
Advanced Hemodynamic Monitoring Allows Recognition of Early Response Patterns to Diuresis in Congestive Heart Failure Patients
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Considerations
2.2. Study Participants
2.3. Study Design
2.4. The Photoplethysmography-Based Monitoring Device
2.5. Data Collection
2.6. Statistical Analysis
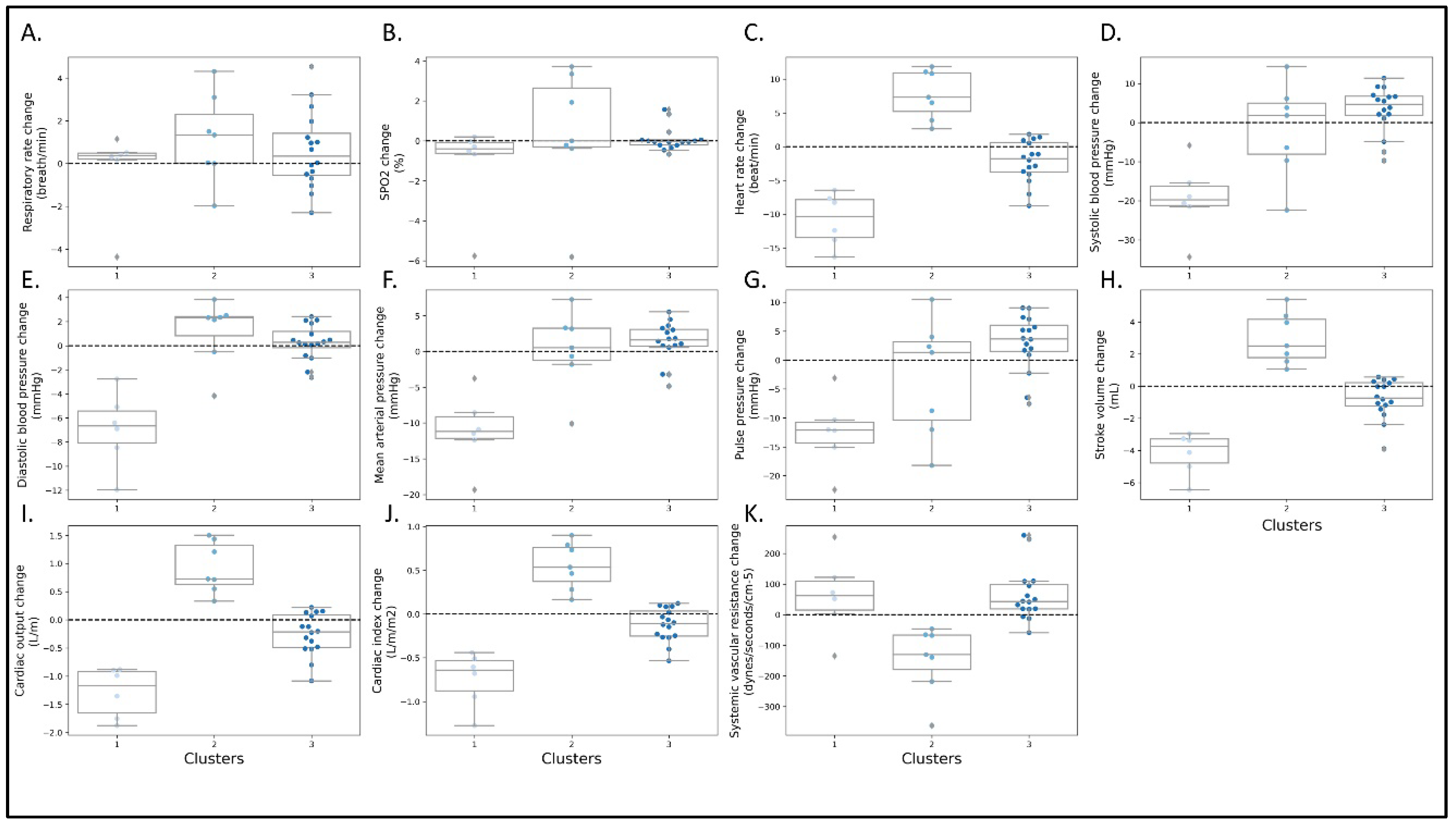
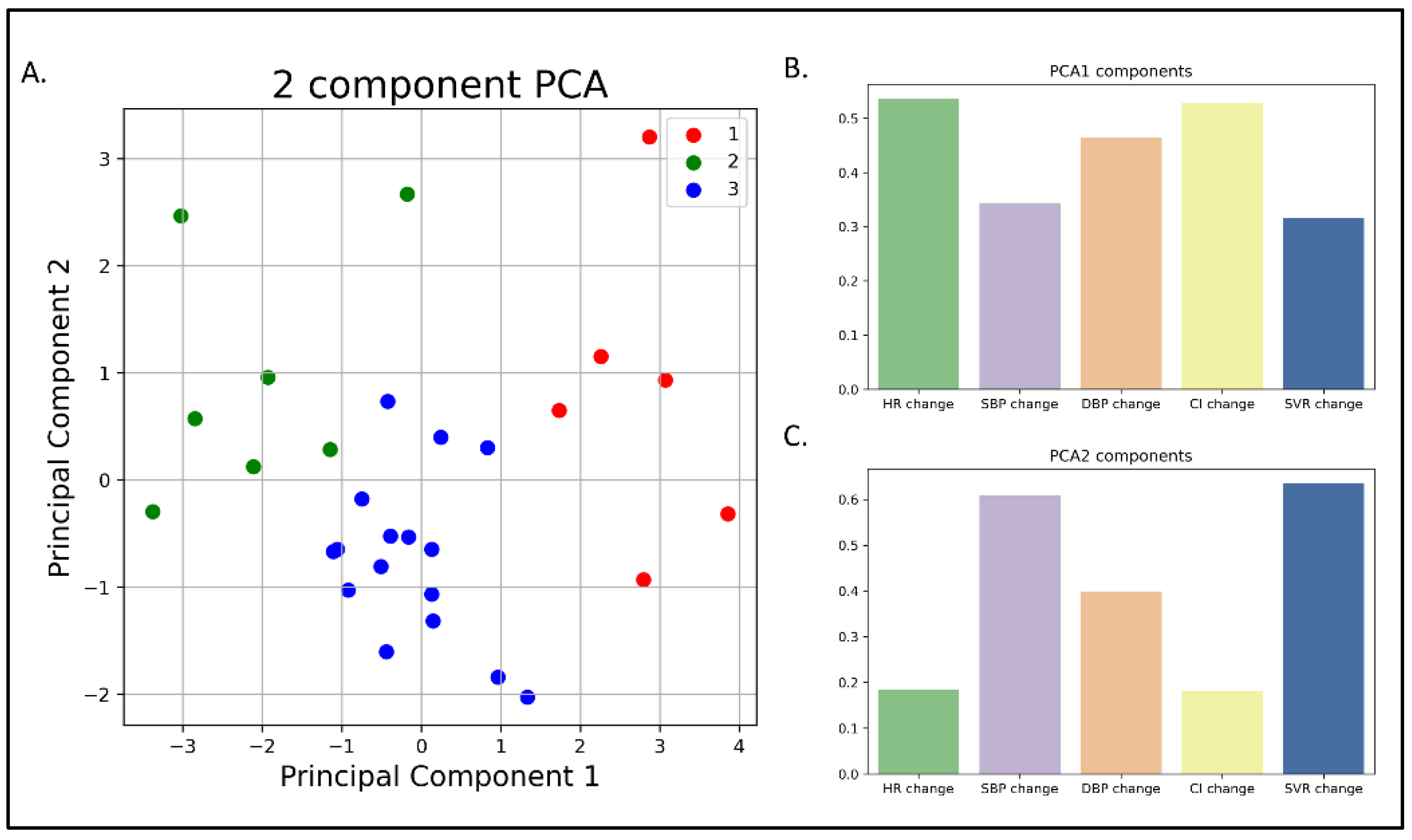
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Braunwald, E. Shattuck lecture--cardiovascular medicine at the turn of the millennium: Triumphs, concerns, and opportunities. N. Engl. J. Med. 1997, 337, 1360–1369. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Anker, S.D.; AlHabib, K.F.; Cowie, M.R.; Force, T.L.; Hu, S.; Jaarsma, T.; Krum, H.; Rastogi, V.; Rohde, L.E.; et al. Heart failure: Preventing disease and death worldwide. ESC Heart Fail. 2014, 1, 4–25. [Google Scholar] [CrossRef] [PubMed]
- Dunlay, S.M.; Shah, N.D.; Shi, Q.; Morlan, B.; VanHouten, H.; Long, K.H.; Roger, V.L. Lifetime costs of medical care after heart failure diagnosis. Circ. Cardiovasc. Qual. Outcomes 2011, 4, 68–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gheorghiade, M.; Vaduganathan, M.; Fonarow, G.C.; Bonow, R.O. Rehospitalization for heart failure: Problems and perspectives. J. Am. Coll. Cardiol. 2013, 61, 391–403. [Google Scholar] [CrossRef] [Green Version]
- Pham, D.; Grodin, J.L. Dilemmas in the Dosing of Heart Failure Drugs: Titrating Diuretics in Chronic Heart Failure. Card. Fail. Rev. 2017, 3, 108–112. [Google Scholar] [CrossRef]
- Lewin, J.; Ledwidge, M.; O’Loughlin, C.; McNally, C.; McDonald, K. Clinical deterioration in established heart failure: What is the value of BNP and weight gain in aiding diagnosis? Eur. J. Heart Fail. 2005, 7, 953–957. [Google Scholar] [CrossRef]
- Zhang, J.; Goode, K.M.; Cuddihy, P.E.; Cleland, J.G.; TEN-HMS Investigators. Predicting hospitalization due to worsening heart failure using daily weight measurement: Analysis of the Trans-European Network-Home-Care Management System (TEN-HMS) study. Eur. J. Heart Fail. 2009, 11, 420–427. [Google Scholar] [CrossRef]
- Abraham, W.T.; Adamson, P.B.; Costanzo, M.R.; Eigler, N.; Gold, M.; Klapholz, M.; Maurer, M.; Saxon, L.; Singh, J.; Troughton, R. Hemodynamic monitoring in advanced heart failure: Results from the LAPTOP-HF trial. J. Card. Fail. 2016, 22, 940. [Google Scholar] [CrossRef]
- Binanay, C.; Califf, R.M.; Hasselblad, V.; O’Connor, C.; Shah, M.R.; Sopko, G.; Stevenson, L.W.; Francis, G.S.; Leier, C.V.; Miller, L.W.; et al. Evaluation study of congestive heart failure and pulmonary artery catheterization effectiveness: The ESCAPE trial. JAMA 2005, 294, 1625–1633. [Google Scholar]
- Desai, A.S. Implantable Hemodynamic Monitoring in Ambulatory Heart Failure: Who, When, Why, How? Curr. Cardiol. Rep. 2015, 17, 113. [Google Scholar] [CrossRef]
- Nachman, D.; Constantini, K.; Poris, G.; Wagnert-Avraham, L.; Gertz, S.D.; Littman, R.; Kabakov, E.; Eisenkraft, A.; Gepner, Y. Wireless, non-invasive, wearable device for continuous remote monitoring of hemodynamic parameters in a swine model of controlled hemorrhagic shock. Sci. Rep. 2020, 10, 17684. [Google Scholar] [CrossRef]
- Taylor, S.H. Diuretic therapy in congestive heart failure. Cardiol. Rev. 2000, 8, 104–114. [Google Scholar] [CrossRef]
- Silke, B. Haemodynamic impact of diuretic therapy in chronic heart failure. Cardiology 1994, 84, 115–123. [Google Scholar] [CrossRef]
- Francis, G.S.; Siegel, R.M.; Goldsmith, S.R.; Olivari, M.T.; Levine, T.B.; Cohn, J.N. Acute vasoconstrictor response to intravenous furosemide in patients with chronic congestive heart failure. Activation of the neurohumoral axis. Ann. Intern. Med. 1985, 103, 1–6. [Google Scholar] [CrossRef]
- Raftery, E.B. Haemodynamic effects of diuretics in heart failure. Br. Heart J. 1994, 72, S44–S47. [Google Scholar] [CrossRef] [Green Version]
- Wilson, J.R.; Reichek, N.; Dunkman, W.B.; Goldberg, S. Effect of diuresis on the performance of the failing left ventricle in man. Am. J. Med. 1981, 70, 234–239. [Google Scholar] [CrossRef]
- Pickkers, P.; Dormans, T.P.; Russel, F.G.; Hughes, A.D.; Thien, T.; Schaper, N.; Smits, P. Direct vascular effects of furosemide in humans. Circulation 1997, 96, 1847–1852. [Google Scholar] [CrossRef] [Green Version]
- Musini, V.M.; Rezapour, P.; Wright, J.M.; Bassett, K.; Jauca, C.D. Blood pressure lowering efficacy of loop diuretics for primary hypertension. Cochrane Database Syst. Rev. 2012, 8, CD003825. [Google Scholar]
- Dikshit, K.; Vyden, J.K.; Forrester, J.S.; Chatterjee, K.; Prakash, R.; Swan, H.J. Renal and extrarenal hemodynamic effects of furosemide in congestive heart failure after acute myocardial infarction. N. Engl. J. Med. 1973, 288, 1087–1090. [Google Scholar] [CrossRef]
- Frazier, C.G.; Alexander, K.P.; Newby, L.K.; Anderson, S.; Iverson, E.; Packer, M.; Cohn, J.; Goldstein, S.; Douglas, P.S. Associations of gender and etiology with outcomes in heart failure with systolic dysfunction: A pooled analysis of 5 randomized control trials. J. Am. Coll. Cardiol. 2007, 49, 1450–1458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMurray, J.J.V.; Jackson, A.M.; Lam, C.S.P.; Redfield, M.M.; Anand, I.S.; Ge, J.; Lefkowitz, M.P.; Maggioni, A.P.; Martinez, F.; Packer, M.; et al. Effects of Sacubitril-Valsartan Versus Valsartan in Women Compared with Men With Heart Failure and Preserved Ejection Fraction: Insights From PARAGON-HF. Circulation 2020, 141, 338–351. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.U.; Klein, L.; Lloyd-Jones, D.M. Heart failure in women: Epidemiology, biology and treatment. Womens Health 2009, 5, 517–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, A.; Braunwald, E.; McNulty, S.; Felker, G.M.; Gilbert, E.M.; Alharethi, R.; Lee, K.L.; Anstrom, K.J.; Redfield, M.M.; Goldsmith, S.R.; et al. Obesity and the response to intensified diuretic treatment in decompensated heart failure: A DOSE trial substudy. J. Card. Fail. 2012, 18, 837–844. [Google Scholar] [CrossRef] [Green Version]
- Brandoni, A.; Villar, S.R.; Torres, A.M. Gender-related differences in the pharmacodynamics of furosemide in rats. Pharmacology 2004, 70, 107–112. [Google Scholar] [CrossRef]
- Cubbon, R.M.; Adams, B.; Rajwani, A.; Mercer, B.N.; Patel, P.A.; Gherardi, G.; Gale, C.P.; Batin, P.D.; Ajjan, R.; Kearney, L.; et al. Diabetes mellitus is associated with adverse prognosis in chronic heart failure of ischaemic and non-ischaemic aetiology. Diab. Vasc. Dis. Res. 2013, 10, 330–336. [Google Scholar] [CrossRef]
- Cunha, F.M.; Pereira, J.; Marques, P.; Ribeiro, A.; Bettencourt, P.; Lourenço, P. Diabetic patients need higher furosemide doses: A report on acute and chronic heart failure patients. J. Cardiovasc. Med. 2020, 21, 21–26. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic (Mean ± SD) | |
|---|---|
| Age (Years) | 75.5 ± 9.7 |
| Sex (Male/Female) | 17/12 |
| BMI (kg/m2) | 27.0 ± 4.5 |
| Outpatient clinic visits per month | 2.6 ± 1.7 |
| Creatinine on the day of recruitment (μmol/L) | 163.6 ± 112.7 |
| Baseline hemodynamic parameters (mean ± SD) | |
| Pulse rate (beats/min) | 76.2 ± 8.5 |
| Systolic blood pressure (mmHg) | 130.0 ± 30.7 |
| Diastolic blood pressure (mmHg) | 71.5 ± 18.3 |
| Mean arterial pressure (mmHg) | 91.1 ± 20.3 |
| Pulse pressure (mmHg) | 58.4 ± 24.0 |
| Stroke volume (mL) | 89.8 ± 7.0 |
| Cardiac output (L/min) | 6.8 ± 0.8 |
| Cardiac index (L/min/m2) | 3.9 ± 0.6 |
| Systemic vascular resistance (dynes/sec/cm−5) | 1080 ± 250 |
| Smoking status N (%) | |
| Current | 5 (17.2) |
| Past | 12 (41.4) |
| Never | 12 (41.4) |
| Diabetes status N (%) | |
| HbA1c (%, mean ± SD) | 6.8 ± 1.4 |
| Not diabetic | 9 (31.0) |
| Prediabetic | 4 (13.8) |
| Diabetic | 16 (55.2) |
| Heart failure type N (%) | |
| HFrEF | 15 (53.3) |
| HFpEF | 14 (46.7) |
| Medical history N (%) | |
| Ischemic heart disease | 21 (72.4) |
| Coronary artery bypass graft (CABG) | 5 (17.2) |
| Hypertension | 22 (75.9) |
| Dyslipidemia | 23 (79.3) |
| Medication use N (%) | |
| Furosemide | 29 (100) |
| The total daily dose of oral furosemide (mg, mean ± SD) | 83.0 ± 32.9 |
| β blockers | 20 (68.9) |
| ACE inhibitors | 4 (13.7) |
| ARBs | 10 (34.4) |
| Aldosterone antagonists | 13 (44.8) |
| Sacubitril/Valsartan | 6 (20.6) |
| Digoxin | 3 (10.3) |
| Metolazone | 4 (13.7) |
| Cluster 1 | Cluster 2 | Cluster 3 | p-Value | Post Hoc (p < 0.05) | |
|---|---|---|---|---|---|
| Characteristic | |||||
| Age (Years) | 74.3 ± 12.3 | 73.6 ± 8.7 | 76.8 ± 9.6 | ns | |
| Sex (M/F) | 5/1 | 1/6 | 11/5 | 0.02 | |
| BMI (Kg/m2) | 25.5 ± 5.5 | 28.3 ± 6.1 | 27.0 ± 3.3 | ns | |
| CHF type (HFrEF/HFpEF) | 4/2 | 3/4 | 8/8 | ns | |
| Hypertension (yes/no) | 5/1 | 4/3 | 13/3 | ns | |
| Chronic kidney disease (yes/no) | 5/1 | 2/5 | 12/2 | 0.058 | |
| Type 2 diabetes (no/pre/T2DM) | 2/2/2 | 1/1/5 | 6/1/9 | ns | |
| HbA1c (%) | 5.9 ± 0.5 | 7.6 ± 2.1 | 6.8 ± 0.9 | 0.085 | |
| Creatinine (µmol/L) | 274.8 ± 182.6 | 95.9 ± 22.4 | 151.6 ± 71.6 | 0.009 | (1,2), (1,3) |
| Baseline parameters | |||||
| Heart rate (beats/min) | 80.4 ± 8.2 | 69.5 ± 7.7 | 77.6 ± 7.8 | 0.038 | |
| Systolic blood pressure (mmHg) | 141.4 ± 32.9 | 135.8 ± 26.4 | 123.1 ± 31.7 | ns | |
| Diastolic blood pressure (mmHg) | 70.3 ± 26.2 | 64.1 ± 10.9 | 75.2 ± 17.6 | ns | |
| Mean arterial pressure (mmHg) | 94.1 ± 28.2 | 88.0 ± 15.3 | 91.2 ± 20.1 | ns | |
| Pulse pressure (mmHg) | 71.1 ± 10.9 | 71.7 ± 18.6 | 47.8 ± 25.1 | 0.025 | |
| Stroke volume (mL) | 93.7 ± 9.3 | 88.1 ± 7.9 | 89.1 ± 5.5 | ns | |
| Cardiac output (L/min) | 7.5 ± 0.8 | 6.1 ± 0.6 | 6.9 ± 0.6 | 0.002 | (1,2), (2,3) |
| Cardiac index (L/min/m2) | 4.3 ± 0.9 | 3.6 ± 0.5 | 3.8 ± 0.5 | ns | |
| SVR (dynes/sec/cm−5) | 1015 ± 284 | 1180 ± 307 | 1061 ± 213 | ns | |
| Change after treatment | |||||
| VAS change (cm) | −0.1 ± 0.2 | −0.5 ± 0.6 | −0.5 ± 1.3 | ns | |
| Weight loss (%) | −1.3 ± 2.3 | −1.3 ± 1.4 | −1.1 ± 1.6 | ns |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dagan, M.; Kolben, Y.; Goldstein, N.; Ben Ishay, A.; Fons, M.; Merin, R.; Eisenkraft, A.; Amir, O.; Asleh, R.; Ben-Yehuda, A.; et al. Advanced Hemodynamic Monitoring Allows Recognition of Early Response Patterns to Diuresis in Congestive Heart Failure Patients. J. Clin. Med. 2023, 12, 45. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12010045
Dagan M, Kolben Y, Goldstein N, Ben Ishay A, Fons M, Merin R, Eisenkraft A, Amir O, Asleh R, Ben-Yehuda A, et al. Advanced Hemodynamic Monitoring Allows Recognition of Early Response Patterns to Diuresis in Congestive Heart Failure Patients. Journal of Clinical Medicine. 2023; 12(1):45. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12010045
Chicago/Turabian StyleDagan, Maya, Yotam Kolben, Nir Goldstein, Arik Ben Ishay, Meir Fons, Roei Merin, Arik Eisenkraft, Offer Amir, Rabea Asleh, Arie Ben-Yehuda, and et al. 2023. "Advanced Hemodynamic Monitoring Allows Recognition of Early Response Patterns to Diuresis in Congestive Heart Failure Patients" Journal of Clinical Medicine 12, no. 1: 45. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12010045