
Advances in Imaging for Tricuspid Transcatheter Edge-to-Edge Repair: Lessons Learned and Future Perspectives
 , , , , ,
, , , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
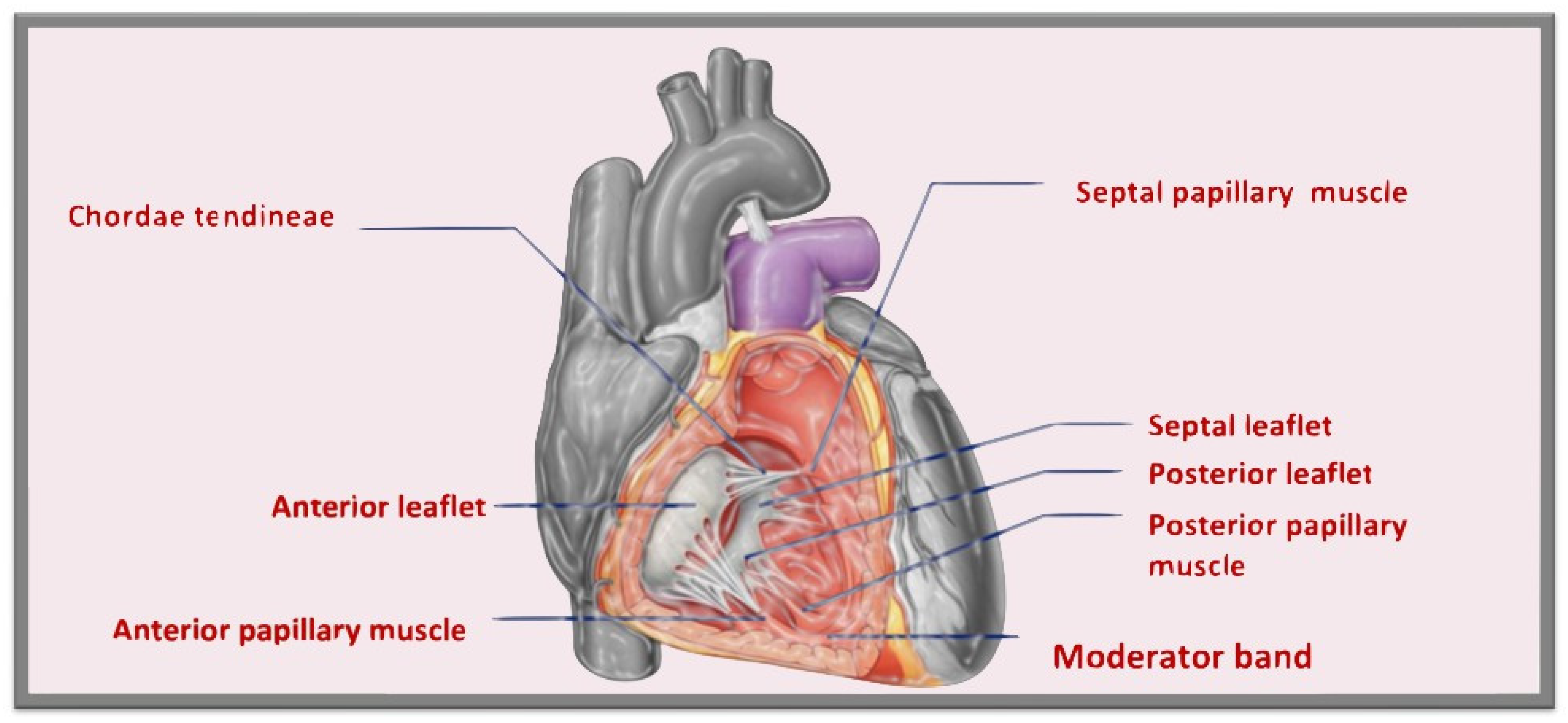
1.1. Tricuspid Valve Anatomy
1.2. Tricuspid Transcatheter Edge-to-Edge Repair
2. Pre-Procedural Evaluation for Tricuspid Transcatheter Edge-to-Edge Repair
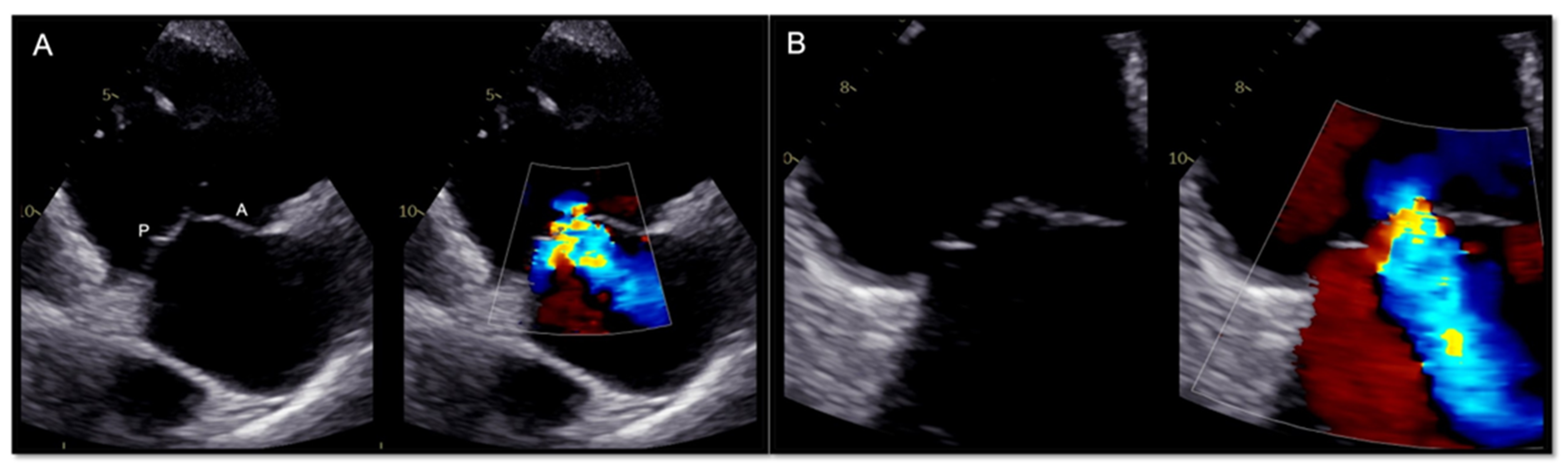
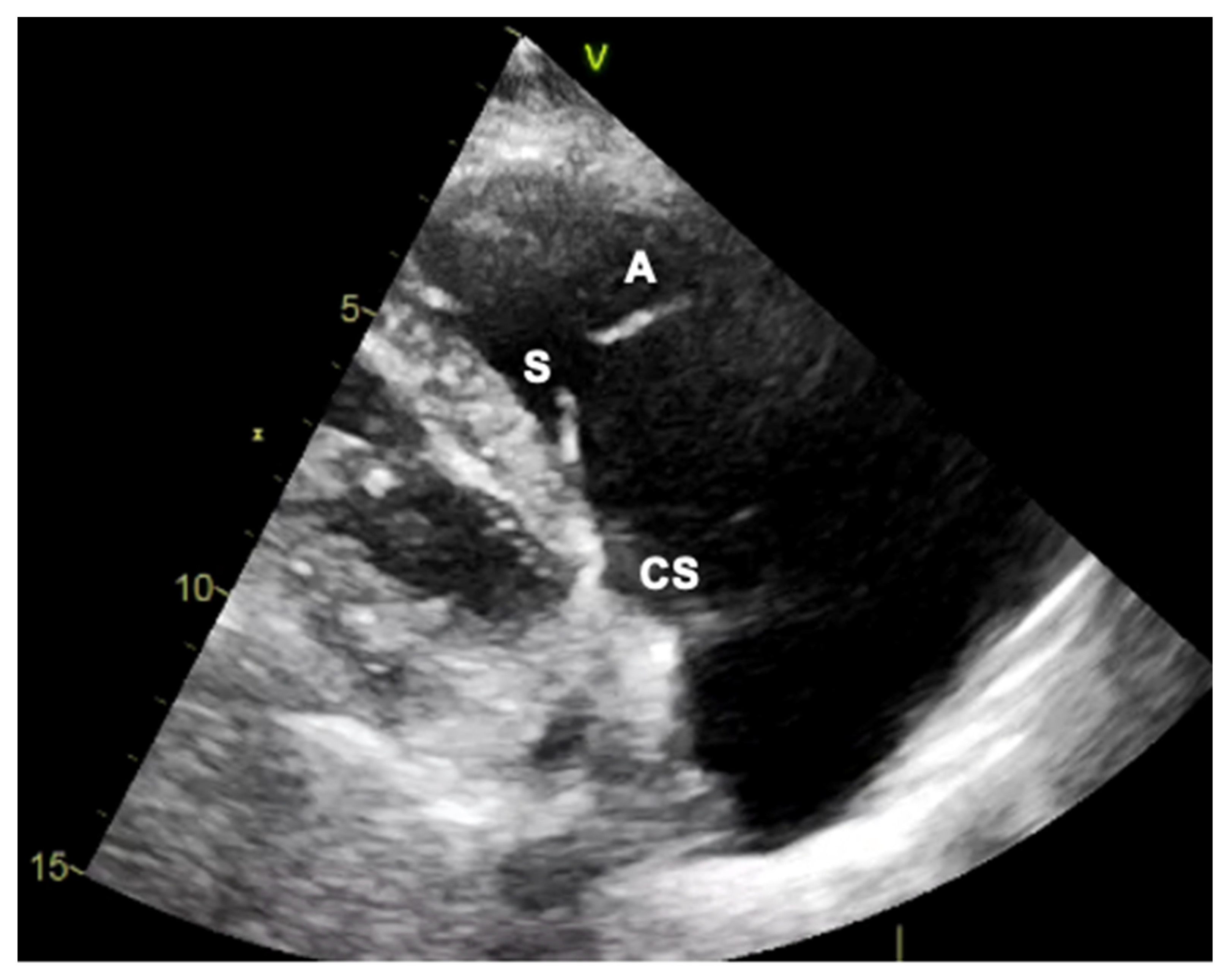
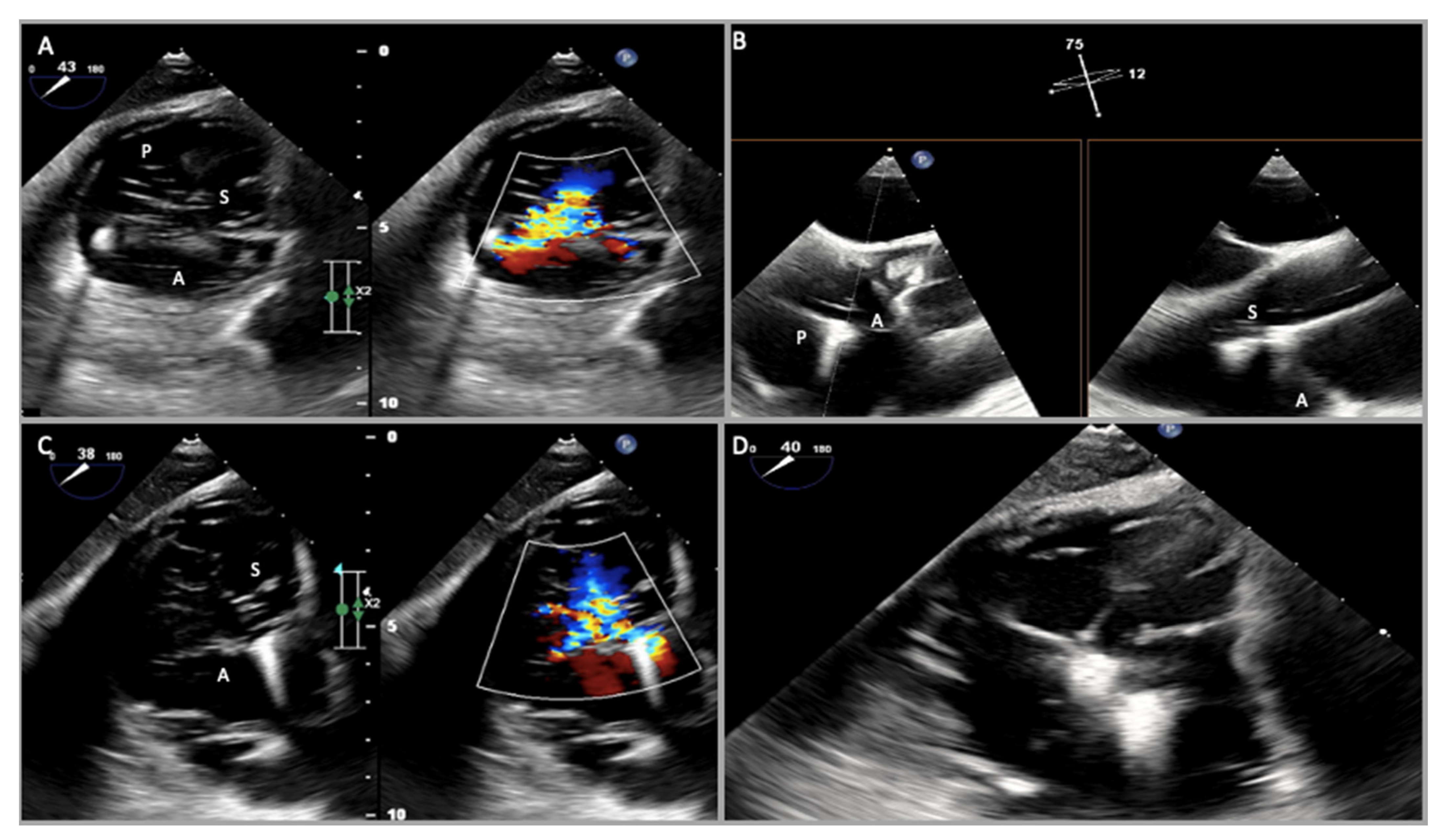
2.1. Two-Dimensional and Three-Dimensional Transthoracic and Transesophageal Echocardiography
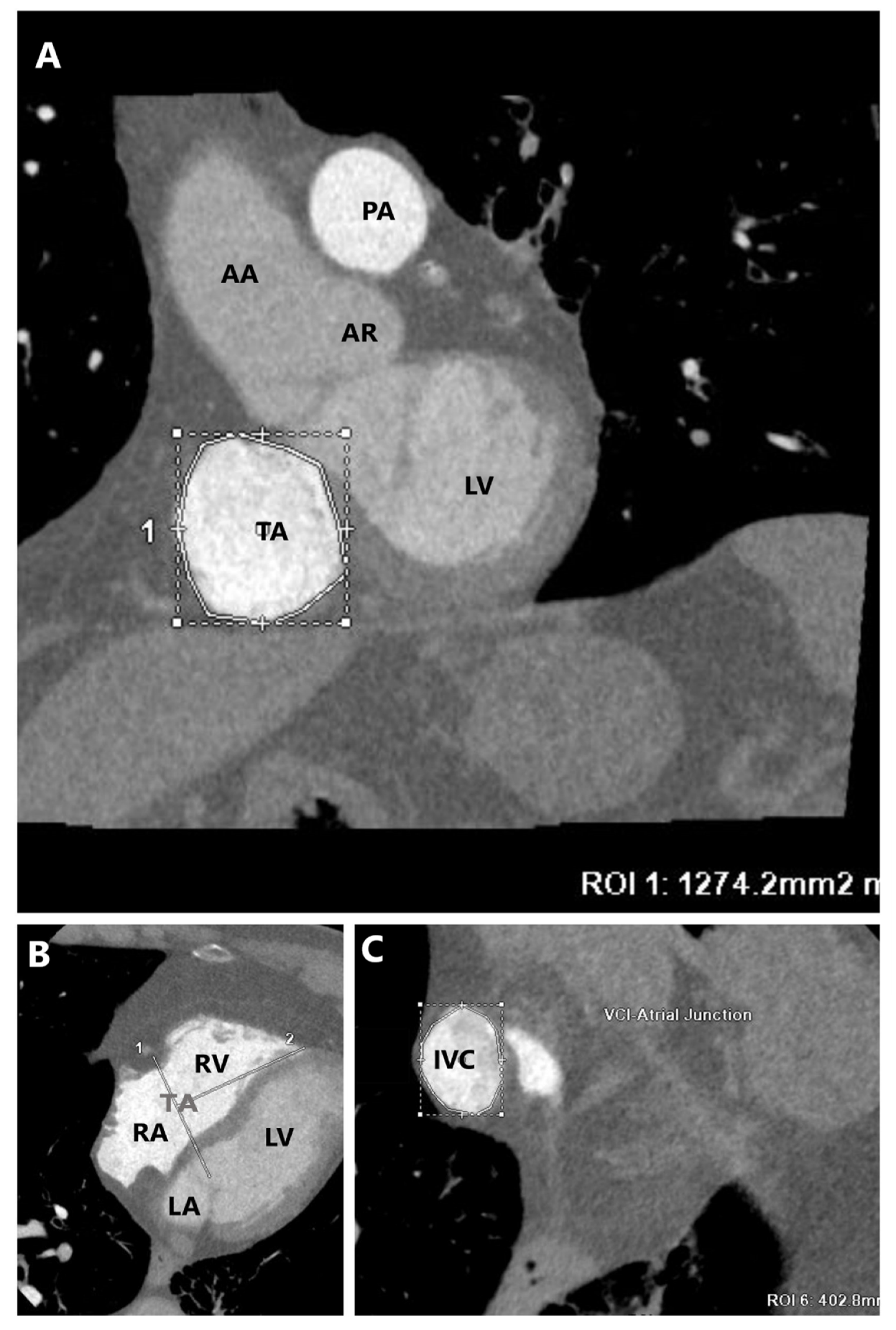
2.2. Cardiac Computed Tomography
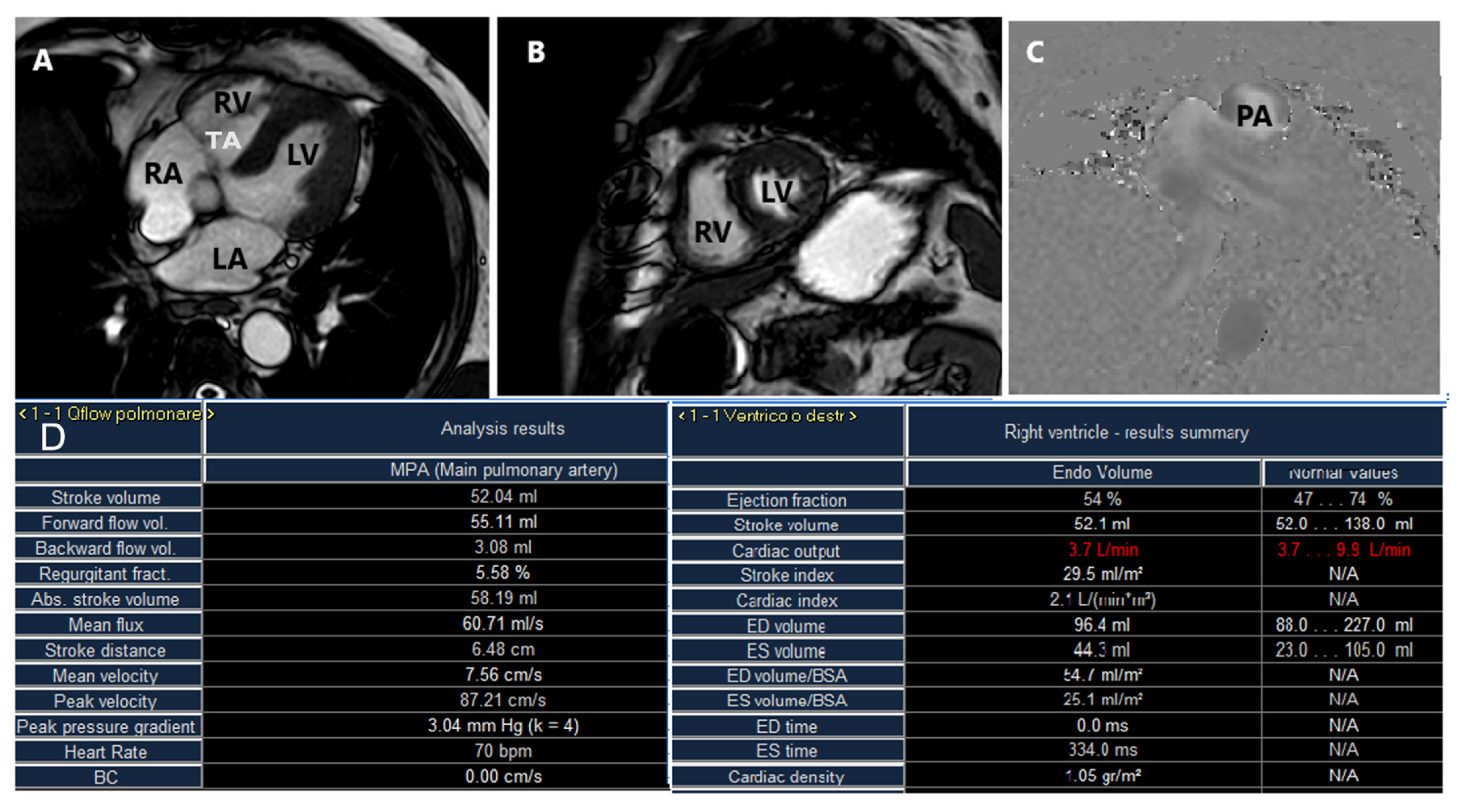
2.3. Cardiac Magnetic Resonance
3. Intra-Procedural Guidance for Tricuspid Transcatheter Edge-to-Edge Repair
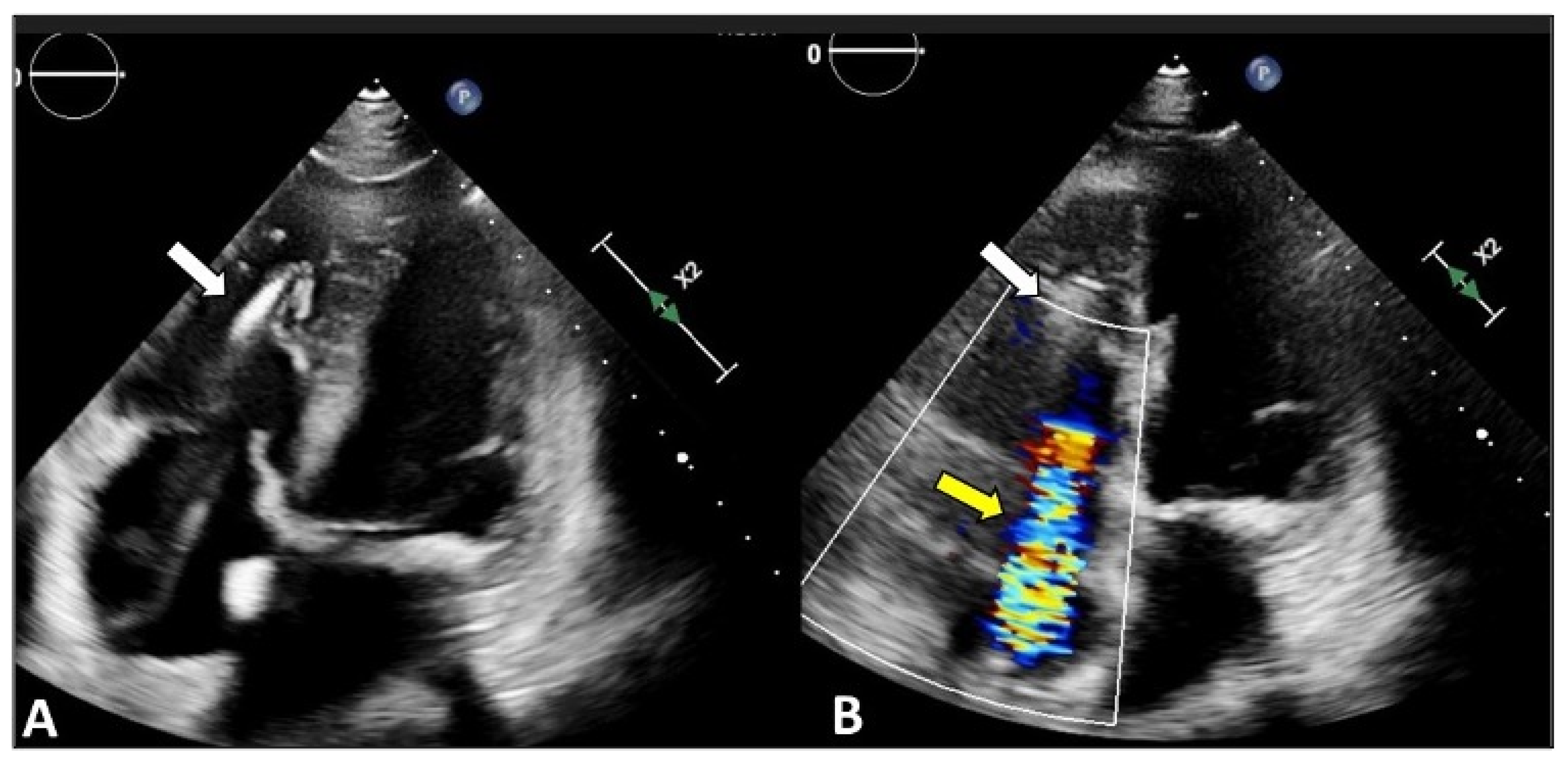
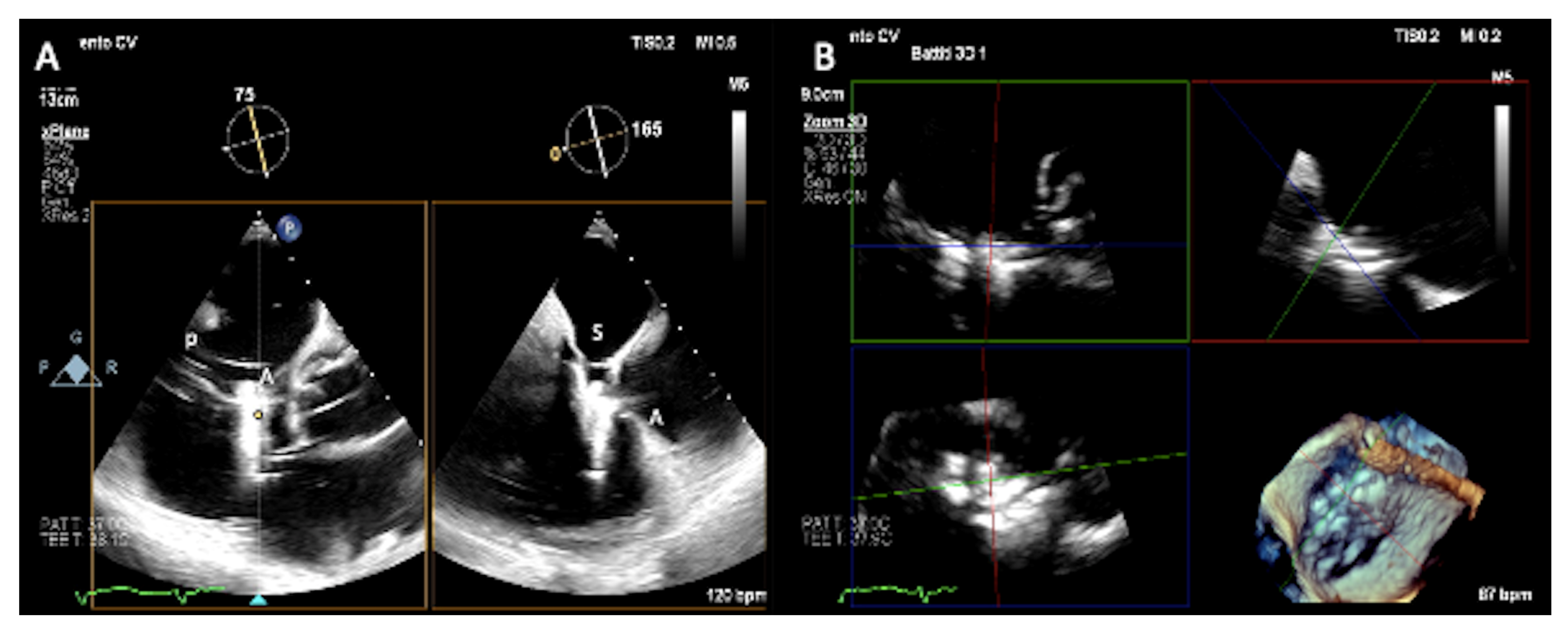
3.1. Two-Dimensional and Three-Dimensional Transesophageal Echocardiography
3.2. Intracardiac Echocardiography: Strenghts and Limitations
3.3. Fluoroscopy
3.4. Fusion Imaging
4. Follow-Up of Tricuspid Transcatheter Edge-to-Edge Repair
4.1. Two-Dimensional and Three-Dimensional Transthoracic and Transesophageal Echocardiography
4.2. Cardiac Computed Tomography and Cardiac Magnetic Resonance
5. Future Directions: 3D Printing, Computational Models, and Artificial Intelligence
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hahn, R.T. State-of-the-Art Review of Echocardiographic Imaging in the Evaluation and Treatment of Functional Tricuspid Regurgitation. Circ. Cardiovasc. Imaging 2016, 9, e005332. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, S.; Saracino, G.; Matsumura, Y.; Daimon, M.; Tran, H.; Greenberg, N.L.; Hozumi, T.; Yoshikawa, J.; Thomas, J.D.; Shiota, T. Three-dimensional geometry of the tricuspid annulus in healthy subjects and in patients with functional tricuspid regurgitation: A real-time, 3-dimensional echocardiographic study. Circulation 2006, 114, I492–I498. [Google Scholar] [CrossRef] [PubMed]
- Ton-Nu, T.T.; Levine, R.A.; Handschumacher, M.D.; Dorer, D.J.; Yosefy, C.; Fan, D.; Hua, L.; Jiang, L.; Hung, J. Geometric determinants of functional tricuspid regurgitation: Insights from 3-dimensional echocardiography. Circulation 2006, 114, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Lama, P.; Tamang, B.K.; Kulkarni, J. Morphometry and aberrant morphology of the adult human tricuspid valve leaflets. Anat. Sci. Int. 2015, 91, 143–150. [Google Scholar] [CrossRef]
- Dahou, A.; Levin, D.; Reisman, M.; Hahn, R.T. Anatomy and Physiology of the Tricuspid Valve. JACC Cardiovasc. Imaging 2019, 12, 458–468. [Google Scholar] [CrossRef] [PubMed]
- Pluchinotta, S.P.S.a.F.R. Tricuspid Valve: Embryology and Anatomy. In The Tricuspid Valve in Congenital Heart Disease; Giamberti, M.C.A., Ed.; Springer: New York, NY, USA, 2014; pp. 1–13. [Google Scholar]
- Asmarats, L.; Puri, R.; Latib, A.; Navia, J.L.; Rodés-Cabau, J. Transcatheter Tricuspid Valve Interventions: Landscape, Challenges, and Future Directions. J. Am. Coll. Cardiol. 2018, 71, 2935–2956. [Google Scholar] [CrossRef]
- Topilsky, Y.; Maltais, S.; Inojosa, J.M.; Oguz, D.; Michelena, H.; Maalouf, J.; Mahoney, D.W.; Enriquez-Sarano, M. Burden of tricuspid regurgitation in patients diagnosed in the community setting. JACC Cardiovasc. Imaging 2019, 12, 433442. [Google Scholar] [CrossRef]
- Lee, J.W.; Song, J.M.; Park, J.P.; Kang, D.H.; Song, J.K. Long-term prognosis of isolated significant tricuspid regurgitation. Circ. J. 2010, 74, 375–380. [Google Scholar] [CrossRef]
- Zack, C.J.; Fender, E.A.; Chandrashekar, P.; Reddy, Y.N.; Bennett, C.E.; Stulak, J.M.; Miller, V.M.; Nishimura, R.A. National trends and outcomes in isolated tricuspid valve surgery. J. Am. Coll. Cardiol. 2017, 70, 2953–2960. [Google Scholar] [CrossRef]
- Dreyfus, J.; Flagiello, M.; Bazire, B.; Eggenspieler, F.; Viau, F.; Riant, E.; Mbaki, Y.; Bohbot, Y.; Eyharts, D.; Senage, T.; et al. Isolated tricuspid valve surgery: Impact of aetiology and clinical presentation on outcomes. Eur. Heart J. 2020, 41, 4304–4317. [Google Scholar] [CrossRef]
- Beyersdorf, F.; Vahanian, A.; Milojevic, M.; Praz, F.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. J. Cardiothorac. Surg. 2022, 61, 964. [Google Scholar] [CrossRef]
- Taramasso, M.; Benfari, G.; van der Bijl, P.; Alessandrini, H.; Attinger-Toller, A.; Biasco, L.; Lurz, P.; Braun, D.; Brochet, E.; Connelly, K.A.; et al. Transcatheter Versus Medical Treatment of Patients with Symptomatic Severe Tricuspid Regurgitation. J. Am. Coll. Cardiol. 2019, 74, 2998–3008. [Google Scholar] [CrossRef] [PubMed]
- Schlotter, F.; Miura, M.; Kresoja, K.-P.; Alushi, B.; Alessandrini, H.; Attinger-Toller, A.; Besler, C.; Biasco, L.; Braun, D.; Brochet, E.; et al. Outcomes of transcatheter tricuspid valve intervention by right ventricular function: A multicentre propensity-matched analysis. Eurointervention 2021, 17, e343–e352. [Google Scholar] [CrossRef]
- Lurz, P.; von Bardeleben, R.S.; Weber, M.; Sitges, M.; Sorajja, P.; Hausleiter, J.; Denti, P.; Trochu, J.-N.; Nabauer, M.; Tang, G.H.; et al. Transcatheter Edge-to-Edge Repair for Treatment of Tricuspid Regurgitation. J. Am. Coll. Cardiol. 2021, 77, 229–239. [Google Scholar] [CrossRef] [PubMed]
- Kodali, S.; Hahn, R.T.; Eleid, M.F.; Kipperman, R.; Smith, R.; Lim, D.S.; Gray, W.A.; Narang, A.; Pislaru, S.V.; Koulogiannis, K.; et al. Feasibility Study of the Transcatheter Valve Repair System for Severe Tricuspid Regurgitation. J. Am. Coll. Cardiol. 2021, 77, 345–356. [Google Scholar] [CrossRef] [PubMed]
- Praz, F.; Muraru, D.; Kreidel, F.; Lurz, P.; Hahn, R.T.; Delgado, V.; Senni, M.; von Bardeleben, R.S.; Nickenig, G.; Hausleiter, J.; et al. Transcatheter treatment for tricuspid valve disease. Eurointervention 2021, 17, 791–808. [Google Scholar] [CrossRef]
- Prihadi, E.A.; Delgado, V.; Hahn, R.T.; Leipsic, J.; Min, J.K.; Bax, J.J. Imaging Needs in Novel Transcatheter Tricuspid Valve Interventions. JACC Cardiovasc. Imaging 2018, 11, 736–754. [Google Scholar] [CrossRef]
- Anwar, A.M.; Geleijnse, M.L.; Soliman, O.I.I.; McGhie, J.S.; Frowijn, R.; Nemes, A.; Bosch, A.E.V.D.; Galema, T.W.; Cate, F.J.T. Assessment of normal tricuspid valve anatomy in adults by real-time three-dimensional echocardiography. Int. J. Cardiovasc. Imaging 2007, 23, 717–724. [Google Scholar] [CrossRef]
- Hahn, R.T.; Zamorano, J.L. The need for a new tricuspid regurgitation grading scheme. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 1342–1343. [Google Scholar] [CrossRef]
- Spinner, E.M.; Lerakis, S.; Higginson, J.; Pernetz, M.; Howell, S.; Veledar, E.; Yoganathan, A.P. Correlates of Tricuspid Regurgitation as Determined by 3D Echocardiography: Pulmonary Arterial Pressure, Ventricle Geometry, Annular Dilatation, and Papillary Muscle Displacement. Circ. Cardiovasc. Imaging 2012, 5, 43–50, Erratum in Circ. Cardiovasc. Imaging 2012, 5, e54. [Google Scholar] [CrossRef]
- Gopal, A.S.; Chukwu, E.O.; Iwuchukwu, C.J.; Katz, A.S.; Toole, R.S.; Schapiro, W.; Reichek, N. Normal values of right ventricular size and function by real-time 3-dimensional echocardiography: Comparison with cardiac magnetic resonance imaging. J. Am. Soc. Echocardiogr. 2007, 20, 445–455. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Tsang, W.; Adams, D.H.; Agricola, E.; Buck, T.; Faletra, F.F.; Franke, A.; Hung, J.; de Isla, L.P.; et al. EAE/ASE Recommendations for Image Acquisition and Display Using Three-Dimensional Echocardiography. J. Am. Soc. Echocardiogr. 2012, 25, 3–46. [Google Scholar] [CrossRef] [PubMed]
- Nickenig, G.; Weber, M.; Lurz, P.; von Bardeleben, R.S.; Sitges, M.; Sorajja, P.; Hausleiter, J.; Denti, P.; Trochu, J.-N.; Näbauer, M.; et al. Transcatheter edge-to-edge repair for reduction of tricuspid regurgitation: 6-month outcomes of the TRILUMINATE single-arm study. Lancet 2019, 394, 2002–2011, Erratum in Lancet 2020, 395, 870. [Google Scholar] [CrossRef]
- Hahn, R.T.; Saric, M.; Faletra, F.F.; Garg, R.; Gillam, L.D.; Horton, K.; Khalique, O.K.; Little, S.H.; Mackensen, G.B.; Oh, J.; et al. Recommended Standards for the Performance of Transesophageal Echocardiographic Screening for Structural Heart Intervention: From the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2021, 35, 1–76, Erratum in J. Am. Soc. Echocardiogr. 2022, 35, 447. [Google Scholar] [CrossRef] [PubMed]
- Hahn, R.T.; Kodali, S.K. State-of-the-art intra-procedural imaging for the mitral and tricuspid PASCAL Repair System. Eur. Heart J. Cardiovasc. Imaging 2022, 23, e94–e110. [Google Scholar] [CrossRef]
- Muntané-Carol, G.; Alperi, A.; Faroux, L.; Bédard, E.; Philippon, F.; Rodés-Cabau, J. Transcatheter Tricuspid Valve Intervention: Coaptation Devices. Front. Cardiovasc. Med. 2020, 7, 139. [Google Scholar] [CrossRef] [PubMed]
- Orban, M.; Wolff, S.; Braun, D.; Stolz, L.; Higuchi, S.; Stark, K.; Mehr, M.; Stocker, T.J.; Dischl, D.; Scherer, C.; et al. Right Ventricular Function in Transcatheter Edge-to-Edge Tricuspid Valve Repair. JACC Cardiovasc. Imaging 2021, 14, 2477–2479. [Google Scholar] [CrossRef]
- Ricci, F.; Bufano, G.; Galusko, V.; Sekar, B.; Benedetto, U.; Awad, W.I.; Di Mauro, M.; Gallina, S.; Ionescu, A.; Badano, L.; et al. Tricuspid regurgitation management: A systematic review of clinical practice guidelines and recommendations. Eur. Heart J. Qual. Care Clin. Outcomes 2021, 8, 238–248. [Google Scholar] [CrossRef]
- Naoum, C.; Blanke, P.; Cavalcante, J.L.; Leipsic, J. Cardiac Computed Tomography and Magnetic Resonance Imaging in the Evaluation of Mitral and Tricuspid Valve Disease: Implications for Transcatheter Interventions. Circ. Cardiovasc. Imaging 2017, 10, e005331. [Google Scholar] [CrossRef]
- Gheorghe, L.L.; Hegeman, R.; Vrijkorte, M.; Wunderlich, N.; Cavalcante, J.; Wang, D.D.; Rana, B.; Vannan, M.; Timmers, L.; Swaans, M. The evolving role of multi-modality imaging in transcatheter tricuspid valve interventions. Front. Cardiovasc. Med. 2022, 9, 793267. [Google Scholar] [CrossRef]
- Hashimoto, G.; Fukui, M.; Sorajja, P.; Cavalcante, J.L. Essential roles for CT and MRI in timing of therapy in tricuspid regurgitation. Prog. Cardiovasc. Dis. 2019, 62, 459–462. [Google Scholar] [CrossRef] [PubMed]
- Pulerwitz, T.C.; Khalique, O.K.; Leb, J.; Hahn, R.T.; Nazif, T.; Leon, M.B.; George, I.; Vahl, T.P.; D’souza, B.; Bapat, V.N.; et al. Optimizing Cardiac CT Protocols for Comprehensive Acquisition Prior to Percutaneous MV and TV Repair/Replacement. JACC Cardiovasc. Imaging 2020, 13, 836–850. [Google Scholar] [CrossRef] [PubMed]
- Khalique, O.K.; Cavalcante, J.L.; Shah, D.; Guta, A.C.; Zhan, Y.; Piazza, N.; Muraru, D. Multimodality Imaging of the Tricuspid Valve and Right Heart Anatomy. JACC Cardiovasc. Imaging 2019, 12, 516–531, Erratum in JACC Cardiovasc. Imaging 2019, 12, 2611–2612. [Google Scholar] [CrossRef] [PubMed]
- Cammalleri, V.; Carpenito, M.; Bono, M.C.; Mega, S.; Ussia, G.P.; Grigioni, F. Transcatheter Tricuspid Valve Therapy: From Anatomy to Intervention. Front. Cardiovasc. Med. 2021, 8, 778445. [Google Scholar] [CrossRef] [PubMed]
- Sugiura, A.; Tanaka, T.; Kavsur, R.; Oeztuerk, C.; Vogelhuber, J.; Wilde, N.; Becher, M.U.; Zimmer, S.; Nickenig, G.; Weber, M. Leaflet Configuration and Residual Tricuspid Regurgitation after Transcatheter Edge-to-Edge Tricuspid Repair. JACC Cardiovasc. Interv. 2021, 14, 2260–2270. [Google Scholar] [CrossRef] [PubMed]
- Pugliese, L.; Ricci, F.; Luciano, A.; De Stasio, V.; Presicce, M.; Spiritigliozzi, L.; Di Tosto, F.; Di Donna, C.; D’errico, F.; Benelli, L.; et al. Role of computed tomography in transcatheter replacement of ‘other valves’: A comprehensive review of preprocedural imaging. J. Cardiovasc. Med. 2022, 23, 575–588. [Google Scholar] [CrossRef] [PubMed]
- Cammalleri, V.; Carpenito, M.; De Stefano, D.; Ussia, G.P.; Bono, M.C.; Mega, S.; Nusca, A.; Cocco, N.; Nobile, E.; De Filippis, A.; et al. Novel Computed Tomography Variables for Assessing Tricuspid Valve Morphology: Results from the TRIMA (Tricuspid Regurgitation IMAging) Study. J. Clin. Med. 2022, 11, 2825. [Google Scholar] [CrossRef]
- Carpenito, M.; Cammalleri, V.; Vitez, L.; De Filippis, A.; Nobile, E.; Bono, M.C.; Mega, S.; Bunc, M.; Grigioni, F.; Ussia, G.P. Edge-to-Edge Repair for Tricuspid Valve Regurgitation. Preliminary Echo-Data and Clinical Implications from the Tricuspid Regurgitation IMAging (TRIMA) Study. J. Clin. Med. 2022, 11, 5609. [Google Scholar] [CrossRef]
- Agricola, E.; Asmarats, L.; Maisano, F.; Cavalcante, J.L.; Liu, S.; Milla, F.; Meduri, C.; Rodés-Cabau, J.; Vannan, M.; Pibarot, P. Imaging for Tricuspid Valve Repair and Replacement. JACC Cardiovasc. Imaging 2021, 14, 61–111. [Google Scholar] [CrossRef]
- Maffei, E.; Messalli, G.; Martini, C.; Nieman, K.; Catalano, O.; Rossi, A.; Seitun, S.; Guaricci, A.I.; Tedeschi, C.; Mollet, N.R.; et al. Left and right ventricle assessment with Cardiac CT: Validation study vs. Cardiac MR. Eur. Radiol. 2012, 22, 1041–1049. [Google Scholar] [CrossRef] [PubMed]
- Plumhans, C.; Mühlenbruch, G.; Rapaee, A.; Sim, K.-H.; Seyfarth, T.; Günther, R.W.; Mahnken, A.H. Assessment of Global Right Ventricular Function on 64-MDCT Compared with MRI. Am. J. Roentgenol. 2008, 190, 1358–1361. [Google Scholar] [CrossRef]
- Layoun, H.; Schoenhagen, P.; Wang, T.K.M.; Puri, R.; Kapadia, S.R.; Harb, S.C. Roles of Cardiac Computed Tomography in Guiding Transcatheter Tricuspid Valve Interventions. Curr. Cardiol. Rep. 2021, 23, 114. [Google Scholar] [CrossRef] [PubMed]
- Cavalcante, J.L.; Lalude, O.O.; Schoenhagen, P.; Lerakis, S. Cardiovascular Magnetic Resonance Imaging for Structural and Valvular Heart Disease Interventions. JACC Cardiovasc. Interv. 2016, 9, 399–425. [Google Scholar] [CrossRef] [PubMed]
- Hundley, W.G.; Bluemke, D.A.; Finn, J.P.; Flamm, S.D.; Fogel, M.A.; Friedrich, M.G.; Ho, V.B.; Jerosch-Herold, M.; Kramer, C.M.; Manning, W.J.; et al. ACCF/ACR/AHA/NASCI/SCMR 2010 Expert Consensus Document on Cardiovascular Magnetic Resonance: A Report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents. J. Am. Coll. Cardiol. 2010, 55, 2614–2662. [Google Scholar] [CrossRef] [PubMed]
- Hadley, M.B.; Prandi, F.R.; Barillà, F.; Sharma, S.; Kini, A.; Lerakis, S. Case report: Paravalvular regurgitation post transcatheter aortic valve replacement: When in doubt choose cardiac magnetic resonance. Front. Cardiovasc. Med. 2022, 9, 925120. [Google Scholar] [CrossRef]
- Zhan, Y.; Debs, D.; Khan, M.A.; Nguyen, D.T.; Graviss, E.A.; Khalaf, S.; Little, S.H.; Reardon, M.J.; Nagueh, S.; Quiñones, M.A.; et al. Natural History of Functional Tricuspid Regurgitation Quantified by Cardiovascular Magnetic Resonance. J. Am. Coll. Cardiol. 2020, 76, 1291–1301. [Google Scholar] [CrossRef] [PubMed]
- Park, J.-B.; Kim, H.-K.; Jung, J.-H.; Klem, I.; Yoon, Y.E.; Lee, S.-P.; Park, E.-A.; Hwang, H.-Y.; Lee, W.; Kim, K.-H.; et al. Prognostic value of cardiac MR imaging for preoperative assessment of patients with severe functional tricuspid regurgitation. Radiology 2016, 280, 723–734. [Google Scholar] [CrossRef] [PubMed]
- Kresoja, K.-P.; Rommel, K.-P.; Lücke, C.; Unterhuber, M.; Besler, C.; von Roeder, M.; Schöber, A.R.; Noack, T.; Gutberlet, M.; Thiele, H.; et al. Right Ventricular Contraction Patterns in Patients Undergoing Transcatheter Tricuspid Valve Repair for Severe Tricuspid Regurgitation. JACC Cardiovasc. Interv. 2021, 14, 1551–1561. [Google Scholar] [CrossRef]
- García-Alvarez, A.; Friera, L.F.; Mirelis, J.G.; Sawit, S.; Nair, A.; Kallman, J.; Fuster, V.; Sanz, J. Non-invasive estimation of pulmonary vascular resistance with cardiac magnetic resonance. Eur. Heart J. 2011, 32, 2438–2445. [Google Scholar] [CrossRef]
- Hahn, R.T.; Nabauer, M.; Zuber, M.; Nazif, T.M.; Hausleiter, J.; Taramasso, M.; Pozzoli, A.; George, I.; Kodali, S.; Bapat, V.; et al. Intraprocedural Imaging of Transcatheter Tricuspid Valve Interventions. JACC Cardiovasc. Imaging 2019, 12, 532–553. [Google Scholar] [CrossRef]
- Ro, R.; Tang, G.H.L.; Seetharam, K.; Khera, S.; Sharma, S.K.; Kini, A.S.; Lerakis, S. Echocardiographic Imaging for Transcatheter Tricuspid Edge-to-Edge Repair. J. Am. Heart Assoc. 2020, 9, e015682. [Google Scholar] [CrossRef] [PubMed]
- Cieszynski, T. Intracardiac method for the investigation of structure of the heart with the aid of ultrasonics. Arch. Immunol. Ther. Exp. 1960, 8, 551–557. [Google Scholar]
- Valdes-Cruz, L.M.; Sideris, E.; Sahn, D.J.; Murillo-Olivas, A.; Knudson, O.; Omoto, R.; Kyo, S.; Gulde, R. Transvascular intracardiac applications of a miniaturized phased-array ultrasonic endoscope. Initial experience with intracardiac imaging in piglets. Circulation 1991, 83, 1023–1027. [Google Scholar] [CrossRef]
- Hijazi, Z.M.; Shivkumar, K.; Sahn, D.J. Intracardiac Echocardiography during Interventional and Electrophysiological Cardiac Catheterization. Circulation 2009, 119, 587–596. [Google Scholar] [CrossRef] [PubMed]
- Robinson, A.A.; Chadwell, K.; Fowler, D.E.; Ailawadi, G.; Lim, D.S. Multiplane Intracardiac Echocardiography: A Novel System to Guide Percutaneous Tricuspid Repair. JACC Cardiovasc. Interv. 2018, 11, 2540–2542. [Google Scholar] [CrossRef]
- Eleid, M.F.; Alkhouli, M.; Thaden, J.J.; Zahr, F.; Chadderdon, S.; Guerrero, M.; Reeder, G.S.; Rihal, C.S. Utility of Intracardiac Echocardiography in the Early Experience of Transcatheter Edge to Edge Tricuspid Valve Repair. Circ. Cardiovasc. Interv. 2021, 14, e011118. [Google Scholar] [CrossRef]
- Pozzoli, A.; Taramasso, M.; Zuber, M.; Maisano, F. Transcatheter tricuspid valve repair with the MitraClip system using intracardiac echocardiography: Proof of concept. Eurointervention 2017, 13, e1452–e1453. [Google Scholar] [CrossRef] [PubMed]
- Alkhouli, M.; Hijazi, Z.M.; Holmes, D.R., Jr.; Rihal, C.S.; Wiegers, S.E. Intracardiac Echocardiography in Structural Heart Disease Interventions. JACC Cardiovasc. Interv. 2018, 11, 2133–2147. [Google Scholar] [CrossRef]
- Tang, G.H.; Yakubov, S.J.; Soto, C.E.S. 4-Dimensional Intracardiac Echocardiography in Transcatheter Tricuspid Valve Repair with the MitraClip System. JACC Cardiovasc. Imaging 2020, 13, 1591–1600. [Google Scholar] [CrossRef]
- Silvestry, F.E.; Kadakia, M.B.; Willhide, J.; Herrmann, H.C. Initial experience with a novel real-time three-dimensional intracardiac ultrasound system to guide percutaneous cardiac structural interventions: A phase 1 feasibility study of volume intracardiac echocardiography in the assessment of patients with structural heart disease undergoing percutaneous transcatheter therapy. J. Am. Soc. Echocardiogr. 2014, 27, 978–983. [Google Scholar] [CrossRef]
- Pozzoli, A.; Maisano, F.; Kuwata, S.; Guidotti, A.; Plass, A.; Zuber, M.; Russo, M.; Nietlispach, F.; Taramasso, M. Fluoroscopic anatomy of the tricuspid valve: Implications for Transcatheter procedures. Int. J. Cardiol. 2017, 244, 119–120. [Google Scholar] [CrossRef]
- Pighi, M.; Thériault-Lauzier, P.; Alosaimi, H.; Spaziano, M.; Martucci, G.; Xiong, T.-Y.; Buithieu, J.; Ybarra, L.F.; Afilalo, J.; Leipsic, J.; et al. Fluoroscopic Anatomy of Right-Sided Heart Structures for Transcatheter Interventions. JACC Cardiovasc. Interv. 2018, 11, 1614–1625. [Google Scholar] [CrossRef] [PubMed]
- Pascual, I.; Pozzoli, A.; Taramasso, M.; Maisano, F.; Ho, E.C. Fusion imaging for transcatheter mitral and tricuspid interventions. Ann. Transl. Med. 2020, 8, 965. [Google Scholar] [CrossRef] [PubMed]
- Faletra, F.F.; Pedrazzini, G.; Pasotti, E.; Murzilli, R.; Leo, L.A.; Moccetti, T. Echocardiography–X-ray Image Fusion. JACC Cardiovasc. Imaging 2016, 9, 1114–1117. [Google Scholar] [CrossRef] [PubMed]
- Afzal, S.; Veulemans, V.; Balzer, J.; Rassaf, T.; Hellhammer, K.; Polzin, A.; Kelm, M.; Zeus, T. Safety and efficacy of transseptal puncture guided by real-time fusion of echocardiography and fluoroscopy. Neth. Heart J. 2017, 25, 131–136. [Google Scholar] [CrossRef]
- Jone, P.-N.; Ross, M.M.; Bracken, J.A.; Mulvahill, M.J.; Di Maria, M.V.; Fagan, T.E. Feasibility and Safety of Using a Fused Echocardiography/Fluoroscopy Imaging System in Patients with Congenital Heart Disease. J. Am. Soc. Echocardiogr. 2016, 29, 513–521. [Google Scholar] [CrossRef]
- Jungen, C.; Zeus, T.; Balzer, J.; Eickholt, C.; Petersen, M.; Kehmeier, E.; Veulemans, V.; Kelm, M.; Willems, S.; Meyer, C. Left Atrial Appendage Closure Guided by Integrated Echocardiography and Fluoroscopy Imaging Reduces Radiation Exposure. PLoS ONE 2015, 10, e0140386. [Google Scholar] [CrossRef]
- Anastasius, M.; Tang, G.H.; Love, B.; Krishnamoorthy, P.; Sharma, S.; Kini, A.; Lerakis, S. A Novel Hybrid Imaging Approach for Guidance of Percutaneous Transcatheter Tricuspid Valve Edge-to-Edge Repair. J. Am. Soc. Echocardiogr. 2021, 34, 567–568. [Google Scholar] [CrossRef]
- Barreiro-Perez, M.; Estevez-Loureiro, R.; Baz, J.A.; Piñón, M.A.; Maisano, F.; Puga, L.; Caneiro-Queija, B.; Iñiguez-Romo, A. Cardiovalve Transfemoral Tricuspid Valve Replacement Assisted with CT–Fluoroscopy Fusion Imaging. JACC Cardiovasc. Interv. 2022, 15, e197–e199. [Google Scholar] [CrossRef]
- Boeder, N.F.; Bayer, M.; Dörr, O.; Nef, H.M. Fusion imaging guided implantation of a Tricento transcatheter heart valve for severe tricuspid regurgitation. Catheter. Cardiovasc. Interv. 2021, 98, E780–E784. [Google Scholar] [CrossRef]
- Bertsche, D.; Keßler, M.; Buckert, D.; Schneider, L.-M.; Rottbauer, W.; Rasche, V.; Markovic, S.; Vernikouskaya, I. How to improve navigation during cardioband transcatheter tricuspid annuloplasty. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 611–613. [Google Scholar] [CrossRef] [PubMed]
- Sanz, A.P.; Recalde, Á.S.; Tahoces, L.S.; Lobán, C.F.-G.; Gómez, J.L.Z. MSCT-fluoroscopy fusion imaging for guidance in percutaneous bicaval valve implantation for transcatheter treatment of tricuspid regurgitation. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 1303. [Google Scholar] [CrossRef] [PubMed]
- Fortuni, F.; Marques, A.I.; Bax, J.J.; Marsan, N.A.; Delgado, V. Echocardiography–computed tomography fusion imaging for guidance of transcatheter tricuspid valve annuloplasty. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 937–938. [Google Scholar] [CrossRef]
- Ancona, F.; Stella, S.; Taramasso, M.; Marini, C.; Latib, A.; Denti, P.; Grigioni, F.; Enriquez-Sarano, M.; Alfieri, O.; Colombo, A.; et al. Multimodality imaging of the tricuspid valve with implication for percutaneous repair approaches. Heart 2017, 103, 1073–1081. [Google Scholar] [CrossRef] [PubMed]
- Agricola, E.; Ancona, F.; Stella, S.; Rosa, I.; Marini, C.; Spartera, M.; Denti, P.; Margonato, A.; Hahn, R.T.; Alfieri, O.; et al. Use of Echocardiography for Guiding Percutaneous Tricuspid Valve Procedures. JACC Cardiovasc. Imaging 2017, 10, 1194–1198. [Google Scholar] [CrossRef]
- Lancellotti, P.; Pibarot, P.; Chambers, J.; Edvardsen, T.; Delgado, V.; Dulgheru, R.; Pepi, M.; Cosyns, B.; Dweck, M.R.; Garbi, M.; et al. Recommendations for the imaging assessment of prosthetic heart valves: A report from the European Association of Cardiovascular Imaging endorsed by the Chinese Society of Echocardiography, the Inter-American Society of Echocardiography, and the Brazilian Department of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 589–590. [Google Scholar] [CrossRef]
- Coisne, A.; Scotti, A.; Taramasso, M.; Granada, J.F.; Ludwig, S.; Rodés-Cabau, J.; Lurz, P.; Hausleiter, J.; Fam, N.; Kodali, S.K.; et al. Prognostic Value of Tricuspid Valve Gradient after Transcatheter Edge-to-Edge Repair. JACC Cardiovasc. Interv. 2023, 16, 706–717. [Google Scholar] [CrossRef]
- Brener, M.I.; Lurz, P.; Hausleiter, J.; Rodés-Cabau, J.; Fam, N.; Kodali, S.K.; Rommel, K.-P.; Muntané-Carol, G.; Gavazzoni, M.; Nazif, T.M.; et al. Right Ventricular-Pulmonary Arterial Coupling and Afterload Reserve in Patients Undergoing Transcatheter Tricuspid Valve Repair. J. Am. Coll. Cardiol. 2022, 79, 448–461. [Google Scholar] [CrossRef]
- Montalto, C.; Sticchi, A.; Crimi, G.; Laricchia, A.; Khokhar, A.; Giannini, F.; Ferlini, M.; Colombo, A.; Latib, A.; Mangieri, A. Functional and Echocardiographic Improvement after Transcatheter Repair for Tricuspid Regurgitation: A Systematic Review and Pooled Analysis. JACC Cardiovasc. Interv. 2020, 13, 2719–2729. [Google Scholar] [CrossRef]
- Fortuni, F.; Hirasawa, K.; Bax, J.J.; Delgado, V.; Marsan, N.A. Multi-Modality Imaging for Interventions in Tricuspid Valve Disease. Front. Cardiovasc. Med. 2021, 8, 638487. [Google Scholar] [CrossRef]
- Rommel, K.-P.; Besler, C.; Noack, T.; Blazek, S.; von Roeder, M.; Fengler, K.; Ender, J.; Gutberlet, M.; Desch, S.; Borger, M.A.; et al. Physiological and Clinical Consequences of Right Ventricular Volume Overload Reduction after Transcatheter Treatment for Tricuspid Regurgitation. JACC Cardiovasc. Interv. 2019, 12, 1423–1434. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-K.; Kim, Y.-J.; Park, E.-A.; Bae, J.-S.; Lee, W.; Kim, K.-H.; Kim, K.-B.; Sohn, D.-W.; Ahn, H.; Park, J.-H.; et al. Assessment of haemodynamic effects of surgical correction for severe functional tricuspid regurgitation: Cardiac magnetic resonance imaging study. Eur. Heart J. 2010, 31, 1520–1528. [Google Scholar] [CrossRef] [PubMed]
- Tuncay, V.; Van Ooijen, P.M.A. 3D printing for heart valve disease: A systematic review. Eur. Radiol. Exp. 2019, 3, 9. [Google Scholar] [CrossRef] [PubMed]
- Qian, Z.; Wang, K.; Liu, S.; Zhou, X.; Rajagopal, V.; Meduri, C.; Kauten, J.R.; Chang, Y.-H.; Wu, C.; Zhang, C.; et al. Quantitative Prediction of Paravalvular Leak in Transcatheter Aortic Valve Replacement Based on Tissue-Mimicking 3D Printing. JACC Cardiovasc. Imaging 2017, 10, 719–731. [Google Scholar] [CrossRef]
- Nedadur, R.; Wang, B.; Tsang, W. Artificial intelligence for the echocardiographic assessment of valvular heart disease. Heart 2022, 108, 1592–1599. [Google Scholar] [CrossRef]
- Mahmood, F.; Jeganathan, J.; Knio, Z.; Amador, Y.; Hai, T.; Khamooshian, A.; Matyal, R.; Khabbaz, K.R. Artificial intelligence in mitral valve analysis. Ann. Card. Anaesth. 2017, 20, 129–134. [Google Scholar] [CrossRef]
- Casaclang-Verzosa, G.; Shrestha, S.; Khalil, M.J.; Cho, J.S.; Tokodi, M.; Balla, S.; Alkhouli, M.; Badhwar, V.; Narula, J.; Miller, J.D.; et al. Network Tomography for Understanding Phenotypic Presentations in Aortic Stenosis. JACC Cardiovasc. Imaging 2019, 12, 236–248. [Google Scholar] [CrossRef]
- Fatima, H.; Mahmood, F.; Sehgal, S.; Belani, K.; Sharkey, A.; Chaudhary, O.; Baribeau, Y.; Matyal, R.; Khabbaz, K.R. Artificial Intelligence for Dynamic Echocardiographic Tricuspid Valve Analysis: A New Tool in Echocardiography. J. Cardiothorac. Vasc. Anesth. 2020, 34, 2703–2706. [Google Scholar] [CrossRef]


















Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prandi, F.R.; Lerakis, S.; Belli, M.; Illuminato, F.; Margonato, D.; Barone, L.; Muscoli, S.; Chiocchi, M.; Laudazi, M.; Marchei, M.; et al. Advances in Imaging for Tricuspid Transcatheter Edge-to-Edge Repair: Lessons Learned and Future Perspectives. J. Clin. Med. 2023, 12, 3384. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12103384
Prandi FR, Lerakis S, Belli M, Illuminato F, Margonato D, Barone L, Muscoli S, Chiocchi M, Laudazi M, Marchei M, et al. Advances in Imaging for Tricuspid Transcatheter Edge-to-Edge Repair: Lessons Learned and Future Perspectives. Journal of Clinical Medicine. 2023; 12(10):3384. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12103384
Chicago/Turabian StylePrandi, Francesca Romana, Stamatios Lerakis, Martina Belli, Federica Illuminato, Davide Margonato, Lucy Barone, Saverio Muscoli, Marcello Chiocchi, Mario Laudazi, Massimo Marchei, and et al. 2023. "Advances in Imaging for Tricuspid Transcatheter Edge-to-Edge Repair: Lessons Learned and Future Perspectives" Journal of Clinical Medicine 12, no. 10: 3384. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12103384