
Efficacy of the New Inotropic Agent Istaroxime in Acute Heart Failure

 ,
, 
Abstract
:1. Introduction
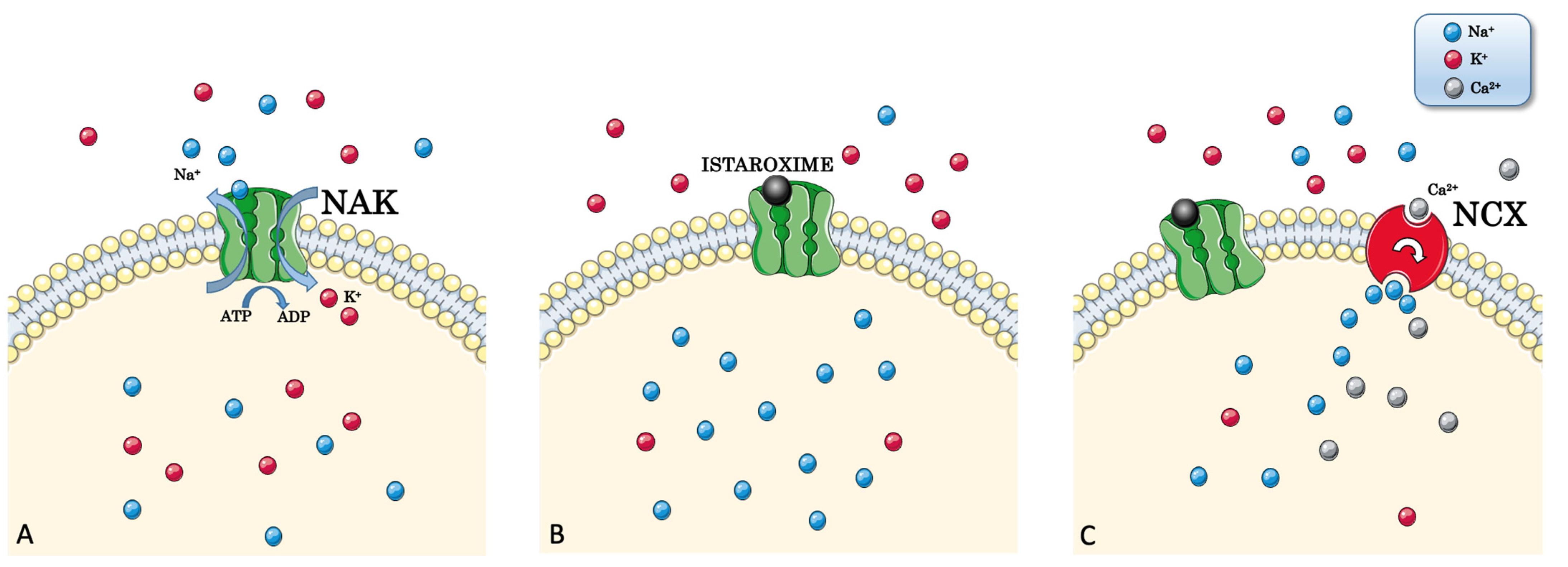
2. NKA: Na+/K+-ATPase Pump
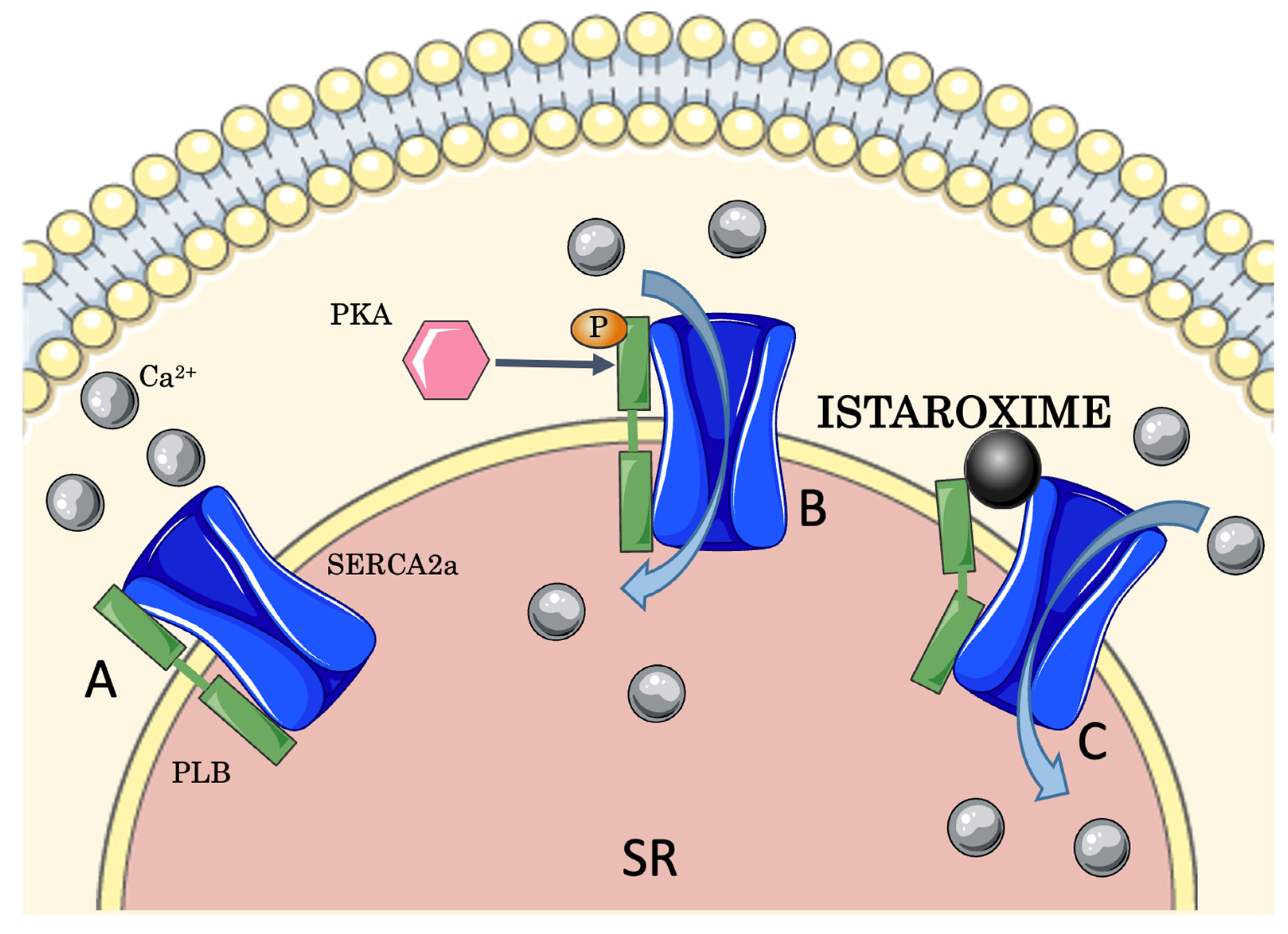
3. SERCA2a: Sarcoendoplasmic Reticular Adenosine Triphosphate-Driven Ca2+ Pump
4. Ca2+ and SERCA2a Function in Cardiac Contractility
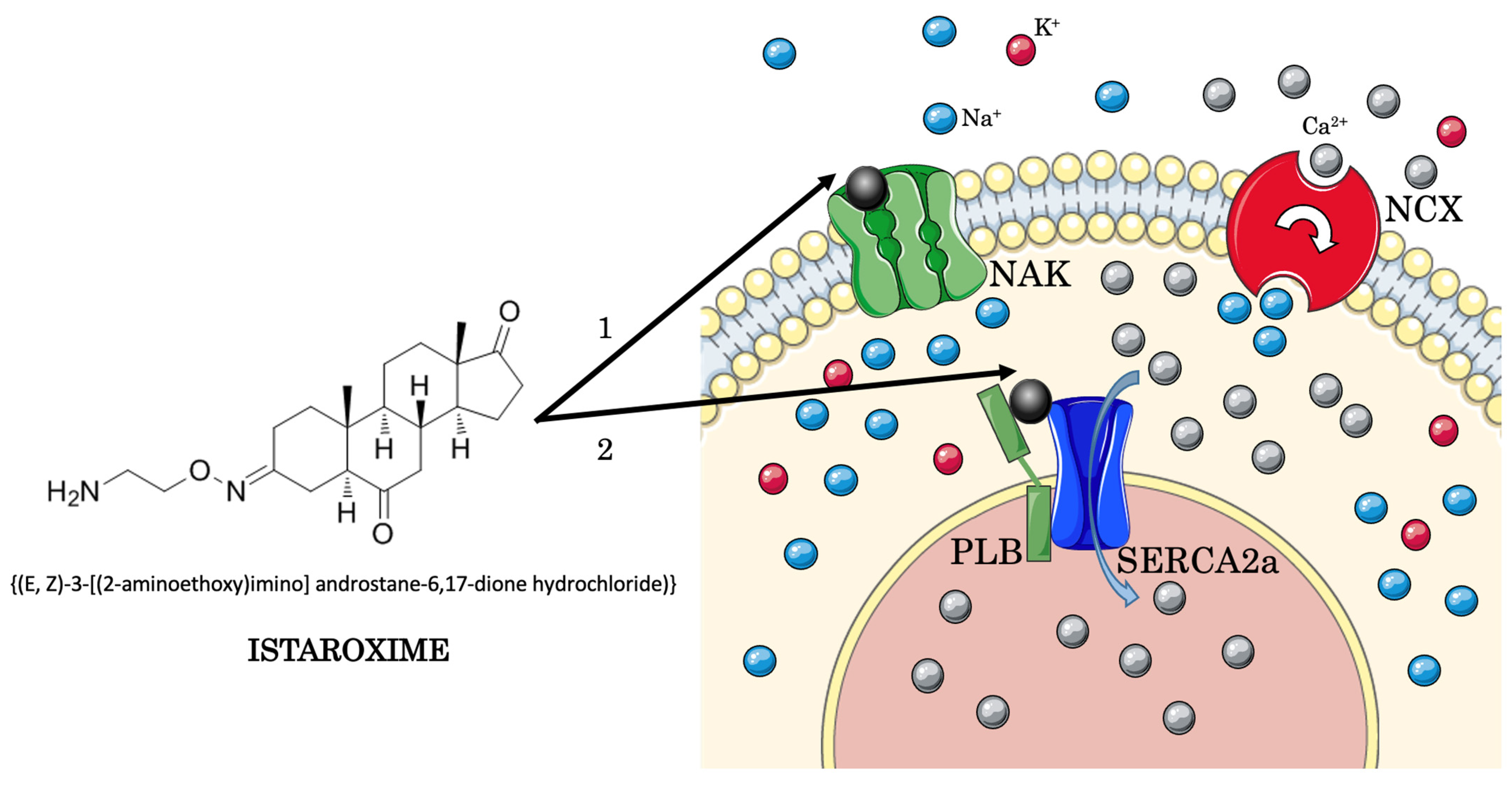
5. Istaroxime
Other Therapeutical Applications of Istaroxime
6. Preclinical Studies
7. Clinical Investigations
8. Future Perspectives
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Santulli, G.; Wang, X.; Mone, P. Updated ACC/AHA/HFSA 2022 guidelines on heart failure: What is new? From epidemiology to clinical management. Eur. Heart J. Cardiovasc. Pharmacother. 2022, 8, e23–e24. [Google Scholar] [CrossRef]
- Savarese, G.; Becher, P.M.; Lund, L.H.; Seferovic, P.; Rosano, G.M.C.; Coats, A. Global burden of heart failure: A com-prehensive and updated review of epidemiology. Cardiovasc. Res. 2022. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Jenca, D.; Melenovsky, V.; Stehlik, J.; Stanek, V.; Kettner, J.; Kautzner, J.; Adamkova, V.; Wohlfahrt, P. Heart failure after myocardial infarction: Incidence and predictors. ESC Heart Fail. 2021, 8, 222–237. [Google Scholar] [CrossRef]
- Huffman, M.D.; Berry, J.D.; Ning, H.; Dyer, A.R.; Garside, D.B.; Cai, X.; Daviglus, M.L.; Lloyd-Jones, D.M. Lifetime risk for heart failure among white and black Americans: Cardiovascular lifetime risk pooling project. J. Am. Coll. Cardiol. 2013, 61, 1510–1517. [Google Scholar] [CrossRef] [Green Version]
- Emmons-Bell, S.; Johnson, C.; Roth, G. Prevalence, incidence and survival of heart failure: A systematic review. Heart 2022, 108, 1351–1360. [Google Scholar] [CrossRef]
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2021 Update: A Report From the American Heart Association. Circulation 2021, 143, e254–e743. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Albert, N.M.; Allen, L.A.; Bluemke, D.A.; Butler, J.; Fonarow, G.C.; Ikonomidis, J.S.; Khavjou, O.; Konstam, M.A.; Maddox, T.M.; et al. Forecasting the impact of heart failure in the United States: A policy statement from the American Heart Association. Circ. Heart Fail. 2013, 6, 606–619. [Google Scholar] [CrossRef] [Green Version]
- Masip, J.; Frank Peacok, W.; Arrigo, M.; Rossello, X.; Platz, E.; Cullen, L.; Mebazaa, A.; Price, S.; Bueno, H.; Di Somma, S.; et al. Acute Heart Failure in the 2021 ESC Heart Failure Guidelines: A scientific statement from the Association for Acute CardioVascular Care (ACVC) of the European Society of Cardiology. Eur. Heart J. Acute Cardiovasc. Care 2022, 11, 173–185. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e895–e1032. [Google Scholar] [CrossRef]
- Kurmani, S.; Squire, I. Acute Heart Failure: Definition, Classification and Epidemiology. Curr. Heart Fail. Rep. 2017, 14, 385–392. [Google Scholar] [CrossRef]
- Nieminen, M.S.; Harjola, V.P. Definition and epidemiology of acute heart failure syndromes. Am. J. Cardiol. 2005, 96, 5G–10G. [Google Scholar] [CrossRef] [PubMed]
- Gheorghiade, M.; Zannad, F.; Sopko, G.; Klein, L.; Pina, I.L.; Konstam, M.A.; Massie, B.M.; Roland, E.; Targum, S.; Collins, S.P.; et al. Acute heart failure syndromes: Current state and framework for future research. Circulation 2005, 112, 3958–3968. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ter Maaten, J.M.; Valente, M.A.; Damman, K.; Hillege, H.L.; Navis, G.; Voors, A.A. Diuretic response in acute heart failure-pathophysiology, evaluation, and therapy. Nat. Rev. Cardiol. 2015, 12, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Masip, J.; Peacock, W.F.; Price, S.; Cullen, L.; Martin-Sanchez, F.J.; Seferovic, P.; Maisel, A.S.; Miro, O.; Filippatos, G.; Vrints, C.; et al. Indications and practical approach to non-invasive ventilation in acute heart failure. Eur. Heart J. 2018, 39, 17–25. [Google Scholar] [CrossRef] [Green Version]
- Schumann, J.; Henrich, E.C.; Strobl, H.; Prondzinsky, R.; Weiche, S.; Thiele, H.; Werdan, K.; Frantz, S.; Unverzagt, S. Inotropic agents and vasodilator strategies for the treatment of cardiogenic shock or low cardiac output syndrome. Cochrane Database Syst. Rev. 2018, 1, CD009669. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.S.; Shim, H.; Cho, Y.H. Mechanical Circulatory Support for Acute Heart Failure Complicated by Cardiogenic Shock. Int. J. Heart Fail. 2020, 2, 23–44. [Google Scholar] [CrossRef] [Green Version]
- Mebazaa, A.; Tolppanen, H.; Mueller, C.; Lassus, J.; DiSomma, S.; Baksyte, G.; Cecconi, M.; Choi, D.J.; Cohen Solal, A.; Christ, M.; et al. Acute heart failure and cardiogenic shock: A multidisciplinary practical guidance. Intensive Care Med. 2016, 42, 147–163. [Google Scholar] [CrossRef]
- Thiele, H.; Zeymer, U.; Neumann, F.J.; Ferenc, M.; Olbrich, H.G.; Hausleiter, J.; Richardt, G.; Hennersdorf, M.; Empen, K.; Fuernau, G.; et al. Intraaortic balloon support for myocardial infarction with cardiogenic shock. N. Engl. J. Med. 2012, 367, 1287–1296. [Google Scholar] [CrossRef] [Green Version]
- Abraham, W.T.; Adams, K.F.; Fonarow, G.C.; Costanzo, M.R.; Berkowitz, R.L.; LeJemtel, T.H.; Cheng, M.L.; Wynne, J.; Committee, A.S.A.; ADHERE Scientific Advisory Committee and Investigators; et al. In-hospital mortality in patients with acute decompensated heart failure requiring intravenous vasoactive medications: An analysis from the Acute Decompensated Heart Failure National Registry (ADHERE). J. Am. Coll. Cardiol. 2005, 46, 57–64. [Google Scholar] [CrossRef] [Green Version]
- Nieminen, M.S.; Brutsaert, D.; Dickstein, K.; Drexler, H.; Follath, F.; Harjola, V.P.; Hochadel, M.; Komajda, M.; Lassus, J.; Lopez-Sendon, J.L.; et al. EuroHeart Failure Survey II (EHFS II): A survey on hospitalized acute heart failure patients: Description of population. Eur. Heart J. 2006, 27, 2725–2736. [Google Scholar] [CrossRef]
- Abraham, W.T.; Fonarow, G.C.; Albert, N.M.; Stough, W.G.; Gheorghiade, M.; Greenberg, B.H.; O’Connor, C.M.; Sun, J.L.; Yancy, C.W.; Young, J.B.; et al. Predictors of in-hospital mortality in patients hospitalized for heart failure: Insights from the Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF). J. Am. Coll. Cardiol. 2008, 52, 347–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Matteis, G.; Covino, M.; Burzo, M.L.; Della Polla, D.A.; Franceschi, F.; Mebazaa, A.; Gambassi, G. Clinical Characteristics and Predictors of In-Hospital Mortality among Older Patients with Acute Heart Failure. J. Clin. Med. 2022, 11, 439. [Google Scholar] [CrossRef] [PubMed]
- Spinar, J.; Parenica, J.; Vitovec, J.; Widimsky, P.; Linhart, A.; Fedorco, M.; Malek, F.; Cihalik, C.; Spinarova, L.; Miklik, R.; et al. Baseline characteristics and hospital mortality in the Acute Heart Failure Database (AHEAD) Main registry. Crit. Care 2011, 15, R291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kansakar, U.; Varzideh, F.; Jankauskas, S.S.; Gambardella, J.; Trimarco, B.; Santulli, G. Advances in the understanding of excitation-contraction coupling: The pulsing quest for drugs against heart failure and arrhythmias. Eur. Heart J. Cardiovasc. Pharmacother. 2021, 7, e91–e93. [Google Scholar] [CrossRef] [PubMed]
- Psotka, M.A.; Gottlieb, S.S.; Francis, G.S.; Allen, L.A.; Teerlink, J.R.; Adams, K.F., Jr.; Rosano, G.M.C.; Lancellotti, P. Cardiac Calcitropes, Myotropes, and Mitotropes: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2019, 73, 2345–2353. [Google Scholar] [CrossRef]
- van Diepen, S.; Katz, J.N.; Albert, N.M.; Henry, T.D.; Jacobs, A.K.; Kapur, N.K.; Kilic, A.; Menon, V.; Ohman, E.M.; Sweitzer, N.K.; et al. Contemporary Management of Cardiogenic Shock: A Scientific Statement From the American Heart Association. Circulation 2017, 136, e232–e268. [Google Scholar] [CrossRef]
- Tavares, M.; Rezlan, E.; Vostroknoutova, I.; Khouadja, H.; Mebazaa, A. New pharmacologic therapies for acute heart failure. Crit. Care Med. 2008, 36, S112–S120. [Google Scholar] [CrossRef]
- Skou, J.C. The influence of some cations on an adenosine triphosphatase from peripheral nerves. Biochim. Biophys. Acta 1957, 23, 394–401. [Google Scholar] [CrossRef]
- Manoj, K.M.; Gideon, D.A.; Bazhin, N.M.; Tamagawa, H.; Nirusimhan, V.; Kavdia, M.; Jaeken, L. Na,K-ATPase: A murzyme facilitating thermodynamic equilibriums at the membrane-interface. J. Cell Physiol. 2022, in press. [Google Scholar] [CrossRef]
- Fedosova, N.U.; Habeck, M.; Nissen, P. Structure and Function of Na,K-ATPase-The Sodium-Potassium Pump. Compr. Physiol. 2021, 12, 2659–2679. [Google Scholar] [CrossRef]
- Morth, J.P.; Pedersen, B.P.; Toustrup-Jensen, M.S.; Sorensen, T.L.; Petersen, J.; Andersen, J.P.; Vilsen, B.; Nissen, P. Crystal structure of the sodium-potassium pump. Nature 2007, 450, 1043–1049. [Google Scholar] [CrossRef]
- Kanai, R.; Cornelius, F.; Ogawa, H.; Motoyama, K.; Vilsen, B.; Toyoshima, C. Binding of cardiotonic steroids to Na(+),K(+)-ATPase in the E2P state. Proc. Natl. Acad. Sci. USA 2021, 118, e2020438118. [Google Scholar] [CrossRef]
- Kravtsova, V.V.; Bouzinova, E.V.; Matchkov, V.V.; Krivoi, I.I. Skeletal Muscle Na,K-ATPase as a Target for Circulating Ouabain. Int. J. Mol. Sci. 2020, 21, 2875. [Google Scholar] [CrossRef] [Green Version]
- Triana-Martinez, F.; Picallos-Rabina, P.; Da Silva-Alvarez, S.; Pietrocola, F.; Llanos, S.; Rodilla, V.; Soprano, E.; Pedrosa, P.; Ferreiros, A.; Barradas, M.; et al. Identification and characterization of Cardiac Glycosides as senolytic compounds. Nat. Commun. 2019, 10, 4731. [Google Scholar] [CrossRef] [Green Version]
- Altamirano, J.; Li, Y.; DeSantiago, J.; Piacentino, V., 3rd; Houser, S.R.; Bers, D.M. The inotropic effect of cardioactive glycosides in ventricular myocytes requires Na+-Ca2+ exchanger function. J. Physiol. 2006, 575, 845–854. [Google Scholar] [CrossRef]
- Shattock, M.J.; Ottolia, M.; Bers, D.M.; Blaustein, M.P.; Boguslavskyi, A.; Bossuyt, J.; Bridge, J.H.; Chen-Izu, Y.; Clancy, C.E.; Edwards, A.; et al. Na+/Ca2+ exchange and Na+/K+-ATPase in the heart. J. Physiol. 2015, 593, 1361–1382. [Google Scholar] [CrossRef] [Green Version]
- Primeau, J.O.; Armanious, G.P.; Fisher, M.E.; Young, H.S. The SarcoEndoplasmic Reticulum Calcium ATPase. Subcell. Biochem. 2018, 87, 229–258. [Google Scholar] [CrossRef]
- Tada, M.; Kadoma, M.; Fujii, J.; Kimura, Y.; Kijima, Y. Molecular structure and function of phospholamban: The regulatory protein of calcium pump in cardiac sarcoplasmic reticulum. Adv. Exp. Med. Biol. 1989, 255, 79–89. [Google Scholar] [CrossRef]
- Gruber, S.J.; Haydon, S.; Thomas, D.D. Phospholamban mutants compete with wild type for SERCA binding in living cells. Biochem. Biophys. Res. Commun. 2012, 420, 236–240. [Google Scholar] [CrossRef] [Green Version]
- Arnold, M.E.; Dostmann, W.R.; Martin, J.; Previs, M.J.; Palmer, B.; LeWinter, M.; Meyer, M. SERCA2a-phospholamban interaction monitored by an interposed circularly permutated green fluorescent protein. Am. J. Physiol. Heart Circ. Physiol. 2021, 320, H2188–H2200. [Google Scholar] [CrossRef]
- Liu, Y.; Chen, J.; Fontes, S.K.; Bautista, E.N.; Cheng, Z. Physiological and pathological roles of protein kinase A in the heart. Cardiovasc. Res. 2022, 118, 386–398. [Google Scholar] [CrossRef] [PubMed]
- Izzo, R.; Cipolletta, E.; Ciccarelli, M.; Campanile, A.; Santulli, G.; Palumbo, G.; Vasta, A.; Formisano, S.; Trimarco, B.; Iaccarino, G. Enhanced GRK2 expression and desensitization of betaAR vasodilatation in hypertensive patients. Clin. Transl. Sci. 2008, 1, 215–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santulli, G.; Campanile, A.; Spinelli, L.; Assante di Panzillo, E.; Ciccarelli, M.; Trimarco, B.; Iaccarino, G. G protein-coupled receptor kinase 2 in patients with acute myocardial infarction. Am. J. Cardiol. 2011, 107, 1125–1130. [Google Scholar] [CrossRef]
- Sorriento, D.; Ciccarelli, M.; Santulli, G.; Illario, M.; Trimarco, B.; Iaccarino, G. Trafficking GRK2: Cellular and Metabolic consequences of GRK2 subcellular localization. Transl. Med. UniSa 2014, 10, 3–7. [Google Scholar]
- Sorriento, D.; Santulli, G.; Franco, A.; Cipolletta, E.; Napolitano, L.; Gambardella, J.; Gomez-Monterrey, I.; Campiglia, P.; Trimarco, B.; Iaccarino, G.; et al. Integrating GRK2 and NFkappaB in the Pathophysiology of Cardiac Hypertrophy. J. Cardiovasc. Transl. Res. 2015, 8, 493–502. [Google Scholar] [CrossRef]
- Selby, D.E.; Palmer, B.M.; LeWinter, M.M.; Meyer, M. Tachycardia-induced diastolic dysfunction and resting tone in myocardium from patients with a normal ejection fraction. J. Am. Coll. Cardiol. 2011, 58, 147–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhalla, N.S.; Panagia, V.; Singal, P.K.; Makino, N.; Dixon, I.M.; Eyolfson, D.A. Alterations in heart membrane calcium transport during the development of ischemia-reperfusion injury. J. Mol. Cell. Cardiol. 1988, 20 (Suppl. S2), 3–13. [Google Scholar] [CrossRef] [PubMed]
- Gambardella, J.; Wang, X.J.; Ferrara, J.; Morelli, M.B.; Santulli, G. Cardiac BIN1 Replacement Therapy Ameliorates Inotropy and Lusitropy in Heart Failure by Regulating Calcium Handling. JACC Basic Transl. Sci. 2020, 5, 579–581. [Google Scholar] [CrossRef]
- Santulli, G.; Iaccarino, G. Adrenergic signaling in heart failure and cardiovascular aging. Maturitas 2016, 93, 65–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciccarelli, M.; Santulli, G.; Pascale, V.; Trimarco, B.; Iaccarino, G. Adrenergic receptors and metabolism: Role in development of cardiovascular disease. Front. Physiol. 2013, 4, 265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santulli, G. Adrenal signaling in heart failure: Something more than a distant ship’s smoke on the horizon. Hypertension 2014, 63, 215–216. [Google Scholar] [CrossRef] [PubMed]
- Gambardella, J.; Jankauskas, S.S.; D’Ascia, S.L.; Sardu, C.; Matarese, A.; Minicucci, F.; Mone, P.; Santulli, G. Glycation of ryanodine receptor in circulating lymphocytes predicts the response to cardiac resynchronization therapy. J. Heart Lung Transplant. 2022, 41, 438–441. [Google Scholar] [CrossRef] [PubMed]
- Jin, X.; Amoni, M.; Gilbert, G.; Dries, E.; Donate Puertas, R.; Tomar, A.; Nagaraju, C.K.; Pradhan, A.; Yule, D.I.; Martens, T.; et al. InsP(3)R-RyR Ca(2+) channel crosstalk facilitates arrhythmias in the failing human ventricle. Basic Res. Cardiol. 2022, 117, 60. [Google Scholar] [CrossRef] [PubMed]
- Santulli, G.; Lewis, D.; des Georges, A.; Marks, A.R.; Frank, J. Ryanodine Receptor Structure and Function in Health and Disease. Subcell. Biochem. 2018, 87, 329–352. [Google Scholar] [CrossRef] [Green Version]
- Braunwald, E. Heart failure. JACC Heart Fail. 2013, 1, 1–20. [Google Scholar] [CrossRef]
- Maning, J.; Desimine, V.L.; Pollard, C.M.; Ghandour, J.; Lymperopoulos, A. Carvedilol Selectively Stimulates betaArrestin2-Dependent SERCA2a Activity in Cardiomyocytes to Augment Contractility. Int. J. Mol. Sci. 2022, 23, 11315. [Google Scholar] [CrossRef]
- Chung, Y.J.; Luo, A.; Park, K.C.; Loonat, A.A.; Lakhal-Littleton, S.; Robbins, P.A.; Swietach, P. Iron-deficiency anemia reduces cardiac contraction by downregulating RyR2 channels and suppressing SERCA pump activity. JCI Insight 2019, 4, e125618. [Google Scholar] [CrossRef] [Green Version]
- Gambardella, J.; Trimarco, B.; Iaccarino, G.; Santulli, G. New Insights in Cardiac Calcium Handling and Excitation-Contraction Coupling. Adv. Exp. Med. Biol. 2018, 1067, 373–385. [Google Scholar] [CrossRef] [Green Version]
- Kushnir, A.; Santulli, G.; Reiken, S.R.; Coromilas, E.; Godfrey, S.J.; Brunjes, D.L.; Colombo, P.C.; Yuzefpolskaya, M.; Sokol, S.I.; Kitsis, R.N.; et al. Ryanodine Receptor Calcium Leak in Circulating B-Lymphocytes as a Biomarker in Heart Failure. Circulation 2018, 138, 1144–1154. [Google Scholar] [CrossRef]
- Santulli, G.; Nakashima, R.; Yuan, Q.; Marks, A.R. Intracellular calcium release channels: An update. J. Physiol. 2017, 595, 3041–3051. [Google Scholar] [CrossRef] [Green Version]
- Sardu, C.; Santulli, G.; Guerra, G.; Trotta, M.C.; Santamaria, M.; Sacra, C.; Testa, N.; Ducceschi, V.; Gatta, G.; Amico, M.; et al. Modulation of SERCA in Patients with Persistent Atrial Fibrillation Treated by Epicardial Thoracoscopic Ablation: The CAMAF Study. J. Clin. Med. 2020, 9, 544. [Google Scholar] [CrossRef]
- Hoydal, M.A.; Kirkeby-Garstad, I.; Karevold, A.; Wiseth, R.; Haaverstad, R.; Wahba, A.; Stolen, T.L.; Contu, R.; Condorelli, G.; Ellingsen, O.; et al. Human cardiomyocyte calcium handling and transverse tubules in mid-stage of post-myocardial-infarction heart failure. ESC Heart Fail. 2018, 5, 332–342. [Google Scholar] [CrossRef] [Green Version]
- Rocchetti, M.; Alemanni, M.; Mostacciuolo, G.; Barassi, P.; Altomare, C.; Chisci, R.; Micheletti, R.; Ferrari, P.; Zaza, A. Modulation of sarcoplasmic reticulum function by PST2744 [istaroxime; (E,Z)-3-((2-aminoethoxy)imino) androstane-6,17-dione hydrochloride)] in a pressure-overload heart failure model. J. Pharmacol. Exp. Ther. 2008, 326, 957–965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arici, M.; Ferrandi, M.; Barassi, P.; Hsu, S.C.; Torre, E.; Luraghi, A.; Ronchi, C.; Chang, G.J.; Peri, F.; Ferrari, P.; et al. Istaroxime metabolite PST3093 selectively stimulates SERCA2a and reverses disease-induced changes in cardiac function. J. Pharmacol. Exp. Ther. 2022, in press. [Google Scholar] [CrossRef] [PubMed]
- Khan, H.; Metra, M.; Blair, J.E.; Vogel, M.; Harinstein, M.E.; Filippatos, G.S.; Sabbah, H.N.; Porchet, H.; Valentini, G.; Gheorghiade, M. Istaroxime, a first in class new chemical entity exhibiting SERCA-2 activation and Na-K-ATPase inhibition: A new promising treatment for acute heart failure syndromes? Heart Fail. Rev. 2009, 14, 277–287. [Google Scholar] [CrossRef] [PubMed]
- Cornelius, F.; Mahmmoud, Y.A.; Toyoshima, C. Metal fluoride complexes of Na,K-ATPase: Characterization of fluoride-stabilized phosphoenzyme analogues and their interaction with cardiotonic steroids. J. Biol. Chem. 2011, 286, 29882–29892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Micheletti, R.; Mattera, G.G.; Rocchetti, M.; Schiavone, A.; Loi, M.F.; Zaza, A.; Gagnol, R.J.; De Munari, S.; Melloni, P.; Carminati, P.; et al. Pharmacological profile of the novel inotropic agent (E,Z)-3-((2-aminoethoxy)imino)androstane-6,17-dione hydrochloride (PST2744). J. Pharmacol. Exp. Ther. 2002, 303, 592–600. [Google Scholar] [CrossRef] [Green Version]
- Ferrandi, M.; Barassi, P.; Tadini-Buoninsegni, F.; Bartolommei, G.; Molinari, I.; Tripodi, M.G.; Reina, C.; Moncelli, M.R.; Bianchi, G.; Ferrari, P. Istaroxime stimulates SERCA2a and accelerates calcium cycling in heart failure by relieving phospholamban inhibition. Br. J. Pharmacol. 2013, 169, 1849–1861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bossu, A.; Kostense, A.; Beekman, H.D.M.; Houtman, M.J.C.; van der Heyden, M.A.G.; Vos, M.A. Istaroxime, a positive inotropic agent devoid of proarrhythmic properties in sensitive chronic atrioventricular block dogs. Pharmacol. Res. 2018, 133, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Schwinger, R.H.; Brixius, K.; Bavendiek, U.; Hoischen, S.; Muller-Ehmsen, J.; Bolck, B.; Erdmann, E. Effect of cyclopiazonic acid on the force-frequency relationship in human nonfailing myocardium. J. Pharmacol. Exp. Ther. 1997, 283, 286–292. [Google Scholar] [PubMed]
- Abrol, N.; de Tombe, P.P.; Robia, S.L. Acute inotropic and lusitropic effects of cardiomyopathic R9C mutation of phospholamban. J. Biol. Chem. 2015, 290, 7130–7140. [Google Scholar] [CrossRef] [PubMed]
- Alemanni, M.; Rocchetti, M.; Re, D.; Zaza, A. Role and mechanism of subcellular Ca2+ distribution in the action of two inotropic agents with different toxicity. J. Mol. Cell. Cardiol. 2011, 50, 910–918. [Google Scholar] [CrossRef] [PubMed]
- Alevizopoulos, K.; Dimas, K.; Papadopoulou, N.; Schmidt, E.M.; Tsapara, A.; Alkahtani, S.; Honisch, S.; Prousis, K.C.; Alarifi, S.; Calogeropoulou, T.; et al. Functional characterization and anti-cancer action of the clinical phase II cardiac Na+/K+ ATPase inhibitor istaroxime: In vitro and in vivo properties and cross talk with the membrane androgen receptor. Oncotarget 2016, 7, 24415–24428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stagno, M.J.; Zacharopoulou, N.; Bochem, J.; Tsapara, A.; Pelzl, L.; Al-Maghout, T.; Kallergi, G.; Alkahtani, S.; Alevizopoulos, K.; Dimas, K.; et al. Istaroxime Inhibits Motility and Down-Regulates Orai1 Expression, SOCE and FAK Phosphorylation in Prostate Cancer Cells. Cell. Physiol. Biochem. 2017, 42, 1366–1376. [Google Scholar] [CrossRef] [Green Version]
- Wallner, M.; Khafaga, M.; Kolesnik, E.; Vafiadis, A.; Schwantzer, G.; Eaton, D.M.; Curcic, P.; Kostenberger, M.; Knez, I.; Rainer, P.P.; et al. Istaroxime, a potential anticancer drug in prostate cancer, exerts beneficial functional effects in healthy and diseased human myocardium. Oncotarget 2017, 8, 49264–49274. [Google Scholar] [CrossRef] [Green Version]
- Mijatovic, T.; Van Quaquebeke, E.; Delest, B.; Debeir, O.; Darro, F.; Kiss, R. Cardiotonic steroids on the road to anti-cancer therapy. Biochim. Biophys. Acta 2007, 1776, 32–57. [Google Scholar] [CrossRef]
- Torre, E.; Arici, M.; Lodrini, A.M.; Ferrandi, M.; Barassi, P.; Hsu, S.C.; Chang, G.J.; Boz, E.; Sala, E.; Vagni, S.; et al. SERCA2a stimulation by istaroxime improves intracellular Ca2+ handling and diastolic dysfunction in a model of diabetic cardiomyopathy. Cardiovasc. Res. 2022, 118, 1020–1032. [Google Scholar] [CrossRef]
- Sabbah, H.N.; Imai, M.; Cowart, D.; Amato, A.; Carminati, P.; Gheorghiade, M. Hemodynamic properties of a new-generation positive luso-inotropic agent for the acute treatment of advanced heart failure. Am. J. Cardiol. 2007, 99, 41A–46A. [Google Scholar] [CrossRef]
- Adamson, P.B.; Vanoli, E.; Mattera, G.G.; Germany, R.; Gagnol, J.P.; Carminati, P.; Schwartz, P.J. Hemodynamic effects of a new inotropic compound, PST-2744, in dogs with chronic ischemic heart failure. J. Cardiovasc. Pharmacol. 2003, 42, 169–173. [Google Scholar] [CrossRef]
- Lo Giudice, P.; Mattera, G.G.; Gagnol, J.P.; Borsini, F. Chronic istaroxime improves cardiac function and heart rate variability in cardiomyopathic hamsters. Cardiovasc. Drugs Ther. 2011, 25, 133–138. [Google Scholar] [CrossRef]
- Rocchetti, M.; Besana, A.; Mostacciuolo, G.; Ferrari, P.; Micheletti, R.; Zaza, A. Diverse toxicity associated with cardiac Na+/K+ pump inhibition: Evaluation of electrophysiological mechanisms. J. Pharmacol. Exp. Ther. 2003, 305, 765–771. [Google Scholar] [CrossRef] [PubMed]
- Tseng, G.N.; Wit, A.L. Characteristics of a transient inward current that causes delayed afterdepolarizations in atrial cells of the canine coronary sinus. J. Mol. Cell. Cardiol. 1987, 19, 1105–1119. [Google Scholar] [CrossRef] [PubMed]
- Hancox, J.C.; Levi, A.J. Actions of the digitalis analogue strophanthidin on action potentials and L-type calcium current in single cells isolated from the rabbit atrioventricular node. Br. J. Pharmacol. 1996, 118, 1447–1454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holmes, M.; Hurley, M.E.; Sheard, T.M.D.; Benson, A.P.; Jayasinghe, I.; Colman, M.A. Increased SERCA2a sub-cellular heterogeneity in right-ventricular heart failure inhibits excitation-contraction coupling and modulates arrhythmogenic dynamics. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2022, 377, 20210317. [Google Scholar] [CrossRef]
- Racioppi, M.F.; Burgos, J.I.; Morell, M.; Gonano, L.A.; Vila Petroff, M. Cellular Mechanisms Underlying the Low Cardiotoxicity of Istaroxime. J. Am. Heart Assoc. 2021, 10, e018833. [Google Scholar] [CrossRef]
- Ghali, J.K.; Smith, W.B.; Torre-Amione, G.; Haynos, W.; Rayburn, B.K.; Amato, A.; Zhang, D.; Cowart, D.; Valentini, G.; Carminati, P.; et al. A phase 1-2 dose-escalating study evaluating the safety and tolerability of istaroxime and specific effects on electrocardiographic and hemodynamic parameters in patients with chronic heart failure with reduced systolic function. Am. J. Cardiol. 2007, 99, S47–S56. [Google Scholar] [CrossRef]
- Blair, J.E.; Macarie, C.; Ruzyllo, W.; Bacchieri, A.; Valentini, G.; Bianchetti, M.; Pang, P.S.; Harinstein, M.E.; Sabbah, H.N.; Filippatos, G.S.; et al. Rationale and design of the hemodynamic, echocardiographic and neurohormonal effects of istaroxime, a novel intravenous inotropic and lusitropic agent: A randomized controlled trial in patients hospitalized with heart failure (HORIZON-HF) trial. Am. J. Ther. 2008, 15, 231–240. [Google Scholar] [CrossRef]
- Shah, S.J.; Blair, J.E.; Filippatos, G.S.; Macarie, C.; Ruzyllo, W.; Korewicki, J.; Bubenek-Turconi, S.I.; Ceracchi, M.; Bianchetti, M.; Carminati, P.; et al. Effects of istaroxime on diastolic stiffness in acute heart failure syndromes: Results from the Hemodynamic, Echocardiographic, and Neurohormonal Effects of Istaroxime, a Novel Intravenous Inotropic and Lusitropic Agent: A Randomized Controlled Trial in Patients Hospitalized with Heart Failure (HORIZON-HF) trial. Am. Heart J. 2009, 157, 1035–1041. [Google Scholar] [CrossRef]
- Gheorghiade, M.; Blair, J.E.; Filippatos, G.S.; Macarie, C.; Ruzyllo, W.; Korewicki, J.; Bubenek-Turconi, S.I.; Ceracchi, M.; Bianchetti, M.; Carminati, P.; et al. Hemodynamic, echocardiographic, and neurohormonal effects of istaroxime, a novel intravenous inotropic and lusitropic agent: A randomized controlled trial in patients hospitalized with heart failure. J. Am. Coll. Cardiol. 2008, 51, 2276–2285. [Google Scholar] [CrossRef] [Green Version]
- Carubelli, V.; Zhang, Y.; Metra, M.; Lombardi, C.; Felker, G.M.; Filippatos, G.; O’Connor, C.M.; Teerlink, J.R.; Simmons, P.; Segal, R.; et al. Treatment with 24 hour istaroxime infusion in patients hospitalised for acute heart failure: A randomised, placebo-controlled trial. Eur. J. Heart Fail. 2020, 22, 1684–1693. [Google Scholar] [CrossRef]
- Thomas, S.S.; Nohria, A. Hemodynamic classifications of acute heart failure and their clinical application:—An update. Circ. J. 2012, 76, 278–286. [Google Scholar] [CrossRef] [PubMed]
- Weatherley, B.D.; Milo-Cotter, O.; Felker, G.M.; Uriel, N.; Kaluski, E.; Vered, Z.; O’Connor, C.M.; Adams, K.F.; Cotter, G. Early worsening heart failure in patients admitted with acute heart failure—A new outcome measure associated with long-term prognosis? Fundam. Clin. Pharmacol. 2009, 23, 633–639. [Google Scholar] [CrossRef]
- Metra, M.; Chioncel, O.; Cotter, G.; Davison, B.; Filippatos, G.; Mebazaa, A.; Novosadova, M.; Ponikowski, P.; Simmons, P.; Soffer, J.; et al. Safety and efficacy of istaroxime in patients with acute heart failure-related pre-cardiogenic shock—A multicentre, randomized, double-blind, placebo-controlled, parallel group study (SEISMiC). Eur. J. Heart Fail. 2022, 24, 1967–1977. [Google Scholar] [CrossRef] [PubMed]
- Luciani, P.; Fevre, M.; Leroux, J.C. Development and physico-chemical characterization of a liposomal formulation of istaroxime. Eur. J. Pharm. Biopharm. 2011, 79, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, T.M. Newer inotropes in pediatric heart failure. J. Cardiovasc. Pharmacol. 2011, 58, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Luraghi, A.; Ferrandi, M.; Barassi, P.; Arici, M.; Hsu, S.C.; Torre, E.; Ronchi, C.; Romerio, A.; Chang, G.J.; Ferrari, P.; et al. Highly Selective SERCA2a Activators: Preclinical Development of a Congeneric Group of First-in-Class Drug Leads against Heart Failure. J. Med. Chem. 2022, 65, 7324–7333. [Google Scholar] [CrossRef]
- Lyon, A.R.; Samara, M.A.; Feldman, D.S. Cardiac contractility modulation therapy in advanced systolic heart failure. Nat. Rev. Cardiol. 2013, 10, 584–598. [Google Scholar] [CrossRef]
- Abi-Samra, F.; Gutterman, D. Cardiac contractility modulation: A novel approach for the treatment of heart failure. Heart Fail. Rev. 2016, 21, 645–660. [Google Scholar] [CrossRef] [Green Version]
- Neelagaru, S.B.; Sanchez, J.E.; Lau, S.K.; Greenberg, S.M.; Raval, N.Y.; Worley, S.; Kalman, J.; Merliss, A.D.; Krueger, S.; Wood, M.; et al. Nonexcitatory, cardiac contractility modulation electrical impulses: Feasibility study for advanced heart failure in patients with normal QRS duration. Heart Rhythm 2006, 3, 1140–1147. [Google Scholar] [CrossRef]
- Borggrefe, M.M.; Lawo, T.; Butter, C.; Schmidinger, H.; Lunati, M.; Pieske, B.; Misier, A.R.; Curnis, A.; Bocker, D.; Remppis, A.; et al. Randomized, double blind study of non-excitatory, cardiac contractility modulation electrical impulses for symptomatic heart failure. Eur. Heart J. 2008, 29, 1019–1028. [Google Scholar] [CrossRef] [PubMed]
- Kadish, A.; Nademanee, K.; Volosin, K.; Krueger, S.; Neelagaru, S.; Raval, N.; Obel, O.; Weiner, S.; Wish, M.; Carson, P.; et al. A randomized controlled trial evaluating the safety and efficacy of cardiac contractility modulation in advanced heart failure. Am. Heart J. 2011, 161, 329–337.e2. [Google Scholar] [CrossRef] [PubMed]
- Abraham, W.T.; Nademanee, K.; Volosin, K.; Krueger, S.; Neelagaru, S.; Raval, N.; Obel, O.; Weiner, S.; Wish, M.; Carson, P.; et al. Subgroup analysis of a randomized controlled trial evaluating the safety and efficacy of cardiac contractility modulation in advanced heart failure. J. Card. Fail. 2011, 17, 710–717. [Google Scholar] [CrossRef] [PubMed]
- Abraham, W.T.; Kuck, K.H.; Goldsmith, R.L.; Lindenfeld, J.; Reddy, V.Y.; Carson, P.E.; Mann, D.L.; Saville, B.; Parise, H.; Chan, R.; et al. A Randomized Controlled Trial to Evaluate the Safety and Efficacy of Cardiac Contractility Modulation. JACC Heart Fail. 2018, 6, 874–883. [Google Scholar] [CrossRef] [PubMed]
- Wiegn, P.; Chan, R.; Jost, C.; Saville, B.R.; Parise, H.; Prutchi, D.; Carson, P.E.; Stagg, A.; Goldsmith, R.L.; Burkhoff, D. Safety, Performance, and Efficacy of Cardiac Contractility Modulation Delivered by the 2-Lead Optimizer Smart System: The FIX-HF-5C2 Study. Circ. Heart Fail. 2020, 13, e006512. [Google Scholar] [CrossRef]
- Muller, D.; Remppis, A.; Schauerte, P.; Schmidt-Schweda, S.; Burkhoff, D.; Rousso, B.; Gutterman, D.; Senges, J.; Hindricks, G.; Kuck, K.H. Clinical effects of long-term cardiac contractility modulation (CCM) in subjects with heart failure caused by left ventricular systolic dysfunction. Clin. Res. Cardiol. 2017, 106, 893–904. [Google Scholar] [CrossRef] [Green Version]
- Liu, M.; Fang, F.; Luo, X.X.; Shlomo, B.H.; Burkhoff, D.; Chan, J.Y.; Chan, C.P.; Cheung, L.; Rousso, B.; Gutterman, D.; et al. Improvement of long-term survival by cardiac contractility modulation in heart failure patients: A case-control study. Int. J. Cardiol. 2016, 206, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Masarone, D.; Kittleson, M.M.; De Vivo, S.; D’Onofrio, A.; Ammendola, E.; Nigro, G.; Contaldi, C.; Martucci, M.L.; Errigo, V.; Pacileo, G. The Effects of Device-Based Cardiac Contractility Modulation Therapy on Left Ventricle Global Longitudinal Strain and Myocardial Mechano-Energetic Efficiency in Patients with Heart Failure with Reduced Ejection Fraction. J. Clin. Med. 2022, 11, 5866. [Google Scholar] [CrossRef]
- Avvisato, R.; Jankauskas, S.S.; Santulli, G. Istaroxime and Beyond: New Therapeutic Strategies to Specifically Activate SERCA and Treat Heart Failure. J. Pharmacol. Exp. Ther. 2023, 384, 1–3. [Google Scholar] [CrossRef]
- Sze, S.; Pellicori, P.; Zhang, J.; Weston, J.; Clark, A.L. Which frailty tool best predicts morbidity and mortality in ambulatory patients with heart failure? A prospective study. Eur. Heart J. Qual. Care Clin. Outcomes 2022, in press. [Google Scholar] [CrossRef]
- Pocock, S.J.; Ferreira, J.P.; Gregson, J.; Anker, S.D.; Butler, J.; Filippatos, G.; Gollop, N.D.; Iwata, T.; Brueckmann, M.; Januzzi, J.L.; et al. Novel biomarker-driven prognostic models to predict morbidity and mortality in chronic heart failure: The EMPEROR-Reduced trial. Eur. Heart J. 2021, 42, 4455–4464. [Google Scholar] [CrossRef]
- Rich, J.D.; Burns, J.; Freed, B.H.; Maurer, M.S.; Burkhoff, D.; Shah, S.J. Meta-Analysis Global Group in Chronic (MAGGIC) Heart Failure Risk Score: Validation of a Simple Tool for the Prediction of Morbidity and Mortality in Heart Failure With Preserved Ejection Fraction. J. Am. Heart Assoc. 2018, 7, e009594. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.C.; Wu, P.J.; Fang, H.Y.; Fang, Y.N.; Chen, H.C.; Tong, M.S.; Sung, P.H.; Lee, C.H.; Chung, W.J. Levosimendan Administration May Provide More Benefit for Survival in Patients with Non-Ischemic Cardiomyopathy Experiencing Acute Decompensated Heart Failure. J. Clin. Med. 2022, 11, 3997. [Google Scholar] [CrossRef] [PubMed]
- Dass, B.; Dimza, M.; Singhania, G.; Schwartz, C.; George, J.; Bhatt, A.; Radhakrishnan, N.; Bansari, A.; Bozorgmehri, S.; Mohandas, R. Renin-Angiotensin-Aldosterone System Optimization for Acute Decompensated Heart Failure Patients (ROAD-HF): Rationale and Design. Am. J. Cardiovasc. Drugs 2020, 20, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Scrutinio, D.; Ammirati, E.; Guida, P.; Passantino, A.; Raimondo, R.; Guida, V.; Sarzi Braga, S.; Canova, P.; Mastropasqua, F.; Frigerio, M.; et al. The ADHF/NT-proBNP risk score to predict 1-year mortality in hospitalized patients with advanced decompensated heart failure. J. Heart Lung Transplant. 2014, 33, 404–411. [Google Scholar] [CrossRef]
- Arrigo, M.; Jessup, M.; Mullens, W.; Reza, N.; Shah, A.M.; Sliwa, K.; Mebazaa, A. Acute heart failure. Nat. Rev. Dis. Primers 2020, 6, 16. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Clinical Condition | Animal Model | Endpoint | Conclusion |
|---|---|---|---|
| DCM | DCM STZ induced in rats | DD | Istaroxime improved DD stimulating SERCA2a and reducing alterations in intracellular Ca2+ handling. |
| ADHF | Canine model of HF produced by multiple sequential intracoronary embolizations with microspheres | LVEF (%); LVEDV (mL); LVESV (mL). | Istaroxime improved hemodynamic and echocardiographic parameters. |
| Chronic ischemic HF, comparing istaroxime to dobutamine | Canine model of HF produced by ligation of the left anterior descending coronary artery and intracoronary embolizations | LV function | Istaroxime was shown to be an effective inotropic agent without positive chronotropic actions. |
| Progressive HF | Hamster model of progressive HF | Heart/body weight ratio; max dP/dT; min dP/dT; LVSP; CFR | Istaroxime improved cardiac function and heart rate variability |
| Electrophysiological effects of istaroxime and digoxin | Guinea pig isolated ventricular myocytes | Effects on ITI | Istaroxime inhibited ITI (effect not evident with digoxin) |
| Cardiotoxic effects of equi-inotropic concentrations of istaroxime and ouabain | Rat isolated ventricular myocytes | Cell viability; Apoptosis; CaMKII activation. | Istaroxime had a significant inotropic effect, neither activating CaMKII nor promoting cardiomyocytes death (contrary to digoxin) |
| Clinical Trial | Primary Endpoint | Main Results |
|---|---|---|
| HORIZON-HF (NCT00616161) | Change in PCWP (mmHg) | Istaroxime: −3.2 ± 6.8, −3.3 ± 5.5, and −4.7 ± 5.9 vs. placebo: 0.0 ± 3.6; p < 0.05 (for all doses) |
| The Clinical Study of the Safety and Efficacy of Istaroxime in Treatment of ADHF (NCT02617446) | E/e’ ratio change from baseline to 24 h | cohort 1: istaroxime 0.5 μg/kg/min: −4.55 ± 4.75 vs. placebo: −1.55 ± 4.11, p = 0.029; cohort 2: 59 istaroxime 1.0 μg/kg/min: −3.16 ± 2. vs. placebo: −1.08 ± 2.72, p = 0.009 |
| SEISMiC (NCT04325035) | AUC (mmHg × hour; change in SBP from baseline through 6 h) | Istaroxime: 53.1 ± 6.88 vs. placebo: 30.9 ± 6.76, p = 0.017 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Forzano, I.; Mone, P.; Mottola, G.; Kansakar, U.; Salemme, L.; De Luca, A.; Tesorio, T.; Varzideh, F.; Santulli, G. Efficacy of the New Inotropic Agent Istaroxime in Acute Heart Failure. J. Clin. Med. 2022, 11, 7503. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11247503
Forzano I, Mone P, Mottola G, Kansakar U, Salemme L, De Luca A, Tesorio T, Varzideh F, Santulli G. Efficacy of the New Inotropic Agent Istaroxime in Acute Heart Failure. Journal of Clinical Medicine. 2022; 11(24):7503. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11247503
Chicago/Turabian StyleForzano, Imma, Pasquale Mone, Gaetano Mottola, Urna Kansakar, Luigi Salemme, Antonio De Luca, Tullio Tesorio, Fahimeh Varzideh, and Gaetano Santulli. 2022. "Efficacy of the New Inotropic Agent Istaroxime in Acute Heart Failure" Journal of Clinical Medicine 11, no. 24: 7503. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11247503