
Proprioceptive Cervicogenic Dizziness Care Trajectories in Patient Subpopulations: A Scoping Review

1
School of Rehabilitation, Faculty of Medicine, University of Montreal, Montreal, QC H3N 1X7, Canada
2
Center for Interdisciplinary Research in Rehabilitation of Greater Montreal (IURDPM), CRIR, CIUSSS South-Center, Montreal, QC H3S 1M9, Canada
3
Collège d’Études Ostéopathique de Montréal (CEOM), Montréal, QC H3G 1W7, Canada
4
Division of Otolaryngology, Head and Neck Surgery—Otology and Neurotology, Montreal University Hospital Center (CHUM), University of Montreal, Montreal, QC H2X 3E4, Canada
*
Author to whom correspondence should be addressed.
J. Clin. Med. 2023, 12(5), 1884; https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12051884
Submission received: 24 January 2023
/
Revised: 12 February 2023
/
Accepted: 24 February 2023
/
Published: 27 February 2023
(This article belongs to the Special Issue Recent Advances in Diagnosis and Treatment of Vestibular Disorders)
Abstract
:Proprioceptive cervicogenic dizziness (PCGD) is the most prevalent subcategory of cervicogenic dizziness. There is considerable confusion regarding this clinical syndrome’s differential diagnosis, evaluation, and treatment strategy. Our objectives were to conduct a systematic search to map out characteristics of the literature and of potential subpopulations of PCGD, and to classify accordingly the knowledge contained in the literature regarding interventions, outcomes and diagnosis. A Joanna Briggs Institute methodology-informed scoping review of the French, English, Spanish, Portuguese and Italian literature from January 2000 to June 2021 was undertaken on PsycInfo, Medline (Ovid), Embase (Ovid), All EBM Reviews (Ovid), CINAHL (Ebsco), Web of Science and Scopus databases. All pertinent randomized control trials, case studies, literature reviews, meta-analyses, and observational studies were retrieved. Evidence-charting methods were executed by two independent researchers at each stage of the scoping review. The search yielded 156 articles. Based on the potential etiology of the clinical syndrome, the analysis identified four main subpopulations of PCGD: chronic cervicalgia, traumatic, degenerative cervical disease, and occupational. The three most commonly occurring differential diagnosis categories are central causes, benign paroxysmal positional vertigo and otologic pathologies. The four most cited measures of change were the dizziness handicap inventory, visual analog scale for neck pain, cervical range of motion, and posturography. Across subpopulations, exercise therapy and manual therapy are the most commonly encountered interventions in the literature. PCGD patients have heterogeneous etiologies which can impact their care trajectory. Adapted care trajectories should be used for the different subpopulations by optimizing differential diagnosis, treatment, and evaluation of outcomes.
1. Introduction
1.1. Background and Rationale
The prevalence of dizziness among people of working age (18 to 65 years old) is 20%–30% [1,2,3,4], and it is the number one reason for medical consultations for people over 75 years old [5]. Cervicogenic dizziness, cervical vertigo, and cervicogenic vertigo are interchangeable terms that refer to dizziness that is closely associated with neck pain, neck injury, or neck pathology. Many consider it to be one of the most common causes of dizziness, as it contributes to major social costs, insurance claims and handicap [3,6,7,8]. Throughout this manuscript, dizziness is understood as a non-rotatory illusion of movement, accompanied by disequilibrium and lightheadedness.
As a consequence of the absence of a gold standard testing procedure, cervicogenic dizziness’s diagnosis is based on clinical presentation and the exclusion of other possible causes of dizziness [9,10,11]. However, researchers and clinicians should not only distinguish this syndrome from other pathologies, but should also distinguish between the many potential etiologies that can lead to cervicogenic dizziness [11]. Indeed, patients with cervicogenic dizziness are not a homogeneous group, and have been classified into subgroups of individuals who share similar clinical characteristics. They were categorized to account for the differences in clinical presentation and care trajectory, as well as the notion that subgrouping improves disease knowledge acquisition [11]. The care trajectory refers to the itinerary of a patient through the healthcare system and among the different actors over a continuous period from the onset of the illness to its resolution [12]. However, even if the concept of subgroups has developed over the past two decades, it is still poorly understood, underused in the clinical and research setting, and has not yet been systematically examined. Before undertaking this review, a preliminary search using Medline (Ovid), Embase (Ovid), All EBM Reviews (Ovid), and CINAHL (Ebsco) for existing scoping reviews and systematic reviews on the subject was conducted on 5 May 2021. Most reviews were narrative and, although very informative, related to the general concept of cervicogenic dizziness, implying different subsets of patients and lacking systematic reporting of charting methods. The few systematic reviews were not scoping reviews. Therefore, this scoping review focuses on the care trajectory of the most common subset of cervicogenic dizziness in an articulated scope of inquiry, that of proprioceptive cervicogenic dizziness (PCGD) [9,11,13,14,15].
PCGD is experienced as non-rotatory vertigo, instability and disequilibrium associated with neck pain caused by abnormal afferent cervical proprioceptive activity [3,9,16]. It corresponds to what numerous authors would refer to as cervicogenic dizziness. The term PCGD will be used in this article, as proposed by Devaraja (2018), because it is more precise and eliminates other possible causes of cervicogenic dizziness, such as cervical vascular etiology [11,17]. Thus, this review will focus exclusively on the potential proprioceptive etiology of cervicogenic dizziness. PCGD is a diagnosis of exclusion [3,9,10,11,18] and exhibits a complex and heterogeneous nature. Different groups of patients are diagnosed with PCGD [11]. The specific proprioceptive mechanisms leading to PCGD may be different across individuals [9,11] and there is still confusion regarding this clinical syndrome. Indeed, encounters with dizzy patients should be distinguishing into vascular, vestibular, central, metabolic, pharmaceutical, orthopedic, iatrogenic, psychological, optometric and somatosensory pathologies [9,10,11]. Comorbidities are often encountered in this complex clinical context. Accordingly, there is inappropriate and insufficient diagnostic accuracy and treatment related to PCGD, which often results in lengthy care trajectories [8]. Differential diagnoses, diagnostic criteria, optimal treatment [4], and outcome measures must be mapped out to help shorten care trajectories for these complex patients.
1.2. Objectives and Review Questions
Hence, the objectives of this scoping review are to clarify the conceptual boundaries of PCGD and to map out the main research designs used to study PCGD and the key characteristics of affected patient populations. To do so, we will: (1) systematically identify the key characteristics of the literature and populations that have PCGD and (2) classify accordingly the knowledge contained in the literature in regard to interventions, outcomes and diagnosis.
Therefore, our review question can be summarized by the following: How has PCGD been studied, diagnosed, evaluated and treated in the pertinent literature, considering the key characteristics of patient subpopulations? This question implies the following interrogations: (1) What are the main research designs used to study PCGD? (2) Which subpopulations of patients does a PCGD diagnosis represent? (3) Which common differential diagnoses are associated with those subpopulations? (4) What evaluation tools are mentioned to identify the diagnosis? (5) What interventions have been considered by researchers for the management of PCGD? (6) What outcome measures have been used?
2. Materials and Methods
Protocol and registration: This scoping review was informed by the Joanna Briggs Institute methodology [19]. As such, Preferred Reporting Items for Systematic Reviews and meta-analyses (PRISMA ScR) guidelines were followed to redact this systematic scoping review [20,21]. There was no a priori protocol published, because it was not recommended at the time of the beginning of the study.
Eligibility criteria: French, English, Spanish, Portuguese, and Italian articles were included in the review, as these languages are the ones fully understood by the reviewers. Randomized control trials, case studies, literature reviews, meta-analyses, and observational studies were included in this article. Expert advice, commentaries and letters were excluded to focus on higher evidence-level articles. Articles on animals were excluded because they cannot answer the research question. Research protocols were excluded as they do not yet contain a sample of patients and therefore cannot help to reach the scoping review’s objectives. Conference abstracts were excluded as they can potentially contain mistakes and have not been properly peer-reviewed.
Types of participants: Articles concerning patients that have proprioceptive cervicogenic dizziness (PCGD) with or without associated conditions were included to identify all subpopulations and pertinent information on the specific characteristics and care trajectories associated with PCGD. Articles related exclusively to patients that did not present PCGD, with dizziness of vascular, central, vestibular or pharmacological causes, were excluded as they do not contain information about PCGD. Studies on healthy subjects were included if they were related to PCGD.
Concept: The relevant care trajectory elements to extract included differential diagnoses, diagnostic and predictive tools, and evaluative assessments to measure change and interventions.
Context: Articles written before 2000 were excluded. The recent introduction of new diagnosis entities with similar clinical presentations such as persistent postural-perceptual dizziness (PPPD) and vestibular migraine suggests that only the recent literature informed by those new diagnoses can have homogeneous samples of PCGD. Additionally, the separation of cervicogenic dizziness from proprioceptive etiologies (PCGD) and cervicogenic dizziness from other etiologies (i.e., vascular) was not suggested before 2000, to our knowledge.
Information sources and search strategy: A first limited search of MEDLINE (Ovid) and CINAHL to analyze the text words contained in the title and abstract of retrieved papers, and of the index terms used to describe the articles, was performed. The PsycINFO, Medline (Ovid), Embase (Ovid), All EBM Reviews (Ovid), CINAHL (Ebsco), Web of Science and Scopus databases were then searched using a Boolean strategy recommended by the university’s research librarian. As an example, «((cervicogenic or cervical or proprioceptive) adj3 (vertigo* or dizziness)).ab,kf,ti.» was used to search Embase (Ovid). The rest of the strategies and corresponding databases can be consulted in Supplementary Appendix SA: SEARCH STRATEGY. The results yielded from this second step were exported in «.ris» format to the Covidence digital application to complete the review’s methodology on 14 June 2021.
Evidence screening and selection: Both the title and abstract screening and the full-text review were carried out by two independent reviewers (including the main author) to identify potential literature and exclude irrelevant articles. Conflicts were settled by the main author and another independent researcher in consensus. Two separate reviewers extracted information from the articles, and consensus was reached with the main author of this scoping review. Additionally, cross-referencing was used to access primary sources concerning themes such as measuring tools, competing diagnoses, and epidemiology. A particular effort was made to find grey literature through contact with the main authors on the subject, but no unpublished literature was recruited with this approach.
Extraction and data charting process: A pilot testing of the extraction tool available in Covidence software was conducted by separate reviewers. This resulted in the modification and personalization of the final extraction tool, which allowed for all relevant results to be extracted to meet the scoping review’s objective (Supplementary Appendix SB).
Data items: Due to feasibility considerations, we limited the amount of data that we reported to study designs, subpopulations, differential diagnoses, diagnostic tools, interventions and outcome measures.
Synthesis of result: A descriptive quantitative synthesis of the evidence is provided by a tabulation and census of articles that relate each aspect of the care trajectory. Review articles are treated separately in some figures, and are not considered in other figures in order to give a true representation of the literature and to avoid double counting of data. A descriptive narrative of evidence is also presented.
3. Results
3.1. Extracting and Charting the Results
The aforementioned methodology yielded 1741 studies. A total of 797 articles were left after Covidence automatically removed articles recognized to be duplicates (n = 944). The selected articles were then screened by two independent reviewers based on title and abstract. Some 516 studies were excluded because they were found irrelevant based on inclusion/exclusion criteria. A total of 281 articles were assessed for eligibility in a full-text selection process by two independent reviewers. Some 125 studies were excluded following a full-text review based on the exclusion criteria (see Supplementary Appendix SC for the list and reason for exclusion). Conflicts were settled by consensus both in the title and abstract selection stage, and the full-text selection stage with the input of a third party (the last author of this paper). Finally, 156 studies were identified and selected for inclusion in the scoping review. A detailed search decision flowchart is presented in Figure 1.
3.1.1. Study Designs
A variety of different study designs were included: 17 randomized control trials (RCT) [22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38], 14 quasi-experimental studies [39,40,41,42,43,44,45,46,47,48,49,50,51,52], 84 observational studies of various designs (6 prospective cohort studies [53,54,55,56,57,58], 15 retrospective cohort studies [6,59,60,61,62,63,64,65,66,67,68,69,70,71,72], 20 case reports and case series [73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92], 33 cross-sectional studies [14,16,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123], 10 case–control studies [15,124,125,126,127,128,129,130,131,132]), 9 systematic reviews [18,133,134,135,136,137,138,139,140], and 32 narrative reviews [1,3,4,7,9,10,11,141,142,143,144,145,146,147,148,149,150,151,152,153,154,155,156,157,158,159,160,161,162,163,164,165]. No qualitative studies, scoping reviews or pragmatic control trials have been published on PCGD. Figure 2 illustrates a quantitative synthesis of the study designs in the PCGD literature.
3.1.2. Subpopulations of PCGD
A total of 81.9% of articles, reviews and other designs acknowledge at least one subpopulation in PCGD. Some 43.9% of articles acknowledge more than one subpopulation. A total of 28 of the 156 selected articles do not mention subpopulations in PCGD (18.1%). In total, four subpopulations of PCGD are identified in the literature: (A) chronic cervicalgia [7,13,14,15,22,24,25,26,28,29,30,31,34,36,37,41,45,46,50,56,58,60,61,63,64,65,66,68,73,74,75,77,78,81,82,84,85,86,89,90,92,95,98,99,100,109,110,115,116,118,120,124,126,142,146,148,153,163,166,167], (B) traumatic [1,6,7,9,10,11,13,16,23,24,29,31,37,38,39,42,45,50,55,62,63,64,65,66,69,75,77,81,82,86,87,88,90,95,96,98,99,103,106,107,109,112,114,116,119,124,125,127,137,138,140,141,142,143,145,148,149,150,152,154,157,158,162,163,164,168], (C) degenerative cervical disease [1,3,6,7,9,10,11,15,16,23,24,27,31,36,45,51,52,56,58,69,71,72,78,79,80,90,94,96,98,99,101,104,106,108,115,117,120,124,126,127,128,131,132,137,143,145,149,152,153,154,156,158,163,166,169,170], and (D) occupational postures and muscle fatigue or spasm [4,7,9,55,61,79,84,102,104,113,114,115,124,143,146,153,171] (see Table 1). Those potential etiological factors may alter in their specific ways the function of mechanoreceptors found in the smooth tissues (muscle, cartilage, tendons and ligaments) of the cervical region [4,16,146]. An illustrated quantitative synthesis of PCGD subpopulations’ occurrence in the literature may be found in Figure 3.
3.1.3. Assessments Used for the Diagnosis of PCGD
- Differential diagnoses and their assessment tools
As PCGD is a diagnosis of exclusion, the literature mentions 23 potential pathologies or group of pathologies to be ruled out. These are presented in a quantitative illustrated synthesis in Figure 4. Central causes [15,16,23,26,27,29,30,31,33,34,35,40,41,42,44,46,50,52,54,57,58,59,63,65,66,67,68,70,71,73,74,76,82,83,85,89,93,95,96,98,101,102,103,104,106,107,108,109,110,112,114,115,118,120,123,125,126,128,130,131,132,166], benign paroxysmal positional vertigo (BPPV) [15,16,22,23,24,25,26,29,30,31,32,39,42,54,55,56,57,59,63,65,66,67,70,74,76,82,83,84,86,88,90,99,101,102,103,104,107,108,109,110,111,112,114,115,125,126,132,156,166] and otologic pathologies [22,23,24,28,31,32,33,34,40,44,49,53,54,56,58,59,60,61,68,74,75,76,77,78,80,81,82,83,92,95,100,102,104,106,107,108,112,123,125,128,131] are the three most commonly occurring differential diagnosis categories in the literature on PCGD. The occurrence of differential diagnoses in articles mentioning different subpopulations of PCGD is presented in Table 2.
Furthermore, a total of 32 measuring tools contributing to the differential diagnosis process were mentioned in the literature. The most mentioned tools enabling this differential diagnosis process in the literature are presented in a quantitative illustrated synthesis in Figure 5. The Dix-Hallpike maneuver [10,15,16,22,23,24,26,29,30,31,35,38,39,42,55,56,57,59,65,66,75,76,81,82,84,86,90,99,101,104,107,108,109,112,115,123,125,128,130,132], magnetic resonance imaging (MRI) [6,31,42,56,58,60,67,70,71,78,81,82,86,90,92,93,95,98,99,100,106,107,108,109,110,114,115,117,126,128,132,166], cervical spine x-ray imagery (X-ray) [15,27,28,35,39,46,56,57,58,69,70,71,77,81,84,89,90,93,96,99,100,102,106,116,119,123,124,128,129] and audiological testing [15,41,42,47,51,55,56,58,60,62,67,69,70,74,81,82,93,95,98,99,101,106,107,108,109,110,114,123,125,129] are the four most reported tools to guide the differential diagnosis process. The Dix-Hallpike maneuver can identify BPPV, MRI can objectify some central causes, cervical x-rays can identify a vertebral fracture and audiological testing helps in the diagnosis of different otologic pathologies.
- Inclusive diagnostic tools (rule-in)
While exclusion diagnosis implies clinicians will «rule out» other pathologies, some clinical tests can also help to inform clinicians by trying to «rule in» PCGD. A list of the most often-cited tests is found in Figure 6. The two most cited clinical tests mentioned in the literature are palpation for segmental tenderness [6,10,16,23,24,25,26,28,29,34,35,36,40,43,45,51,55,60,61,66,73,74,76,77,78,81,84,85,87,90,93,95,98,100,103,104,107,109,120,126,128,129] and manual spinal evaluation [10,16,22,23,26,27,28,31,35,36,40,41,51,55,56,59,61,69,72,73,74,75,77,78,81,82,85,87,90,93,103,104,125,126,128].
3.1.4. Interventions and Outcome Measures
Many therapeutic interventions were found (n = 34) in the PCGD literature (see Table 3). These included modalities from physiotherapy, Chinese medicine, pharmacology, allopathic medicine, chiropractic medicine, and other approaches. Across subpopulations, exercise therapy [22,23,25,26,27,31,34,37,38,40,42,51,59,60,65,74,81,82,84,85,87,90,125,128,166] and manual therapy [22,23,24,25,26,27,28,31,33,36,38,40,41,42,46,59,60,76,78,79,82,84,87,90,101,107,124,128] are the most commonly encountered intervention in the relevant literature, as shown in Figure 7. The occurrence of interventions in articles mentioning different subpopulations of PCGD are presented in Table 4.
While evaluating the efficiency of treatment, the 17 most commonly encountered outcome measures relevant to PCGD literature are presented in Figure 8. A total of 77 measuring tools were found in the literature. The four most cited measures of change were: dizziness handicap inventory (DHI) [16,23,24,25,26,27,28,29,30,31,32,33,34,35,42,56,66,68,76,77,78,81,85,89,90,95,98,104,107,108,109,110,117,120,128,130], Visual analog scale (VAS) for neck pain [16,23,24,25,26,27,30,31,34,40,41,51,54,60,64,68,71,73,74,76,77,78,81,84,86,90,100,106,109,110,116,117,118,126,128,166], cervical range of motion (CROM) [22,23,24,25,26,28,29,33,40,41,46,51,52,60,76,78,84,85,87,106,108,109,120,128] and posturography [16,23,24,25,26,29,33,34,39,40,43,46,47,48,62,85,95,106,107,110,119] (see Figure 8). Across subpopulations, measures of change used in trials are fairly similar (see Table 5). Dizziness is a multidimensional rehabilitation problem [172]. These dimensions should be considered when measuring treatment effectiveness. Figure 9 uses the International Classification of Functioning, Disability and Health to classify the most common health outcomes of functioning and disability found in the PCGD literature. The body function category (Figure 9) regroups many self-reported and performance-reported outcomes related to the many dimensions of PCGD: proprioceptive and sensorimotor performance (posturography, joint position error test (JPE) and Romberg), self-reported pain (VAS for cervicalgia and headaches), the amplitude of cervical movement (CROM), frequency and intensity of dizziness, level of self-perceived disability (DHI, neck disability index (NDI)), quality of life (SF-36), medical imagery of the cervical spine (X-Ray), and levels of anxiety and depression (Hospital Anxiety and Depression Scale (HADS)). Some self-reported outcomes measuring body functions also comprise items relative to activity and, to a much lesser degree, to the participation category (DHI and SF-36). Indeed, dizziness can limit social participation and engagement and the ability to work, and may even exclude a patient from his profession [172]. DHI and SF-36 do not include specific items related to the social contribution of patients, such as their ability to work, their days on sick leave and the personal economic impact of the disease. In the literature, only one article reported on sick leave in PCGD [105].
4. Discussion
This article focused on the following central questions: (1) What are the main research designs used to study PCGD? (2) Which subpopulations of patients does a PCGD diagnosis represent? (3) What common differential diagnoses are associated with those subpopulations? (4) What evaluation tools are mentioned to identify the diagnosis? (5) What interventions have been considered by researchers for management? (6) Which outcome measures have been used?
To our knowledge, this is the first scoping review undertaken on the topic of PCGD. Four subpopulations of PCGD have been identified: chronic neck pain, degenerative cervical disease, traumatic and occupational subpopulations (muscle spasm). Central causes of dizziness and BPPV are the most often-mentioned potential diagnoses that compete with PCGD. The Dix-Hallpike maneuver is the most cited tool to inform differential diagnosis. Manual therapy and exercise therapy are the most studied interventions in the field. DHI is the most often-encountered measure of change used in this literature.
4.1. Designs
Many study designs were selected for this review (see Figure 2). Randomized control trials represent only approximately 10% of the selected literature. Observational studies are the most common designs. No qualitative protocols on the subject were found in any database; this type of research should be encouraged because evidence-informed practice, value-based healthcare approaches and patient participatory paradigms require a more qualitative knowledge of the experience of patients suffering from PCGD in order to focus on what matters to them [173].
4.2. Subpopulations
Four subpopulations of PCGD have been identified that reflect the relatively heterogeneous population of PCGD. The reasons that some people develop PCGD and others do not, even though they are part of traumatic, degenerative cervical disease, muscle spasms or chronic neck pain populations, remain unknown [158]. Maybe differences in sensorial strategies between individuals could account for that. Patients keener on using proprioceptive input will be more at risk of developing PCGD in comparison with patients who rely more heavily on vestibular or visual cues for posture and gait. As patients can be part of more than one subpopulation of PCGD, research could investigate how cumulating etiological factors could predict poor prognosis [174]. Because PCGD pertains to different subpopulations, it is a «cross-cutting complaint» that concerns different specialties. As such, our results support the Bárány Society’s recommendation to form multidisciplinary research teams to study PCGD [175], and their calls for interdisciplinary efforts in the clinic.
4.3. Competing Diagnoses, Differential Diagnosis and Comorbidity
Since PCGD is an exclusion diagnosis, central causes, cardiac disease and otological pathologies are among the four most cited pathological categories to be ruled out (see Figure 4). Unfortunately, these categories lack precision because they regroup numerous pathologies and are too elusive to effectively orient the differential diagnosis process and inform clinicians. BPPV, on the other hand, is the most cited specific diagnosis in this literature. It is also cited often as an important diagnosis to rule out, no matter what the subpopulation of PCGD is (see Table 2). It is therefore no surprise that the relatively simple Dix-Hallpike maneuver is the most cited test to rule out competing pathologies with PCGD (see Figure 5). Indeed, this test associated with adequate nystagmus analysis; paroxysmal presentation of symptoms and history taking can signal a BPPV diagnosis, but only for posterior canal issues. Lateral canal issues are not objectified with this test.
Knowledge of subpopulations could orient clinicians toward the most accurate and pertinent use of resources in terms of diagnostic tools. Indeed, certain differential diagnostic processes are more often encountered in articles recognizing specific subpopulations of PCGD.
In the literature on the traumatic subpopulation of PCGD, vertebral fractures and particularly traumatic brain injury are more often mentioned than in any other subpopulation. Additionally, there are relatively fewer mentions of the necessity to exclude cardiac diseases in the literature on the traumatic subpopulation of PCGD compared with other subpopulations. Clinicians could orient their diagnostic process toward a rather orthopedic direction rather than a cardiovascular direction in this subpopulation. While MRI, neurological examination and X-ray are cited in the literature on PCGD to help with differential diagnoses (see Figure 5), there are relatively few mentions of orthopedic examination for vertebral fracture signs and ligament testing. This could indicate that clinicians rely more on imagery than clinical testing, and could use clinical testing more, especially with the traumatic population.
In the literature on the degenerative cervical disease subpopulation of PCGD, cardiac disease and drug-induced dizziness are relatively more often cited than in any other subpopulation. This might be because the degenerative cervical disease subpopulation is more likely to be elderly, have cardiac conditions and be exposed to multiple drug issues [176]. Indeed, cardiac history and testing is the 7th most cited evaluation used in differential diagnosis (see Figure 5).
Incidentally, psychogenic vertigo is cited relatively more often in both the traumatic and the degenerative cervical disease subpopulations than in the other subgroups. This could be explained by the potential psychological impacts related to trauma or ageing. Paradoxically, no mention of psychological assessment is present in the tests to inform differential diagnosis. More psychological testing should be carried out in a neurotological context, as vertigo and dizziness can also cause anxiety, panic and depression, and these could in turn also cause dizziness [177].
Other important aspects to discuss are persistent postural perceptual dizziness (PPPD) and vestibular migraine. PPPD was recognized by the International Classification of Diseases (ICD-11) only in 2017 [178], and vestibular migraine has been described by the members of the Bárány Society only since 2012 [179]. Although migraine is cited relatively often as a diagnosis of exclusion in PCGD, especially in the traumatic and chronic cervicalgia subpopulations, there is no golden standard to «rule in» migraine and diagnosis is based on clinical presentation [180]. This result supports the importance of controlling for migraine and developing subgroup analysis for migraine as a confounding factor in future interventional studies, as prompted by the Bárány Society’s recent milestone article on ‘Cervical Dizziness’ [175]. Persistent postural perceptual dizziness is a common long-lasting cause of dizziness [178]. Paradoxically, it is not mentioned in the exclusion process of PCGD. Migraine and persistent postural perceptual dizziness are both exclusion diagnoses and can co-exist with other conditions. This situation adds to diagnosis uncertainty.
Early diagnosis and rehabilitation could optimize health outcomes for patients and add value to healthcare by reducing the social-economic burden of disease. One of the main issues with the lengthy care trajectory of PCGD is that despite being an exclusion diagnosis, it may also coexist with other disorders, and often does. Moreover, in elderly people at risk of falls, road accident victims suffering from post-concussion syndrome or whiplash, and patients suffering from neck pain or chronic headaches, 45.2% to 84% of patients have potentially one or more diagnoses in addition to PCGD [11,123,181]. In these subpopulations, dizziness is associated with higher levels of disability and more psychosocial consequences compared to patients in the same groups without dizziness [13,113,135,154,182]. This multi-morbid situation makes the trajectory of care longer, and often results in therapeutic wandering for these patients, and a greater social and economic burden. There is a lack of a single gold standard test or accepted clinical prediction rule to limit diagnosis uncertainty [18]. Only one article has studied the possibility of combining different tests to shorten the exclusion process [16]. The issue of multi-morbidity calls for investigation of clinical prediction rules and the specificity of tests to «rule-in» PCGD. Indeed, while sensitive tests such as manual spinal evaluation and palpation for segmental tenderness are very often used in the literature, potentially more specific tests [10] such as cervical torsion [10,16,64,84,90,97,115], the head–neck differentiation test [10,97,123], joint position error test [10,16,50,65,87,90,98] and smooth pursuit neck torsion test [10,16,23,26,50,57,64,65,99,103,125,128] have a relatively lower rate of occurrence in the literature. Unfortunately, in comparison with the literature reporting tools to «rule out» other pathologies, the literature reporting clinical testing that is useful to «rule in» PCGD with more specific tools is scarce, and therefore should be encouraged (see Figure 5 and Figure 6).
4.4. Measuring Change
In PCGD, many outcome measures are needed not only because of its multidimensional nature, but because self-reported outcomes and perceived level of handicap poorly correlate with the measurement of the level of sensorimotor performance [183]. This suggests they rely on other constructs [183]. The most commonly encountered outcome measures in PCGD are DHI, VAS for cervical pain, CROM and posturography (see Figure 8). Posturography and JPE are the only tests that can be found both among the tools for inclusion and for measuring change (see Figure 6 and Figure 8), and this raises the question of their potential combined specificity and sensitivity to change. These six tools should be used to facilitate comparison between trials and meta-analysis of outcomes, and a psychological outcome such as HADS should also be included. Social engagement and personal economic impacts of disease should be reported in PCGD. As PCGD remains elusive in its exact aetiopathogenesis, primary clinical outcomes and secondary «mechanistically based» outcomes should also help to establish a basis for hypothesized pathophysiological mechanisms [175].
4.5. Interventions
Manual therapy and exercise therapy are generally the most common interventions encountered in the literature. However, surgeries were considered more often for degenerative cervical disease subpopulations suffering from PCGD than in any other subpopulation (see Table 4). The reason for this might be that surgeries are aimed at degenerative changes and herniated disc issues rather than for dizziness itself, even if they may have an indirect impact on dizziness. In the same way, injections were mostly reported in the literature for the chronic cervical pain subpopulation, as they are a common treatment for chronic neck pain. Patient education was the third most studied intervention in the muscle spasm (occupational) subpopulation. Indeed, patient education about occupational habits aims to reducing muscle spasms, and indirectly could impact dizziness.
Knowledge of subpopulations’ characteristics should also be reflected in the multimorbid context of PCGD. It enables the clinician to consider not only the type of intervention but the strategy of intervention that might be considered.
4.6. Limitations
Relevant sources of information may have been omitted in the literature written in languages that were not included in the review, notably Chinese and German articles. Another limitation of this study is that the proprioceptive etiology of cervicogenic dizziness is yet to be recognized by The International Classification of Vestibular Disorders. It is a working definition and is the most plausible cause of dizziness in cervicogenic dizziness, but still requires further investigation into its pathophysiological mechanism. In this scoping review, as no quality assessment of protocols was performed, the validity of the literature has not been put to the test. Care should be taken while interpreting the results.
In the differential diagnosis process, since some authors simply excluded general cardiac, central and otologic conditions without naming any particular pathology, specific conditions pertaining to those categories might be under-represented in our results in Figure 4. Additionally, relatively recent diagnoses in otology and neurotology make some pathologies unlikely to have been put forward in the differential diagnosis of PCGD before 2010, and even today. For example, a potentially relevant competing diagnosis such as PPPD might have been reported using other terms such as phobic postural vertigo or visual vertigo, but only two articles mentioned each pathology.
Some 43.9% of articles acknowledge more than one subpopulation. This introduces bias in subpopulation analysis. Particularly in the chronic cervicalgia analysis, 34 of the 53 articles also recognize at least one other subpopulation for PCGD, and in so doing, introduce bias to our data. For example, these articles could mention vertebral fractures or instability as a pathology to exclude, because the authors recognize the potential contribution of trauma or degenerative cervical disease subpopulations in PCGD.
5. Conclusions
This is the first scoping review of the literature on PCGD, to the authors’ knowledge. Qualitative methods are inexistent in the literature on PCGD. The specific characteristics of PCGD patients differ according to their etiological categories. Subpopulation knowledge should inform subgroup analysis in PCGD trials and observational studies as well as clinical practice. Namely, there are four main subpopulations of PCGD: chronic cervical pain, traumatic, degenerative cervical disease and occupational. These subgroups have different care trajectories according to commonly encountered pathologies, probable comorbidities, usual red flags, and treatment strategies. This raised awareness will have important impact on future research in relation to subgroup analysis and in clinical practice, as it enables optimized differential diagnosis, treatment, and evaluation. Studies should also investigate the reason that some patients from a single subpopulation develop PCGD and others do not; more randomized control studies are needed. Trials should use common outcome measures encompassing all dimensions of PCGD, including the social and economic categories, to facilitate future systematic reviews and elucidate pathophysiological mechanisms. Future studies should report on clinical testing to «rule in» PCGD.
Supplementary Materials
The following supporting information can be downloaded at: https://0-www-mdpi-com.brum.beds.ac.uk/article/10.3390/jcm12051884/s1, Appendix SA: Search strategy. Supplementary Appendix SB: Data extraction instrument. Supplementary Appendix SC: Sources excluded following full-text review.
Author Contributions
Conceptualization, J.G.-L., D.B. and, I.S.; Methodology, J.G.-L. and, D.B.; Validation, J.G.-L., D.B. and, I.S.; Formal analysis, J.G.-L. and, D.B.; Data curation, J.G.-L.; Writing—original draft, J.G.-L.; Writing—review & editing, D.B. and, I.S.; Supervision, D.B. and, I.S.; Project administration, D.B All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data is contained within the article and in the Supplementary Materials.
Acknowledgments
The authors would like to extend their gratitude to Myrian Grondin, the university’s librarian, for help with setting up this review. The authors would also like to thank Marie Phaneuf Thibault, Kariane Grilli-Cadieux, Pier-Étienne Daigle, Antony Trujilo, Catherine Peleaz-Bouchard, Anne-Sophie Chagnon and Tanya Froedrich and Helga Tonkov for their work on reading, revising and selecting articles.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Yacovino, D.A.; Hain, T.C. Clinical characteristics of cervicogenic-related dizziness and vertigo. Semin. Neurol. 2013, 33, 244–255. [Google Scholar] [PubMed] [Green Version]
- Yardley, L.; Owen, N.; Nazareth, I.; Luxon, L. Prevalence and presentation of dizziness in a general practice community sample of working age people. Br. J. Gen. Pr. 1998, 48, 1131–1135. [Google Scholar]
- Liu, T.-H.; Liu, Y.-Q.; Peng, B.-G. Cervical intervertebral disc degeneration and dizziness. World J. Clin. Cases 2021, 9, 2146–2152. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Peng, B. Pathogenesis, Diagnosis, and Treatment of Cervical Vertigo. Pain Phys. 2015, 18, E583–E595. [Google Scholar]
- Furman, J.M.; Raz, Y.; Whitney, S.L. Geriatric vestibulopathy assessment and management. Curr. Opin. Otolaryngol. Head Neck Surg. 2010, 18, 386–391. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, S. Importance of cervicogenic general dizziness. J. Rural Med. 2018, 13, 48–56. [Google Scholar] [CrossRef] [Green Version]
- Sung, Y.-H. Upper cervical spine dysfunction and dizziness. J. Exerc. Rehabil. 2020, 16, 385–391. [Google Scholar] [CrossRef]
- Grill, E.; Akdal, G.; Becker-Bense, S.; Hubinger, S.; Huppert, D.; Kentala, E.; Strobl, R.; Zwergal, A.; Celebisoy, N. Multicenter data banking in management of dizzy patients: First results from the DizzyNet registry project. J. Neurol. 2018, 265, 3–8. [Google Scholar] [CrossRef]
- Wrisley, D.M.; Sparto, P.J.; Whitney, S.L.; Furman, J.M. Cervicogenic dizziness: A review of diagnosis and treatment. J. Orthop. Sport. Phys. Ther. 2000, 30, 755–766. [Google Scholar] [CrossRef] [Green Version]
- Reiley, A.S.; Vickory, F.M.; Funderburg, S.E.; Cesario, R.A.; Clendaniel, R.A. How to diagnose cervicogenic dizziness. Arch. Physiother. 2017, 7, 12. [Google Scholar] [CrossRef] [Green Version]
- Devaraja, K. Approach to cervicogenic dizziness: A comprehensive review of its aetiopathology and management. Eur. Arch. Oto-Rhino-Laryngol. 2018, 275, 2421–2433. [Google Scholar] [CrossRef] [PubMed]
- Defossez, G.; Rollet, A.; Dameron, O.; Ingrand, P. Temporal representation of care trajectories of cancer patients using data from a regional information system: An application in breast cancer. BMC Med. Inform. Decis. Mak. 2014, 14, 24. [Google Scholar] [CrossRef] [PubMed]
- Treleaven, J.; Jull, G.; Sterling, M. Dizziness and unsteadiness following whiplash injury: Characteristic features and relationship with cervical joint position error. J. Rehabil. Med. 2003, 35, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Grande-Alonso, M.; Moral Saiz, B.; Minguez Zuazo, A.; Lerma Lara, S.; La Touche, R. Biobehavioural analysis of the vestibular system and posture control in patients with cervicogenic dizziness. A cross-sectional study. Neurologia 2018, 33, 98–106. [Google Scholar] [CrossRef]
- Ghosh, S.; Dey, S.; Guha, R. Cervical spondylosis and vertigo: A controversy put to test. Indian J. Otol. 2009, 15, 7–11. [Google Scholar]
- L’Heureux-Lebeau, B.; Godbout, A.; Berbiche, D.; Saliba, I. Evaluation of paraclinical tests in the diagnosis of cervicogenic dizziness. Otol Neurotol. 2014, 35, 1858–1865. [Google Scholar] [CrossRef]
- Grgić, V. Cervicogenic proprioceptive vertigo: Etiopathogenesis, clinical manifestations, diagnosis and therapy with special emphasis on manual therapy. Lijec Vjesn 2006, 128, 288–295. [Google Scholar]
- Knapstad, M.K.; Nordahl, S.H.G.; Goplen, F.K. Clinical characteristics in patients with cervicogenic dizziness: A systematic review. Health Sci. Rep. 2019, 2, e134. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Godfrey, C.; McInerney, P.; Munn, Z.; Tricco, A.C.; Khalil, H. Chapter 11: Scoping Reviews (2020 version). In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Miami, FL, USA, 2020. [Google Scholar]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, T.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Reid, S.A.; Rivett, D.A.; Katekar, M.G.; Callister, R. Comparison of mulligan sustained natural apophyseal glides and maitland mobilizations for treatment of cervicogenic dizziness: A randomized controlled trial. Phys. Ther. 2014, 94, 466–476. [Google Scholar] [CrossRef] [Green Version]
- Reid, S.A.; Rivett, D.A.; Katekar, M.G.; Callister, R. Efficacy of manual therapy treatments for people with cervicogenic dizziness and pain: Protocol of a randomised controlled trial. BMC Musculoskelet. Disord. 2012, 13, 201. [Google Scholar] [CrossRef] [Green Version]
- Reid, S.A.; Rivett, D.A.; Katekar, M.G.; Callister, R. Sustained natural apophyseal glides (SNAGs) are an effective treatment for cervicogenic dizziness. Man. Ther. 2008, 13, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Reid, S.A.; Callister, R.; Snodgrass, S.J.; Katekar, M.G.; Rivett, D.A. Manual therapy for cervicogenic dizziness: Long-term outcomes of a randomised trial. Man. Ther. 2015, 20, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Reid, S.A.; Callister, R.; Katekar, M.G.; Rivett, D.A. Effects of cervical spine manual therapy on range of motion, head repositioning, and balance in participants with cervicogenic dizziness: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2014, 95, 1603–1612. [Google Scholar] [CrossRef] [PubMed]
- Moustafa, I.M.; Diab, A.A.; Harrison, D.E. The effect of normalizing the sagittal cervical configuration on dizziness, neck pain, and cervicocephalic kinesthetic sensibility: A 1-year randomized controlled study. Eur. J. Phys. Rehabil. Med. 2017, 53, 57–71. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, A.A.; Shendy, W.S.; Semary, M.; Mourad, H.S.; Battecha, K.H.; Soliman, E.S.; El Sayed, S.H.; Mohamed, G.I. Combined use of cervical headache snag and cervical snag half rotation techniques in the treatment of cervicogenic headache. J. Phys. Ther. Sci. 2019, 31, 376–381. [Google Scholar] [CrossRef] [Green Version]
- Micarelli, A.; Viziano, A.; Granito, I.; Carlino, P.; Micarelli, R.X.; Augimeri, I.; Alessandrini, M. Postural and clinical outcomes of sustained natural apophyseal glides treatment in cervicogenic dizziness patients: A randomised controlled trial. Clin. Rehabil. 2021, 35, 1566–1576. [Google Scholar] [CrossRef]
- Kendall, J.C.; French, S.D.; Hartvigsen, J.; Azari, M.F. Chiropractic treatment including instrument-assisted manipulation for non-specific dizziness and neck pain in community-dwelling older people: A feasibility randomised sham-controlled trial. Chiropr. Man. Ther. 2018, 26, 14. [Google Scholar] [CrossRef] [Green Version]
- Jaroshevskyi, O.A.; Payenok, O.S.; Logvinenko, A.V. Evalution of the effectiveness of multimodal approach to the management of cervical vertigo. Wiad. Lekarskie 2017, 70 3 Pt 2, 571–573. [Google Scholar]
- Dorn, L.J.; Lappat, A.; Neuhuber, W.; Scherer, H.; Olze, H.; Holzl, M. Tonic Investigation Concept of Cervico-vestibular Muscle Afferents. Int. Arch. Otorhinolaryngol. 2017, 21, 46–57. [Google Scholar]
- Carrasco-Uribarren, A.; Rodriguez-Sanz, J.; Lopez-de-Celis, C.; Perez-Guillen, S.; Tricas-Moreno, J.M.; Cabanillas-Barea, S. Short-term effects of the traction-manipulation protocol in dizziness intensity and disability in cervicogenic dizziness: A randomized controlled trial. Disabil. Rehabil. 2021, 44, 3601–3609. [Google Scholar] [CrossRef] [PubMed]
- Aydin, T.; Dernek, B.; Ege, T.S.; Karan, A.; Aksoy, C. The effectiveness of dry needling and exercise therapy in patients with dizziness caused by cervical myofascial pain syndrome: Prospective randomized clinical study. Pain Med. 2019, 20, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Yao, M.; Tang, Z.-Y.; Cui, X.-J.; Sun, Y.-L.; Ye, X.-L.; Wang, P.; Zhong, W.-H.; Zhang, R.-C.; Li, H.-Y.; Hu, Z.-J.; et al. Shi-Style Cervical Mobilizations Versus Massage for Cervical Vertigo: A Multicenter, Randomized, Controlled Clinical Trial. J. Altern. Complement. Med. 2020, 26, 58–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, Q.; Duan, X.; Shi, Y.; Lv, X.; Wang, Y.; Tao, Y.; Zhong, L.; Sun, J.; Lei, H.; Yin, W.; et al. Microneedle interventional therapy combined with cervical spine manipulation for cervicogenic dizziness. Int. J. Clin. Exp. Med. 2018, 11, 3704–3716. [Google Scholar]
- Treleaven, J.; Peterson, G.; Ludvigsson, M.L.; Kammerlind, A.-S.; Peolsson, A. Balance, dizziness and proprioception in patients with chronic whiplash associated disorders complaining of dizziness: A prospective randomized study comparing three exercise programs. Man. Ther. 2016, 22, 122–130. [Google Scholar] [CrossRef] [Green Version]
- Reneker, J.C.; Hassen, A.; Phillips, R.S.; Moughiman, M.C.; Donaldson, M.; Moughiman, J. Feasibility of early physical therapy for dizziness after a sports-related concussion: A randomized clinical trial. Scand. J. Med. Sci. Sport. 2017, 27, 2009–2018. [Google Scholar] [CrossRef]
- Nacci, A.; Bruschini, L.; Dallan, I.; Fattori, B.; Ursino, F.; Cingolani, C. Acupuncture treatment of whiplash injury. Int. Tinnitus J. 2004, 10, 156–160. [Google Scholar]
- Malmstrom, E.-M.; Karlberg, M.; Melander, A.; Magnusson, M.; Moritz, U. Cervicogenic dizziness - musculoskeletal findings before and after treatment and long-term outcome. Disabil. Rehabil. 2007, 29, 1193–1205. [Google Scholar] [CrossRef]
- Heikkila, H.; Johansson, M.; Wenngren, B.I. Effects of acupuncture, cervical manipulation and NSAID therapy on dizziness and impaired head repositioning of suspected cervical origin: A pilot study. Man. Ther. 2000, 5, 151–157. [Google Scholar] [CrossRef]
- Ernst, A.; Basta, D.; Seidl, R.O.; Todt, I.; Scherer, H.; Clarke, A. Management of posttraumatic vertigo. Otolaryngol. Head Neck Surg. 2005, 132, 554–558. [Google Scholar] [CrossRef]
- Eva-Maj, M.; Hans, W.; Per-Anders, F.; Mikael, K.; Mans, M. Experimentally induced deep cervical muscle pain distorts head on trunk orientation. Eur. J. Appl. Physiol. 2013, 113, 2487–2499. [Google Scholar] [CrossRef] [PubMed]
- Johnston, J.L.; Daye, P.M.; Thomson, G.T.D. Inaccurate Saccades and Enhanced Vestibulo-Ocular Reflex Suppression during Combined Eye-Head Movements in Patients with Chronic Neck Pain: Possible Implications for Cervical Vertigo. Front. Neurol. 2017, 8, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, W.; Tan, L.; Wang, S.-Q. Sixty-five cases of cervical vertigo treated by needling Jngjiaj points in combination with acupressure. World J. Acupunct.-Moxibustion 2013, 23, 49–52. [Google Scholar] [CrossRef]
- Lin, Y.-C.; Lai, C.-H.; Chang, W.-H.; Tu, L.-W.; Lin, J.-C.; Chou, S.-W. Immediate effects of ischemic compression on neck function in patients with cervicogenic cephalic syndrome. J. Manip. Physiol. Ther. 2012, 35, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Malmstrom, E.M.; Fransson, P.A.; Bruinen, T.J.; Facic, S.; Tjernstrom, F. Disturbed cervical proprioception affects perception of spatial orientation while in motion. Exp. Brain Res. 2017, 235, 2755–2766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schieppati, M. Fatigue of neck muscles impairs postural control. Funct. Neurol. 2003, 18, 106. [Google Scholar]
- Schikora, N.; Klunter, H.; Delank, S.; Eysel-Gosepath, K. Influence of cervical spine stabilization via Stiff Neck on the postural system in healthy patients: Compensation or decompensation of the postural system? Eur. Arch. Otorhinolaryngol. 2010, 267, 1623–1628. [Google Scholar] [CrossRef] [PubMed]
- Slangen, R.; Kingma, H.; Patijn, J. Cervical dizziness: The Hautant procedure in normal and whiplash-associated-disorder subjects. Int. Musculoskelet. Med. 2011, 33, 54–60. [Google Scholar] [CrossRef]
- Unlu, Z.; Cerrahoglu, L.; Aslan, A.; Tarhan, S. Efficacy of collar treatment for patients with cervical spondylatrosis complaining of vertigo. J. Phys. Ther. Sci. 2001, 13, 115–120. [Google Scholar] [CrossRef] [Green Version]
- Zheng, S.; Muheremu, A.; Sun, Y.; Tian, W.; Wu, C.-A. Preoperative imaging differences of patients with cervical spondylosis with cervical vertigo indicate the prognosis after cervical total disc replacement. J. Int. Med. Res. 2020, 48, 300060519877033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morinaka, S.; Nakamura, H. Middle ear pressure in patients with dizziness. Ann. Otol. Rhinol. Laryngol. 2004, 113, 906–913. [Google Scholar] [CrossRef]
- Michels, T.; Lehmann, N.; Moebus, S. Cervical vertigo–cervical pain: An alternative and efficient treatment. J. Altern. Complement. Med. 2007, 13, 513–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, S.; Jungade, S.; Ranjan, A.; Singh, P.; Panicker, A.; Singh, C.; Bhalerao, P. Revisiting “Meniere’s Disease” as “Cervicogenic Endolymphatic Hydrops” and Other Vestibular and Cervicogenic Vertigo as “Spectrum of Same Disease”: A Novel Concept. Indian, J. Otolaryngol. Head Neck Surg. 2021, 73, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Olusesi, A.D.; Abubakar, J. 10 years of Vertigo Clinic at National Hospital Abuja, Nigeria: What have we learned? Eur. Arch. Otorhinolaryngol. 2016, 273, 3567–3572. [Google Scholar] [CrossRef]
- Somefun, O.A.; Giwa, O.S.; Bamgboye, B.A.; Okeke-Igbokwe, I.I.; Azeez, A.A.A. Vestibular disorders among adults in a tertiary hospital in Lagos, Nigeria. Eur. Arch. Otorhinolaryngol. 2010, 267, 1515–1521. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Qi, Y.; Liu, G.; Yin, X.; Jin, Y.; Jiang, Z.; Li, P.; Kang, X.; Ye, C. Long-Term Clinical Outcomes of Percutaneous Cervical Nucleoplasty for Cervical Degenerative Diseases with Neck Pain and Cervical Vertigo. World Neurosurg. 2020, 133, e205–e210. [Google Scholar] [CrossRef]
- do Prado, G.F.; Teixeira, L.J. Impact of physical therapy in vertigo treatment. Rev. Neurocienc. 2009, 17, 112–118. [Google Scholar]
- Krabak, B.J.; Borg-Stein, J.; Oas, J.A. Chronic cervical myofascial pain syndrome: Improvement in dizziness and pain with a multidisciplinary rehabilitation program. A pilot study. J. Back Musculoskelet. Rehabil. 2000, 15, 83–87. [Google Scholar] [CrossRef]
- Baron, E.P.; Cherian, N.; Tepper, S.J. Role of greater occipital nerve blocks and trigger point injections for patients with dizziness and headache. Neurology 2011, 17, 312–317. [Google Scholar] [CrossRef]
- Durà, M.J.; Larrosa, F.; Cordón, A.; Hernández, A.; García-Ibáñez, L. Results of balance control and vestibular function tests in 51 patients with whiplash injury complaining of dizziness and imbalance. Rehabilitacion 2012, 46, 215–221. [Google Scholar] [CrossRef]
- Elster, E. Sixty patients with chronic vertigo undergoing upper cervical chiropractic care to correct vertebral subluxation: A retrospective analysis. J. Vertebr. Subluxation Res. 2006, 1–9. [Google Scholar]
- Hahn, T.; Halatsch, M.-E.; Wirtz, C.; Klessinger, S. Response to Cervical Medial Branch Blocks in Patients with Cervicogenic Vertigo. Pain Physician 2018, 21, 285–294. [Google Scholar] [PubMed]
- Hammerle, M.; Swan, A.A.; Nelson, J.T.; Treleaven, J.M. Retrospective Review: Effectiveness of Cervical Proprioception Retraining for Dizziness After Mild Traumatic Brain Injury in a Military Population with Abnormal Cervical Proprioception. J. Manip. Physiol. Ther. 2019, 42, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Hansson, E.E.; Mansson, N.O.; Hakansson, A. Balance performance and self-perceived handicap among dizzy patients in primary health care. Scand. J. Prim. Health Care 2005, 23, 215–220. [Google Scholar] [CrossRef]
- Isaradisaikul, S.; Navacharoen, N.; Hanprasertpong, C.; Kangsanarak, J.; Panyathong, R. Causes and time-course of vertigo in an ear, nose, and throat clinic. Eur. Arch. Otorhinolaryngol. 2010, 267, 1837–1841. [Google Scholar] [CrossRef]
- Li, S.; Chen, R.; Chen, Y.; Mo, G.; Zhang, L.; Xie, P.; Wang, Q.; Liu, B.; Dong, J.; Rong, L. Therapeutic Effects and Safety of Percutaneous Disc Decompression with Coblation Nucleoplasty in Cervical Vertigo: A Retrospective Outcome Study with 74 Consecutive Patients and Minimum 1-Year Follow-Up. Pain Physician 2019, 22, E205–E214. [Google Scholar]
- Nwaorgu, O.G.; Onakaoya, P.A.; Usman, M.A. Cervical vertigo and cervical spondylosis--a need for adequate evaluation. Niger. J. Med. J. Natl. Assoc. Resid. Dr. Niger. 2003, 12, 140–144. [Google Scholar]
- Polaczkiewicz, L.A.; Olszewski, J. An analysis of causes and results of VNG examinations in patients with vertigo and balance disorders in private ENT practice. Pol. J. Otolaryngol. 2020, 74, 23–30. [Google Scholar]
- Ren, L.; Guo, B.; Zhang, J.; Han, Z.; Zhang, T.; Bai, Q.; Zeng, Y. Mid-term efficacy of percutaneous laser disc decompression for treatment of cervical vertigo. Eur. J. Orthop. Surg. Traumatol. Orthop. Traumatol. 2014, 24 (Suppl. 1), S153–S158. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.R.; Fang, M.; Hu, J.; Shen, G.Q.; Jiang, S.Y. Action of tuina on retro-positioning of skull spatial offset in patients with cervical vertigo. J. Acupunct. Tuina Sci. 2008, 6, 83–86. [Google Scholar] [CrossRef]
- Bittar, R.; Alves, N.G.P.; Bertoldo, C.; Brugnera, C.; Oiticica, J. Efficacy of Carbon Microcoils in Relieving Cervicogenic Dizziness. Int. Arch. Otorhinolaryngol. 2017, 21, 4–7. [Google Scholar] [CrossRef] [Green Version]
- Bracher, E.S.; Almeida, C.I.; Almeida, R.R.; Duprat, A.C.; Bracher, C.B. A combined approach for the treatment of cervical vertigo. J. Manip. Physiol. Ther. 2000, 23, 96–100. [Google Scholar] [CrossRef]
- Brandt, T.; Huppert, D. A new type of cervical vertigo: Head motion-induced spells in acute neck pain. Neurology 2016, 86, 974–975. [Google Scholar] [CrossRef] [PubMed]
- Chu, E.C.P.; Lo, F.S.; Bhaumik, A. Short-term effects of an upper cervical spine traction-manipulation program in patients with cervicogenic dizziness: A case series study. J. Back Musculoskelet. Rehabil. 2020, 33, 961–967. [Google Scholar]
- Chaibi, A.; Tuchin, P.J. Chiropractic spinal manipulative treatment of cervicogenic dizziness using Gonstead method: A case study. J. Chiropr. Med. 2011, 10, 194–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, E.C.P.; Chin, W.L.; Bhaumik, A. Cervicogenic dizziness. Oxf. Med. Case Rep. 2019, 2019, 476–478. [Google Scholar] [CrossRef] [Green Version]
- Chu, E.C.P.; Lo, F.S.; Bhaumik, A. Plausible impact of forward head posture on upper cervical spine stability. J. Fam. Med. Prim. Care 2020, 9, 2517–2520. [Google Scholar] [CrossRef]
- Xue-ying, Z.; Gui-zhen, Y. Treatment of 40 cases of cervical vertigo by acupuncture. J. Acupunct. Tuina Sci. 2003, 1, 41–42. [Google Scholar] [CrossRef]
- Gerstin, G.; Oakley, P.A.; Harrison, D.E. The treatment of dizziness by improving cervical lordosis: A Chiropractic BioPhysics R case report. J. Phys. Ther. Sci. 2020, 32, 864–868. [Google Scholar] [CrossRef]
- Heidenreich, K.D.; Beaudoin, K.; White, J.A. Cervicogenic dizziness as a cause of vertigo while swimming: An unusual case report. Am. J. Otolaryngol. 2008, 29, 429–431. [Google Scholar] [CrossRef] [PubMed]
- Jung, F.C.; Mathew, S.; Littmann, A.E.; MacDonald, C.W. Clinical Decision Making in the Management of Patients with Cervicogenic Dizziness: A Case Series. J. Orthop. Sport. Phys. Ther. 2017, 47, 874–884. [Google Scholar] [CrossRef] [PubMed]
- Kondratek, M.; Creighton, D.; Krauss, J. Use of translatoric mobilization in a patient with cervicogenic dizziness and motion restriction: A case report. J. Man. Manip. Ther. 2006, 14, 140–151. [Google Scholar] [CrossRef]
- Minguez-Zuazo, A.; Grande-Alonso, M.; Saiz, B.M.; La Touche, R.; Lara, S.L. Therapeutic patient education and exercise therapy in patients with cervicogenic dizziness: A prospective case series clinical study. J. Exerc. Rehabil. 2016, 12, 216–225. [Google Scholar] [CrossRef] [PubMed]
- Odderson, I. A new treatment for cervical vertigo with botulinum toxin. Mov. Disord. Clin. Pract. 2020, 7 (Suppl. 1), S31. [Google Scholar] [CrossRef]
- Saviola, K.; Coleman, T.; Ross, M.; Schenk, R. Cervicogenic Dizziness Post-concussion: A Case Report. Orthop. Phys. Ther. Pract. 2016, 28, 238–243. [Google Scholar]
- Serra, F.A.; Grillo, C.; Abela, S.; Maiolino, L.; Grillo, C. Cervical whiplash: Vestibular–Spinal implications. Acta Med. Mediterr. 2007, 23, 31–33. [Google Scholar]
- Strunk, R.G.; Hawk, C. Effects of chiropractic care on dizziness, neck pain, and balance: A single-group, preexperimental, feasibility study. J. Chiropr. Med. 2009, 8, 156–164. [Google Scholar] [CrossRef] [Green Version]
- Treleaven, J. Sensorimotor disturbances in neck disorders affecting postural stability, head and eye movement control–Part 2: Case studies. Man. Ther. 2008, 13, 266–275. [Google Scholar] [CrossRef]
- Vuillerme, N.L.; Pinsault, N. Experimental neck muscle pain impairs standing balance in humans. Exp. Brain Res. 2009, 192, 723–729. [Google Scholar] [CrossRef] [Green Version]
- Zhu, X.; Grover, M.J. Cervicogenic Dizziness Successfully Treated with Upper Cervical Medial Branch Nerve Radiofrequency Ablation: A Case Report. A A Pract. 2018, 10, 150–153. [Google Scholar] [CrossRef] [Green Version]
- Zamyslowska-Szmytke, E.; Adamczewski, T.; Ziaber, J.; Majak, J.; Kujawa, J.; Sliwinska-Kowalska, M. Cervico-ocular reflex upregulation in dizzy patients with asymmetric neck pathology. Int. J. Occup. Med. Environ. Health 2019, 32, 723–733. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Wang, X.; Zhang, G.; Guo, Z.; Wang, Y.; Wang, R.; Xiang, H.; Chen, B. Histologic Observation and Significance of Sympathetic Nerve Fiber Distribution on Human Cervical Ligamentum Flavum. Orthop. Surg. 2020, 12, 1811–1825. [Google Scholar] [CrossRef] [PubMed]
- Viziano, A.; Micarelli, A.; Carlino, P.; Granito, I.; Alessandrini, M. Bridging the gap between temporomandibular disorders, static balance impairment and cervicogenic dizziness: Posturographic and clinical outcomes. J. Electromyogr. Kinesiol. Off. J. Int. Soc. Electrophysiol. Kinesiol. 2020, 54, 102455. [Google Scholar] [CrossRef]
- Ullucci, P.A.; Kalach, A.; Reis, B.; Avena, S.; Hinckley, R.; Picard, K.; Gibson, S. Seated cervical flexion-rotation test equivalent to supine for identifying cervical dysfunction in patients with dizziness/vertigo. Physiother. Pract. Res. 2020, 41, 171–176. [Google Scholar] [CrossRef]
- Treleaven, J.; Joloud, V.; Nevo, Y.; Radcliffe, C.; Ryder, M. Normative Responses to Clinical Tests for Cervicogenic Dizziness: Clinical Cervical Torsion Test and Head-Neck Differentiation Test. Phys. Ther. 2020, 100, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Thompson-Harvey, A.; Hain, T.C. Symptoms in cervical vertigo. Laryngoscope Investig. Otolaryngol. 2019, 4, 109–115. [Google Scholar] [CrossRef] [Green Version]
- Tenenbaum, A.; Sandstrom, S.; Tjell, C. Smooth pursuit neck torsion test–A specific test for whiplash associated disorders? J. Whiplash Relat. Disord. 2002, 1, 9–24. [Google Scholar]
- Talebi, R.Z.; Rezasoltani, A.; Khalkhalizavieh, M.; Manshadi, F.D.; Baghban, A.A. Evaluation of cervical spine muscles thickness in patients with cervical vertigo and healthy controls through ultrasonography. J. Phys. Ther. Sci. 2020, 32, 439–443. [Google Scholar] [CrossRef]
- Simoceli, L.; Saraiva Bittar, R.M.; Bottino, M.A.; Ferreira Bento, R. Diagnostic approach of balance in the elderly: Preliminary results. Rev. Bras. De Otorrinolaringol. 2003, 69, 772–777. [Google Scholar] [CrossRef] [Green Version]
- Santos Perez, S.; Vaamonde Lago, P.; Labella Caballero, T.; Soto Varela, A. The usefulness of craniocorpography in diagnosing patients with dizziness and increasing muscle tension in the neck. Acta Otorrinolaringol. Esp. 2001, 52, 398–403. [Google Scholar]
- Reneker, J.C.; Cheruvu, V.K.; Yang, J.; James, M.A.; Cook, C.E. Physical examination of dizziness in athletes after a concussion: A descriptive study. Musculoskelet. Sci. Pract. 2018, 34, 8–13. [Google Scholar] [CrossRef]
- Reid, S.A.; Callister, R.; Katekar, M.G.; Treleaven, J.M. Utility of a brief assessment tool developed from the Dizziness Handicap Inventory to screen for Cervicogenic dizziness: A case control study. Musculoskelet. Sci. Pract. 2017, 30, 42–48. [Google Scholar] [CrossRef] [Green Version]
- Pippal, S.K.; Soni, S.; Sharma, P.; Asif, S.K. A study of incidence of vertigo, its clinico pathological profile and etiology. Indian, J. Otol. 2009, 15, 7–14. [Google Scholar]
- Peolsson, A.; Kammerlind, A.S.; Ledin, T. Dynamic posturography in patients with cervical disc disease compared with patients with whiplash-associated disorders and healthy volunteers. Adv. Physiother. 2004, 6, 173–181. [Google Scholar] [CrossRef]
- Micarelli, A.; Viziano, A.; Micarelli, B.; Giulia, D.F.; Alessandrini, M. Usefulness of postural sway spectral analysis in the diagnostic route and clinical integration of cervicogenic and vestibular sources of dizziness: A cross-sectional preliminary study. J. Vestib. Res Equilib. Orientat. 2021, 31, 353–364. [Google Scholar]
- Micarelli, A.; Viziano, A.; Granito, I.; Micarelli, R.X.; Augimeri, I.; Alessandrini, M. Temporomandibular disorders and cervicogenic dizziness: Relations between cervical range of motion and clinical parameters. Cranio, J. Craniomandib. Pract. 2022, 40, 348–357. [Google Scholar] [CrossRef] [PubMed]
- Micarelli, A.; Viziano, A.; Carlino, P.; Granito, I.; Micarelli, R.X.; Alessandrini, M. Reciprocal roles of joint position error, visual dependency and subjective perception in cervicogenic dizziness. Somatosens. Mot. Res. 2020, 37, 262–270. [Google Scholar] [PubMed]
- Micarelli, A.; Viziano, A.; Augimeri, I.; Micarelli, B.; Capoccia, D.; Alessandrini, M. Diagnostic route of cervicogenic dizziness: Usefullness of posturography, objective and subjective testing implementation and their correlation. Disabil. Rehabil. 2021, 43, 1730–1737. [Google Scholar] [CrossRef]
- Meldrum, D.; Burrows, L.; Cakrt, O.; Kerkeni, H.; Lopez, C.; Tjernstrom, F.; Vereeck, L.; Zur, O.; Jahn, K. Vestibular rehabilitation in Europe: A survey of clinical and research practice. J. Neurol. 2020, 267 (Suppl. 1), 24–35. [Google Scholar] [CrossRef]
- Lopez-Escamez, J.A.; Lopez-Nevot, A.; Gamiz, M.J.; Moreno, P.M.; Bracero, F.; Castillo, J.L.; Salinero, J. Diagnosis of common causes of vertigo using a structured clinical history. Acta Otorrinolaringol. Esp. 2000, 51, 25–30. [Google Scholar] [PubMed]
- Leaver, A.M.; Maher, C.G.; McAuley, J.H.; Jull, G.A.; Refshauge, K.M. Characteristics of a new episode of neck pain. Man. Ther. 2013, 18, 254–257. [Google Scholar] [CrossRef] [PubMed]
- Kotait, M.A.; Younes, R.L. Ocular vestibular evoked myogenic potentials (o-VEMPs) testing in cervicogenic vertigo and its relation to radiological findings: A correlation study. Hear. Balance Commun. 2017, 15, 235–243. [Google Scholar] [CrossRef]
- Kadanka, Z.; Jura, R.; Bednarik, J. Vertigo in patients with degenerative cervical myelopathy. J. Clin. Med. 2021, 10, 2496. [Google Scholar] [CrossRef] [PubMed]
- Humphreys, B.K.; Peterson, C.; Bolton, J.; Wood, A. A cross-sectional study of the association between pain and disability in neck pain patients with dizziness of suspected cervical origin. J. Whiplash Relat. Disord. 2002, 1, 63–73. [Google Scholar]
- Hermansen, A.; Peolsson, A.; Hedlund, R.; Kammerlind, A.-S. Balance problems and dizziness after neck surgery–associations with pain and health-related quality of life. Physiother. Theory Pract. 2020, 36, 1145–1152. [Google Scholar] [CrossRef] [Green Version]
- Ferrer-Pena, R.; Vicente-de-Frutos, G.; Flandez-Santos, D.; Martin-Gomez, C.; Roncero-Jorge, C.; Calvo-Lobo, C. Patient-reported outcomes measured with and without dizziness associated with non-specific chronic neck pain: Implications for primary care. PEERJ 2019, 7, e7449. [Google Scholar] [CrossRef]
- Endo, K.; Suzuki, H.; Yamamoto, K. Consciously postural sway and cervical vertigo after whiplash injury. Spine 2008, 33, E539–E542. [Google Scholar] [CrossRef]
- Cuenca-Martinez, F.; Bartrina-Rodriguez, I.; Suso-Marti, L.; La Touche, R.; Ferrer-Pena, R. Association between somatosensory, motor and psychological variables by levels of disability in patients with cervicogenic dizziness. Somatosens. Mot. Res. 2018, 35, 247–252. [Google Scholar] [CrossRef]
- Chen, H.; Shi, Z.; Feng, H.; Wang, R.; Zhang, Y.; Xie, J.; Yao, S.; Zhou, H. The relationship between dizziness and cervical artery stenosis. NeuroRep. Rapid Commun. Neurosci. Res. 2015, 26, 1112–1118. [Google Scholar] [CrossRef]
- Budhiraja, G.; Guram, D.; Singh, H. Incidence of cervical spondylosis as cause of vertigo in a tertiary care hospital in malwa region of Punjab. Indian, J. Public Health Res. Dev. 2020, 11, 112–114. [Google Scholar]
- Abdul-Baqi, K.J.; Mohammed, F.I.; Shubair, K.S.; Sarhan, Y.S.; Tawalbeh, M.I. Evaluation of dizziness at Jordan University Hospital. Saudi Med. J. 2004, 25, 625–631. [Google Scholar] [PubMed]
- Chang, S.-Y.; Zhang, W.-Q.; Chen, Y.; Li, S.-S.; Zhang, G.-Q.; Li, J.-M. Correlation between cervical curvature abnormality and symptoms of adolescent headache. Chin. J. Clin. Rehabil. 2004, 8, 7286–7289. [Google Scholar]
- Dispenza, F.; De Stefano, A.; Mathur, N.; Croce, A.; Gallina, S. Benign paroxysmal positional vertigo following whiplash injury: A myth or a reality? Am. J. Otolaryngol. 2011, 32, 376–380. [Google Scholar] [CrossRef] [Green Version]
- He, L.-L.; Lai, R.-J.; Leff, J.; Yuan, R.; Yue, J.-N.; Ni, J.-X.; Yang, L.-Q. Cervicogenic dizziness alleviation after coblation discoplasty: A retrospective study. Ann. Med. 2021, 53, 639–646. [Google Scholar] [CrossRef]
- Li, H.; Ma, X.; Wu, X.; Liu, F.; Yu, T.; Yue, B.; Xiang, H.; Chen, B. Morphological observation of sympathetic nerve fibers in the human posterior longitudinal ligament. Spine 2014, 39, 2119–2126. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.-M.; Pan, F.-M.; Yong, Z.-Y.; Ba, Z.-Y.; Wang, S.-J.; Liu, Z.; Zhao, W.-D.; Wu, D.-S. Does the longus colli have an effect on cervical vertigo? A retrospective study of 116 patients. Medicine 2017, 96, e6365. [Google Scholar] [CrossRef] [PubMed]
- Morinaka, S. Musculoskeletal diseases as a causal factor of cervical vertigo. Auris Nasus Larynx 2009, 36, 649–654. [Google Scholar] [CrossRef]
- Soylemez, E.; Ertugrul, S. Clinical Characteristics of Patients with Dizziness According to the Level of Dizziness-related Disability. Electron. J. Gen. Med. 2021, 18, 1–6. [Google Scholar] [CrossRef]
- Yang, L.; Yang, C.; Pang, X.; Li, D.; Yang, H.; Zhang, X.; Yang, Y.; Peng, B. Mechanoreceptors in Diseased Cervical Intervertebral Disc and Vertigo. Spine 2017, 42, 540–546. [Google Scholar] [CrossRef]
- Yi, Y.-Y.; Xu, H.-W.; Zhang, S.-B.; Hu, T.; Wang, S.-J.; Wu, D.-S. Does the C3/4 disc play a role in cervical spondylosis with dizziness? A retrospective study. Int. Orthop. 2020, 44, 1159–1168. [Google Scholar] [CrossRef]
- Bronfort, G.; Haas, M.; Evans, R.; Leininger, B.; Triano, J. Effectiveness of manual therapies: The UK evidence report. Chiropr. Osteopat. 2010, 18, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hawk, C.; Khorsan, R.; Lisi, A.J.; Ferrance, R.J.; Evans, M.W. Chiropractic care for nonmusculoskeletal conditions: A systematic review with implications for whole systems research. J. Altern. Complement. Med. 2007, 13, 491–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kendall, J.C.; Hartvigsen, J.; Azari, M.F.; French, S.D. Effects of Nonpharmacological Interventions for Dizziness in Older People: Systematic Review. Phys. Ther. 2016, 96, 641–649. [Google Scholar] [CrossRef] [Green Version]
- Lystad, R.P.; Bell, G.; Bonnevie-Svendsen, M.; Carter, C.V. Manual therapy with and without vestibular rehabilitation for cervicogenic dizziness: A systematic review. Chiropr. Man. Ther. 2011, 19, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reid, S.A.; Rivett, D.A. Manual therapy treatment of cervicogenic dizziness: A systematic review. Man. Ther. 2005, 10, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, Q.; Vesci, B.; McLeod, T.C.V. Physical Activity and Intermittent Postconcussion Symptoms After a Period of Symptom-Limited Physical and Cognitive Rest. J. Athl. Train. 2016, 51, 739–742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yaseen, K.; Hendrick, P.; Ismail, A.; Felemban, M.; Alshehri, M.A. The effectiveness of manual therapy in treating cervicogenic dizziness: A systematic review. J. Phys. Ther. Sci. 2018, 30, 96–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheever, K.; McDevitt, J.; Phillips, J.; Kawata, K. The Role of Cervical Symptoms in Post-concussion Management: A Systematic Review. Sport Med. 2021, 51, 1875–1891. [Google Scholar] [CrossRef]
- Whitney, S.L.; Sparto, P.J.; Furman, J.M. Vestibular Rehabilitation and Factors That Can Affect Outcome. Semin. Neurol. 2020, 40, 165–172. [Google Scholar] [CrossRef]
- Valda-Rodrigo, J.; Benito-Orejas, J.I.; Vielba-Varea, J.A. Review of cervical vertigo. Rev. Orl 2018, 9, 97–104. [Google Scholar]
- Tudini, F.; Chui, K.K.; Grimes, J.; Laufer, R.; Kim, S.; Vaughan, V.; Yen, S.-C. Cervical spine manual therapy for aging and older adults. Top. Geriatr. Rehabil. 2016, 32, 88–105. [Google Scholar] [CrossRef]
- Peng, B. Cervical Vertigo: Historical Reviews and Advances. World Neurosurg. 2018, 109, 347–350. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, A.; Chatterjee, S.K.; Chakravarty, A. Vertigo and dizziness--a clinical approach. J. Assoc. Physicians India 2003, 51, 1095–1101. [Google Scholar]
- Magnusson, M.; Malmstrom, E.M. The conundrum of cervicogenic dizziness. Handb. Clin. Neurol. 2016, 137, 365–369. [Google Scholar]
- Kim, Y.; Cho, S.H. Pharmacopuncture for Cervicogenic Dizziness. J. Pharmacopunct. 2018, 21, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Kane, A.W.; Diaz, D.S.; Moore, C. Physical therapy management of adults with mild traumatic brain injury. Semin. Speech Lang. 2019, 40, 36–47. [Google Scholar]
- Huijbregts, P.; Vidal, P. Dizziness in orthopaedic physical therapy practice: History and physical examination. J. Man. Manip. Ther. 2005, 13, 221–250. [Google Scholar]
- Hain, T.C. Cervicogenic causes of vertigo. Curr. Opin. Neurol. 2015, 28, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Guinand, N.; Guyot, J.P. Cervical vertigo: Myth or reality? Rev. Med. Suisse 2009, 5, 1922–1924. [Google Scholar]
- Gnerre, P.; Casati, C.; Frualdo, M.; Cavalleri, M.; Guizzetti, S. Management of vertigo: From evidence to clinical practice. Ital. J. Med. 2015, 9, 180–192. [Google Scholar] [CrossRef] [Green Version]
- Escaloni, J.; Butts, R.; Dunning, J. The use of dry needling as a diagnostic tool and clinical treatment for cervicogenic dizziness: A narrative review & case series. J. Bodyw. Mov. Ther. 2018, 22, 947–955. [Google Scholar]
- Diaz, D.S. Management of athletes with postconcussion syndrome. Semin. Speech Lang. 2014, 35, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Cherchi, M. Infrequent causes of disequilibrium in the adult. Otolaryngol. Clin. N. Am. 2011, 44, 405–414. [Google Scholar] [CrossRef] [PubMed]
- Chang, A.K. An Introduction to Clinical Emergency Medicine: Guide for Practitioners in the Emergency Department; Ma-hadevan, S.V., Garmel, G.M., Eds.; Cambridge University Press: West Nyack, NY, USA, 2005; Volume 1, Chapter 19; pp. 241–252. [Google Scholar]
- Cancelliere, C.; Mohammed, R.J. Brain Drain: Psychosocial Factors Influence Recovery Following Mild Traumatic Brain Injury-3 Recommendations for Clinicians Assessing Psychosocial Factors. J. Orthop. Sports Phys. Ther. 2019, 49, 842–844. [Google Scholar] [CrossRef]
- Brandt, T.; Bronstein, A.M. Cervical vertigo. J. Neurol. Neurosurg. Psychiatry 2001, 71, 8–12. [Google Scholar] [CrossRef] [Green Version]
- Berthelot, J.M. Cervical dizziness is a reality, but cervical vertigo does not exist. Revue du Rhumatisme Monographies 2021, 1, 329–334. [Google Scholar] [CrossRef]
- AlSaif, A.A.; Johnson, E.G. Cervicogenic dizziness: Implications for physical therapy. Indian J. Physiother. Occup. Ther. 2011, 5, 6–11. [Google Scholar]
- Borg-Stein, J.; Rauch, S.D.; Krabak, B. Evaluation and management of cervicogenic dizziness. Crit. Rev. Phys. Rehabil. Med. 2001, 13, 255–264. [Google Scholar] [CrossRef]
- Smouha, E. Inner ear disorders. NeuroRehabilitation 2013, 32, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Taneja, M.K. Cervico-ocular reflex in cervical vertigo. Indian J. Otol. 2011, 17, 51–53. [Google Scholar] [CrossRef]
- Tassinari, C.; Romeo, A.; Broggi, L.; Vanti, C. Criteri Diagnostici Per Vertigine Cervicogenica: Revisione Narrative Della Letteratura. Sci. Riabil. 2013, 15, 24–35. [Google Scholar]
- Whitman, G.T. Dizziness. Am. J. Med. 2018, 131, 1431–1437. [Google Scholar] [CrossRef]
- Yang, L.; Chen, J.; Yang, C.; Pang, X.; Li, D.; Wu, B.; Wu, Y.; Lu, X.; Xu, J.; Chen, X.; et al. Cervical Intervertebral Disc Degeneration Contributes to Dizziness: A Clinical and Immunohistochemical Study. World Neurosurg. 2018, 119, e686–e693. [Google Scholar] [CrossRef] [PubMed]
- Wrisley, D.M. The Influence of Head Position on Postural Sway during Galvanic Vestibular Stimulation; University of Pittsburgh: Pittsburgh, PA, USA, 2002; 199p. [Google Scholar]
- Samji, A.; Yeoh, R.; Thiagarajan, V. Whiplash injury and neuro-otological sequelae: An evidence based systematic review. Hear. Balance Commun. 2014, 12, 66–77. [Google Scholar] [CrossRef]
- Peng, B.; Yang, L.; Yang, C.; Pang, X.; Chen, X.; Wu, Y. The effectiveness of anterior cervical decompression and fusion for the relief of dizziness in patients with cervical spondylosis: A multicentre prospective cohort study. Bone Jt. J. 2018, 100-B, 81–87. [Google Scholar] [CrossRef]
- Wang, Z.; Wang, X.; Yuan, W.; Jiang, D. Degenerative pathological irritations to cervical PLL may play a role in presenting sympathetic symptoms. Med. Hypotheses 2011, 77, 921–923. [Google Scholar] [CrossRef]
- Vonk, J.; Horlings, C.G.; Allum, J.H. Differentiating malingering balance disorder patients from healthy controls, compensated unilateral vestibular loss, and whiplash patients using stance and gait posturography. Audiol. Neurootol. 2010, 15, 261–272. [Google Scholar] [CrossRef] [Green Version]
- Kovacs, E.; Wang, X.; Grill, E. Economic burden of vertigo: A systematic review. Health Econ. Rev. 2019, 9, 37. [Google Scholar] [CrossRef]
- Teisberg, E.; Wallace, S.; O’Hara, S. Defining and Implementing Value-Based Health Care: A Strategic Framework. Acad. Med. J. Assoc. Am. Med. Coll. 2020, 95, 682–685. [Google Scholar] [CrossRef] [PubMed]
- Malik, K.; Eseonu, K.C.; Pang, D.; Fakouri, B. Is Preexisting Cervical Degeneration a Risk Factor for Poor Prognosis in Whiplash-Associated Disorder? Int. J. Spine Surg. 2021, 15, 710–717. [Google Scholar] [CrossRef] [PubMed]
- Seemungal, B.M.; Agrawal, Y.; Bisdorff, A.; Bronstein, A.; Cullen, K.E.; Goadsby, P.J.; Lempert, T.; Kothari, S.; Lim, P.B.; Magnusson, M.; et al. The Bárány Society position on ‘Cervical Dizziness’. J. Vestib. Res. 2022, 32, 487–499. [Google Scholar] [CrossRef] [PubMed]
- Dagli, R.J.; Sharma, A. Polypharmacy: A global risk factor for elderly people. J. Int. Oral Health 2014, 6, i–ii. [Google Scholar]
- Furman, J.M.; Jacob, R.G. A clinical taxonomy of dizziness and anxiety in the otoneurological setting. J. Anxiety Disord. 2001, 15, 9–26. [Google Scholar] [CrossRef] [PubMed]
- Staab, J.P.; Eckhardt-Henn, A.; Horii, A.; Jacob, R.; Strupp, M.; Brandt, T.; Bronstein, A. Diagnostic criteria for persistent postural-perceptual dizziness (PPPD): Consensus document of the committee for the Classification of Vestibular Disorders of the Bárány Society. J. Vestib. Res. 2017, 27, 191–208. [Google Scholar] [CrossRef] [Green Version]
- Lempert, T.; Olesen, J.; Furman, J.; Waterston, J.; Seemungal, B.; Carey, J.; Bisdorff, A.; Versino, M.; Evers, S.; Newman-Toker, D. Vestibular migraine: Diagnostic criteria. J. Vestib. Res. 2012, 22, 167–172. [Google Scholar] [CrossRef] [Green Version]
- Bisdorff, A.R. Management of vestibular migraine. Ther. Adv. Neurol. Disord. 2011, 4, 183–191. [Google Scholar] [CrossRef] [Green Version]
- Ardç, F.N.; Topuz, B.; Kara, C.O. Impact of Multiple Etiology on Dizziness Handicap. Otol. Neurotol. 2006, 27, 676–680. [Google Scholar] [CrossRef]
- Cobo, E.P.; Mesquida, M.E.; Fanegas, E.P.; Atanasio, E.M.; Pastor, M.B.; Pont, C.P.; Prieto, C.M.; Gómez, G.R.; Cano, L.G. What factors have influence on persistence of neck pain after a whiplash? Spine 2010, 35, E338–E343. [Google Scholar] [CrossRef]
- Mijovic, T.; Carriot, J.; Zeitouni, A.; Cullen, K.E. Head movements in patients with vestibular lesion: A novel approach to functional assessment in daily life setting. Otol. Neurotol. Off. Publ. Am. Otol. Soc. Am. Neurotol. Soc. Eur. Acad. Otol. Neurotol. 2014, 35, e348–e357. [Google Scholar] [CrossRef]
Figure 1.
Prisma flow chart showing the identification of studies via databases.

Figure 2.
Research designs on proprioceptive cervicogenic dizziness. The number of articles selected by this scoping review is classified by study designs. RCT: randomized control trials.
Figure 2.
Research designs on proprioceptive cervicogenic dizziness. The number of articles selected by this scoping review is classified by study designs. RCT: randomized control trials.

Figure 3.
Quantitative synthesis of PCGD subpopulations’ occurrence in the literature. Articles mentioning more than one subpopulation were counted in each pertinent category, except when all four subgroups were mentioned. No subgroups: no subpopulations are specified in the articles.
Figure 3.
Quantitative synthesis of PCGD subpopulations’ occurrence in the literature. Articles mentioning more than one subpopulation were counted in each pertinent category, except when all four subgroups were mentioned. No subgroups: no subpopulations are specified in the articles.

Figure 4.
Pertinent differential diagnosis. SSCD: superior semicircular canal dehiscence syndrome; BPPV: benign paroxysmal positional vertigo; PPPD: persistent postural-perceptual dizziness; TIA: transient ischemic attack TBI: traumatic brain injury Vx: vertebral.
Figure 4.
Pertinent differential diagnosis. SSCD: superior semicircular canal dehiscence syndrome; BPPV: benign paroxysmal positional vertigo; PPPD: persistent postural-perceptual dizziness; TIA: transient ischemic attack TBI: traumatic brain injury Vx: vertebral.

Figure 5.
Pertinent tests for differential diagnosis. Cardiac hx: cardiac history, vx: vertebral, MRI: magnetic resonance imaging, VBIt: vertebrobasilar insufficiency testing, vHIT-hit: video head impulse test-head impulse test, VNG: videonystagmography, Vx Fx signs: vertebral fracture signs, X-ray: cervical spine X-ray imagery.
Figure 5.
Pertinent tests for differential diagnosis. Cardiac hx: cardiac history, vx: vertebral, MRI: magnetic resonance imaging, VBIt: vertebrobasilar insufficiency testing, vHIT-hit: video head impulse test-head impulse test, VNG: videonystagmography, Vx Fx signs: vertebral fracture signs, X-ray: cervical spine X-ray imagery.

Figure 6.
Clinical tests (to «rule-in») PCGD. FRT: flexion rotation test, JPE: joint position error test, MSE: manual spinal evaluation, PST: palpation for segmental tenderness, SNAG: sustained natural apophyseal glide SPNT: smooth pursuit neck torsion test.
Figure 6.
Clinical tests (to «rule-in») PCGD. FRT: flexion rotation test, JPE: joint position error test, MSE: manual spinal evaluation, PST: palpation for segmental tenderness, SNAG: sustained natural apophyseal glide SPNT: smooth pursuit neck torsion test.

Figure 7.
Interventions on PCGD in the literature.

Figure 8.
Tools to measure change CROM: cervical range of motion, DHI: dizziness handicap inventory, GPE: global perceived effect, VNG: videonystagmography, HADS: Hospital Anxiety and Depression Scale, JPE: joint position error test, NDI: neck disability index, HRQoL: health-related quality of life, TSK: Tampa Scale for Kinesiophobia, VAS: visual analog scale.
Figure 8.
Tools to measure change CROM: cervical range of motion, DHI: dizziness handicap inventory, GPE: global perceived effect, VNG: videonystagmography, HADS: Hospital Anxiety and Depression Scale, JPE: joint position error test, NDI: neck disability index, HRQoL: health-related quality of life, TSK: Tampa Scale for Kinesiophobia, VAS: visual analog scale.

Figure 9.
Measurement instruments in proprioceptive cervicogenic dizziness: an ICF classification (some measurement instruments are suitable in more than one ICF component). CROM: cervical range of motion, DHI: dizziness handicap inventory, GPE: global perceived effect, GROC-scale: global rating of change, HADS: Hospital Anxiety and Depression Scale, JPE: joint position error test, NDI: neck disability index, HRQoL: health-related quality of life, TSK: Tampa Scale for Kinesiophobia, VAS: visual analog scale.
Figure 9.
Measurement instruments in proprioceptive cervicogenic dizziness: an ICF classification (some measurement instruments are suitable in more than one ICF component). CROM: cervical range of motion, DHI: dizziness handicap inventory, GPE: global perceived effect, GROC-scale: global rating of change, HADS: Hospital Anxiety and Depression Scale, JPE: joint position error test, NDI: neck disability index, HRQoL: health-related quality of life, TSK: Tampa Scale for Kinesiophobia, VAS: visual analog scale.


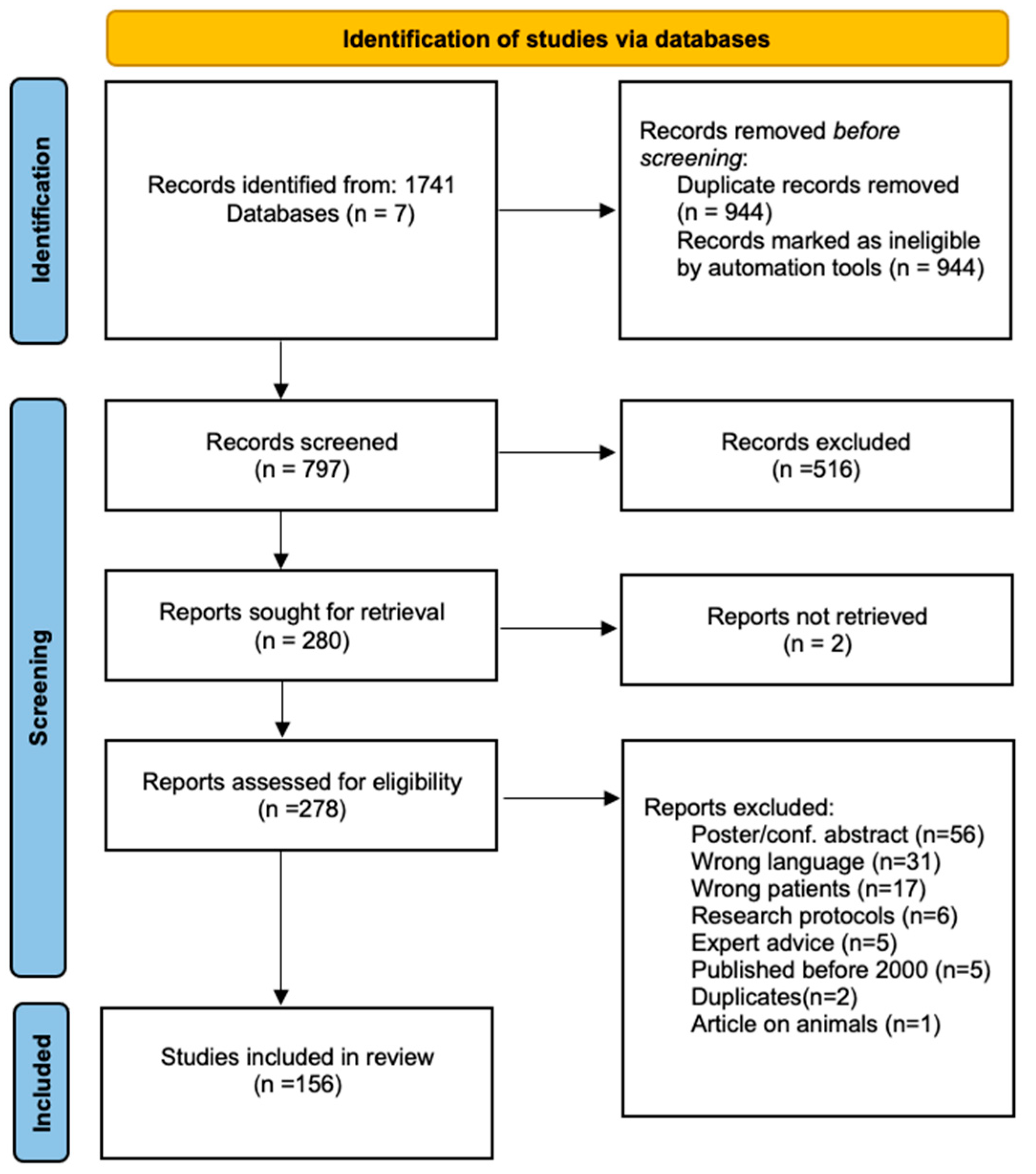{kind=link}
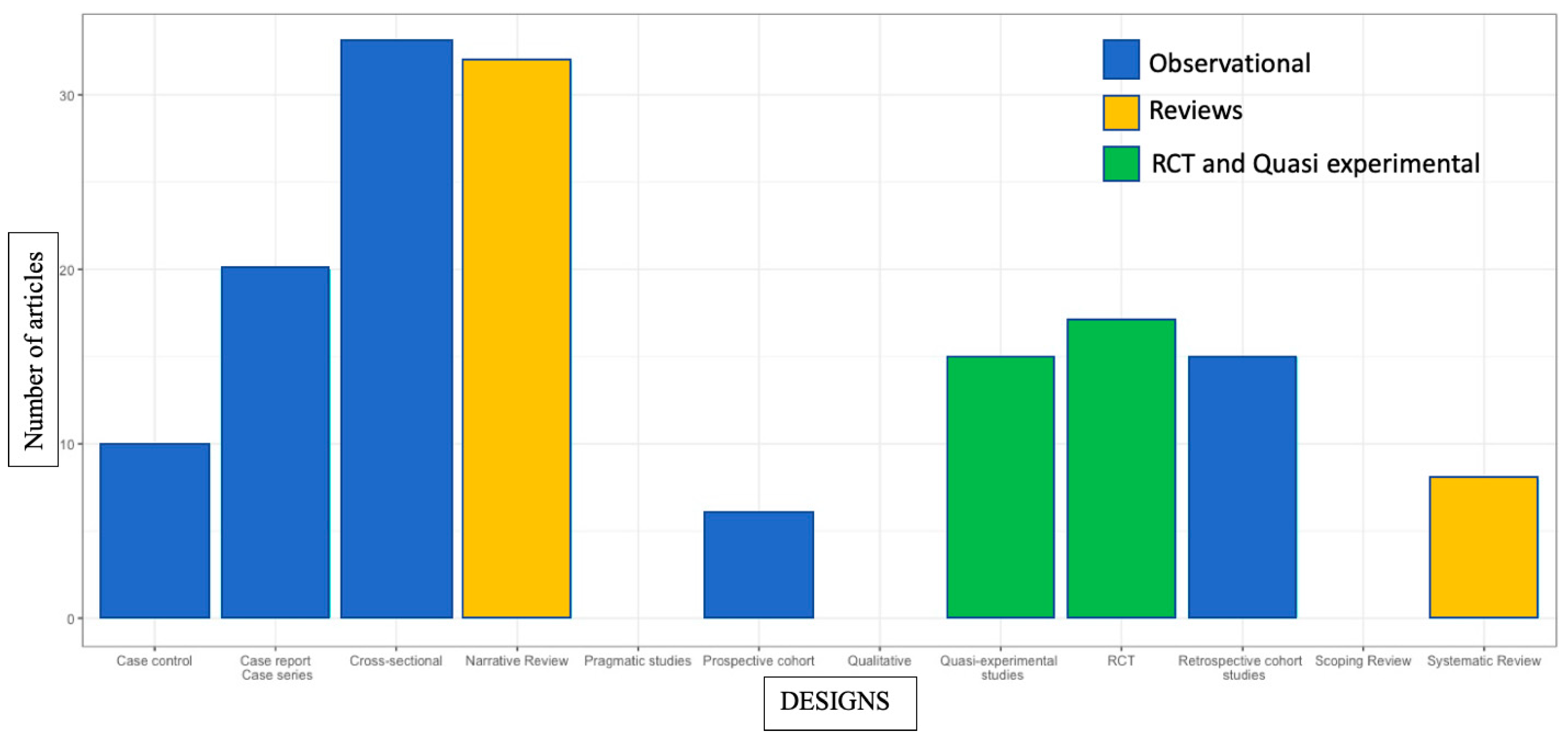{kind=link}
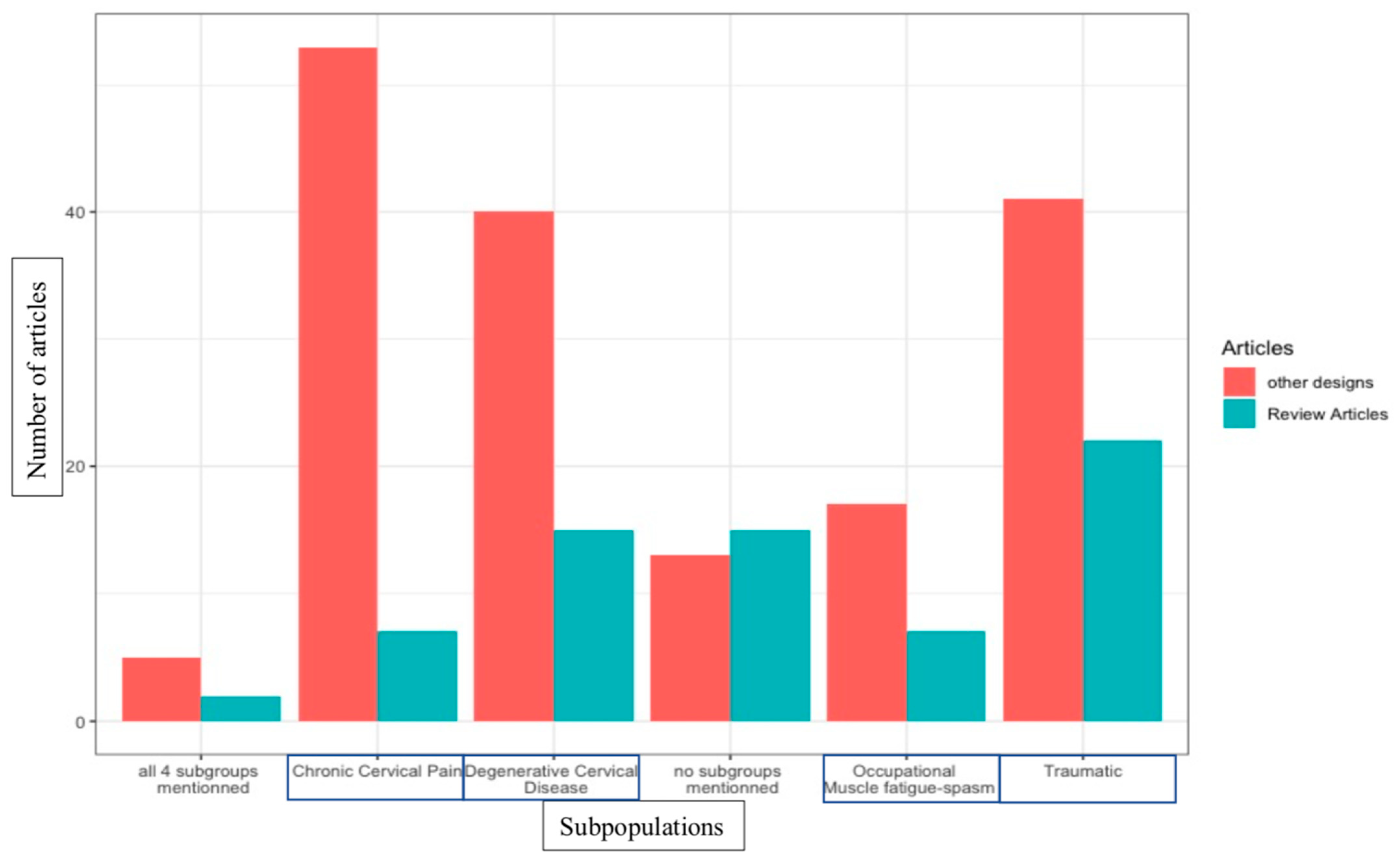{kind=link}
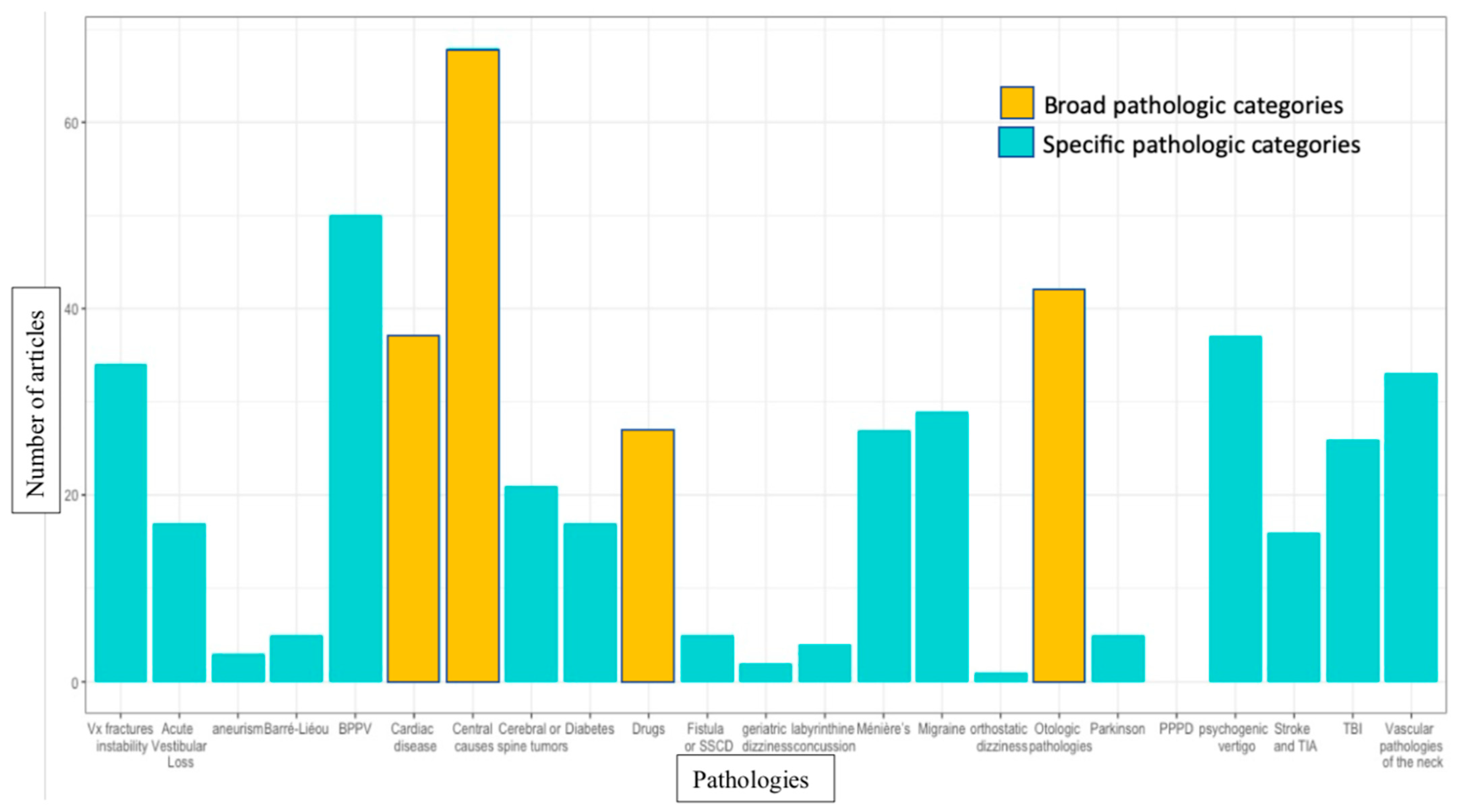{kind=link}
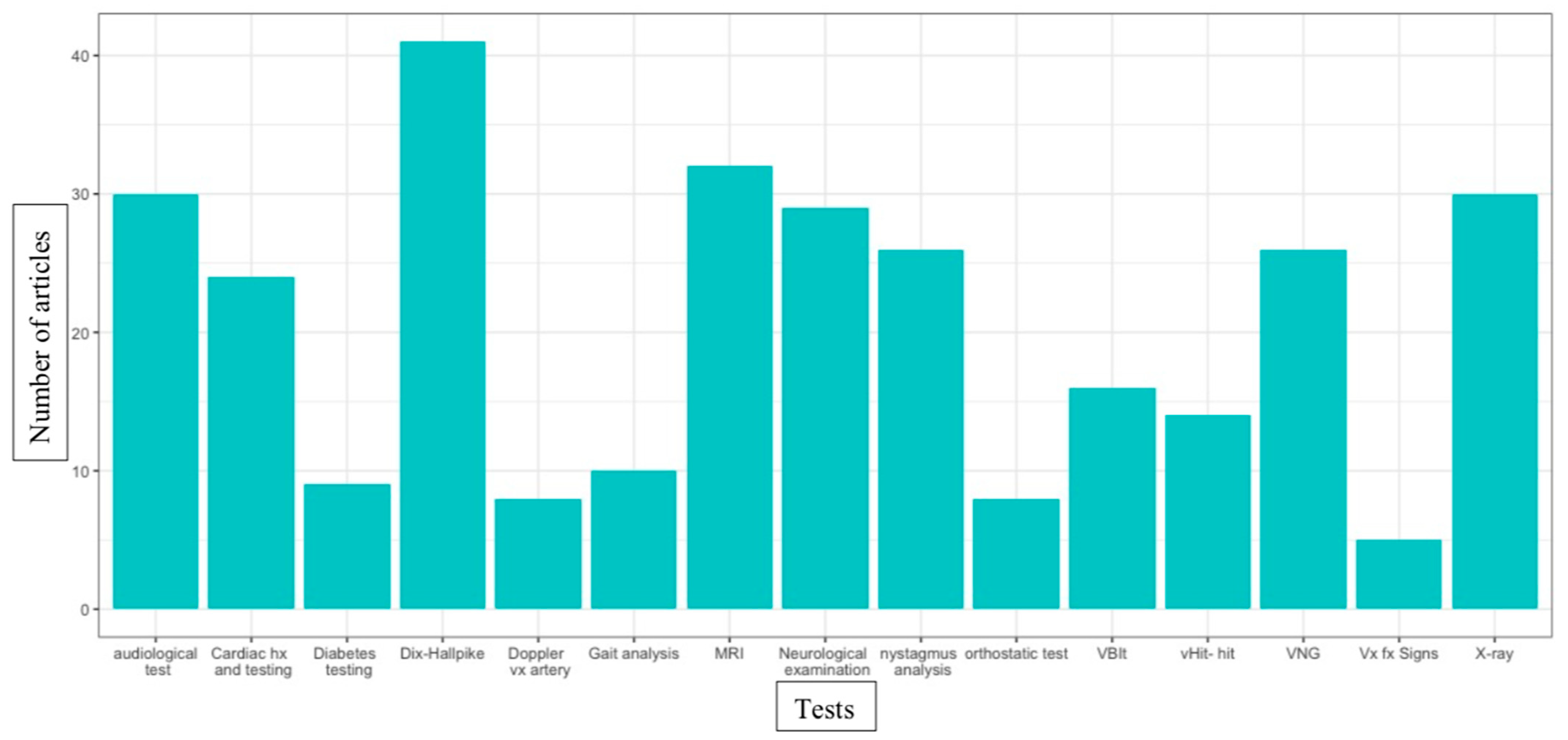{kind=link}
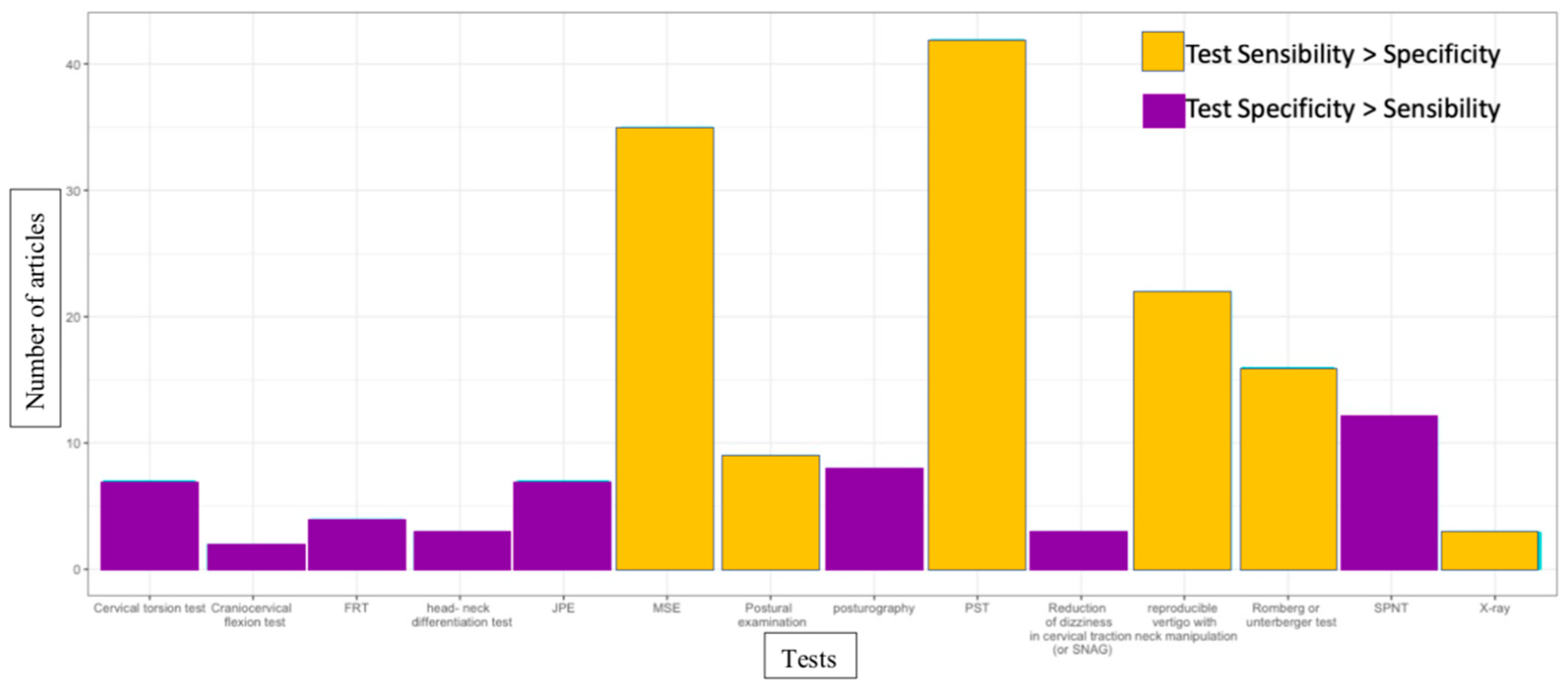{kind=link}
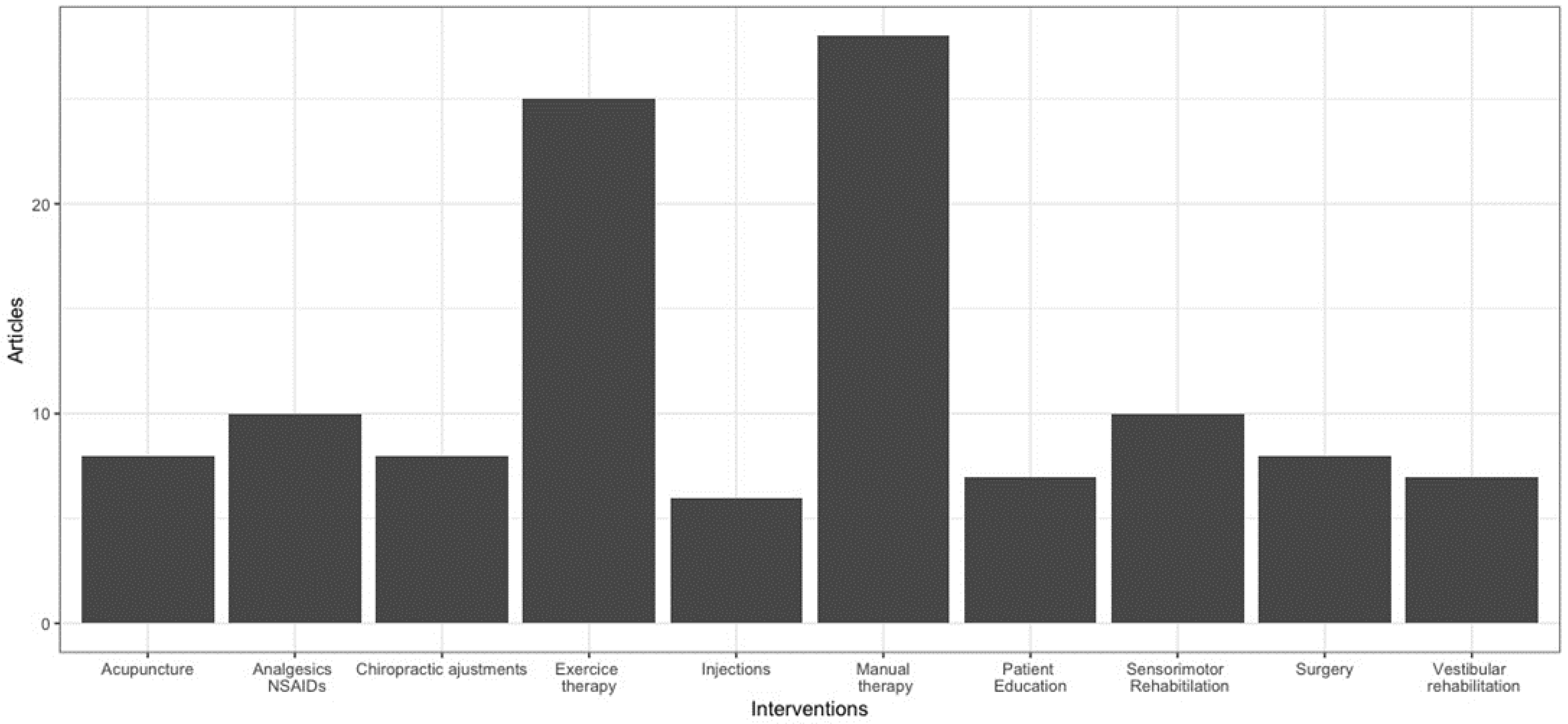{kind=link}
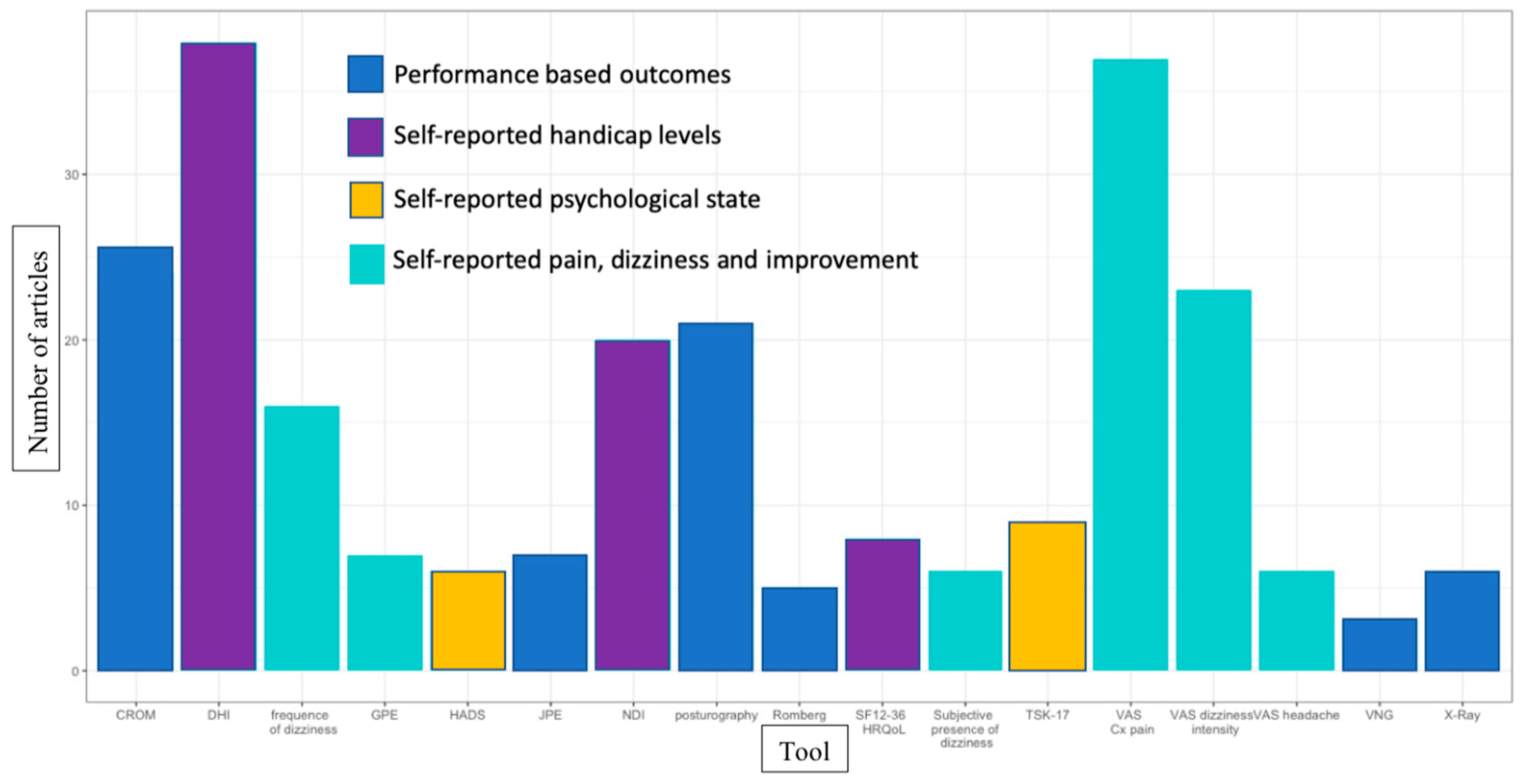{kind=link}
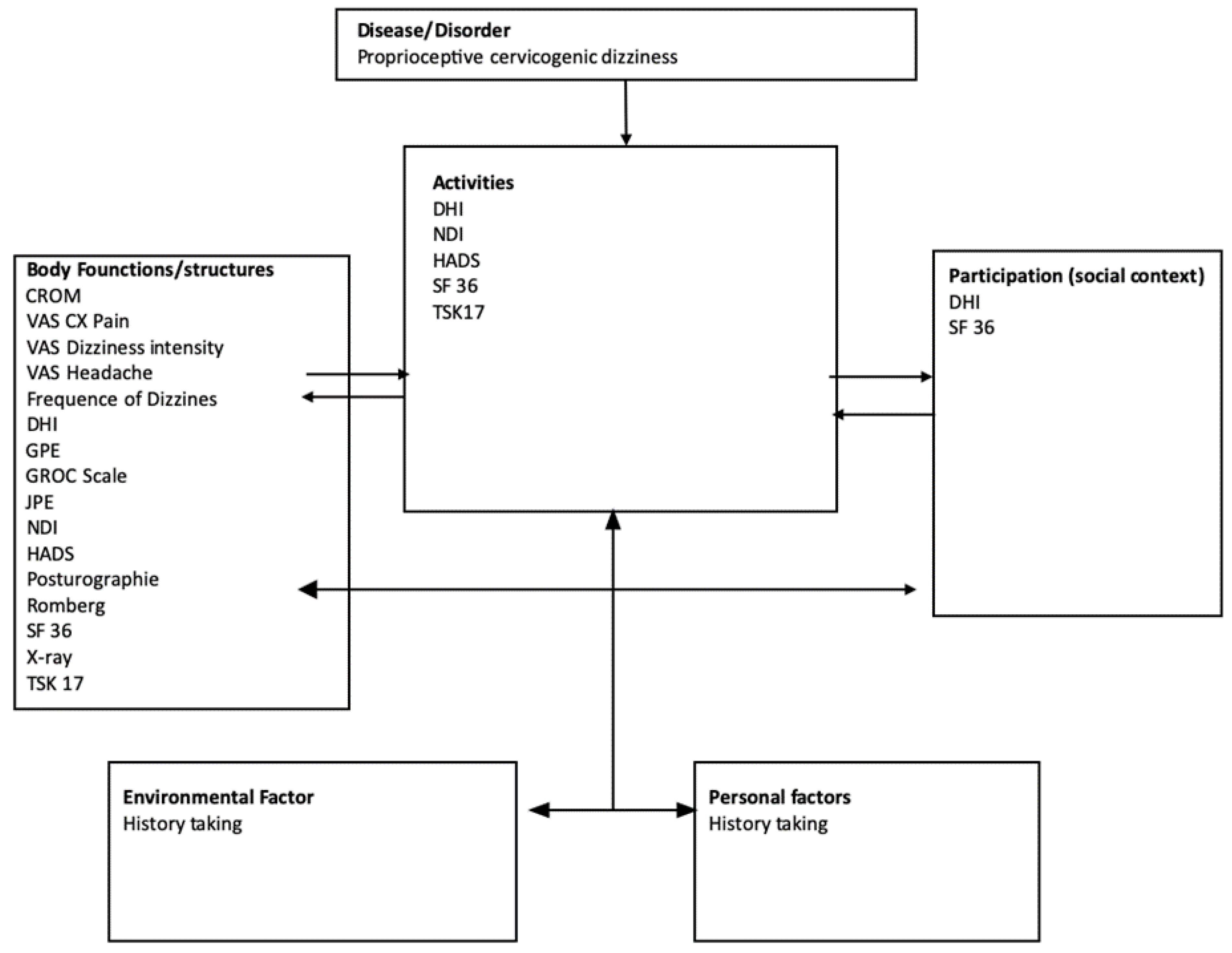{kind=link}
Table 1.
Subpopulations, clinical presentation and hypothesized etiological mechanism.
| Subpopulations | Clinical Presentation | Hypothesized Etiological Mechanism |
|---|---|---|
| Chronic cervical pain | Patients with cervical pain for more than 12 weeks with no history of trauma or presence of muscle spasm that present dizziness. | Pain potentially alters proprioception |
| Traumatic | Patients have a history of 1 WAD or 2 PCS. Along with dizziness and cervical pain, patients may present the following symptoms: ataxia, unsteadiness of gait, postural imbalance, limited neck range of motion and potentially headache. | Pain, limitation of movement, and strains of joint capsules, paravertebral ligaments, and cervical musculature can alter cervical proprioception |
| Degenerative cervical disease | Mostly elderly populations presenting dizziness associated with degenerative cervical changes and cervical pain. Some patients may complain of headaches, or shoulder pain and some radicular symptoms or possible. | Histological changes and inflammatory processes can alter cervical proprioception |
| Occupational muscle spasm or fatigue | Sedentary populations that present dizziness associated with neck muscle fatigue or spasm without trauma. Patients could present limited cervical range of motion. | Muscle spasm may alter proprioceptive input |
1 WAD: whiplash associated disorders. 2 PCS: post-concussion syndrome.
Table 2.
Occurrences of differential diagnoses in articles mentioning different subpopulations of PCGD.
Table 2.
Occurrences of differential diagnoses in articles mentioning different subpopulations of PCGD.
| Traumatic | Degenerative Cervical Disease | Chronic Cervicalgia | Occupational (Muscle Spasm) |
|---|---|---|---|
| 1 BPPV (n = 22) | Central causes (n = 22) | Central causes (n = 28) | 1 BPPV (n = 11) |
| Central causes (n = 19) | Cardiac disease (n = 17) | 1 BPPV (n = 23) | Central causes (n = 9) |
| 3 Vx fracture instability (n = 17) | 1 BPPV (n = 16) | Cardiac disease (n = 20) | Cardiac disease (n = 8) |
| Migraine (n = 13) | 3 Vx fracture instability (n = 14) | 3 Vx fracture instability (n = 19) | Vascular pathologies of the neck (n = 7) |
| Psychogenic vertigo (n = 15) | Psychogenic vertigo (n = 13) | Migraine (n = 19) | Migraine (n = 7) |
| 2 TBI (n = 12) | Drugs and vascular pathologies of the neck (n = 11 for both) | Otologic pathologies (n = 18) | Drugs (n = 6) |
1 BPPV: Benign paroxysmal positional vertigo 2 TBI: traumatic brain injury 3 Vx: vertebral.
Table 3.
Intervention modalities in Proprioceptive cervicogenic dizziness *.
| Chinese Medicine | Physiotherapy | Pharmacology | Surgery-Injection |
|---|---|---|---|
| Acupuncture Tuina Acupressure Herbs | Manual therapy Transcutaneous electrical nerve stimulation Vestibular rehabilitation Dry needling Exercise therapy Sensorimotor rehabitilation Ultrasound Termal therapy Sustained natural apophyseal glide | Non-steroidal anti-inflammatory drugs Acetaminophen Analgesics Betahistine Muscle relaxant | Total disc replacement (TDR) Medial branch blocks (MMBs) Occipital nerve blocks (GON) Trigger point injections (TPI) Mepivacaine, bupivacaine Anterior cerical discetomy and fusion (ACDF) Percutaneous laser disc decompression (PLDD) and disc decompression. Botulinum toxin injection Coblation discoplasty Carbon fiber fusion cage (CIFC) |
* Other modalities included are chiropractic adjustments; chuna manual therapy; helical patches; cervical traction; and patient education.
Table 4.
Occurrences of interventions in articles mentioning different subpopulations of proprioceptive cervicogenic dizziness.
Table 4.
Occurrences of interventions in articles mentioning different subpopulations of proprioceptive cervicogenic dizziness.
| Traumatic | Degenerative Cervical Disease | Chronic Cervicalgia | Occupational (Muscle Spasm) |
|---|---|---|---|
| Exercise therapy (n = 10) | Manual therapy (n = 9) | Manual therapy (n = 15) | Manual therapy (n = 4) |
| Manual therapy (n = 10) | Surgery (n = 8) | Exercise therapy (n = 13) | Exercise therapy (n = 3) |
| Sensorimotor rehabilitation (n = 6) | Analgesic NSAID 1 (n = 6) | Chiropractic adjustments (n = 7) | Patient education (n = 3) |
| Analgesic NSAID 1 (n = 5) | Exercise therapy (n = 6) | Injection (n = 5)Analgesic NSAID 1 (n = 5) | Analgesic NSAID 1 (n = 3) |
| Patient education (n = 5) | Acupuncture (n = 4) | Acupuncture (n = 5) | Chiropractic adjustments (n = 2) |
1 NSAID: Non-steroidal anti-inflammatory drugs.
Table 5.
Measures of change used across subpopulations.
| Traumatic | Degenerative cervical disease | Chronic cervicalgia | Occupational (muscle spasm) |
|---|---|---|---|
| 1 DHI (n = 15) | 1 DHI (n = 16) | 2 VAS Cervical pain (n = 24) | 1 DHI (n = 5) |
| 2 VAS Cervical pain (n = 12) | 2 VAS Cervical pain (n = 16) | 1 DHI (n = 23) | 2 VAS Cervical pain (n = 5) |
| Posturography (n = 10) | 4 CROM (n = 9) | 4 CROM (n = 14) | 5 TSK-17 (n = 3) |
| 3 NDI (n = 9) | 3 NDI (n = 8) | 3 NDI (n = 13) | 3 NDI (n = 2) |
| 4 CROM (n = 7) | 2 VAS intensity and frequency of dizziness both (n = 8) | 2 VAS intensity and frequency (n = 13) | Posturography (n = 2) and 4 CROM (n = 2) |
1 DHI: dizziness handicap inventory; 2 VAS: visual analog scale; 3 NDI: neck disability index; 4 CROM: cervical range of motion; 5 TSK: Tampa Scale for Kinesiophobia.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Gill-Lussier, J.; Saliba, I.; Barthélemy, D. Proprioceptive Cervicogenic Dizziness Care Trajectories in Patient Subpopulations: A Scoping Review. J. Clin. Med. 2023, 12, 1884. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12051884
AMA Style
Gill-Lussier J, Saliba I, Barthélemy D. Proprioceptive Cervicogenic Dizziness Care Trajectories in Patient Subpopulations: A Scoping Review. Journal of Clinical Medicine. 2023; 12(5):1884. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12051884
Chicago/Turabian StyleGill-Lussier, Joseph, Issam Saliba, and Dorothy Barthélemy. 2023. "Proprioceptive Cervicogenic Dizziness Care Trajectories in Patient Subpopulations: A Scoping Review" Journal of Clinical Medicine 12, no. 5: 1884. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12051884
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.