

Connection between Cardiac Fibrosis Biomarkers and Echocardiography Parameters in Advanced Chronic Kidney Disease Patients
 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
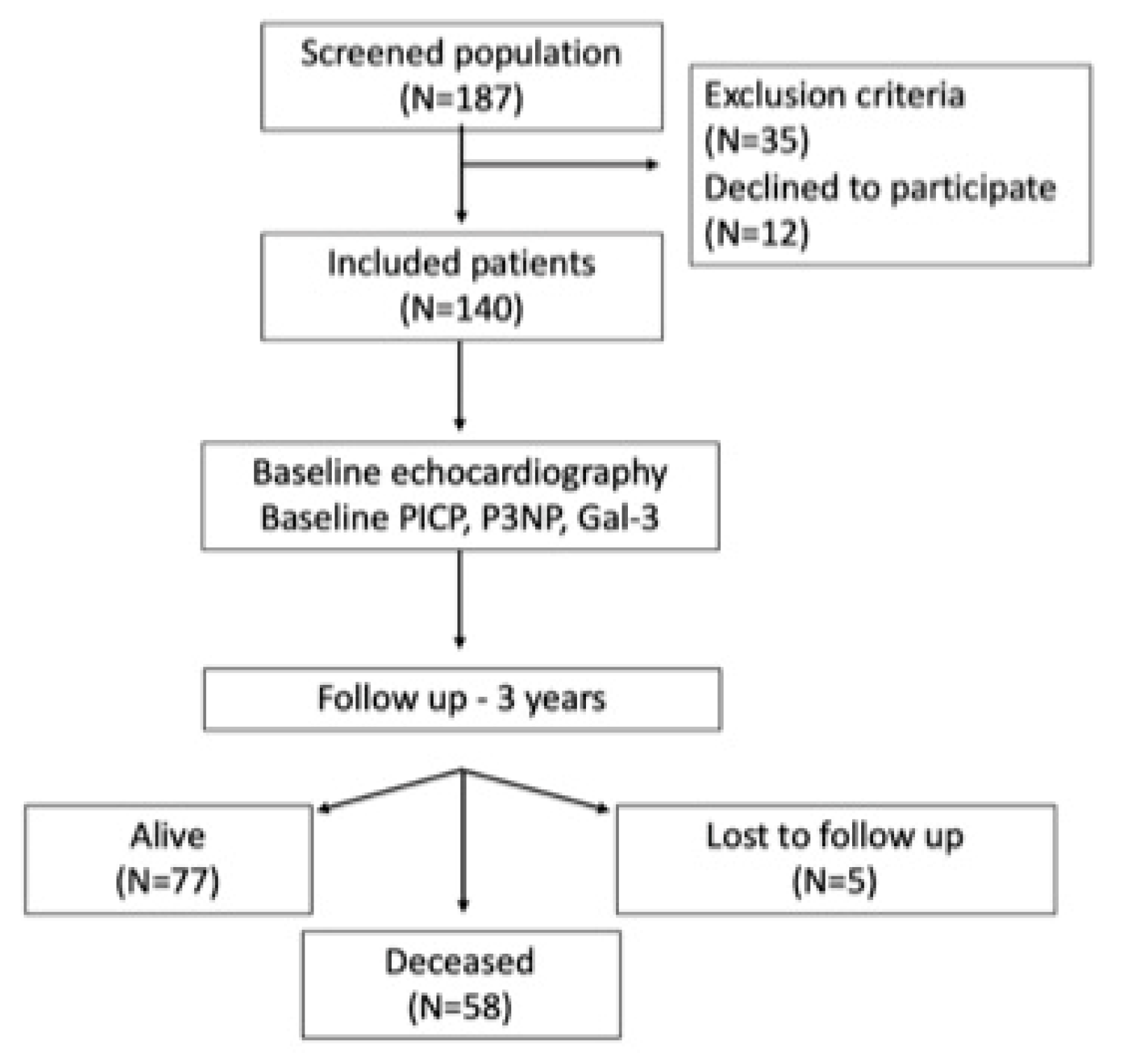
2.1. Study Population
2.2. Study Design
2.3. Transthoracic Echocardiography
2.4. Determination of Serum Biomarkers
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Echocardiographic Parameters
3.3. Serum Biomarkers
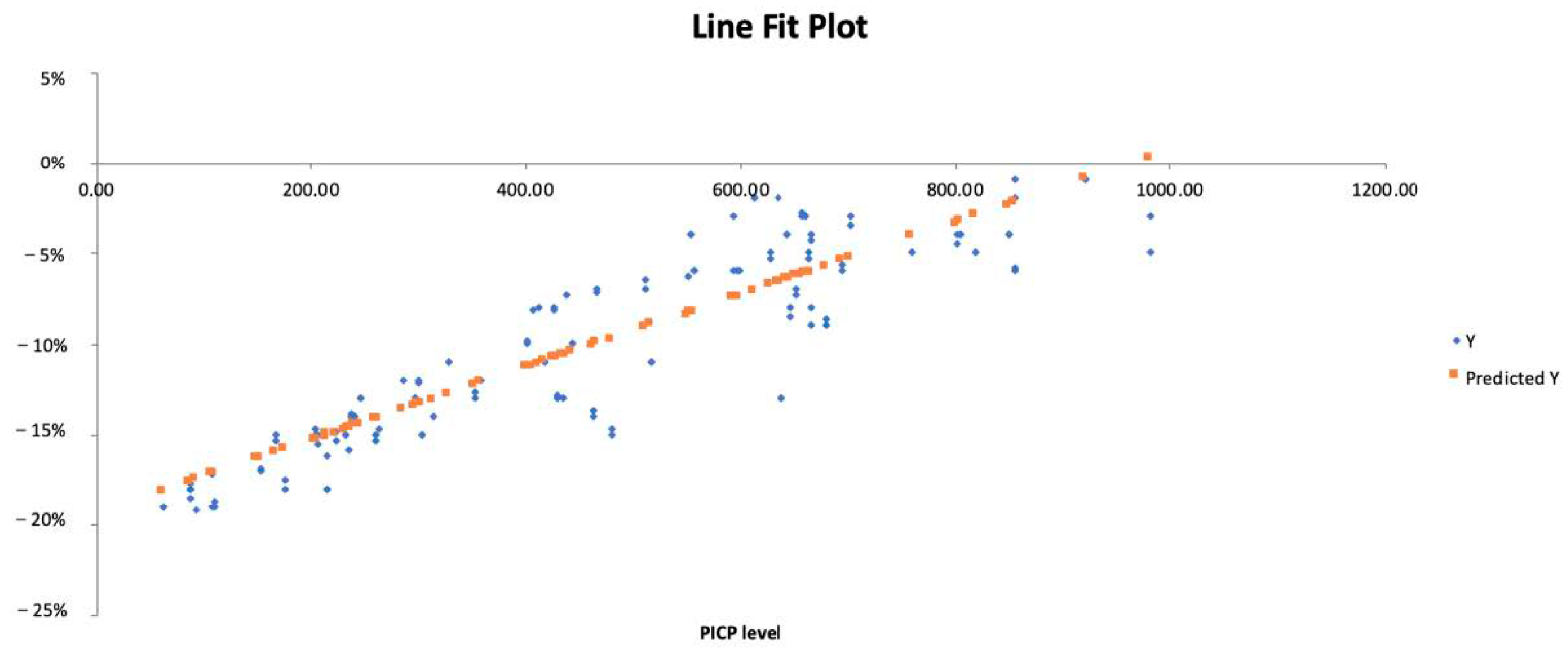
3.4. Regression Analysis
3.5. Subgroup Analysis by Diabetes and Smoking Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jankowski, J.; Floege, J.; Fliser, D.; Böhm, M.; Marx, N. Cardiovascular Disease in Chronic Kidney Disease: Pathophysiological Insights and Therapeutic Options. Circulation 2021, 143, 1157–1172. [Google Scholar] [CrossRef]
- House, A.A.; Wanner, C.; Sarnak, M.J.; Piña, I.L.; McIntyre, C.W.; Komenda, P.; Kasiske, B.L.; Deswal, A.; Defilippi, C.R.; Cleland, J.G.F.; et al. Heart failure in chronic kidney disease: Conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2019, 95, 1304–1317. [Google Scholar] [CrossRef]
- Ortiz, A.; Covic, A.; Fliser, D.; Fouque, D.; Goldsmith, D.; Kanbay, M.; Mallamaci, F.; Massy, Z.A.; Rossignol, P.; Vanholder, R.; et al. Board of the EURECA-m Working Group of ERA-EDTA. Epidemiology, contributors to, and clinical trials of mortality risk in chronic kidney failure. Lancet 2014, 383, 1831–1843. [Google Scholar] [CrossRef]
- Tonelli, M.; Karumanchi, S.A.; Thadhani, R. Epidemiology and Mechanisms of Uremia-Related Cardiovascular Disease. Circulation 2016, 133, 518–536. [Google Scholar] [CrossRef]
- Hinderer, S.; Schenke-Layland, K. Cardiac fibrosis—A short review of causes and therapeutic strategies. Adv. Drug Deliv. Rev. 2019, 146, 77–82. [Google Scholar] [CrossRef]
- Jiang, W.; Xiong, Y.; Li, X.; Yang, Y. Cardiac Fibrosis: Cellular Effectors, Molecular Pathways, and Exosomal Roles. Front. Cardiovasc. Med. 2021, 8, 715258. [Google Scholar] [CrossRef]
- Rutherford, E.; Talle, M.A.; Mangion, K.; Bell, E.; Rauhalammi, S.M.; Roditi, G.; McComb, C.; Radjenovic, A.; Welsh, P.; Woodward, R.; et al. Defining myocardial tissue abnormalities in end-stage renal failure with cardiac magnetic resonance imaging using native T1 mapping. Kidney Int. 2016, 90, 845–852. [Google Scholar] [CrossRef]
- Hensen, L.C.; Goossens, K.; Podlesnikar, T.; Rotmans, J.I.; Jukema, J.W.; Delgado, V.; Bax, J.J. Left Ventricular Mechanical Dispersion and Global Longitudinal Strain and Ventricular Arrhythmias in Predialysis and Dialysis Patients. J. Am. Soc. Echocardiogr. 2018, 31, 777–783. [Google Scholar] [CrossRef]
- Hensen, L.C.R.; Goossens, K.; Delgado, V.; Abou, R.; Rotmans, J.I.; Jukema, J.W.; Bax, J.J. Prevalence of left ventricular systolic dysfunction in pre-dialysis and dialysis patients with preserved left ventricular ejection fraction. Eur. J. Heart Fail. 2018, 20, 560–568. [Google Scholar] [CrossRef]
- Hensen, L.C.R.; Goossens, K.; Delgado, V.; Rotmans, J.I.; Jukema, J.W.; Bax, J.J. Prognostic Implications of Left Ventricular Global Longitudinal Strain in Predialysis and Dialysis Patients. Am. J. Cardiol. 2017, 120, 500–504. [Google Scholar] [CrossRef]
- Valocikova, I.; Vachalcova, M.; Valocik, G.; Kurecko, M.; Dvoroznakova, M.; Mitro, P.; Cocherova, J.; Bujnakova, S.B.; Holoubek, D. Incremental value of global longitudinal strain in prediction of all-cause mortality in predialysis and dialysis chronic kidney disease patients. Wien. Klin. Wochenschr. 2016, 128, 495–503. [Google Scholar] [CrossRef]
- Ding, Y.; Wang, Y.; Zhang, W.; Jia, Q.; Wang, X.; Li, Y.; Lv, S.; Zhang, J. Roles of Biomarkers in Myocardial Fibrosis. Aging Dis. 2020, 11, 1157–1174. [Google Scholar] [CrossRef]
- Hara, A.; Niwa, M.; Kanayama, T.; Noguchi, K.; Niwa, A.; Matsuo, M.; Kuroda, T.; Hatano, Y.; Okada, H.; Tomita, H. Galectin-3: A Potential Prognostic and Diagnostic Marker for Heart Disease and Detection of Early Stage Pathology. Biomolecules 2020, 10, 1277. [Google Scholar] [CrossRef]
- Dupuy, A.M.; Kuster, N.; Curinier, C.; Huet, F.; Plawecki, M.; Solecki, K.; Roubille, F.; Cristol, J.P. Exploring collagen remodeling and regulation as prognosis biomarkers in stable heart failure. Clin. Chim. Acta 2019, 490, 167–171. [Google Scholar] [CrossRef]
- Lopez-Andrès, N.; Rossignol, P.; Iraqi, W.; Fay, R.; Nuée, J.; Ghio, S.; Cleland, J.G.F.; Zannad, F.; Lacolley, P. Association of galectin-3 and fibrosis markers with long-term cardiovascular outcomes in patients with heart failure, left ventricular dysfunction, and dyssynchrony: Insights from the CARE-HF (Cardiac Resynchronization in Heart Failure) trial. Eur. J. Heart Fail. 2012, 14, 74–81. [Google Scholar] [CrossRef]
- Ureche, C.; Nedelcu, A.E.; Sascău, R.A.; Stătescu, C.; Kanbay, M.; Covic, A. Role of collagen turnover biomarkers in the noninvasive assessment of myocardial fibrosis: An update. Biomark. Med. 2020, 14, 1265–1275. [Google Scholar] [CrossRef]
- Pellicori, P.; Ferreira, J.P.; Mariottoni, B.; Brunner-La Rocca, H.P.; Ahmed, F.Z.; Verdonschot, J.; Collier, T.; Cuthbert, J.J.; Petutschnigg, J.; Mujaj, B.; et al. Effects of spironolactone on serum markers of fibrosis in people at high risk of developing heart failure: Rationale, design and baseline characteristics of a proof-of-concept, randomised, precision-medicine, prevention trial. The Heart OMics in AGing (HOMAGE) trial. Eur. J. Heart Fail. 2020, 22, 1711–1723. [Google Scholar]
- Zile, M.R.; Jhund, P.S.; Baicu, C.F.; Claggett, B.L.; Pieske, B.; Voors, A.A.; Prescott, M.F.; Shi, V.; Lefkowitz, M.; McMurray, J.J.V.; et al. Plasma Biomarkers Reflecting Profibrotic Processes in Heart Failure With a Preserved Ejection Fraction: Data From the Prospective Comparison of ARNI With ARB on Management of Heart Failure With Preserved Ejection Fraction Study. Circ. Heart Fail. 2016, 9, e002551. [Google Scholar] [CrossRef]
- Zhang, W.R.; Parikh, C.R. Biomarkers of Acute and Chronic Kidney Disease. Annu. Rev. Physiol. 2019, 81, 309–333. [Google Scholar] [CrossRef]
- Stein, N.R.; Zelnick, L.R.; Anderson, A.H.; Christenson, R.H.; deFilippi, C.R.; Deo, R.; Go, A.S.; He, J.; Ky, B.; Lash, J.P.; et al. Associations Between Cardiac Biomarkers and Cardiac Structure and Function in CKD. Kidney Int. Rep. 2020, 5, 1052–1060. [Google Scholar] [CrossRef]
- Ureche, C.; Dodi, G.; Tapoi, L.; Ailoaei, S.; Nedelcu, A.; Sascau, R.; Statescu, C.; Covic, A. Association between global longitudinal strain and myocardial fibrosis biomarkers in patients with end-stage chronic kidney disease. Eur. Heart J. 2022, 43, ehac544.2609. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 233–271. [Google Scholar] [CrossRef]
- Nagata, Y.; Takeuchi, M.; Mizukoshi, K.; Wu, V.C.; Lin, F.C.; Negishi, K.; Nakatani, S.; Otsuji, Y. Intervendor variability of two-dimensional strain using vendor-specific and vendor-independent software. J. Am. Soc. Echocardiogr. 2015, 28, 630–641. [Google Scholar] [CrossRef]
- Banerjee, T.; Mukherjee, S.; Ghosh, S.; Biswas, M.; Dutta, S.; Pattari, S.; Chatterjee, S.; Bandyopadhyay, A. Clinical significance of markers of collagen metabolism in rheumatic mitral valve disease. PLoS ONE 2014, 9, e90527. [Google Scholar] [CrossRef]
- Khan, S.; Subedi, D.; Chowdhury, M.M. Use of amino terminal type III procollagen peptide (P3NP) assay in methotrexate therapy for psoriasis. Postgrad. Med. J. 2006, 82, 353–354. [Google Scholar] [CrossRef]
- Hogas, S.; Bilha, S.C.; Branisteanu, D.; Hogas, M.; Gaipov, A.; Kanbay, M.; Covic, A. Potential novel biomarkers of cardiovascular dysfunction and disease: Cardiotrophin-1, adipokines and galectin-3. Arch. Med. Sci. 2017, 13, 897–913. [Google Scholar] [CrossRef]
- Kim, M.K.; Kim, B.; Lee, J.Y.; Kim, J.S.; Han, B.G.; Choi, S.O.; Yang, J.W. Tissue Doppler-derived E/e′ ratio as a parameter for assessing diastolic heart failure and as a predictor of mortality in patients with chronic kidney disease. Korean J. Intern. Med. 2013, 28, 35–44. [Google Scholar] [CrossRef]
- Demir, S.; Ede, H.; Kaplan, M.; Yavuz, F.; Yucel, C.; Kurt, I.H. The novel diagnostic marker in low-LVEF heart failure patients. Bratisl. Med. J. 2018, 119, 421–424. [Google Scholar] [CrossRef]
- Luneva, E.B.; Vasileva, A.A.; Karelkina, E.V.; Boyarinova, M.A.; Mikhaylov, E.N.; Ryzhkov, A.V.; Babenko, A.Y.; Konradi, A.O.; Moiseeva, O.M. Simple Predictors for Cardiac Fibrosis in Patients with Type 2 Diabetes Mellitus: The Role of Circulating Biomarkers and Pulse Wave Velocity. J. Clin. Med. 2022, 11, 2843. [Google Scholar] [CrossRef]
- Duprez, D.A.; Gross, M.D.; Kizer, J.R.; Ix, J.H.; Hundley, W.G.; Jacobs, D.R., Jr. Predictive Value of Collagen Biomarkers for Heart Failure With and Without Preserved Ejection Fraction: MESA (Multi-Ethnic Study of Atherosclerosis). J. Am. Heart Assoc. 2018, 7, e007885. [Google Scholar] [CrossRef]
- Kobayashi, M.; Girerd, N.; Ferreira, J.P.; Kevin, D.; Huttin, O.; González, A.; Bozec, E.; Clark, A.L.; Cosmi, F.; Cuthbert, J.; et al. The association between markers of type I collagen synthesis and echocardiographic response to spironolactone in patients at risk of heart failure: Findings from the HOMAGE trial. Eur. J. Heart Fail. 2022, 24, 1559–1568. [Google Scholar] [CrossRef]
- Eiros, R.; Romero-González, G.; Gavira, J.J.; Beloqui, O.; Colina, I.; Landecho, M.F.; López, B.; González, A.; Díez, J.; Ravassa, S. Does Chronic Kidney Disease Facilitate Malignant Myocardial Fibrosis in Heart Failure with Preserved Ejection Fraction of Hypertensive Origin? J. Clin. Med. 2020, 9, 404. [Google Scholar] [CrossRef]
- Su, C.T.; Liu, Y.W.; Lin, J.W.; Chen, S.I.; Yang, C.S.; Chen, J.H.; Hung, K.-Y.; Tsai, W.-C.; Huang, J.-W. Increased procollagen type I C-terminal peptide levels indicate diastolic dysfunction in end-stage renal disease patients undergoing maintenance dialysis therapy. J. Am. Soc. Echocardiogr. 2012, 25, 895–901. [Google Scholar] [CrossRef]
- Ureche, C.; Dodi, G.; Șerban, A.M.; Covic, A.S.; Voroneanu, L.; Hogaș, S.; Sascău, R.A.; Stătescu, C.; Covic, A. Predictive Value of Collagen Biomarkers in Advanced Chronic Kidney Disease Patients. Biomolecules 2023, 13, 389. [Google Scholar] [CrossRef]
- Lieb, W.; Song, R.J.; Xanthakis, V.; Vasan, R.S. Association of Circulating Tissue Inhibitor of Metalloproteinases-1 and Procollagen Type III Aminoterminal Peptide Levels With Incident Heart Failure and Chronic Kidney Disease. J. Am. Heart Assoc. 2019, 8, e011426. [Google Scholar] [CrossRef]
- Ghoul, B.E.; Squalli, T.; Servais, A.; Elie, C.; Meas-Yedid, V.; Trivint, C.; Vanmassenhove, J.; Grünfeld, J.-P.; Olivo-Marin, J.-C.; Thervet, E.; et al. Urinary procollagen III aminoterminal propeptide (PIIINP): A fibrotest for the nephrologist. Clin. J. Am. Soc. Nephrol. 2010, 5, 205–210. [Google Scholar] [CrossRef]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2013, 62, e147–e239. [Google Scholar] [CrossRef]
- Obokata, M.; Sunaga, H.; Ishida, H.; Ito, K.; Ogawa, T.; Ando, Y.; Kurabayashi, M.; Negishi, K. Independent and incremental prognostic value of novel cardiac biomarkers in chronic hemodialysis patients. Am. Heart J. 2016, 179, 29–41. [Google Scholar] [CrossRef]
- Rebholz, C.M.; Selvin, E.; Liang, M.; Ballantyne, C.M.; Hoogeveen, R.C.; Aguilar, D.; McEvoy, J.W.; Grams, M.E.; Coresh, J. Plasma galectin-3 levels are associated with the risk of incident chronic kidney disease. Kidney Int. 2018, 93, 252–259. [Google Scholar] [CrossRef]
- Salib, M.; Girerd, S.; Girerd, N.; März, W.; Scharnagl, H.; Massy, Z.A.; Leroy, C.; Duarte, K.; Holdaas, H.; Jardine, A.G.; et al. Serum markers of fibrosis, cardiovascular and all-cause mortality in hemodialysis patients: The AURORA trial. Clin. Res. Cardiol. 2022, 111, 614–626. [Google Scholar] [CrossRef]
- Hogas, S.; Schiller, A.; Voroneanu, L.; Constantinescu, D.; Timar, R.; Cianga, P.; Kanbay, M.; Banach, M.; Covic, A.; Mihaescu, A.; et al. Predictive Value for Galectin 3 and Cardiotrophin 1 in Hemodialysis Patients. Angiology 2016, 67, 854–859. [Google Scholar] [CrossRef] [PubMed]
- Drechsler, C.; Delgado, G.; Wanner, C.; Blouin, K.; Pilz, S.; Tomaschitz, A.; Kleber, M.E.; Dressel, A.; Willmes, C.; Krane, V.; et al. Galectin-3, renal function, and clinical outcomes: Results from the LURIC and 4D studies. J. Am. Soc. Nephrol. 2015, 26, 2213–2221. [Google Scholar] [CrossRef] [PubMed]
- Tuegel, C.; Katz, R.; Alam, M.; Bhat, Z.; Bellovich, K.; de Boer, I.; Brosius, F.; Gadegbeku, C.; Gipson, D.; Hawkins, J.; et al. GDF-15, galectin 3, soluble ST2, and risk of mortality and cardiovascular events in CKD. Am. J. Kidney Dis. 2018, 72, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Russo, I.; Frangogiannis, N.G. Diabetes-associated cardiac fibrosis: Cellular effectors, molecular mechanisms and therapeutic opportunities. J. Mol. Cell. Cardiol. 2016, 90, 84–93. [Google Scholar] [CrossRef]
- Jin, Z.Q. MicroRNA targets and biomarker validation for diabetes-associated cardiac fibrosis. Pharmacol. Res. 2021, 174, 105941. [Google Scholar] [CrossRef]
- Boor, P.; Casper, S.; Celec, P.; Hurbánková, M.; Beno, M.; Heidland, A.; Amann, K.; Šebeková, K. Renal, vascular and cardiac fibrosis in rats exposed to passive smoking and industrial dust fibre amosite. J. Cell. Mol. Med. 2009, 13, 4484–4491. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameter (N = 140) | Value |
|---|---|
| Age (Average ± SD) | 59 ± 15 |
| Sex (Number, %) | 62 F (44.3%), 78 M (55.7%) |
| Egfr (Average ± SD) (mL/min/1.73 m2) | 8.7 ± 3.3 |
| Creatinine (Average ± SD) (mg/dL, umol/L) | 6.6 ± 2.4 (583.57 ± 212.21) |
| Mean duration of the renal disease (months) | 43.2 ± 14.5 |
| BMI (Average ± SD) (kg/m2) | 27.04 ± 5 |
| Obesity (Number, %) | 36 (25.7%) |
| Smoking (Number, %) | 23 (16.4%) |
| HTN grade (Number, %) | 11 Grade 2 (7.8%), 129 Grade 3 (92.2%) |
| Systolic blood pressure (Average ± SD) (mmHg) | 140 ± 15 |
| Diastolic blood pressure (Average ± SD) (mmHg) | 76 ± 5 |
| Heart rate (Average ± SD) (beats/minute) | 73 ± 4.8 |
| NYHA class (Number, %) | Class I (52.1%), Class II (47.9%) |
| Diabetes mellitus (Number, %) | 47 (33.5%) |
| History of MI (Number, %) | 16 (11.4%) |
| CABG/PTCA (Number, %) | 8 (5.7%) |
| Hemoglobin (Average ± SD) (g/dL) | 9.72 ± 2 |
| Uric acid (Average ± SD) (mg/dL) | 7.51 ± 2 |
| NT pro BNP (Average ± SD) (pg/mL) | 250 ± 56 |
| Mortality (Number, %) | 58 (41.4%) |
| Parameter (N = 140) | Value (Mean ± SD) |
|---|---|
| Ventricular septum width (mm) | 13.1 ± 1.8 |
| Posterior wall width (mm) | 13 ± 2.2 |
| Left ventricular end-diastolic diameter (mm) | 51 ± 5.8 |
| Left ventricular end-systolic diameter (mm) | 31.7 ± 7.4 |
| Left ventricular end-diastolic volume (mL) | 137.1 ± 46.3 |
| Left ventricular end-systolic volume (mL) | 63.6 ± 33.2 |
| Ejection fraction (%) | 53.63 ± 8 |
| Left ventricular GLS (%) | −10.2 ± 5.3 |
| Mean E/e’ | 9.8 ± 4.3 |
| Left atrial volume indexed (mL/m2) | 45.8 ± 14.2 |
| Right atrial volume (mL) | 52.7 ± 26.4 |
| TAPSE (mm) | 23.1 ± 3.8 |
| S’ velocity (cm/s) | 9.3 ± 2.6 |
| Right ventricular fractional area change (%) | 42.3 ± 5.9 |
| Inferior vena cava (mm) | 17 ± 3.5 |
| Parameter | Whole Sample (N = 140) | Normal Range (General Population) |
|---|---|---|
| GLS (%) | −10.2 ± 5.3 * | −19.4 ± 1.86 [23] |
| PICP (µg/L) | 457.2 ± 240 | 50–350 [24] |
| P3NP (µg/L) | 242 ± 199.9 | 1.2–4.2 [25] |
| Gal 3 (ng/mL) | 10.7 ± 3.7 | <17.8 ng/mL [26] |
| PICP (µg/L) | P3NP (µg/L) | Gal-3 (ng/mL) | |
|---|---|---|---|
| Ejection fraction (%) | p = 0.0002 | p = 0.01 | p = 0.02 |
| R2 = 0.69 | R2 = 0.31 | R2 = 0.35 | |
| Global longitudinal strain (%) | p = 0.00001 | p = 0.19 | p = 0.3 |
| R2 = 0.81 | R2 = 0.1 | R2 = 0.08 | |
| Mean E/e’ | p = 0.00002 | p = 0.06 | p = 0.2 |
| R2 = 0.89 | R2 = 0.3 | R2 = 0.1 | |
| LAVI (mL/m2) | p = 0.003 | p = 0.42 | p = 0.22 |
| R2 = 0.73 | R2 = 0.04 | R2 = 0.01 |
| Alive Group (n = 77) | Deceased Group (n = 58) | p Value * | |
|---|---|---|---|
| Age (Average ± SD) | 53.43 ± 15.9 | 67.47 ± 9.73 | <0.0001 |
| Sex (Number, %) | 38 F (49.3%), 39 B (50.7%) | 20 F (34.5%), 38 M (65.5%) | 0.114 |
| BMI (Average ± SD) (kg/m2) | 27.2 ± 6.05 | 24.83 ± 4.37 | 0.02 |
| Obesity (Number, %) | 22 (28.5%) | 14 (24.1%) | 0.56 |
| Smoking (Number, %) | 11 (14.3%) | 12 (20.6%) | 0.361 |
| NYHA class (Number) | 46 Class I, 31 Class II | 24 Class I, 34 Class II | 0.038 |
| Diabetes mellitus (Number, %) | 15 (19.5%) | 31 (53.4%) | <0.0001 |
| Hb (Average ± SD) (g/dL) | 9.96 ± 1.98 | 9.38 ± 1.55 | 0.06 |
| Uric acid (Average ± SD) (mg/dL) | 7.93 ± 1.7 | 6.92 ± 1.87 | 0.001 |
| Ejection fraction (%) | 54.48 ± 7.91 | 52.45 ± 8.32 | 0.146 |
| Global longitudinal strain (%) | −10.86 ± 5.6 | −9 ± 4.8 | 0.005 |
| Mean E/e’ | 9.64 ± 4.15 | 10.13 ± 4.61 | 0.5 |
| LAVI (ml/m2) | 43.69 ± 12.71 | 48.79 ± 15.7 | 0.036 |
| PICP (µg/L) | 425.08 ± 258.8 | 502.66 ± 204.43 | 0.003 |
| P3NP (µg/L) | 240.69 ± 218.13 | 244.26 ± 172.9 | 0.0001 |
| Gal 3 (ng/mL) | 10.5 ± 4.02 | 11.07 ± 3.32 | 0.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ureche, C.; Dodi, G.; Covic, A.; Nedelcu, A.; Volovăț, S.R.; Sascău, R.A.; Stătescu, C.; Covic, A. Connection between Cardiac Fibrosis Biomarkers and Echocardiography Parameters in Advanced Chronic Kidney Disease Patients. J. Clin. Med. 2023, 12, 3003. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12083003
Ureche C, Dodi G, Covic A, Nedelcu A, Volovăț SR, Sascău RA, Stătescu C, Covic A. Connection between Cardiac Fibrosis Biomarkers and Echocardiography Parameters in Advanced Chronic Kidney Disease Patients. Journal of Clinical Medicine. 2023; 12(8):3003. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12083003
Chicago/Turabian StyleUreche, Carina, Gianina Dodi, Alexandra Covic, Alina Nedelcu, Simona R. Volovăț, Radu A. Sascău, Cristian Stătescu, and Adrian Covic. 2023. "Connection between Cardiac Fibrosis Biomarkers and Echocardiography Parameters in Advanced Chronic Kidney Disease Patients" Journal of Clinical Medicine 12, no. 8: 3003. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12083003