

Personalized Respiratory Support in ARDS: A Physiology-to-Bedside Review
 , , , and
, , , and
Abstract
:
1. Introduction
2. The Concept of Baby Lung
2.1. Patient Self-Inflicted Lung Injury (P-SILI)
2.2. Ventilator-Induced Lung Injury (VILI)
3. Noninvasive Support
3.1. The Benefits and Harms of Maintaining Spontaneous Breathing
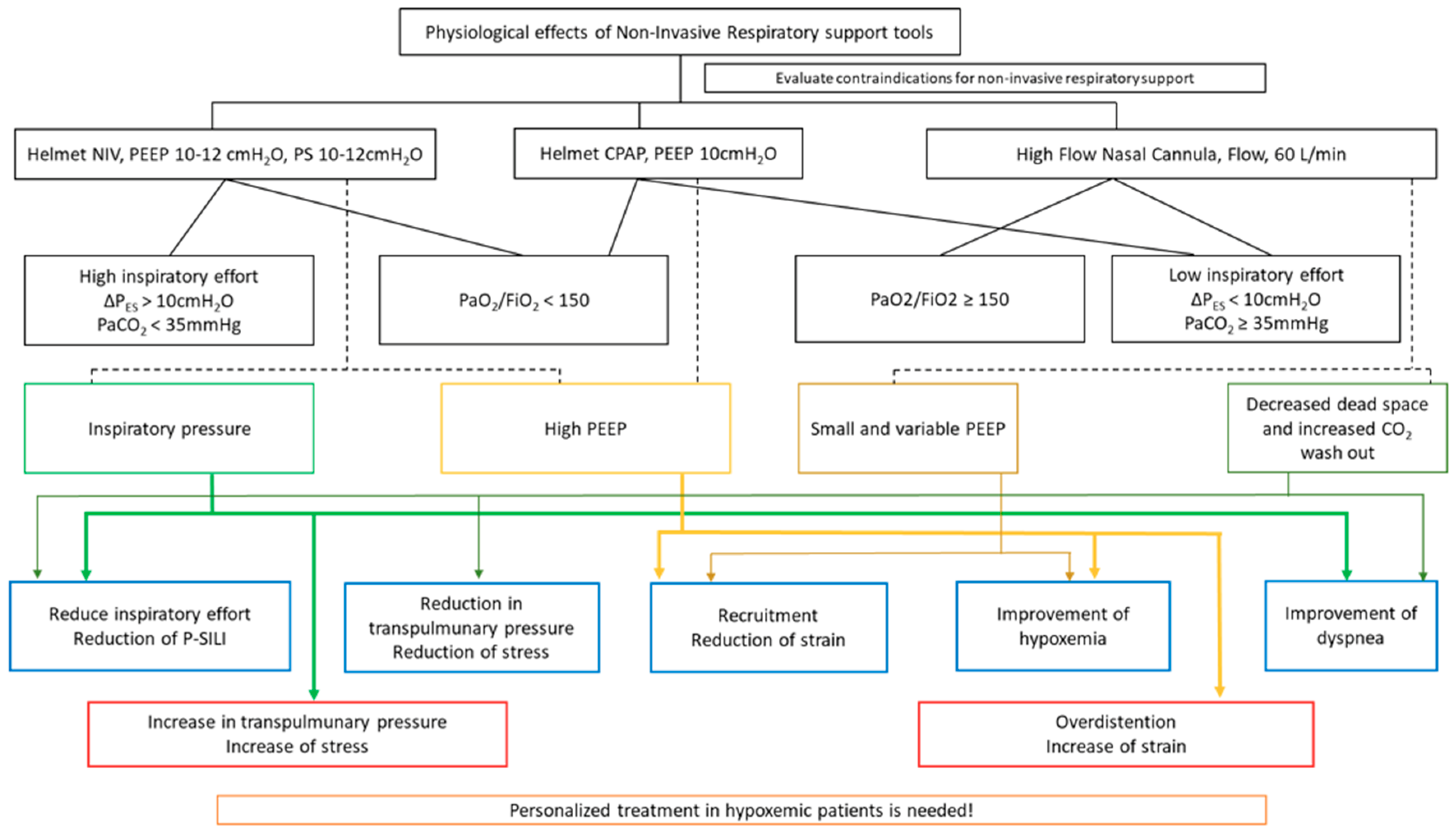
3.2. Strategies and Setting
3.2.1. High-Flow Oxygen Therapy
3.2.2. Continuous Positive Airway Pressure
3.2.3. Noninvasive Ventilation
3.3. Clinical Evidence
3.4. Physiological Rationale for Using High PEEP
3.5. How to Assess the Safety of Spontaneous Breathing
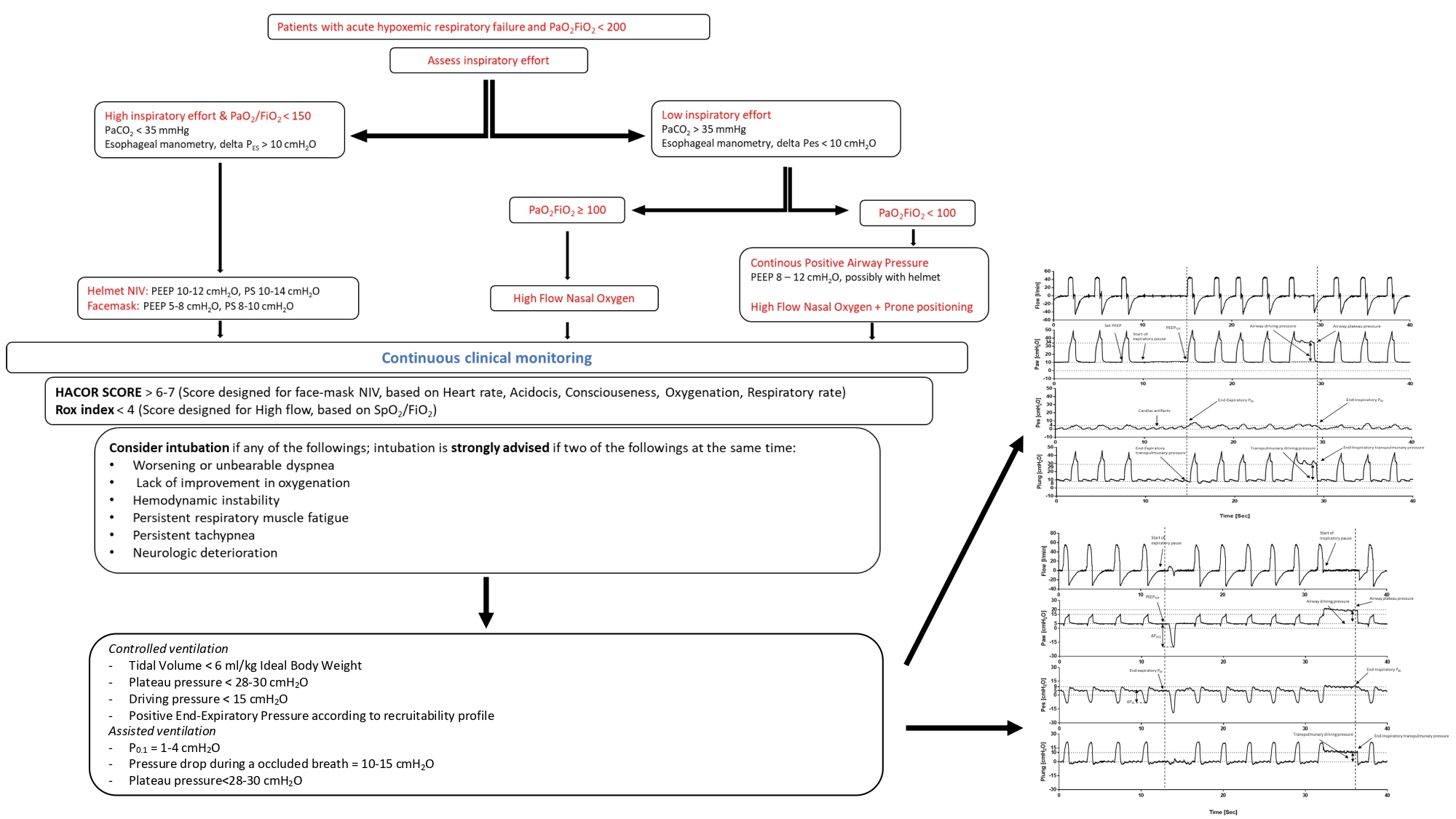
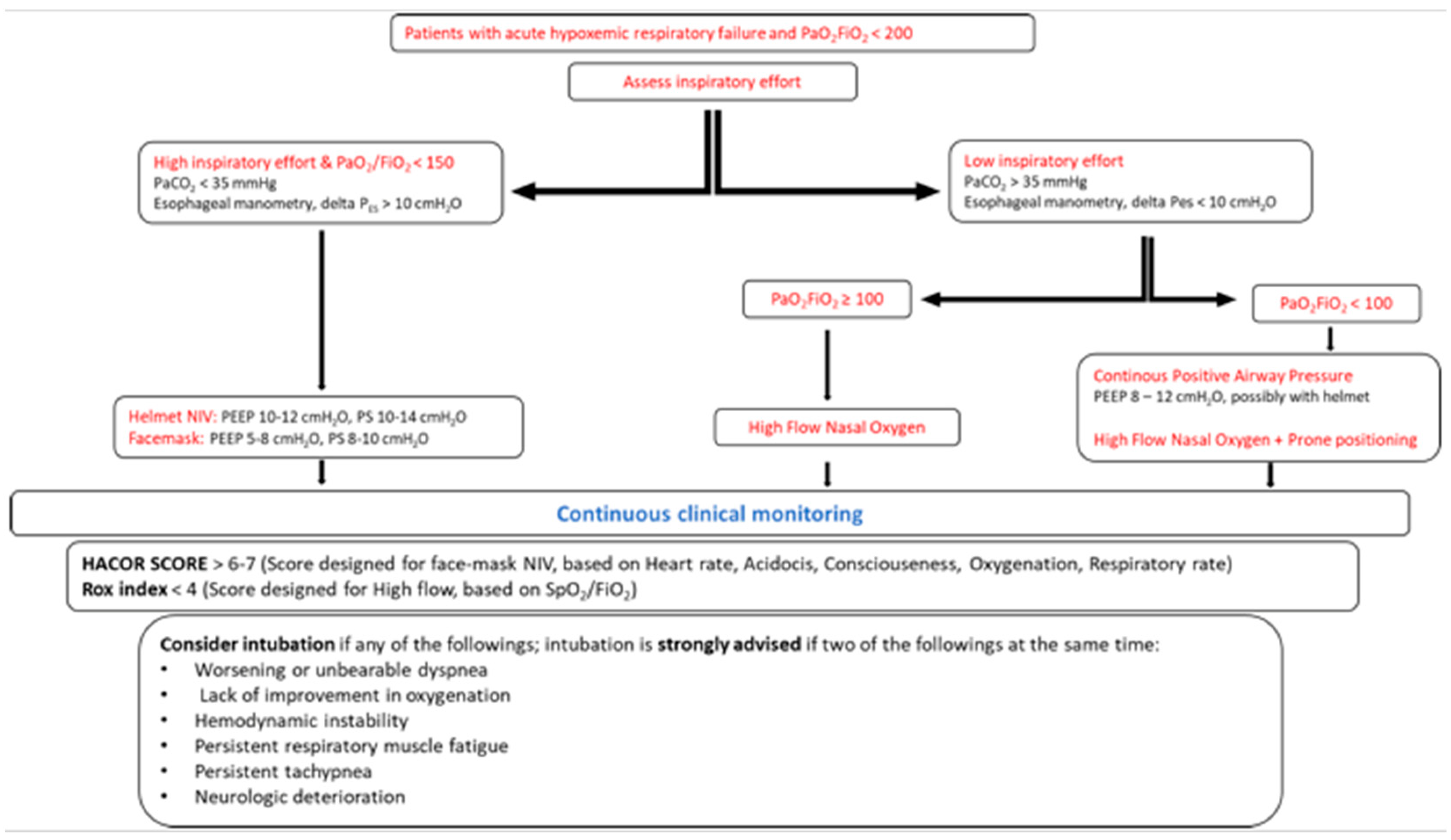
3.6. Monitoring Tools of NIRS Failure
- An expired tidal volume of >9–9.5 mL/kg predicts the body weight and may predict facemask-NIV failure [80], but it is not applicable during helmet-NIV;
- The inspiratory effort assessed by ΔPES > 15 cmH2O or lack of early ΔPES reduction over time (within the first 2 h of treatment) may predict NIV failure at 24 h [81];
- The ROX index, defined as the ratio of SpO2/FIO2 to respiratory rate, may identify patients at risk of HFOT failure and the need for intubation and invasive mechanical ventilation [82]. Additionally, the ROX index has been recently demonstrated to moderately predict NIV failure in patients with AHRF [83];
- The HACOR scale takes into account heart rate, acidosis, stream of consciousness, oxygenation, and respiratory rate, with highest possible score of 25 points. Specifically, a score of 5 as the cutoff has a good diagnostic accuracy for identifying patients at risk of NIV failure in the different subgroups classified for diagnosis, age, disease severity, and those at a different timepoint. In those patients with a HACOR score > 5 at 1 h after NIV initiation, early intubation (≤12 h) may decrease hospital mortality [79]. Recently, Duan et al. [84] reported a significantly improved predictive power for NIV failure in an updated version of the HACOR scale that takes into account six baseline variables (pneumonia, cardiogenic pulmonary edema, pulmonary ARDS, immunosuppression, septic shock, and the SOFA score). Patients with updated HACOR scores of ≤7, 7.5–10.5, 11–14, and >14 were classified at a low, moderate, high, and very high probability of NIV failure.
4. Invasive Mechanical Ventilation
4.1. Main Aims
4.2. Controlled Mechanical Ventilation
4.3. How to Set VT
4.4. How to Set PEEP
- The recruitment-to-inflation ratio (R/I): this index reflects the amount of recruited lung units that are normalized to the CRS during a single-breath de-recruitment maneuver [110] from high PEEP (15 cmH2O) to low PEEP (5 cmH2O) while taking into account the airway opening pressure [111]. Briefly, a R/I ratio above 0.5 identifies patients for whom a higher PEEP level increases the FRC with negligible alveolar hyperinflation, while a R/I ratio below 0.5 identifies those who develop PEEP-induced hyperinflation and may benefit from lower PEEP levels. A clinical trial investigating whether a PEEP-setting strategy based on the R/I ratio can improve clinical outcome in ARDS is currently ongoing (NCT03963622).
- Electrical impedance tomography (EIT): this is a noninvasive, radiation-free imaging method that tracks the global and regional lung volume changes induced by PEEP. EIT shows good reliability in the assessment of lung recruitment vs. hyperinflation compared with CT-scans [112]. For instance, in a supine position, the percent of the dorsal-to-ventral thorax diameter is expressed as the center of ventilation (COV) [113], and this may help to describe the distribution of VT between the ventral nondependent aerated lung regions (COV > 50%) vs. dorsal-dependent non-aerated lung regions (COV < 50%). Accordingly, a COV > 50% may be a marker of the inhomogeneous VT distribution that is associated with a high risk of ventral hyperinflation and dorsal atelectasis. Moreover, EIT provides functional information on the recruitable alveolar collapse by measuring changes in pixel compliance via a decremental PEEP trial: a decreased pixel compliance when lowering PEEP is suggestive of collapse, thus indicating potential for recruitment, whereas increased pixel compliance is suggestive of overdistention [112]. Future clinical investigations in this context are urgently needed.
- Esophageal manometry: this method measures Pes, which is an estimation of PPL in the mid-thorax region adjacent to the esophageal balloon. A recent validation study on supine pigs and human cadavers [114] showed that injured lungs exhibit a vertical PPL gradient, which increases from ventral non-dependent regions to dorsal-dependent lung regions. The PL can be estimated by the equation of motion that substitutes PPL with the end-expiratory PES and by the elastance-derived method at end inspiration, whose value is representative of the non-dependent part of the chest cavity [74,102]. In this context, a post hoc analysis of the EPVent-2 (esophageal pressure-guided ventilation 2) trial [115] found a significant improvement in ventilator-free, shock-free days and in the survival rates, regardless of the treatment group, among patients receiving PEEP and yielding a positive end-expiratory PL close to 0 cmH2O. This finding may be particularly of interest in the management of obese patients with considerable chest wall elastance that leads to high ΔP, even when the PL remains within safe limits [116]. In this context, a PEEP-setting strategy for obtaining a positive end-expiratory PL was associated with survival improvement in a large multicenter study [117].
- Volumetric capnography (Vcap) is a noninvasive tool that may help to assess the amount of alveolar and airway dead space [118], which are directly associated with increased mortality in patients with ARDS [119]. In ARDS patients, preliminary evidence has suggested a role for Vcap in PEEP titration in terms of reaching the highest compliance in conjunction with the lowest ratio of dead space to VT [120]. Although this tool may provide important insight into lung mechanics, especially when esophageal manometry is not available at the bedside, it warrants further investigation to clarify its role in the setting of ARDS.
4.5. How to Assess the Safety of Assisted Invasive Mechanical Ventilation
5. Neuromuscular Blockage, Prone Position, and Inhaled Pulmonary Vasodilators
5.1. Neuromuscular Blocking Agent
5.2. Prone Position
5.3. Inhaled Pulmonary Vasodilators
6. Potential Issues for the Implementation of Personalized Respiratory Support Strategies and Eventual Solutions
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bellani, G.; Laffey, J.G.; Pham, T.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; van Haren, F.; Larsson, A.; McAuley, D.F.; et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA 2016, 315, 788–800. [Google Scholar] [CrossRef] [PubMed]
- Fanelli, V.; Ranieri, V.M. Mechanisms and clinical consequences of acute lung injury. Ann. Am. Thorac. Soc. 2015, 12 (Suppl. S1), S3–S8. [Google Scholar] [CrossRef]
- Thompson, B.T.; Chambers, R.C.; Liu, K.D. Acute respiratory distress syndrome. N. Engl. J. Med. 2017, 377, 562–572. [Google Scholar] [CrossRef]
- Gattinoni, L.; Pesenti, A. The concept of “baby lung”. Intensive Care Med. 2005, 31, 776–784. [Google Scholar] [CrossRef]
- Ashbaugh, D.G.; Bigelow, D.B.; Petty, T.L.; Levine, B.E. Acute respiratory distress in adults. Lancet 1967, 2, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Force, A.D.T.; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The berlin definition. JAMA 2012, 307, 2526–2533. [Google Scholar]
- Ranieri, V.M.; Tonetti, T.; Navalesi, P.; Nava, S.; Antonelli, M.; Pesenti, A.; Grasselli, G.; Grieco, D.L.; Menga, L.S.; Pisani, L.; et al. High-flow nasal oxygen for severe hypoxemia: Oxygenation response and outcome in patients with COVID-19. Am. J. Respir. Crit. Care Med. 2022, 205, 431–439. [Google Scholar] [CrossRef] [PubMed]
- Rochwerg, B.; Brochard, L.; Elliott, M.W.; Hess, D.; Hill, N.S.; Nava, S.; Navalesi, P.; Antonelli, M.; Brozek, J.; Conti, G.; et al. Official ers/ats clinical practice guidelines: Noninvasive ventilation for acute respiratory failure. Eur. Respir. J. 2017, 50, 1602426. [Google Scholar] [CrossRef] [Green Version]
- Fan, E.; Del Sorbo, L.; Goligher, E.C.; Hodgson, C.L.; Munshi, L.; Walkey, A.J.; Adhikari, N.K.J.; Amato, M.B.P.; Branson, R.; Brower, R.G.; et al. An official american thoracic society/european society of intensive care medicine/society of critical care medicine clinical practice guideline: Mechanical ventilation in adult patients with acute respiratory distress syndrome. Am. J. Respir. Crit Care Med. 2017, 195, 1253–1263. [Google Scholar] [CrossRef]
- Bos, L.D.J.; Ware, L.B. Acute respiratory distress syndrome: Causes, pathophysiology, and phenotypes. Lancet 2022, 400, 1145–1156. [Google Scholar] [CrossRef]
- Maddali, M.V.; Churpek, M.; Pham, T.; Rezoagli, E.; Zhuo, H.; Zhao, W.; He, J.; Delucchi, K.L.; Wang, C.; Wickersham, N.; et al. Validation and utility of ards subphenotypes identified by machine-learning models using clinical data: An observational, multicohort, retrospective analysis. Lancet Respir. Med. 2022, 10, 367–377. [Google Scholar] [CrossRef]
- Matthay, M.A.; Arabi, Y.M.; Siegel, E.R.; Ware, L.B.; Bos, L.D.J.; Sinha, P.; Beitler, J.R.; Wick, K.D.; Curley, M.A.Q.; Constantin, J.M.; et al. Phenotypes and personalized medicine in the acute respiratory distress syndrome. Intensive Care Med. 2020, 46, 2136–2152. [Google Scholar] [CrossRef]
- Calfee, C.S.; Delucchi, K.; Parsons, P.E.; Thompson, B.T.; Ware, L.B.; Matthay, M.A.; Network, N.A. Subphenotypes in acute respiratory distress syndrome: Latent class analysis of data from two randomised controlled trials. Lancet Respir. Med. 2014, 2, 611–620. [Google Scholar] [CrossRef] [Green Version]
- Gattinoni, L.; Pesenti, D. Ards: The non-homogeneous lung; facts and hypothesis. Intensive Crit. Care Dig. 1987, 6, 4. [Google Scholar]
- Gattinoni, L.; Pesenti, A.; Avalli, L.; Rossi, F.; Bombino, M. Pressure-volume curve of total respiratory system in acute respiratory failure. Computed tomographic scan study. Am. Rev. Respir. Dis. 1987, 136, 730–736. [Google Scholar] [CrossRef] [PubMed]
- Gattinoni, L.; Pesenti, A.; Baglioni, S.; Vitale, G.; Rivolta, M.; Pelosi, P. Inflammatory pulmonary edema and positive end-expiratory pressure: Correlations between imaging and physiologic studies. J. Thorac. Imaging 1988, 3, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Gattinoni, L.; D’Andrea, L.; Pelosi, P.; Vitale, G.; Pesenti, A.; Fumagalli, R. Regional effects and mechanism of positive end-expiratory pressure in early adult respiratory distress syndrome. JAMA 1993, 269, 2122–2127. [Google Scholar] [CrossRef]
- Langer, M.; Mascheroni, D.; Marcolin, R.; Gattinoni, L. The prone position in ards patients. A clinical study. Chest 1988, 94, 103–107. [Google Scholar] [CrossRef]
- Gattinoni, L.; Pelosi, P.; Vitale, G.; Pesenti, A.; D’Andrea, L.; Mascheroni, D. Body position changes redistribute lung computed-tomographic density in patients with acute respiratory failure. Anesthesiology 1991, 74, 15–23. [Google Scholar] [CrossRef]
- Gattinoni, L.; Marini, J.J.; Pesenti, A.; Quintel, M.; Mancebo, J.; Brochard, L. The “baby lung” became an adult. Intensive Care Med. 2016, 42, 663–673. [Google Scholar] [CrossRef] [PubMed]
- Bone, R.C. The ards lung. New insights from computed tomography. JAMA 1993, 269, 2134–2135. [Google Scholar] [CrossRef]
- Yoshida, T.; Grieco, D.L.; Brochard, L.; Fujino, Y. Patient self-inflicted lung injury and positive end-expiratory pressure for safe spontaneous breathing. Curr. Opin. Crit. Care 2020, 26, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Grieco, D.L.; Menga, L.S.; Eleuteri, D.; Antonelli, M. Patient self-inflicted lung injury: Implications for acute hypoxemic respiratory failure and ards patients on non-invasive support. Minerva Anestesiol. 2019, 85, 1014–1023. [Google Scholar] [CrossRef]
- Carteaux, G.; Parfait, M.; Combet, M.; Haudebourg, A.F.; Tuffet, S.; Mekontso Dessap, A. Patient-self inflicted lung injury: A practical review. J. Clin. Med. 2021, 10, 2738. [Google Scholar] [CrossRef] [PubMed]
- Carteaux, G.; Millan-Guilarte, T.; De Prost, N.; Razazi, K.; Abid, S.; Thille, A.W.; Schortgen, F.; Brochard, L.; Brun-Buisson, C.; Mekontso Dessap, A. Failure of noninvasive ventilation for de novo acute hypoxemic respiratory failure: Role of tidal volume. Crit. Care Med. 2016, 44, 282–290. [Google Scholar] [CrossRef] [PubMed]
- Frat, J.P.; Ragot, S.; Coudroy, R.; Constantin, J.M.; Girault, C.; Prat, G.; Boulain, T.; Demoule, A.; Ricard, J.D.; Razazi, K.; et al. Predictors of intubation in patients with acute hypoxemic respiratory failure treated with a noninvasive oxygenation strategy. Crit. Care Med. 2018, 46, 208–215. [Google Scholar] [CrossRef]
- Cressoni, M.; Chiumello, D.; Algieri, I.; Brioni, M.; Chiurazzi, C.; Colombo, A.; Colombo, A.; Crimella, F.; Guanziroli, M.; Tomic, I.; et al. Opening pressures and atelectrauma in acute respiratory distress syndrome. Intensive Care Med. 2017, 43, 603–611. [Google Scholar] [CrossRef]
- Chiumello, D.; Chierichetti, M.; Tallarini, F.; Cozzi, P.; Cressoni, M.; Polli, F.; Colombo, R.; Castelli, A.; Gattinoni, L. Effect of a heated humidifier during continuous positive airway pressure delivered by a helmet. Crit. Care 2008, 12, R55. [Google Scholar] [CrossRef] [Green Version]
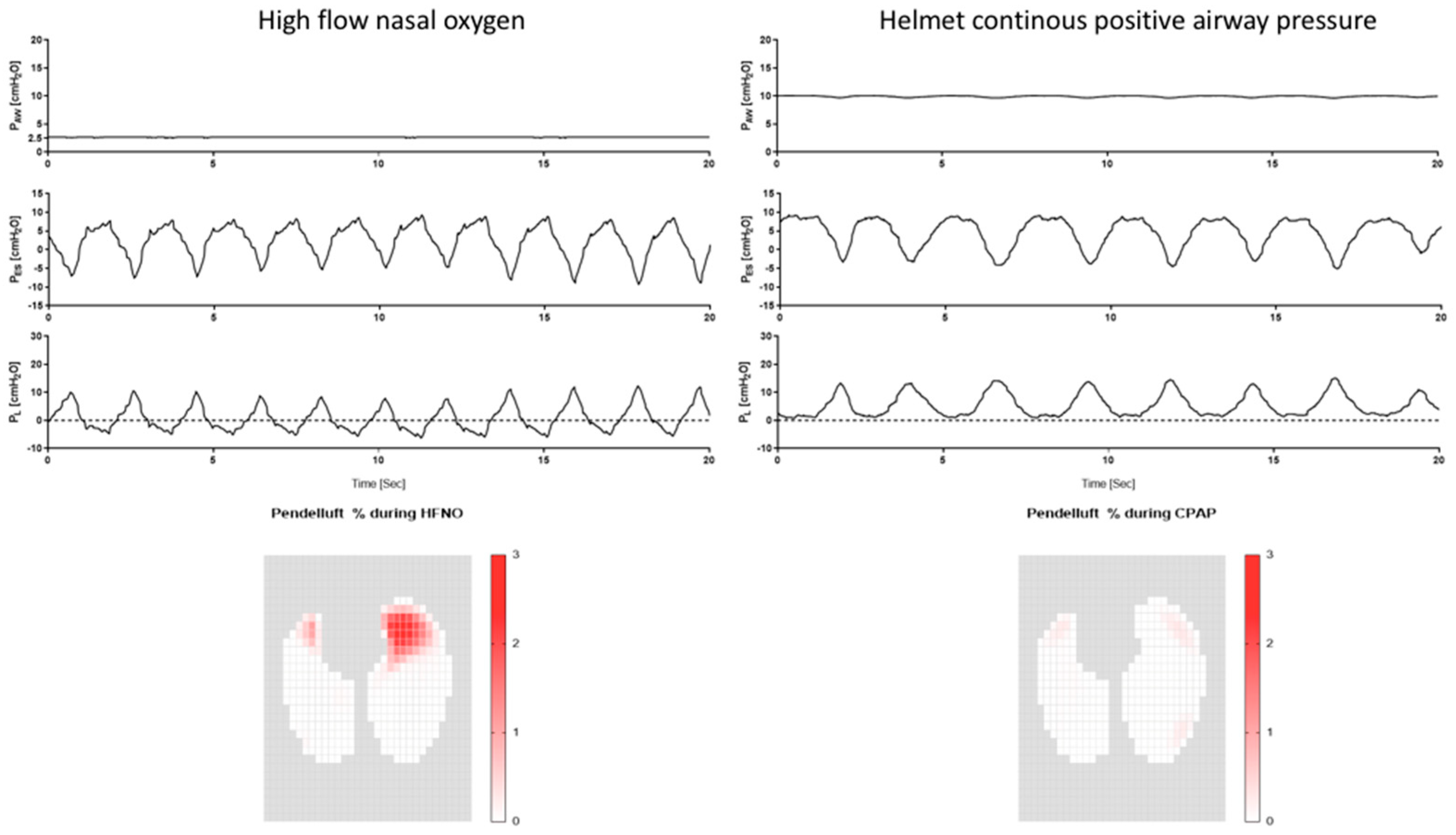
- Yoshida, T.; Torsani, V.; Gomes, S.; De Santis, R.R.; Beraldo, M.A.; Costa, E.L.; Tucci, M.R.; Zin, W.A.; Kavanagh, B.P.; Amato, M.B. Spontaneous effort causes occult pendelluft during mechanical ventilation. Am. J. Respir. Crit. Care Med. 2013, 188, 1420–1427. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, T.; Roldan, R.; Beraldo, M.A.; Torsani, V.; Gomes, S.; De Santis, R.R.; Costa, E.L.; Tucci, M.R.; Lima, R.G.; Kavanagh, B.P.; et al. Spontaneous effort during mechanical ventilation: Maximal injury with less positive end-expiratory pressure. Crit. Care Med. 2016, 44, e678–e688. [Google Scholar] [CrossRef] [PubMed]
- Slutsky, A.S.; Ranieri, V.M. Ventilator-induced lung injury. N. Engl. J. Med. 2013, 369, 2126–2136. [Google Scholar] [CrossRef] [Green Version]
- Kumar, A.; Pontoppidan, H.; Falke, K.J.; Wilson, R.S.; Laver, M.B. Pulmonary barotrauma during mechanical ventilation. Crit. Care Med. 1973, 1, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Slutsky, A.S. Lung injury caused by mechanical ventilation. Chest 1999, 116, 9S–15S. [Google Scholar] [CrossRef] [PubMed]
- Grieco, D.L.; Maggiore, S.M.; Roca, O.; Spinelli, E.; Patel, B.K.; Thille, A.W.; Barbas, C.S.V.; de Acilu, M.G.; Cutuli, S.L.; Bongiovanni, F.; et al. Non-invasive ventilatory support and high-flow nasal oxygen as first-line treatment of acute hypoxemic respiratory failure and ards. Intensive Care Med. 2021, 47, 851–866. [Google Scholar] [CrossRef]
- Luyt, C.E.; Bouadma, L.; Morris, A.C.; Dhanani, J.A.; Kollef, M.; Lipman, J.; Martin-Loeches, I.; Nseir, S.; Ranzani, O.T.; Roquilly, A.; et al. Pulmonary infections complicating ards. Intensive Care Med. 2020, 46, 2168–2183. [Google Scholar] [CrossRef]
- Antonelli, M.; Conti, G.; Rocco, M.; Bufi, M.; De Blasi, R.A.; Vivino, G.; Gasparetto, A.; Meduri, G.U. A comparison of noninvasive positive-pressure ventilation and conventional mechanical ventilation in patients with acute respiratory failure. N. Engl. J. Med. 1998, 339, 429–435. [Google Scholar] [CrossRef] [Green Version]
- Putensen, C.; Mutz, N.J.; Putensen-Himmer, G.; Zinserling, J. Spontaneous breathing during ventilatory support improves ventilation-perfusion distributions in patients with acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 1999, 159, 1241–1248. [Google Scholar] [CrossRef]
- Chanques, G.; Constantin, J.M.; Devlin, J.W.; Ely, E.W.; Fraser, G.L.; Gelinas, C.; Girard, T.D.; Guerin, C.; Jabaudon, M.; Jaber, S.; et al. Analgesia and sedation in patients with ards. Intensive Care Med. 2020, 46, 2342–2356. [Google Scholar] [CrossRef]
- Alhazzani, W.; Belley-Cote, E.; Moller, M.H.; Angus, D.C.; Papazian, L.; Arabi, Y.M.; Citerio, G.; Connolly, B.; Denehy, L.; Fox-Robichaud, A.; et al. Neuromuscular blockade in patients with ards: A rapid practice guideline. Intensive Care Med. 2020, 46, 1977–1986. [Google Scholar] [CrossRef] [PubMed]
- Bellani, G.; Laffey, J.G.; Pham, T.; Madotto, F.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; Bumbasirevic, V.; Piquilloud, L.; et al. Noninvasive ventilation of patients with acute respiratory distress syndrome. Insights from the lung safe study. Am. J. Respir. Crit. Care Med. 2017, 195, 67–77. [Google Scholar] [CrossRef] [Green Version]
- Demoule, A.; Girou, E.; Richard, J.C.; Taille, S.; Brochard, L. Benefits and risks of success or failure of noninvasive ventilation. Intensive Care Med. 2006, 32, 1756–1765. [Google Scholar] [CrossRef]
- Brochard, L.; Slutsky, A.; Pesenti, A. Mechanical ventilation to minimize progression of lung injury in acute respiratory failure. Am. J. Respir. Crit. Care Med. 2017, 195, 438–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cesarano, M.; Grieco, D.L.; Michi, T.; Munshi, L.; Menga, L.S.; Delle Cese, L.; Ruggiero, E.; Rosa, T.; Natalini, D.; Sklar, M.C.; et al. Helmet noninvasive support for acute hypoxemic respiratory failure: Rationale, mechanism of action and bedside application. Ann. Intensive Care 2022, 12, 94. [Google Scholar] [CrossRef]
- Cutuli, S.L.; Grieco, D.L.; Menga, L.S.; De Pascale, G.; Antonelli, M. Noninvasive ventilation and high-flow oxygen therapy for severe community-acquired pneumonia. Curr. Opin. Infect. Dis. 2021, 34, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Rochwerg, B.; Einav, S.; Chaudhuri, D.; Mancebo, J.; Mauri, T.; Helviz, Y.; Goligher, E.C.; Jaber, S.; Ricard, J.D.; Rittayamai, N.; et al. The role for high flow nasal cannula as a respiratory support strategy in adults: A clinical practice guideline. Intensive Care Med. 2020, 46, 2226–2237. [Google Scholar] [CrossRef] [PubMed]
- Natalini, D.; Grieco, D.L.; Santantonio, M.T.; Mincione, L.; Toni, F.; Anzellotti, G.M.; Eleuteri, D.; Di Giannatale, P.; Antonelli, M.; Maggiore, S.M. Physiological effects of high-flow oxygen in tracheostomized patients. Ann. Intensive Care 2019, 9, 114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiumello, D.; Pelosi, P.; Carlesso, E.; Severgnini, P.; Aspesi, M.; Gamberoni, C.; Antonelli, M.; Conti, G.; Chiaranda, M.; Gattinoni, L. Noninvasive positive pressure ventilation delivered by helmet vs. Standard face mask. Intensive Care Med. 2003, 29, 1671–1679. [Google Scholar] [CrossRef]
- Taccone, P.; Hess, D.; Caironi, P.; Bigatello, L.M. Continuous positive airway pressure delivered with a “helmet”: Effects on carbon dioxide rebreathing. Crit. Care Med. 2004, 32, 2090–2096. [Google Scholar] [CrossRef]
- Mojoli, F.; Iotti, G.A.; Gerletti, M.; Lucarini, C.; Braschi, A. Carbon dioxide rebreathing during non-invasive ventilation delivered by helmet: A bench study. Intensive Care Med. 2008, 34, 1454–1460. [Google Scholar] [CrossRef]
- MacIntyre, N.R. Physiologic effects of noninvasive ventilation. Respir. Care 2019, 64, 617–628. [Google Scholar] [CrossRef]
- L’Her, E.; Deye, N.; Lellouche, F.; Taille, S.; Demoule, A.; Fraticelli, A.; Mancebo, J.; Brochard, L. Physiologic effects of noninvasive ventilation during acute lung injury. Am. J. Respir. Crit. Care Med. 2005, 172, 1112–1118. [Google Scholar] [CrossRef]
- Mehta, S.; Hill, N.S. Noninvasive ventilation. Am. J. Respir. Crit. Care Med. 2001, 163, 540–577. [Google Scholar] [CrossRef] [PubMed]
- Cabrini, L.; Landoni, G.; Oriani, A.; Plumari, V.P.; Nobile, L.; Greco, M.; Pasin, L.; Beretta, L.; Zangrillo, A. Noninvasive ventilation and survival in acute care settings: A comprehensive systematic review and metaanalysis of randomized controlled trials. Crit. Care Med. 2015, 43, 880–888. [Google Scholar] [CrossRef] [PubMed]
- Luce, J.M. The cardiovascular effects of mechanical ventilation and positive end-expiratory pressure. JAMA 1984, 252, 807–811. [Google Scholar] [CrossRef] [PubMed]
- Luecke, T.; Pelosi, P. Clinical review: Positive end-expiratory pressure and cardiac output. Crit. Care 2005, 9, 607–621. [Google Scholar] [CrossRef] [Green Version]
- Ueta, K.; Tomita, T.; Uchiyama, A.; Ohta, N.; Iguchi, N.; Goto, Y.; Fujino, Y. Influence of humidification on comfort during noninvasive ventilation with a helmet. Respir. Care 2013, 58, 798–804. [Google Scholar] [CrossRef] [Green Version]
- Lucchini, A.; Bambi, S.; Elli, S.; Bruno, M.; Dallari, R.; Puccio, P.; Villa, S.; Rona, R.; Fumagalli, R.; Bellani, G.; et al. Water content of delivered gases during helmet continuous positive airway pressure in healthy subjects. Acta Biomed. 2019, 90, 65–71. [Google Scholar]
- Lenique, F.; Habis, M.; Lofaso, F.; Dubois-Rande, J.L.; Harf, A.; Brochard, L. Ventilatory and hemodynamic effects of continuous positive airway pressure in left heart failure. Am. J. Respir. Crit. Care Med. 1997, 155, 500–505. [Google Scholar] [CrossRef]
- Rittayamai, N.; Beloncle, F.; Goligher, E.C.; Chen, L.; Mancebo, J.; Richard, J.M.; Brochard, L. Effect of inspiratory synchronization during pressure-controlled ventilation on lung distension and inspiratory effort. Ann. Intensive Care 2017, 7, 100. [Google Scholar] [CrossRef] [Green Version]
- Richard, J.C.; Lyazidi, A.; Akoumianaki, E.; Mortaza, S.; Cordioli, R.L.; Lefebvre, J.C.; Rey, N.; Piquilloud, L.; Sferrazza Papa, G.F.; Mercat, A.; et al. Potentially harmful effects of inspiratory synchronization during pressure preset ventilation. Intensive Care Med. 2013, 39, 2003–2010. [Google Scholar] [CrossRef] [Green Version]
- Grieco, D.L.; Menga, L.S.; Raggi, V.; Bongiovanni, F.; Anzellotti, G.M.; Tanzarella, E.S.; Bocci, M.G.; Mercurio, G.; Dell’Anna, A.M.; Eleuteri, D.; et al. Physiological comparison of high-flow nasal cannula and helmet noninvasive ventilation in acute hypoxemic respiratory failure. Am. J. Respir. Crit. Care Med. 2020, 201, 303–312. [Google Scholar] [CrossRef]
- Frat, J.P.; Thille, A.W.; Mercat, A.; Girault, C.; Ragot, S.; Perbet, S.; Prat, G.; Boulain, T.; Morawiec, E.; Cottereau, A.; et al. High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure. N. Engl. J. Med. 2015, 372, 2185–2196. [Google Scholar] [CrossRef] [Green Version]
- Ospina-Tascon, G.A.; Calderon-Tapia, L.E.; Garcia, A.F.; Zarama, V.; Gomez-Alvarez, F.; Alvarez-Saa, T.; Pardo-Otalvaro, S.; Bautista-Rincon, D.F.; Vargas, M.P.; Aldana-Diaz, J.L.; et al. Effect of high-flow oxygen therapy vs conventional oxygen therapy on invasive mechanical ventilation and clinical recovery in patients with severe COVID-19: A randomized clinical trial. JAMA 2021, 326, 2161–2171. [Google Scholar] [CrossRef] [PubMed]
- Ferreyro, B.L.; Angriman, F.; Munshi, L.; Del Sorbo, L.; Ferguson, N.D.; Rochwerg, B.; Ryu, M.J.; Saskin, R.; Wunsch, H.; da Costa, B.R.; et al. Association of noninvasive oxygenation strategies with all-cause mortality in adults with acute hypoxemic respiratory failure: A systematic review and meta-analysis. JAMA 2020, 324, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Perkins, G.D.; Ji, C.; Connolly, B.A.; Couper, K.; Lall, R.; Baillie, J.K.; Bradley, J.M.; Dark, P.; Dave, C.; De Soyza, A.; et al. Effect of noninvasive respiratory strategies on intubation or mortality among patients with acute hypoxemic respiratory failure and COVID-19: The recovery-rs randomized clinical trial. JAMA 2022, 327, 546–558. [Google Scholar] [CrossRef] [PubMed]
- Grieco, D.L.; Menga, L.S.; Cesarano, M.; Rosa, T.; Spadaro, S.; Bitondo, M.M.; Montomoli, J.; Falo, G.; Tonetti, T.; Cutuli, S.L.; et al. Effect of helmet noninvasive ventilation vs high-flow nasal oxygen on days free of respiratory support in patients with COVID-19 and moderate to severe hypoxemic respiratory failure: The henivot randomized clinical trial. JAMA 2021, 325, 1731–1743. [Google Scholar] [CrossRef]
- Arabi, Y.M.; Aldekhyl, S.; Al Qahtani, S.; Al-Dorzi, H.M.; Abdukahil, S.A.; Al Harbi, M.K.; Al Qasim, E.; Kharaba, A.; Albrahim, T.; Alshahrani, M.S.; et al. Effect of helmet noninvasive ventilation vs usual respiratory support on mortality among patients with acute hypoxemic respiratory failure due to COVID-19: The helmet-covid randomized clinical trial. JAMA 2022, 328, 1063–1072. [Google Scholar] [CrossRef] [PubMed]
- Radermacher, P.; Maggiore, S.M.; Mercat, A. Fifty years of research in ards. Gas exchange in acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2017, 196, 964–984. [Google Scholar] [CrossRef]
- Morais, C.C.A.; Koyama, Y.; Yoshida, T.; Plens, G.M.; Gomes, S.; Lima, C.A.S.; Ramos, O.P.S.; Pereira, S.M.; Kawaguchi, N.; Yamamoto, H.; et al. High positive end-expiratory pressure renders spontaneous effort noninjurious. Am. J. Respir. Crit. Care Med. 2018, 197, 1285–1296. [Google Scholar] [CrossRef]
- Lindqvist, J.; van den Berg, M.; van der Pijl, R.; Hooijman, P.E.; Beishuizen, A.; Elshof, J.; de Waard, M.; Girbes, A.; Spoelstra-de Man, A.; Shi, Z.H.; et al. Positive end-expiratory pressure ventilation induces longitudinal atrophy in diaphragm fibers. Am. J. Respir. Crit. Care Med. 2018, 198, 472–485. [Google Scholar] [CrossRef]
- Sklienka, P.; Frelich, M.; Bursa, F. Patient self-inflicted lung injury-a narrative review of pathophysiology, early recognition, and management options. J. Pers. Med. 2023, 13, 593. [Google Scholar] [CrossRef] [PubMed]
- Brochard, L.; Harf, A.; Lorino, H.; Lemaire, F. Inspiratory pressure support prevents diaphragmatic fatigue during weaning from mechanical ventilation. Am. Rev. Respir. Dis. 1989, 139, 513–521. [Google Scholar] [CrossRef]
- Brochard, L.; Isabey, D.; Piquet, J.; Amaro, P.; Mancebo, J.; Messadi, A.A.; Brun-Buisson, C.; Rauss, A.; Lemaire, F.; Harf, A. Reversal of acute exacerbations of chronic obstructive lung disease by inspiratory assistance with a face mask. N. Engl. J. Med. 1990, 323, 1523–1530. [Google Scholar] [CrossRef] [PubMed]
- Coudroy, R.; Chen, L.; Pham, T.; Piraino, T.; Telias, I.; Brochard, L. Acute respiratory distress syndrome: Respiratory monitoring and pulmonary physiology. Semin. Respir. Crit. Care Med. 2019, 40, 66–80. [Google Scholar] [CrossRef] [PubMed]
- Dangers, L.; Montlahuc, C.; Kouatchet, A.; Jaber, S.; Meziani, F.; Perbet, S.; Similowski, T.; Resche-Rigon, M.; Azoulay, E.; Demoule, A.; et al. Dyspnoea in patients receiving noninvasive ventilation for acute respiratory failure: Prevalence, risk factors and prognostic impact: A prospective observational study. Eur. Respir. J. 2018, 52, 1702637. [Google Scholar] [CrossRef] [Green Version]
- Grieco, D.L.; Menga, L.S.; Cesarano, M.; Spadaro, S.; Bitondo, M.M.; Berardi, C.; Rosa, T.; Bongiovanni, F.; Maggiore, S.M.; Antonelli, M.; et al. Phenotypes of patients with COVID-19 who have a positive clinical response to helmet noninvasive ventilation. Am. J. Respir. Crit. Care Med. 2022, 205, 360–364. [Google Scholar] [CrossRef]
- Menga, L.S.; Delle Cese, L.; Rosa, T.; Cesarano, M.; Scarascia, R.; Michi, T.; Biasucci, D.G.; Ruggiero, E.; dell’Anna, A.M.; Cutuli, S.L.; et al. Respective effects of helmet pressure support, continuous positive airway pressure and nasal high-flow in hypoxemic respiratory failure: A randomized crossover clinical trial. Am. J. Respir. Crit. Care Med. 2023, 207, 1310–1323. [Google Scholar] [CrossRef]
- Kangelaris, K.N.; Ware, L.B.; Wang, C.Y.; Janz, D.R.; Zhuo, H.; Matthay, M.A.; Calfee, C.S. Timing of intubation and clinical outcomes in adults with acute respiratory distress syndrome. Crit. Care Med. 2016, 44, 120–129. [Google Scholar] [CrossRef]
- Duan, J.; Han, X.; Bai, L.; Zhou, L.; Huang, S. Assessment of heart rate, acidosis, consciousness, oxygenation, and respiratory rate to predict noninvasive ventilation failure in hypoxemic patients. Intensive Care Med. 2017, 43, 192–199. [Google Scholar] [CrossRef]
- Spinelli, E.; Mauri, T.; Beitler, J.R.; Pesenti, A.; Brodie, D. Respiratory drive in the acute respiratory distress syndrome: Pathophysiology, monitoring, and therapeutic interventions. Intensive Care Med. 2020, 46, 606–618. [Google Scholar] [CrossRef] [PubMed]
- Tonelli, R.; Fantini, R.; Tabbi, L.; Castaniere, I.; Pisani, L.; Pellegrino, M.R.; Della Casa, G.; D’Amico, R.; Girardis, M.; Nava, S.; et al. Early inspiratory effort assessment by esophageal manometry predicts noninvasive ventilation outcome in de novo respiratory failure. A pilot study. Am. J. Respir. Crit. Care Med. 2020, 202, 558–567. [Google Scholar] [CrossRef] [Green Version]
- Roca, O.; Caralt, B.; Messika, J.; Samper, M.; Sztrymf, B.; Hernandez, G.; Garcia-de-Acilu, M.; Frat, J.P.; Masclans, J.R.; Ricard, J.D. An index combining respiratory rate and oxygenation to predict outcome of nasal high-flow therapy. Am. J. Respir. Crit. Care Med. 2019, 199, 1368–1376. [Google Scholar] [CrossRef]
- Duan, J.; Yang, J.; Jiang, L.; Bai, L.; Hu, W.; Shu, W.; Wang, K.; Yang, F. Prediction of noninvasive ventilation failure using the rox index in patients with de novo acute respiratory failure. Ann. Intensive Care 2022, 12, 110. [Google Scholar] [CrossRef]
- Duan, J.; Chen, L.; Liu, X.; Bozbay, S.; Liu, Y.; Wang, K.; Esquinas, A.M.; Shu, W.; Yang, F.; He, D.; et al. An updated hacor score for predicting the failure of noninvasive ventilation: A multicenter prospective observational study. Crit. Care 2022, 26, 196. [Google Scholar] [CrossRef]
- Lassen, H.C. A preliminary report on the 1952 epidemic of poliomyelitis in copenhagen with special reference to the treatment of acute respiratory insufficiency. Lancet 1953, 1, 37–41. [Google Scholar] [CrossRef]
- Papazian, L.; Forel, J.M.; Gacouin, A.; Penot-Ragon, C.; Perrin, G.; Loundou, A.; Jaber, S.; Arnal, J.M.; Perez, D.; Seghboyan, J.M.; et al. Neuromuscular blockers in early acute respiratory distress syndrome. N. Engl. J. Med. 2010, 363, 1107–1116. [Google Scholar] [CrossRef] [Green Version]
- National Heart, L.; Blood Institute, P.C.T.N.; Moss, M.; Huang, D.T.; Brower, R.G.; Ferguson, N.D.; Ginde, A.A.; Gong, M.N.; Grissom, C.K.; Gundel, S.; et al. Early neuromuscular blockade in the acute respiratory distress syndrome. N. Engl. J. Med. 2019, 380, 1997–2008. [Google Scholar]
- Dreyfuss, D.; Soler, P.; Basset, G.; Saumon, G. High inflation pressure pulmonary edema. Respective effects of high airway pressure, high tidal volume, and positive end-expiratory pressure. Am. Rev. Respir. Dis. 1988, 137, 1159–1164. [Google Scholar] [CrossRef]
- Amato, M.B.; Barbas, C.S.; Medeiros, D.M.; Magaldi, R.B.; Schettino, G.P.; Lorenzi-Filho, G.; Kairalla, R.A.; Deheinzelin, D.; Munoz, C.; Oliveira, R.; et al. Effect of a protective-ventilation strategy on mortality in the acute respiratory distress syndrome. N. Engl. J. Med. 1998, 338, 347–354. [Google Scholar] [CrossRef]
- Acute Respiratory Distress Syndrome, N.; Brower, R.G.; Matthay, M.A.; Morris, A.; Schoenfeld, D.; Thompson, B.T.; Wheeler, A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N. Engl. J. Med. 2000, 342, 1301–1308. [Google Scholar]
- Terragni, P.P.; Rosboch, G.; Tealdi, A.; Corno, E.; Menaldo, E.; Davini, O.; Gandini, G.; Herrmann, P.; Mascia, L.; Quintel, M.; et al. Tidal hyperinflation during low tidal volume ventilation in acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2007, 175, 160–166. [Google Scholar] [CrossRef]
- Chiumello, D.; Carlesso, E.; Cadringher, P.; Caironi, P.; Valenza, F.; Polli, F.; Tallarini, F.; Cozzi, P.; Cressoni, M.; Colombo, A.; et al. Lung stress and strain during mechanical ventilation for acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2008, 178, 346–355. [Google Scholar] [CrossRef] [Green Version]
- Amato, M.B.; Meade, M.O.; Slutsky, A.S.; Brochard, L.; Costa, E.L.; Schoenfeld, D.A.; Stewart, T.E.; Briel, M.; Talmor, D.; Mercat, A.; et al. Driving pressure and survival in the acute respiratory distress syndrome. N. Engl. J. Med. 2015, 372, 747–755. [Google Scholar] [CrossRef] [Green Version]
- Gattinoni, L.; Tonetti, T.; Cressoni, M.; Cadringher, P.; Herrmann, P.; Moerer, O.; Protti, A.; Gotti, M.; Chiurazzi, C.; Carlesso, E.; et al. Ventilator-related causes of lung injury: The mechanical power. Intensive Care Med. 2016, 42, 1567–1575. [Google Scholar] [CrossRef]
- Camporota, L.; Busana, M.; Marini, J.J.; Gattinoni, L. The 4dprr index and mechanical power: A step ahead or four steps backward? Am. J. Respir. Crit. Care Med. 2021, 204, 491–492. [Google Scholar] [CrossRef]
- Costa, E.L.V.; Slutsky, A.S.; Brochard, L.J.; Brower, R.; Serpa-Neto, A.; Cavalcanti, A.B.; Mercat, A.; Meade, M.; Morais, C.C.A.; Goligher, E.; et al. Ventilatory variables and mechanical power in patients with acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2021, 204, 303–311. [Google Scholar] [CrossRef]
- Huhle, R.; Serpa Neto, A.; Schultz, M.J.; Gama de Abreu, M. Is mechanical power the final word on ventilator-induced lung injury?-no. Ann. Transl. Med. 2018, 6, 394. [Google Scholar] [CrossRef]
- Maggiore, S.M.; Jonson, B.; Richard, J.C.; Jaber, S.; Lemaire, F.; Brochard, L. Alveolar derecruitment at decremental positive end-expiratory pressure levels in acute lung injury: Comparison with the lower inflection point, oxygenation, and compliance. Am. J. Respir. Crit. Care Med. 2001, 164, 795–801. [Google Scholar] [CrossRef]
- Richard, J.C.; Maggiore, S.M.; Jonson, B.; Mancebo, J.; Lemaire, F.; Brochard, L. Influence of tidal volume on alveolar recruitment. Respective role of peep and a recruitment maneuver. Am. J. Respir. Crit. Care Med. 2001, 163, 1609–1613. [Google Scholar] [CrossRef]
- Bellani, G.; Guerra, L.; Musch, G.; Zanella, A.; Patroniti, N.; Mauri, T.; Messa, C.; Pesenti, A. Lung regional metabolic activity and gas volume changes induced by tidal ventilation in patients with acute lung injury. Am. J. Respir. Crit. Care Med. 2011, 183, 1193–1199. [Google Scholar] [CrossRef] [Green Version]
- Gattinoni, L.; Caironi, P.; Cressoni, M.; Chiumello, D.; Ranieri, V.M.; Quintel, M.; Russo, S.; Patroniti, N.; Cornejo, R.; Bugedo, G. Lung recruitment in patients with the acute respiratory distress syndrome. N. Engl. J. Med. 2006, 354, 1775–1786. [Google Scholar] [CrossRef]
- Grieco, D.L.; Chen, L.; Brochard, L. Transpulmonary pressure: Importance and limits. Ann. Transl. Med. 2017, 5, 285. [Google Scholar] [CrossRef] [Green Version]
- Writing Group for the Alveolar Recruitment for Acute Respiratory Distress Syndrome Trial (ART) Investigators; Cavalcanti, A.B.; Suzumura, E.A.; Laranjeira, L.N.; Paisani, D.M.; Damiani, L.P.; Guimaraes, H.P.; Romano, E.R.; Regenga, M.M.; Taniguchi, L.N.T.; et al. Effect of lung recruitment and titrated positive end-expiratory pressure (peep) vs low peep on mortality in patients with acute respiratory distress syndrome: A randomized clinical trial. JAMA 2017, 318, 1335–1345. [Google Scholar]
- Brower, R.G.; Lanken, P.N.; MacIntyre, N.; Matthay, M.A.; Morris, A.; Ancukiewicz, M.; Schoenfeld, D.; Thompson, B.T.; National Heart, L.; Blood Institute, A.C.T.N. Higher versus lower positive end-expiratory pressures in patients with the acute respiratory distress syndrome. N. Engl. J. Med. 2004, 351, 327–336. [Google Scholar]
- Meade, M.O.; Cook, D.J.; Guyatt, G.H.; Slutsky, A.S.; Arabi, Y.M.; Cooper, D.J.; Davies, A.R.; Hand, L.E.; Zhou, Q.; Thabane, L.; et al. Ventilation strategy using low tidal volumes, recruitment maneuvers, and high positive end-expiratory pressure for acute lung injury and acute respiratory distress syndrome: A randomized controlled trial. JAMA 2008, 299, 637–645. [Google Scholar] [CrossRef] [Green Version]
- Mercat, A.; Richard, J.C.; Vielle, B.; Jaber, S.; Osman, D.; Diehl, J.L.; Lefrant, J.Y.; Prat, G.; Richecoeur, J.; Nieszkowska, A.; et al. Positive end-expiratory pressure setting in adults with acute lung injury and acute respiratory distress syndrome: A randomized controlled trial. JAMA 2008, 299, 646–655. [Google Scholar] [CrossRef] [Green Version]
- Kacmarek, R.M.; Villar, J.; Sulemanji, D.; Montiel, R.; Ferrando, C.; Blanco, J.; Koh, Y.; Soler, J.A.; Martinez, D.; Hernandez, M.; et al. Open lung approach for the acute respiratory distress syndrome: A pilot, randomized controlled trial. Crit. Care Med. 2016, 44, 32–42. [Google Scholar] [CrossRef]
- Briel, M.; Meade, M.; Mercat, A.; Brower, R.G.; Talmor, D.; Walter, S.D.; Slutsky, A.S.; Pullenayegum, E.; Zhou, Q.; Cook, D.; et al. Higher vs lower positive end-expiratory pressure in patients with acute lung injury and acute respiratory distress syndrome: Systematic review and meta-analysis. JAMA 2010, 303, 865–873. [Google Scholar] [CrossRef] [Green Version]
- Constantin, J.M.; Jabaudon, M.; Lefrant, J.Y.; Jaber, S.; Quenot, J.P.; Langeron, O.; Ferrandiere, M.; Grelon, F.; Seguin, P.; Ichai, C.; et al. Personalised mechanical ventilation tailored to lung morphology versus low positive end-expiratory pressure for patients with acute respiratory distress syndrome in france (the live study): A multicentre, single-blind, randomised controlled trial. Lancet Respir. Med. 2019, 7, 870–880. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Del Sorbo, L.; Grieco, D.L.; Junhasavasdikul, D.; Rittayamai, N.; Soliman, I.; Sklar, M.C.; Rauseo, M.; Ferguson, N.D.; Fan, E.; et al. Potential for lung recruitment estimated by the recruitment-to-inflation ratio in acute respiratory distress syndrome. A clinical trial. Am. J. Respir. Crit. Care Med. 2020, 201, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Del Sorbo, L.; Grieco, D.L.; Shklar, O.; Junhasavasdikul, D.; Telias, I.; Fan, E.; Brochard, L. Airway closure in acute respiratory distress syndrome: An underestimated and misinterpreted phenomenon. Am. J. Respir. Crit. Care Med. 2018, 197, 132–136. [Google Scholar] [CrossRef]
- Costa, E.L.; Borges, J.B.; Melo, A.; Suarez-Sipmann, F.; Toufen, C., Jr.; Bohm, S.H.; Amato, M.B. Bedside estimation of recruitable alveolar collapse and hyperdistension by electrical impedance tomography. Intensive Care Med. 2009, 35, 1132–1137. [Google Scholar] [CrossRef]
- Yoshida, T.; Piraino, T.; Lima, C.A.S.; Kavanagh, B.P.; Amato, M.B.P.; Brochard, L. Regional ventilation displayed by electrical impedance tomography as an incentive to decrease positive end-expiratory pressure. Am. J. Respir. Crit. Care Med. 2019, 200, 933–937. [Google Scholar] [CrossRef]
- Yoshida, T.; Amato, M.B.P.; Grieco, D.L.; Chen, L.; Lima, C.A.S.; Roldan, R.; Morais, C.C.A.; Gomes, S.; Costa, E.L.V.; Cardoso, P.F.G.; et al. Esophageal manometry and regional transpulmonary pressure in lung injury. Am. J. Respir. Crit. Care Med. 2018, 197, 1018–1026. [Google Scholar] [CrossRef] [PubMed]
- Sarge, T.; Baedorf-Kassis, E.; Banner-Goodspeed, V.; Novack, V.; Loring, S.H.; Gong, M.N.; Cook, D.; Talmor, D.; Beitler, J.R.; Group, E.P.-S. Effect of esophageal pressure-guided positive end-expiratory pressure on survival from acute respiratory distress syndrome: A risk-based and mechanistic reanalysis of the epvent-2 trial. Am. J. Respir. Crit. Care Med. 2021, 204, 1153–1163. [Google Scholar] [CrossRef] [PubMed]
- De Jong, A.; Verzilli, D.; Jaber, S. Ards in obese patients: Specificities and management. Crit. Care 2019, 23, 74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.; Grieco, D.L.; Beloncle, F.; Chen, G.Q.; Tiribelli, N.; Madotto, F.; Fredes, S.; Lu, C.; Antonelli, M.; Mercat, A.; et al. Partition of respiratory mechanics in patients with acute respiratory distress syndrome and association with outcome: A multicentre clinical study. Intensive Care Med. 2022, 48, 888–898. [Google Scholar] [CrossRef]
- Suarez-Sipmann, F.; Bohm, S.H.; Tusman, G. Volumetric capnography: The time has come. Curr. Opin. Crit. Care 2014, 20, 333–339. [Google Scholar] [CrossRef]
- Kallet, R.H.; Zhuo, H.; Liu, K.D.; Calfee, C.S.; Matthay, M.A.; National Heart, L.; Blood Institute, A.N.I. The association between physiologic dead-space fraction and mortality in subjects with ards enrolled in a prospective multi-center clinical trial. Respir. Care 2014, 59, 1611–1618. [Google Scholar] [CrossRef] [Green Version]
- Fengmei, G.; Jin, C.; Songqiao, L.; Congshan, Y.; Yi, Y. Dead space fraction changes during peep titration following lung recruitment in patients with ards. Respir. Care 2012, 57, 1578–1585. [Google Scholar] [CrossRef] [Green Version]
- Pham, T.; Telias, I.; Piraino, T.; Yoshida, T.; Brochard, L.J. Asynchrony consequences and management. Crit. Care Clin. 2018, 34, 325–341. [Google Scholar] [CrossRef] [PubMed]
- de Vries, H.; Jonkman, A.; Shi, Z.H.; Spoelstra-de Man, A.; Heunks, L. Assessing breathing effort in mechanical ventilation: Physiology and clinical implications. Ann. Transl. Med. 2018, 6, 387. [Google Scholar] [CrossRef] [PubMed]
- Carson, S.S.; Kress, J.P.; Rodgers, J.E.; Vinayak, A.; Campbell-Bright, S.; Levitt, J.; Bourdet, S.; Ivanova, A.; Henderson, A.G.; Pohlman, A.; et al. A randomized trial of intermittent lorazepam versus propofol with daily interruption in mechanically ventilated patients. Crit. Care Med. 2006, 34, 1326–1332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaschetto, R.; Cammarota, G.; Colombo, D.; Longhini, F.; Grossi, F.; Giovanniello, A.; Della Corte, F.; Navalesi, P. Effects of propofol on patient-ventilator synchrony and interaction during pressure support ventilation and neurally adjusted ventilatory assist. Crit. Care Med. 2014, 42, 74–82. [Google Scholar] [CrossRef]
- Bouillon, T.; Bruhn, J.; Roepcke, H.; Hoeft, A. Opioid-induced respiratory depression is associated with increased tidal volume variability. Eur. J. Anaesthesiol. 2003, 20, 127–133. [Google Scholar] [CrossRef]
- Pattinson, K.T. Opioids and the control of respiration. Br. J. Anaesth. 2008, 100, 747–758. [Google Scholar] [CrossRef] [Green Version]
- Belleville, J.P.; Ward, D.S.; Bloor, B.C.; Maze, M. Effects of intravenous dexmedetomidine in humans. I. Sedation, ventilation, and metabolic rate. Anesthesiology 1992, 77, 1125–1133. [Google Scholar] [CrossRef]
- Telias, I.; Abbott, M.; Brochard, L. Monitoring respiratory drive and effort during mechanical ventilation. J. Transl. Crit. Care Med. 2021, 3, 13. [Google Scholar] [CrossRef]
- Whitelaw, W.A.; Derenne, J.P.; Milic-Emili, J. Occlusion pressure as a measure of respiratory center output in conscious man. Respir. Physiol. 1975, 23, 181–199. [Google Scholar] [CrossRef]
- Bertoni, M.; Telias, I.; Urner, M.; Long, M.; Del Sorbo, L.; Fan, E.; Sinderby, C.; Beck, J.; Liu, L.; Qiu, H.; et al. A novel non-invasive method to detect excessively high respiratory effort and dynamic transpulmonary driving pressure during mechanical ventilation. Crit. Care 2019, 23, 346. [Google Scholar] [CrossRef] [Green Version]
- Bellani, G.; Grassi, A.; Sosio, S.; Foti, G. Plateau and driving pressure in the presence of spontaneous breathing. Intensive Care Med. 2019, 45, 97–98. [Google Scholar] [CrossRef] [PubMed]
- Guerin, C.; Reignier, J.; Richard, J.C.; Beuret, P.; Gacouin, A.; Boulain, T.; Mercier, E.; Badet, M.; Mercat, A.; Baudin, O.; et al. Prone positioning in severe acute respiratory distress syndrome. N. Engl. J. Med. 2013, 368, 2159–2168. [Google Scholar] [CrossRef]
- Munshi, L.; Del Sorbo, L.; Adhikari, N.K.J.; Hodgson, C.L.; Wunsch, H.; Meade, M.O.; Uleryk, E.; Mancebo, J.; Pesenti, A.; Ranieri, V.M.; et al. Prone position for acute respiratory distress syndrome. A systematic review and meta-analysis. Ann. Am. Thorac. Soc. 2017, 14, S280–S288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papazian, L.; Munshi, L.; Guerin, C. Prone position in mechanically ventilated patients. Intensive Care Med. 2022, 48, 1062–1065. [Google Scholar] [CrossRef] [PubMed]
- Sardo, S.; Osawa, E.A.; Finco, G.; Gomes Galas, F.R.B.; de Almeida, J.P.; Cutuli, S.L.; Frassanito, C.; Landoni, G.; Hajjar, L.A. Nitric oxide in cardiac surgery: A meta-analysis of randomized controlled trials. J. Cardiothorac. Vasc. Anesth. 2018, 32, 2512–2519. [Google Scholar] [CrossRef] [Green Version]
- Gebistorf, F.; Karam, O.; Wetterslev, J.; Afshari, A. Inhaled nitric oxide for acute respiratory distress syndrome (ards) in children and adults. Cochrane Database Syst. Rev. 2016, 2016, CD002787. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Noninvasive Respiratory Supports | Settings | Benefits | Pitfalls | |
|---|---|---|---|---|
| High-flow oxygen therapy |
|
|
| |
| CPAP/NIV | Facemask |
|
|
|
| Helmet |
|
|
| |
| Parameter | Monitoring Tool | Clinical Threshold Associated with Failure | Limitations |
|---|---|---|---|
| SpO2/FiO2 | Pulse oximetry | <120 and/or worsening trend | Underestimation of clinical severity for low PaCO2 levels |
| PaO2/FIO2 | Arterial blood gas analysis | <150–200 and/or worsening trend | Intermittent |
| Respiratory rate | Clinical examination | >25–30 and/or not decreasing | Low correlation with effort |
| Expired tidal volume | Mechanical ventilator | >9–9.5 mL/kg PBW | Not feasible during HFOT and helmet-NIV/CPAP |
| ΔPES | Esophageal balloon catheter | Absolute value > 10–15 cmH2O Reduction of less than 10 cmH2O after two hours of NIV | Needs some expertise |
| ROX index | (SpO2/FIO2)/Respiratory rate | <2.85 at 2 h of HFOT initiation <3.47 at 6 h of HFOT initiation <3.85 at 12 h of HFOT initiation | Validated for HFOT and NIV |
| HACOR scale | Heart rate, acidosis, stream of consciousness, oxygenation, and respiratory rate. An updated version takes into account some baseline variables as pneumonia, cardiogenic pulmonary edema, pulmonary ARDS, immunosuppression, septic shock, and the SOFA score | >5 points at 1 h of NIV initiation. A HACOR score of ≤7, 7.5–10.5, 11–14, and >14 were updated to be classified at low, moderate, high, or a very high probability of NIV failure | Intermittent, time consuming, and validated only for NIV |
| Ventilatory Variables | Initial Setting | Safe Limits |
|---|---|---|
| Controlled ventilation | ||
| VT | 6 mL/kg IBW, targeting a ΔP < 15 cmH2O and PPLAT < 28–30 cmH2O | Up to 8 mL/kg of IBW if PPLAT and ΔP remain within a safe limit and if 4 × ΔP + RR is reduced |
| ΔP | / | <15 cmH2O, unless more than 4 breaths per minute are needed to maintain isocapnia for each cmH2O of ΔP reduction (4 × ΔP + RR is increased) |
| PPLAT | / | <28–30 cmH2O |
| PEEP | High or low PEEP set according to the recruitability profile (e.g., CT-scan, R/I ratio, EIT, esophageal manometry) | PPLAT should be kept within the safe limit; hemodynamic instability should be avoided and treated; and high PEEP in non-recruitable patients is discouraged |
| RR | Set to maintain PaCO2 and pH in the desired range | Check for the presence of PEEPi and set I:E accordingly, and variations of RR should be made in relation with Vt, not to increase 4 × ΔP + RR |
| Assisted ventilation | ||
| P0.1 | / | 1–4 cmH2O |
| ΔPOCC | / | 10–15 cmH2O |
| PPLAT | / | <28–30 cmH2O |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cutuli, S.L.; Grieco, D.L.; Michi, T.; Cesarano, M.; Rosà, T.; Pintaudi, G.; Menga, L.S.; Ruggiero, E.; Giammatteo, V.; Bello, G.; et al. Personalized Respiratory Support in ARDS: A Physiology-to-Bedside Review. J. Clin. Med. 2023, 12, 4176. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12134176
Cutuli SL, Grieco DL, Michi T, Cesarano M, Rosà T, Pintaudi G, Menga LS, Ruggiero E, Giammatteo V, Bello G, et al. Personalized Respiratory Support in ARDS: A Physiology-to-Bedside Review. Journal of Clinical Medicine. 2023; 12(13):4176. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12134176
Chicago/Turabian StyleCutuli, Salvatore Lucio, Domenico Luca Grieco, Teresa Michi, Melania Cesarano, Tommaso Rosà, Gabriele Pintaudi, Luca Salvatore Menga, Ersilia Ruggiero, Valentina Giammatteo, Giuseppe Bello, and et al. 2023. "Personalized Respiratory Support in ARDS: A Physiology-to-Bedside Review" Journal of Clinical Medicine 12, no. 13: 4176. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12134176