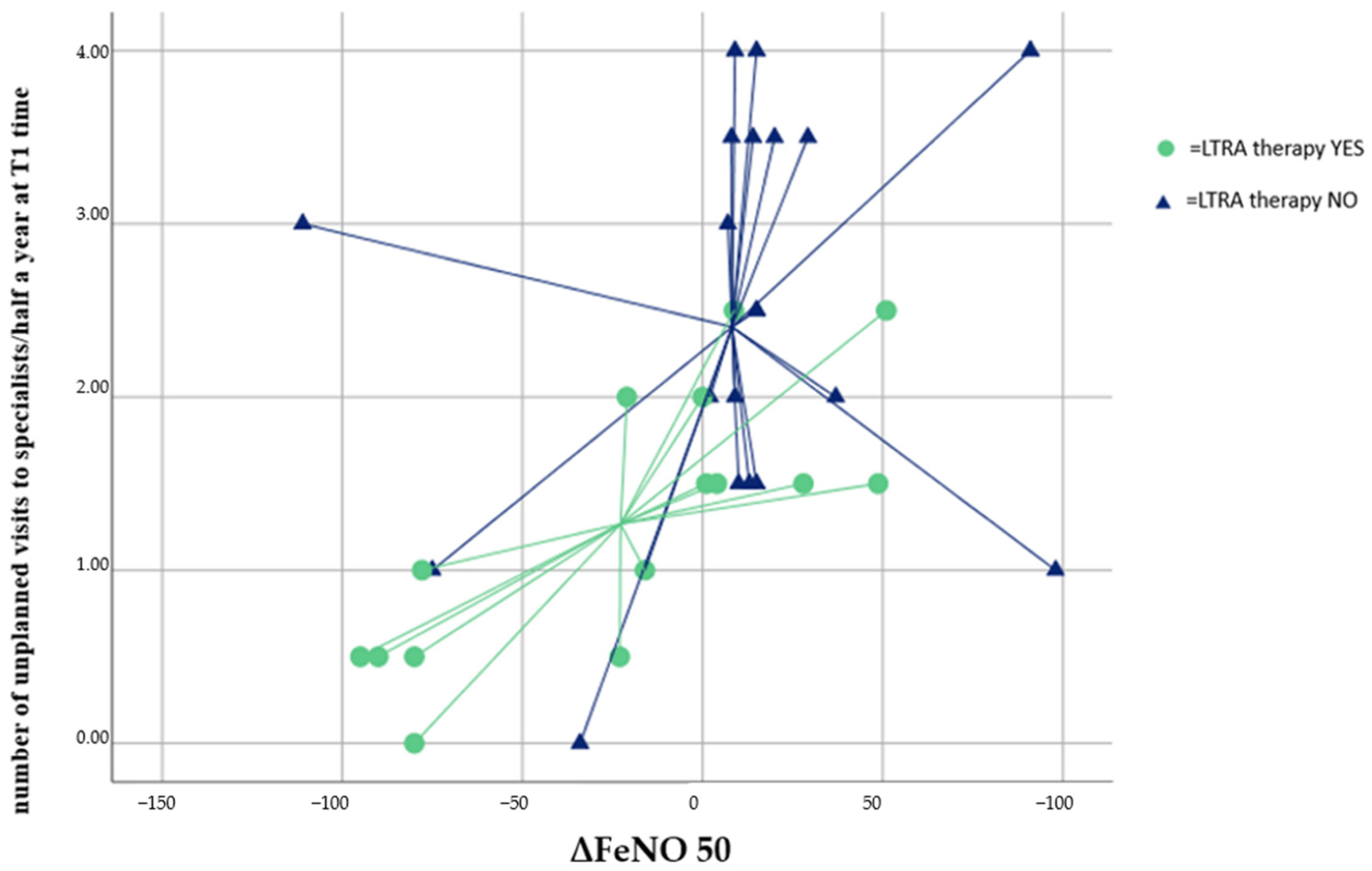
3.2.3. Comparison of Subgroups Based on the Parameter ΔFeNO (ΔFeNO < 0 Group and ΔFeNO 50 ≥ 0 Group)
3.3. Prediction Analysis on LTRA Therapy Efficacy and FeNO Reduction
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| cysLT/cysLTR1 | cysteinyl leukotriene/cysteinyl leukotriene receptor 1 |
| LTRA | leukotriene receptor antagonist |
| non-CF | non-cystic fibrosis |
| non-ABPA | non-allergic bronchopulmonary aspergillosis |
| ACT | asthma control test |
| ACQ | asthma control questionnaire |
| IgE | immunoglobulin E |
| FeNO 50 | fractional exhaled nitric oxide 50 |
| ΔFeNO | FeNO 50 T1 − FeNO 50 T0 |
| TH2 | T helper type 2 |
| ppb | parts per billion |
| iNOS | inducible nitric oxide synthase |
| NO | nitric oxide |
| SA-centers | severe asthma centers |
| CT | computed tomography |
| GINA | Global Initiative for Asthma |
| T0 | baseline |
| T1 | after 6 months of biological therapy |
| SPT | skin prick test |
| F/V | flow/volume |
| FVC | forced vital capacity |
| FEV1 | forced expiratory volume during the first second of the forced breath |
| RV | residual volume |
| ACT | Asthma Control Test |
| ACQ | Asthma Control Questionnaire |
| BSI | bronchiectasis severity index |
| FACED | FEV1, age, chronic pseudomonas aeruginosa bronchial infection colonization, radiological extension and dyspnea |
| WBC | white blood cell |
| EOS | eosinophilia |
| OCS | oral corticosteroid |
| CVA | cross-validated accuracy |
| BMI | body mass index |
| GERD | gastro-esophageal reflux disease |
| ASA sensibility | acetylsalicylic acid sensibility |
References
- Polverino, E.; Dimakou, K.; Hurst, J.; Martinez-Garcia, M.A.; Miravitlles, M.; Paggiaro, P.; Shteinberg, M.; Aliberti, S.; Chalmers, J.D. The overlap between bronchiectasis and chronic airway diseases: State of the art and future directions. Eur. Respir. J. 2018, 52, 1800328. [Google Scholar] [CrossRef] [PubMed]
- Bisaccioni, C.; Aun, M.V.; Cajuela, E.; Kalil, J.; Agondi, R.C.; Giavina-Bianchi, P. Comorbidities in severe asthma: Frequency of rhinitis, nasal polyposis, gastroesophageal reflux disease, vocal cord dysfunction and bronchiectasis. Clinics 2009, 64, 769–773. [Google Scholar] [CrossRef] [PubMed]
- Menzies, D.; Holmes, L.; Mccumesky, G.; Niven, R. Aspergillus sensitization is associated with airflow limitation and bronchiectasis in severe asthma. Allergy 2011, 66, 679–685. [Google Scholar] [CrossRef] [PubMed]
- Global Iniative for Asthma (GINA) 2022. Global Strategy for Asthma Management and Prevention, 2022. Update 2022. Available online: www.ginasthma.org (accessed on 13 July 2022).
- Polverino, E.; Goeminne, P.C.; McDonnell, M.J.; Aliberti, S.; Marshall, S.E.; Loebinger, M.R.; Murris, M.; Cantón, R.; Torres, A.; Dimakou, K.; et al. European Respiratory Society guidelines for the management of adult bronchiectasis. Eur. Respir. J. 2017, 50, 1700629. [Google Scholar] [CrossRef]
- Hill, A.T.; Sullivan, A.L.; Chalmers, J.D.; De Soyza, A.; Elborn, S.J.; Floto, A.R.; Grillo, L.; Gruffydd-Jones, K.; Harvey, A.; Haworth, C.S.; et al. British Thoracic Society Guideline for bronchiectasis in adults. Thorax 2019, 74, 1–69. [Google Scholar] [CrossRef]
- Chen, F.J.; Liao, H.; Huang, X.Y.; Xie, C.M. Importance of fractional exhaled nitricvoxide in diagnosis of bronchiectasis accompanied with bronchial asthma. J. Thorac. Dis. 2016, 8, 992–999. [Google Scholar] [CrossRef]
- Carpagnano, G.E.; Scioscia, G.; Lacedonia, D.; Curradi, G. Foschino Barbaro MP. Severe uncontrolled asthma with bronchiectasis: A pilot study of an emerging phenotype that responds to mepolizumab. J. Asthma Allergy 2019, 12, 83–90. [Google Scholar] [CrossRef]
- Kharitonov, S.A.; Wells, A.U.; O’Connor, B.J.; Cole, P.J.; Hansell, D.M.; Logan-Sinclair, R.B.; Barnes, P.J. Elevated levels of exhaled nitric oxide in bronchiectasis. Am. J. Respir. Crit. Care Med. 1995, 151, 1889–1893. [Google Scholar] [CrossRef]
- Theron, A.J.; Steel, H.C.; Tintinger, G.R.; Gravett, C.M.; Anderson, R.; Feldman, C. Cysteinyl leukotriene receptor-1 antagonists as modulators of innate immune cell function. Rev. J. Immunol. Res. 2014, 2014, 608930. [Google Scholar] [CrossRef]
- Chung, K.F.; Wenzel, S.E.; Brozek, J.L.; Bush, A.; Castro, M.; Sterk, P.J.; Adcock, I.M.; Bateman, E.D.; Bel, E.H.; Bleecker, E.R.; et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur. Respir. J. 2014, 43, 343–373. [Google Scholar] [CrossRef]
- Chalmers, J.D.; Goeminne, P.; Aliberti, S.; McDonnell, M.J.; Lonni, S.; Davidson, J.; Poppelwell, L.; Salih, W.; Pesci, A.; Dupont, L.J.; et al. The Bronchiectasis Severity Index. An international derivation and validation study. Am. J. Respir. Crit. Care Med. 2014, 189, 576–585. [Google Scholar] [CrossRef]
- Bousquet, J.; Heinzerling, L.; Bachert, C.; Papadopoulos, N.G.; Bousquet, P.J.; Burney, P.G.; Canonica, G.W.; Carlsen, K.H.; Cox, L.; Haahtela, T.; et al. Practical guide to skin prick tests in allergy to aeroallergens. Allergy 2012, 67, 18–24. [Google Scholar] [CrossRef]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.M.; Gustafsson, P.; et al. Standardisation of spirometry, ATS/ERS Task Force. Practice Guideline. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef]
- Dweik, R.A.; Boggs, P.B.; Erzurum, S.C.; Irvin, C.G.; Leigh, M.W.; Lundberg, J.O.; Olin, A.; Plummer, A.L.; Taylor, D.R. American Thoracic Society Committee on Interpretation of Exhaled Nitric Oxide Levels (FENO) for Clinical Applications. An official ATS clinical practice guideline: Interpretation of exhaled nitric oxide levels (FENO) for clinical applications. Practice Guideline. Am. J. Respir. Crit. Care Med. 2011, 184, 602–615. [Google Scholar] [CrossRef]
- American Thoracic Society/European Respiratory Society. ATS/ERS recommendations for standardized procedures for the online and offline measurement of exhaled lower respiratory nitric oxide and nasal nitric oxide. Am. J. Respir. Crit. Care Med. 2005, 171, 912–930. [Google Scholar] [CrossRef]
- Thomas, M.; Kay, S.; Pike, J.; Williams, A.; Rosenzweig, J.R.C.; Hillyer, E.V.; Price, D. The Asthma Control Test (ACT) as a predictor of GINA guideline-defined asthma control: Analysis of a multinational cross-sectional survey. Prim. Care Respir. J. 2009, 18, 41–49. [Google Scholar] [CrossRef]
- Juniper, E.F.; O’Byrne, P.M.; Guyatt, G.H.; Ferrie, P.J.; King, D.R. Development and validation of a questionnaire to measure asthma control. Eur. Respir. J. 1999, 14, 902–907. [Google Scholar] [CrossRef]
- Martínez-García, M.Á.; De Gracia, J.; Relat, M.V.; Girón, R.M.; Carro, L.M.; de la Rosa Carrillo, D.; Olveira, C. Multidimensional approach to BQNFQ the FACED score. Eur. Respir. J. 2014, 43, 1357–1367. [Google Scholar] [CrossRef]
- Trinh, H.K.T.; Lee, S.H.; Cao, T.B.T.; Park, H.S. Asthma pharmacotherapy: An update on leukotriene treatments. Expert Rev. Respir. Med. 2019, 13, 1169–1178. [Google Scholar] [CrossRef]
- Narang, I.; Ersu, R.; Wilson, N.M.; Bush, A. Nitric oxide in chronic airway inflammation in children: Diagnostic use and pathophysiological significance. Thorax 2002, 57, 586–589. [Google Scholar] [CrossRef]
- Cho, Y.-J.; Lim, H.-Y.; Park, J.S.; Lee, J.H.; Lee, C.-T.; Yoon, H.I. Measurement of fractional exhaled nitric oxide in stable bronchiectasis. Tuberc. Respir. Dis. 2013, 74, 7–14. [Google Scholar] [CrossRef]
- Corless, J.A.; Warburton, C.J. Leukotriene receptor antagonists for non-cystic fibrosis bronchiectasis. Cochrane Database Syst. Rev. 2000, 2, CD002174. [Google Scholar] [CrossRef]
- Pavord, I.D.; Korn, S.; Howarth, P.; Bleecker, E.R.; Buhl, R.; Keene, O.N.; Ortega, H.; Chanez, P. Mepolizumab for severe eosinophilic asthma (DREAM): A multicentre, double-blind, placebo-controlled trial. Lancet 2012, 380, 651–659. [Google Scholar] [CrossRef]
- Pouliquen, I.J.; Kornmann, O.; Barton, S.V.; Price, J.A.; Ortega, H.G. Characterization of the relationship between dose and blood eosinophil response following subcutaneous administration of mepolizumab. Int. J. Clin. Pharmacol. Ther. 2015, 53, 1015–1027. [Google Scholar] [CrossRef]
- Varricchi, G.; Bagnasco, D.; Borriello, F.; Heffler, E.; Canonica, G.W. Interleukin-5 pathway inhibition in the treatment of eosinophilic respiratory disorders: Evidence and unmet needs. Curr. Opin. Allergy Clin. Immunol. 2016, 16, 186–200. [Google Scholar] [CrossRef]
- Crimi, C.; Campisi, R.; Nolasco, S.; Cacopardo, G.; Intravaia, R.; Porto, M.; Impellizzeri, P.; Pelaia, C.; Crimi, N. Mepolizumab effectiveness in patients with severe eosinophilic asthma and co-presence of bronchiectasis: A real-world retrospective pilot study. Respir. Med. 2021, 185, 106491. [Google Scholar] [CrossRef]
- Katsaounou, P.; Buhl, R.; Brusselle, G.; Pfister, P.; Martínez, R.; Wahn, U.; Bousquet, J. Omalizumab as alternative to chronic use of oral corticosteroids in severe asthma. Respir. Med. 2019, 150, 51–62. [Google Scholar] [CrossRef]
- Kudlaty, E.; Patel, G.B.; Prickett, M.L.; Yeh, C.; Peters, A.T. Efficacy of type 2-targeted biologics in patients with asthma and bronchiectasis. Allergy Asthma. Immunol. 2021, 126, 302–304. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Clinical Feature | |
|---|---|
| Age, year m ± sd | 59.08 ± 11.09 |
| Female sex, % | 50 |
| BMI, kg/m2 m ± sd | 24.86 ± 3.53 |
| Smoker, % | |
| current | 13.9 |
| former | 27.8 |
| never | 58.3 |
| BSI score, m ± sd | 7.09 ± 3.98 |
| Bilateral bronchiectasis yes, % | 84.6 |
| Nodular pattern yes, % | 13.9 |
| Time of asthmatic disease, year m ± sd | 27.52 ± 18.11 |
| Family history of asthma yes, % | 19.4 |
| GERD yes, % | 30.6 |
| ASA sensibility yes, % | 11.1 |
| Allergic rhinitis yes, % | 33.3 |
| LTRA therapy yes, % | 41.7 |
| Biological therapy, % | |
| omalizumab | 16.7 |
| mepolizumab | 63.9 |
| bernalizumab | 19.4 |
| TO Time | T1 Time | p Value | |
|---|---|---|---|
| FeNO 50, ppb m ± sd | 73.40 ± 76.41 | 68.86 ± 69.74 | 0.595 |
| EOS, cells/μL median (IQ 25–75) | 680.00 (500.00–959.00) | 130.00 (97.50–447.50) | 0.004 |
| IGE tot, KU/L median (IQ 25–75) | 234.00 (119.00–534.50) | 400.00 (215.00–700.00) | 0.756 |
| FEV1, m ± sd % predicted | 73.37 ± 21.72 | 85.67 ± 16.07 | 0.000 |
| FVC, m ± sd % predicted | 94.66 ± 17.91 | 96.51 ± 16.13 | 0.000 |
| RV, m ± sd % predicted | 110.28 ± 28.08 | 112.00 ± 23.99 | 0.113 |
| ACT, score m ± sd | 14.41 ± 5.03 | 20.70 ± 4.31 | 0.219 |
| ACQ, score m ± sd | 1.95 ± 0.96 | 0.93 ± 0.69 | 0.431 |
| Need of inhaled reliever medication, % | 63.8 | 21.2 | 0.007 |
| OCS, yes % | 66.6 | 45.7 | 0.353 |
| Average dose of OCS, mg m ± sd | 13.59 ± 12.37 | 4.05 ± 7.04 | 0.550 |
| FACED, score m ± sd | 2.18 ± 1.16 | 1.42 ± 1.27 | 0.172 |
| % Positive sputum | 16.7 | 5.5 | 0.125 |
| Mucolytic therapy, yes % | 35 | 35 | 1.000 |
| Adherence to therapy % | 89 | 95 | 0.200 |
| WBCs, cells/μL median (IQ 25–75) | 7000.00 (6500.00–9725.00) | 7100.00 (6590.00–10,420.00) | 0.998 |
| T1 TIME | |||
|---|---|---|---|
| LTRA Yes (n = 15) | LTRA No (n = 24) | p Value | |
| FeNO 50, ppb m ± sd | 30.83 ± 24.30 | 88.93 ± 77.96 | 0.009 |
| EOS, cells/μL median (IQ 25–75) | 150.00 (125.00 380.00) | 100.00 (65.00–265.00) | 0.201 |
| IgE, KU/L median (IQ 25–75) | 555.00 (400.00–700.00) | 215.00 (132.00–324.00) | 0.067 |
| FEV1, m ± sd % predicted | 80.34 ± 19.20 | 87.58 ± 18.59 | 0.305 |
| FVC, m ± sd % predicted | 94.97 ± 23.91 | 98.64 ± 27.07 | 0.707 |
| ACT, score m ± sd | 20.13 ± 4.06 | 22.00 ± 4.26 | 0.193 |
| ACQ, score m ± sd | 1.12 ± 0.88 | 0.94 ± 0.81 | 0.663 |
| Need of inhaled reliever medication, % | 20.0 | 20.0 | 0.709 |
| OCS yes, % | 40.0 | 47.6 | 0.456 |
| Average dose of OCS, mg m ± sd | 3.55 ± 4.99 | 4.19 ± 8.30 | 0.503 |
| Adherence to therapy, % | 90.0 | 100.0 | 0.500 |
| WBCs, cells/μL median (IQ 25–75) | 8950.00 (7000.00–10,900.00 | 7100.00(6590–9275) | 0.555 |
| OCS course, n m ± sd | 0.53 ± 1.34 | 0.69 ± 1.79 | |
| Bronchial exacerbation/6 months n m ± sd | 0.41 ± 0,77 | 0.53 ± 0.80 | 0.639 |
| antibiotic courses/6 months n m ± sd | 0.20 ± 0.41 | 0.28 ± 0.51 | 0.584 |
| Number of hospitalizations/6 months n m ± sd | 0.10 ± 0.20 | 0.50 ± 0.70 | 0.052 |
| Unplanned visits to specialists/6 months n m ± sd | 1.26 ± 0.07 | 2.40 ± 1.17 | 0.003 |
| Parameters | T0 Time | T1 Time | ||||
|---|---|---|---|---|---|---|
| Group1 | Group 0 | p | Group 1 | Group 0 | p | |
| * FeNO 50, ppb m ± sd | 125.32 ± 99.57 | 45.28 ± 36.55 | 0.019 | 71.36 ± 96.08 | 64.37 ± 52.07 | 0.781 |
| * EOS, cells/μL median (IQ 25–75) | 700.00 (555.00–1084.00) | 620.00(500.00–898.00) | 0.379 | 130.00 (110.00–150.00) | 400.00 (90.00–700.00) | 0.548 |
| IgE, KU/L median (IQ 25–75) | 300.00 (118.00–899.00) | 213.00 (147.50–384.50) | 0.450 | 500.00 (400.00–650.00) | 260.00–(173.50–631.50) | 0.344 |
| * # FEV1, m ± sd % predicted | 68.00 ± 10.81 | 74.15 ± 26.01 | 0.504 | 83.83 ± 13.08 | 84.36 ± 21.21 | 0.934 |
| FVC, m ± sd % predicted | 81.50 ± 16.26 | 92.20 ± 24.79 | 0.550 | 83.20 ± 16.68 | 103.10± 25.34 | 0.295 |
| RV, m ± sd % predicted | 118.75 ± 35.18 | 112.82 ± 30.89 | 0.789 | 94.66 ± 9.07 | 119.42 ± 24.93 | 0.051 |
| * # ACT, score m ± sd | 14.54 ± 5.55 | 14.34 ± 4.89 | 0.921 | 22.41 ± 3.23 | 20.62 ± 4.59 | 0.236 |
| * ACQ, score m ± sd | 1.87 ± 0.93 | 2.14 ± 1.21 | 0.753 | 0.72 ± 0.48 | 1.31 ± 0.99 | 0.137 |
| Positive sputum, % | 33.8 | 8.3 | 0.080 | 8.3 | 4.2 | 0.562 |
| * Need of inhaled reliever medication, % | 66.7 | 60.7 | 0.570 | 5 | 30 | 0.172 |
| LTRA Therapy, yes % | 66.7 | 29.2 | 0.037 | 66.7 | 29.2 | 0.037 |
| OCS, yes % | 63.6 | 70.8 | 0.479 | 27.3 | 54.2 | |
| * Avarage dose of OCS | 9.22 ± 9.31 | 15.56 ± 13.26 | 0.154 | 1.15 ± 3.37 | 5.12 ± 7.99 | 0.183 |
| OCS course, n m ± sd | 6.14 ± 3.07 | 6.22 ± 3.03 | 0.960 | 0.50 ± 1.73 | 0.69 ± 1.57 | 0.746 |
| Bronchial of exacerbation/n m ± sd | 4.54 ± 2.16 | 6.12 ± 4.11 | 0.241 | 0.34 ± 0.61 | 0.55 ± 0.86 | 0.416 |
| Mucolytic therapy, yes % | 50 | 20 | 0.175 | 50 | 20 | 0.175 |
| Adherence therapy % | 81.8 | 91.7 | 0.372 | 100 | 90 | 0.500 |
| WBCs, cells/μL median (IQ 25–75) | 7000 (6500–8500) | 10,400 (7700.00–11,100.00) | 0.069 | 7000.00 (6785.00–7050.00) | 9250.00 (7160.00–10,660.00) | 0.256 |
| * Antibiotic courses, n m ± sd | 2.00 ± 1.33 | 4.14 ± 1.34 | 0.005 | 0.12 ± 0.22 | 0.31 ± 0.55 | 0.266 |
| Hospitalizations n m ± sd | 0.88 ± 0.78 | 1.00 ± 1.05 | 0.796 | 0.10 ± 0.31 | 0.40 ± 0.69 | 0.232 |
| Unplanned visits to specialists n m ± sd | 4.66 ± 2.00 | 4.60 ± 2.06 | 0.944 | 0.92 ± 0.85 | 2.44 ± 0.96 | 0.000 |
| ODD | CI | p | |
|---|---|---|---|
| Biological therapy | 1.26 | 0.39–4.03 | 0.695 |
| LTRA therapy | 4.85 | 1.09–21.51 | 0.037 |
| Unplanned visits to specialists at T1 time | 0.10 | 0.02–0.50 | 0.005 |
| ΔACT | 1.01 | 0.91–1.01 | 0.762 |
| Age | 1.01 | 0.94–1.06 | 0.948 |
| Sex | 1.65 | 0.40–6.71 | 0.481 |
| Univariate Regression Analysis | Multivariate Regression Analysis | |||||
|---|---|---|---|---|---|---|
| ODD | IC 95% | p Value | ODD | IC 95% | p Value | |
| Age, y | 1.008 | 0.949–1.072 | 0.787 | 1.049 | 0.947–1.163 | 0.360 |
| Sex, female sex | 1.257 | 0.333–4.742 | 0.735 | 0.484 | 0.034–4.994 | 0.484 |
| BMI, kg/m2 | 1.176 | 0.957–1.445 | 0.123 | 0.136 | 0.909–2.008 | 1.351 |
| FeNO 50 T1, ppb | 0.97 | 0.93–0.99 | 0.024 | 0.955 | 0.919–0.993 | 0.021 |
| Unplanned visits to specialists T1/6 months | 0.331 | 0.144–0.761 | 0.009 | 0.179 | 0.048–0.673 | 0.011 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quaranta, V.N.; Dragonieri, S.; Crimi, N.; Crimi, C.; Santus, P.; Menzella, F.; Pelaia, C.; Scioscia, G.; Caruso, C.; Bargagli, E.; et al. Can Leukotriene Receptor Antagonist Therapy Improve the Control of Patients with Severe Asthma on Biological Therapy and Coexisting Bronchiectasis? A Pilot Study. J. Clin. Med. 2022, 11, 4702. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11164702
Quaranta VN, Dragonieri S, Crimi N, Crimi C, Santus P, Menzella F, Pelaia C, Scioscia G, Caruso C, Bargagli E, et al. Can Leukotriene Receptor Antagonist Therapy Improve the Control of Patients with Severe Asthma on Biological Therapy and Coexisting Bronchiectasis? A Pilot Study. Journal of Clinical Medicine. 2022; 11(16):4702. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11164702
Chicago/Turabian StyleQuaranta, Vitaliano Nicola, Silvano Dragonieri, Nunzio Crimi, Claudia Crimi, Pierachille Santus, Francesco Menzella, Corrado Pelaia, Giulia Scioscia, Cristiano Caruso, Elena Bargagli, and et al. 2022. "Can Leukotriene Receptor Antagonist Therapy Improve the Control of Patients with Severe Asthma on Biological Therapy and Coexisting Bronchiectasis? A Pilot Study" Journal of Clinical Medicine 11, no. 16: 4702. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11164702