
Systemic Lupus Erythematosus and Lung Involvement: A Comprehensive Review
 , , , and add
Show full author list
, , , and add
Show full author list
Abstract
:1. Introduction
2. Epidemiology
2.1. General Incidence
2.2. Incidence of Pleural Involvement in SLE
2.3. Incidence of Pulmonary Parenchyma Involvement in SLE
3. Pathogenesis
4. Diagnosis
4.1. Chest X-ray (CXR)
4.2. Computerized Tomography (CT)
4.3. Pulmonary Function Test
4.4. Biopsy
4.5. Bronchoalveolar Lavage (BAL)
4.6. FDG-PET
4.7. Dynamic Magnetic Resonance Imaging (MRI)
4.8. Summary
5. Types of Pulmonary Involvement
5.1. Lupus Pleuritis
5.1.1. Clinical Manifestation
5.1.2. Treatment
5.1.3. Sequelae and Outcomes
5.2. Pleural Effusion
5.2.1. Clinical Manifestation
5.2.2. Treatment
5.2.3. Sequelae and Outcomes
5.3. Acute Lupus Pneumonitis (ALP)
5.3.1. Clinical Manifestation
5.3.2. Treatment
5.3.3. Sequelae and Outcomes
5.4. Diffuse Alveolar Hemorrhage
5.4.1. Clinical Manifestation
5.4.2. Treatment
5.4.3. Sequelae and Outcomes
5.5. Interstitial Lung Disease (ILD)
5.5.1. Clinical Manifestation
5.5.2. Treatment
5.5.3. Sequelae and Outcomes
5.6. Shrinking Lung Syndrome
5.6.1. Clinical Manifestation
5.6.2. Treatment
5.6.3. Sequelae and Outcomes
5.7. Pulmonary Arterial Hypertension
5.7.1. Clinical Manifestation
5.7.2. Treatment
5.7.3. Sequelae and Outcomes
5.8. Pulmonary Embolism
5.8.1. Clinical Manifestation
5.8.2. Treatment
5.8.3. Sequelae and Outcomes
5.9. Drug Toxicity and Lung Involvement of SLE

| Clinical Symptom | Treatment | Outcome | Summary | Ref | |
|---|---|---|---|---|---|
| Lupus pleuritis | Options vary upon the severity of symptoms. NSAIDs can be used for mild pleuritis, and antimalarials may be added [88,89]. Systemic corticosteroid is a treatment choice for severe pleuritis [90]. Aspiration may be needed for massive pleural effusion [87]. Cyclophosphamide, MMF, rituximab can be considered for steroid-resistance or when renal involvement is present [88,92]. The use of IVIG (alone or combined with cyclosporin) has been reported, but further studies are needed [94,95]. Pleurectomy may be needed in rare cases [96]. | Prognosis and treatment response are good in general [98]. Severe lung restriction and fibrothorax can occur. Rare complications like fibrothorax can occur, due to misdiagnosis and inadequate treatment [87]. | Lupus pleuritis can be treated by immunosuppressive drugs, and has good prognosis in general. Some rare complications can occur, because it can be misdiagnosed initilally. | [87,88,89,90,91,92,93,94,95,96,97,98] | |
| Pleural effusion | The criterion is imaging evidence: US, X-ray, CT, MRI [5]. Pleural effusion in SLE may be due to autoimmune pleuritis, but it’s hard to distinguish it from other causes [6]. | It usually shows a rapid response to corticosteroids [99]. Some may have persistent steroid resistant pleural effusion; in such cases tetracycline pleurodesis use and pleurectomy have been reported [100,101,102]. | No statistically meaningful studies were found. | Pleural effusion is identified by imaging, and it may be caused by autoimmune pleuritis. It responds well to corticosteroids. There were no studies regarding the outcome of SLE-associated pleural effusion. | [5,6,100,101,102] |
| Acute lupus pneumonitis | Empirical broad-spectrum antibiotic therapy should be initiated immediately [107]. Aggressive immunotherapy should be given after infectious etiologies are excluded; high dose IV methylprednisolone, oral corticosteroids, IV cyclophosphamide, rituximab, plasma exchnage, IVIG can be considered [91,108,109]. | No studies have been reported since 1975, but current treatment has improved the prognosis. Patients with pulmonary infection are at risk of persistent abnormalities of lung function and restrictive lung disease [51,104]. | Empirical broad-spectrum antibiotics therapy must be given and aggressive immunosuppressive therapy should be initiated after excluding infections. Studies have not been reported since 1975 about the prognosis, but current options are likely associated with better outcomes. | [51,91,104,107,108,109] | |
| Diffuse alveolar hemorrhage | DAH is common vascular involvement, and it might help to diagnose SLE [1,6]. | There is no well established guideline for DAH. High-dose methylprednisolone is often used [110]. Cyclophosaphamide alone and plasma exchange combined with cyclophosphamide or methylpredniosolone are used, without well defined efficacy in SLE-DAH yet [77,119]. | SLE-associated pulmonary hemorrhage shows high mortality [132]. Several factors related to high mortality are severe dyspnea, need for mechanical ventilation, renal failure, neuropsychiatric complications, etc [42,111,112,113]. Early and aggressive treatment can increase survival rate [114]. | DAH is a quite common and life-threatening condition, showing high mortality rate. High-dose methylprednisolone can be used for treatment. | [1,6,42,76,77,110,111,112,113,114,115,116,117,119] |
| Interstitial lung disease | SLE-ILD includes NSIP, organizing pneumonia, LIP, follicular bronchiolitis, etc. It typically manifests as an insidious onset of chronic nonproductive cough, dyspnea, decreased exercise tolerance, etc. | Treatment depends on expert opinion [121]. Recent studies suggest corticosteroids alone or with cyclophosaphamide or MMF as an induction therapy, and azathioprine or MMF as a maintenance therapy. | 55 SLE-ILD patients showed overall 5yr survival rate of 85.3% [122].Factors predicting worse outcome include current smoking, thrombocytopenia, significant lung fibrosis [122]. Lupus-associated pneumonitis had common progression to respiratory failure and high mortality [111]. It is difficult to estimate the outcome of SLE-ILD. | SLE-ILD includes various types of ILD, and it shows slowly-developing respiratory symptoms. Treatment options are based on expert opinion, but recent algorithms suggest the use of corticosteroids and immunosuppressive agents. Its clinical outcome is hard to estimate accurately. | [103,107,111,118,119,120,121,122,123] |
| Shrinking lung syndrome | SLS is rare, and it shows a large female predominance [66]. All patients show respiratory symptoms; dyspnea, coughing, pleuritic chest pain. SLS causes progressive decrease in lung volumes on PFT [65,127]. | There are no clinical guidelines, Glucocorticoid alone or with immunosuppressive agents are frequently used [66,81,128]. Theophylline, beta-agonists, rituximab alone or with cyclophosphamide and beta-agonist, belimumab can be considered [81,128,129,130,131,132,133,134] | Corticosteroids and immunosuppresion shows a good response. Most will cure from SLS, but some complications such as pneumonia can remain [81,136]. | SLS is a rare condition, characterized by progressive decline of lung volumes on PFT. It responds well to corticosteroids and immunosuppresive therapy, but some complications may occur. | [65,66,81,124,125,126,127,128,129,130,131,132,133,134,135,136] |
| Pulmonary arterial hypertension | It may cause irreversible changes of right ventricle or lung capillaries [137]. Risk factors for PAH include hypertension, high fibrinogen levels, thrombocytopenia, serositis, etc. | Immunosuppresion based on IV cyclophosphamide have been shown to be successful. Other options include IV cyclophosphamide with prednisolone, immunosuppresion in combination with vasodilators, IV epoprostenol, bosentan, and sildenafil [144,145,146,147,148,149]. | PAH is the third most common cause of death in SLE [154]. CTD-PAH showed poorer survival than idiopathic PAH [155]. | PAH can cause irreversible damage to heart or lung, and it show high mortality rate. Immunosuppresion can be used as a treatment. | [137,138,139,140,141,142,143,144,145,146,147,148,149,150,151,152,153,154,155,156,157,158] |
| Pulmonary embolism | PE is a rare but life-threatening condition. SLE patients are susceptible to PE. Risk factors include high BMI, fast progression of SLE, hypoalbuminemia, antiphospholipid antibodies, high dose glucocorticoids [70,159,160]. | Studies on the treatment of SLE associated PE have rarely been performed. Anticoagulation therapy needs to be commenced [161]. Massive PE and persistent hypotension requires thrombolysis [162]. | Life-long anticoagulation may be warranted. Corticosteroids or immunosuppressive agents as a intensive treatment may be required [164]. | PE is rare but can be fatal, and SLE patients are at risk of PE. Early anticoagulation should be initiated, and some might need thrombolysis. Some refractory cases may need life-long anticoagulation or intensive treatment. | [8,70,158,159,160,161,162,163,164] |
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Bertsias, G.K.; Pamfil, C.; Fanouriakis, A.; Boumpas, D.T. Diagnostic criteria for systemic lupus erythematosus: Has the time come? Nat. Rev. Rheumatol. 2013, 9, 687–694. [Google Scholar] [CrossRef] [PubMed]
- Stojan, G.; Petri, M. Epidemiology of systemic lupus erythematosus: An update. Curr. Opin. Rheumatol. 2018, 30, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Moulton, V.R.; Suarez-Fueyo, A.; Meidan, E.; Li, H.; Mizui, M.; Tsokos, G.C. Pathogenesis of human systemic lupus erythematosus: A cellular perspective. Trends Mol. Med. 2017, 23, 615–635. [Google Scholar] [CrossRef] [PubMed]
- Kokosi, M.; Lams, B.; Agarwal, S. Systemic lupus erythematosus and antiphospholipid antibody syndrome. Clin. Chest Med. 2019, 40, 519–529. [Google Scholar] [CrossRef]
- Aringer, M.; Costenbader, K.; Daikh, D.; Brinks, R.; Mosca, M.; Ramsey-Goldman, R.; Smolen, J.S.; Wofsy, D.; Boumpas, D.T.; Kamen, D.L.; et al. 2019 European League Against Rheumatism/American College of Rheumatology classification criteria for systemic lupus erythematosus. Arthritis Rheumatol. 2019, 71, 1400–1412. [Google Scholar] [CrossRef] [Green Version]
- Hannah, J.R.; D’Cruz, D.P. Pulmonary complications of systemic lupus erythematosus. Semin. Respir. Crit. Care Med. 2019, 40, 227–234. [Google Scholar] [CrossRef]
- Vitali, C.; Bencivelli, W.; Isenberg, D.A.; Smolen, J.S.; Snaith, M.L.; Sciuto, M.; d’Ascanio, A.; Bombardieri, S. Disease activity in systemic lupus erythematosus: Report of the Consensus Study Group of the European Workshop for Rheumatology Research. I. A descriptive analysis of 704 European lupus patients. European Consensus Study Group for Disease Activity in SLE. Clin. Exp. Rheumatol. 1992, 10, 527–539. [Google Scholar]
- Çiftçi, E.; Yalçinkaya, F.; İnce, E.; Ekim, M.; İleri, M.; Örgerin, Z.; Fitöz, S.; Güriz, H.; Aysev, A.D.; Dogru, Ü. Pulmonary involvement in childhood-onset systemic lupus erythematosus: A report of five cases. Rheumatology 2004, 43, 587–591. [Google Scholar] [CrossRef] [Green Version]
- Rabinovich, C.E. Pulmonary complications of childhood rheumatic disease. Paediatr. Respir. Rev. 2012, 13, 29–36. [Google Scholar] [CrossRef]
- Cerveri, I.; Bruschi, C.; Ravelli, A.; Zoia, M.C.; Fanfulla, F.; Zonta, L.; Pellegrini, G.; Martini, A. Pulmonary function in childhood connective tissue diseases. Eur. Respir. J. 1992, 5, 733–738. [Google Scholar] [CrossRef]
- Silberstein, S.L.; Barland, P.; Grayzel, A.I.; Koerner, S.K. Pulmonary dysfunction in systemic lupus erythematosus:prevalence classification and correlation with other organ involvement. J. Rheumatol. 1980, 7, 187–195. [Google Scholar] [PubMed]
- Trapani, S.; Camiciottoli, G.; Ermini, M.; Castellani, W.; Falcini, F. Pulmonary involvement in juvenile systemic lupus erythematosus: A study on lung function in patients asymptomatic for respiratory disease. Lupus 1998, 7, 545–550. [Google Scholar] [CrossRef] [PubMed]
- Lilleby, V.; Aaløkken, T.M.; Johansen, B.; Førre, Ø. Pulmonary involvement in patients with childhood-onset systemic lupus erythematosus. Clin. Exp. Rheumatol. 2006, 24, 203–208. [Google Scholar] [PubMed]
- Bertoli, A.M.; Vila, L.M.; Apte, M.; Fessler, B.J.; Bastian, H.M.; Reveille, J.D.; Alarcon, G.S. Systemic lupus erythematosus in a multiethnic US Cohort LUMINA XLVIII: Factors predictive of pulmonary damage. Lupus 2007, 16, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Narváez, J.; Borrell, H.; Sánchez-Alonso, F.; Rúa-Figueroa, I.; López-Longo, F.J.; Galindo-Izquierdo, M.; Calvo-Alén, J.; Fernández-Nebro, A.; Olivé, A.; Andreu, J.L.; et al. Primary respiratory disease in patients with systemic lupus erythematosus: Data from the Spanish rheumatology society lupus registry (RELESSER) cohort. Arthritis Res. Ther. 2018, 20, 280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsokos, G.C. Systemic lupus erythematosus. N. Engl. J. Med. 2011, 365, 2110–2121. [Google Scholar] [CrossRef] [Green Version]
- Duarte, C.; Couto, M.; Ines, L.; Liang, M.H. Epidemiology of systemic lupus erythematosus. In Systemic Lupus Erythematosus; Lahita, R.G., Tsokos, G.C., Buyon, J., Koike, T., Eds.; Elsevier: London, UK, 2011; pp. 673–696. [Google Scholar]
- Pons-Estel, G.J.; Alarcón, G.S.; Scofield, L.; Reinlib, L.; Cooper, G.S. Understanding the epidemiology and progression of systemic lupus erythematosus. Semin. Arthritis Rheum. 2010, 39, 257–268. [Google Scholar] [CrossRef] [Green Version]
- Uramoto, K.M.; Michet Jr, C.J.; Thumboo, J.; Sunku, J.; O’Fallon, W.M.; Gabriel, S.E. Trends in the incidence and mortality of systemic lupus erythematosus, 1950–1992. Arthritis Rheum. 1999, 42, 46–50. [Google Scholar] [CrossRef]
- Mccarty, D.J.; Manzi, S.; Medsger JR, T.A.; Ramsey-Goldman, R.; Laporte, R.E.; Kwoh, C.K. Incidence of systemic lupus erythematosus race and gender differences. Arthritis Rheum. 1995, 38, 1260–1270. [Google Scholar] [CrossRef]
- Johnson, A.E.; Gordon, C.; Palmer, R.G.; Bacon, P.A. The prevalence and incidence of systemic lupus erythematosus in Birmingham, England. Arthritis Rheum. 1995, 38, 551–558. [Google Scholar] [CrossRef]
- Hopkinson, N.D.; Doherty, M.; Powell, R.J. The prevalence and incidence of systemic lupus erythematosus in Nottingham, UK, 1989–1990. Br. J. Rheumatol. 1993, 32, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Chakravarty, E.F.; Bush, T.M.; Manzi, S.; Clarke, A.E.; Ward, M.M. Prevalence of adult systemic lupus erythematosus in California and Pennsylvania in 2000: Estimates obtained using hospitalization data. Arthritis Rheum. 2007, 56, 2092–2094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samanta, A.; Feehally, J.; Roy, S.; Nichol, F.E.; Sheldon, P.J.; Walls, J. High prevalence of systemic disease and mortality in Asian subjects with systemic lupus erythematosus. Ann. Rheum. Dis. 1991, 50, 490–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hochberg, M.C. The incidence of systemic lupus erythematosus in Baltimore, Maryland, 1970–1977. Arthritis Rheum. 1985, 28, 80–86. [Google Scholar] [CrossRef]
- Danchenko, N.; Satia, J.A.; Anthony, M.S. Epidemiology of systemic lupus erythematosus: A comparison of worldwide disease burden. Lupus 2006, 15, 308–318. [Google Scholar] [CrossRef]
- Petri, M. Epidemiology of systemic lupus erythematosus. Best Pract. Res. Clin. Rheumatol. 2002, 16, 847–858. [Google Scholar] [CrossRef]
- Lahita, R.G. The role of sex hormones in systemic lupus erythematosus. Curr. Opin. Rheumatol. 1999, 11, 352–356. [Google Scholar] [CrossRef]
- Hiraki, L.T.; Benseler, S.M.; Tyrrell, P.N.; Hebert, D.; Harvey, E.; Silverman, E.D. Clinical and laboratory characteristics and long-term outcome of pediatric systemic lupus erythematosus: A longitudinal study. J. Pediatr. 2008, 152, 550–556. [Google Scholar] [CrossRef]
- Lehman, T.J.; McCurdy, D.K.; Bernstein, B.H.; King, K.K.; Hanson, V. Systemic lupus erythematosus in the first decade of life. Pediatrics 1989, 83, 235–239. [Google Scholar] [CrossRef]
- Bader-Meunier, B.; Armengaud, J.B.; Haddad, E.; Salomon, R.; Deschenes, G.; Kone-Paut, I.; Leblanc, T.; Loirat, C.; Niaudet, P.; Piette, J.C.; et al. Initial presentation of childhood-onset systemic lupus erythematosus: A French multicenter study. J. Pediatr. 2005, 146, 648–653. [Google Scholar] [CrossRef]
- Watson, L.; Leone, V.; Pilkington, C.; Tullus, K.; Rangaraj, S.; McDonagh, J.E.; Gardner-Medwin, J.; Wilkinson, N.; Riley, P.; Tizard, J.; et al. Disease activity, severity, and damage in the UK Juvenile-Onset Systemic Lupus Erythematosus Cohort. Arthritis Rheum. 2012, 64, 2356–2365. [Google Scholar] [CrossRef] [PubMed]
- Boddaert, J.; Huong, D.L.T.; Amoura, Z.; Wechsler, B.; Godeau, P.; Piette, J.C. Late-onset systemic lupus erythematosus: A personal series of 47 patients and pooled analysis of 714 cases in the literature. Medicine 2004, 83, 348–359. [Google Scholar] [CrossRef] [PubMed]
- Crestani, B. The respiratory system in connective tissue disorders. Allergy 2005, 60, 715–734. [Google Scholar] [CrossRef] [PubMed]
- Aguilera-Pickens, G.; Abud-Mendoza, C. Pulmonary manifestations in systemic lupus erythematosus: Pleural involvement, acute pneumonitis, chronic interstitial lung disease and diffuse alveolar hemorrhage. Reumatol. Clin. 2018, 14, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Amarnani, R.; Yeoh, S.A.; Denneny, E.K.; Wincup, C. Lupus and the Lungs: The Assessment and Management of Pulmonary Manifestations of Systemic Lupus Erythematosus. Front. Med. 2020, 7, 610257. [Google Scholar] [CrossRef]
- Murin, S.; Wiedemann, H.P.; Matthay, R.A. Pulmonary manifestations of systemic lupus erythematosus. Clin. Chest Med. 1998, 19, 641–665. [Google Scholar] [CrossRef]
- Zamora, M.R.; Warner, M.L.; Tuder, R.; Schwarz, M.I. Diffuse alveolar hemorrhage and systemic lupus erythematosus. Clinical presentation, histology, survival, and outcome. Medicine 1997, 76, 192–202. [Google Scholar] [CrossRef]
- Liu, M.F.; Lee, J.H.; Weng, T.H.; Lee, Y.Y. Clinical experience of 13 cases with severe pulmonary hemorrhage in systemic lupus erythematosus with active nephritis. Scand. J. Rheumatol. 1998, 27, 291–295. [Google Scholar] [CrossRef]
- Santos-Ocampo, A.S.; Mandell, B.F.; Fessler, B.J. Alveolar hemorrhage in systemic lupus erythematosus: Presentation and management. Chest 2000, 118, 1083–1090. [Google Scholar] [CrossRef] [Green Version]
- Badsha, H.; Teh, C.L.; Kong, K.O.; Lian, T.Y.; Chng, H.H. Pulmonary hemorrhage in systemic lupus erythematosus. Semin. Arthritis Rheum. 2004, 33, 414–421. [Google Scholar] [CrossRef]
- Chang, M.Y.; Fang, J.T.; Chen, Y.C.; Huang, C.C. Diffuse alveolar hemorrhage in systemic lupus erythematosus: A single center retrospective study in Taiwan. Ren. Fail. 2002, 24, 791–802. [Google Scholar] [CrossRef] [PubMed]
- Canas, C.; Tobon, G.J.; Granados, M.; Fernandez, L. Diffuse alveolar hemorrhage in Colombian patients with systemic lupus erythematosus. Clin. Rheumatol. 2007, 26, 1947–1949. [Google Scholar] [CrossRef] [PubMed]
- Koh, W.H.; Thumboo, J.; Boey, M.L. Pulmonary haemorrhage in Oriental patients with systemic lupus erythematosus. Lupus 1997, 6, 713–716. [Google Scholar] [CrossRef]
- Schwab, E.P.; Schumacher, H.R.; Freundlich, B.; Callegari, P.E. Pulmonary alveolar hemorrhage in systemic lupus erythematosus. Semin. Arthritis Rheum. 1993, 23, 8–15. [Google Scholar] [CrossRef]
- Lee, J.G.; Joo, K.W.; Chung, W.K.; Jung, Y.C.; Zheung, S.H.; Yoon, H.J.; Kim, Y.S.; Ahn, C.; Han, J.S.; Kim, S.; et al. Diffuse alveolar hemorrhage in lupus nephritis. Clin. Nephrol. 2001, 55, 282–288. [Google Scholar] [PubMed]
- Myers, J.L.; Katzenstein, A.A. Microangiitis in lupus-induced pulmonary hemorrhage. Am. J. Clin. Pathol. 1986, 85, 552–556. [Google Scholar] [CrossRef] [PubMed]
- Mok, C.C.; Lau, C.S. Pathogenesis of systemic lupus erythematosus. J. Clin. Pathol. 2003, 56, 481–490. [Google Scholar] [CrossRef] [Green Version]
- Lahita, R.G. Systemic Lupus Erythematosus, 5th ed.; Elsevier Academic Press: Amsterdam, The Netherlands, 2010. [Google Scholar]
- Memet, B.; Ginzler, E.M. Pulmonary manifestations of systemic lupus erythematosus. Semin. Respir. Crit. Care Med. 2007, 28, 441–450. [Google Scholar] [CrossRef]
- Kamen, D.L.; Strange, C. Pulmonary manifestations of systemic lupus erythematosus. Clin. Chest Med. 2010, 31, 479–488. [Google Scholar] [CrossRef]
- Wallace, D.J.; Hahn, B. Dubois’ Lupus Erythematosus and Related Syndromes, 9th ed.; Elsevier: Edinburgh, UK, 2018. [Google Scholar]
- Gouda, W.; Alsaqabi, F.; Moshrif, A.; Abbas, A.S.; Abdel-Aziz, T.M.; Islam, M.A. Macrophage activation syndrome triggered by systemic lupus erythematosus flare: Successful treatment with a combination of dexamethasone sodium phosphate, intravenous immunoglobulin, and cyclosporine: A case report. J. Med. Case Rep. 2021, 15, 497. [Google Scholar] [CrossRef]
- Liu, A.C.; Yang, Y.; Li, M.T.; Jia, Y.; Chen, S.; Ye, S.; Zeng, X.Z.; Wang, Z.; Zhao, J.X.; Liu, X.Y.; et al. Macrophage activation syndrome in systemic lupus erythematosus: A multicenter, case-control study in China. Clin. Rheumatol. 2018, 37, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Poudel, P.; Swe, T.; Rayancha, S. A Rare Case of Macrophage Activation Syndrome Presenting as the First Manifestation of Systemic Lupus Erythematosus. J. Investig. Med. High Impact Case Rep. 2018, 6, 2324709618812196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, S.; Uejima, Y.; Arakawa, Y.; Furuichi, M.; Suganuma, E.; Fujinaga, S.; Nakazawa, A.; Kawano, Y. Clinical features of macrophage activation syndrome as the onset manifestation of juvenile systemic lupus erythematosus. Rheumatol. Adv. Pract. 2019, 3, rkz013. [Google Scholar] [CrossRef] [Green Version]
- Nielepkowicz-Gozdzinska, A.; Fendler, W.; Robak, E.; Kulczycka-Siennicka, L.; Gorski, P.; Pietras, T.; Brzezianska, E.; Antczak, A. Exhaled cytokines in systemic lupus erythematosus with lung involvement. Pol. Arch. Med. Wewn. 2013, 123, 141–148. [Google Scholar] [CrossRef] [Green Version]
- Zhuang, H.; Han, S.; Lee, P.Y.; Khaybullin, R.; Shumyak, S.; Lu, L.; Chatha, A.; Afaneh, A.; Zhang, Y.; Xie, C.; et al. Pathogenesis of diffuse alveolar hemorrhage in murine lupus. Arthritis Rheumatol. 2017, 69, 1280–1293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, S.; Wu, P.W.; Seo, J.J.; Fernando, T.; Jin, M.; Contreras, J.; Montano, E.N.; Gabhann, J.N.; Cunningham, K.; Widaa, A.; et al. IL-16/miR-125a axis controls neutrophil recruitment in pristane-induced lung inflammation. JCI Insight 2018, 3, e120798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jarrot, P.A.; Tellier, E.; Plantureux, L.; Crescence, L.; Robert, S.; Chareyre, C.; Daniel, L.; Secq, V.; Garcia, S.; Dignat-George, F.; et al. Neutrophil extracellular traps are associated with the pathogenesis of diffuse alveolar hemorrhage in murine lupus. J. Autoimmun. 2019, 100, 120–130. [Google Scholar] [CrossRef]
- Pego-Reigosa, J.M.; Medeiros, D.A.; Isenberg, D.A. Respiratory manifestations of systemic lupus erythematosus: Old and new concepts. Best Pract. Res. Clin. Rheumatol. 2009, 23, 469–480. [Google Scholar] [CrossRef]
- Vincze, K.; Odler, B.; Müller, V. Pulmonary manifestations in systemic lupus erythematosus. Orv. Hetil. 2016, 157, 1154–1160. [Google Scholar] [CrossRef] [Green Version]
- Deeb, M.; Tselios, K.; Gladman, D.D.; Su, J.; Urowitz, M.B. Shrinking lung syndrome in systemic lupus erythematosus: A single-centre experience. Lupus 2018, 27, 365–371. [Google Scholar] [CrossRef]
- Meinicke, H.; Heinzmann, A.; Geiger, J.; Berner, R.; Hufnagel, M. Symptoms of shrinking lung syndrome reveal systemic lupus erythematosus in a 12-year-old girl. Pediatr. Pulmonol. 2013, 48, 1246–1249. [Google Scholar] [CrossRef] [PubMed]
- Allen, D.; Fischer, A.; Bshouty, Z.; Robinson, D.B.; Peschken, C.A.; Hitchon, C.; El-Gabalawy, H.; Meyers, M.; Mittoo, S. Evaluating systemic lupus erythematosus patients for lung involvement. Lupus 2012, 21, 1316–1325. [Google Scholar] [CrossRef] [PubMed]
- Duron, L.; Cohen-Aubart, F.; Diot, E.; Borie, R.; Abad, S.; Richez, C.; Banse, C.; Vittecoq, O.; Saadoun, D.; Haroche, J.; et al. Shrinking lung syndrome associated with systemic lupus erythematosus: A multicenter collaborative study of 15 new cases and a review of the 155 cases in the literature focusing on treatment response and long-term outcomes. Autoimmun. Rev. 2016, 15, 994–1000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fenlon, H.M.; Doran, M.; Sant, S.M.; Breatnach, E. High-resolution chest CT in systemic lupus erythematosus. AJR Am. J. Roentgenol. 1996, 166, 301–307. [Google Scholar] [CrossRef] [Green Version]
- El-Khalik, K.A.; El-Sayed, Z.A.; Faheem, M.S.; Fouda, E.; Abdurrahman, L.; Abd El-Ghany, S. High resolution computed tomography and pulmonary function tests in childhood systemic lupus erythematosus and juvenile rheumatoid arthritis. Egypt J Pediatr Allergy Immunol 2004, 2, 8–15. [Google Scholar]
- Dai, G.; Li, L.; Wang, T.; Jiang, W.; Ma, J.; Yan, Y.; Chen, Z. Pulmonary Involvement in Children With Systemic Lupus Erythematosus. Front. Pediatr. 2020, 8, 617137. [Google Scholar] [CrossRef]
- Annangi, S.; Dammalapati, T.R.; Nutalapati, S.; Henriques King, M.N. Prevalence of pulmonary embolism among systemic lupus erythematosus discharges: A decade of analysis of the national hospital discharge survey. J. Clin. Rheumatol. 2017, 23, 200–206. [Google Scholar] [CrossRef]
- Nakano, M.; Hasegawa, H.; Takada, T.; Ito, S.; Muramatsu, Y.; Satoh, M.; Suzuki, E.; Gejyo, F. Pulmonary diffusion capacity in patients with systemic lupus erythematosus. Respirology 2002, 7, 45–49. [Google Scholar] [CrossRef]
- Fidler, L.; Keen, K.J.; Touma, Z.; Mittoo, S. Impact of pulmonary disease on patient-reported outcomes and patient-performed functional testing in systemic lupus erythematosus. Lupus 2016, 25, 1004–1011. [Google Scholar] [CrossRef]
- Keane, M.P.; Lynch, J.P. Pleuropulmonary manifestations of systemic lupus erythematosus. Thorax 2000, 55, 159–166. [Google Scholar] [CrossRef] [Green Version]
- Koh, W.H.; Boey, M.L. Open lung biopsy in systemic lupus erythematosus patients with pulmonary disease. Ann. Acad. Med. Singap. 1993, 22, 323–325. [Google Scholar]
- Chhajed, P.N.; Doshi, K.P.; Athavale, A.U.; Bichile, L.S.; Shah, A.C. Bronchoalveolar lavage (BAL) in newly diagnosed patients with collagen vascular diseases. Indian J. Chest Dis. Allied Sci. 1998, 40, 243–250. [Google Scholar]
- Shen, M.; Zeng, X.; Tian, X.; Zhang, F.; Zeng, X.; Zhang, X.; Xu, W. Diffuse alveolar hemorrhage in systemic lupus erythematosus: A retrospective study in China. Lupus 2010, 19, 1326–1330. [Google Scholar] [CrossRef]
- Martínez-Martínez, M.U.; Abud-Mendoza, C. Diffuse alveolar hemorrhage in patients with systemic lupus erythematosus. Clinical manifestations, treatment, and prognosis. Reumatol. Clin. 2014, 10, 248–253. [Google Scholar] [CrossRef]
- Al-Adhoubi, N.K.; Bystrom, J. Systemic lupus erythematosus and diffuse alveolar hemorrhage, etiology and novel treatment strategies. Lupus 2020, 29, 355–363. [Google Scholar] [CrossRef]
- Wang, L.; Xiong, C.; Li, M.; Zeng, X.; Wang, Q.; Fang, W.; Zhao, L. Assessment of lung glucose uptake in patients with systemic lupus erythematosus pulmonary arterial hypertension: A quantitative FDG-PET imaging study. Ann. Nucl. Med. 2020, 34, 407–414. [Google Scholar] [CrossRef]
- Nemec, M.; Pradella, M.; Jahn, K.; Tamm, M.; Walker, U.A. Magnetic Resonance Imaging-Confirmed Pleuritis in Systemic Lupus Erythematosus-Associated Shrinking Lung Syndrome. Arthritis Rheumatol. 2015, 67, 1880. [Google Scholar] [CrossRef] [Green Version]
- Borrell, H.; Narvaez, J.; Alegre, J.J.; Castellvi, I.; Mitjavila, F.; Aparicio, M.; Armengol, E.; Molina-Molina, M.; Nolla, J.M. Shrinking lung syndrome in systemic lupus erythematosus: A case series and review of the literature. Medicine 2016, 95, e4626. [Google Scholar] [CrossRef]
- Ciancio, N.; Pavone, M.; Torrisi, S.E.; Vancheri, A.; Sambataro, D.; Palmucci, S.; Vancheri, C.; Di Marco, F.; Sambataro, G. Contribution of pulmonary function tests (PFTs) to the diagnosis and follow up of connective tissue diseases. Multidiscip. Respir. Med. 2019, 14, 17. [Google Scholar] [CrossRef] [Green Version]
- Torre, O.; Harari, S. Pleural and pulmonary involvement in systemic lupus erythematosus. La Presse Médicale 2011, 40, e41–e51. [Google Scholar] [CrossRef]
- Good, J.T., Jr.; King, T.E.; Antony, V.B.; Sahn, S.A. Lupus pleuritis. Clinical features and pleural fluid characteristics with special reference to pleural fluid antinuclear antibodies. Chest 1983, 84, 714–718. [Google Scholar] [CrossRef]
- Alamoudi, O.S.; Attar, S.M. Pulmonary manifestations in systemic lupus erythematosus: Association with disease activity. Respirology 2015, 20, 474–480. [Google Scholar] [CrossRef]
- King, T.E., Jr.; Kim, E.J.; Kinder, B.W. Connective tissue diseases. In Interstitial Lung Disease, 5th ed.; Schwartz, M.I., King, T.E., Jr., Eds.; People’s Medical Publishing House: Shelton, CT, USA, 2011. [Google Scholar]
- Sharma, S.; Smith, R.; Al-Hameed, F. Fibrothorax and severe lung restriction secondary to lupus pleuritis and its successful treatment by pleurectomy. Can. Respir. J. 2002, 9, 335–337. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.Y. Diagnosis and management of lupus pleuritis. Curr. Opin. Pulm. Med. 2002, 8, 312–316. [Google Scholar] [CrossRef]
- Breuer, G.S.; Deeb, M.; Fisher, D.; Nesher, G. Therapeutic options for refractory massive pleural effusion in systemic lupus erythematosus: A case study and review of the literature. Semin. Arthritis Rheum. 2005, 34, 744–749. [Google Scholar] [CrossRef]
- Hunder, G.G.; McDuffie, F.C.; Hepper, N.G. Pleural fluid complement in systemic lupus erythematosus and rheumatoid arthritis. Ann. Intern. Med. 1972, 76, 357–363. [Google Scholar] [CrossRef]
- Winslow, W.A.; Ploss, L.N.; Loitman, B. Pleuritis in systemic lupus erythmatosus: Importance as an early manifestation in diagnosis. Ann. Intern. Med. 1958, 49, 70–88. [Google Scholar] [CrossRef]
- Karim, M.Y.; Alba, P.; Cuadrado, M.J.; Abbs, I.C.; D’Cruz, D.P.; Khamashta, M.A.; Hughes, G.R.V. Mycophenolate mofetil for systemic lupus erythematosus refractory to other immunosuppressive agents. Rheumatology 2002, 41, 876–882. [Google Scholar] [CrossRef] [Green Version]
- Ng, K.P.; Leandro, M.J.; Edwards, J.C.; Ehrenstein, M.R.; Cambridge, G.; Isenberg, D.A. Repeated B cell depletion in treatment of refractory systemic lupus erythematosus. Ann. Rheum. Dis. 2006, 65, 942–945. [Google Scholar] [CrossRef] [Green Version]
- Meissner, M.; Sherer, Y.; Levy, Y.; Chwalinska-Sadowska, H.; Langevitz, P.; Shoenfeld, Y. Intravenous immunoglobulin therapy in a patient with lupus serositis and nephritis. Rheumatol. Int. 2000, 19, 199–201. [Google Scholar] [CrossRef]
- Sherer, Y.; Langevitz, P.; Levy, Y.; Fabrizzi, F.; Shoenfeld, Y. Treatment of chronic bilateral pleural effusions with intravenous immunoglobulin and cyclosporin. Lupus 1999, 8, 324–327. [Google Scholar] [CrossRef]
- Kim, S.; Park, H.-b.; Cho, Y.K.; Yi, S.; Oh, K.; Kim, D.K.; Yoo, B. Refractory pleural effusion in systemic lupus erythematosus treated by pleurectomy. J. Rheum. Dis. 2017, 24, 43–47. [Google Scholar] [CrossRef] [Green Version]
- Choi, B.Y.; Yoon, M.J.; Shin, K.; Lee, Y.J.; Song, Y.W. Characteristics of pleural effusions in systemic lupus erythematosus: Differential diagnosis of lupus pleuritis. Lupus 2015, 24, 321–326. [Google Scholar] [CrossRef]
- Palavutitotai, N.; Buppajarntham, T.; Katchamart, W. Etiologies and outcomes of pleural effusions in patients with systemic lupus erythematosus. J. Clin. Rheumatol. 2014, 20, 418–421. [Google Scholar] [CrossRef]
- Karkhanis, V.S.; Joshi, J.M. Pleural effusion: Diagnosis, treatment, and management. Open Access Emerg. Med. 2012, 4, 31–52. [Google Scholar] [CrossRef] [Green Version]
- Gilleece, M.H.; Evans, C.C.; Bucknall, R.C. Steroid resistant pleural effusion in systemic lupus erythematosus treated with tetracycline pleurodesis. Ann. Rheum. Dis. 1988, 47, 1031–1032. [Google Scholar] [CrossRef] [Green Version]
- McKnight, K.M.; Adair, N.E.; Agudelo, C.A. Successful use of tetracycline pleurodesis to treat massive pleural effusion secondary to systemic lupus erythematosus. Arthritis Rheum. 1991, 34, 1483–1484. [Google Scholar] [CrossRef]
- Elborn, J.S.; Conn, P.; Roberts, S.D. Refractory massive pleural effusion in systemic lupus erythematosus treated by pleurectomy. Ann. Rheum. Dis. 1987, 46, 77–80. [Google Scholar] [CrossRef] [Green Version]
- Wiedemann, H.P.; Matthay, R.A. Pulmonary manifestations of systemic lupus erythematosus. J. Thorac. Imaging 1992, 7, 1–18. [Google Scholar] [CrossRef]
- Matthay, R.A.; Schwarz, M.I.; Petty, T.L.; Stanford, R.E.; Gupta, R.C.; Sahn, S.A.; Steigerwald, J.C. Pulmonary manifestations of systemic lupus erythematosus: Review of twelve cases of acute lupus pneumonitis. Medicine 1975, 54, 397–409. [Google Scholar] [CrossRef]
- Haupt, H.M.; Moore, G.W.; Hutchins, G.M. The lung in systemic lupus erythematosus. Analysis of the pathologic changes in 120 patients. Am. J. Med. 1981, 71, 791–798. [Google Scholar] [CrossRef]
- Swigris, J.J.; Fischer, A.; Gillis, J.; Meehan, R.T.; Brown, K.K. Pulmonary and thrombotic manifestations of systemic lupus erythematosus. Chest 2008, 133, 271–280. [Google Scholar] [CrossRef]
- Gutsche, M.; Rosen, G.D.; Swigris, J.J. Connective tissue disease-associated interstitial lung disease: A review. Curr. Respir. Care Rep. 2012, 1, 224–232. [Google Scholar] [CrossRef]
- Todd, D.J.; Costenbader, K.H. Dyspnoea in a young woman with active systemic lupus erythematosus. Lupus 2009, 18, 777–784. [Google Scholar] [CrossRef]
- Cervera, R.; Khamashta, M.A.; Font, J.; Sebastiani, G.D.; Gil, A.; Lavilla, P.; Aydintug, A.O.; Jedryka-Goral, A.; de Ramon, E.; Fernandez-Nebro, A.; et al. Morbidity and mortality in systemic lupus erythematosus during a 5-year period. A multicenter prospective study of 1000 patients. European Working Party on Systemic Lupus Erythematosus. Medicine 1999, 78, 167–175. [Google Scholar] [CrossRef]
- Barile, L.A.; Jara, L.J.; Medina-Rodriguez, F.; Garcia-Figueroa, J.L.; Miranda-Limon, J.M. Pulmonary hemorrhage in systemic lupus erythematosus. Lupus 1997, 6, 445–448. [Google Scholar] [CrossRef]
- Martinez-Martinez, M.U.; Abud-Mendoza, C. Predictors of mortality in diffuse alveolar haemorrhage associated with systemic lupus erythematosus. Lupus 2011, 20, 568–574. [Google Scholar] [CrossRef]
- Masoodi, I.; Sirwal, I.A.; Anwar, S.K.; Alzaidi, A.; Balbaid, K.A. Predictors of mortality in pulmonary haemorrhage during SLE: A single centre study over eleven years. Open Access Maced. J. Med. Sci. 2019, 7, 92–96. [Google Scholar] [CrossRef] [Green Version]
- Kwok, S.K.; Moon, S.J.; Ju, J.H.; Park, K.S.; Kim, W.U.; Cho, C.S.; Kim, H.Y.; Park, S.H. Diffuse alveolar hemorrhage in systemic lupus erythematosus: Risk factors and clinical outcome: Results from affiliated hospitals of Catholic University of Korea. Lupus 2011, 20, 102–107. [Google Scholar] [CrossRef]
- Finucci Curi, P.; Pierrestegui, M.; Ortiz, A.; Ceccato, F.; Paira, S. Pulmonary hemorrhage in patients with systemic lupus erythematosus. Clinical manifestations and prognosis. Med. Clin. 2015, 145, 375–379. [Google Scholar] [CrossRef]
- Rojas-Serrano, J.; Pedroza, J.; Regalado, J.; Robledo, J.; Reyes, E.; Sifuentes-Osornio, J.; Flores-Suarez, L.F. High prevalence of infections in patients with systemic lupus erythematosus and pulmonary haemorrhage. Lupus 2008, 17, 295–299. [Google Scholar] [CrossRef] [PubMed]
- Shi, D.; Wang, D.; Li, X.; Zhang, H.; Che, N.; Lu, Z.; Sun, L. Allogeneic transplantation of umbilical cord-derived mesenchymal stem cells for diffuse alveolar hemorrhage in systemic lupus erythematosus. Clin. Rheumatol. 2012, 31, 841–846. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.-y.; Yang, H.-j.; Tong, S.-q.; Li, Y.-j.; Guo, A.-r.; Pang, H.-w. Value of bronchoalveolar lavage as a rescue measurement for systemic lupus erythematosus complicated with diffuse alveolar hemorrhage. Zhonghua Yi Xue Za Zhi 2011, 91, 1917–1919. [Google Scholar] [PubMed]
- Weinrib, L.; Sharma, O.P.; Quismorio, F.P., Jr. A long-term study of interstitial lung disease in systemic lupus erythematosus. Semin. Arthritis Rheum. 1990, 20, 48–56. [Google Scholar] [CrossRef]
- Tansey, D.; Wells, A.U.; Colby, T.V.; Ip, S.; Nikolakoupolou, A.; Du Bois, R.M.; Hansell, D.M.; Nicholson, A.G. Variations in histological patterns of interstitial pneumonia between connective tissue disorders and their relationship to prognosis. Histopathology 2004, 44, 585–596. [Google Scholar] [CrossRef]
- Pope, J. An update in pulmonary hypertension in systemic lupus erythematosus—Do we need to know about it? Lupus 2008, 17, 274–277. [Google Scholar] [CrossRef]
- Robles-Perez, A.; Molina-Molina, M. Treatment considerations of lung involvement in rheumatologic disease. Respiration 2015, 90, 265–274. [Google Scholar] [CrossRef]
- Enomoto, N.; Egashira, R.; Tabata, K.; Hashisako, M.; Kitani, M.; Waseda, Y.; Ishizuka, T.; Watanabe, S.; Kasahara, K.; Izumi, S.; et al. Analysis of systemic lupus erythematosus-related interstitial pneumonia: A retrospective multicentre study. Sci. Rep. 2019, 9, 7355. [Google Scholar] [CrossRef] [Green Version]
- Mira-Avendano, I.; Abril, A.; Burger, C.D.; Dellaripa, P.F.; Fischer, A.; Gotway, M.B.; Lee, A.S.; Lee, J.S.; Matteson, E.L.; Yi, E.S.; et al. Interstitial lung disease and other pulmonary manifestations in connective tissue diseases. Mayo Clin. Proc. 2019, 94, 309–325. [Google Scholar] [CrossRef] [Green Version]
- Hoffbrand, B.I.; Beck, E.R. “Unexplained” dyspnoea and shrinking lungs in systemic lupus erythematosus. Br. Med. J. 1965, 1, 1273–1277. [Google Scholar] [CrossRef] [Green Version]
- Gheita, T.A.; Azkalany, G.S.; El-Fishawy, H.S.; Nour Eldin, A.M. Shrinking lung syndrome in systemic lupus erythematosus patients; clinical characteristics, disease activity and damage. Int. J. Rheum. Dis. 2011, 14, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Branger, S.; Schleinitz, N.; Gayet, S.; Veit, V.; Kaplanski, G.; Badier, M.; Magnan, A.; Harlé, J.R. Le syndrome des poumons rétractés et les maladies auto-immunes. Rev. Med. Interne 2004, 25, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Karim, M.Y.; Miranda, L.C.; Tench, C.M.; Gordon, P.A.; D’Cruz, D.P.; Khamashta, M.A.; Hughes, G.R. Presentation and prognosis of the shrinking lung syndrome in systemic lupus erythematosus. Semin. Arthritis Rheum. 2002, 31, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Langenskiöld, E.; Bonetti, A.; Fitting, J.W.; Heinzer, R.; Dudler, J.; Spertini, F.; Lazor, R. Shrinking lung syndrome successfully treated with rituximab and cyclophosphamide. Respiration 2012, 84, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Van Veen, S.; Peeters, A.J.; Sterk, P.J.; Breedveld, F.C. The “Shrinking lung syndrome” in SLE, treatment with theophylline. Clin. Rheumatol. 1993, 12, 462–465. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Rodríguez, F.; Font, J.; Badia, J.; Miret, C.; Barberà, J.; Cervera, R.; Ingelmo, M. Shrinking lungs syndrome in systemic lupus erythematosus: Improvement with inhaled beta-agonist therapy. Lupus 1997, 6, 412–414. [Google Scholar] [CrossRef]
- Guleria, V.S.; Singh, P.K.; Saxena, P.; Subramanian, S. Shrinking lung syndrome in systemic lupus erythematosus-scleroderma overlap. Lung India 2014, 31, 407–409. [Google Scholar] [CrossRef]
- Benham, H.; Garske, L.; Vecchio, P.; Eckert, B.W. Successful treatment of shrinking lung syndrome with rituximab in a patient with systemic lupus erythematosus. J. Clin. Rheumatol. 2010, 16, 68–70. [Google Scholar] [CrossRef]
- Penacoba Toribio, P.; Corica Albani, M.E.; Mayos Perez, M.; Rodriguez de la Serna, A. Rituximab in the treatment of shrinking lung syndrome in systemic lupus erythematosus. Reumatol. Clin. 2014, 10, 325–327. [Google Scholar] [CrossRef]
- Robles-Perez, A.; Dorca, J.; Castellvi, I.; Nolla, J.M.; Molina-Molina, M.; Narvaez, J. Rituximab effect in severe progressive connective tissue disease-related lung disease: Preliminary data. Rheumatol. Int. 2020, 40, 719–726. [Google Scholar] [CrossRef]
- Reyes, F.; Lazaro, D. Systemic lupus erythematosus complicated by shrinking lung syndrome treated with belimumab: A case report. Chest 2016, 150, 300A. [Google Scholar] [CrossRef]
- Martens, J.; Demedts, M.; Vanmeenen, M.T.; Dequeker, J. Respiratory muscle dysfunction in systemic lupus erythematosus. Chest 1983, 84, 170–175. [Google Scholar] [CrossRef]
- Shah, S.J. Pulmonary hypertension. JAMA 2012, 308, 1366–1374. [Google Scholar] [CrossRef]
- Chen, H.A.; Hsu, T.C.; Yang, S.C.; Weng, C.T.; Wu, C.H.; Sun, C.Y.; Lin, C.Y. Incidence and survival impact of pulmonary arterial hypertension among patients with systemic lupus erythematosus: A nationwide cohort study. Arthritis Res. Ther. 2019, 21, 82. [Google Scholar] [CrossRef]
- Xu, S.Z.; Yan, L.; Li, X.P.; Li, X.M.; Shuai, Z.W.; Leng, R.X.; Pan, H.F.; Ye, D.Q. Features associated with pulmonary arterial hypertension in Chinese hospitalized systemic lupus erythematosus patients. Clin. Rheumatol. 2018, 37, 1547–1553. [Google Scholar] [CrossRef] [PubMed]
- Hachulla, E.; Jais, X.; Cinquetti, G.; Clerson, P.; Rottat, L.; Launay, D.; Cottin, V.; Habib, G.; Prevot, G.; Chabanne, C.; et al. Pulmonary arterial hypertension associated with systemic lupus erythematosus: Results from the French pulmonary hypertension registry. Chest 2018, 153, 143–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donnarumma, J.F.S.; Ferreira, E.V.M.; Ota-Arakaki, J.; Kayser, C. Nailfold capillaroscopy as a risk factor for pulmonary arterial hypertension in systemic lupus erythematosus patients. Adv. Rheumatol. 2019, 59, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Lian, F.; Chen, D.; Wang, Y.; Ye, Y.; Wang, X.; Zhan, Z.; Xu, H.; Liang, L.; Yang, X. Clinical features and independent predictors of pulmonary arterial hypertension in systemic lupus erythematosus. Rheumatol. Int. 2012, 32, 1727–1731. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Leng, X.; Li, Z.; Ye, Z.; Li, C.; Li, X.; Zhu, P.; Wang, Z.; Zheng, Y.; Li, X. Chinese SLE treatment and research group registry: III. association of autoantibodies with clinical manifestations in Chinese patients with systemic lupus erythematosus. J. Immunol. Res. 2014, 2014, 809389. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez-Lopez, L.; Cardona-Muñoz, E.G.; Celis, A.; García-de la Torre, I.; Orozco-Barocio, G.; Salazar-Paramo, M.; Garcia-Gonzalez, C.; Garcia-Gonzalez, A.; Sanchez-Ortiz, A.; Trujillo-Hernandez, B.; et al. Therapy with intermittent pulse cyclophosphamide for pulmonary hypertension associated with systemic lupus erythematosus. Lupus 2004, 13, 105–112. [Google Scholar] [CrossRef]
- Sanchez, O.; Sitbon, O.; Jais, X.; Simonneau, G.; Humbert, M. Immunosuppressive therapy in connective tissue diseases-associated pulmonary arterial hypertension. Chest 2006, 130, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Miyamichi-Yamamoto, S.; Fukumoto, Y.; Sugimura, K.; Ishii, T.; Satoh, K.; Miura, Y.; Tatebe, S.; Nochioka, K.; Aoki, T.; Do, E.Z.; et al. Intensive immunosuppressive therapy improves pulmonary hemodynamics and long-term prognosis in patients with pulmonary arterial hypertension associated with connective tissue disease. Circ. J. 2011, 75, 2668–2674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kommireddy, S.; Bhyravavajhala, S.; Kurimeti, K.; Chennareddy, S.; Kanchinadham, S.; Rajendra Vara Prasad, I.; Rajasekhar, L. Pulmonary arterial hypertension in systemic lupus erythematosus may benefit by addition of immunosuppression to vasodilator therapy: An observational study. Rheumatology 2015, 54, 1673–1679. [Google Scholar] [CrossRef] [Green Version]
- Robbins, I.M.; Gaine, S.P.; Schilz, R.; Tapson, V.F.; Rubin, L.J.; Loyd, J.E. Epoprostenol for treatment of pulmonary hypertension in patients with systemic lupus erythematosus. Chest 2000, 117, 14–18. [Google Scholar] [CrossRef]
- Shirai, Y.; Yasuoka, H.; Takeuchi, T.; Satoh, T.; Kuwana, M. Intravenous epoprostenol treatment of patients with connective tissue disease and pulmonary arterial hypertension at a single center. Mod. Rheumatol. 2013, 23, 1211–1220. [Google Scholar] [CrossRef] [PubMed]
- Rubin, L.J.; Badesch, D.B.; Barst, R.J.; Galie, N.; Black, C.M.; Keogh, A.; Pulido, T.; Frost, A.; Roux, S.; Leconte, I.; et al. Bosentan therapy for pulmonary arterial hypertension. N. Engl. J. Med. 2002, 346, 896–903. [Google Scholar] [CrossRef] [PubMed]
- Mok, M.Y.; Tsang, P.L.; Lam, Y.M.; Lo, Y.; Wong, W.S.; Lau, C.S. Bosentan use in systemic lupus erythematosus patients with pulmonary arterial hypertension. Lupus 2007, 16, 279–285. [Google Scholar] [CrossRef]
- Molina, J.; Lucero, E.; Luluaga, S.; Bellomio, V.; Spindler, A.; Berman, A. Systemic lupus erythematosus-associated pulmonary hypertension: Good outcome following sildenafil therapy. Lupus 2003, 12, 321–323. [Google Scholar] [CrossRef]
- Badesch, D.B.; Hill, N.S.; Burgess, G.; Rubin, L.J.; Barst, R.J.; Galie, N.; Simonneau, G.; Group, S.S. Sildenafil for pulmonary arterial hypertension associated with connective tissue disease. J. Rheumatol. 2007, 34, 2417–2422. [Google Scholar]
- Magliano, M.; Isenberg, D.A.; Hillson, J. Pulmonary hypertension in autoimmune rheumatic diseases: Where are we now? Arthritis Rheum. 2002, 46, 1997–2009. [Google Scholar] [CrossRef]
- Chung, L.; Liu, J.; Parsons, L.; Hassoun, P.M.; McGoon, M.; Badesch, D.B.; Miller, D.P.; Nicolls, M.R.; Zamanian, R.T. Characterization of connective tissue disease-associated pulmonary arterial hypertension from REVEAL: Identifying systemic sclerosis as a unique phenotype. Chest 2010, 138, 1383–1394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, K.Y.; Jeon, C.H.; Choi, S.J.; Yoon, B.Y.; Choi, C.B.; Lee, C.H.; Suh, C.H.; Lee, C.W.; Cho, C.S.; Nam, E.J.; et al. Survival and prognostic factors in patients with connective tissue disease-associated pulmonary hypertension diagnosed by echocardiography: Results from a Korean nationwide registry. Int. J. Rheum. Dis. 2017, 20, 1227–1236. [Google Scholar] [CrossRef] [PubMed]
- Qian, J.; Wang, Y.; Huang, C.; Yang, X.; Zhao, J.; Wang, Q.; Tian, Z.; Li, M.; Zeng, X. Survival and prognostic factors of systemic lupus erythematosus-associated pulmonary arterial hypertension: A PRISMA-compliant systematic review and meta-analysis. Autoimmun. Rev. 2016, 15, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Quadrelli, S.A.; Alvarez, C.; Arce, S.C.; Paz, L.; Sarano, J.; Sobrino, E.M.; Manni, J. Pulmonary involvement of systemic lupus erythematosus: Analysis of 90 necropsies. Lupus 2009, 18, 1053–1060. [Google Scholar] [CrossRef] [PubMed]
- Aviña-Zubieta, J.A.; Lacaille, D.; Sayre, E.C.; Kopec, J.; Choi, H.K.; Esdaile, J.M. Risk of pulmonary embolism and deep vein thrombosis in systemic lupus erythematosus: A population-based cohort study. Arthritis Res. Ther. 2012, 14, A53. [Google Scholar] [CrossRef]
- You, H.; Zhao, J.; Wang, Q.; Tian, X.; Li, M.; Zeng, X. Characteristics and risk factors of pulmonary embolism in patients with systemic lupus erythematosus: A case control study. Clin. Exp. Rheumatol. 2020, 38, 940–948. [Google Scholar]
- Smith, S.B.; Geske, J.B.; Maguire, J.M.; Zane, N.A.; Carter, R.E.; Morgenthaler, T.I. Early anticoagulation is associated with reduced mortality for acute pulmonary embolism. Chest 2010, 137, 1382–1390. [Google Scholar] [CrossRef] [Green Version]
- Kearon, C.; Akl, E.A.; Ornelas, J.; Blaivas, A.; Jimenez, D.; Bounameaux, H.; Huisman, M.; King, C.S.; Morris, T.A.; Sood, N.; et al. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest 2016, 149, 315–352. [Google Scholar] [CrossRef]
- Meyer, G.; Vieillard-Baron, A.; Planquette, B. Recent advances in the management of pulmonary embolism: Focus on the critically ill patients. Ann. Intensive Care 2016, 6, 19. [Google Scholar] [CrossRef] [Green Version]
- Orens, J.B.; Martinez, F.J.; Lynch, J.P., 3rd. Pleuropulmonary manifestations of systemic lupus erythematosus. Rheum. Dis. Clin. North Am. 1994, 20, 159–193. [Google Scholar] [CrossRef]
- Skeoch, S.; Weatherley, N.; Swift, A.J.; Oldroyd, A.; Johns, C.; Hayton, C.; Giollo, A.; Wild, J.M.; Waterton, J.C.; Buch, M.; et al. Drug-Induced Interstitial Lung Disease: A Systematic Review. J. Clin. Med. 2018, 7, 356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spagnolo, P.; Bonniaud, P.; Rossi, G.; Sverzellati, N.; Cottin, V. Drug-induced interstitial lung disease. Eur. Respir. J. 2022, 60, 2102776. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}

| Published Year | Study Type | Key Finding | Comments |
|---|---|---|---|
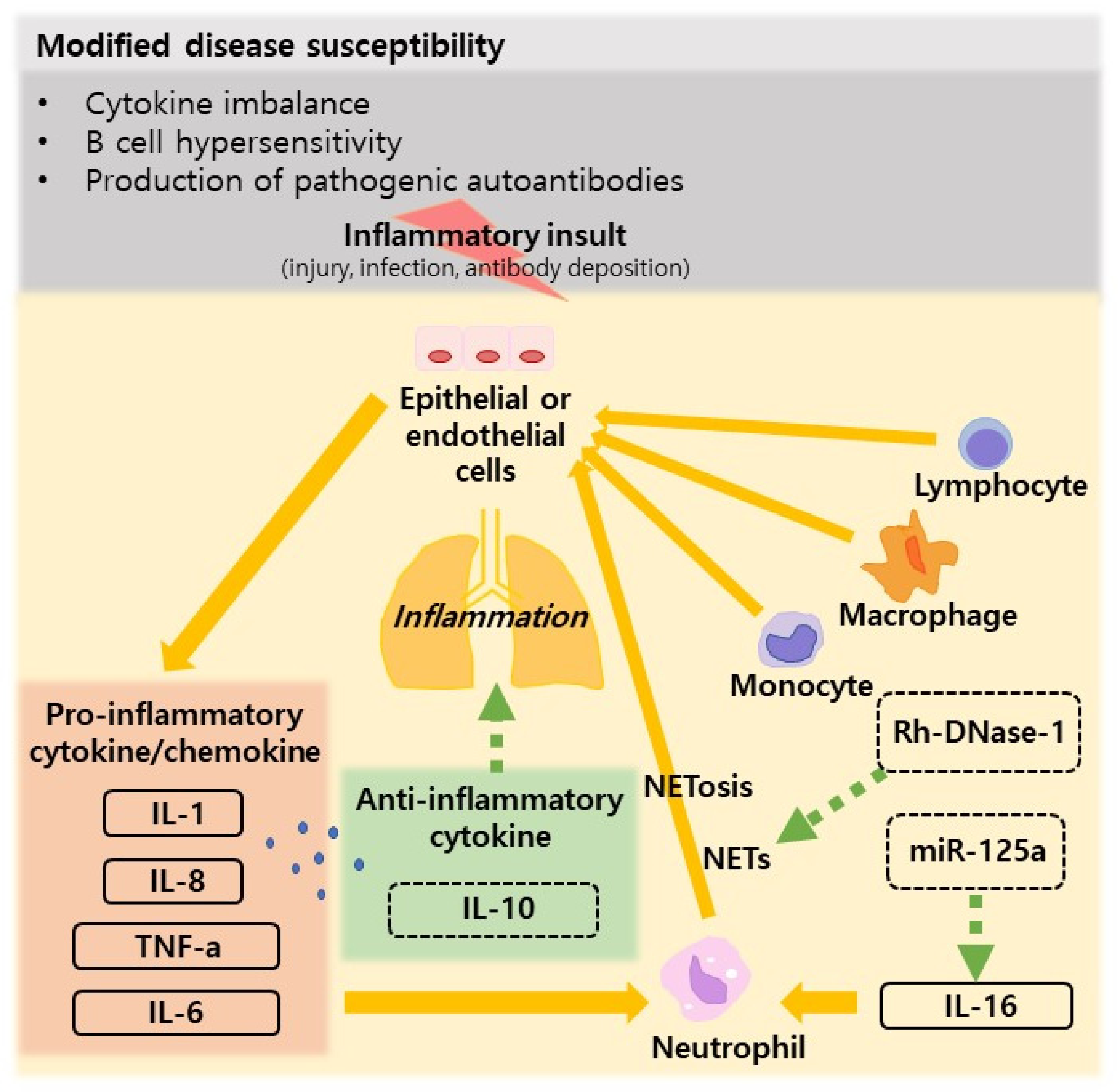
| Nielepkowicz- Goździńska A et al. (2013) [57] | In vivo | Exhaled cytokines in SLE with lung involvement | The mean IL-6 and IL-10 concentrations in the BALF and the IL-10 concentration in the EBC were higher in patients with SLE compared with healthy controls. Study showed that IL-6 and IL-10 are involved in the pathogenesis of SLE and it is likely that IL-10 protects against pulmonary manifestations of SLE. |
| Zhuang H et al. (2017) [58] | In vivo | Pathogenesis of diffuse alveolar hemorrhage in murine lupus | The pathogenesis of DAH involves opsonization of dead cells by natural IgM and complement followed by complement receptor-mediated lung inflammation. The disease is macrophage dependent, and IL-10 is protective. Complement inhibition and/or macrophage-targeted therapies may reduce mortality in lupus-associated DAH. |
| Smith S et al. (2018) [59] | In vivo/ In vitro | IL-16/miR-125a axis controls neutrophil recruitment in pristane-induced lung inflammation | Neutrophil infiltration was markedly reduced in the peritoneal lavage of pristane-treated IL-16-deficient mice and elevated following administration of IL-16. miR-125a mimic reduced pristane-induced IL-16 expression and neutrophil recruitment and abrogated the induced lung pathology. To sum up, IL-16 acts directly on the pulmonary epithelium and markedly enhances neutrophil chemoattractant expression both in vitro and in vivo, while the miR-125a mimic can prevent this. |
| Jarrot P-A et al. (2019) [60] | In vivo | NETs are associated with the pathogenesis of diffuse alveolar hemorrhage in murine lupus | PMNs and NETs play an important pathogenic role in lung injury during pristane-induced DAH. Targeting NETs with Rh-DNase-1 inhalations could be an interesting adjuvant therapy in human DAH. |
| Key Finding | Comments | Ref | |
|---|---|---|---|
| CXR | CXR findings vary upon diseases, and usually correlate with clinical symptoms [35]. | CXR is the most basic imaging method, and its sensitivity is low. | [35,61,62,63,64,65,66] |
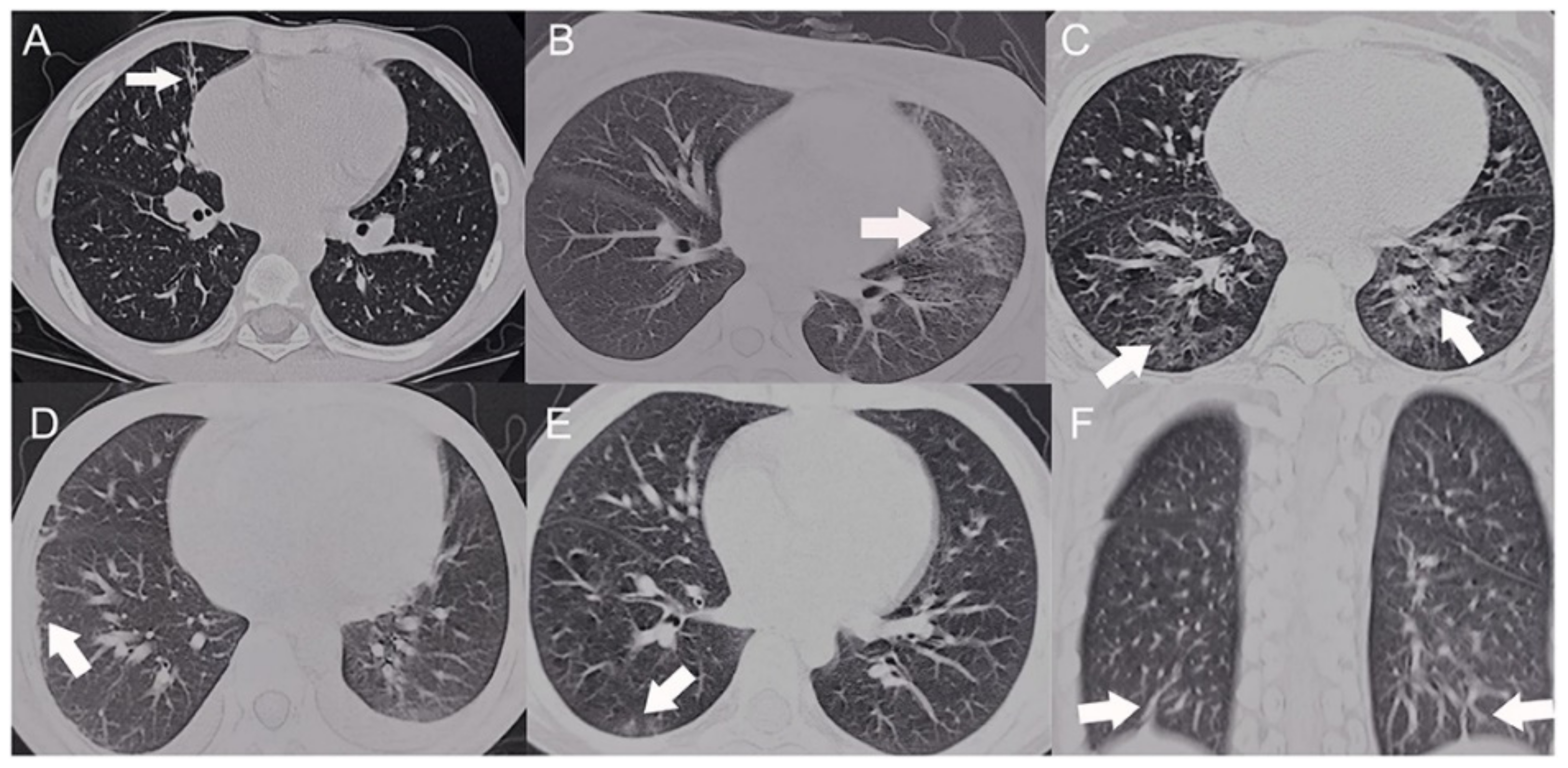
| CT | 70% of the patients showed abnormal findings such as interlobular septa thickening, parenchymal bands, etc [67]. | CT imaging is useful to make an early diagnosis of pulmonary involvement, and it provides precise expectation of pulmonary function [64]. | [67,68,70] |
| PFT | DLco shows the most prominent abnormality among the spirometric values [71] | PFT provides an option to early detect of pulmonary involvement in SLE patients, but it lacks sensitivity [71,72]. | [71,72] |
| Biopsy | Pleural involvement shows results such as fibrosis, lymphocytic/plasma cell infiltration, etc. ALP show alveolar wall damage and necrosis, etc. Bland hemorrhage is predominantly found in DAH [45,47,73]. | Biopsy is rarely used in the diagnostic work-up; it is used only when the diagnosis is unclear and other findings are nonspecific, and it is avoided due to postoperative complications [45]. | [45,47,73] |
| BAL | It shows increased cellularity in ALP, lymphocytic/neutrophilic predominance in ILD, predominance of macrophage in SLE, and the presence of hemosiderophage in DAH [35,51,75,76,77]. | BAL is mainly performed to exclude other causes such as infections [35]. | [35,51,75,76,77] |
| FDG-PET | SLE disease activity and immune/inflammatory status is correlated with high FDG uptake PAH in patients with SLE [79]. | It can be the potential marker for intrapulmonary disease activity in SLE-PAH patients [79]. | [79] |
| Dynamic MRI | Dynamic MRI sequences on forced voluntary ventilation can confirm physiologic movements of both diaphragms and all auxiliary respiratory muscles | Magnetic resonance imaging-confirmed pleuritis in systemic lupus erythematosus-associated shrinking lung syndrome | [80,81] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, J.I.; Lee, K.H.; Park, S.; Yang, J.W.; Kim, H.J.; Song, K.; Lee, S.; Na, H.; Jang, Y.J.; Nam, J.Y.; et al. Systemic Lupus Erythematosus and Lung Involvement: A Comprehensive Review. J. Clin. Med. 2022, 11, 6714. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11226714
Shin JI, Lee KH, Park S, Yang JW, Kim HJ, Song K, Lee S, Na H, Jang YJ, Nam JY, et al. Systemic Lupus Erythematosus and Lung Involvement: A Comprehensive Review. Journal of Clinical Medicine. 2022; 11(22):6714. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11226714
Chicago/Turabian StyleShin, Jae Il, Keum Hwa Lee, Seoyeon Park, Jae Won Yang, Hyung Ju Kim, Kwanhyuk Song, Seungyeon Lee, Hyeyoung Na, Yong Jun Jang, Ju Yun Nam, and et al. 2022. "Systemic Lupus Erythematosus and Lung Involvement: A Comprehensive Review" Journal of Clinical Medicine 11, no. 22: 6714. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11226714