
Autonomous Robotic Surgery for Immediately Loaded Implant-Supported Maxillary Full-Arch Prosthesis: A Case Report

Abstract
:1. Introduction
2. Materials and Methods
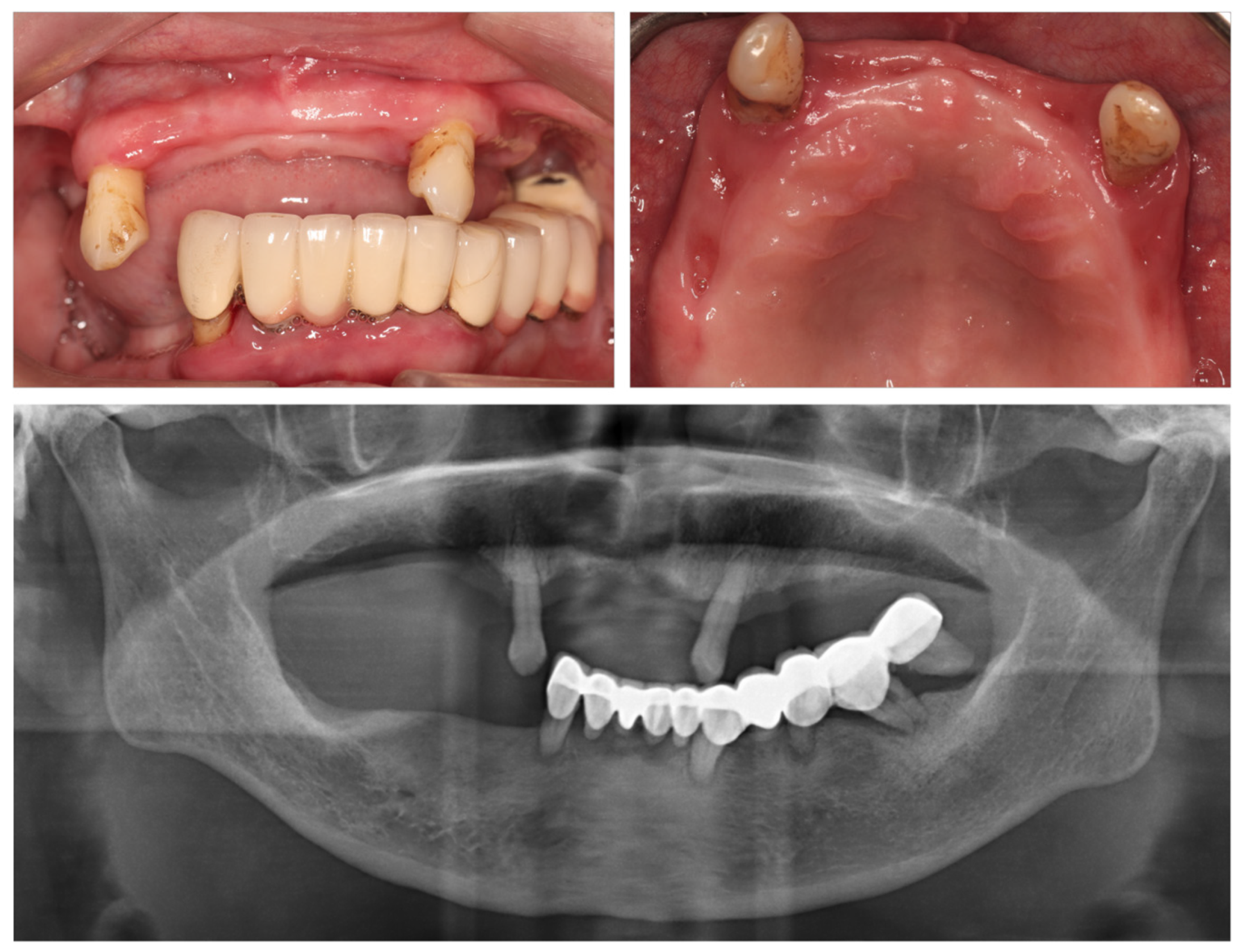
2.1. Initial Status and Treatment Plan
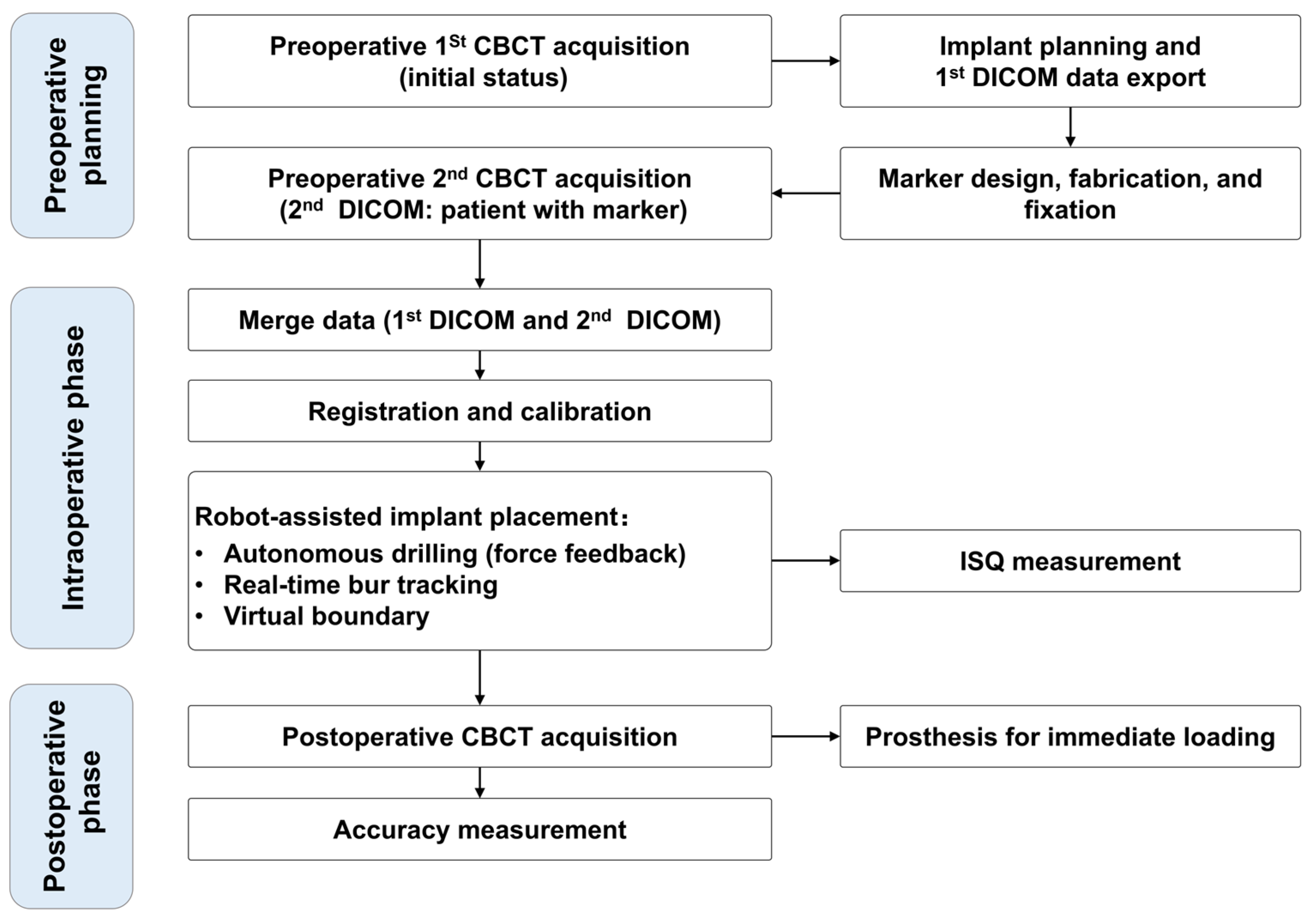
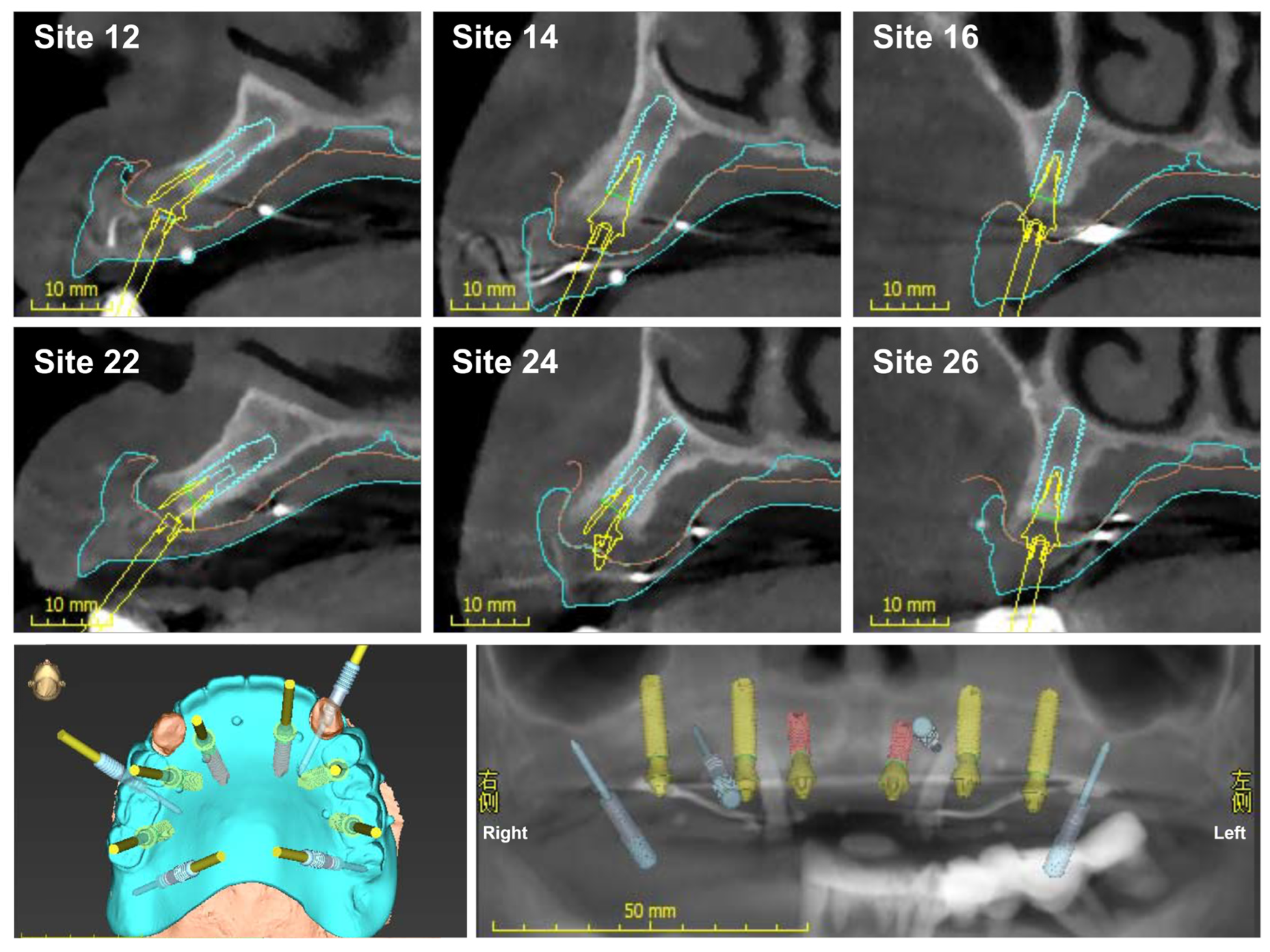
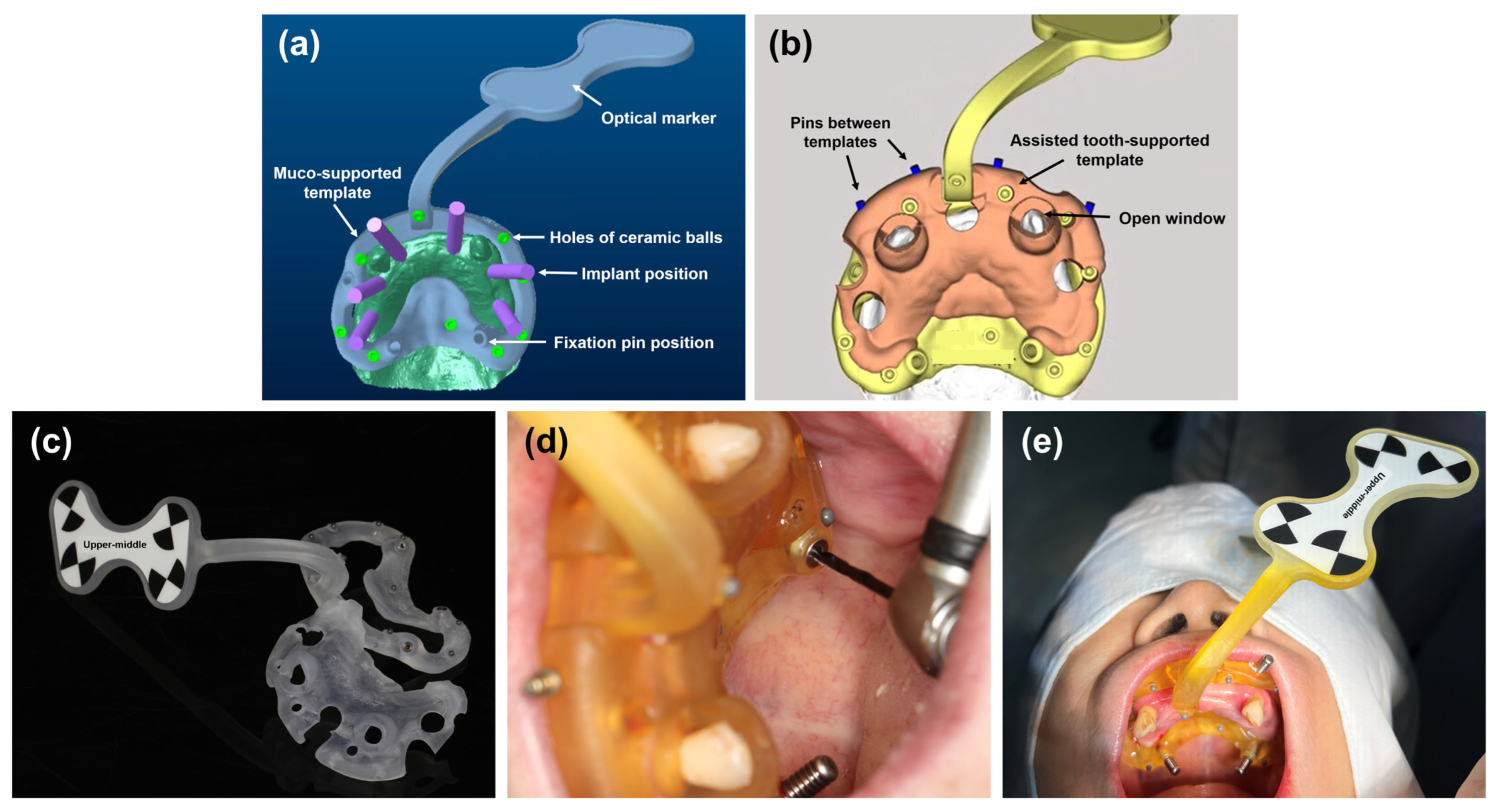
2.2. Preoperative Planning
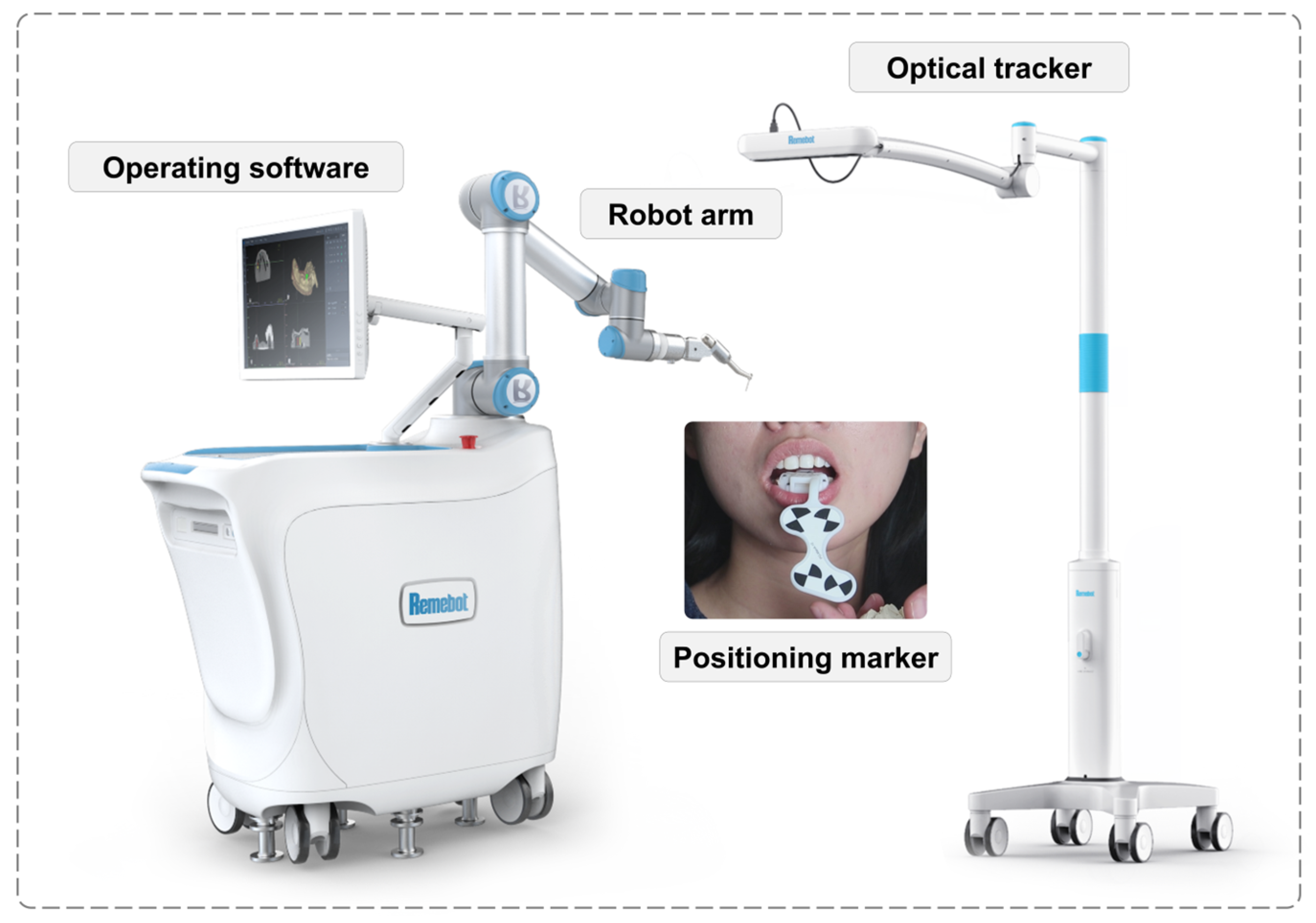
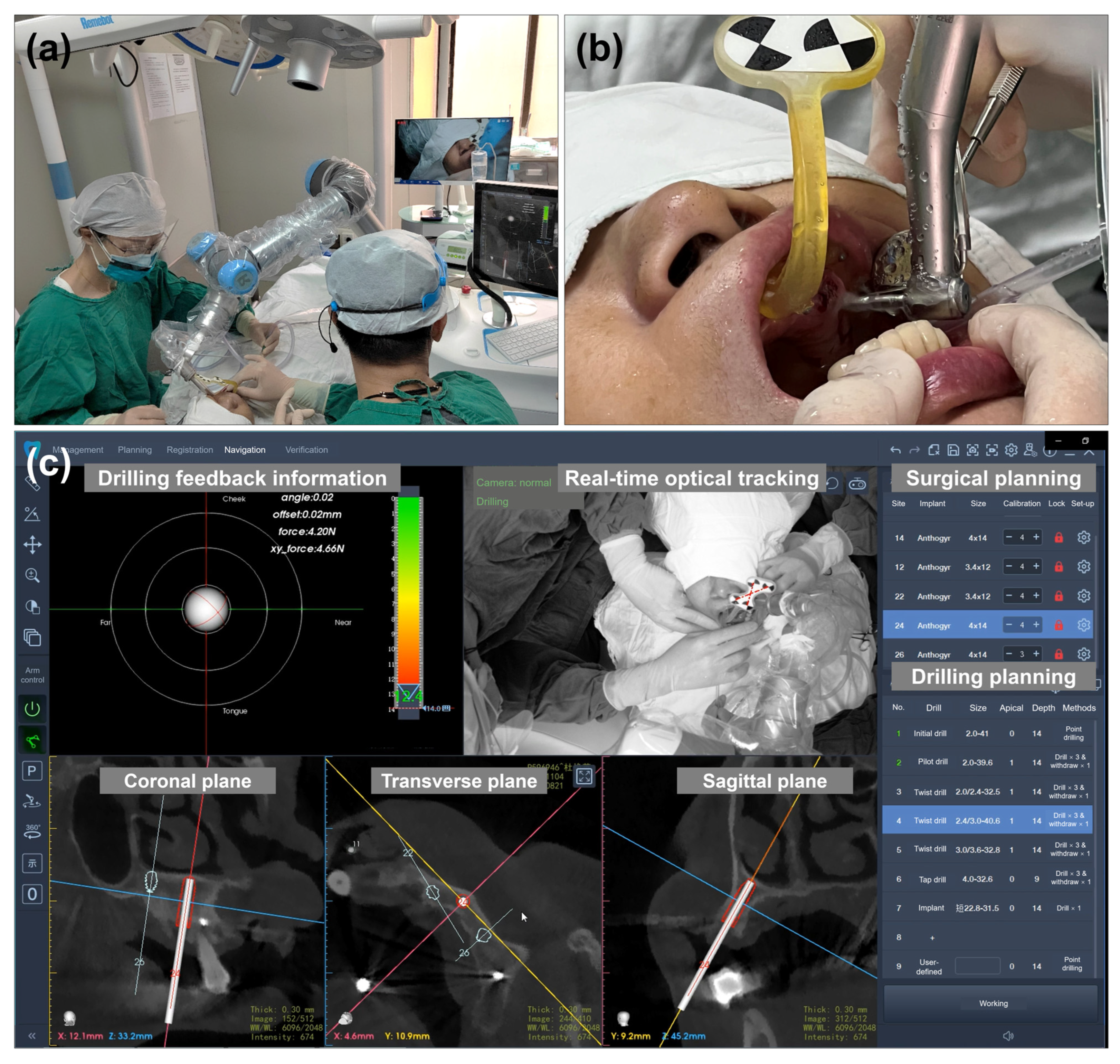
2.3. Intraoperative Phase
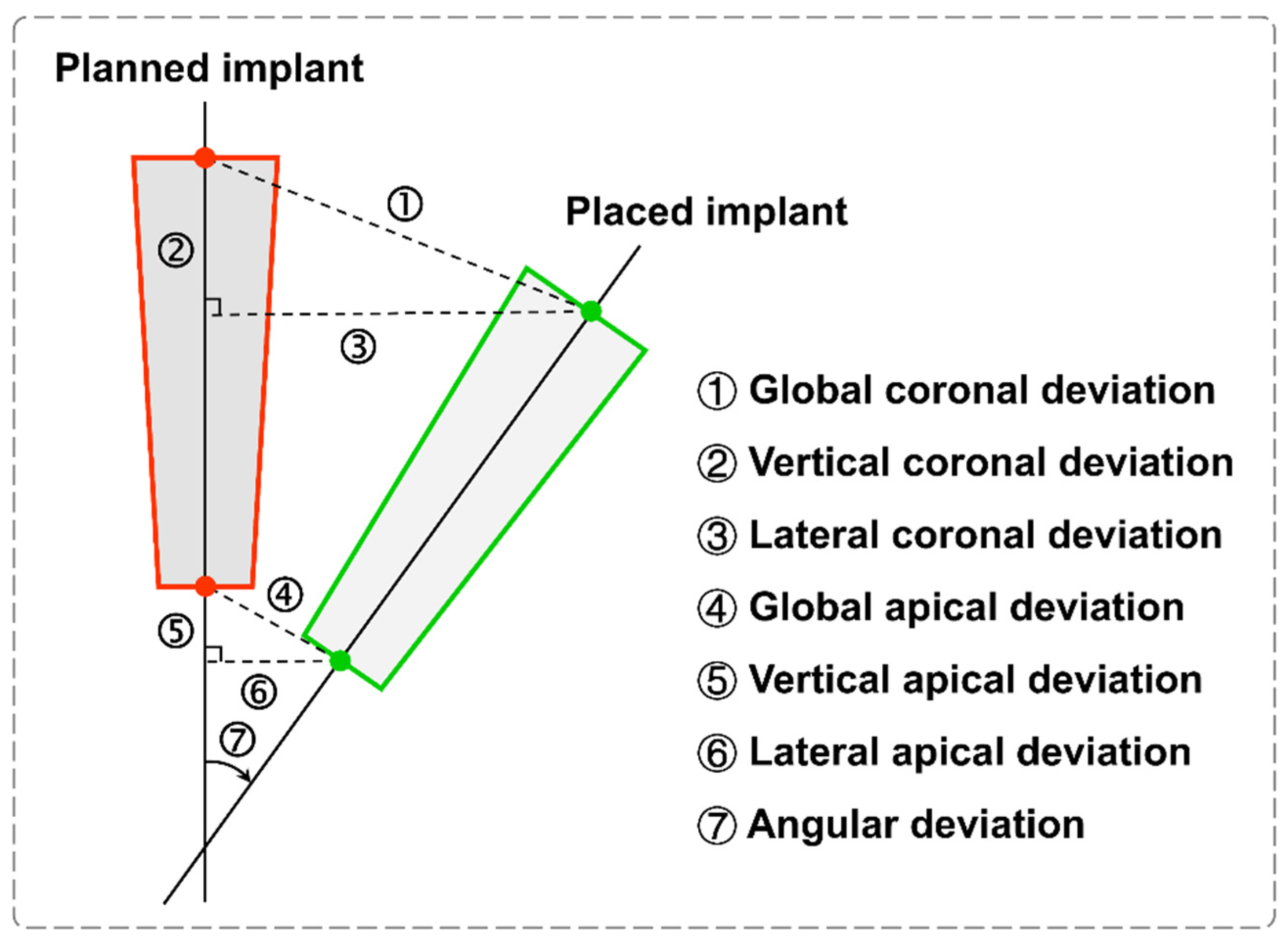
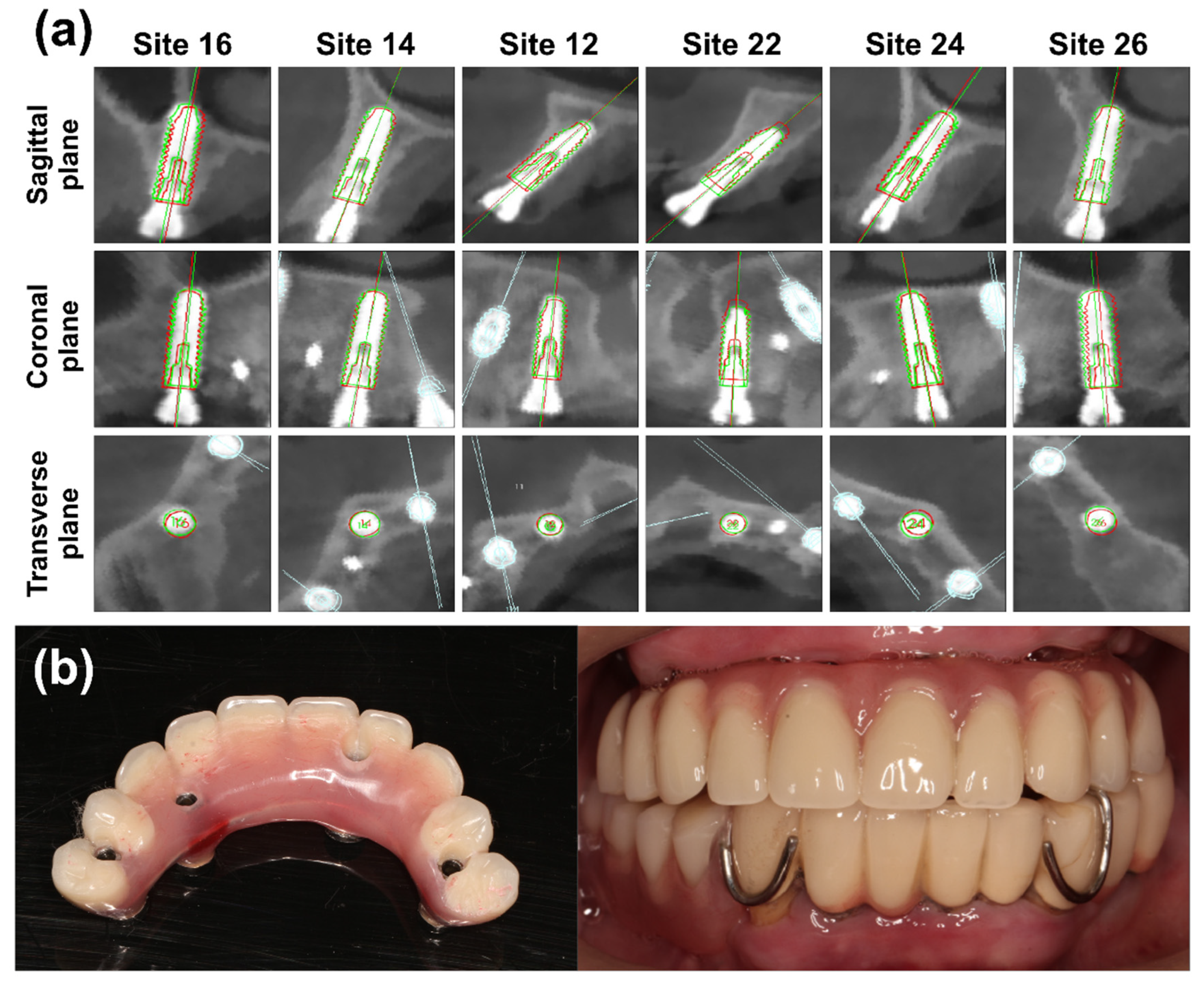
2.4. Postoperative Accuracy Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ramanauskaite, A.; Becker, K.; Wolfart, S.; Lukman, F.; Schwarz, F. Efficacy of rehabilitation with different approaches of implant-supported full-arch prosthetic designs: A systematic review. J. Clin. Periodontol. 2022, 49, 272–290. [Google Scholar] [CrossRef] [PubMed]
- Riemann, M.; Wachtel, H.; Beuer, F.; Bolz, W.; Schuh, P.; Niedermaier, R.; Stelzle, F. Biologic and Technical Complications of Implant-Supported Immediately Loaded Fixed Full-Arch Prostheses: An Evaluation of Up to 6 Years. Int. J. Oral Maxillofac. Implants 2019, 34, 1482–1492. [Google Scholar] [CrossRef]
- Strub, J.; Jurdzik, B.; Tuna, T. Prognosis of immediately loaded implants and their restorations: A systematic literature review. J. Oral Rehabil. 2012, 39, 704–717. [Google Scholar] [CrossRef] [PubMed]
- Thomé, G.; Caldas, W.; Bernardes, S.R.; Cartelli, C.A.; Gracher, A.H.P.; Trojan, L.C. Implant and prosthesis survival rates of full-arch immediate prostheses supported by implants with and without bicortical anchorage: Up to 2 years of follow-up retrospective study. Clin. Oral Implants Res. 2021, 32, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Martinez, H.; Davarpanah, M.; Missika, P.; Celletti, R.; Lazzara, R. Optimal implant stabilization in low density bone. Clin. Oral Implants Res. 2001, 12, 423–432. [Google Scholar] [CrossRef]
- Maló, P.; de Araújo Nobre, M.; Lopes, A.; Moss, S. Posterior maxillary implants inserted with bicortical anchorage and placed in immediate function for partial or complete edentulous rehabilitations. A retrospective clinical study with a median follow-up of 7 years. Oral Maxillofac. Surg. 2015, 19, 19–27. [Google Scholar] [CrossRef]
- Kalpidis, C.D.; Konstantinidis, A.B. Critical hemorrhage in the floor of the mouth during implant placement in the first mandibular premolar position: A case report. Implant Dent. 2005, 14, 117–124. [Google Scholar] [CrossRef]
- Tahmaseb, A.; Wu, V.; Wismeijer, D.; Coucke, W.; Evans, C. The accuracy of static computer-aided implant surgery: A systematic review and meta-analysis. Clin. Oral Implants Res. 2018, 29, 416–435. [Google Scholar] [CrossRef] [Green Version]
- Giacomo, G.A.D.; Cury, P.R.; de Araujo, N.S.; Sendyk, W.R.; Sendyk, C.L. Clinical application of stereolithographic surgical guides for implant placement: Preliminary results. J. Periodontol. 2005, 76, 503–507. [Google Scholar] [CrossRef]
- Cassetta, M.; Giansanti, M.; Di Mambro, A.; Calasso, S.; Barbato, E. Accuracy of two stereolithographic surgical templates: A retrospective study. Clin. Implant Dent. Relat. Res. 2013, 15, 448–459. [Google Scholar] [CrossRef]
- Jorba-García, A.; González-Barnadas, A.; Camps-Font, O.; Figueiredo, R.; Valmaseda-Castellón, E. Accuracy assessment of dynamic computer–aided implant placement: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 2479–2494. [Google Scholar] [CrossRef] [PubMed]
- Papaspyridakos, P.; De Souza, A.; Bathija, A.; Kang, K.; Chochlidakis, K. Complete digital workflow for mandibular full-arch implant rehabilitation in 3 appointments. J. Prosthodont. 2021, 30, 548–552. [Google Scholar] [CrossRef] [PubMed]
- Yogui, F.; Verri, F.; de Luna Gomes, J.; Lemos, C.; Cruz, R.; Pellizzer, E. Comparison between computer-guided and freehand dental implant placement surgery: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2021, 50, 242–250. [Google Scholar] [CrossRef]
- D’haese, J.; Ackhurst, J.; Wismeijer, D.; De Bruyn, H.; Tahmaseb, A. Current state of the art of computer-guided implant surgery. Periodontology 2000 2017, 73, 121–133. [Google Scholar] [CrossRef] [PubMed]
- Van Riet, T.C.; Sem, K.T.C.J.; Ho, J.-P.T.; Spijker, R.; Kober, J.; de Lange, J. Robot technology in dentistry, part one of a systematic review: Literature characteristics. Dent. Mater. 2021, 37, 1217–1226. [Google Scholar] [CrossRef]
- Van Riet, T.C.; Sem, K.T.C.J.; Ho, J.-P.T.; Spijker, R.; Kober, J.; de Lange, J. Robot technology in dentistry, part two of a systematic review: An overview of initiatives. Dent. Mater. 2021, 37, 1227–1236. [Google Scholar] [CrossRef]
- Bolding, S.L.; Reebye, U.N. Accuracy of haptic robotic guidance of dental implant surgery for completely edentulous arches. J. Prosthet. Dent. 2022, 128, 639–647. [Google Scholar] [CrossRef]
- Wu, Y.; Wang, F.; Fan, S.; Chow, J.K.-F. Robotics in dental implantology. Oral Maxillofac. Surg. Clin. N. Am. 2019, 31, 513–518. [Google Scholar] [CrossRef]
- Zhang, K.; Yu, M.; Cao, C.; Xu, B. Preliminary Research on the Accuracy of Implant Surgery Assisted by Implant Surgery Robots. China Med. Device Informat. 2021, 27, 25–28. [Google Scholar] [CrossRef]
- Siqueira, R.; Chen, Z.; Galli, M.; Saleh, I.; Wang, H.L.; Chan, H.L. Does a fully digital workflow improve the accuracy of computer-assisted implant surgery in partially edentulous patients? A systematic review of clinical trials. Clin. Implant Dent. Relat. Res. 2020, 22, 660–671. [Google Scholar] [CrossRef]
- Schnutenhaus, S.; Edelmann, C.; Knipper, A.; Luthardt, R.G. Accuracy of dynamic computer-assisted implant placement: A systematic review and meta-analysis of clinical and in vitro studies. J. Clin. Med. 2021, 10, 704. [Google Scholar] [CrossRef] [PubMed]
- Bergkvist, G.; Koh, K.-J.; Sahlholm, S.; Klintström, E.; Lindh, C. Bone density at implant sites and its relationship to assessment of bone quality and treatment outcome. Int. J. Oral Maxillofac. Implants 2010, 25, 321–328. [Google Scholar] [PubMed]
- Lin, C.-C.; Wu, C.-Z.; Huang, M.-S.; Huang, C.-F.; Cheng, H.-C.; Wang, D.P. Fully digital workflow for planning static guided implant surgery: A prospective accuracy study. J. Clin. Med. 2020, 9, 980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pellegrino, G.; Ferri, A.; Del Fabbro, M.; Prati, C.; Giovanna Gandolfi, M.; Marchetti, C. Dynamic Navigation in Implant Dentistry: A Systematic Review and Meta-analysis. Int. J. Oral Maxillofac. Implants 2021, 36, e121–e140. [Google Scholar] [CrossRef] [PubMed]
- Ma, F.; Sun, F.; Wei, T.; Ma, Y. Comparison of the accuracy of two different dynamic navigation system registration methods for dental implant placement: A retrospective study. Clin. Implant Dent. Relat. Res. 2022, 24, 352–360. [Google Scholar] [CrossRef]
- Bolding, S.; Reebye, U. Robotic-Guided Dental Implant Placement in Fully Edentulous Patients: Preliminary Results of a Prospective Multi-Center Clinical Study. J. Oral Maxillofac. Surg. 2020, 78, e22–e23. [Google Scholar] [CrossRef]
- Bai, S.; Ren, N.; Feng, Z.; Xie, R.; Dong, Y.; Li, Z.; Zhao, Y. Animal experiment on the accuracy of the Autonomous Dental Implant Robotic System. Chin. J. Stomatol. 2021, 56, 170–174. [Google Scholar] [CrossRef]
- Yan, B.; Zhang, W.; Cai, L.; Zheng, L.; Bao, K.; Rao, Y.; Yang, L.; Ye, W.; Guan, P.; Yang, W. Optics-guided Robotic System for Dental Implant Surgery. Chin. J. Mech. Eng. 2022, 35, 55. [Google Scholar] [CrossRef]
- Tang, T.; Huang, Z.; Liao, L.; Gu, X.; Zhang, J.; Zhang, X. Factors that influence direction deviation in freehand implant placement. J. Prosthodont. 2019, 28, 511–518. [Google Scholar] [CrossRef]
- Abduo, J.; Lau, D. Accuracy of static computer-assisted implant placement in long span edentulous area by novice implant clinicians: A cross-sectional in vitro study comparing fully-guided, pilot-guided, and freehand implant placement protocols. Clin. Implant Dent. Relat. Res. 2021, 23, 361–372. [Google Scholar] [CrossRef]
- Fatemitabar, S.A.; Nikgoo, A. Multichannel computed tomography versus cone-beam computed tomography: Linear accuracy of in vitro measurements of the maxilla for implant placement. Int. J. Oral Maxillofac. Implants 2010, 25, 499–505. [Google Scholar] [PubMed]
- Schnutenhaus, S.; Knipper, A.; Wetzel, M.; Edelmann, C.; Luthardt, R. Accuracy of computer-assisted dynamic navigation as a function of different intraoral reference systems: An in vitro study. Int. J. Environ. Res. Public Health 2021, 18, 3244. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Evaluation Parameters | Site 16 | Site 14 | Site 12 | Site 22 | Site 24 | Site 26 | Mean ± SD |
|---|---|---|---|---|---|---|---|
| Global coronal deviation (mm) | 0.61 | 0.33 | 0.65 | 1.03 | 0.46 | 0.50 | 0.59 ± 0.24 |
| Vertical coronal deviation (mm) | 0.34 | 0.27 | 0.48 | −1.01 | 0.35 | 0.20 | 0.11 ± 0.55 |
| Lateral coronal deviation (mm) | 0.51 | 0.19 | 0.44 | 0.19 | 0.30 | 0.45 | 0.35 ± 0.14 |
| Global apical deviation (mm) | 0.59 | 0.31 | 0.56 | 1.03 | 0.55 | 0.61 | 0.61 ± 0.23 |
| Vertical apical deviation (mm) | 0.34 | 0.27 | 0.47 | −1.02 | 0.35 | 0.20 | 0.10 ± 0.56 |
| Lateral apical deviation (mm) | 0.48 | 0.17 | 0.30 | 0.16 | 0.42 | 0.57 | 0.35 ± 0.17 |
| Angular deviation (°) | 0.41 | 1.44 | 0.87 | 0.98 | 0.54 | 1.09 | 0.89 ± 0.38 |
| Implant stability quotients (ISQ) | 83 | 81 | 61 | 55 | 76 | 86 | 73.67 ± 12.71 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, S.; Chen, J.; Li, A.; Li, P.; Xu, S. Autonomous Robotic Surgery for Immediately Loaded Implant-Supported Maxillary Full-Arch Prosthesis: A Case Report. J. Clin. Med. 2022, 11, 6594. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11216594
Yang S, Chen J, Li A, Li P, Xu S. Autonomous Robotic Surgery for Immediately Loaded Implant-Supported Maxillary Full-Arch Prosthesis: A Case Report. Journal of Clinical Medicine. 2022; 11(21):6594. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11216594
Chicago/Turabian StyleYang, Shuo, Jiahao Chen, An Li, Ping Li, and Shulan Xu. 2022. "Autonomous Robotic Surgery for Immediately Loaded Implant-Supported Maxillary Full-Arch Prosthesis: A Case Report" Journal of Clinical Medicine 11, no. 21: 6594. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11216594