
COVID-19 Related Myocarditis in Adults: A Systematic Review of Case Reports

 ,
,  , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
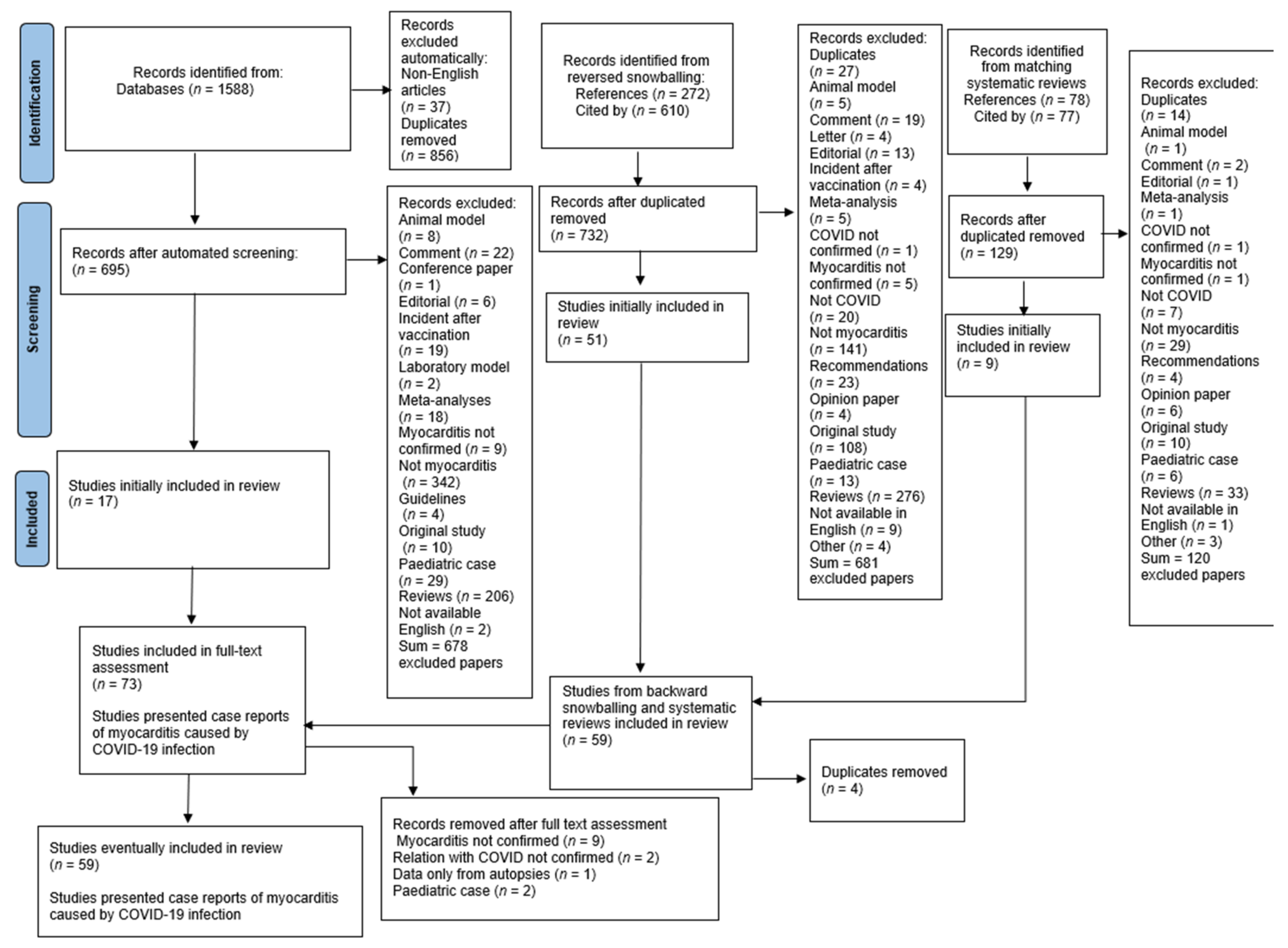
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction and Studies Quality Assessment
3. Results
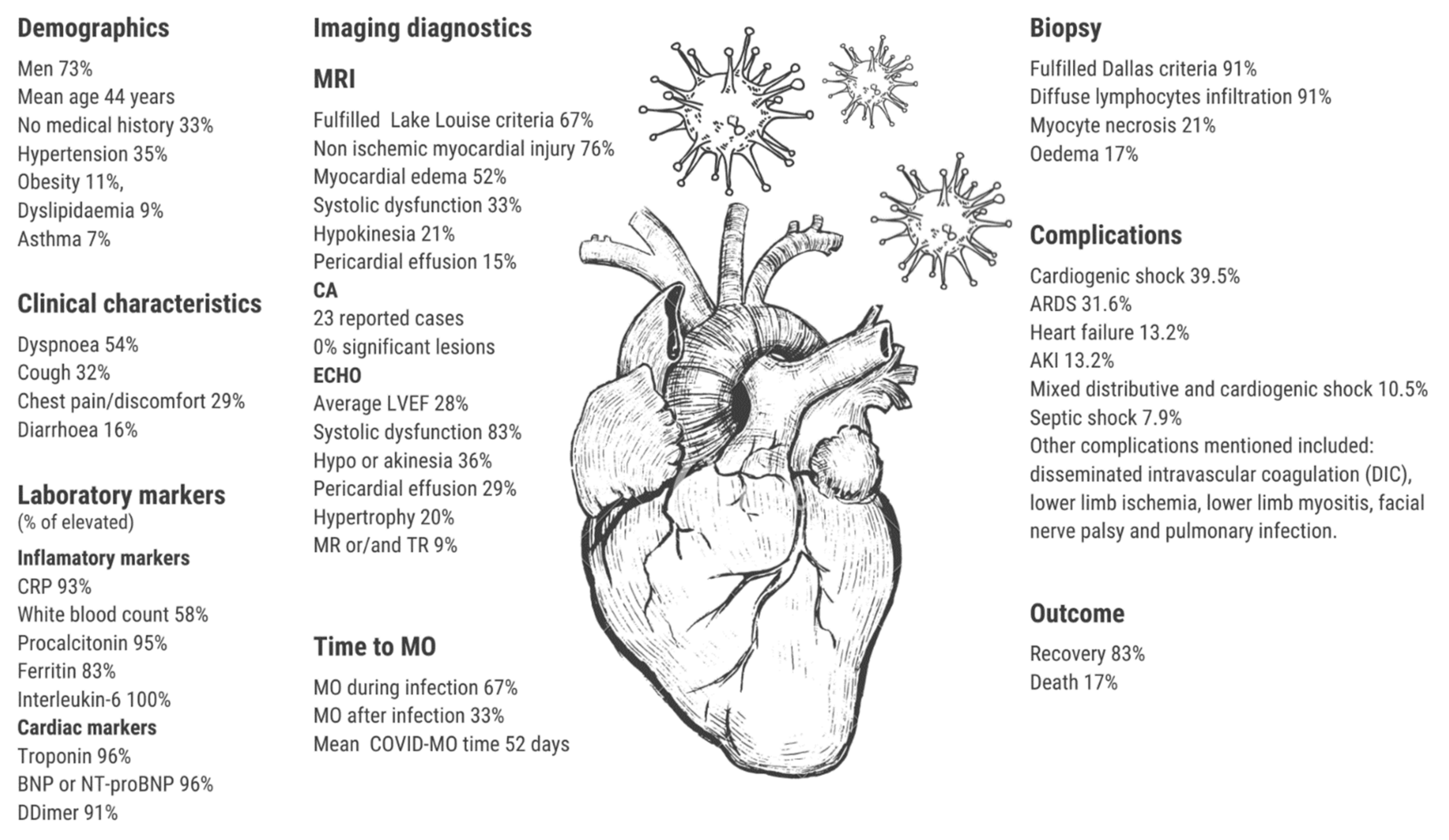
3.1. Demographics
3.2. Clinical Characteristics
3.3. Time of COVID-Related Myocarditis
3.4. Laboratory Markers
3.5. ECG
3.6. Imaging Diagnostics
3.6.1. X-ray
3.6.2. CA
3.6.3. CT
3.6.4. MRI
3.6.5. ECHO
3.7. Biopsy
3.8. ESC Criteria
3.9. Treatment
3.9.1. Pharmacotherapy
3.9.2. Procedures
3.10. Complications
3.11. Outcome
4. Discussion
4.1. Clinical Characteristics of Patients
4.2. Clinical Presentation
4.3. Imaging Diagnostics
4.4. Treatment
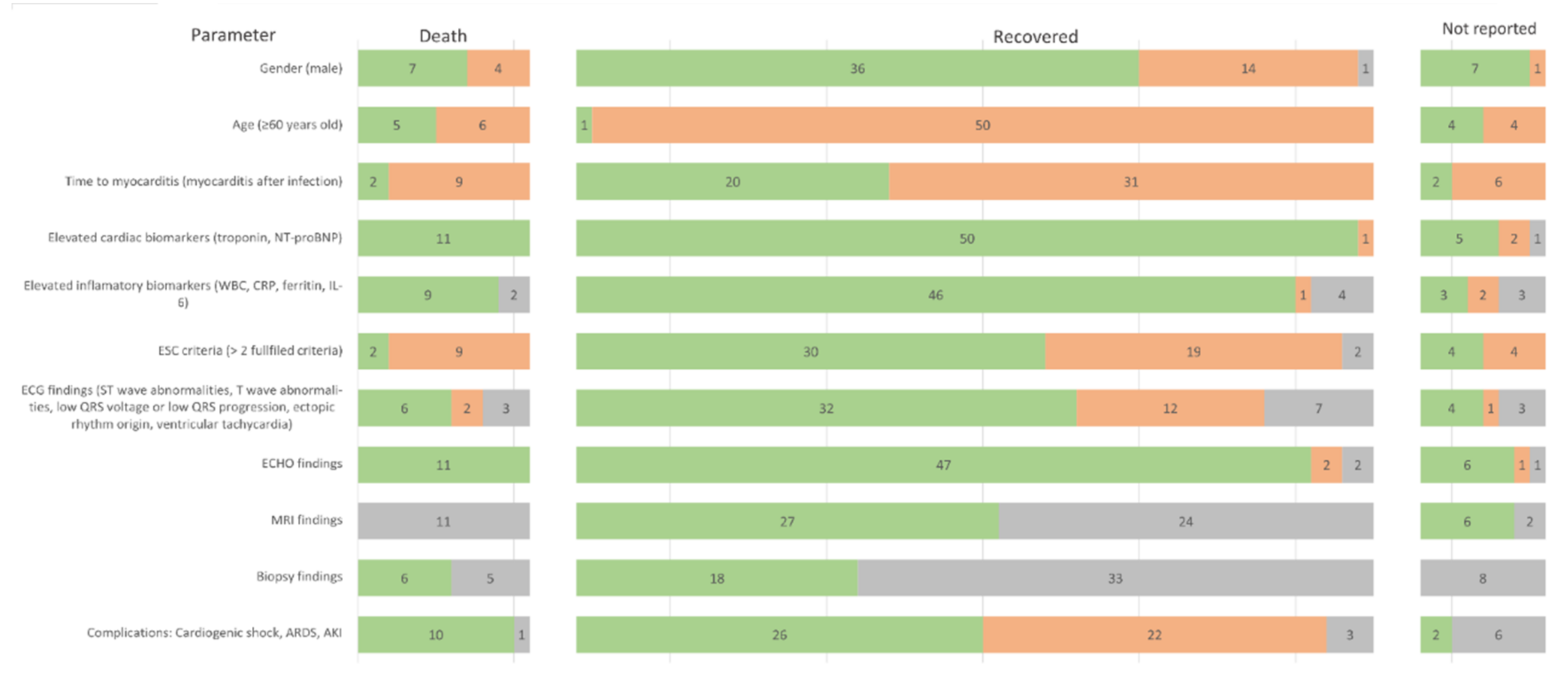
4.5. Prognosis and Outcome
4.6. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coronavirus Death Toll and Trends—Worldometer, (n.d.). Available online: https://www.worldometers.info/coronavirus/coronavirus-death-toll/ (accessed on 9 August 2022).
- Ahmad, I.; Rathore, F.A. Neurological manifestations and complications of COVID-19: A literature review. J. Clin. Neurosci. 2020, 77, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Sarfraz, Z.; Sarfraz, A.; Barrios, A.; Garimella, R.; Dominari, A.; KC, M.; Pandav, K.; Pantoja, J.C.; Retnakumar, V.; Cherrez-Ojeda, I. Cardio-Pulmonary Sequelae in Recovered COVID-19 Patients: Considerations for Primary Care. J. Prim. Care Community Health 2021, 12, 21501327211023726. [Google Scholar] [CrossRef] [PubMed]
- Sokolski, M.; Gajewski, P.; Zymliński, R.; Biegus, J.; Berg, J.M.T.; Bor, W.; Braunschweig, F.; Caldeira, D.; Cuculi, F.; D’Elia, E.; et al. Impact of Coronavirus Disease 2019 (COVID-19) Outbreak on Acute Admissions at the Emergency and Cardiology Departments Across Europe. Am. J. Med. 2021, 134, 482–489. [Google Scholar] [CrossRef] [PubMed]
- Bielecka-Dabrowa, A.; Cichocka-Radwan, A.; Lewek, J.; Pawliczak, F.; Maciejewski, M.; Banach, M. Cardiac manifestations of COVID-19. Rev. Cardiovasc. Med. 2021, 22, 365–371. [Google Scholar] [CrossRef]
- Caforio, A.L.P.; Pankuweit, S.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; Fu, M.; Heliö, T.; Heymans, S.; Jahns, R.; et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases, (n.d.). Eur. Heart J. 2013, 34, 2636–2648. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Castiello, T.; Georgiopoulos, G.; Finocchiaro, G.; Claudia, M.; Gianatti, A.; Delialis, D.; Aimo, A.; Prasad, S. COVID-19 and myocarditis: A systematic review and overview of current challenges. Heart Fail. Rev. 2022, 27, 251–261. [Google Scholar] [CrossRef]
- Ho, J.S.; Sia, C.H.; Chan, M.Y.; Lin, W.; Wong, R.C. Coronavirus-induced myocarditis: A meta-summary of cases. Heart Lung 2020, 49, 681–685. [Google Scholar] [CrossRef]
- Doyen, D.; Moceri, P.; Ducreux, D.; Dellamonica, J. Myocarditis in a patient with COVID-19: A cause of raised troponin and ECG changes. Lancet 2020, 395, 1516. [Google Scholar] [CrossRef]
- Luetkens, J.A.; Isaak, A.; Zimmer, S.; Nattermann, J.; Sprinkart, A.M.; Boesecke, C.; Rieke, G.J.; Zachoval, C.; Heine, A.; Velten, M.; et al. Diffuse Myocardial Inflammation in COVID-19 Associated Myocarditis Detected by Multiparametric Cardiac Magnetic Resonance Imaging. Circ. Cardiovasc. Imaging 2020, 13, 10897. [Google Scholar] [CrossRef]
- Kim, I.C.; Kim, J.Y.; Kim, H.A.; Han, S. COVID-19-related myocarditis in a 21-year-old female patient. Eur. Heart J. 2020, 41, 1859. [Google Scholar] [CrossRef]
- Sala, S.; Peretto, G.; Gramegna, M.; Palmisano, A.; Villatore, A.; Vignale, D.; de Cobelli, F.; Tresoldi, M.; Cappelletti, A.M.; Basso, C.; et al. Acute myocarditis presenting as a reverse Tako-Tsubo syndrome in a patient with SARS-CoV-2 respiratory infection. Eur. Heart J. 2020, 41, 1861–1862. [Google Scholar] [CrossRef]
- Bonnet, M.; Champagnac, A.; Lantelme, P.; Harbaoui, B. Endomyocardial biopsy findings in Kawasaki-like disease associated with SARS-CoV-2. Eur. Heart J. 2020, 41, 3863–3864. [Google Scholar] [CrossRef]
- Ishikura, H.; Maruyama, J.; Hoshino, K.; Matsuoka, Y.; Yano, M.; Arimura, T.; Katano, H.; Kato, S.; Kitamura, T.; Nakamura, Y. Coronavirus disease (COVID-19) associated delayed-onset fulminant myocarditis in patient with a history of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. J. Infect. Chemother. 2021, 27, 1760–1764. [Google Scholar] [CrossRef]
- Meyer, M.; Vogel, T.; Meyer, A.; Constancias, F.; Porter, L.F.; Kaltenbach, G.; Schmitt, E.; Chayer, S.; Zeyons, F.; Riou, M.; et al. Presence of active myocarditis at the 6 month follow-up appointment for a severe form of COVID-19: A case report. ESC Heart Fail. 2021, 8, 4307–4312. [Google Scholar] [CrossRef]
- Roest, S.; Brugts, J.J.; van Kampen, J.J.A.; von der Thüsen, J.H.; Constantinescu, A.A.; Caliskan, K.; Hirsch, A.; Manintveld, O.C. COVID-19-related myocarditis post-heart transplantation. Int. J. Infect. Dis. 2021, 107, 34–36. [Google Scholar] [CrossRef]
- Inciardi, R.M.; Lupi, L.; Zaccone, G.; Italia, L.; Raffo, M.; Tomasoni, D.; Cani, D.S.; Cerini, M.; Farina, D.; Gavazzi, E.; et al. Cardiac Involvement in a Patient with Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 819–824. [Google Scholar] [CrossRef]
- Hu, H.; Ma, F.; Wei, X.; Fang, Y. Coronavirus fulminant myocarditis treated with glucocorticoid and human immunoglobulin. Eur. Heart J. 2021, 42, 206. [Google Scholar] [CrossRef]
- Zeng, J.H.; Liu, Y.X.; Yuan, J.; Wang, F.X.; Wu, W.B.; Li, J.X.; Wang, L.F.; Gao, H.; Wang, Y.; Dong, C.F.; et al. First case of COVID-19 complicated with fulminant myocarditis: A case report and insights. Infection 2020, 48, 773–777. [Google Scholar] [CrossRef]
- Aldeghaither, S.; Qutob, R.; Assanangkornchai, N.; Issa-Chergui, B.; Tam, M.; Larotondo, R.; Samoukovic, G. Clinical and Histopathologic Features of Myocarditis in Multisystem Inflammatory Syndrome (Adult)-Associated COVID-19. Crit. Care Explor. 2022, 10, e0630. [Google Scholar] [CrossRef]
- Amin, A.; Eftekhar, S.P.; Ziaie, N.; Roudbari, S.; Salehi, P.; Jalali, F.; Jafaripour, I.; Ghaffari, S.; Salehi, M.M.; Ebadi, R. Clinically suspected myocarditis in COVID-19 patients: Case series and review of the literature. Clin. Case Rep. 2021, 9, e05236. [Google Scholar] [CrossRef]
- Menter, T.; Cueni, N.; Gebhard, E.C.; Tzankov, A. Case Report: Co-occurrence of Myocarditis and Thrombotic Microangiopathy Limited to the Heart in a COVID-19 Patient. Front. Cardiovasc. Med. 2021, 8, 695010. [Google Scholar] [CrossRef]
- Ashok, V.; Loke, W.I.; Dinov, B.; Robert, S.; David, N.; Camm, C.F.; Ross, T. Case report: High-grade atrioventricular block in suspected COVID-19 myocarditis. Eur. Heart J. Case Rep. 2020, 4, 1–6. [Google Scholar] [CrossRef]
- Li, A.; Garcia-Bengochea, Y.; Stechel, R.; Azari, B.M.; Aboumarie, H.S.; Miglioranza, M.H.; Cameli, M.; Camm, C.F.; Thomson, R. Management of COVID-19 myopericarditis with reversal of cardiac dysfunction after blunting of cytokine storm: A case report. Eur. Heart J. Case Rep. 2020, 4, 1–6. [Google Scholar] [CrossRef]
- Nakatani, S.; Ohta-Ogo, K.; Nishio, M.; Amemiya, K.; Sato, S.; Sawano, H.; Hatakeyama, K.; Katano, H.; Suzuki, T.; Hirooka, K. Microthrombosis as a cause of fulminant myocarditis-like presentation with COVID-19 proven by endomyocardial biopsy. Cardiovasc. Pathol. 2022, 60, 107435. [Google Scholar] [CrossRef]
- Ismayl, M.; Abusnina, W.; Thandra, A.; Sabri, A.; Groh, D.; Kanmanthareddy, A.; Alla, V.M. Delayed acute myocarditis with COVID-19 infection. Proc. Bayl. Univ. Med. Cent. 2022, 35, 366–368. [Google Scholar] [CrossRef]
- Thomson, A.; Totaro, R.; Cooper, W.; Dennis, M. Fulminant Delta COVID-19 myocarditis: A case report of fatal primary cardiac dysfunction. Eur. Heart J. Case Rep. 2022, 6, ytac142. [Google Scholar] [CrossRef]
- Campoamor, D.; Seixas, R.; Gama, L.; Duarte, J.; Araújo, T. Arrhythmogenic Cardiomyopathy as a Late Complication of COVID-19-Induced Myocarditis. Cureus 2022, 14, e21941. [Google Scholar] [CrossRef]
- Flagiello, M.; Al Harthy, A.; Boccalini, S.; Jacquemet, L.; Obadia, J.F.; Baudry, G.; Pozzi, M. Veno-arterial extracorporeal membrane oxygenation for COVID-19-associated acute myocardial injury complicated by refractory cardiogenic shock. J. Card. Surg. 2021, 36, 4396. [Google Scholar] [CrossRef]
- Pascariello, G.; Cimino, G.; Calvi, E.; Bernardi, N.; Grigolato, M.; Garyfallidis, P.; Fabbricatore, D.; Pezzola, E.; Lombardi, C.M.; Metra, M.; et al. Cardiogenic Shock due to COVID-19-Related Myocarditis in a 19-Year-Old Autistic Patient. J. Med. Cases 2020, 11, 207–210. [Google Scholar] [CrossRef] [PubMed]
- Gaudriot, B.; Mansour, A.; Thibault, V.; Lederlin, M.; Cauchois, A.; Lelong, B.; Ross, J.T.; Leurent, G.; Tadié, J.M.; Revest, M.; et al. Successful heart transplantation for COVID-19-associated post-infectious fulminant myocarditis. ESC Heart Fail. 2021, 8, 2625–2630. [Google Scholar] [CrossRef] [PubMed]
- Shah, J.Z.; Kumar, S.A.; Patel, A.A. Myocarditis and Pericarditis in Patients with COVID-19. Heart Views 2020, 21, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Shabbir, A.; Camm, C.F.; Elkington, A.; Tilling, L.; Stirrup, J.; Chan, A.; Bull, S. Myopericarditis and myositis in a patient with COVID-19: A case report. Eur. Heart J. Case Rep. 2020, 4, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Gauchotte, G.; Venard, V.; Segondy, M.; Cadoz, C.; Esposito-Fava, A.; Barraud, D.; Louis, G. SARS-CoV-2 fulminant myocarditis: An autopsy and histopathological case study. Int. J. Legal Med. 2021, 135, 577–581. [Google Scholar] [CrossRef]
- Bernal-Torres, W.; Herrera-Escandón, Á.; Hurtado-Rivera, M.; Plata-Mosquera, C.A.; Savarese, G.; David, S.; Ferrannini, G.; Camm, C.F. COVID-19 fulminant myocarditis: A case report. Eur. Heart J. Case Rep. 2020, 4, 1–6. [Google Scholar] [CrossRef]
- Oleszak, F.; Maryniak, A.; Botti, E.; Abrahim, C.; Salifu, M.O.; Youssef, M.; Henglein, V.L.; McFarlane, S.I. Myocarditis Associated with COVID-19. Am. J. Med. Case Rep. 2020, 8, 498. [Google Scholar] [CrossRef]
- Gay, H.C.; Sinha, A.; Michel, E.; Mozer, A.B.; Budd, A.; Feinstein, M.J.; Benzuly, K.H.; Al-Qamari, A.; Pawale, A.A.; Vorovich, E.E. Fulminant myocarditis in a patient with coronavirus disease 2019 and rapid myocardial recovery following treatment. ESC Heart Fail. 2020, 7, 4367–4370. [Google Scholar] [CrossRef]
- Gomila-Grange, A.; Espasa, M.; Moglia, E. Cardiogenic Shock Caused by SARS-CoV-2 in a Patient with Serial Negative Nucleic Acid Amplification Tests. Case Report. SN Compr. Clin. Med. 2020, 2, 1903–1905. [Google Scholar] [CrossRef]
- Richard, I.; Robinson, B.; Dawson, A.; Aya, A.; Ali, R. An Atypical Presentation of Fulminant Myocarditis Secondary to COVID-19 Infection. Cureus 2020, 12, e9179. [Google Scholar] [CrossRef]
- Wenzel, P.; Kopp, S.; Gobel, S.; Jansen, T.; Geyer, M.; Hahn, F.; Kreitner, K.F.; Escher, F.; Schultheiss, H.P.; Münzel, T. Evidence of SARS-CoV-2 mRNA in endomyocardial biopsies of patients with clinically suspected myocarditis tested negative for COVID-19 in nasopharyngeal swab. Cardiovasc. Res. 2020, 116, 1661–1663. [Google Scholar] [CrossRef]
- Bemtgen, X.; Klingel, K.; Hufnagel, M.; Janda, A.; Bode, C.; Staudacher, D.L.; Supady, A.; Jandova, I. Case Report: Lymphohistiocytic Myocarditis with Severe Cardiogenic Shock Requiring Mechanical Cardiocirculatory Support in Multisystem Inflammatory Syndrome Following SARS-CoV-2 Infection. Front. Cardiovasc. Med. 2021, 9, 1091. [Google Scholar] [CrossRef]
- Beşler, M.S.; Arslan, H. Acute myocarditis associated with COVID-19 infection. Am. J. Emerg. Med. 2020, 38, 2489.e1. [Google Scholar] [CrossRef]
- Meel, R.; Ramsamy, T.D.; Narsing, R.; Wong, M. Focal myocarditis in a young male with SARS-CoV-2 infection. Oxf. Med. Case Rep. 2021, 2021, 72–75. [Google Scholar] [CrossRef]
- Paul, J.F.; Charles, P.; Richaud, C.; Caussin, C.; Diakov, C. Myocarditis revealing COVID-19 infection in a young patient. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 776. [Google Scholar] [CrossRef]
- Coyle, J.; Igbinomwanhia, E.; Sanchez-Nadales, A.; Danciu, S.; Chu, C.; Shah, N. A Recovered Case of COVID-19 Myocarditis and ARDS Treated with Corticosteroids, Tocilizumab, and Experimental AT-001. JACC Case Rep. 2020, 2, 1331–1336. [Google Scholar] [CrossRef]
- Irabien-Ortiz, Á.; Carreras-Mora, J.; Sionis, A.; Pàmies, J.; Montiel, J.; Tauron, M. Fulminant myocarditis due to COVID-19. Rev. Española De Cardiol. 2020, 73, 503–504. [Google Scholar] [CrossRef]
- Frustaci, A.; Francone, M.; Verardo, R.; Capobianchi, M.R.; Chimenti, C. Virus-Negative Necrotizing Coronary Vasculitis with Aneurysm Formation in Human SARS-CoV-2 Infection. Infect. Dis. Rep. 2021, 13, 597–601. [Google Scholar] [CrossRef]
- Sardari, A.; Tabarsi, P.; Borhany, H.; Mohiaddin, R.; Houshmand, G. Myocarditis detected after COVID-19 recovery. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 131–132. [Google Scholar] [CrossRef]
- Warchoł, I.; Dȩbska-Kozłowska, A.; Karcz-Socha, I.; Książczyk, M.; Szymańska, K.; Lubiński, A. Terra incognita: Clinically suspected myocarditis in a patient with severe acute respiratory syndrome coronavirus 2 infection. Pol. Arch. Intern. Med. 2020, 130, 446–448. [Google Scholar] [CrossRef]
- Shahrami, B.; Davoudi-Monfared, E.; Rezaie, Z.; Gheibi, S.; Vakili-Ardabili, A.; Arabzadeh, A.A.; Talebi, A.; Mojtahedzadeh, M. Management of a critically ill patient with COVID-19-related fulminant myocarditis: A case report. Respir. Med. Case Rep. 2022, 36, 101611. [Google Scholar] [CrossRef]
- Gaine, S.; Devitt, P.; Coughlan, J.J.; Pearson, I. COVID-19-associated myocarditis presenting as new-onset heart failure and atrial fibrillation. BMJ Case Rep. CP 2021, 14, e244027. [Google Scholar] [CrossRef]
- Taouihar, S.; Bouabdallaoui, A.; Aabdi, M.; Elaidouni, G.; Bkiyar, H.; Aichouni, N.; Smaili, N.; ElOuafi, N.; Skiker, I.; Housni, B. ST elevation revealing acute myocarditis with SARS-CoV-2 infection: Case report. Ann. Med. Surg. 2021, 65, 102313. [Google Scholar] [CrossRef]
- Dahl, E.H.; Mosevoll, K.A.; Cramariuc, D.; Vedeler, C.A.; Blomberg, B. COVID-19 myocarditis and postinfection Bell’s palsy. BMJ Case Rep. CP 2021, 14, e240095. [Google Scholar] [CrossRef]
- Matsumura, K.; Kawano, H.; Kurobe, M.; Akashi, R.; Yoshimuta, T.; Ikeda, S.; Ueki, N.; Nakashima, M.; Maemura, K. Delayed Acute Perimyocarditis and Bilateral Facial Nerve Palsy in a Patient with COVID-19. Intern. Med. 2022, 61, 2327–2332. [Google Scholar] [CrossRef]
- Van Praet, J.T.; Hoste, L.; Haerynck, F. Acute Perimyocarditis in a Case of Multisystem Inflammatory Syndrome in Adults. J. Rheumatol. 2022, 49, 538–539. [Google Scholar] [CrossRef]
- Masiak, A.; Lass, A.; Kowalski, J.; Hajduk, A.; Zdrojewski, Z. Self-limiting COVID-19-associated Kikuchi-Fujimoto disease with heart involvement: Case-based review. Rheumatol. Int. 2022, 42, 341–348. [Google Scholar] [CrossRef]
- Noori, M.A.M.; Rushdy, A.; Fichadiya, H.; Sherif, R.; Younes, I.; Lenchur, P.D.; Lenchur, P.M.; Shamoon, F. Stemi mimicking post COVID: A case of focal myopericarditis post COVID infection. J. Community Hosp. Intern. Med. Perspect. 2021, 11, 769. [Google Scholar] [CrossRef] [PubMed]
- Okor, I.; Sleem, A.; Zhang, A.; Kadakia, R.; Bob-Manuel, T.; Krim, S.R. Suspected COVID-19-Induced Myopericarditis. Ochsner J. 2021, 21, 181–186. [Google Scholar] [CrossRef]
- Bulbul, R.F.; Al Suwaidi, J.; Al-Hijji, M.; Al Tamimi, H.; Fawzi, I. COVID-19 Complicated by Acute Respiratory Distress Syndrome, Myocarditis, and Pulmonary Embolism. A Case Report. J. Crit. Care Med. (Univ. De Med. Si Farm. Din Targu Mures) 2021, 7, 123–129. [Google Scholar] [CrossRef]
- Khatri, A.; Wallach, F. Coronavirus disease 2019 (COVID-19) presenting as purulent fulminant myopericarditis and cardiac tamponade: A case report and literature review. Heart Lung 2020, 49, 858–863. [Google Scholar] [CrossRef] [PubMed]
- Nicol, M.; Cacoub, L.; Baudet, M.; Nahmani, Y.; Cacoub, P.; Cohen-Solal, A.; Henry, P.; Adle-Biassette, H.; Logeart, D. Delayed acute myocarditis and COVID-19-related multisystem inflammatory syndrome. ESC Heart Fail. 2020, 7, 4371–4376. [Google Scholar] [CrossRef] [PubMed]
- Hudowenz, O.; Klemm, P.; Lange, U.; Rolf, A.; Schultheiss, H.P.; Hamm, C.; Müller-Ladner, U.; Wegner, F. Case report of severe PCR-confirmed COVID-19 myocarditis in a European patient manifesting in mid January 2020. Eur. Heart J. Case Rep. 2020, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, W.; Lammens, M.; Kerckhofs, A.; Voets, E.; van San, E.; van Coillie, S.; Peleman, C.; Mergeay, M.; Sirimsi, S.; Matheeussen, V.; et al. Fatal lymphocytic cardiac damage in coronavirus disease 2019 (COVID-19): Autopsy reveals a ferroptosis signature. ESC Heart Fail. 2020, 7, 3772–3781. [Google Scholar] [CrossRef]
- Hussain, H.; Fadel, A.; Alwaeli, H.; Guardiola, V. Coronavirus (COVID-19) Fulminant Myopericarditis and Acute Respiratory Distress Syndrome (ARDS) in a Middle-Aged Male Patient. Cureus 2020, 12, e8808. [Google Scholar] [CrossRef]
- Rehman, M.; Gondal, A.; Rehman, N.U. Atypical Manifestation of COVID-19-Induced Myocarditis. Cureus 2020, 12, e8685. [Google Scholar] [CrossRef]
- Monmeneu, J.V.; Mafe, E.D.; Soler, J.A.; Perez, B.V.; Caravaca, J.S.; Torres, R.B.; García-Gonzalez, P.; Ortega, L.H.; Lopez-Lereu, M.P.; MacEira, A.M.; et al. Subacute perimyocarditis in a young patient with COVID-19 infection. Eur. Heart J. Case Rep. 2020, 4, 1–3. [Google Scholar] [CrossRef]
- Tavazzi, G.; Pellegrini, C.; Maurelli, M.; Belliato, M.; Sciutti, F.; Bottazzi, A.; Sepe, P.A.; Resasco, T.; Camporotondo, R.; Bruno, R.; et al. Myocardial localization of coronavirus in COVID-19 cardiogenic shock. Eur. J. Heart Fail. 2020, 22, 911–915. [Google Scholar] [CrossRef]
- Boehmer, T.K.; Kompaniyets, L.; Lavery, A.M.; Hsu, J.; Ko, J.Y.; Yusuf, H.; Harris, A.M. Association Between COVID-19 and Myocarditis Using Hospital-Based Administrative Data—United States, March 2020–January 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1228–1232. [Google Scholar] [CrossRef]
- Wong, H.L.; Hu, M.; Zhou, C.K.; Lloyd, P.C.; Amend, K.L.; Beachler, D.C.; Secora, A.; McMahill-Walraven, C.N.; Lu, Y.; Wu, Y.; et al. Risk of myocarditis and pericarditis after the COVID-19 mRNA vaccination in the USA: A cohort study in claims databases. Lancet 2022, 399, 2191–2199. [Google Scholar] [CrossRef]
- Le Vu, S.; Bertrand, M.; Jabagi, M.-J.; Botton, J.; Drouin, J.; Baricault, B.; Weill, A.; Dray-Spira, R.; Zureik, M. Age and sex-specific risks of myocarditis and pericarditis following COVID-19 messenger RNA vaccines. Nat. Commun. 2022, 13, 1–9. [Google Scholar] [CrossRef]
- Block, J.P.; Boehmer, T.K.; Forrest, C.B.; Carton, T.W.; Lee, G.M.; Ajani, U.A.; Christakis, D.A.; Cowell, L.G.; Draper, C.; Ghildayal, N.; et al. Cardiac Complications After SARS-CoV-2 Infection and mRNA COVID-19 Vaccination—PCORnet, United States, January 2021–January 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 517–523. [Google Scholar] [CrossRef] [PubMed]
- Jaiswal, V.; Sarfraz, Z.; Sarfraz, A.; Mukherjee, D.; Batra, N.; Hitawala, G.; Yaqoob, S.; Patel, A.; Agarwala, P.; Ruchika; et al. COVID-19 Infection and Myocarditis: A State-of-the-Art Systematic Review. J. Prim. Care Community Health 2021, 12, 21501327211056800. [Google Scholar] [CrossRef] [PubMed]
- Maslennikov, R.; Poluektova, E.; Ivashkin, V.; Svistunov, A. Diarrhoea in adults with coronavirus disease-beyond incidence and mortality: A systematic review and meta-analysis. Infect. Dis. 2021, 53, 348–360. [Google Scholar] [CrossRef]
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chen, H.; Yu, H.; et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J. Clin. Investig. 2020, 130, 2620–2629. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Oudit, G.Y.; Kassiri, Z.; Jiang, C.; Liu, P.P.; Poutanen, S.M.; Penninger, J.M.; Butany, J. SARS-coronavirus modulation of myocardial ACE2 expression and inflammation in patients with SARS. Eur. J. Clin. Investig. 2009, 39, 618–625. [Google Scholar] [CrossRef]
- Nicin, L.; Abplanalp, W.T.; Mellentin, H.; Kattih, B.; Tombor, L.; John, D.; Schmitto, j.; Heineke, J.; Emrich, F.; Arsalan, M.; et al. Cell type-specific expression of the putative SARS-CoV-2 receptor ACE2 in human hearts. Eur. Heart J. 2020, 41, 1804–1806. [Google Scholar] [CrossRef]
- Guo, T.; Fan, Y.; Chen, M.; Wu, X.; Zhang, L.; He, T.; Wang, H.; Wan, J.; Wang, X.; Lu, Z. Cardiovascular Implications of Fatal Outcomes of Patients with Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 811–818. [Google Scholar] [CrossRef]
- Rav-Acha, M.; Orlev, A.; Itzhaki, I.; Zimmerman, S.F.; Fteiha, B.; Bohm, D.; Kurd, R.; Samuel, T.Y.; Asher, E.; Helviz, Y.; et al. Cardiac arrhythmias amongst hospitalised Coronavirus 2019 (COVID-19) patients: Prevalence, characterisation, and clinical algorithm to classify arrhythmic risk. Int. J. Clin. Pract. 2021, 75, e13788. [Google Scholar] [CrossRef]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Calabrese, L.H. Cytokine storm and the prospects for immunotherapy with COVID-19. Clevel. Clin. J. Med. 2020, 87, 389–393. [Google Scholar] [CrossRef]
- Cremer, P.C.; Sheng, C.C.; Sahoo, D.; Dugar, S.; Prada, R.A.; Wang, T.K.M.; Hassan, O.K.A.; Hernandez-Montfort, J.; Wolinsky, D.A.; Culver, D.A.; et al. Double-blind randomized proof-of-concept trial of canakinumab in patients with COVID-19 associated cardiac injury and heightened inflammation. Eur. Heart J. Open 2021, 1, oeab002. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M. Targeting cytokine storm in COVID-19: What have we learned? Eur. Heart J. Open 2021, 1, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Gordon, A.C.; Angus, D.C.; Derde, L.P.G. Interleukin-6 Receptor Antagonists in Critically Ill Patients with COVID-19. N. Engl. J. Med. 2021, 385, 1147–1149. [Google Scholar] [CrossRef]
- Veinot, J.P. Diagnostic endomyocardial biopsy—still useful after all these years. Can. J. Cardiol. 2009, 25, e55. [Google Scholar] [CrossRef]
- Kindermann, I.; Kindermann, M.; Kandolf, R.; Klingel, K.; Bültmann, B.; Müller, T.; Lindinger, A.; Böhm, M. Predictors of outcome in patients with suspected myocarditis. Circulation 2008, 118, 639–648. [Google Scholar] [CrossRef]
- Leone, O.; Veinot, J.P.; Angelini, A.; Baandrup, U.T.; Basso, C.; Berry, G.; Bruneval, P.; Burke, M.; Butany, J.; Calabrese, F.; et al. 2011 consensus statement on endomyocardial biopsy from the Association for European Cardiovascular Pathology and the Society for Cardiovascular Pathology. Cardiovasc. Pathol. 2012, 21, 245–274. [Google Scholar] [CrossRef]
- Kindermann, I.; Barth, C.; Mahfoud, F.; Ukena, C.; Lenski, M.; Yilmaz, A.; Klingel, K.; Kandolf, R.; Sechtem, U.; Cooper, L.T.; et al. Update on myocarditis. J. Am. Coll. Cardiol. 2012, 59, 779–792. [Google Scholar] [CrossRef]
- Tymińska, A.; Ozierański, K.; Caforio, A.L.P.; Marcolongo, R.; Marchel, M.; Kapłon-Cieślicka, A.; Baritussio, A.; Filipiak, K.J.; Opolski, G.; Grabowski, M. Myocarditis and inflammatory cardiomyopathy in 2021: An update. Pol. Arch. Intern. Med. 2021, 131, 594–606. [Google Scholar] [CrossRef]
- Tschöpe, C.; Ammirati, E.; Bozkurt, B.; Caforio, A.L.P.; Cooper, L.T.; Felix, S.B.; Hare, J.M.; Heidecker, B.; Heymans, S.; Hübner, N.; et al. Myocarditis and inflammatory cardiomyopathy: Current evidence and future directions. Nat. Rev. Cardiol. 2021, 18, 169–193. [Google Scholar] [CrossRef]
- Georgiopoulos, G.; Figliozzi, S.; Sanguineti, F.; Aquaro, G.D.; di Bella, G.; Stamatelopoulos, K.; Chiribiri, A.; Garot, J.; Masci, P.G.; Ismail, T.F. Prognostic Impact of Late Gadolinium Enhancement by Cardiovascular Magnetic Resonance in Myocarditis: A Systematic Review and Meta-Analysis. Circ. Cardiovasc. Imaging 2021, 14, E011492. [Google Scholar] [CrossRef] [PubMed]
- Rafiee, M.J.; Fard, F.B.; Friedrich, M.G. COVID-19, myocardial edema and dexamethasone. Med. Hypotheses 2020, 145, 110307. [Google Scholar] [CrossRef]
- Liguori, C.; Farina, D.; Vaccher, F.; Ferrandino, G.; Bellini, D.; Carbone, I. Myocarditis: Imaging up to date. La Radiol. Med. 2020, 125, 1124. [Google Scholar] [CrossRef]
- Amin, H.; Siddiqui, W.J. Cardiomegaly. In Diagnostic Atlas of Pediatric Imaging: Chest and Mediastinum; Jaypee Brothers Medical Pub.: New Delhi, India, 2021; p. 88. [Google Scholar] [CrossRef]
- Tymińska, A.; Ozierański, K.; Skwarek, A.; Kapłon-Cieślicka, A.; Baritussio, A.; Grabowski, M.; Marcolongo, R.; Caforio, A.L.P. Personalized Management of Myocarditis and Inflammatory Cardiomyopathy in Clinical Practice. J. Pers. Med. 2022, 12, 183. [Google Scholar] [CrossRef]
- RECOVERY Collaborative Group. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- RECOVERY Collaborative Group. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2021, 397, 1637–1645. [Google Scholar] [CrossRef]
- Mazeraud, A.; Jamme, M.; Mancusi, R.L.; Latroche, C.; Megarbane, B.; Siami, S.; Zarka, J.; Moneger, G.; Santoli, F.; Argaud, L.; et al. Intravenous immunoglobulins in patients with COVID-19-associated moderate-to-severe acute respiratory distress syndrome (ICAR): Multicentre, double-blind, placebo-controlled, phase 3 trial. Lancet Respir. Med. 2022, 10, 158. [Google Scholar] [CrossRef]
- De la Concepción, M.L.R.; Ainsua-Enrich, E.; Reynaga, E.; Ávila-Nieto, C.; Santos, J.R.; Roure, S.; Mateu, L.; Paredes, R.; Puig, J.; Jimenez, J.M.; et al. High-dose intravenous immunoglobulins might modulate inflammation in COVID-19 patients. Life Sci. Alliance 2021, 4, lsa.202001009. [Google Scholar] [CrossRef]
- Tardif, J.C.; Bouabdallaoui, N.; L’Allier, P.L.; Gaudet, D.; Shah, B.; Pillinger, M.H.; Lopez-Sendon, J.; da Luz, P.; Verret, L.; Audet, S.; et al. Colchicine for community-treated patients with COVID-19 (COLCORONA): A phase 3, randomised, double-blinded, adaptive, placebo-controlled, multicentre trial. Lancet Respir. Med. 2021, 9, 924–932. [Google Scholar] [CrossRef]
- Maisch, B.; Alter, P. Treatment options in myocarditis and inflammatory cardiomyopathy: Focus on i. v. immunoglobulins. Herz 2018, 43, 423–430. [Google Scholar] [CrossRef]
- Mirna, M.; Schmutzler, L.; Topf, A.; Boxhammer, E.; Sipos, B.; Hoppe, U.C.; Lichtenauer, M. Treatment with Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) Does Not Affect Outcome in Patients with Acute Myocarditis or Myopericarditis. J. Cardiovasc. Dev. Dis. 2022, 9, 32. [Google Scholar] [CrossRef]
- Rathore, S.S.; Rojas, G.A.; Sondhi, M.; Pothuru, S.; Pydi, R.; Kancherla, N.; Singh, R.; Ahmed, N.K.; Shah, J.; Tousif, S.; et al. Myocarditis associated with COVID-19 disease: A systematic review of published case reports and case series. Int. J. Clin. Pract. 2021, 75, e14470. [Google Scholar] [CrossRef]
- Chedid, M.; Waked, R.; Haddad, E.; Chetata, N.; Saliba, G.; Choucair, J. Antibiotics in treatment of COVID-19 complications: A review of frequency, indications, and efficacy. J. Infect. Public Health 2021, 14, 570–576. [Google Scholar] [CrossRef]
- Horby, P.W.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Emberson, J.; Palfreeman, A.; Raw, J.; Elmahi, E.; Prudon, B.; et al. Lopinavir–ritonavir in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2020, 396, 1345–1352. [Google Scholar] [CrossRef]
- WHO Solidarity Trial Consortium. Repurposed Antiviral Drugs for COVID-19—Interim WHO Solidarity Trial Results. N. Engl. J. Med. 2021, 384, 497–511. [Google Scholar] [CrossRef]
- Vegivinti, C.T.R.; Evanson, K.W.; Lyons, H.; Akosman, I.; Barrett, A.; Hardy, N.; Kane, B.; Keesari, P.R.; Pulakurthi, Y.S.; Sheffels, E.; et al. Efficacy of antiviral therapies for COVID-19: A systematic review of randomized controlled trials. BMC Infect. Dis. 2022, 22, 1–45. [Google Scholar] [CrossRef]
- Pollack, A.; Kontorovich, A.R.; Fuster, V.; Dec, G.W. Viral myocarditis—diagnosis, treatment options, and current controversies. Nat. Rev. Cardiol. 2015, 12, 670–680. [Google Scholar] [CrossRef]
- Ammirati, E.; Cipriani, M.; Moro, C.; Raineri, C.; Pini, D.; Sormani, P.; Mantovani, R.; Varrenti, M.; Pedrotti, P.; Conca, C.; et al. Clinical Presentation and Outcome in a Contemporary Cohort of Patients with Acute Myocarditis: Multicenter Lombardy Registry. Circulation 2018, 138, 1088–1099. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author (One Surname et al.) | Age (Years) | Sex (m/f) | Reported Symptoms | Medical History (Comorbidities, Previous Surgeries, Events) | Myocarditis during COVID (yes/no) | Myocarditis Post COVID (How Long) | Troponin | NT-probnp | ECHO Findings |
|---|---|---|---|---|---|---|---|---|---|
| Doyen et al. [10] | 69 | m | vomiting and diarrhoea 7 days before, cough, fever of 39 °C, dyspnoea, | hypertension | yes | no | 9002 ng/L (<40) | NR | mild LVH |
| Luetkens et al. [11] | 79 | m | fatigue, shortness of breath, recurrent syncopes, | asthma | yes | no | 18.8 ng/L ->63.5 ng/L | normal → 1178 pg/mL | normal |
| In-Cheol et al. [12] | 21 | f | febrile sensation, coughing, sputum, diarrhoea, shortness of breath | NR | yes | no | 1.26 ng/mL (<0.3) | 1929 pg/mL (<125 pg/mL) | severe LV systolic dysfunction |
| Sala et al. [13] | 43 | f | oppressive chest pain, dyspnoea | NR | yes | no | 135-107-106 ng/L (<14) | 512 pg/mL (<153) | mild LV systolic dysfunction, LVEF 43%, with inferolateral wall hypokinesis |
| Bonet et al. [14] | 19 | m | recurrent fever, cough, cervical adenopathy, chest pain and dyspnoea | NR | no | 4 weeks | 4200 ng/L (<79) | 17,377 (<500) | LVEF 20%, low cardiac output |
| Ishikura et al. [15] | 45 | m | NR | NR | no | 5 weeks | 31.516 pg/mL (≤30) | NR | severe hypokinesis, LVEF 7.4% |
| Meyer et al. [16] | 81 | m | no symptoms | hypertension, prostate adenocarcinoma | no | 6 months | NR | NR | LVEF 39%, global mild hypokinesia and severe inferior wall hypokinesia |
| Roest et al. [17] | 50 | NR | acute symptoms of cardiac decompensation | 6 years post heart transplantation | no | 5,5 months | 55 ng/L | 212 pmol/L (elevated) | biventricular failure and congestion |
| Inciardi et al. [18] | 53 | f | severe fatigue, fever and cough week before | No previous history of cardiovascular disease | yes | no | 0.24 ng/mL (<0.01) | 5647 pg/mL (<300) | LVEF 40%, increased wall thickness, the diffuse echo-bright appearance of the myocardium, diffuse hypokinesis, LV diastolic function mildly impaired with mitral inflow patterns, E/A ratio of 0.7 and E/e’ ratio of 12, pericardial effusion (max 11 mm) without signs of tamponade |
| Hu et al. [19] | 37 | m | chest pain and dyspnoea for 3 days, accompanied by diarrhoea | NR | yes | no | >10,000 ng/L (elevated) | 21,025 ng/L (elevated) | LVEF 27%, enlarged heart LVED 58 mm, LAED 39 mm, RVED 25 mm, RAED 48 mm, trace (2 mm) pericardial effusion |
| Zeng et al. [20] | 63 | m | expectoration of the white sputum, shortness of breath, chest tightness after activity, | allergic cough for 5 years, previous smoking history | yes | no | 11.37 g/L (elevated) | 22.600 pg/mL (elevated) | LVEF 32%, diffuse myocardial dyskinesia, enlarged left ventricle, pulmonary hypertension 44 mmHg |
| Aldeghaither et al. [21] | 39 | f | fever, dyspnoea, chest pain, diarrhoea | NR | No | 4 weeks (asymptomatic) | 11,810 ng/L | NR | large pericardial effusion with severe biventricular dysfunction and LVEF of 10–15% (cardiac tamponade with concurrent cardiogenic shock) |
| Aldeghaither et al. | 25 | m | dyspnoea, fever, hypotension | NR | no | 5 weeks (asymptomatic) | 1557 ng/L | NR | severe LV systolic dysfunction with LVEF 15–20% and moderate RV systolic dysfunction |
| Aldeghaither et al. | 21 | m | dyspnoea, fever | NR | yes | no | 27,000 ng/L | NR | severe biventricular systolic dysfunction with LVEF 5–10% |
| Amin et al. [22] | 18 | f | loss of consciousness, fever, headache | NR | yes | no | 3 × UNL | 21,000 pg/mL (<125) | small LV, LVEDD: 42 mm, LVEF: 10%with global hypokinesis, a normal RV, and PAP, no PE or thrombosis, and no significant valve lesions or dysfunction |
| Amin et al. | 32 | m | syncope after an episode of chest pain with fever and myalgia, dyspnoea, dry cough | NR | yes | no | 2 × UNL | 10,000 pg/mL (<125) | LVEF: 25%, an enlarged LVEDD, normal RV size (mild dysfunction), and normal valvular and pericardial function, increased wall thickness. |
| Amin et al. | 34 | f | losing consciousness, fever and headache for six consecutive days | NR | yes | no | 4 × UNL | 3000 pg/mL (<125) | normal LV and RV size, moderate TVR and MVR, sPAP: 30 mmHg, LVEF: 30%. |
| Amin et al. | 22 | m | dry cough, dyspnoea | no previous medical history | yes | no | 3 × UNL | 21,000 pg/mL (<125) | LVEF 30–35%, LVEDD of 5 cm, moderate RV enlargement and dysfunction, dilated inferior vena cava, and mild left-sided pleural effusion |
| Amin et al. | 45 | m | fever, dyspnoea, pleuritic chest pain | NR | yes | no | 2 × UNL | 4300 pg/mL (<125) | LVEF of 45%, normal LV size and function without regional wall motion abnormalities, and circumferential pericardial effusion without significant respiratory changes in the mitral and tricuspid valves |
| Amin et al. | 28 | m | chest pain, fever, dry cough | NR | yes | no | 2 × UNL | 1200 pg/mL (<125) | LVEF 30–35%, hypokinesis in the anterior wall, normal LV size as well as normal RV size and function |
| Amin et al. | 51 | f | fever, cough, cardiopulmonary arrest | NR | yes | no | 3 × UNL | 22,000 pg/mL (<125) | LVEF 35%, normal LV size, increased LV wall thickness |
| Amin et al. | 39 | f | chest pain, cough, orthopnea | asthma | yes | no | 2 × UNL | 23,000 pg/mL <125 pg/ml | LVEF 30–35%, mild pericardial effusion, RV enlargement, hypermobile thrombus in the LV (1.5 × 1.5 cm) |
| Menter et al. [23] | 47 | f | oligosymptomatic flu-like disease for a week, then—she was found unconscious and apneic at home | obesity [body mass index (BMI) 31.6], depression | yes | no | 507 ng/L (elevated) | >70,000 ng/L (elevated) | moderately reduced left ventricular function LVEF 30% and normal right ventricular size and function. There was no evidence of left ventricular hypertrophy or dilatation. |
| Ashok et al. [24] | 53 | m | fever and right upper quadrant abdominal pain | no previous medical history | yes | no | 2.6 ng/L (normal) | NR | LV systolic impairment with no obvious regional wall motion abnormalities |
| Li et al. [25] | 60 | m | 8 days of fever, cough, and worsening dyspnoea, with mild abdominal pain and diarrhoea despite completing a 3-day course of azithromycin as an outpatient. Denied chest pain, nausea, or vomiting. | hypertension and hyperlipidaemia | yes | no | 582 ng/L (<6–14) | 15,642 pg/mL (0–300) | significant for severe segmental LV systolic dysfunction, LVEF 15–20% with hypokinesis of the apex, distal anterior septum, and anterior and lateral walls, with a small pericardial effusion. Right ventricular size and function were normal |
| Nakatani et al. [26] | 49 | m | NR | no previous medical history | yes | no | 1.010 ng/mL (≤0.014) | 27,541 pg/mL, (≤125.0) | low LVEF: <20% and diffuse myocardial hypertrophy |
| Ismayl et al. [27] | 53 | m | chest pain, diaphoresis, intense fatigue, and body aches | no previous medical history | no | 35 days | 2.83 ng/mL (<0.04), with a peak of 13.6 ng/mL | 60,230 pg/mL | severe global hypokinesis of the left ventricle LVEF: 25% |
| Thomson et al. [28] | 39 | f | 1-day history of profuse diarrhoea, vomiting, abdominal pain, and no respiratory symptoms | laparotomy with ovarian cystectomy | yes | no | 118 ng/L (<14) | 6543 (norm: <125) | severely reduced biventricular function, normal cardiac chamber size, and a globally thickened, bright myocardium (measuring 16 mm in the septum and inferolateral wall) with a small-to-moderate-sized pericardial effusion. |
| Campoamor et al. [29] | 32 | m | acute chest pain, palpitations | After COVID-19, only dry cough and odynophagia were exhibited, resolved after symptomatic treatment with paracetamol. otherwise healthy | no | 40 days | 149.87 pg/mL (24–30 pg/mL) | 70.89 pg/mL (<125) | a dilated LV, mild diffuse hypokinesia with light impairment of global systolic function, and a dilated LA |
| Flagiello et al. [30] | 30 | f | fever, chest pain, and worsening dyspnoea for 5 days | No previous medical history | yes | no | 5891 ng/L (elevated) | 16,569 ng/L (elevated) | 20-mm pericardial effusion compressing the right heart chambers and LV systolic dysfunction, LVEF: 35%, with global hypokinesis |
| Pascariello et al. [31] | 19 | m | worsening of the flu syndrome, presented with fever, cough and diarrhoea and vomits for 3 days. | autism spectrum | yes | no | 1033 ng/mL (<14) | 47,650 ng/mL (<300) | enlarged LV: 56 mm, diffuse myocardial hypo-akinesia along with severe left ventricular ejection systolic dysfunction LVEF: 15–20%, decrease in right cardiac function |
| Gaudriot et al. [32] | 38 | m | chest pain and vomiting | suggested chronic lymphopenia | no | 5 weeks | 1600 pg/mL (<14) | 10,500 pg/mL (<300) | biventricular infiltrative myocardial hypertrophy, associated with a circumferential non-compressive pericardial effusion and a restrictive mitral inflow profile, no systolic dysfunction |
| Shah et al. [33] | 19/38 | m/m | 7-day history of fever, generalized weakness, cough, and shortness of breath/chest pain, not related to breathing, exertion, or posture | no previous medical history | yes/no | no/3 weeks | 1. 256 ng/mL (<15)/2. 1264 ng/L (<15) | NR | normal left ventricle size with severe global hypokinesia and severely reduced LV systolic function LVEF:24%, and there was mild-to-moderate MR, RV function was also severely reduced, with moderate-to-severe TR and mildly increased PAP 40 mm Hg, no pericardial effusion/normal left ventricular systolic function, LVEF: 53%, apex was noted to be akinetic while other segments were moving normally, no pericardial effusion |
| Shabbir et al. [34] | 50 | f | 4-day history of central chest pain, which was made worse on lying flat and on deep inspiration | hypertension, previous myocarditis, reactive arthritis | no | no | 77 ng/L (0–14) | NR | a trivial anterior pericardial effusion with good biventricular function |
| Gauchotte et al. [35] | 69 | m | fever, asthenia, abdominal pain progressing for a week. | diabetes, hypertension, ischemic heart disease | no | no | 8066 pg/mL (elevated) | NR | a non-dilated LV and severe and diffuse LV hypokinesia, LVEF: 30% |
| Bernal-Torres et al. [36] | 38 | f | palpitations that started suddenly 3 days prior to presentation and were associated with haemodynamic instability | no previous medical history | yes | no | 1190 ng/mL (<14) | BNP 13,000 pg/mL (<100) | LV with global hypokinesia, severely reduced systolic function, LVEF:30%, without valvular heart disease, and mild pericardial effusion (2 mm) |
| Oleszak et al. [37] | 52 | m | cough, subjective fever, shortness of breath, trace hemoptysis over the last 5 days | hypertension, previous myocarditis, reactive arthritis | yes | no | 0.017 ng/mL (elevated) | proBNP 1220 pg/mL (elevated) | LVEF: 10–15%, reduced RV systolic function, and global dilatation of all 4 chambers, RV, RA and LA moderately dilated, compared to mild LV dilation, LVIDd: 5.8 cm, lLVIDs: 5.1 cm, IVS: 1.3 cm, sPAP: 18 mm Hg, no significant valvular pathology, mild MVR and TVR, pericardial effusion was not visualized |
| Gay et al. [38,39] | 56 | m | dyspnoea and lethargy | obesity, hyperlipidemia | yes | no | troponin I: 1.3 ng/mL (elevated) | BNP 790 pg/mL (elevated) | extreme concentric LVH with a wall thickness of 2.0 cm, reduced biventricular function, LVEF: 20%, and a small pericardial effusion |
| Gomila-Grange et al. [39] | 39 | m | fever, right flank pain and diarrhoea for 6 days | former smoker, 68 g daily alcohol use | yes | no | troponin I: 3800 ng/mL (<13) | pro-BNP 27,696 pg/mL (< 125) | biventricular dysfunction, LVEF: 30% due to diffuse hypokinesis, diastolic dysfunction and slight posterior pericardial effusion without tamponade signs |
| Richard et al. [40] | 28 | f | found lethargic and covered in coffee ground emesis at home | diabetes mellitus type 1, diabetic gastroparesis, asthma, anxiety, depression with multiple previous episodes of DKA, questionable history of IV drug use | no | yes (time not reported) | 0.04 ng/mL (<0.04) | NR | LVEF: 26–30% and MVR |
| Wenzel et al. [41] | 39/36 | m/m | shortness of breath | Both patients were obese and had a history of upper airway infection with headache, fever, and cough up to 4 weeks before admission. A; dyslipidemia B: hypertension, smoking dyslipidemia, CAD heart failure, lung disease | no | approx 30 days | 0.372/0.057 ng/mL (<0.024) | BNP—109/258 ng/L (<100) | signs of LV dysfunction (decreased global and regional longitudinal strain or reduced LVEF and increased LVEDD) A—preserved LVEF: 60% without any wall motion abnormalities, but the focal echo-bright appearance of the interventricular septum (not shown) and slightly impaired global longitudinal strain. |
| Bemtgen et al. [42] | 18 | m | hyperpyrexia (42 °C), chills and tachycardia | NR | no | 2 months | 341 ng/L, (<14) | NR | severely impaired LVEF, LVEF: 25% |
| Beşler et al. [43] | 20 | m | febrile sensation and chest pain | NR | yes | 0.572 ng/mL (<0.045) | 127 ng/L (<125) | NR | |
| Meel et al. [44] | 31 | m | exertional dyspnoea | NR | no | 3 weeks | 319 ng/L (< 14) | 143 ng/L (<300) | preserved LV and RV contractility and no regional wall motion abnormality ormyocardial hypertrophy. |
| Paul et al. [45] | 35 | m | chest pain and fatigue | NR | yes | no | 2885 ng/L (elevated) | NR | normal systolic function with no pericardial effusion |
| Coyle et al. [46] | 57 | m | shortness of breath, fevers, cough, myalgias, decreased appetite, nausea, and diarrhoea for 1 week | hypertension | yes | no | 0.02 → 7.33 ng/mL (<0.05) | 859 pg/mL (<126) | moderate diffuse hypokinesis withrelative apical sparing and an LVEF: 35% to 40% |
| Irabien-Ortiz et al. [47] | 59 | f | feverish feeling for 5 days, accompanied by squeezing anginal chest pain, no respiratory symptoms | hypertension, cervical degenerative arthropathy, chronic lumbar radiculopathy, lymph node tuberculosis diagnosed due to erythema nodosum, and migraine | yes | no | 220 → 1100 ng/dL (elevated) | 4421 ng/L (elevated) | disclosed moderate concentric hypertrophy, diminished intraventricular volumes with preserved LVEF, no segmental abnormalities, and moderate pericardial effusion with no signs of hemodynamic worsening 2 h after admission—severe biventricular failure and diffuse myocardial oedema |
| Frustaci et al. [48] | 50 | f | fever, dry cough and shortness of breath | no | yes/no | no | 0.077 mcg/L, (<0.014) | NR | normal size and function of the LV with mild pericardial effusion |
| Sardari et al. [49] | 31 | m | dyspnoea on exertion and low-grade fever | NR | no | 3 weeks | <0.03 ng/mL (normal) | NR | mild LV dysfunction |
| Warchoł et al. [50] | 74 | m | hemodynamically unstable new onset VT- lasting 12 h | atrial fibrillation, catheter ablation 3 times, hypertension, type 2 diabetes, and hypothyroidism | yes | no | troponin T 72 ng/L (<14 ng/L) | 2451 ng/L (<125) | NR |
| Shahrami et al. [51] | 78 | m | shortness of breath, cough, anosmia, and myalgia | hypertension | yes | no | 103 ng/mL (0–0.3) | NR | reduced LVEF: 15%, PAP = 50 mmHg, mildly enlarged LV and moderate to severe LV dysfunction, mild diastolic dysfunction, mild MVR, and normal septal thickness |
| Gaine et al. [52] | 58 | m | recent-onset palpitations and progressive dyspnoea | no previous medical history | yes | no | T 25 ng/L (0–14) | 3428 pg/mL (0–400) | severely impaired LVEF: 20%, MR |
| Taouihar et al. [53] | 51 | m | intense epigastric pain at rest and effort, associated with nausea and vomiting progressing for 5 days | hyperthyroidism | yes | no | 20,000 ng/L (<20) | NR | akinesia of the tip of the anteroseptal and inferior wall of the LV with severe hypokinesia of the inferior wall, a systolic dysfunction of LV, LVEF: 40% |
| Dahl et al. [54] | 37 | m | fever, headache, unilateral, painful neck swelling | no previous medical history | yes | no | T 90 ng/L (0–15) | 160 ng/L (0–85) | good ventricular function, no hypokinesia and significant valve pathology at admission. Echo repeated on day 2 revealed a deterioration of the LV function with reduced LVEF: 40% |
| Matsumura et al. [55] | 41 | m | general fatigue and a high fever | hypertension | no | no | 0.094 ng/mL | 4938 pg/mL (elevated) | impaired LV systolic function, LVEF: 53%, LVDDand LVDS: 42 and 31 mm, respectively, IVS: 12 mm; LVPW: 12 mm, and mild pericardial effusion |
| Praet et al. [56] | 31 | f | fever, cough, rapidly progressive shortness of breath, an episode of cramping abdominal pain and diarrhoea one week earlier | no previous medical history | no | 2 months before | hs-TnT 151 ng/L (elevated) | 25,386 pg/mL (elevated) | severely depressed LV function due to moderate to severe hypokinesia |
| Masiak et al. [57] | 43 | m | anosmia and ageusia for 1-day, mild fever for a few days. All symptoms disappeared completely. Five weeks later admitted to the hospital due to fever with sweats, sore throat, fatigue, dyspnoea, dry cough, skin changes for 8 days prior to the hospitalization. Additionally, discomfort in the right lower abdomen, discoloured stools, and dark-coloured urine. | no previous medical history | no | 5 weeks later | 0.119 ng/mL (<0.03) | BNP 965 pg/mL (<7) | globally reduced myocardial contractility, decreased LVEF: 40% |
| Noori et al. [58] | 44 | m | dry cough associated with generalized body ache but denied any chest pain, shortness of breath, palpitation, orthopnea, or fever | NSTEMI 2 weeks before, COVID pneumonia 1 month ago | no | 1 month | 11.67 (elevated) | NR | LVEF: 40–45%, mildly decreased globular LV systolic function and moderate to severe hypokinesis involving inferior, inferoposterior wall without thinning of myocardium |
| Okor et al. [59] | 72 | f | worsening shortness of breath, | hypertension, chronic obstructive pulmonary disease | no | 1 week | 1.0 ng/mL | 2336 pg/mL (0–99) | severely reduced LV systolic function, LVEF: 20%, multiple LV wall abnormalities including akinetic inferolateral and apical anterior walls and hypokinetic basal and septal walls, small pericardial effusion was also noted, initial echocardiogram in 4-chamber view showed multiple segmental abnormalities and an LVEF: 20%. Parasternal long axis view showed multiple segmental abnormalities, trace effusion, and low LVEF: 20%. |
| Bulbul et al. [60] | 49 | f | cough, shortness of breath | NR | yes | no | 9 ng/L (3–10) | 430 pg/mL (<125) | significant reduction in the LVEF: 25%, diffusely hypokinetic walls and a reduction in RV function. |
| Khatri et al. [61] | 50 | m | fevers, chills, generalized malaise, non-productive cough, dyspnoea for 3–4 days and an episode of near-syncope | hypertension and ischemic stroke. | yes | no | 544 ng/L | NR | severe global LV systolic dysfunction, RV enlargement, RV systolic dysfunction, moderate to large pericardial effusion, Intermittent RVimpaired filling and collapse (s/o tamponade) |
| Nicol et al. [62] | 40 | m | fever, odynophagia, and left neck pain | obesity (BMI 34.8) | no | 4 weeks | 485 ng/L (<34) | 2960 ng/L (elevated) | decrease in LVEF: 45%, low cardiac output (3 L/min), and both subtle hypertrophy and akinesia of posterolateral left ventricular wall with small pericardial effusion opposite |
| Hudowenz et al. [63] | 48 | m | high-grade fever, dyspnoea and haemoptysis | NR | yes | no | 3264 pg/mL (0–14) | 12,232 pg/mL (1–300) | highly reduced LVEF: 22%, RVEF 28% |
| Jacobs et al. [64] | 48 | m | fever, diarrhoea, cough, dysosmia, and dyspnoea | hypertension | yes | no | 14,932 ng/L (<45) | 9223 pg/mL (<125) | hyperdynamic ventricular function, although under massive support of inotropic agentsand vasopressors |
| Hussain et al. [65] | 51 | m | dry cough, fatigue, dyspnoea, and a fever | hypertension | yes | no | 0.29 ng/mL (elevated) | 1287 pg/mL (elevated) | enlarged heart with a decrease in systolic function and an LVEF: 20% |
| Rehman et al. [66] | 39 | m | midsternal chest pain | NR | yes | no | 5.97 ng/mL (elevated) | 379 pg/mL | LVEF: 55–60%, no wall motion abnormalities, no evidence of pericarditis or pericardial effusion |
| Monmeneu et al. [67] | 43 | m | fever for 14 days, dry cough, haemoptoic sputum, | NR | yes | no | T 9 → 24 → 24 → 18 → 15 ng/L (<14 ng/L) | 456 pg/mL (<125) | NR |
| Tavazzi et al. [68] | 69 | m | worsening dyspnoea, persistent cough, weakness for 4 days, | NR | yes | no | 4332 ng/L (elevated) | NR | LVEF: 34%, LVEDD: 56 mm, severe and diffuse LV hypokinesia |
| Author (One Surname et al.) | MR Findings | Biopsy Findings | Complications | Outcome |
|---|---|---|---|---|
| Doyen D. et al. | subepicardial late gadolinium enhancement of apex and inferolateral wall | NR | NR | NR |
| Luetkens et al. | mild systolic dysfunction (LVEF: 49%) with discrete global hypokinesis, pericardial effusion localized mainly around the LV lateral wall (~10 mm), diffuse interstitial myocardial oedema with an increased T2 signal intensity ratio, prolonged T1 relaxation times | NR | NR | NR |
| In-Cheol et al. | diffuse high signal intensity in the LV myocardium, myocardial wall thickening (which suggested myocardial wall oedema), extensive transmural late gadolinium enhancement | NR | NR | NR |
| Sala et al. | recovery of systolic function (day-7), with the persistence of mild hypokinesia at basal and mid LV segments, diffuse myocardial oedema, determining wall pseudo-hypertrophy, | diffuse T-lymphocytic inflammatory infiltrates (CD3+ >7/mm2) with huge interstitial oedema and limited foci of necrosis | NR | recovered |
| Bonet et al. | NR | myocarditis with inflammatory infiltrates consisting of a majority of lymphocytes and neutrophils, oedema but not typical myocyte necrosis, CD-4-positive T lymphocytes, RT-PCR for SARS-CoV-2 and PCR for other cardiotropic viruses was negative | NR | recovered |
| Ishikura et al. | NR | diffuse lymphocyte infiltration in the interstitium of the myocardial tissue, atrophy and shedding degeneration myofibrils, no myocardial necrosis | cardiogenic shock | recovered |
| Meyer et al. | focal infero-basal LV wall oedema, elevated T1 and T2 myocardial relaxation times, the post-contrast sequences showed sub-epicardial and mid-wall late gadolinium enhancement in the basal inferior, basal inferolateral, and anterior LV walls | NR | NR | NR |
| Roest et al. | LVEF: 22%, late gadolinium enhancement images showed a pattern of extensive subepicardial and several midwall subepicardial spots of enhancement of the left ventricle, myocardial oedema was absent (post-myocarditis state without active myocarditis) | focal subendocardial fibrosis and no signs of clinical relevant rejection | heart failure | recovered |
| Inciardi et al. | increased wall thickness with diffuse biventricular hypokinesis, especially in the apical segments, severe LV dysfunction (LVEF: 35%), biventricular myocardial interstitial oedema, phase-sensitive inversion recovery sequences showed diffuse late gadolinium enhancement extended to the entire biventricular wall, pericardial effusion was confirmed, | NR | heart failure | recovered |
| Hu et al. | NR | NR | cardiogenic shock and pulmonary infection | recovered |
| Zeng et al. | NR | NR | septic shock and DIC | death on the 33rd day of hospitalization |
| Aldeghaither et al. | NR | eosinophilic infiltrate of the myocardium (infiltrate consisting mainly of mononuclear cells—few lymphocytes and histiocytes with many eosinophils) | cardiogenic tamponade with concurrent cardiogenic shock | discharged home 28 days after admission |
| Aldeghaither et al. | NR | mixed inflammatory infiltrate with lymphocytes, histiocytes, neutrophils, eosinophils | cardiogenic and vasodilatory shock | discharged home 23 days after admission on intermittent hemodialysis, which was stopped 3 weeks later after improvement of the renal function |
| Aldeghaither et al. | NR | mild lymph-histiocytic interstitial myocardial infiltrate with occasional neutrophil | cardiogenic and vasodilatory shock | recovery. After 14 days of hospitalization, the patient was discharged home. At this time, both MCS devices were explanted. |
| Amin et al. | NR | NR | NR | death. she died due to cardiac arrest (less than 24 h after admission) |
| Amin et al. | NR | NR | NR | recovery. discharged after 2 weeks with an ejection fraction of 45%, Follow-up of the patient for 3 months revealed an LVEF of 45% and normal RV function. |
| Amin et al. | NR | NR | NR | recovery. Follow-up of the patient for 3 months showed an LVEF of 45–50% |
| Amin et al. | NR | NR | NR | recovery. discharged after 7 days with stable hemodynamics. Follow-up of the patient for 3 months showed an LVEF of 45% and a normal cTnI value. |
| Amin et al. | NR | NR | NR | recovery. discharged in a satisfying condition. Follow-up of the patient for 3 months showed an LVEF of 45%, mild pericardial effusion, and normal right ventricular size and function. |
| Amin et al. | NR | NR | NR | recovered within 3 days and was discharged in a satisfying condition. Follow-up of the patient for 3 months revealed LVEF of 45–50% and a normal cardiac function |
| Amin et al. | NR | NR | NR | recovery, discharged in a satisfying condition after 10 days. Follow-up of the patient over 3 months demonstrated an LVEF of 50% |
| Amin et al. | myocardial oedema and hyperemia suggestive of active myocarditis | NR | NR | recovery. discharged in a satisfying condition |
| Menter et al. | NR | multifocal inflammatory infiltrates consisting of neutrophilic granulocytes, lymphocytes and histiocytes, capillarostasis, and perifocal single-cell necroses of cardiomyocytes | the patient died of cardio-respiratory failure within 48 h of admission | |
| Ashok et al. | NR | no | NR | recovery |
| Li et al. | NR | NR | - | Recovery. The patient was ultimately discharged for physical rehabilitation on hospital day 52. |
| Nakatani et al. | NR | Mild lymphocytic infiltration and moderate to severe perivascular fibrosis with wall thickening of intramural arterioles, no sign of severe myocardial injury compatible with typical active myocarditis, ischemic changes were found with a focal coagulative necrotic area at microvascular level (approximately 0.08 mm2 in area) with losing nuclei, accompanied by microthrombi with fibrin and platelets in small vessels, scattered megakaryocytes were also seen in the capillaries, microthrombi were seen throughout the specimens and myocytes in non-necrotic areas often showed diffuse cytoplasmic vacuolization, presence of platelets in obstructive and non-obstructive microthrombi within the lumens of microvessels was confirmed by immunohistochemical expression of CD61, fibrin-rich microthrombi were also present as confirmed by phosphotungstic acid-hematoxylin stain, microvessels including intramural arterioles often showed swollen endothelial cells | Cardiogenic shock | death on day 5 due to intractable cardiogenic shock |
| Ismayl et al. | NR | diffuse interstitial and perivascular neutrophilic and lymphocytic infiltration with rare eosinophils and rare myocyte necrosis, suggesting fulminant myocarditis | combined right and left ventricular failure, multiorgan failure | significant improvement in hemodynamics and ejection fraction over the next 5 days |
| Thomson et al. | NR | A subtle mild interstitial infiltrate consists primarily of CD68 + macrophages and a lesser number of CD3+ T cells. Microthrombi were identified, with the degradation products suggesting a sub-acute microangiopathic process. No fibrosis nor myocardial necrosis was present. No viral particles were seen on electron microscopy. Concerning other causes of myocarditis, the EMB did not show interstitial fibrosis, iron accumulation, evidence of sarcoid or amyloid, or changes consistent with hypertrophic obstructive cardiomyopathy. | Pulseless electrical activity cardiac arrest with ECMO and CPR. Distal perfusion cannulae placed. Development of ischaemic right lower leg (without ECMO cannulae) requiring DSA and fasciotomy. | death after 9 days of hospitalization |
| Campoamor et al. | extensive subepicardial fibrosis with diffuse pericardial contrast uptake | NR | none | Recovery. The patient remained asymptomatic for the rest of the hospitalization period and was discharged home after 22 days of hospitalization |
| Flagiello et al. | area of myocardial late enhancement compatible with the diagnosis of myocarditis | slight interstitial fibrosis without inflammation, Immunohistochemical staining (CD3, CD20, and CD68) confirmed the absence of interstitial inflammation | Cardiogenic shock in less than 12 h with signs of systemic hypoperfusion (systemic arterial pressure <60 mm Hg, sweating, vomiting, oliguria, and lactate 4.5 mmol/L) and further degradation of the left ventricular systolic function (LVEF 10%, left ventricular outflow tract time-velocity integral 6 cm) despite an escalation of the inotropic (dobutamine 10 μg/kg/min) and vasopressor (noradrenaline 0.17 μg/kg/min) support. Ventilator-associated pneumonia (Streptococcus pneumoniae and Haemophilus influenzae). | Recovery. At 3-month follow-up, echocardiography confirmed the complete myocardial recovery (LVEF 65%) and cardiac magnetic resonance imaging showed no signs of residual myocardial fibrosis. |
| Pascariello et al. | NR | no | clinical deterioration, cardiogenic shock with severe hypotension, tachycardia, oliguria, anaemia and desaturation | Recovery. Discharged after 3 weeks. |
| Gaudriot et al. | T2 sequences showed diffuse hyperintense myocardium but suffered from too many artefacts to be considered diagnostic quality. Steady-state free precession cine images demonstrated biventricular cardiomyopathy (LVEF: 25%) with myocardial wall thickening. First-pass contrast-enhanced CMR did not reveal a subendocardial perfusion defect. Late gadolinium enhancement images demonstrated massive, heterogeneous, and predominantly subepicardial enhancement of the LV myocardium indicating a severe inflammation without evidence for ischaemic heart disease | Explantated heart, with large areas of myocardial necrosis, suppurated lesions, lymphocytic infiltration, polymorphic inflammatory infiltrate, mostly in myocardium areas but focally extended to endocardium and pericardium. Lymphocytes were predominant. Infiltrate also contained plasmocytes, neutrophils, eosinophils, and histiocytic and giant cells. Clusters of neutrophils with leucocytoclasia suggested suppurated lesions. Myocardial cells suffered from clarified cytoplasm, sometimes fibrillary or eosinophil, and enlarged dystrophic nucleus. Large areas of necrosis and haemorrhage were seen among these inflammatory areas. The adjacent myocardium showed interstitial oedema and focally recent interstitial fibrosis. Ziehl, Grocott, Gram, and EBER ISH stains were negative. Most lymphocytes were T phenotype CD5+, with only a few associated B lymphocytes CD20+. Numerous histiocytic cells were revealed by CD163 immunostaining. Cytomegalovirus immunostaining was negative as well as Epstein–Barr virus in situ hybridization. | patient became hypotensive and hypoxaemic (nasal cannula, oxygen 4 L/min) with clinical signs of pulmonary oedema, rapidly progressive biventricular hypokinetic non-dilated cardiomyopathy, myocarditis fulminant with cardiogenic shock | The patient recovered and was discharged for cardiovascular rehabilitation without any persistent respiratory or cardiac symptoms. |
| Shah et al. | NR/normal biventricular volumes and function, akinesia of the apico-lateral, apico-inferior walls and apical cap, myocardial hyperemia, and myocardial scar/necrosis consistent with a diagnosis of myocarditis | NR | acute kidney injury, ARDS/NR | discharged on day 16/chest pain-free upon discharge |
| Shabbir et al. | MRI of both lower limbs confirmed features of diffuse myositis with symmetrical appearances involving the anterior, medial and posterior muscle compartments of the thighs with subcutaneous oedema. A cardiac MRI showed normal LV and RV function, with possible evidence of myocardial oedema in the basal inferoseptum, in keeping with myocarditis, as well as a 16 mm circumferential pericardial effusion | NR | myositis | discharged day 13 |
| Gauchotte et al. | NR | Biopsy after death—Microscopic examination of the heart revealed the existence of a multifocal inflammatory infiltration in both ventricles and septum, composed in its majority of macrophages and lymphocytes, associated with a mild polymorphonuclear neutrophils infiltrate. The myocardium was edematous, containing dystrophic cardiomyocytes, without necrosis. A hypocellular confluent area of fibrosis was found in the posterior wall of LV. There was no significant inflammatory infiltrate in the wall of capillaries and vessels. | AKI KDIGO 3, need for vasoactive support, cardiogenic shock | deceased 6 days after admission |
| Bernal-Torres et al. | inflammatory manifestations, with the recovery of the ejection fraction | patient did not consent | cardiogenic shock | discharged day 16 |
| Oleszak et al. | NR | NR | respiratory distress | discharged |
| Gay et al. | NR | NR | respiratory failure and shock, oliguric kidney failure | recovered from critical illness, awaiting discharge to a rehabilitation centre |
| Gomila-Grange et al. | NR | NR | cardiogenic shock | One month after discharge, he was completely recovered |
| Richard et al. | myocardial necrosis, fibrosis, and hyperemia, indicating myocarditis according to the Lake Louise criteria | NR | ARDS, ventricular tachycardia, cardiogenic shock due to myocarditis fulminant, acute oliguric renal failure | The Impella device was removed, dobutamine was weaned off, and the patient was extubated the next day. |
| Wenzel et al. | patient A—native T1 map showing prolonged T1 relaxation times in the posterior interventricular septum and corresponding late gadolinium enhancement image with enhancement in the posterior septum, consistent with acute myocarditis. patient B—T2-short TI inversion recovery image, showing diffuse myocardial oedema and late gadolinium enhancement image with a subtle subepicardial enhancement of the lateral wall. | Immunohistochemistry and histology revealed myocardial inflammation in the absence of cardiomyocyte necrosis (Dallas criteria of ‘borderline myocarditis’6), with increased lymphocytes (CD3, LFA-1, and CD45R0) and macrophages (Mac-1), in part with highly abundant perforin-positive cytotoxic T cells. The inflammatory process seemed to be paralleled by increased thickness of small arteries | NR | discharged |
| Bemtgen et al. | NR | Significant infiltration of immune cells. Especially CD68+ macrophages and CD3+ T cells were found to be located primarily around small vessels within the myocardium, as shown by immunohistochemical stainings. Masson Trichrome and HE stainings further demonstrated the presence of perivascular fibrosis in serial tissue sections, but no myocyte necrosis | septic shock, severe end-organ failure | recovery |
| Beşler et al. | LV function, volumes, and mass were in normal range (LVEF: 64%, SV: 62.2 mL, LVEDV: 97 mL, LVESV: 34.8 mL, mass 128 g), T2 short tau inversion recovery sequence showed a subepicardial high-intensity signal in the mid posterolateral wall of LV which suggests myocardial wall oedema, subepicardial late gadolinium enhancement of the posterolateral wall in the mid-ventricle suggestive of myocarditis at 5 and 10 min after contrast administration, respectively | no | no | recovery |
| Meel et al. | normal LV and RV function and wall thickness with an LVEF: 65%, RVEF: 56% and wall thickness at end-diastole of 7 mm, delayed late gadolinium enhancement within the mid-wall as well as the epicardial regions involving the LV basal inferolateral wall, mid-anterolateral and mid-inferolateral wall T2 short tau inversion recovery black blood, high signal intensity within the LV anterolateral, inferolateral wall at the base and mid-ventricle level, on non-contrast T1 mapping, there was a prolongation of T1 time at the mid-ventricle segment 5 (1212 ± 141 ms) and segment 6 (1113 ± 93.8 ms) | no | no | recovery |
| Paul et al. | late subepicardial enhancement predominating in the inferior and lateral wall | no | no | recovery |
| Coyle et al. | diffuse biventricular and biatrial oedema with a small area of late gadolinium enhancement | no | cardiogenic shock, severe ARDS, | recovery |
| Irabien-Ortiz et al. | NR | no | cardiac arrest—electrical activity with no pulse and requiring cardiopulmonary resuscitation, emergent pericardiocentesis (drainage of serous fluid), and high-dose vasopressors for hemodynamic recovery | recovery |
| Frustaci et al. | confirmed normal LV dimensions and function (LVEF: 59%) and revealed the presence of right and left apical microaneurysms, late gadolinium enhancement imaging showed a subepicardial area in the inferolateral wall on basal and midventricular planes; corresponding mapping sequences documented a focal increase in native T1 values, extracellular volume fraction and T2 mapping values consistent with diffuse oedema and combined extracellular matrix expansion | diffusely mononuclear infiltrates associated with necrosis of adjacent myocytes and necrotizing vasculitis of intramural coronary arteries associated to positivity of CD45RO+ T-lymphocytes of the affected vessel wall. Arterioles not infiltrated by inflammatory cells presented at immunohistochemistry complement fractions (C3d) deposition suggesting coexisting endothelitis. Moreover, real-time PCR on two frozen endomyocardial samples for SARS-CoV-2 and the most common cardiotropic viruses, including adenovirus, cytomegalovirus, parvovirus B19, Epstein–Barr virus, human herpes virus 6, and herpes simplex virus 1 and 2, enterovirus, influenza virus A H1N1 and B and hepatitis C virus were negative | no | recovery |
| Sardari et al. | normal LV size with mildly reduced LVEF: 50%; T2-weighted oedema sequence with its post-analysis T2 ratio showed oedema/inflammation in the mid inferoseptal and inferior wall. Late gadolinium enhancement showed subepicardial fibrosis in the mid-inferior wall | not performed | no | NR |
| Warchoł et al. | LA enlargement and global left ventricular hypokinesia LVEF: 20%, T2-weighted sequence did not show myocardial oedema, late gadolinium enhancement with a large, patchy, and linear nonischemic pattern of fibrosis localized subepicardially and intramurally in the basal and mid cavity segments of the inferior and inferolateral wall and the apical segments of the inferior wall | not performed | NR | NR |
| Shahrami et al. | NR | not performed | a combination of cardiogenic and septic shock, respiratory arrest | death |
| Gaine et al. | biventricular dysfunction with an LVEF of 30%, STIR sequences showed biventricular oedema and reduced myocardial T1 | not performed | NR | recovery |
| Taouihar et al. | focal hypertrophy in the anteroseptal and inferior segment of the LV extended over approximately 62 mm, and in anteroinferior of the RV extended over 27 mm, in hyper signal T2, with an intense enhancement on the tardive injected sequences compared to the rest of the myocardium in favour of a myocarditis | not performed | NR | discharged on day 7 |
| Dahl et al.. | diffuse myocardial oedema | not performed | respiratory distress with oliguria and hypotension, facial nerve palsy after discharge | discharged 11 days after admission |
| Matsumura et al.. | high signal of T2-weighted black blood in anterior, interventricular septal, and posterolateral walls of the LV, late gadolinium enhancement in the posterolateral wall of the LV | infiltration of interstitial mononuclear cells Infiltrating cells included: T-cells and macrophages, more CD4-positive cells than CD8-positive cells, and few B-cells. RT-PCR SARS-CoV-2 negative in the myocardium. Electron microscopy showed inflammatory cell infiltration and myocyte damage compatible with myocarditis. Viral particles were not found in the high-power fields. Tests for antibodies against adenovirus, coxsackie virus, echovirus, and parainfluenza virus were negative. | Ten days after admission, bilateral peripheral facial nerve palsy occurred; | discharged 24 days after admission |
| Praet et al.. | minimal pericardial effusion and contrast enhancement in pericardium but not in myocardium | Mononuclear infiltration of the myocardium, predominantly with T lymphocytes and macrophages, Myocardial biopsy shows mononuclear infiltration of the myocardium, with CD3-positive lymphocytes (arrow) and CD68-positive macrophages (arrow), without formation of granulomas | NR | recovered |
| Masiak et al. | NR | NR | Kikuchi-Fujimoto disease | discharged, at 7 months, physical impairment persists, and on echocardiography reduced LVEF: 53% with impaired global systolic heart function is still present |
| Noori et al. | mild to moderately reduced LVEF: 38%; moderate hypokinesis of midventricular inferolateral wall; oedema/inflammation of epicardium and epicardial scar of basal anteroseptal and anterior wall and midventricular anterolateral, inferolateral and inferior wall | not performed | no | discharged |
| Okor et al. | NR | NR | acute on chronic respiratory failure | death |
| Bulbul et al. | NR | NR | cardiogenic shock secondary to severe myocarditis | recovery |
| Khatri et al. | NR | NR | gastrointestinal bleeding and multiorgan failure | death |
| Nicol et al. | normal left ventricular size (LVEDV index: 75 mL/m2) and mild systolic dysfunction (LVEF: 45%) with global hypokinesia, presence of myocardial inflammation was confirmed by T2 mapping (global T2 relaxation times: 62 ms; centre-specific cut-off value for acute myocarditis: ≥55 ms), late gadolinium enhancement imaging (inversion time by using the Look-Locker technique: 280 ms) showed focal lateral subepicardial enhancement with prolonged T1 relaxation times (global T1 relaxation times: 1160 ms; centre-specific cut-off value for acute myocarditis: ≥1000 ms), small pericardial effusion, | multiple foci of lymphocytes in a diffuse inflammatory and oedematous background. | NR | recovery |
| Hudowenz et al. | late gadolinium enhancement of the entire LV myocardium with intracardial thrombi, T1 and T2 times were markedly prolonged, reflecting acute oedema following myocardial inflammation | active lymphocytic myocarditis | acute renal injury with microhaematuria | recovery |
| Jacobs et al. | NR | Slightly diffuse interstitial mononuclear inflammatory infiltrates, dominated by lymphocytes. No thrombotic events were observed in the microcirculation of the heart. In the patchy areas, the lymphocytes’ interlocked’ the myocytes, resulting in myocyte degeneration and necrosis (piecemeal necrosis). Intermingled with lymphocytes, only a few individual polymorphous neutrophils were found in the affected areas. Signs of inflammation were present in both the epicardium and the myocardium. | cardiogenic shock, ARDS | death |
| Hussain et al. | NR | not performed | ARDS | NR |
| Rehman et al. | not performed | not performed | no | NR |
| Monmeneu et al. | Right pulmonary condensation along with associated pleural effusion, LV of normal volume with concentric hypertrophy and mild depressed systolic function (LVEF: 53%) secondary to diffuse hypokinesia, global longitudinal strain was decreased. Myocardial oedema with a predominant subepicardial pattern was seen in the lateral, anterior, inferior, and apical segments on T2 short tau inversion recovery and T2 mapping sequences, determining wall pseudo-hypertrophy. Pericardial oedema without associated effusion was also observed. Native T1 and extracellular volume were increased in relation to the acute inflammatory process. Late gadolinium sequences showed extensive, patchy intramyocardial/subepicardial enhancement affecting the entire lateral, anterior, inferior, and apical septal walls and the pericardium. | NR | no | recovery |
| Tavazzi et al. | NR | Low-grade interstitial and endocardial inflammation. Large, vacuolated, CD-68-positive macrophages were seen with immunelight microscopy. The ultrastructural study demonstrated single or small groups of viral particles with the morphology and size of coronaviruses. The viral particles were observed in cytopathic, structurally damaged interstitial cells that demonstrated loss of cytoplasmic membrane integrity. Cardiac myocytes showed non-specific features of local myofibrillar lysis and lipid droplets. Interstitial fibrosis was minimal, focal, and mainly perivascular. | cardiogenic shock, sepsis | death |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urban, S.; Fułek, M.; Błaziak, M.; Iwanek, G.; Jura, M.; Fułek, K.; Guzik, M.; Garus, M.; Gajewski, P.; Lewandowski, Ł.; et al. COVID-19 Related Myocarditis in Adults: A Systematic Review of Case Reports. J. Clin. Med. 2022, 11, 5519. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11195519
Urban S, Fułek M, Błaziak M, Iwanek G, Jura M, Fułek K, Guzik M, Garus M, Gajewski P, Lewandowski Ł, et al. COVID-19 Related Myocarditis in Adults: A Systematic Review of Case Reports. Journal of Clinical Medicine. 2022; 11(19):5519. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11195519
Chicago/Turabian StyleUrban, Szymon, Michał Fułek, Mikołaj Błaziak, Gracjan Iwanek, Maksym Jura, Katarzyna Fułek, Mateusz Guzik, Mateusz Garus, Piotr Gajewski, Łukasz Lewandowski, and et al. 2022. "COVID-19 Related Myocarditis in Adults: A Systematic Review of Case Reports" Journal of Clinical Medicine 11, no. 19: 5519. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11195519