
Is It All about Surface Topography? An Intra-Individual Clinical Outcome Analysis of Two Different Implant Surfaces in Breast Reconstruction
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
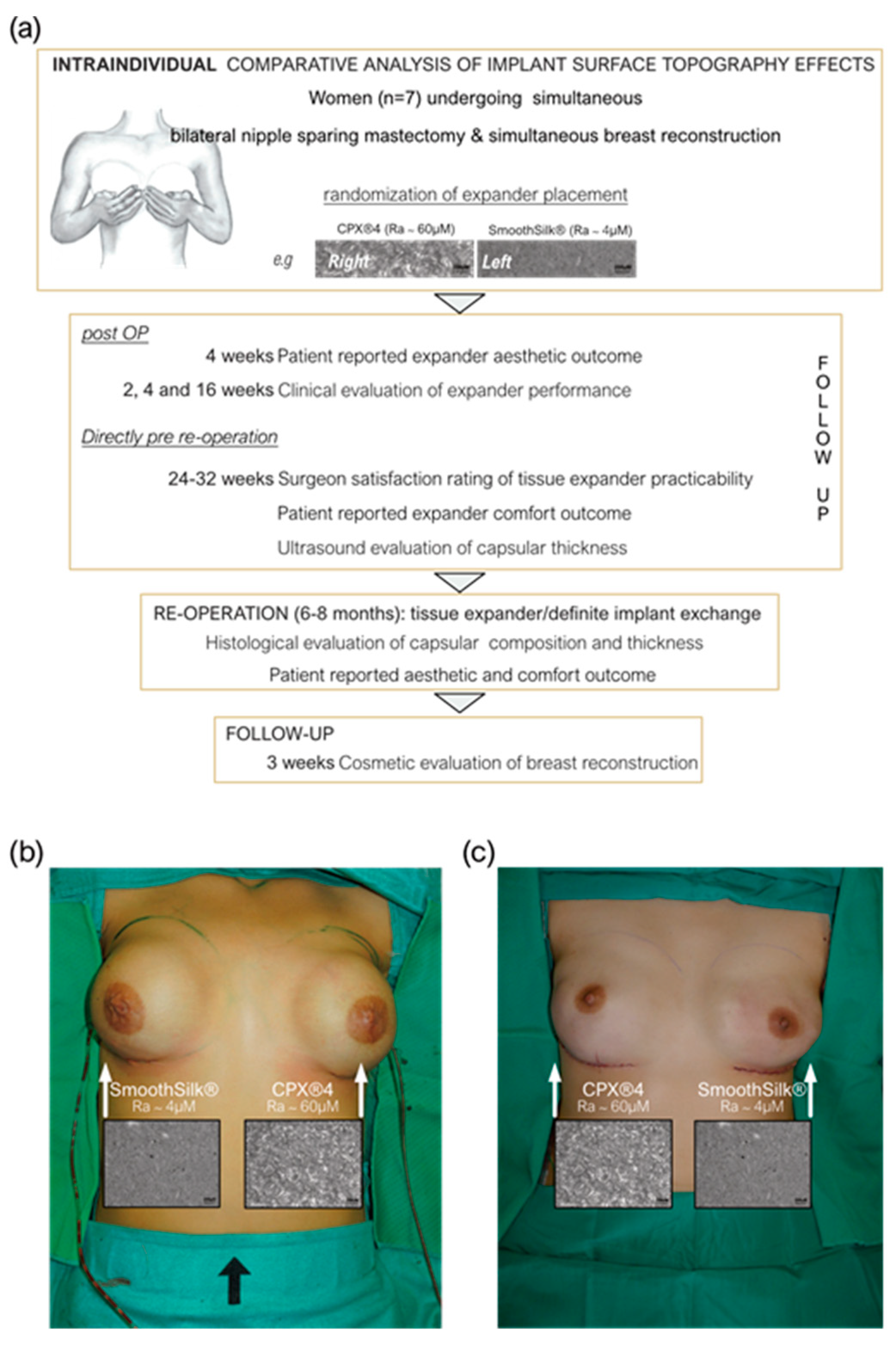
2.2. Study Design
2.3. Statistical Analysis
3. Results
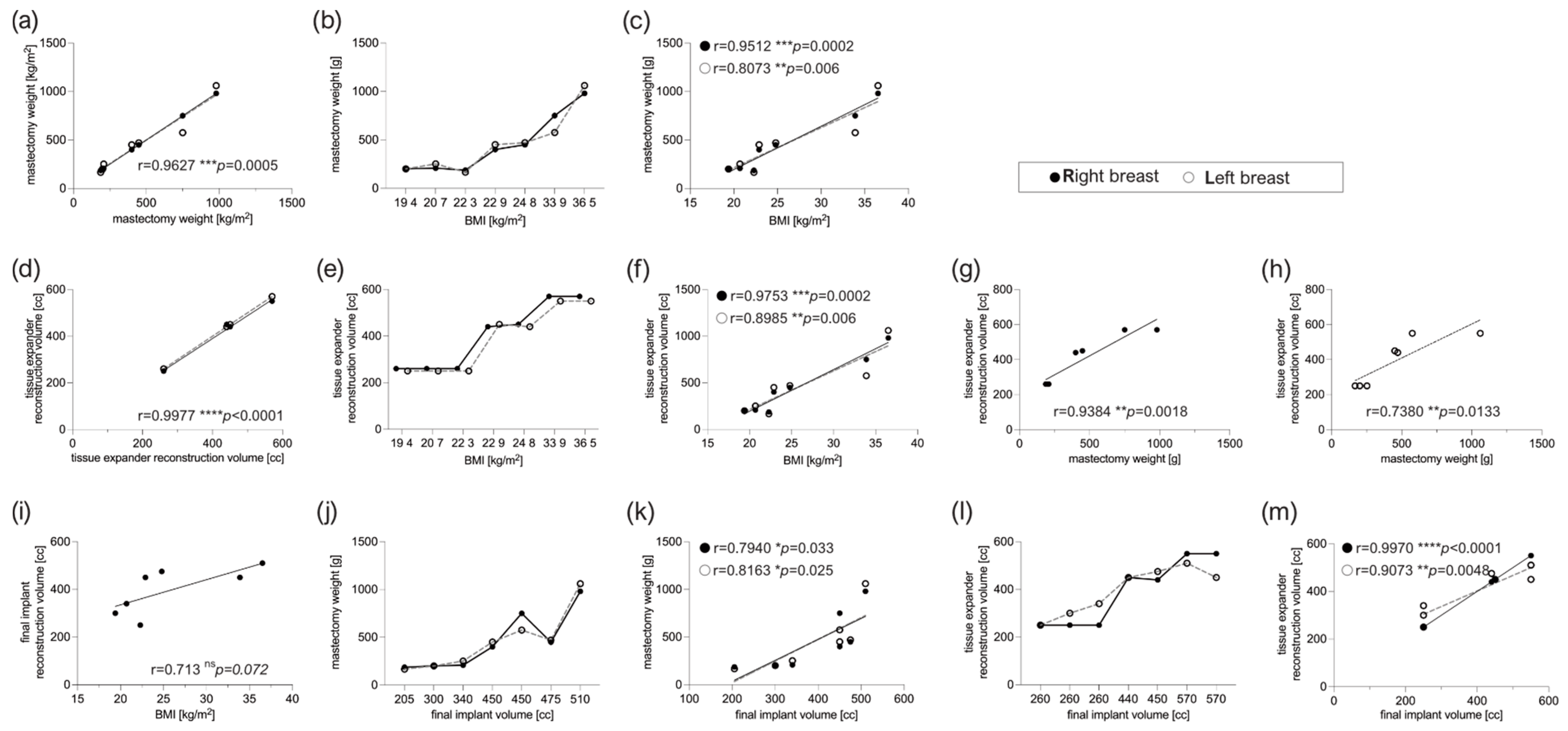
3.1. Patient Characteristics
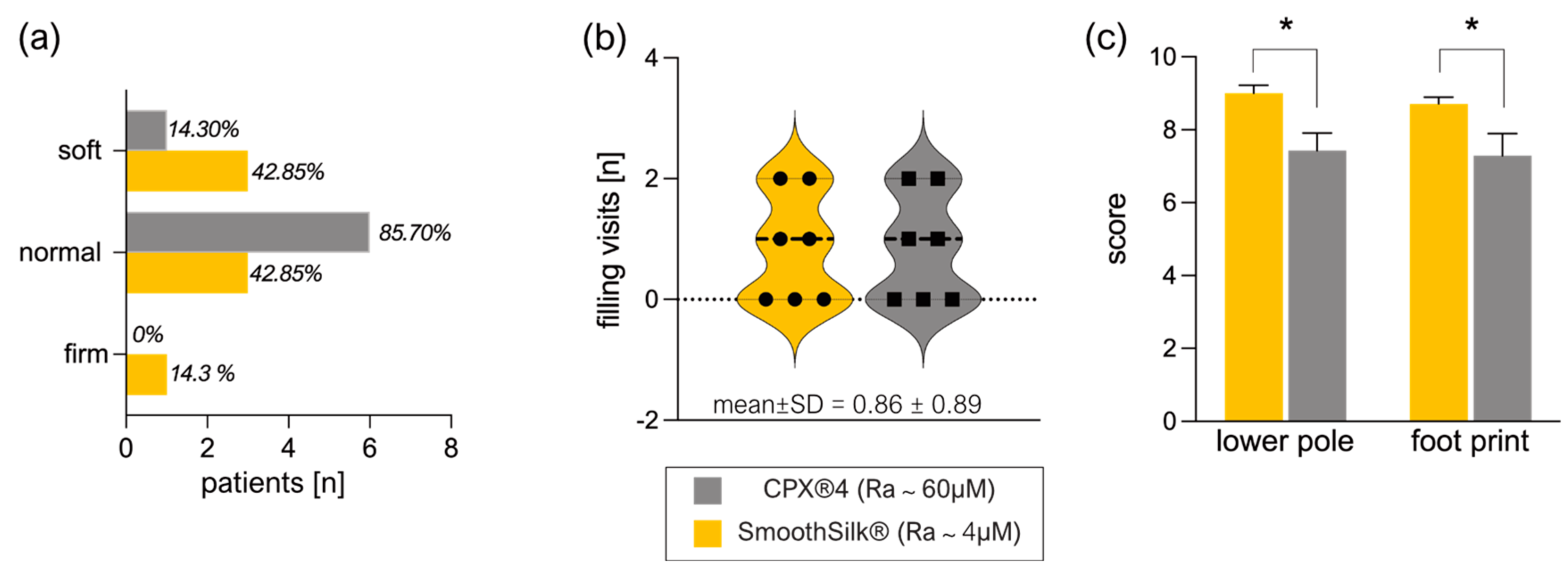
3.2. Clinical Evaluation of Expander Performance
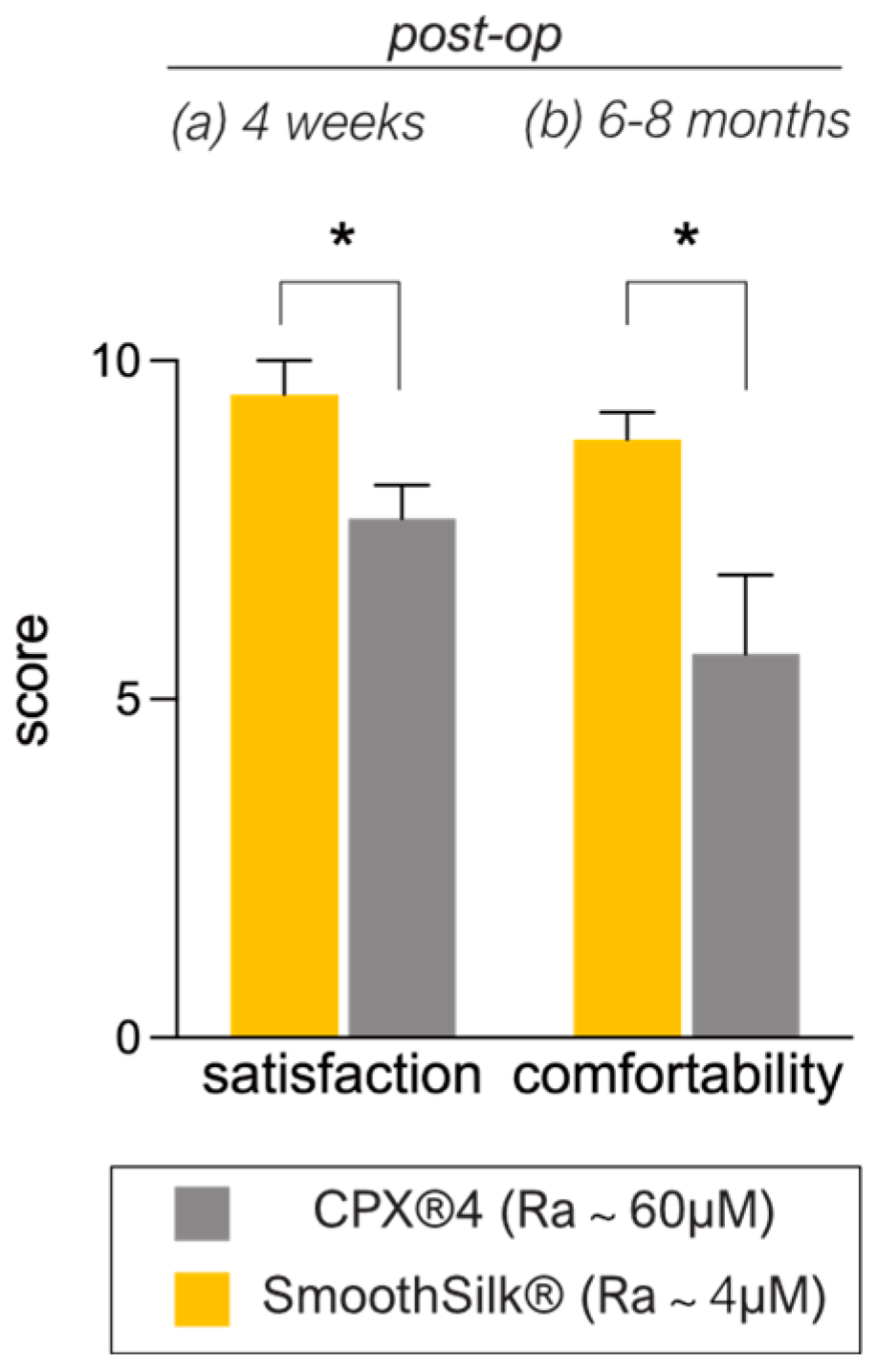
3.3. Patient-Reported Aesthetic and Comfort Outcome after Expander Reconstruction
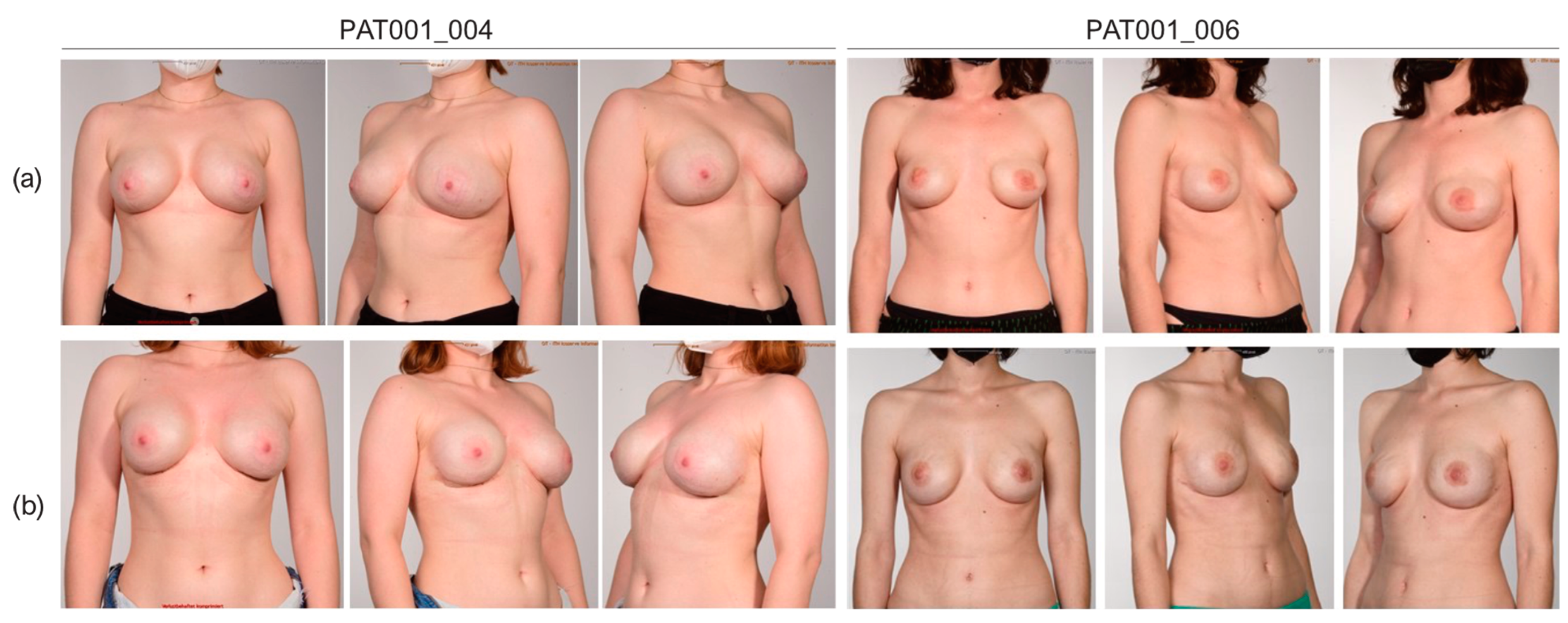
3.4. Cosmetic Results
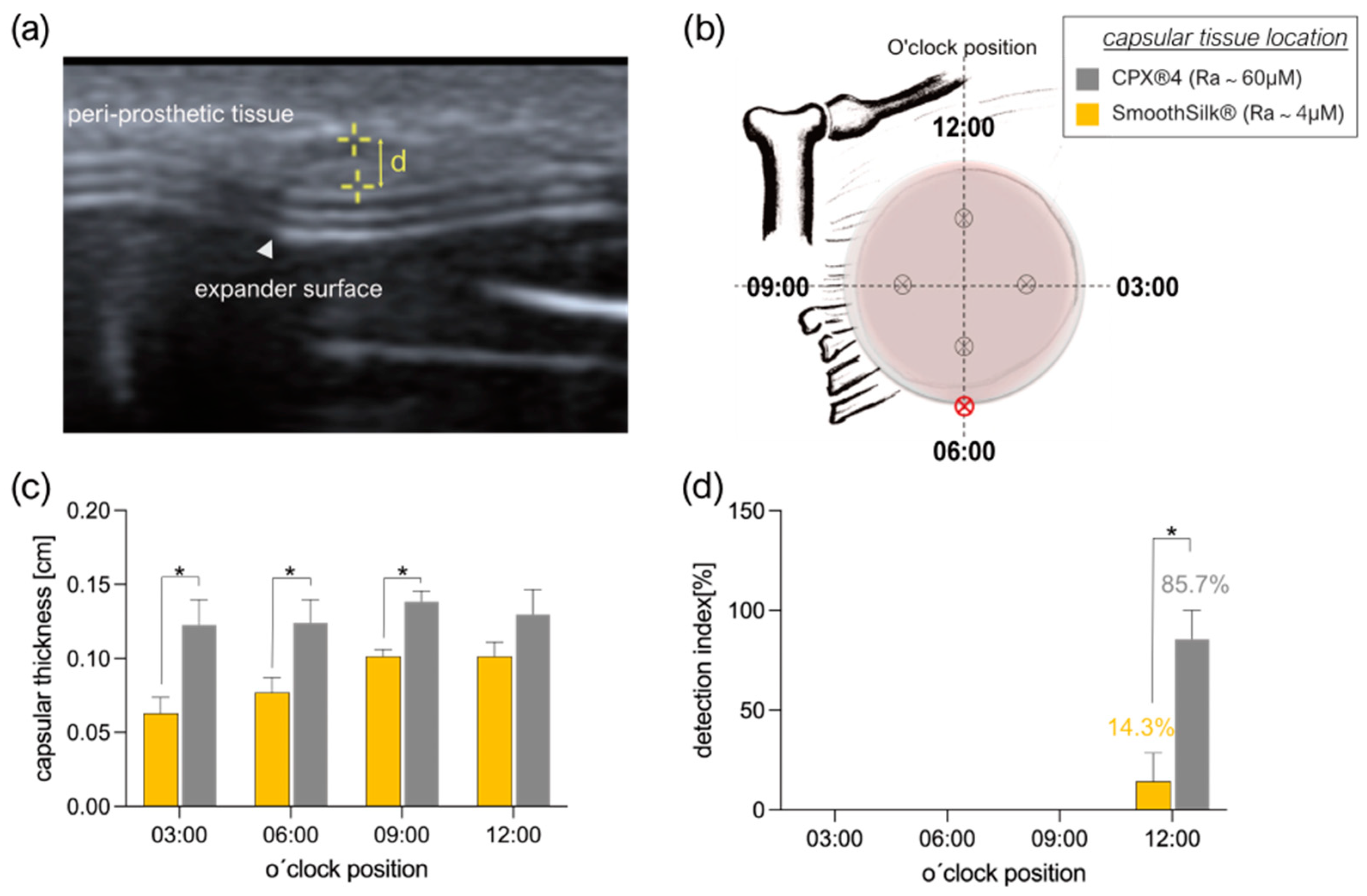
3.5. Intra- and Inter-Individual Comparison of the Fibrotic Capsule Thickness Formed around the CPX®4 and SmoothSilk® Tissue Expander
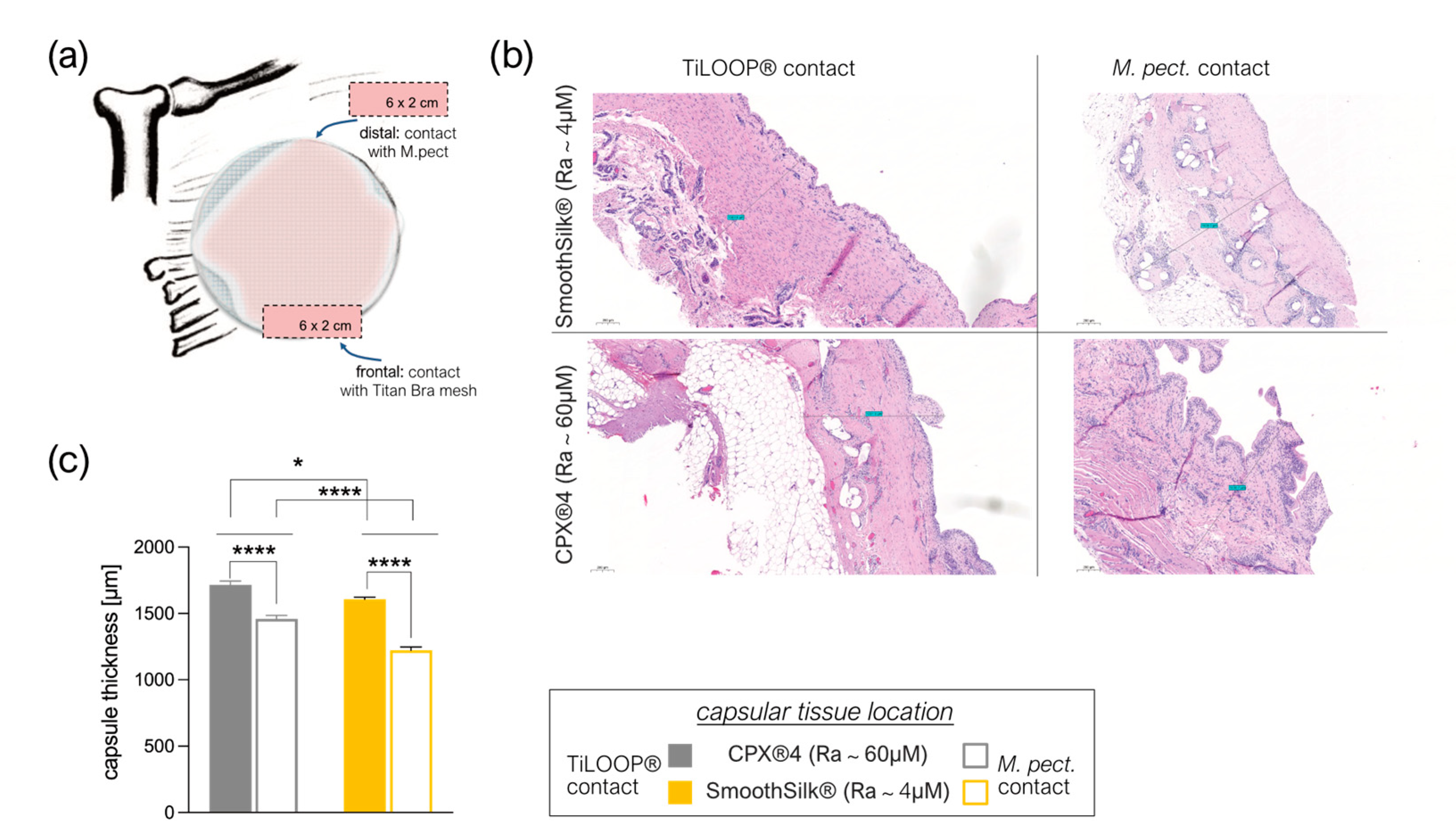
3.6. Titanium Debris from TiLoop® Bra Increases Histopathological Changes of the Capsule
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Society of Plastic Surgeons. Plastic Surgery Statistics. Available online: https://www.plasticsurgery.org/news/plastic-surgery-statistics (accessed on 21 November 2022).
- Collett, D.J.; Rakhorst, H.; Lennox, P.; Magnusson, M.; Cooter, R.; Deva, A. Current Risk Estimate of Breast Implant–Associated Anaplastic Large Cell Lymphoma in Textured Breast Implants. Plast. Reconstr. Surg. 2019, 143, 30S–40S. [Google Scholar] [CrossRef]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef]
- OECD.Stat. Health Care Utilisation: Surgical procedures. Available online: https://stats.oecd.org (accessed on 7 November 2022).
- Fanakidou, I.; Zyga, S.; Alikari, V.; Tsironi, M.; Stathoulis, J.; Theofilou, P. Mental health, loneliness, and illness perception outcomes in quality of life among young breast cancer patients after mastectomy: The role of breast reconstruction. Qual. Life Res. 2018, 27, 539–543. [Google Scholar] [CrossRef]
- Fortunato, L.; Loreti, A.; Cortese, G.; Spallone, D.; Toto, V.; Cavaliere, F.; Farina, M.; La Pinta, M.; Manna, E.; Detto, L.; et al. Regret and Quality of Life after Mastectomy with or without Reconstruction. Clin. Breast Cancer 2021, 21, 162–169. [Google Scholar] [CrossRef]
- Panchal, H.M.; Matros, E.M. Current Trends in Postmastectomy Breast Reconstruction. Plast. Reconstr. Surg. 2017, 140, 7S–13S. [Google Scholar] [CrossRef]
- Santosa, K.B.; Qi, J.; Kim, H.M.; Hamill, J.B.; Wilkins, E.G.; Pusic, A.L. Long-term Patient-Reported Outcomes in Postmastectomy Breast Reconstruction. JAMA Surg. 2018, 153, 891. [Google Scholar] [CrossRef]
- Toyserkani, N.M.; Jørgensen, M.G.; Tabatabaeifar, S.; Damsgaard, T.; Sørensen, J.A. Autologous versus implant-based breast reconstruction: A systematic review and meta-analysis of Breast-Q patient-reported outcomes. J. Plast. Reconstr. Aesthetic Surg. 2020, 73, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Miseré, R.M.; van Kuijk, S.M.; Claassens, E.L.; Heuts, E.M.; Piatkowski, A.A.; van der Hulst, R.R. Breast-related and body-related quality of life following autologous breast reconstruction is superior to implant-based breast reconstruction—A long-term follow-up study. Breast 2021, 59, 176–182. [Google Scholar] [CrossRef]
- Lemaine, V.; Schilz, S.R.; Van Houten, H.K.; Zhu, L.; Habermann, E.B.; Boughey, J.C. Autologous Breast Reconstruction versus Implant-Based Reconstruction: How Do Long-Term Costs and Health Care Use Compare? Plast. Reconstr. Surg. 2020, 145, 303–311. [Google Scholar] [CrossRef] [PubMed]
- American Society of Plastic Surgeons. American Society of Plastic Surgeons Statistics Report2020: National Clearinghous of Plastic Suergery Procedural Statistics. Available online: https://www.plasticsurgery.org (accessed on 7 November 2022).
- Eriksen, C.; Lindgren, E.N.; Frisell, J.; Stark, B. A Prospective Randomized Study Comparing Two Different Expander Approaches in Implant-Based Breast Reconstruction. Plast. Reconstr. Surg. 2012, 130, 254e–264e. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.-T.; Mun, G.-H. Comparison of one-stage vs two-stage prosthesis-based breast reconstruction: A systematic review and meta-analysis. Am. J. Surg. 2016, 212, 336–344. [Google Scholar] [CrossRef] [PubMed]
- Nahabedian, M.Y.; Jacobson, S.R. Two-stage prepectoral breast reconstruction. Gland. Surg. 2019, 8, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.B.; Eldred, D.E.; Kim, G.; Curtis, J.M.; Brandon, H.J.; Klykken, P.C. Assessment of silicone gel breast implant biodurability by NMR and EDS techniques. J. Biomed. Mater. Res. Part A 2008, 85, 684–691. [Google Scholar] [CrossRef] [PubMed]
- Stevens, W.G.; Pacella, S.J.; Gear, A.J.; Freeman, M.E.; McWhorter, C.; Tenenbaum, M.J.; Stoker, D.A. Clinical Experience with a Fourth-Generation Textured Silicone Gel Breast Implant: A Review of 1012 Mentor MemoryGel Breast Implants. Aesthetic Surg. J. 2008, 28, 642–647. [Google Scholar] [CrossRef] [PubMed]
- Bengtson, B.P.; Eaves, F.F. High-Resolution Ultrasound in the Detection of Silicone Gel Breast Implant Shell Failure: Background, In Vitro Studies, and Early Clinical Results. Aesthetic Surg. J. 2012, 32, 157–174. [Google Scholar] [CrossRef]
- Cole, N.M. Consequences of the U.S. Food and Drug Administration–Directed Moratorium on Silicone Gel Breast Implants: 1992 to 2006. Plast. Reconstr. Surg. 2018, 141, 1137–1141. [Google Scholar] [CrossRef] [PubMed]
- Cohen, B.E.; Biggs, T.M.; Cronin, E.D.; Collins, D.R. Assessment and Longevity of the Silicone Gel Breast Implant. Plast. Reconstr. Surg. 1997, 99, 1597–1601. [Google Scholar] [CrossRef]
- Lam, M.C.; Walgenbach-Brünagel, G.; Pryalukhin, A.; Vorhold, J.; Pech, T.; Kalff, J.C.; Kristiansen, G.; Walgenbach, K.J. Management of Capsular Contracture in Cases of Silicone Gel Breast Implant Rupture with Use of Pulse Lavage and Open Capsulotomy. Aesthetic Plast. Surg. 2019, 43, 1173–1185. [Google Scholar] [CrossRef]
- Jasanoff, S. Expert Games in Silicone Gel Breast Implant Litigation. In Science in Court; Routledge: London, UK, 2019. [Google Scholar] [CrossRef]
- Henning, C.; Wang, J.; Swift, R.; Eades, B.; Spektor, T.M.; Berenson, J.R. Removal of a Silicone Gel Breast Implant in a Multiple Myeloma Patient Improved Disease Status: A Case Report. Case Rep. Oncol. 2020, 13, 1103–1108. [Google Scholar] [CrossRef]
- Glazebrook, K.N.; Doerge, S.; Leng, S.; Drees, T.A.; Hunt, K.N.; Zingula, S.N.; Pruthi, S.; Geske, J.R.; Carter, R.E.; McCollough, C.H.; et al. Ability of Dual-Energy CT to Detect Silicone Gel Breast Implant Rupture and Nodal Silicone Spread. Am. J. Roentgenol. 2019, 212, 933–942. [Google Scholar] [CrossRef]
- Brown, S.L.; Pennello, G.; Berg, W.A.; Soo, M.S.; Middleton, M.S. Silicone gel breast implant rupture, extracapsular silicone, and health status in a population of women. J. Rheumatol. 2001, 28, 996–1003. [Google Scholar] [PubMed]
- Alfano, C.; Mazzocchi, M. Mammary Compliance: An Objective Measurement of Capsular Contracture. Aesthetic Plast. Surg. 2004, 28, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Henriksen, T.F.; Fryzek, J.P.; Hölmich, L.R.; McLaughlin, J.K.; Kjøller, K.; Høyer, A.P.; Olsen, J.H.; Friis, S. Surgical Intervention and Capsular Contracture After Breast Augmentation: A prospective study of risk factors. Ann. Plast. Surg. 2005, 54, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Brody, G.S. On the Safety of Breast Implants. Plast. Reconstr. Surg. 1997, 100, 1314–1321. [Google Scholar] [CrossRef] [PubMed]
- Henriksen, T.F.; Hölmich, L.R.; Fryzek, J.P.; Friis, S.; McLaughlin, J.K.; Høyer, A.P.; Kjøller, K.; Olsen, J.H. Incidence and Severity of Short-Term Complications After Breast Augmentation: Results from a Nationwide Breast Implant Registry. Ann. Plast. Surg. 2003, 51, 531–539. [Google Scholar] [CrossRef]
- Handel, N.; Cordray, T.; Gutierrez, J.; Jensen, J.A. A Long-Term Study of Outcomes, Complications, and Patient Satisfaction with Breast Implants. Plast. Reconstr. Surg. 2006, 117, 757–767. [Google Scholar] [CrossRef]
- Wick, G.; Grundtman, C.; Mayerl, C.; Wimpissinger, T.-F.; Feichtinger, J.; Zelger, B.; Sgonc, R.; Wolfram, D. The Immunology of Fibrosis. Annu. Rev. Immunol. 2013, 31, 107–135. [Google Scholar] [CrossRef]
- Ji, L.; Wang, T.; Tian, L.; Song, H.; Gao, M. Roxatidine inhibits fibrosis by inhibiting NF-κB and MAPK signaling in macrophages sensing breast implant surface materials. Mol. Med. Rep. 2019, 21, 161–172. [Google Scholar] [CrossRef]
- Kuehlmann, B.A.; Bonham, C.A.; Gurtner, G.C. Abstract 114. Plast. Reconstr. Surg.-Glob. Open 2019, 7, 80. [Google Scholar] [CrossRef]
- Kuo, Y.-L.; Jou, I.-M.; Jeng, S.-F.; Chu, C.-H.; Huang, J.-S.; Hsu, T.-I.; Chang, L.-R.; Huang, P.-W.; Chen, J.-A.; Chou, T.-M. Hypoxia-induced epithelial-mesenchymal transition and fibrosis for the development of breast capsular contracture. Sci. Rep. 2019, 9, 10269. [Google Scholar] [CrossRef]
- Biernacka, A.; Dobaczewski, M.; Frangogiannis, N.G. TGF-β signaling in fibrosis. Growth Factors 2011, 29, 196–202. [Google Scholar] [CrossRef]
- Chaikuad, A.; Bullock, A.N. Structural Basis of Intracellular TGF-β Signaling: Receptors and Smads. Cold Spring Harb. Perspect. Biol. 2016, 8, a022111. [Google Scholar] [CrossRef] [PubMed]
- Meng, X.-M.; Nikolic-Paterson, D.J.; Lan, H.Y. TGF-β: The master regulator of fibrosis. Nat. Rev. Nephrol. 2016, 12, 325–338. [Google Scholar] [CrossRef]
- Lan, H.Y. Diverse Roles of TGF-β/Smads in Renal Fibrosis and Inflammation. Int. J. Biol. Sci. 2011, 7, 1056–1067. [Google Scholar] [CrossRef]
- Margadant, C.; Sonnenberg, A. Integrin–TGF-β crosstalk in fibrosis, cancer and wound healing. EMBO Rep. 2010, 11, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.-H.; Chen, D.-Q.; Wang, Y.-N.; Feng, Y.-L.; Cao, G.; Vaziri, N.D.; Zhao, Y.-Y. New insights into TGF-β/Smad signaling in tissue fibrosis. Chem. Interact. 2018, 292, 76–83. [Google Scholar] [CrossRef] [PubMed]
- ISO 14607:2018; Non-Active Surgical Implants—Mammary Implants—Particular Requirements. ISO: London, UK, 2018. Available online: https://www.iso.org/standard/63973.html (accessed on 17 November 2022).
- Stevens, W.G.; Nahabedian, M.Y.; Calobrace, M.B.; Harrington, J.L.; Capizzi, P.J.; Cohen, R.; D’Incelli, R.C.; Beckstrand, M. Risk Factor Analysis for Capsular Contracture: A 5-year sientra study analysis using round, smooth, and textured implants for breast augmentation. Plast. Reconstr. Surg. 2013, 132, 1115–1123. [Google Scholar] [CrossRef] [PubMed]
- Webb, L.H.; Aime, V.L.; Do, A.; Mossman, K.; Mahabir, R.C. Textured Breast Implants: A Closer Look at the Surface Debris Under the Microscope. Plast. Surg. 2017, 25, 179–183. [Google Scholar] [CrossRef]
- Martin, S.V.; Ho, W.; Khan, K. An extended 7-year review of textured breast implants for primary breast augmentation: Allergan versus Mentor. Ann. Breast Surg. 2019, 3, 14. [Google Scholar] [CrossRef]
- Doloff, J.C.; Veiseh, O.; de Mezerville, R.; Sforza, M.; Perry, T.A.; Haupt, J.; Jamiel, M.; Chambers, C.; Nash, A.; Aghlara-Fotovat, S.; et al. The surface topography of silicone breast implants mediates the foreign body response in mice, rabbits and humans. Nat. Biomed. Eng. 2021, 5, 1115–1130. [Google Scholar] [CrossRef] [PubMed]
- Cappellano, G.; Ploner, C.; Lobenwein, S.; Sopper, S.; Hoertnagl, P.; Mayerl, C.; Wick, N.; Pierer, G.; Wick, G.; Wolfram, D. Immunophenotypic characterization of human T cells after in vitro exposure to different silicone breast implant surfaces. PLoS ONE 2018, 13, e0192108. [Google Scholar] [CrossRef] [PubMed]
- Lam, M.; Migonney, V.; Falentin-Daudre, C. Review of silicone surface modification techniques and coatings for antibacterial/antimicrobial applications to improve breast implant surfaces. Acta Biomater. 2020, 121, 68–88. [Google Scholar] [CrossRef] [PubMed]
- Atlan, M.; Nuti, G.; Wang, H.; Decker, S.; Perry, T. Breast implant surface texture impacts host tissue response. J. Mech. Behav. Biomed. Mater. 2018, 88, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Z.; Shurer, C.R.; Schmidt, S.; Gupta, V.K.; Chuang, G.; Su, J.; Watkins, A.R.; Shetty, A.; Spector, J.A.; Hui, C.-Y.; et al. The surface stress of biomedical silicones is a stimulant of cellular response. Sci. Adv. 2020, 6, eaay0076. [Google Scholar] [CrossRef] [PubMed]
- Kyle, D.J.; Oikonomou, A.; Hill, E.; Bayat, A. Development and functional evaluation of biomimetic silicone surfaces with hierarchical micro/nano-topographical features demonstrates favourable in vitro foreign body response of breast-derived fibroblasts. Biomaterials 2015, 52, 88–102. [Google Scholar] [CrossRef]
- Valencia-Lazcano, A.A.; Alonso-Rasgado, T.; Bayat, A. Characterisation of breast implant surfaces and correlation with fibroblast adhesion. J. Mech. Behav. Biomed. Mater. 2013, 21, 133–148. [Google Scholar] [CrossRef]
- McLaughlin, C.; Hughes, A.J.B.; Parham, C.S.; Fritsche, M.B.; Potochny, J.D.; Kunselman, A.M.; Ravnic, D.J.D. Smooth Versus Textured Tissue Expander Breast Reconstruction: Complications and Efficacy. Ann. Plast. Surg. 2022, 88, S288–S292. [Google Scholar] [CrossRef]
- Giot, J.-P.; Paek, L.S.; Nizard, N.; El-Diwany, M.; Gaboury, L.A.; Nelea, M.; Bou-Merhi, J.S.; Harris, P.G.; Danino, M.A. The double capsules in macro-textured breast implants. Biomaterials 2015, 67, 65–72. [Google Scholar] [CrossRef]
- Hall-Findlay, E.J. Breast Implant Complication Review: Double Capsules and Late Seromas. Plast. Reconstr. Surg. 2011, 127, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Loch-Wilkinson, A.; Beath, K.; Knight, R.J.W.; Wessels, W.L.F.; Magnusson, M.; Papadopoulos, T.; Connell, T.; Lofts, J.; Locke, M.; Hopper, I.; et al. Breast Implant–Associated Anaplastic Large Cell Lymphoma in Australia and New Zealand: High-Surface-Area Textured Implants Are Associated with Increased Risk. Plast. Reconstr. Surg. 2017, 140, 645–654. [Google Scholar] [CrossRef]
- Hu, H.; Jacombs, A.; Vickery, K.; Merten, S.L.; Pennington, D.G.; Deva, A.K. Chronic Biofilm Infection in Breast Implants Is Associated with an Increased T-Cell Lymphocytic Infiltrate: Implications for Breast Implant–Associated Lymphoma. Plast. Reconstr. Surg. 2015, 135, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.R.; Chien, P.N.; Trinh, X.-T.; Nam, S.-Y.; Heo, C.-Y. Comparison of Formation of Capsule among Different Breast Silicone Implants. In Vivo 2022, 36, 2756–2766. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.-T.; Park, H.Y.; Jeon, B.-J.; Mun, G.-H.; Bang, S.I.; Pyon, J.K. Does the Textured-Type Tissue Expander Affect the Outcomes of Two-Stage Prosthetic Breast Reconstruction? A Propensity Score Matching Analysis between Macrotextured and Microtextured Expanders. Plast. Reconstr. Surg. 2021, 147, 545–555. [Google Scholar] [CrossRef] [PubMed]
- Fairchild, B.; Ellsworth, W.; Selber, J.C.; Bogue, D.P.; Zavlin, D.; Nemir, S.; Checka, C.M.; Clemens, M.W. Safety and Efficacy of Smooth Surface Tissue Expander Breast Reconstruction. Aesthetic Surg. J. 2020, 40, 53–62. [Google Scholar] [CrossRef]
- Chiu, W.-K.; Fracol, M.; Feld, L.N.; Qiu, C.S.; Kim, J.Y.S. Judging an Expander by Its Cover: A Propensity-Matched Analysis of the Impact of Tissue Expander Surface Texture on First-Stage Breast Reconstruction Outcomes. Plast. Reconstr. Surg. 2021, 147, 1e–6e. [Google Scholar] [CrossRef]
- Dolores, W.; Christian, R.; Harald, N.; Hildegunde, P.; Georg, W. Cellular and molecular composition of fibrous capsules formed around silicone breast implants with special focus on local immune reactions. J. Autoimmun. 2004, 23, 81–91. [Google Scholar] [CrossRef]
- Wolfram, D.; Oberreiter, B.; Mayerl, C.; Soelder, E.; Ulmer, H.; Piza-Katzer, H.; Wick, G.; Backovic, A. Altered systemic serologic parameters in patients with silicone mammary implants. Immunol. Lett. 2008, 118, 96–100. [Google Scholar] [CrossRef]
- Duraes, E.F.R.M.; Durand, P.M.; Morisada, M.M.; Scomacao, I.M.; Duraes, L.C.M.; de Sousa, J.M.B.; Abedi, N.M.; Djohan, R.S.M.; Bernard, S.M.; Moreira, A.M.; et al. A Novel Validated Breast Aesthetic Scale. Plast. Reconstr. Surg. 2022, 149, 1297–1308. [Google Scholar] [CrossRef]
- Prantl, L.; Schreml, S.; Fichtner-Feigl, S.; Pöppl, N.; Eisenmann-Klein, M.; Schwarze, H.; Füchtmeier, B. Clinical and Morphological Conditions in Capsular Contracture Formed around Silicone Breast Implants. Plast. Reconstr. Surg. 2007, 120, 275–284. [Google Scholar] [CrossRef]
- Siggelkow, W.; Gescher, D.; Klee, D.; Malik, E.; Rath, W.; Faridi, A. In Vitro Analysis of Modified Surfaces of Silicone Breast Implants. Int. J. Artif. Organs 2004, 27, 1100–1108. [Google Scholar] [CrossRef]
- Siggelkow, W.; Faridi, A.; Spiritus, K.; Klinge, U.; Rath, W.; Klosterhalfen, B. Histological analysis of silicone breast implant capsules and correlation with capsular contracture. Biomaterials 2003, 24, 1101–1109. [Google Scholar] [CrossRef] [PubMed]
- Handel, N.M.; Jensen, J.A.M.; Black, Q.B.; Waisman, J.R.M.; Silverstein, M.J.M. The Fate of Breast Implants. Plast. Reconstr. Surg. 1995, 96, 1521–1533. [Google Scholar] [CrossRef] [PubMed]
- Mempin, M.; Hu, H.; Chowdhury, D.; Deva, A.; Vickery, K. The A, B and C’s of Silicone Breast Implants: Anaplastic Large Cell Lymphoma, Biofilm and Capsular Contracture. Materials 2018, 11, 2393. [Google Scholar] [CrossRef]
- Bizjak, M.; Selmi, C.; Praprotnik, S.; Bruck, O.; Perricone, C.; Ehrenfeld, M.; Shoenfeld, Y. Silicone implants and lymphoma: The role of inflammation. J. Autoimmun. 2015, 65, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Zhang, S. T Cells in Fibrosis and Fibrotic Diseases. Front. Immunol. 2020, 11, 1142. [Google Scholar] [CrossRef]
- Shin, B.H.; Kim, B.H.; Kim, S.; Lee, K.; Bin Choy, Y.; Heo, C.Y. Silicone breast implant modification review: Overcoming capsular contracture. Biomater. Res. 2018, 22, 37. [Google Scholar] [CrossRef]
- FDA. Risks and Complications of Breast Implants. Available online: https://www.fda.gov/medical-devices/breast-implants/risks-and-complications-breast-implants. (accessed on 21 November 2022).
- Sforza, M.; Zaccheddu, R.; Alleruzzo, A.; Seno, A.; Mileto, D.; Paganelli, A.; Sulaiman, H.; Payne, M.; Maurovich-Horvat, L. Preliminary 3-Year Evaluation of Experience with SilkSurface and VelvetSurface Motiva Silicone Breast Implants: A Single-Center Experience with 5813 Consecutive Breast Augmentation Cases. Aesthetic Surg. J. 2017, 38, S62. [Google Scholar] [CrossRef]
- Wu, S.S.B.; Duraes, E.F.R.M.; Scomacao, I.M.; Morisada, M.B.; Djohan, R.S.M.; Bernard, S.L.M.; Moreira, A.M.; Schwarz, G.S.M. Beauty Is in the Eye of the Beholder: Factors Influencing Disparity in Perceptions of Breast Reconstruction Aesthetic Outcomes. Plast. Reconstr. Surg. 2022, 150, 42e–50e. [Google Scholar] [CrossRef]
- Buck, D.W.; Shenaq, D.; Heyer, K.; Kato, C.; Kim, J.Y. Patient-subjective cosmetic outcomes following the varying stages of tissue expander breast reconstruction: The importance of completion. Breast 2010, 19, 521–526. [Google Scholar] [CrossRef]
- Munhoz, A.M.; Chala, L.; de Melo, G.G.; Filho, A.D.A.M.; Tucunduva, T.; Gemperli, R. Usefulness of Radio Frequency Identification Device in Diagnosing Rotation of Motiva SmoothSilk Implants after Augmentation Mammoplasty. Plast. Reconstr. Surg.-Glob. Open 2019, 7, e2497. [Google Scholar] [CrossRef]
- Hallab, N.J.; Samelko, L.; Hammond, D. The Inflammatory Effects of Breast Implant Particulate Shedding: Comparison with Orthopedic Implants. Aesthetic Surg. J. 2019, 39, S36–S48. [Google Scholar] [CrossRef] [PubMed]
- Kappel, R.M.; Klunder, A.J.H.; Pruijn, G.J.M. Silicon chemistry and silicone breast implants. Eur. J. Plast. Surg. 2013, 37, 123–128. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Committee on the Safety of Silicone Breast Implants. Immunology of Silicone; Bondurant, S., Ernster, V., Herdman, R., Eds.; National Academies Press: Washington, DC, USA, 1999. [Google Scholar]
- Dieterich, M.; Paepke, S.; Zwiefel, K.; Dieterich, H.; Blohmer, J.; Faridi, A.; Klein, E.; Gerber, B.; Nestle-Kraemling, C. Implant-Based Breast Reconstruction Using a Titanium-Coated Polypropylene Mesh (TiLOOP Bra). Plast. Reconstr. Surg. 2013, 132, 8e–19e. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.X.; Cheng, L.; Xu, L.Y.; Zhu, Y.L. A short follow-up of prosthesis-based breast reconstruction using TiLOOP Bra surgical mesh. Niger. J. Clin. Pract. 2019, 22, 1115–1119. [Google Scholar] [PubMed]
- Casella, D.; Bernini, M.; Bencini, L.; Roselli, J.; Lacaria, M.T.; Martellucci, J.; Banfi, R.; Calabrese, C.; Orzalesi, L. TiLoop Bra mesh used for immediate breast reconstruction: Comparison of retropectoral and subcutaneous implant placement in a prospective single-institution series. Eur. J. Plast. Surg. 2014, 37, 599–604. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Female sex | 1 | Sever coagulation disorder, representing a potential contraindication for the elective surgery |
| Age > 18 years | 2 | Rheumatic disease accompanied by oblkigatory intake of immunomodulating therapeutic agents |
| High-risk family history for breast and/or ovarian cancer and/or BRCA1/2 gene mutation carrier | 3 | Severe renal functional disorder: renal insufficiency status IV or V (estimated glomerulary filtration rate (GFR) < 30 mL/min) |
| Planned bilateral mastectomy with simultaneous breast reconstruction | 4 | Active hematological or oncological disease |
| Signed Informed consent form. | 5 | HIV-Infection |
| 6 | Hepatitis-Infection | |
| 7 | Pregnancy or breast-feeding | |
| 8 | Intake of anti-inflammatory drugs | |
| 9 | Carrier of silicone implants (e.g., gastric banding, mammary implants) |
| Surgeon Scale | Time Point Post Op | Numeric Scale |
|---|---|---|
| How satisfied are you with the lower pole expansion of the expander? | 6–8 M | not satisfied: 0 to 3 satisfied 4 to 7 very satisfied: 8 to 10 |
| How satisfied are you with the footprint created by the expander? | 6–8 M | |
| Patient Scale | Time Point Post Op | |
| How satisfied are you with the expander? | 4 W | not satisfied: 0 to 3 satisfied 4 to 7 very satisfied: 8 to 10 |
| Please indicate how comfortable the expander was? | 6–8 M | not comfortable: 0 to 3 comfortable 4 to 7 very comfortable: 8 to 10 |
| IMPLANTATION SITE | Left: SmoothSilk®; Right: Mentor CPX4 | Left: Mentor CPX4; Right: SmoothSilk® | |||||
|---|---|---|---|---|---|---|---|
| PAT 001_001 | PAT 001_002 | PAT 001_007 | PAT 001_003 | PAT 001_004 | PAT 001_005 | PAT 001_006 | |
| Vital Parameters | |||||||
| age (y) | 34 | 41 | 30 | 31 | 26 | 60 | 33 |
| weight (kg) | 86,3 | 54 | 108 | 54 | 58 | 105 | 57 |
| size (cm) | 186,5 | 155,5 | 172 | 167 | 159 | 176 | 166 |
| BMI | 24.8 | 22.3 | 36.5 | 19.4 | 22.9 | 33.9 | 20.7 |
| body surface area | 2.12 | 1.52 | 2.9 | 1.6 | 1.59 | 2.2 | 2.7 |
| Status of natural breast | |||||||
| asymmetry | no | no | no | no | no | no | no |
| scars | no | no | no | no | no | no | no |
| diseases | no | no | no | no | no | no | no |
| active smoker | yes | no | no | no | no | no | no |
| allergies | no | no | no | no | no | no | no |
| Chronic diseases | |||||||
| diabetes | no | yes | no | no | no | no | no |
| Other | |||||||
| job | manual job | office job | office job | office job | office job | manual job | office job |
| physical training (h/week) | >2 | >2 | 0.5–2 | >2 | >2 | 0.5–2 | 0.5–2 |
| dominant hand | right | right | right | right | right | right | right |
| 1st operation: tissue expander implantation | |||||||
| Bilateral prophylactic NSME resection weight [g] | |||||||
| right breast | 449 | 187 | 980 | 200 | 400 | 750 | 208 |
| left breast | 471 | 167 | 1060 | 200 | 450 | 575 | 252 |
| Prepectoral reconstruction volume [cc] | |||||||
| Motiva Flora® SmoothSilk® | 450 | 260 | 570 | 260 | 440 | 570 | 260 |
| Mentor CPX4 | 440 | 250 | 550 | 250 | 450 | 550 | 250 |
| Intrapoerative filling (both devices) | 250 | 150 | 550 | 150 | 300 | 500 | 150 |
| SmoothSilkⓇ | Mentor CPX4 | ||||
|---|---|---|---|---|---|
| Surface Roughness | Ra ~ 4 µM | Ra ~ 60 µM | |||
| Mean | (±std) | Mean | (±std) | p Value | |
| age (y) | 35.2 | 11.4 | 35.2 | 11.4 | intraindividual comparison >0.9999 |
| weight (kg) | 71.4 | 24.5 | 71.4 | 24.5 | |
| size (cm) | 168.6 | 10.5 | 168.6 | 10.5 | |
| BMI | 25.1 | 6.7 | 25.1 | 6.7 | |
| Bilateral prophylactic NSME resection weight [g] | |||||
| left breast | 434.9 | 404.0 | 436.9 | 454.0 | 0.993196 |
| right breast | 334.2 | 257.5 | 337.9 | 174.4 | 0.975407 |
| Prepectoral reconstruction volume [cc] | |||||
| left breast | 405.5 | 156.3 | 392.6 | 151.8 | 0.877595 |
| right breast | 360.8 | 151.1 | 352.7 | 150.0 | 0.920737 |
| intaoperative filling [mL] | 254.7 | 169.4 | 254.7 | 169.4 | intraindividual comparison >0.9999 |
| exchange time point [d] | 204.8 | 25.8 | 204.8 | 25.8 | |
| SmoothSilk® | Mentor CPX4 | |||||
|---|---|---|---|---|---|---|
| Surface Roughness | Ra ~ 4 µM | Ra ~ 60 µM | ||||
| Time Point Post Op | Mean | (±std) | Mean | (±std) | p Value | |
| Wound dehiscence | 2 W, 4 W, 16 W | no | no | >0.9999 | ||
| Signs of inflammation | 2 W, 4 W, 16 W | no | no | >0.9999 | ||
| symmetry | 2 W, 4 W, 16 W | yes | yes | >0.9999 | ||
| Breast structure swelling | 2 W, 4 W, 16 W | no | no | >0.9999 | ||
| Expander malposition | 2 W, 4 W, 16 W | no | no | >0.9999 | ||
| filling visits | 6–8 M | 0.86 | 0.90 | 0.86 | 0.90 | >0.9999 |
| Palpation | ||||||
| firm | 2 W, 4 W, 16 W | 1 (14.30%) | 0 (0%) | |||
| normal | 2 W, 4W, 16 W | 3 (42.85%) | 6 (85.70%) | |||
| soft | 2 W, 4 W, 16 W | 3 (42.85%) | 1 (14.30%) | |||
| SmoothSilk® | Mentor CPX4 | |||||
|---|---|---|---|---|---|---|
| Surface Roughness | Ra ~ 4 µM | Ra ~ 60 µM | ||||
| Surgeon scale | time point post op | Mean | (±std) | Mean | (±std) | p value |
| How satisfied are you with the lower pole expansion of the expander? | 6–8 M | 9.00 | 0.63 | 7.33 | 1.37 | 0.021872 * |
| How satisfied are yopu with the footprint created by the expander? | 6–8 M | 8.67 | 0.52 | 7.17 | 1.72 | 0.068264 |
| Patient scale | time point post op | Mean | (±std) | Mean | (±std) | pvalue |
| How satisfied are you with the expander? | 4W | 9.50 | 1.22 | 7.67 | 1.21 | 0.026164 * |
| Please indicate how comfortable the expander was? | 6-8M | 8.83 | 0.98 | 5.67 | 2.88 | 0.028731 * |
| numeric scale | very satisfied: 10 to 7 | satisfied 7 to 4 | not satisfied: 3 to 0 | |||
| very comfortable: 10 to 7 | comfortable 7 to 4 | not comfortable: 3 to 0 | ||||
| First Stage of Reconstruction | Second Stage of Reconstruction | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Expander Type | Mentor CPX4 * | SmoothSilk® * | Mentor CPX4 * | SmoothSilk® * | ||||||
| Surface Roughness | Ra ~ 60 µM | Ra ~ 4 µM | Ra ~ 60 µM | Ra ~ 4 µM | ||||||
| Questions | Mean | (±std) | Mean | (±std) | p-Value | Mean | (std) | Mean | (std) | p-Value |
| Breast | ||||||||||
| Breast position | 4.04 | (0.57) | 4.07 | (0.59) | 0.9173 | 4.25 | (0.50) | 4.25 | (0.58) | >0.999 |
| Inframammary fold | 4.50 | (0.44) | 4.21 | (0.56) | 0.3454 | 4.38 | (0.49) | 4.50 | (0.48) | 0.6933 |
| Volume | 4.36 | (0.35) | 4.36 | (0.35) | >0.999 | 4.38 | (0.66) | 4.29 | (0.68) | 0.8482 |
| Shape and contour | 3.79 | (0.85) | 3.75 | (0.81) | 0.9419 | 4.29 | (0.53) | 4.17 | (0.61) | 0.7355 |
| Scar | ||||||||||
| Appearance | 4.54 | (0.47) | 4.46 | (0.59) | 0.8205 | 4.50 | (0.52) | 4.54 | (0.44) | 0.8943 |
| Nipple-Areola Complex | ||||||||||
| Nipple position | 4.29 | (0.51) | 4.29 | (0.63) | >0.999 | 4.58 | (0.47) | 4.29 | (0.73) | 0.4693 |
| First Stage | Second Stage | ||||
|---|---|---|---|---|---|
| Questions | Mean | (±std) | Mean | (±std) | p-Value |
| Breast | |||||
| Symmetry | 4.29 | (0.54) | 4.42 | (0.49) | 0.6850 |
| Breast position | 4.05 | (0.58) | 4.25 | (0.54) | 0.4035 |
| Inframammary fold | 4.36 | (0.52) | 4.44 | (0.49) | 0.7031 |
| Volume | 4.36 | (0.35) | 4.33 | (0.67) | 0.9125 |
| Shape and contour | 3.77 | (0.83) | 4.23 | (0.57) | 0.1326 |
| Scar | |||||
| Appearance | 4.50 | (0.53) | 4.52 | (0.48) | 0.9216 |
| Nipple-Areola Complex | |||||
| Nipple position | 4.29 | (0.57) | 4.44 | (0.63) | 0.5428 |
| Overall Appearance | 4.04 | (0.65) | 4.31 | (0.71) | 0.3271 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schoberleitner, I.; Augustin, A.; Egle, D.; Brunner, C.; Amort, B.; Zelger, B.; Brunner, A.; Wolfram, D. Is It All about Surface Topography? An Intra-Individual Clinical Outcome Analysis of Two Different Implant Surfaces in Breast Reconstruction. J. Clin. Med. 2023, 12, 1315. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12041315
Schoberleitner I, Augustin A, Egle D, Brunner C, Amort B, Zelger B, Brunner A, Wolfram D. Is It All about Surface Topography? An Intra-Individual Clinical Outcome Analysis of Two Different Implant Surfaces in Breast Reconstruction. Journal of Clinical Medicine. 2023; 12(4):1315. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12041315
Chicago/Turabian StyleSchoberleitner, Ines, Angela Augustin, Daniel Egle, Christine Brunner, Birgit Amort, Bettina Zelger, Andrea Brunner, and Dolores Wolfram. 2023. "Is It All about Surface Topography? An Intra-Individual Clinical Outcome Analysis of Two Different Implant Surfaces in Breast Reconstruction" Journal of Clinical Medicine 12, no. 4: 1315. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12041315