

Association of Chronic Heart Failure with Frailty, Malnutrition, and Sarcopenia Parameters in Older Patients—A Cross-Sectional Study in a Geriatric Ward
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients’ Characteristics
2.2. Statistical Analysis
2.3. Ethics Approval
3. Results
3.1. Study Cohort Characteristics—Sociodemographic and Health Correlates of Heart Failure
3.2. Study Cohort Characteristics—Functional and Nutritional Correlates of Heart Failure
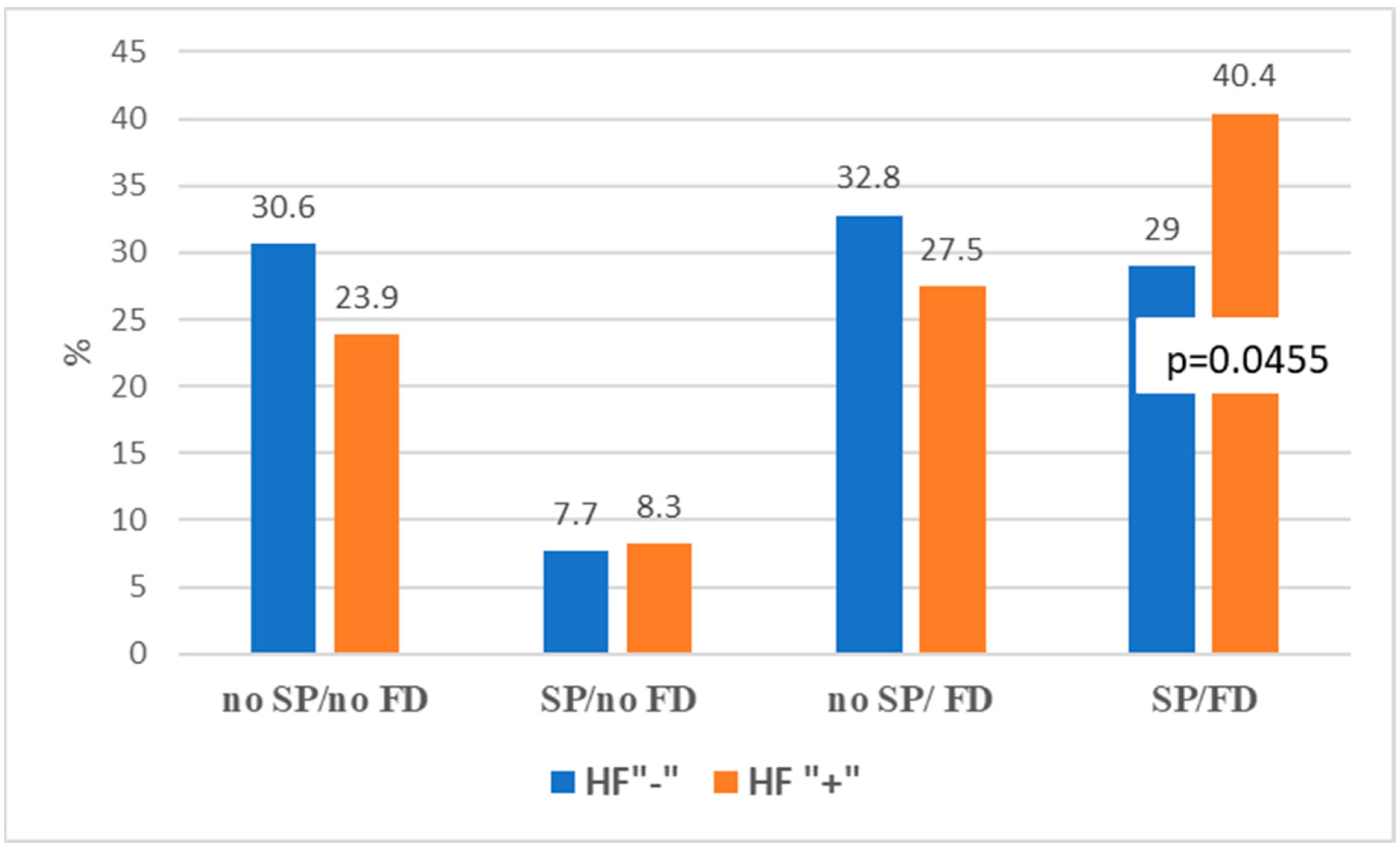
3.3. Heart Failure, Sarcopenia, and Severe Sarcopenia
3.4. Heart Failure and Its Determinants—A Multivariable Logistic Regression Analysis
4. Discussion
5. Conclusions
- The study confirms the high occurrence of geriatric syndromes, such as dynapenia, inactivity, and frailty, in the HF group, indicating a need for comprehensive geriatric assessment in HF patients.
- Obesity and sarcopenic obesity seem to be more frequent clinical problems than sarcopenia alone among geriatric patients with HF.
- High levels of inactivity and dynapenia in geriatric HF patients may indicate a direction of prevention and therapeutic strategies.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics—2020 Update: A Report From the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef]
- Savarese, G.; Lund, L.H. Global Public Health Burden of Heart Failure. Card. Fail. Rev. 2017, 3, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Conrad, N.; Judge, A.; Tran, J.; Mohseni, H.; Hedgecott, D.; Crespillo, A.P.; Allison, M.; Hemingway, H.; Cleland, J.G.; McMurray, J.J.V.; et al. Temporal trends and patterns in heart failure incidence: A population-based study of 4 million individuals. Lancet 2018, 391, 572–580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chioncel, O.; Lainscak, M.; Seferovic, P.M.; Anker, S.D.; Crespo-Leiro, M.G.; Harjola, V.P.; Parissis, J.; Laroche, C.; Piepoli, M.F.; Fonseca, C.; et al. Epidemiology and one-year outcomes in patients with chronic heart failure and preserved, mid-range and reduced ejection fraction: An analysis of the ESC Heart Failure Long-Term Registry. Eur. J. Heart Fail. 2017, 19, 1574–1585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duong, M.H.; Gnjidic, D.; McLachlan, A.J.; Sakiris, M.A.; Goyal, P.; Hilmer, S.N. The Prevalence of Adverse Drug Reactions and Adverse Drug Events from Heart Failure Medications in Frail Older Adults: A Systematic Review. Drugs Aging 2022, 39, 631–643. [Google Scholar] [CrossRef]
- Wang, X.; Zhou, C.; Li, Y.; Li, H.; Cao, Q.; Li, F. Prognostic Value of Frailty for Older Patients with Heart Failure: A Systematic Review and Meta-Analysis of Prospective Studies. BioMed. Res. Int. 2018, 2018, 8739058. [Google Scholar] [CrossRef]
- Sze, S.; Pellicori, P.; Zhang, J.; Clark, A.L. Malnutrition, congestion and mortality in ambulatory patients with heart failure. Heart 2019, 105, 297–306. [Google Scholar] [CrossRef] [Green Version]
- Fernandez-Pombo, A.; Rodriguez-Carnero, G.; Castro, A.I.; Canton-Blanco, A.; Seoane, L.M.; Casanueva, F.F.; Crujeiras, A.B.; Martinez-Olmos, M.A. Relevance of nutritional assessment and treatment to counteract cardiac cachexia and sarcopenia in chronic heart failure. Clin. Nutr. 2021, 40, 5141–5155. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, J.; Ni, W.; Yuan, X.; Zhang, H.; Li, P.; Xu, J.; Zhao, Z. Sarcopenia in heart failure: A systematic review and meta-analysis. ESC Heart Fail. 2021, 8, 1007–1017. [Google Scholar] [CrossRef]
- Collamati, A.; Marzetti, E.; Calvani, R.; Tosato, M.; D’Angelo, E.; Sisto, A.N.; Landi, F. Sarcopenia in heart failure: Mechanisms and therapeutic strategies. J. Geriatr. Cardiol. 2016, 13, 615–624. [Google Scholar] [CrossRef]
- Choi, J.Y.; Rajaguru, V.; Shin, J.; Kim, K.I. Comprehensive geriatric assessment and multidisciplinary team interventions for hospitalized older adults: A scoping review. Arch. Gerontol. Geriatr. 2023, 104, 104831. [Google Scholar] [CrossRef]
- Kaiser, M.J.; Bauer, J.M.; Ramsch, C.; Uter, W.; Guigoz, Y.; Cederholm, T.; Thomas, D.R.; Anthony, P.; Charlton, K.E.; Maggio, M.; et al. Validation of the Mini Nutritional Assessment short-form (MNA-SF): A practical tool for identification of nutritional status. J. Nutr. Health Aging 2009, 13, 782–788. [Google Scholar] [CrossRef]
- Rolland, Y.; Lauwers-Cances, V.; Cournot, M.; Nourhashemi, F.; Reynish, W.; Riviere, D.; Vellas, B.; Grandjean, H. Sarcopenia, calf circumference, and physical function of elderly women: A cross-sectional study. J. Am. Geriatr. Soc. 2003, 51, 1120–1124. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Cheung, A.; Haas, B.; Ringer, T.J.; McFarlan, A.; Wong, C.L. Canadian Study of Health and Aging Clinical Frailty Scale: Does It Predict Adverse Outcomes among Geriatric Trauma Patients? J. Am. Coll. Surg. 2017, 225, 658–665.e653. [Google Scholar] [CrossRef]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Rodjer, L.; Jonsdottir, I.H.; Rosengren, A.; Bjorck, L.; Grimby, G.; Thelle, D.S.; Lappas, G.; Borjesson, M. Self-reported leisure time physical activity: A useful assessment tool in everyday health care. BMC Public Health 2012, 12, 693. [Google Scholar] [CrossRef] [Green Version]
- Fillenbaum, G.G.; Smyer, M.A. The development, validity, and reliability of the OARS multidimensional functional assessment questionnaire. J. Gerontol. 1981, 36, 428–434. [Google Scholar] [CrossRef]
- Tinetti, M.E. Performance-oriented assessment of mobility problems in elderly patients. J. Am. Geriatr. Soc. 1986, 34, 119–126. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Hodkinson, H.M. Evaluation of a mental test score for assessment of mental impairment in the elderly. Age Ageing 1972, 1, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Yesavage, J.A. Geriatric Depression Scale. Psychopharmacol. Bull. 1988, 24, 709–711. [Google Scholar]
- Calculator.net. Sample Size Calculator. Available online: https://www.calculator.net/sample-size-calculator.html (accessed on 16 January 2023).
- Boully, C.; Vidal, J.S.; Guibert, E.; Ghazali, F.N.; Pesce, A.; Beauplet, B.; Roger, J.D.; Carriere, I.; Timbely, B.; Idiri, H.; et al. National survey on the management of heart failure in individuals over 80 years of age in French geriatric care units. BMC Geriatr. 2019, 19, 204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fagotto, V.; Cavarape, A.; Boccanelli, A. Heart failure in the elderly: A geriatric syndrome. Picture of the modern situation. Monaldi Arch. Chest Dis. 2019, 89, 67–68. [Google Scholar] [CrossRef]
- Wojszel, Z.B.; Kasiukiewicz, A. Determinants of anticoagulant therapy in atrial fibrillation at discharge from a geriatric ward: Cross sectional study. J. Thromb. Thrombolysis 2020, 49, 18–26. [Google Scholar] [CrossRef] [Green Version]
- Carretero-Gómez, J.; Pérez-Martínez, P.; Seguí-Ripoll, J.M.; Carrasco-Sánchez, F.J.; Lois Martínez, N.; Fernández Pérez, E.; Pérez Hernández, O.; García Ordoñez, M.Á.; Martín González, C.; Vigueras-Pérez, J.F.; et al. High-Risk Obesity Phenotypes: Target for Multimorbidity Prevention at the ROFEMI Study. J. Clin. Med. 2022, 11, 4644. [Google Scholar] [CrossRef]
- Li, H.; Cen, K.; Sun, W.; Feng, B. Prognostic value of geriatric nutritional risk index in elderly patients with heart failure: A meta-analysis. Aging Clin. Exp. Res. 2021, 33, 1477–1486. [Google Scholar] [CrossRef]
- Jensen, G.L.; Cederholm, T.; Correia, M.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; de Baptista, G.A.; Barazzoni, R.; Blaauw, R.; Coats, A.J.S.; et al. GLIM Criteria for the Diagnosis of Malnutrition: A Consensus Report From the Global Clinical Nutrition Community. JPEN J. Parenter. Enteral Nutr. 2019, 43, 32–40. [Google Scholar] [CrossRef] [Green Version]
- Hu, F.J.; Liu, H.; Liu, X.L.; Jia, S.L.; Hou, L.S.; Xia, X.; Dong, B.R. Mid-Upper Arm Circumference as an Alternative Screening Instrument to Appendicular Skeletal Muscle Mass Index for Diagnosing Sarcopenia. Clin. Interv. Aging 2021, 16, 1095–1104. [Google Scholar] [CrossRef]
- Khan, H.; Kalogeropoulos, A.P.; Georgiopoulou, V.V.; Newman, A.B.; Harris, T.B.; Rodondi, N.; Bauer, D.C.; Kritchevsky, S.B.; Butler, J. Frailty and risk for heart failure in older adults: The health, aging, and body composition study. Am. Heart J. 2013, 166, 887–894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woods, N.F.; LaCroix, A.Z.; Gray, S.L.; Aragaki, A.; Cochrane, B.B.; Brunner, R.L.; Masaki, K.; Murray, A.; Newman, A.B.; Women’s Health, I. Frailty: Emergence and consequences in women aged 65 and older in the Women’s Health Initiative Observational Study. J. Am. Geriatr.Soc. 2005, 53, 1321–1330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Riet, E.E.; Hoes, A.W.; Wagenaar, K.P.; Limburg, A.; Landman, M.A.; Rutten, F.H. Epidemiology of heart failure: The prevalence of heart failure and ventricular dysfunction in older adults over time. A systematic review. Eur. J. Heart Fail. 2016, 18, 242–252. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Bohm, M.; Burri, H.; Butler, J.; Celutkiene, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Rev. Esp. Cardiol. 2022, 75, 523. [Google Scholar] [CrossRef]
- Vitale, C.; Jankowska, E.; Hill, L.; Piepoli, M.; Doehner, W.; Anker, S.D.; Lainscak, M.; Jaarsma, T.; Ponikowski, P.; Rosano, G.M.C.; et al. Heart Failure Association/European Society of Cardiology position paper on frailty in patients with heart failure. Eur. J. Heart Fail. 2019, 21, 1299–1305. [Google Scholar] [CrossRef] [Green Version]
- Emami, A.; Saitoh, M.; Valentova, M.; Sandek, A.; Evertz, R.; Ebner, N.; Loncar, G.; Springer, J.; Doehner, W.; Lainscak, M.; et al. Comparison of sarcopenia and cachexia in men with chronic heart failure: Results from the Studies Investigating Co-morbidities Aggravating Heart Failure (SICA-HF). Eur. J. Heart Fail. 2018, 20, 1580–1587. [Google Scholar] [CrossRef] [Green Version]
- Fulster, S.; Tacke, M.; Sandek, A.; Ebner, N.; Tschope, C.; Doehner, W.; Anker, S.D.; von Haehling, S. Muscle wasting in patients with chronic heart failure: Results from the studies investigating co-morbidities aggravating heart failure (SICA-HF). Eur. Heart J. 2013, 34, 512–519. [Google Scholar] [CrossRef] [Green Version]
- Gorodeski, E.Z.; Goyal, P.; Hummel, S.L.; Krishnaswami, A.; Goodlin, S.J.; Hart, L.L.; Forman, D.E.; Wenger, N.K.; Kirkpatrick, J.N.; Alexander, K.P.; et al. Domain Management Approach to Heart Failure in the Geriatric Patient: Present and Future. J. Am. Coll. Cardiol. 2018, 71, 1921–1936. [Google Scholar] [CrossRef]
- Papadopoulou, S.K.; Papadimitriou, K.; Voulgaridou, G.; Georgaki, E.; Tsotidou, E.; Zantidou, O.; Papandreou, D. Exercise and Nutrition Impact on Osteoporosis and Sarcopenia-The Incidence of Osteosarcopenia: A Narrative Review. Nutrients 2021, 13, 4499. [Google Scholar] [CrossRef]
- Blanquet, M.; Massoulie, G.; Boirie, Y.; Guiguet-Auclair, C.; Mulliez, A.; Anker, S.; Boiteux, M.D.; Jean, F.; Combaret, N.; Souteyrand, G.; et al. Handgrip strength to screen early-onset sarcopenia in heart failure. Clin. Nutr. ESPEN 2022, 50, 183–190. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Total | HF + Group | HF− Group | p Values a | Missing Data |
|---|---|---|---|---|---|
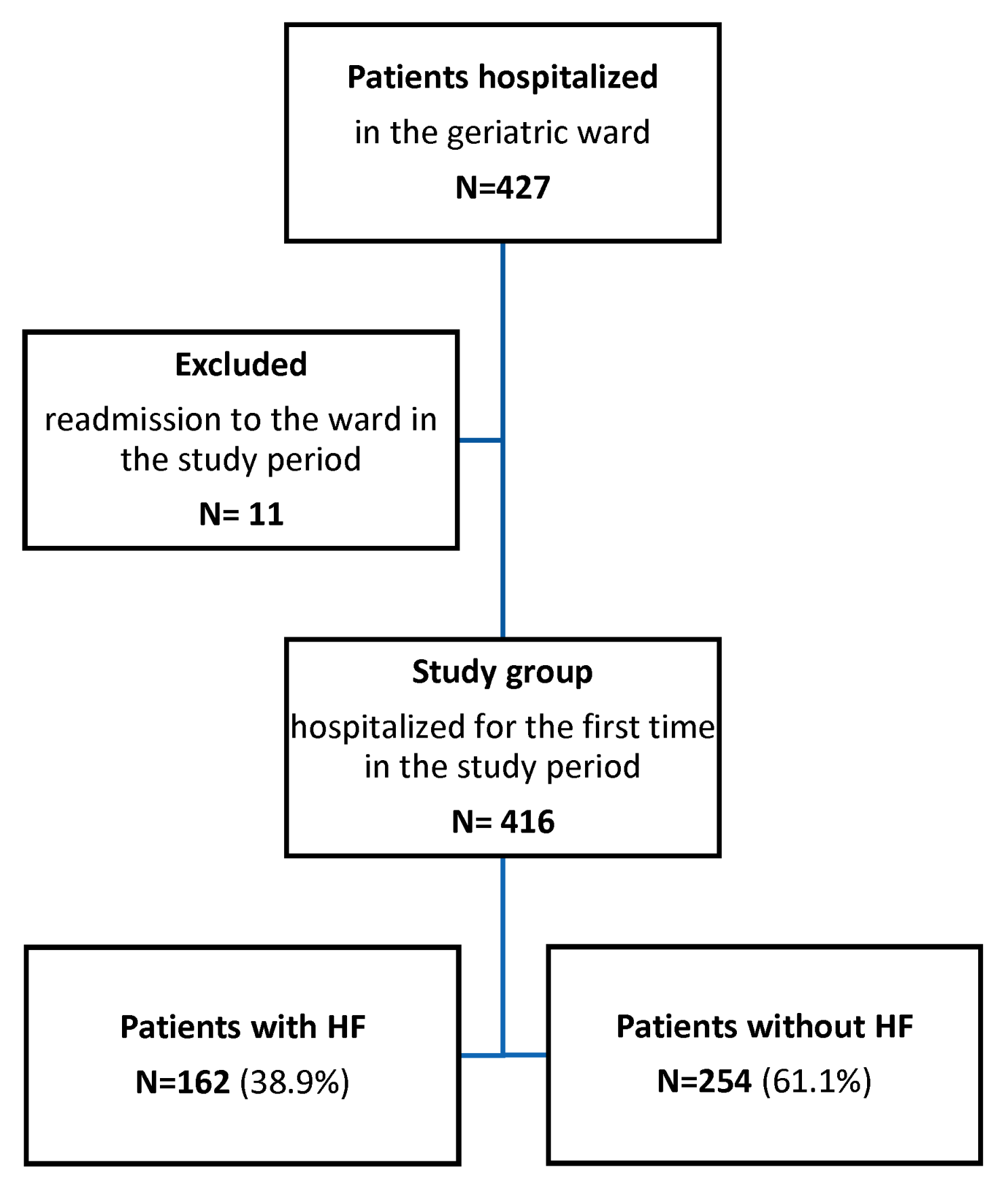
| No. (%) of patients | 416 (100.0) | 162 (38.9) | 254 (61.1) | ||
| Age, y, Me (IQR) | 82 (77.0–86.0) | 83 (78.0–87.0) | 82 (76.0–85.0) | 0.001 | - |
| Age, 75+, n (%) | 350 (84.1) | 147 (90.7) | 203 (79.9) | 0.004 | - |
| Sex, men, n (%) | 94 (22.6) | 45 (27.8) | 49 (19.3) | 0.05 | - |
| Place of residence, rural, n (%) | 87 (20.9) | 36 (22.2) | 51 (20.1) | 0.62 | |
| Living alone, n (%) | 119 (29.8) | 36 (23.5) | 83 (33.7) | 0.03 | 17 |
| Number of chronic diseases b, Me (IQR) | 5.0 (3.0–6.0) | 6.0 (5.0–7.0) | 4.0 (3.0–5.0) | <0.001 | - |
| Multimorbidity c, n (%) | 239 (57.5) | 143 (88.3) | 96 (37.8) | <0.001 | - |
| Number of drugs, Me (IQR) | 7.0 (5.0–9.0) | 8.0 (6.0–10.0) | 6.0 (4.0–9.0) | <0.001 | 9 |
| Polypharmacy d, n (%) | 322 (79.1) | 144 (90.0) | 178 (72.1) | 0.001 | 9 |
| Hospitalization in the last year, n (%) | 122 (29.5) | 63 (39.4) | 59 (23.3) | 0.001 | 3 |
| AMTS, Me (IQR) | 8.0 (6.0–9.0) | 8.0 (6.0–9.0) | 8.0 (6.0–9.0) | 0.54 | 35 |
| Dementia, n (%) | 133 (32.0) | 44 (27.2) | 89 (35.0) | 0.11 | - |
| GDS, Me (IQR) | 7.0 (3.0–10.0) | 7.0 (4.0–10.0) | 6.0 (3.0–10.0) | 0.47 | 52 |
| Depression, n (%) | 181 (56.9) | 73 (59.8) | 108 (55.1) | 0.42 | 98 |
| Hypertension, n (%) | 327 (78.6) | 133 (82.1) | 194 (76.4) | 0.18 | - |
| Ischemic heart disease, n (%) | 223 (53.6) | 108 (66.7) | 115 (45.3) | <0.001 | - |
| Myocardial infarction, n (%) | 39 (9.4) | 32 (19.8) | 7 (2.8) | <0.001 | - |
| Atrial fibrillation, n (%) | 98 (23.6) | 71 (43.8) | 27 (10.6) | <0.001 | - |
| Peripheral arterial disease, n (%) | 64 (15.4) | 42 (25.9) | 22 (8.7) | <0.001 | - |
| Stroke/TIA, n (%) | 56 (13.5) | 29 (17.9) | 27 (10.6) | 0.04 | - |
| Diabetes | 126 (30.3) | 63 (38.9) | 63 (24.8) | 0.003 | - |
| Chronic osteoarthritis, n (%) | 324 (77.9) | 132 (81.5) | 192 (75.6) | 0.18 | - |
| COPD/asthma | 42 (10.1) | 21 (13.0) | 21 (8.3) | 0.14 | |
| Systolic BP at admittance, mmHg, Me (IQR) | 130 (120–140) | 125 (110–140) | 130 (120–140) | <0.001 | 7 |
| Diastolic BP at admittance, mmHg, Me (IQR) | 70 (60–80) | 70 (60–80) | 70 (65–80) | 0.02 | 7 |
| Pulse pressure at admittance, mmHg, Me (IQR) | 60 (50–65) | 55 (47.25–60) | 60 (50–70) | 0.007 | 7 |
| High pulse pressure (>50 mmHg) | 248 (60.6) | 88 (55.0) | 160 (64.3) | 0.06 | 7 |
| Orthostatic hypotension, n (%) | 57 (16.1) | 22 (16.4) | 35 (16.0) | 1.0 | 63 |
| Creatinine, mg/dL Me (IQR) | 0.98 (0.84–1.19) | 1.06 (0.9–1.34) | 0.92 (0.80–1.09) | <0.001 | 11 |
| GFR e, ml/min/1.73 m2, M (SD) | 58.1 (17.0) | 52.4 (16.3) | 61.8 (16.5) | <0.001 | 11 |
| GFR < 60 ml/min/1.73 m2, n (%) | 218 (52.4) | 109 (67.3) | 109 (42.9) | <0.001 | 11 |
| GFR < 30 ml/min/1.73 m2, n (%) | 21 (5.2) | 14 (8.9) | 7 (2.8) | 0.01 | 11 |
| Albumin < 35g/L, n (%) | 58 (14.9) | 22 (14.2) | 36 (15.4) | 0.77 | 27 |
| HAS-BLED ≥ 3, n (%) | 63 (15.2) | 42 (26.1) | 21 (8.3) | <0.001 | - |
| CHA2DS2-VASc > 3, n (%) | 399 (96.4) | 161 (100%) | 238 (94.1) | 0.001 | - |
| Total cholesterol, mmol/L, M (SD) | 4.70 (1.25) | 4.46 (1.25) | 4.86 (1.22) | 0.002 | 27 |
| Triglycerides, mmol/L, Me (IQR) | 11.54 (8.69–14.89) | 12.34 (8.80–15.66) | 10.97 (8.46–14.74) | 0.14 | 102 |
| Hemoglobin, g/dL, Me (IQR) | 12.6 (11.5–13.7) | 12.4 (11.2–13.7) | 12.7 (11.7–13.7) | 0.25 | 12 |
| Anemia, n (%) | 177 (43.8) | 80 (50.3) | 97 (39.6) | 0.04 | 12 |
| Iron, μg/dL, Me (IQR) | 67 (46.0–88) | 68 (41.50–83.0) | 67 (51.5–96.5) | 0.17 | 241 |
| Statins, n (%) | 142 (35.0) | 60 (37.5) | 82 (33.3) | 0.40 | 10 |
| ß-blockers, n (%) | 258 (63.5) | 123 (76.9) | 135 (54.9) | <0.001 | 10 |
| α1-blockers, n (%) | 25 (6.2) | 16 (10.0) | 9 (3.7) | 0.01 | 10 |
| Calcium channel blockers, n (%) | 114 (28.1) | 53 (33.1) | 61 (24.8) | 0.07 | 10 |
| Digoxin, n (%) | 30 (7.4) | 22 (13.8) | 8 (3.3) | <0.001 | 10 |
| Antiarrhythmics, n (%) | 9 (2.2) | 4 (2.5) | 5 (2.0) | 0.74 | 10 |
| ACEI or ARB, n (%) | 259 (63.8) | 116 (72.5) | 143 (58.1) | 0.004 | 10 |
| Cholecalciferol, n (%) | 88 (21.7) | 34 (21.3) | 54 (22.0) | 0.90 | 10 |
| Oral anticoagulants (VKA or NOAC), n (%) | 64 (15.4) | 50 (30.9) | 14 (5.5) | <0.001 | 10 |
| Diuretics, n (%) | 196 (48.3) | 103 (64.4) | 93 (37.8) | <0.001 | 10 |
| Thiazides, n (%) | 83 (20.4) | 25 (15.6) | 58 (23.6) | 0.06 | 10 |
| Loop diuretics, n (%) | 100 (24.6) | 70 (43.8) | 30 (12.2) | <0.001 | 10 |
| ARA (spironolactone, eplerenone), n (%) | 71 (17.5) | 53 (33.1) | 18 (7.3) | <0.001 | 10 |
| Parameter | Total | HF + Group | HF− Group | p Values a | Missing Data |
|---|---|---|---|---|---|
| No. (%) of patients | 416 (100.0) | 162 (38.9) | 254 (61.1) | ||
| BMI, kg/m2, M (SD) | 29.3 (6.0) | 30.7 (6.2) | 28.4 (5.7) | <0.001 | 62 |
| BMI < 24 kg/m2, n (%) | 66 (18.6) | 22 (16.4) | 44 (20.0) | 0.48 | 62 |
| Obesity (BMI > 30 kg/m2), n (%) | 148 (41.8) | 72 (53.7) | 76 (34.5) | 0.001 | 62 |
| WHR, Me (IQR) | 0.91 (0.87–0.95) | 0.91 (0.87–0.96) | 0.91 (0.86–0.95) | 0.35 | 63 |
| Abdominal obesity 1st grade b, n (%) | 295 (81.0) | 127 (80.8) | 168 (77.8) | 0.06 | 63 |
| Abdominal obesity 2nd grade c, n (%) | 233 (64.0) | 103 (69.6) | 130 (60.2) | 0.08 | 63 |
| MNA-SF, Me (IQR) | 12.0 (9.0–13.0) | 11.0 (9.0–13.0) | 12.0 (9.0–13.0) | 0.78 | 12 |
| MNA SF < 12 (malnutrition risk), n (%) | 198 (49.0) | 80 (50.3) | 118 (48.2) | 0.69 | 12 |
| MNA SF < 8 (malnutrition), n (%) | 72 (17.8) | 24 (19.7) | 48 (17.0) | 0.60 | 12 |
| MAC, cm, M (SD) | 28.0 (4.0) | 28.7 (4.0) | 27.6 (3.9) | 0.01 | 49 |
| MAC ≤ 22cm, n (%) | 89 (24.3) | 29 (19.6) | 60 (27.4) | 0.11 | 49 |
| CC, cm, M (SD) | 34.4 (4.6) | 35.6 (4.9) | 33.6 (4.3) | <0.001 | 51 |
| CC < 31 cm, n (%) | 74 (20.3) | 24 (16.4) | 50 (22.8) | 0.15 | 51 |
| Handgrip, kg, Me (IQR) | 18.15 (13.7–22.8) | 16.7 (12.9–22.0) | 18.9 (14.2–23.2) | 0.04 | 66 |
| women | 16.7 (12.9–20.5) | 15.2 (11.6–18.9) | 18.0 (13.5–21.5) | 0.002 | |
| men | 26 (21–32.3) | 26.1 (20.5–32.3) | 25.9 (21.0–32.4) | 0.98 | |
| Low strength d, n (%) | 164 (46.9) | 73 (54.9) | 91 (41.9) | 0.02 | 66 |
| women | 124 (45.3) | 55 (55.0) | 69 (39.7) | 0.02 | |
| men | 40 (52.6) | 18 (54.5) | 22 (51.2) | 0.82 | |
| Weakness e, n (%) | 233 (66.6) | 101 (75.9) | 132 (60.8) | 0.004 | 66 |
| Gait speed, m/s, Me (IQR) | 0.65 (0.40–0.96) | 0.53 (0.35–0.89) | 0.68 (0.44–0.99) | 0.02 | 102 |
| Slowness e, n (%) | 166 (52.9) | 68 (59.1) | 98 (49.2) | 0.10 | 102 |
| Gait speed ≤ 0.8 m/s d, n (%) | 205 (65.3) | 79 (68.7) | 126 (63.3) | 0.39 | 102 |
| Gait speed ≤ 0.8 m/s or immobile, n (%) | 238 (68.6) | 97 (72.9) | 141 (65.9) | 0.19 | |
| CFS, Me (IQR) | 5.0 (4.0–5.0) | 5.0 (4.0–6.0) | 4.0 (4.0–5.0) | <0.001 | - |
| Frailty, n (%) | 230 (55.3) | 106 (65.4) | 124 (48.8) | 0.001 | - |
| Severe frailty e, n (%) | 102 (24.5) | 50 (30.9) | 52 (20.5) | 0.02 | - |
| Barthel Index, Me (IQR) | 90.0 (70.0–100.0) | 85.0 (65.0–95.0) | 95.0 (70.0–100.0) | 0.01 | 6 |
| Duke OARS IADL, Me (IQR) | 7.0 (3.0–11.0) | 6.0 (2.0–9.0) | 8.0 (4.0–11.0) | 0.01 | 10 |
| POMA, Me (IQR) | 23.0 (17.0–28.0) | 21.0 (16.0–28.0) | 24.0 (18.0–28.0) | 0.02 | 94 |
| POMA < 24, n (%) | 181 (56.2) | 76 (63.3) | 105 (52.0) | 0.049 | 94 |
| TUG, s, Me (IQR) | 17.4 (11.87–28.0) | 21.5 (12.6–52.1) | 16.4 (11.5–24.1) | 0.005 | 115 |
| TUG ≥ 14 s, n (%) | 195 (64.8) | 83 (72.8) | 112 (59.9) | 0.03 | 115 |
| TUG ≥ 20 s, n (%) | 128 (42.5) | 61 (53.5) | 67 (35.8) | 0.004 | 115 |
| Norton scale, Me (IQR) | 17 (15-19) | 17 (15-19) | 18 (15-19) | 0.049 | 6 |
| Pressure sores at admission, n (%) | 18 (4.4) | 13 (8.0) | 5 (2.0) | 0.005 | 5 |
| Falls in the last 12 months, n (%) | 157 (43.9) | 66 (48.9) | 91 (40.8) | 0.15 | 58 |
| Non-active in SGPALS, n (%) | 168 (41.0) | 86 (54.4) | 82 (32.5) | <0.001 | 6 |
| Model 1 | Model 2 | Model 3 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | OR | 95% CI | p Value | |
| Age | 1.07 | 1.02–1.12 | 0.008 | 1.07 | 1.02–1.12 | 0.005 | 1.06 | 1.004–1.12 | 0.04 |
| Sex (male) | 2.06 | 0.99–4.29 | 0.053 | 1.89 | 0.99–3.64 | 0.055 | 1.22 | 0.56–2.65 | 0.61 |
| MNA-SF | 0.99 | 0.88–1.11 | 0.862 | ||||||
| Gait speed | 0.78 | 0.30–2.06 | 0.621 | ||||||
| SP | 1.87 | 1.03–3.40 | 0.041 | 1.97 | 1.11–3.50 | 0.021 | 1.94 | 1.01–3.73 | 0.045 |
| MAC | 0.90 | 0.79–1.02 | 0.106 | 0.89 | 0.79–1.01 | 0.077 | 0.83 | 0.72–0.96 | 0.012 |
| CC | 1.15 | 1.04–1.27 | 0.007 | 1.15 | 1.04–1.27 | 0.005 | 1.18 | 1.05–1.32 | 0.006 |
| BMI | 1.12 | 0.99–1.24 | 0.08 | 1.10 | 1.01–1.19 | 0.034 | 1.12 | 1.02–1.24 | 0.020 |
| Waist circumference | 0.99 | 0.95–1.03 | 0.73 | ||||||
| Peripheral arterial disease | 1.88 | 0.80–4.45 | 0.149 | ||||||
| History of stroke/TIA | 1.89 | 0.72–4.98 | 0.195 | ||||||
| Ischaemic heart disease | 3.32 | 1.71–6.46 | <0.001 | ||||||
| Atrial fibrillation | 9.07 | 4.04–20.38 | <0.001 | ||||||
| Diabetes mellitus | 0.79 | 0.37–1.65 | 0.527 | ||||||
| Negelkerk’s R2 | 0.208 | 0.200 | 0.419 | ||||||
| % correctly predicted | 68.7% | 67.2% | 77.1% | ||||||
| sensitivity | 46.6% | 43.7% | 62.1% | ||||||
| specificity | 83.0% | 82.4% | 86.8% | ||||||
| Hosmer–Lemeshow goodness of fit | 0.799 | 0.447 | 0.208 | ||||||
| Regression method | Enter method | Backward analysis of Model 1 | Enter method (Model 2 and diseases correlating with HF) | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Charkiewicz, M.; Wojszel, Z.B.; Kasiukiewicz, A.; Magnuszewski, L.; Wojszel, A. Association of Chronic Heart Failure with Frailty, Malnutrition, and Sarcopenia Parameters in Older Patients—A Cross-Sectional Study in a Geriatric Ward. J. Clin. Med. 2023, 12, 2305. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12062305
Charkiewicz M, Wojszel ZB, Kasiukiewicz A, Magnuszewski L, Wojszel A. Association of Chronic Heart Failure with Frailty, Malnutrition, and Sarcopenia Parameters in Older Patients—A Cross-Sectional Study in a Geriatric Ward. Journal of Clinical Medicine. 2023; 12(6):2305. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12062305
Chicago/Turabian StyleCharkiewicz, Miroslaw, Zyta Beata Wojszel, Agnieszka Kasiukiewicz, Lukasz Magnuszewski, and Aleksandra Wojszel. 2023. "Association of Chronic Heart Failure with Frailty, Malnutrition, and Sarcopenia Parameters in Older Patients—A Cross-Sectional Study in a Geriatric Ward" Journal of Clinical Medicine 12, no. 6: 2305. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12062305