
Extrahepatic Manifestations of Chronic HBV Infection and the Role of Antiviral Therapy
 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
1.1. HBV-Related Cryoglobulinemia Vasculitis
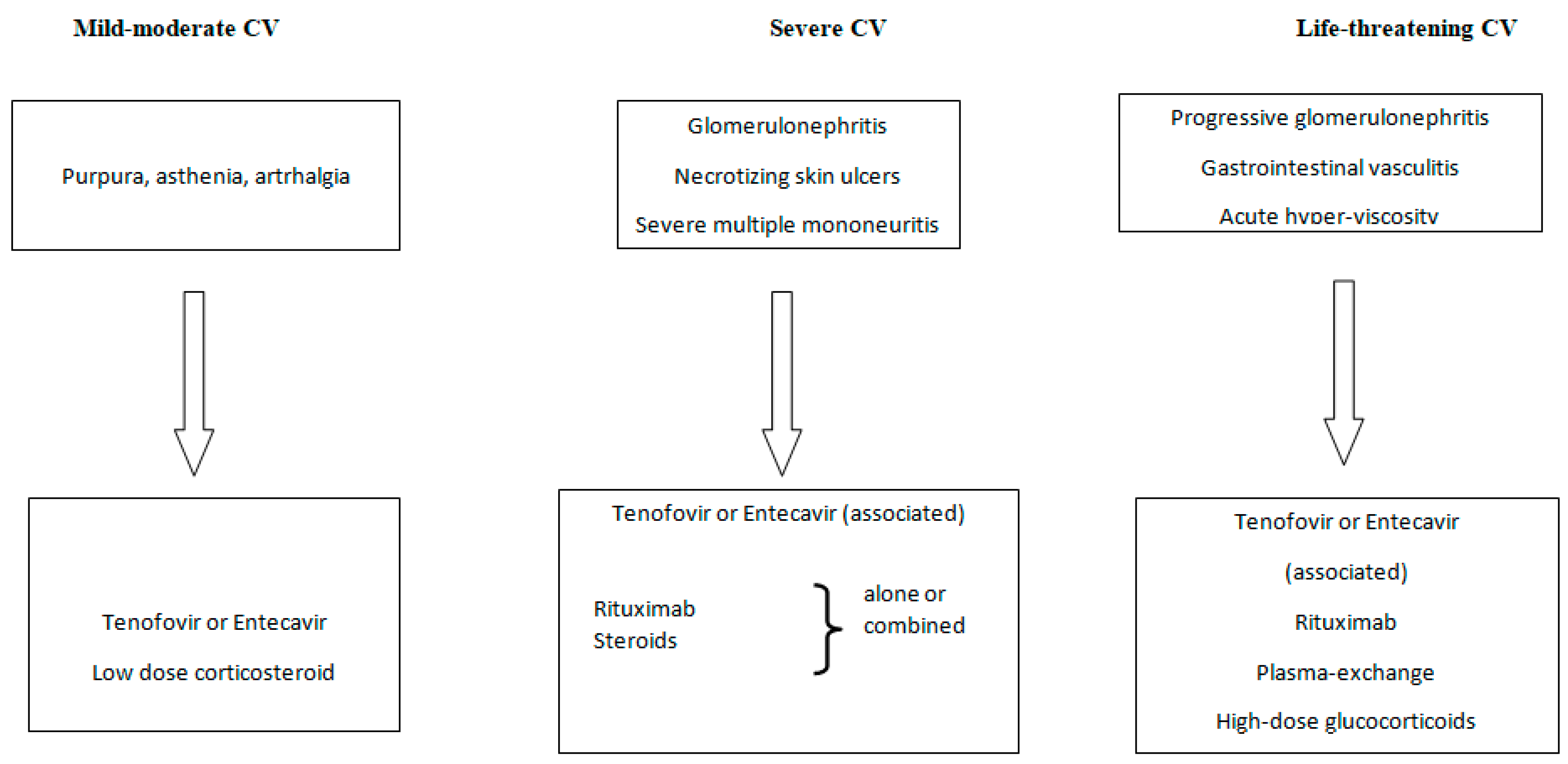
1.2. Treatment of HBV-Related Cryoglobulinemic Vasculitis
- Antiviral therapy (oral nucleot(s)ide analogues);
- B-cell depleting therapy (Rituximab);
- Glucocorticosteroids;
- The removal of circulating cryoglobulins by plasma exchange;
- Nonsteroids anti-inflammatory agents.
2. HBV and Rheumatologic Manifestations
2.1. Serum Sickness-like Syndrome
2.2. Non-Rheumatoid Arthritis
2.3. Polyarteritis Nodosa (PAN)
2.4. Laboratory Rheumatologic Abnormalities
3. Renal Manifestations of Hepatitis B Virus Infection
3.1. HBV-Related Membranous Nephropathy (MN)
3.2. HBV-Related Membranoproliferative Glomerulonephritis (MPGN)
3.3. General Principles of Therapy of HBV-Related Nephropathies
4. HBV and Lymphoma
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Ganem, D.; Prince, A.M. Hepatitis B virus infection-natural history and clinical consequences. N. Engl. J. Med. 2004, 350, 1118–1129. [Google Scholar] [CrossRef] [Green Version]
- Cacoub, P.; Terrier, B. Hepatitis B-related autoimmune manifestations. Rheum. Dis. Clin. N. Am. 2009, 35, 125–137. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [CrossRef] [PubMed] [Green Version]
- Mazzaro, C.; Dal Maso, L.; Mauro, E.; Visentini, M.; Tonizzo, M.; Gattei, V.; Andreone, P.; Pozzato, G. Hepatitis C virus- related cryoglobulinemic vasculitis: A review of the role of the new direct antiviral agents (DAAs) therapy. Autoimmun. Rev. 2020, 19, 102589. [Google Scholar] [CrossRef] [PubMed]
- Boglione, L.; Cusato, J.; Allegra, S.; Esposito, I.; Patti, F.; Cariti, G.; Di Perri, G.; D’Avolio, A. Role of IL28-B polymorphisms in the treatment of chronic hepatitis B HBeAg-negative patients with peginterferon. Antivir. Res. 2014, 102, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Terrier, B.; Marie, I.; Lacraz, A.; Belenotti, P.; Bonnet, F.; Chiche, L.; Graffin, B.; Hot, A.; Kahn, J.E.; Michel, C.; et al. Non HCV-related infectious cryoglobulinemia vasculitis: Results from the French nationwide CryoVas survey and systematic review of the literature. J. Autoimmun. 2015, 65, 74–81. [Google Scholar] [CrossRef]
- Mazzaro, C.; Dal Maso, L.; Urraro, T.; Mauro, E.; Castelnovo, L.; Casarin, P.; Monti, G.; Gattei, V.; Zignego, A.L.; Pozzato, G. Hepatitis B virus related cryoglobulinemic vasculitis: A multicentre open label study from the Gruppo Italiano di Studio delle Crioglobulinemie—GISC. Dig. Liver Dis. 2016, 48, 780–784. [Google Scholar] [CrossRef]
- Gao, Y.; Li, Y.; Meng, Q.; Zhang, Z.; Zhao, P.; Shang, Q.; Li, Y.; Su, M.; Li, T.; Liu, X.; et al. Serum hepatitis B virus DNA, RNA, and HBsAg: Which correlated better with intrahepatic covalently closed circular DNA before and after nucleos (t) ide analogue treatment? J. Clin. Microbiol. 2017, 55, 2972–2982. [Google Scholar] [CrossRef] [Green Version]
- Mazzaro, C.; Maso, L.D.; Gragnani, L.; Visentini, M.; Saccardo, F.; Filippini, D.; Andreone, P.; Zignego, A.L.; Gattei, V.; Monti, G.; et al. Hepatitis B Virus-Related Cryoglobulinemic Vasculitis: Review of the Literature and Long-Term Follow-Up Analysis of 18 Patients Treated with Nucleos(t)ide Analogues from the Italian Study Group of Cryoglobulinemia (GISC). Viruses 2021, 13, 1032. [Google Scholar] [CrossRef]
- Brouet, J.C.; Clauvel, J.P.; Danon, F.; Klein, M.; Seligmann, M. Biologic and clinical significance of cryoglobulins. A report of 86 cases. Am. J. Med. 1974, 57, 775–788. [Google Scholar] [CrossRef]
- Cacoub, P.; Comarmond, C.; Domont, F.; Savey, L.; Saadoun, D. Cryoglobulinemia Vasculitis. Am. J. Med. 2015, 128, 950–955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferri, C.; Zignego, A.L.; Giuggioli, D.; Sebastiani, M.; Cazzato, M.; Antonelli, A.; La Civita, L.; Fadda, P.; Longombardo, G.; Pileri, S. HCV and cryoglobulinemic vasculitis. Clevel. Clin. J. Med. 2002, 69 (Suppl. S2), SII20–SII23. [Google Scholar] [CrossRef] [PubMed]
- Roccatello, D.; Saadoun, D.; Ramos-Casals, M.; Tzioufas, A.G.; Fervenza, F.C.; Cacoub, P.; Zignego, A.L.; Ferri, C. Cryoglobulinaemia. Nat. Rev. Dis. Primers 2018, 4, 11. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, M.; Franklin, E.C. Cryoglobulinemia—A study of twenty-nine patients. I. IgG and IgM cryoglobulins and factors affecting cryoprecipitability. Am. J. Med. 1966, 40, 828–836. [Google Scholar] [CrossRef]
- Cacoub, P.; Saadoun, D. Extrahepatic Manifestations of Chronic HCV Infection. N. Engl. J. Med. 2021, 384, 1038–1052. [Google Scholar] [CrossRef]
- Levo, Y.; Gorevic, P.D.; Kassab, H.J.; Tobias, H.; Franklin, E.C. Liver involvement in the syndrome of mixed cryoglobulinemia. Ann. Intern. Med. 1977, 87, 287–292. [Google Scholar] [CrossRef]
- Monti, G.; Galli, M.; Invernizzi, F.; Pioltelli, P.; Saccardo, F.; Monteverde, A.; Pietrogrande, M.; Renoldi, P.; Bombardieri, S.; Bordin, G.; et al. Cryoglobulinaemias: A multi-centre study of the early clinical and laboratory manifestations of primary and secondary disease. GISC. Italian Group for the Study of Cryoglobulinaemias. QJM 1995, 88, 115–126. [Google Scholar]
- Ferri, C.; Sebastiani, M.; Giuggioli, D.; Cazzato, M.; Longombardo, G.; Antonelli, A.; Puccini, R.; Michelassi, C.; Zignego, A.L. Mixed cryoglobulinemia: Demographic, clinical, and serologic features and survival in 231 patients. Semin. Arthritis Rheum. 2004, 33, 355–374. [Google Scholar] [CrossRef]
- Mazzaro, C.; Maso, L.D.; Mauro, E.; Gattei, V.; Ghersetti, M.; Bulian, P.; Moratelli, G.; Grassi, G.; Zorat, F.; Pozzato, G. Survival and Prognostic Factors in Mixed Cryoglobulinemia: Data from 246 Cases. Diseases 2018, 6, 35. [Google Scholar] [CrossRef] [Green Version]
- Li, S.J.; Xu, S.T.; Chen, H.P.; Zhang, M.C.; Xu, F.; Cheng, S.Q.; Liu, Z.H. Clinical and morphologic spectrum of renal involvement in patients with HBV-associated cryoglobulinaemia. Nephrology 2017, 22, 449–455. [Google Scholar] [CrossRef]
- Roccatello, D.; Baldovino, S.; Rossi, D.; Giachino, O.; Mansouri, M.; Naretto, C.; Di Simone, D.; Francica, S.; Cavallo, R.; Alpa, M.; et al. Rituximab as a therapeutic tool in severe mixed cryoglobulinemia. Clin. Rev. Allergy Immunol. 2008, 34, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Roccatello, D.; Fenoglio, R.; Sciascia, S. The dilemma of treating hepatitis C virus-associated cryoglobulinemia. Curr. Opin. Rheumatol. 2019, 31, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Lohr, H.; Goergen, B.; Weber, W.; Godderz, W.; Meyer zum Buschenfelde, K.H.; Gerken, G. Mixed cryoglobulinemia type II in chronic hepatitis B associated with HBe-minus HBV mutant: Cellular immune reactions and response to interferon treatment. J. Med. Virol. 1994, 44, 330–335. [Google Scholar] [CrossRef] [PubMed]
- La Civita, L.; Zignego, A.L.; Lombardini, F.; Monti, M.; Longombardo, G.; Pasero, G.; Ferri, C. Exacerbation of peripheral neuropathy during alpha-interferon therapy in a patient with mixed cryoglobulinemia and hepatitis B virus infection. J. Rheumatol. 1996, 23, 1641–1643. [Google Scholar]
- Galli, M.; Monti, G.; Marson, P.; Scaini, P.; Pietrogrande, M.; Candela, M.; Castelnovo, L.; Faggioli, P.; Novati, P.; Zani, R.; et al. Recommendations for managing the manifestations of severe and life-threatening mixed cryoglobulinemia syndrome. Autoimmun. Rev. 2019, 18, 778–785. [Google Scholar] [CrossRef] [PubMed]
- Cacoub, P.; Saadoun, D.; Bourliere, M.; Khiri, H.; Martineau, A.; Benhamou, Y.; Varastet, M.; Pol, S.; Thibault, V.; Rotily, M.; et al. Hepatitis B virus genotypes and extrahepatic manifestations. J. Hepatol. 2005, 43, 764–770. [Google Scholar] [CrossRef]
- Kappus, M.R.; Sterling, R.K. Extrahepatic manifestations of acute hepatitis B virus infection. Gastroenterol. Hepatol. 2013, 9, 123–126. [Google Scholar]
- Satsangi, S.; Gupta, N. Rheumatologic Manifestations of Viral Hepatitis B and C. J. Hepat. 2015, 1, 3. [Google Scholar]
- Han, S.H. Extrahepatic manifestations of chronic hepatitis B. Clin. Liver Dis. 2004, 8, 403–418. [Google Scholar] [CrossRef]
- Wands, J.R.; Alpert, E.; Isselbacher, K.J. Arthritis associated with chronic active hepatitis: Complement activation and characterization of circulating immune complexes. Gastroenterology 1975, 69, 1286–1291. [Google Scholar] [CrossRef]
- Lim, M.K.; Sheen, D.H.; Lee, Y.J.; Mun, Y.R.; Park, M.; Shim, S.C. Anti-cyclic citrullinated peptide antibodies distinguish hepatitis B virus (HBV)-associated arthropathy from concomitant rheumatoid arthritis in patients with chronic HBV infection. J. Rheumatol. 2009, 36, 712–716. [Google Scholar] [CrossRef] [PubMed]
- Guillevin, L.; Lhote, F.; Cohen, P.; Sauvaget, F.; Jarrousse, B.; Lortholary, O.; Noel, L.H.; Trepo, C. Polyarteritis nodosa related to hepatitis B virus. A prospective study with long-term observation of 41 patients. Medicine 1995, 74, 238–253. [Google Scholar] [CrossRef] [PubMed]
- Pagnoux, C.; Seror, R.; Henegar, C.; Mahr, A.; Cohen, P.; Le Guern, V.; Bienvenu, B.; Mouthon, L.; Guillevin, L.; French Vasculitis Study, G. Clinical features and outcomes in 348 patients with polyarteritis nodosa: A systematic retrospective study of patients diagnosed between 1963 and 2005 and entered into the French Vasculitis Study Group Database. Arthritis Rheum. 2010, 62, 616–626. [Google Scholar] [CrossRef] [PubMed]
- Hocevar, A.; Tomsic, M.; Perdan Pirkmajer, K. Clinical Approach to Diagnosis and Therapy of Polyarteritis Nodosa. Curr. Rheumatol. Rep. 2021, 23, 14. [Google Scholar] [CrossRef] [PubMed]
- Michalak, T. Immune complexes of hepatitis B surface antigen in the pathogenesis of periarteritis nodosa. A study of seven necropsy cases. Am. J. Pathol. 1978, 90, 619–632. [Google Scholar] [PubMed]
- Fye, K.H.; Becker, M.J.; Theofilopoulos, A.N.; Moutsopoulos, H.; Feldman, J.L.; Talal, N. Immune complexes in hepatitis B antigen-associated periarteritis nodosa. Detection by antibody-dependent cell-mediated cytotoxicity and the Raji cell assay. Am. J. Med. 1977, 62, 783–791. [Google Scholar] [CrossRef]
- Guillevin, L.; Mahr, A.; Callard, P.; Godmer, P.; Pagnoux, C.; Leray, E.; Cohen, P.; French Vasculitis Study, G. Hepatitis B virus-associated polyarteritis nodosa: Clinical characteristics, outcome, and impact of treatment in 115 patients. Medicine 2005, 84, 313–322. [Google Scholar] [CrossRef]
- Guillevin, L.; Lhote, F.; Sauvaget, F.; Deblois, P.; Rossi, F.; Levallois, D.; Pourrat, J.; Christoforov, B.; Trepo, C. Treatment of polyarteritis nodosa related to hepatitis B virus with interferon-alpha and plasma exchanges. Ann. Rheum. Dis. 1994, 53, 334–337. [Google Scholar] [CrossRef] [Green Version]
- Guillevin, L.; Mahr, A.; Cohen, P.; Larroche, C.; Queyrel, V.; Loustaud-Ratti, V.; Imbert, B.; Hausfater, P.; Roudier, J.; Bielefeld, P.; et al. Short-term corticosteroids then lamivudine and plasma exchanges to treat hepatitis B virus-related polyarteritis nodosa. Arthritis Rheum. 2004, 51, 482–487. [Google Scholar] [CrossRef]
- Choi, S.T.; Lee, H.W.; Song, J.S.; Lee, S.K.; Park, Y.B. Analysis of rheumatoid factor according to various hepatitis B virus infectious statuses. Clin. Exp. Rheumatol. 2014, 32, 168–173. [Google Scholar]
- Li, B.A.; Liu, J.; Hou, J.; Tang, J.; Zhang, J.; Xu, J.; Song, Y.J.; Liu, A.X.; Zhao, J.; Guo, J.X.; et al. Autoantibodies in Chinese patients with chronic hepatitis B: Prevalence and clinical associations. World J. Gastroenterol. 2015, 21, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Elwood, J.M.; Ameratunga, R. Autoimmune diseases after hepatitis B immunization in adults: Literature review and meta-analysis, with reference to ‘autoimmune/autoinflammatory syndrome induced by adjuvants’ (ASIA). Vaccine 2018, 36, 5796–5802. [Google Scholar] [CrossRef]
- Zampino, R.; Boemio, A.; Sagnelli, C.; Alessio, L.; Adinolfi, L.E.; Sagnelli, E.; Coppola, N. Hepatitis B virus burden in developing countries. World J. Gastroenterol. 2015, 21, 11941–11953. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Quigg, R.J. Glomerular Diseases Associated with Hepatitis B and C. Adv. Chronic. Kidney Dis. 2015, 22, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Kupin, W.L. Viral-Associated GN: Hepatitis B and Other Viral Infections. Clin. J. Am. Soc. Nephrol. 2017, 12, 1529–1533. [Google Scholar] [CrossRef] [Green Version]
- Lai, K.N.; Lai, F.M. Clinical features and the natural course of hepatitis B virus-related glomerulopathy in adults. Kidney Int. Suppl. 1991, 35, S40–S45. [Google Scholar]
- Basnayake, S.K.; Easterbrook, P.J. Wide variation in estimates of global prevalence and burden of chronic hepatitis B and C infection cited in published literature. J. Viral Hepat. 2016, 23, 545–559. [Google Scholar] [CrossRef] [Green Version]
- Wang, R.; Wu, Y.; Zheng, B.; Zhang, X.; An, D.; Guo, N.; Wang, J.; Guo, Y.; Tang, L. Clinicopathological characteristics and prognosis of hepatitis B associated membranous nephropathy and idiopathic membranous nephropathy complicated with hepatitis B virus infection. Sci. Rep. 2021, 11, 18407. [Google Scholar] [CrossRef]
- Xie, Q.; Li, Y.; Xue, J.; Xiong, Z.; Wang, L.; Sun, Z.; Ren, Y.; Zhu, X.; Hao, C.M. Renal phospholipase A2 receptor in hepatitis B virus-associated membranous nephropathy. Am. J. Nephrol. 2015, 41, 345–353. [Google Scholar] [CrossRef]
- Li, P.; Wei, R.B.; Tang, L.; Wu, J.; Zhang, X.G.; Chen, X.M. Clinical and pathological analysis of hepatitis B virus-related membranous nephropathy and idiopathic membranous nephropathy. Clin. Nephrol. 2012, 78, 456–464. [Google Scholar] [CrossRef]
- Li, C.; Li, H.; Su, W.; Wen, Y.B.; Ye, W.; Ye, W.L.; Cai, J.F.; Qin, X.Z.; Li, X.M.; Li, X.W. Clinicopathological study of mixed cryoglobulinemic glomerulonephritis secondary to hepatitis B virus infection. BMC Nephrol. 2020, 21, 395. [Google Scholar] [CrossRef] [PubMed]
- Trepo, C.; Guillevin, L. Polyarteritis nodosa and extrahepatic manifestations of HBV infection: The case against autoimmune intervention in pathogenesis. J. Autoimmun. 2001, 16, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Mouthon, L. [Periarteritis nodosa induced by hepatitis B virus]. Pathol. Biol. 1999, 47, 237–244. [Google Scholar] [PubMed]
- Rovin, B.H.; Caster, D.J.; Cattran, D.C.; Gibson, K.L.; Hogan, J.J.; Moeller, M.J.; Roccatello, D.; Cheung, M.; Wheeler, D.C.; Winkelmayer, W.C.; et al. Management and treatment of glomerular diseases (part 2): Conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2019, 95, 281–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elewa, U.; Sandri, A.M.; Kim, W.R.; Fervenza, F.C. Treatment of hepatitis B virus-associated nephropathy. Nephron. Clin. Pract. 2011, 119, c41–c49; discussion c49. [Google Scholar] [CrossRef]
- Fu, B.; Ji, Y.; Hu, S.; Ren, T.; Bhuva, M.S.; Li, G.; Yang, H. Efficacy and safety of anti-viral therapy for Hepatitis B virus-associated glomerulonephritis: A meta-analysis. PLoS ONE 2020, 15, e0227532. [Google Scholar] [CrossRef]
- Ott, J.J.; Stevens, G.A.; Groeger, J.; Wiersma, S.T. Global epidemiology of hepatitis B virus infection: New estimates of age-specific HBsAg seroprevalence and endemicity. Vaccine 2012, 30, 2212–2219. [Google Scholar] [CrossRef] [Green Version]
- Galun, E.; Ilan, Y.; Livni, N.; Ketzinel, M.; Nahor, O.; Pizov, G.; Nagler, A.; Eid, A.; Rivkind, A.; Laster, M.; et al. Hepatitis B virus infection associated with hematopoietic tumors. Am. J. Pathol. 1994, 145, 1001–1007. [Google Scholar]
- Kim, J.H.; Bang, Y.J.; Park, B.J.; Yoo, T.; Kim, C.W.; Kim, T.Y.; Heo, D.S.; Lee, H.S.; Kim, N.K. Hepatitis B virus infection and B-cell non-Hodgkin’s lymphoma in a hepatitis B endemic area: A case-control study. Jpn. J. Cancer Res. 2002, 93, 471–477. [Google Scholar] [CrossRef]
- Marcucci, F.; Mele, A.; Spada, E.; Candido, A.; Bianco, E.; Pulsoni, A.; Chionne, P.; Madonna, E.; Cotichini, R.; Barbui, A.; et al. High prevalence of hepatitis B virus infection in B-cell non-Hodgkin’s lymphoma. Haematologica 2006, 91, 554–557. [Google Scholar]
- Engels, E.A.; Cho, E.R.; Jee, S.H. Hepatitis B virus infection and risk of non-Hodgkin lymphoma in South Korea: A cohort study. Lancet Oncol. 2010, 11, 827–834. [Google Scholar] [CrossRef] [Green Version]
- Brechot, C.; Thiers, V.; Kremsdorf, D.; Nalpas, B.; Pol, S.; Paterlini-Brechot, P. Persistent hepatitis B virus infection in subjects without hepatitis B surface antigen: Clinically significant or purely “occult”? Hepatology 2001, 34, 194–203. [Google Scholar] [CrossRef]
- Chen, M.H.; Hsiao, L.T.; Chiou, T.J.; Liu, J.H.; Gau, J.P.; Teng, H.W.; Wang, W.S.; Chao, T.C.; Yen, C.C.; Chen, P.M. High prevalence of occult hepatitis B virus infection in patients with B cell non-Hodgkin’s lymphoma. Ann. Hematol. 2008, 87, 475–480. [Google Scholar] [CrossRef] [PubMed]
- Rossi, D.; Sala, L.; Minisini, R.; Fabris, C.; Falleti, E.; Cerri, M.; Burlone, M.E.; Toniutto, P.; Gaidano, G.; Pirisi, M. Occult hepatitis B virus infection of peripheral blood mononuclear cells among treatment-naive patients with chronic lymphocytic leukemia. Leuk. Lymphoma 2009, 50, 604–611. [Google Scholar] [CrossRef] [PubMed]
- Marcucci, F.; Mele, A. Hepatitis viruses and non-Hodgkin lymphoma: Epidemiology, mechanisms of tumorigenesis, and therapeutic opportunities. Blood 2011, 117, 1792–1798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franceschi, S.; Lise, M.; Trepo, C.; Berthillon, P.; Chuang, S.C.; Nieters, A.; Travis, R.C.; Vermeulen, R.; Overvad, K.; Tjonneland, A.; et al. Infection with hepatitis B and C viruses and risk of lymphoid malignancies in the European Prospective Investigation into Cancer and Nutrition (EPIC). Cancer Epidemiol. Biomark. Prev. 2011, 20, 208–214. [Google Scholar] [CrossRef] [Green Version]
- Andersen, E.S.; Omland, L.H.; Jepsen, P.; Krarup, H.; Christensen, P.B.; Obel, N.; Weis, N.; Study, D.C. Risk of all-type cancer, hepatocellular carcinoma, non-Hodgkin lymphoma and pancreatic cancer in patients infected with hepatitis B virus. J. Viral Hepat. 2015, 22, 828–834. [Google Scholar] [CrossRef]
- Taborelli, M.; Polesel, J.; Montella, M.; Libra, M.; Tedeschi, R.; Battiston, M.; Spina, M.; Di Raimondo, F.; Pinto, A.; Crispo, A.; et al. Hepatitis B and C viruses and risk of non-Hodgkin lymphoma: A case-control study in Italy. Infect. Agent. Cancer 2016, 11, 27. [Google Scholar] [CrossRef]
- Li, M.; Gan, Y.; Fan, C.; Yuan, H.; Zhang, X.; Shen, Y.; Wang, Q.; Meng, Z.; Xu, D.; Tu, H. Hepatitis B virus and risk of non-Hodgkin lymphoma: An updated meta-analysis of 58 studies. J. Viral Hepat. 2018, 25, 894–903. [Google Scholar] [CrossRef]
- Zhou, X.; Wuchter, P.; Egerer, G.; Kriegsmann, M.; Kommoss, F.K.F.; Witzens-Harig, M.; Kriegsmann, K. Serological hepatitis B virus (HBV) activity in patients with HBV infection and B-cell non-Hodgkin’s lymphoma. Eur. J. Haematol. 2020, 104, 469–475. [Google Scholar] [CrossRef]
- Tian, T.; Song, C.; Jiang, L.; Dai, J.; Lin, Y.; Xu, X.; Yu, C.; Ge, Z.; Ding, Y.; Wen, Y.; et al. Hepatitis B virus infection and the risk of cancer among the Chinese population. Int. J. Cancer 2020, 147, 3075–3084. [Google Scholar] [CrossRef] [PubMed]
- Lemaitre, M.; Brice, P.; Frigeni, M.; Hermine, O.; Arcaini, L.; Thieblemont, C.; Besson, C. Hepatitis B virus-associated B-cell non-Hodgkin lymphoma in non-endemic areas in Western Europe: Clinical characteristics and prognosis. J. Infect. 2020, 80, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Tsai, W.L.; Chung, R.T. Viral hepatocarcinogenesis. Oncogene 2010, 29, 2309–2324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gragnani, L.; Fognani, E.; Piluso, A.; Boldrini, B.; Urraro, T.; Fabbrizzi, A.; Stasi, C.; Ranieri, J.; Monti, M.; Arena, U.; et al. Long-term effect of HCV eradication in patients with mixed cryoglobulinemia: A prospective, controlled, open-label, cohort study. Hepatology 2015, 61, 1145–1153. [Google Scholar] [CrossRef]
- Koot, A.W.; Visscher, A.P.; Huits, R.M. Remission of splenic marginal zone lymphoma in a patient treated for hepatitis B: A case of HBV-associated lymphoma. Acta Clin. Belg. 2015, 70, 301–303. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.T.; Fei, G.; Quek, R.; Lim, L.C.; Lee, L.H.; Yap, S.P.; Loong, S.; Tao, M. The relationship of hepatitis B virus infection and non-Hodgkin’s lymphoma and its impact on clinical characteristics and prognosis. Eur. J. Haematol. 2007, 79, 132–137. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Reported Condition |
|---|
| Mixed cryoglobulinemia vasculitis |
| Serum sickness-like syndrome |
| Non-rheumatoid arthritis |
| Rheumatoid arthritis |
| Panarteritis nodosa |
| Glomerulopathies |
| Non-Hodgkin Lymphoma |
| Study, Year | Patients N | Antiviral Agent, Dose = Duration, Weeks (w), Month (m) | Other Treatment | Clinical Manifestation (N) | Cryoglobulinemic Vasculitis Response |
|---|---|---|---|---|---|
| Boglione et al. [5] | 7 | Telbivudine 600 mg/day: 7 (100%) = 48 w | Purpura: 3 (43) Peripheral neuropathy: 4 (57) Skin ulcer: 2 (29) Chronic hepatitis: 7 (100) | CR: Purpura: 3 (43) Peripheral neuropathy: 2 (50) NR: Peripheral neuropathy: 2 (50) Skin ulcer: 2 (100) | |
| Terrier et al. [6] | 3 | Lamivudine 100 mg/day: 1 (33) Entecavir 0.5 mg/day: 2 (67) | PE + CS + RTX: 1 (33) PE + CYC+ CS + RTX: 1 (33) | Purpura: 2 (67) Arthralgias: 2 (67) Glomerulonephritis: 3 (100) Chronic hepatitis: 3 (100) | CR: Purpura: 2 (100) Arthralgias: 2 (100) Glomerulonephritis: 1 (1) Glomerulonephritis (2) |
| Mazzaro et al. [7] | 7 | Entecavir (5) = 48 m Adefovir (1) = 48 m Lamivudine (1) = 48 m | CS alone (1) | Type II (7) Purpura (7) Arthralgias (7) Ulcer on the leg (1) Chronic hepatitis (6) Cirrhosis (1) | CR: Purpura (7) Arthralgias (5) Ulcer on the leg (1) NR: Arthralgias (2) |
| Li et al. [8] | 9 | Entecavir (7) = 16 m Lamivudine (2) = 12 m | CS alone (3) CS + CYC(1) CS + PE + RTX (1) CS + PS + MMF (1) R (9) | Purpura (4) Arthralgias (2) Per neuropathy (2) Gastrointestinal Vasculitis (2) Glomerulonephritis (9) | CR: Glomerulonephritis (2) Purpura (2), Arthralgias (2), Per neuropathy (2) PR: Glomerulonephrirtis (3) NR: Glomerulonephritis (4) (dialysis in 4 patients, 2 died) |
| Mazzaro et al. [9] | 18 | Entecavir: 11(78%) = 66 m Tenofovir: 6 (67%) = 67 m Lamivudine: 1 (5%) = 59 m | Peg-IFN alone: 3 (38%) CS associated Nas: 4 (22%) PE associated NAs: 4 (22%) RTX associated NAs: 2 (11%) | Purpura: 18 (100%) Arthralgias: 11 (61%) Ulcer on the leg: 3 (17%) Sjogren S.: 5 (28%) Peripheral neuropathy: 11 (61%) Chronic hepatitis: 4 (22%) Cirrhosis: 1 (6%) Glomerulonephritis: 1 (6%) NHL: 2 (11%) | RC: Purpura: 14 (78%) Arthralgias: 8 (73%) Ulcex: 2 (67%) Sjogren S.: 2 (40%) Peripheral neuropathy: 6 (55%) NR: Purpura: 2 (11%) Arthralgias: 3 (27%) Neuropathy: 5 (45%) Glomerulonephritis: 1 (100%) NHL: 2 (100%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazzaro, C.; Adinolfi, L.E.; Pozzato, G.; Nevola, R.; Zanier, A.; Serraino, D.; Andreone, P.; Fenoglio, R.; Sciascia, S.; Gattei, V.; et al. Extrahepatic Manifestations of Chronic HBV Infection and the Role of Antiviral Therapy. J. Clin. Med. 2022, 11, 6247. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11216247
Mazzaro C, Adinolfi LE, Pozzato G, Nevola R, Zanier A, Serraino D, Andreone P, Fenoglio R, Sciascia S, Gattei V, et al. Extrahepatic Manifestations of Chronic HBV Infection and the Role of Antiviral Therapy. Journal of Clinical Medicine. 2022; 11(21):6247. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11216247
Chicago/Turabian StyleMazzaro, Cesare, Luigi Elio Adinolfi, Gabriele Pozzato, Riccardo Nevola, Ada Zanier, Diego Serraino, Pietro Andreone, Roberta Fenoglio, Savino Sciascia, Valter Gattei, and et al. 2022. "Extrahepatic Manifestations of Chronic HBV Infection and the Role of Antiviral Therapy" Journal of Clinical Medicine 11, no. 21: 6247. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11216247