

Myocarditis and Pericarditis Post-mRNA COVID-19 Vaccination: Insights from a Pharmacovigilance Perspective
 , ,
, ,  and
and
Abstract
:1. Introduction
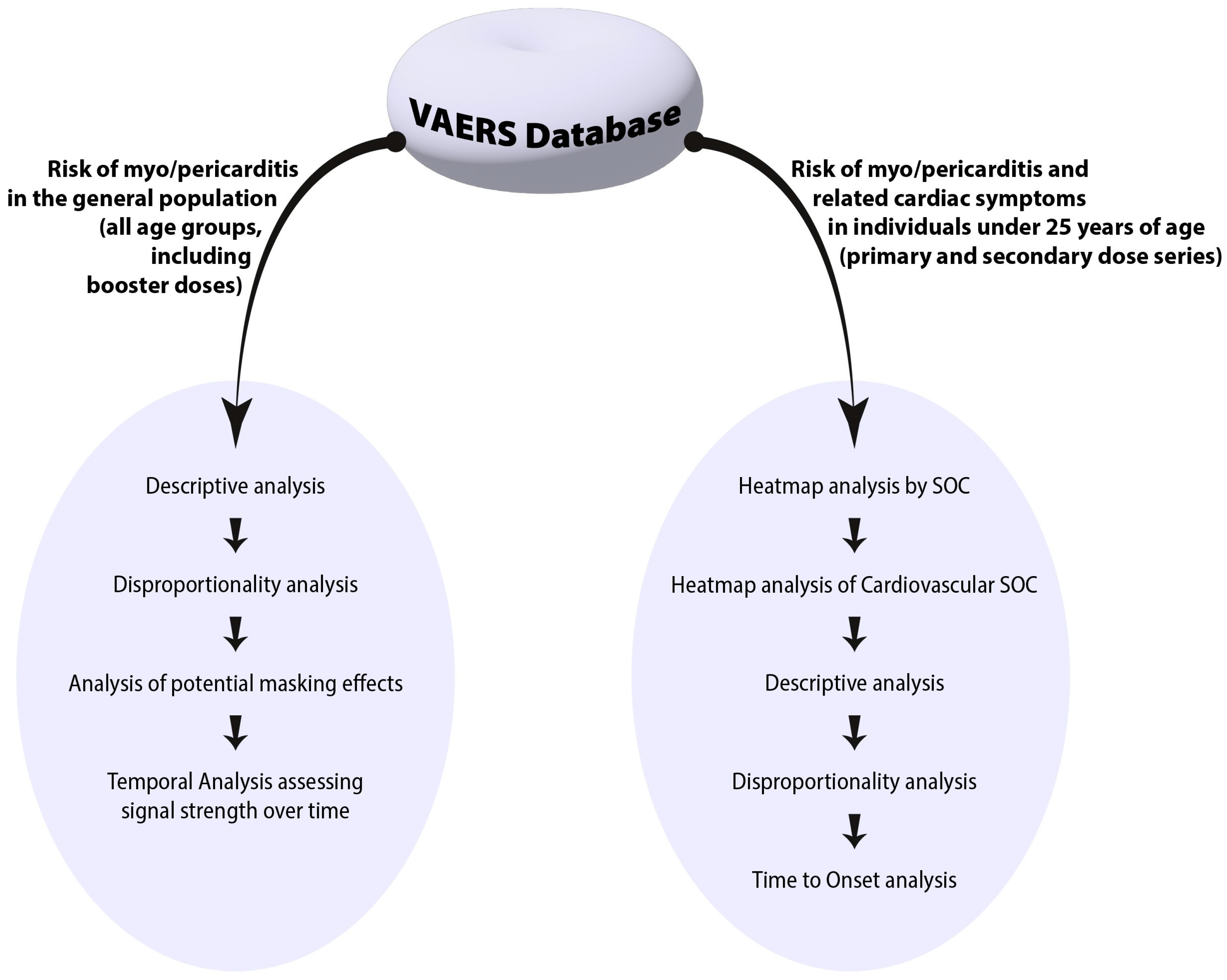
2. Materials and Methods
2.1. Data Source
- (1)
- VAERS DATA dataset: consists of basic demographic information, including VAERS ID, sex, age, vaccination date, allergies, and health history.
- (2)
- VAERS Symptoms dataset: consists of VAERS ID-linked adverse event symptoms, which may include up to five symptoms listed as being related to the administration of a vaccine and experienced by the vaccinee.
- (3)
- VAERS Vaccine dataset: contains VAERS ID-linked information about the administered vaccine, including the vaccine type, manufacturer, lot number, number of doses given, route of administration, and site of injection.
2.2. Data Selection and Processing
2.3. Statistical Analysis
3. Results
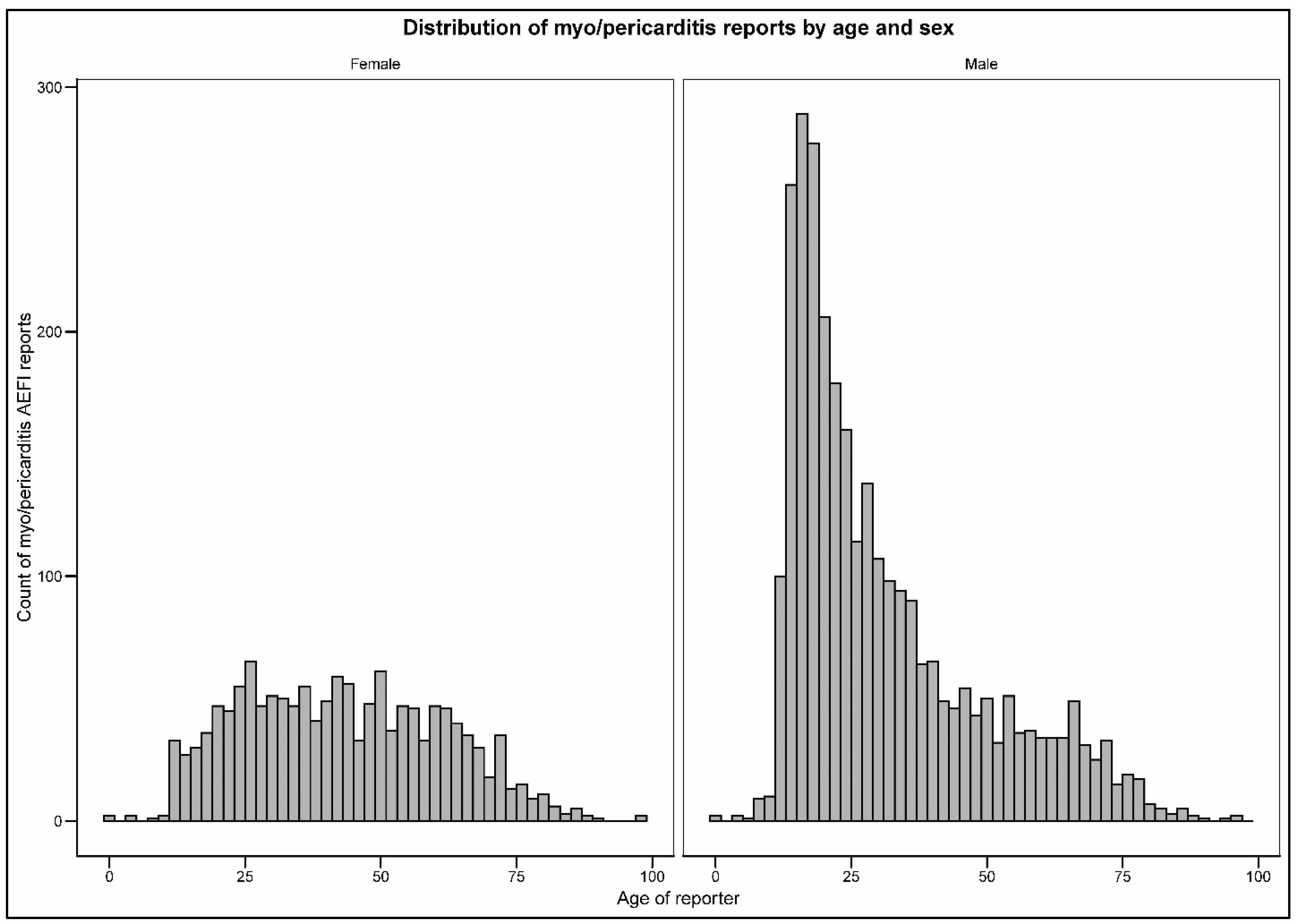
3.1. Descriptive Analysis
3.2. Signal Detection
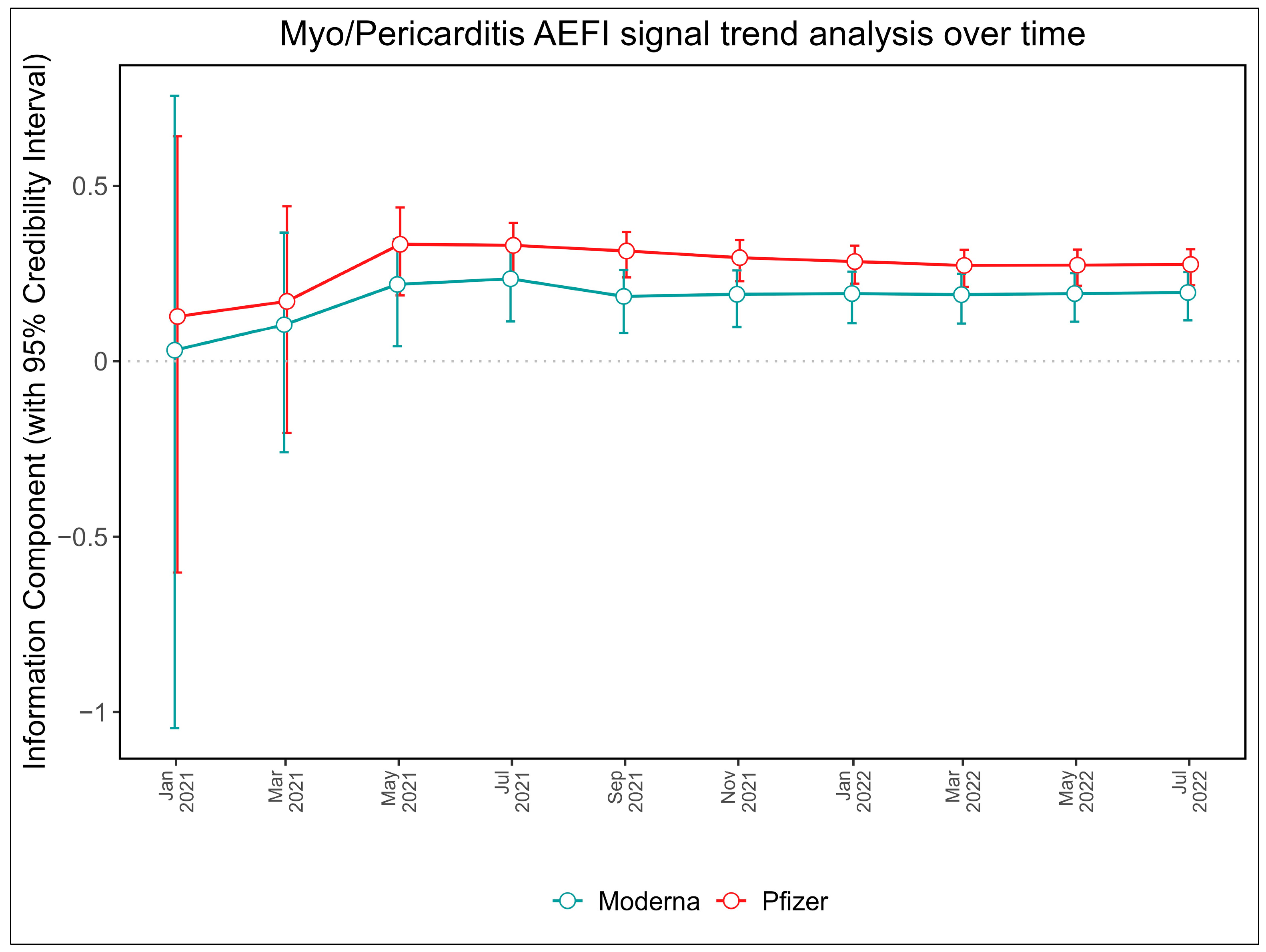
3.3. Signal Trend Analysis over Time for Pfizer-BioNTech and Moderna
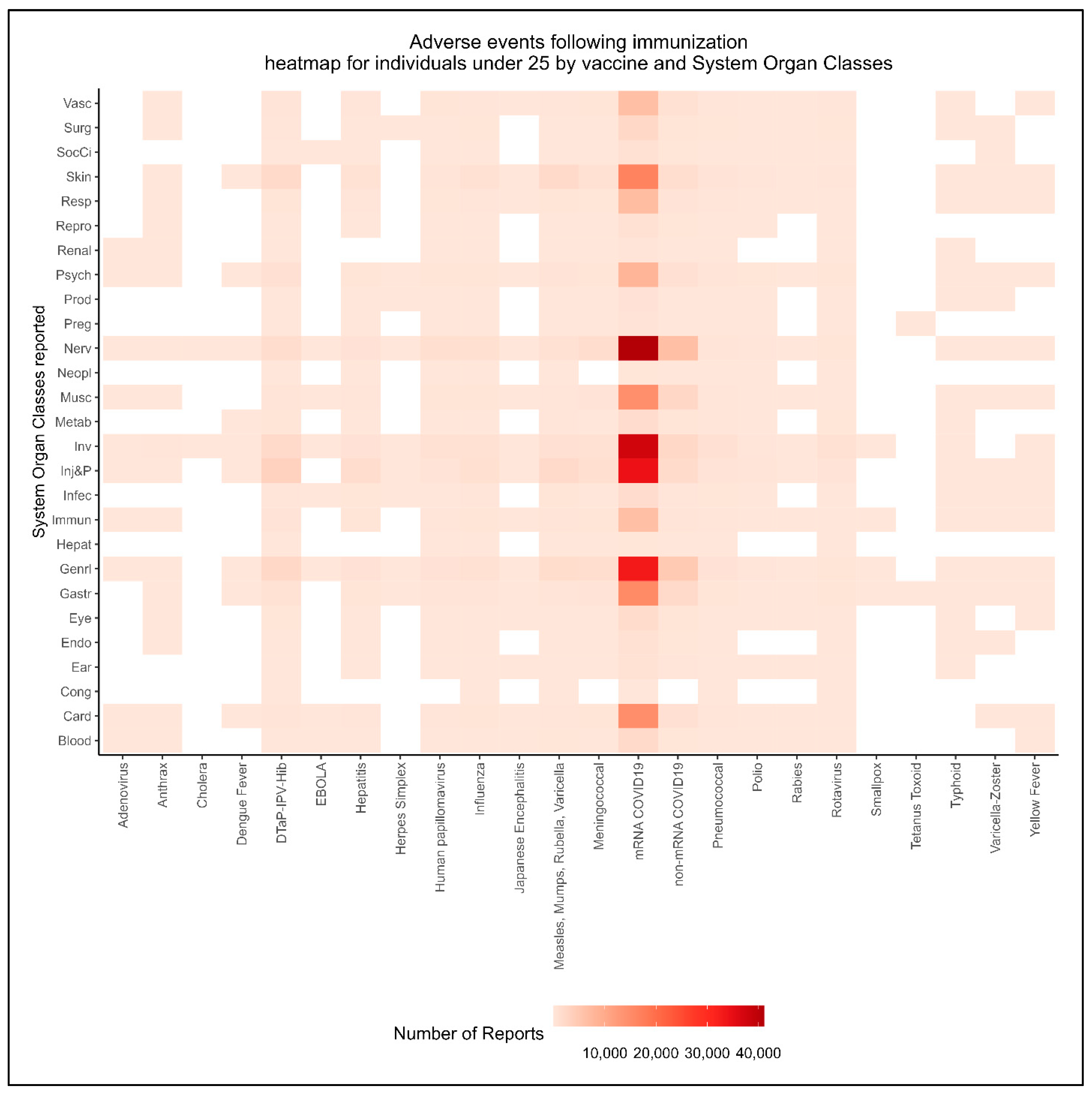
3.4. Myo/Pericarditis after mRNA COVID-19 Vaccination in Younger Individuals
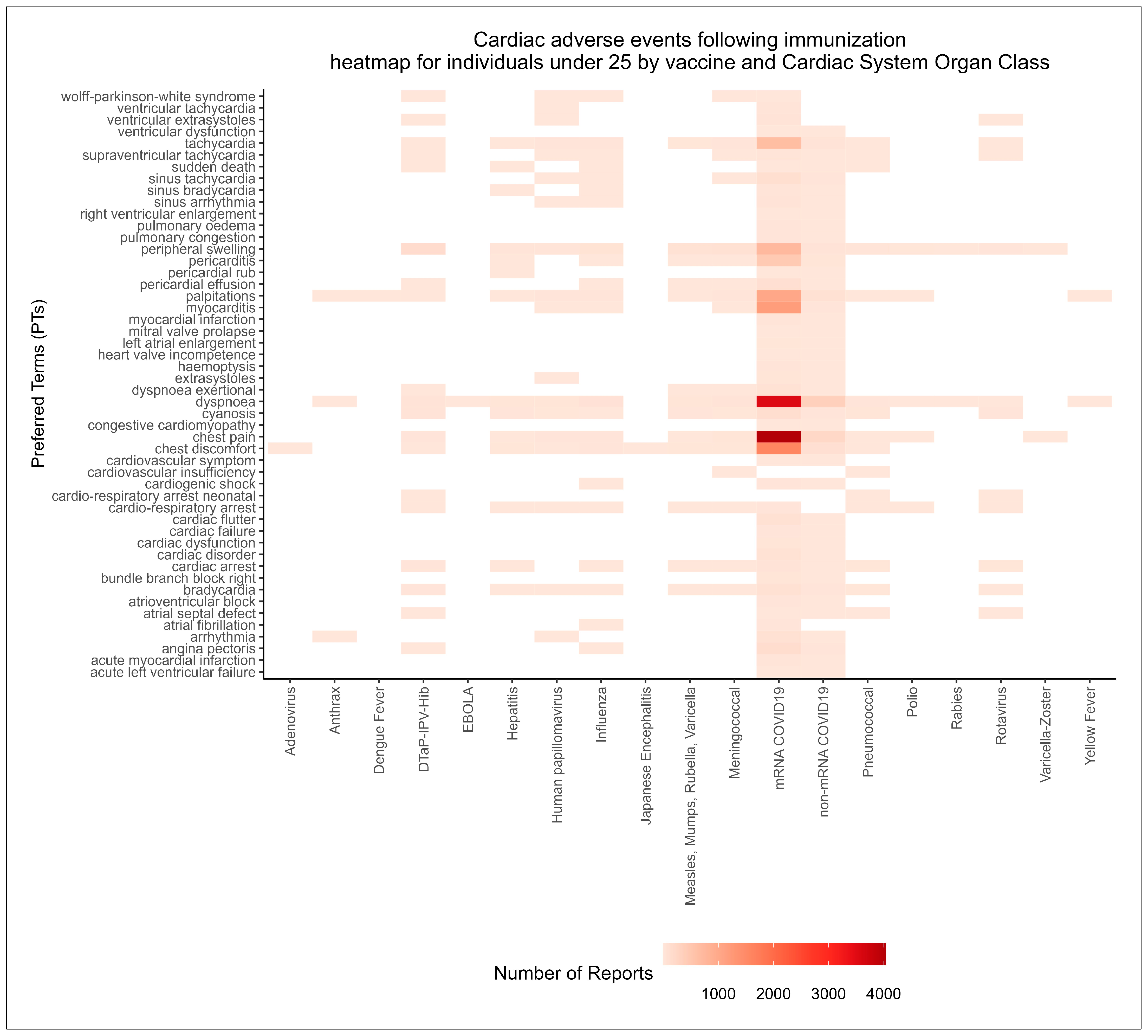
3.4.1. Intensity of Report Counts by System Organ Class and Vaccine Type
3.4.2. Signal Detection for Cardiac AEFIs in Individuals Younger than 25 Years of Age
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rudolph, A.; Mitchell, J.; Barrett, J.; Sköld, H.; Taavola, H.; Erlanson, N.; Melgarejo-González, C.; Yue, Q.-Y. Global safety monitoring of COVID-19 vaccines: How pharmacovigilance rose to the challenge. Ther. Adv. Drug Saf. 2022, 13, 20420986221118972. [Google Scholar] [CrossRef]
- McMurry, R.; Lenehan, P.; Awasthi, S.; Silvert, E.; Puranik, A.; Pawlowski, C.; Venkatakrishnan, A.J.; Anand, P.; Agarwal, V.; O’Horo, J.C.; et al. Real-time analysis of a mass vaccination effort confirms the safety of FDA-authorized mRNA COVID-19 vaccines. Med 2021, 2, 965–978.e965. [Google Scholar] [CrossRef]
- Bellos, I.; Karageorgiou, V.; Viskin, D. Myocarditis following mRNA COVID-19 vaccination: A pooled analysis. Vaccine 2022, 40, 1768–1774. [Google Scholar] [CrossRef]
- Gargano, J.W.; Wallace, M.; Hadler, S.C.; Langley, G.; Su, J.R.; Oster, M.E.; Broder, K.R.; Gee, J.; Weintraub, E.; Shimabukuro, T. Use of mRNA COVID-19 vaccine after reports of myocarditis among vaccine recipients: Update from the Advisory Committee on Immunization Practices—United States, June 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 977–982. [Google Scholar] [CrossRef]
- Bozkurt, B.; Kamat, I.; Hotez, P.J. Myocarditis With COVID-19 mRNA Vaccines. Circulation 2021, 144, 471–484. [Google Scholar] [CrossRef]
- Muthukumar, A.; Narasimhan, M.; Li, Q.-Z.; Mahimainathan, L.; Hitto, I.; Fuda, F.; Batra, K.; Jiang, X.; Zhu, C.; Schoggins, J. In-depth evaluation of a case of presumed myocarditis after the second dose of COVID-19 mRNA vaccine. Circulation 2021, 144, 487–498. [Google Scholar] [CrossRef]
- Talotta, R. Do COVID-19 RNA-based vaccines put at risk of immune-mediated diseases? In reply to “potential antigenic cross-reactivity between SARS-CoV-2 and human tissue with a possible link to an increase in autoimmune diseases”. Clin. Immunol. 2021, 224, 108665. [Google Scholar] [CrossRef]
- Heymans, S.; Cooper, L.T. Myocarditis after COVID-19 mRNA vaccination: Clinical observations and potential mechanisms. Nat. Rev. Cardiol. 2022, 19, 75–77. [Google Scholar] [CrossRef]
- Black, S.B.; Law, B.; Chen, R.T.; Dekker, C.L.; Sturkenboom, M.; Huang, W.-T.; Gurwith, M.; Poland, G. The critical role of background rates of possible adverse events in the assessment of COVID-19 vaccine safety. Vaccine 2021, 39, 2712–2718. [Google Scholar] [CrossRef]
- Piché-Renaud, P.P.; Morris, S.K.; Top, K.A. A narrative review of vaccine pharmacovigilance during mass vaccination campaigns: Focus on myocarditis and pericarditis after COVID-19 mRNA vaccination. Br. J. Clin. Pharmacol. 2023, 89, 967–981. [Google Scholar] [CrossRef]
- Almenoff, J.; Tonning, J.M.; Gould, A.L.; Szarfman, A.; Hauben, M.; Ouellet-Hellstrom, R.; Ball, R.; Hornbuckle, K.; Walsh, L.; Yee, C. Perspectives on the use of data mining in pharmacovigilance. Drug Saf. 2005, 28, 981–1007. [Google Scholar] [CrossRef] [PubMed]
- Abu Mouch, S.; Roguin, A.; Hellou, E.; Ishai, A.; Shoshan, U.; Mahamid, L.; Zoabi, M.; Aisman, M.; Goldschmid, N.; Berar Yanay, N. Myocarditis following COVID-19 mRNA vaccination. Vaccine 2021, 39, 3790–3793. [Google Scholar] [CrossRef]
- Durand, J.; Dogné, J.-M.; Cohet, C.; Browne, K.; Gordillo-Marañón, M.; Piccolo, L.; Zaccaria, C.; Genov, G. Safety Monitoring of COVID-19 Vaccines: Perspective from the European Medicines Agency. Clin. Pharmacol. Ther. 2023, 111, 1223–1234. [Google Scholar] [CrossRef]
- Abraham, N.; Spruin, S.; Rossi, T.; Fireman, B.; Zafack, J.; Blaser, C.; Shaw, A.; Hutchings, K.; Ogunnaike-Cooke, S. Myocarditis and/or pericarditis risk after mRNA COVID-19 vaccination: A Canadian head to head comparison of BNT162b2 and mRNA-1273 vaccines. Vaccine 2022, 40, 4663–4671. [Google Scholar] [CrossRef]
- Salvo, F.; Pariente, A.; Valnet-Rabier, M.B.; Drici, M.-D.; Cholle, C.; Mathieu, C.; Singier, A.; Bagheri, H.; Tebacher, M.; Micallef, J.; et al. Role of spontaneous reporting in investigating the relationship between mRNA COVID-19 vaccines and myocarditis: The French perspective. Therapies 2023. [Google Scholar] [CrossRef]
- Lane, S.; Yeomans, A.; Shakir, S. Reports of myocarditis and pericarditis following mRNA COVID-19 vaccination: A systematic review of spontaneously reported data from the UK, Europe and the USA and of the scientific literature. BMJ Open 2022, 12, e059223. [Google Scholar] [CrossRef]
- Foltran, D.; Delmas, C.; Flumian, C.; De Paoli, P.; Salvo, F.; Gautier, S.; Drici, M.D.; Karsenty, C.; Montastruc, F. Myocarditis and pericarditis in adolescents after first and second doses of mRNA COVID-19 vaccines. Eur. Heart J.-Qual. Care Clin. Outcomes 2021, 8, 99–103. [Google Scholar] [CrossRef]
- Naveed, Z.; Li, J.; Wilton, J.; Spencer, M.; Naus, M.; García, H.A.V.; Kwong, J.C.; Rose, C.; Otterstatter, M.; Janjua, N.Z. Comparative Risk of Myocarditis/Pericarditis Following Second Doses of BNT162b2 and mRNA-1273 Coronavirus Vaccines. J. Am. Coll. Cardiol. 2022, 80, 1900–1908. [Google Scholar] [CrossRef]
- Naveed, Z.; Li, J.; Spencer, M.; Wilton, J.; Naus, M.; García, H.A.V.; Otterstatter, M.; Janjua, N.Z. Observed versus expected rates of myocarditis after SARS-CoV-2 vaccination: A population-based cohort study. Cmaj 2022, 194, E1529–E1536. [Google Scholar] [CrossRef]
- Boehmer, T.K.; Kompaniyets, L.; Lavery, A.M.; Hsu, J.; Ko, J.Y.; Yusuf, H.; Romano, S.D.; Gundlapalli, A.V.; Oster, M.E.; Harris, A.M. Association Between COVID-19 and Myocarditis Using Hospital-Based Administrative Data—United States, March 2020–January 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 1228–1232. [Google Scholar] [CrossRef]
- Karlstad, Ø.; Hovi, P.; Husby, A.; Härkänen, T.; Selmer, R.M.; Pihlström, N.; Hansen, J.V.; Nohynek, H.; Gunnes, N.; Sundström, A.; et al. SARS-CoV-2 Vaccination and Myocarditis in a Nordic Cohort Study of 23 Million Residents. JAMA Cardiol. 2022, 7, 600–612. [Google Scholar] [CrossRef]
- Buchan, S.A.; Seo, C.Y.; Johnson, C.; Alley, S.; Kwong, J.C.; Nasreen, S.; Calzavara, A.; Lu, D.; Harris, T.M.; Yu, K.; et al. Epidemiology of Myocarditis and Pericarditis Following mRNA Vaccination by Vaccine Product, Schedule, and Interdose Interval Among Adolescents and Adults in Ontario, Canada. JAMA Netw. Open 2022, 5, e2218505. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services (HHS). Vaccine Adverse Event Reporting System. Available online: https://vaers.hhs.gov/ (accessed on 5 August 2022).
- Shimabukuro, T.T.; Nguyen, M.; Martin, D.; DeStefano, F. Safety monitoring in the vaccine adverse event reporting system (VAERS). Vaccine 2015, 33, 4398–4405. [Google Scholar] [CrossRef]
- Brown, E.G.; Wood, L.; Wood, S. The medical dictionary for regulatory activities (MedDRA). Drug Saf. 1999, 20, 109–117. [Google Scholar] [CrossRef]
- Hauben, M. A brief primer on automated signal detection. Ann. Pharmacother. 2003, 37, 1117–1123. [Google Scholar] [CrossRef] [PubMed]
- Harpaz, R.; DuMouchel, W.; Shah, N.H.; Madigan, D.; Ryan, P.; Friedman, C. Novel data-mining methodologies for adverse drug event discovery and analysis. Clin. Pharmacol. Ther. 2012, 91, 1010–1021. [Google Scholar] [CrossRef] [PubMed]
- Clothier, H.J.; Lawrie, J.; Russell, M.A.; Kelly, H.; Buttery, J.P. Early signal detection of adverse events following influenza vaccination using proportional reporting ratio, Victoria, Australia. PLoS ONE 2019, 14, e0224702. [Google Scholar] [CrossRef] [PubMed]
- Musonda, P.; Hocine, M.N.; Andrews, N.J.; Tubert-Bitter, P.; Farrington, C.P. Monitoring vaccine safety using case series cumulative sum charts. Vaccine 2008, 26, 5358–5367. [Google Scholar] [CrossRef]
- Sakaeda, T.; Tamon, A.; Kadoyama, K.; Okuno, Y. Data mining of the public version of the FDA Adverse Event Reporting System. Int. J. Med. Sci. 2013, 10, 796–803. [Google Scholar] [CrossRef]
- Martin, D.; Menschik, D.; Bryant-Genevier, M.; Ball, R. Data mining for prospective early detection of safety signals in the Vaccine Adverse Event Reporting System (VAERS): A case study of febrile seizures after a 2010–2011 seasonal influenza virus vaccine. Drug Saf. 2013, 36, 547–556. [Google Scholar] [CrossRef]
- Evans, S.J.; Waller, P.C.; Davis, S. Use of proportional reporting ratios (PRRs) for signal generation from spontaneous adverse drug reaction reports. Pharmacoepidemiol. Drug Saf. 2001, 10, 483–486. [Google Scholar] [CrossRef]
- Almenoff, J.S.; LaCroix, K.K.; Yuen, N.A.; Fram, D.; DuMouchel, W. Comparative performance of two quantitative safety signalling methods: Implications for use in a pharmacovigilance department. Drug Saf. 2006, 29, 875–887. [Google Scholar] [CrossRef]
- Bonneterre, V.; Bicout, D.J.; De Gaudemaris, R. Application of Pharmacovigilance Methods in Occupational Health Surveillance: Comparison of Seven Disproportionality Metrics. Saf. Health Work. 2012, 3, 92–100. [Google Scholar] [CrossRef]
- van Manen, R.P.; Fram, D.; DuMouchel, W. Signal detection methodologies to support effective safety management. Expert Opin. Drug Saf. 2007, 6, 451–464. [Google Scholar] [CrossRef]
- Gravel, C. Statistical Methods for Signal Detection in Pharmacovigilance; Carleton University: Ottawa, ON, Canada, 2009. [Google Scholar]
- Norén, G.N.; Hopstadius, J.; Bate, A. Shrinkage observed-to-expected ratios for robust and transparent large-scale pattern discovery. Stat. Methods Med. Res. 2013, 22, 57–69. [Google Scholar] [CrossRef]
- Farrell, P.J.; Gravel, C.A.; Krewski, D. Signal detection in pharmacovigilance. In Encyclopedia of Biopharmaceutial Statistics; Chow, S.-C., Ed.; CRC Press: Boca Raton, FL, USA, 2018; pp. 1–15. [Google Scholar]
- Bate, A.; Evans, S. Quantitative signal detection using spontaneous ADR reporting. Pharmacoepidemiol. Drug Saf. 2009, 18, 427–436. [Google Scholar] [CrossRef]
- Park, G.; Jung, H.; Heo, S.-J.; Jung, I. Comparison of data mining methods for the signal detection of adverse drug events with a hierarchical structure in postmarketing surveillance. Life 2020, 10, 138. [Google Scholar] [CrossRef]
- Ahmed, I.; Poncet, A.; Ahmed, M.I.; Tcl, S. Package ‘PhViD’. Pharmacology 1998, 54, 315–321. [Google Scholar]
- Maignen, F.; Hauben, M.; Dogné, J.-M. A mathematical framework to quantify the masking effect associated with the confidence intervals of measures of disproportionality. Ther. Adv. Drug Saf. 2017, 8, 231–244. [Google Scholar] [CrossRef]
- Pariente, A.; Didailler, M.; Avillach, P.; Miremont-Salamé, G.; Fourrier-Reglat, A.; Haramburu, F.; Moore, N. A potential competition bias in the detection of safety signals from spontaneous reporting databases. Pharmacoepidemiol. Drug Saf. 2010, 19, 1166–1171. [Google Scholar] [CrossRef]
- Harpaz, R.; DuMouchel, W.; Van Manen, R.; Nip, A.; Bright, S.; Szarfman, A.; Tonning, J.; Lerch, M. Signaling COVID-19 Vaccine Adverse Events. Drug Saf. 2022, 45, 765–780. [Google Scholar] [CrossRef]
- Li, M.; Yuan, J.; Lv, G.; Brown, J.; Jiang, X.; Lu, Z.K. Myocarditis and Pericarditis following COVID-19 Vaccination: Inequalities in Age and Vaccine Types. J. Pers. Med. 2021, 11, 1106. [Google Scholar] [CrossRef]
- Yong, S.-J.; Halim, A.; Halim, M.; Al Mutair, A.; Alhumaid, S.; Al-Sihati, J.; Albayat, H.; Alsaeed, M.; Garout, M.; Al Azmi, R. Rare adverse events associated with BNT162b2 mRNA vaccine (Pfizer-BioNTech): A review of large-scale, controlled surveillance studies. Vaccines 2022, 10, 1067. [Google Scholar] [CrossRef]
- Chen, J.H.; Ikwuanusi, I.A.; Bommu, V.J.L.; Patel, V.; Aujla, H.; Kaushik, V.; Cheriyath, P. COVID-19 Vaccine-Related Myocarditis: A Descriptive Study of 40 Case Reports. Cureus 2022, 14, e21740. [Google Scholar] [CrossRef]
- Wong, H.-L.; Hu, M.; Zhou, C.K.; Lloyd, P.C.; Amend, K.L.; Beachler, D.C.; Secora, A.; McMahill-Walraven, C.N.; Lu, Y.; Wu, Y.; et al. Risk of myocarditis and pericarditis after the COVID-19 mRNA vaccination in the USA: A cohort study in claims databases. Lancet 2022, 399, 2191–2199. [Google Scholar] [CrossRef]
- Esposito, S.; Caminiti, C.; Giordano, R.; Argentiero, A.; Ramundo, G.; Principi, N. Myocarditis Following COVID-19 Vaccine Use: Can It Play a Role for Conditioning Immunization Schedules? Front. Immunol. 2022, 13, 915580. [Google Scholar] [CrossRef]
- Oster, M.E.; Shay, D.K.; Su, J.R.; Gee, J.; Creech, C.B.; Broder, K.R.; Edwards, K.; Soslow, J.H.; Dendy, J.M.; Schlaudecker, E.; et al. Myocarditis Cases Reported After mRNA-Based COVID-19 Vaccination in the US From December 2020 to August 2021. JAMA 2022, 327, 331–340. [Google Scholar] [CrossRef]
- Goddard, K.; Hanson, K.E.; Lewis, N.; Weintraub, E.; Fireman, B.; Klein, N.P. Incidence of Myocarditis/Pericarditis Following mRNA COVID-19 Vaccination Among Children and Younger Adults in the United States. Ann. Intern. Med. 2022, 175, 1169–1771. [Google Scholar] [CrossRef]
- Truong, D.T.; Dionne, A.; Muniz, J.C.; McHugh, K.E.; Portman, M.A.; Lambert, L.M.; Thacker, D.; Elias, M.D.; Li, J.S.; Toro-Salazar, O.H.; et al. Clinically Suspected Myocarditis Temporally Related to COVID-19 Vaccination in Adolescents and Young Adults: Suspected Myocarditis After COVID-19 Vaccination. Circulation 2022, 145, 345–356. [Google Scholar] [CrossRef]
- Hammershaimb, E.A.; Cole, L.D.; Liang, Y.; Hendrich, M.A.; Das, D.; Petrin, R.; Cataldi, J.R.; O’Leary, S.T.; Campbell, J.D. COVID-19 Vaccine Acceptance Among US Parents: A Nationally Representative Survey. J. Pediatr. Infect. Dis. Soc. 2022, 11, 361–370. [Google Scholar] [CrossRef]
- Siegel, D.A.; Reses, H.E.; Cool, A.J.; Shapiro, C.N.; Hsu, J.; Boehmer, T.K.; Cornwell, C.R.; Gray, E.B.; Henley, S.J.; Lochner, K.; et al. Trends in COVID-19 Cases, Emergency Department Visits, and Hospital Admissions Among Children and Adolescents Aged 0–17 Years—United States, August 2020–August 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 1249–1254. [Google Scholar] [CrossRef] [PubMed]
- Du, J.; Cai, Y.; Chen, Y.; Tao, C. Trivalent influenza vaccine adverse symptoms analysis based on MedDRA terminology using VAERS data in 2011. J. Biomed. Semant. 2016, 7, 13. [Google Scholar] [CrossRef]
- Blauwet, L.A.; Cooper, L.T. Myocarditis. Prog. Cardiovasc. Dis. 2010, 52, 274–288. [Google Scholar] [CrossRef]
- Rroku, A.; Kottwitz, J.; Heidecker, B. Update on myocarditis—What we know so far and where we may be heading. Eur. Heart J. Acute Cardiovasc. Care 2020, 10, 455–467. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.F.; Tseng, W.C.; Wang, J.K.; Chen, Y.S.; Chen, C.A.; Lin, M.T.; Lu, C.W.; Wu, M.H.; Chiu, S.N. Management of cardiovascular symptoms after Pfizer-BioNTech COVID-19 vaccine in teenagers in the emergency department. J. Formos. Med. Assoc. 2023, 122, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Orre, R.; Lansner, A.; Bate, A.; Lindquist, M. Bayesian neural networks with confidence estimations applied to data mining. Comput. Stat. &Amp; Data Anal. 2000, 34, 473–493. [Google Scholar]
- Kravchenko, D.; Isaak, A.; Mesropyan, N.; Bischoff, L.M.; Pieper, C.C.; Attenberger, U.; Kuetting, D.; Zimmer, S.; Hart, C.; Luetkens, J.A. Cardiac magnetic resonance follow-up of COVID-19 vaccine associated acute myocarditis. Front. Cardiovasc. Med. 2022, 9, 1049256. [Google Scholar] [CrossRef]
- Heidecker, B.; Dagan, N.; Balicer, R.; Eriksson, U.; Rosano, G.; Coats, A.; Tschöpe, C.; Kelle, S.; Poland, G.A.; Frustaci, A.; et al. Myocarditis following COVID-19 vaccine: Incidence, presentation, diagnosis, pathophysiology, therapy, and outcomes put into perspective. A clinical consensus document supported by the Heart Failure Association of the European Society of Cardiology (ESC) and the ESC Working Group on Myocardial and Pericardial Diseases. Eur. J. Heart Fail. 2022, 24, 2000–2018. [Google Scholar]
- Kim, H.W.; Jenista, E.R.; Wendell, D.C.; Azevedo, C.F.; Campbell, M.J.; Darty, S.N.; Parker, M.A.; Kim, R.J. Patients With Acute Myocarditis Following mRNA COVID-19 Vaccination. JAMA Cardiol. 2021, 6, 1196–1201. [Google Scholar] [CrossRef]
- Kim, M.S.; Jung, S.Y.; Ahn, J.G.; Park, S.J.; Shoenfeld, Y.; Kronbichler, A.; Koyanagi, A.; Dragioti, E.; Tizaoui, K.; Hong, S.H.; et al. Comparative safety of mRNA COVID-19 vaccines to influenza vaccines: A pharmacovigilance analysis using WHO international database. J. Med. Virol. 2022, 94, 1085–1095. [Google Scholar] [CrossRef] [PubMed]
- Alami, A.; Krewski, D.; Mattison, D.; Wilson, K.; Gravel, C.A.; Villeneuve, P.J.; Farrell, P.J.; Crispo, J.A.G.; Perez-Lloret, S. Risk of Myocarditis and Pericarditis among Young Adults following mRNA COVID-19 Vaccinations. Vaccines 2022, 10, 722. [Google Scholar] [CrossRef] [PubMed]
- Straus, W.; Urdaneta, V.; Esposito, D.B.; Mansi, J.A.; Rodriguez, C.S.; Burton, P.; Vega, J.M. Analysis of Myocarditis Among 252 Million mRNA-1273 Recipients Worldwide. Clin. Infect. Dis. 2022, 76, e544–e552. [Google Scholar] [CrossRef] [PubMed]
- Shimabukuro, T.T. COVID-19 Vaccine Safety Update: Primary Series in Young Children and Booster Doses in Older Children and Adults. Advisory Committee on Immunization Practices. Meeting (2022 September 1–2: Atlanta, GA). ACIP Meeting COVID-19 Vaccines. CDC COVID-19 Immunization Safety Unit. Available online: https://stacks.cdc.gov/view/cdc/120824 (accessed on 20 June 2023).
- Lai, F.T.T.; Li, X.; Peng, K.; Huang, L.; Ip, P.; Tong, X.; Chui, C.S.L.; Wan, E.Y.F.; Wong, C.K.H.; Chan, E.W.Y.; et al. Carditis After COVID-19 Vaccination With a Messenger RNA Vaccine and an Inactivated Virus Vaccine: A Case-Control Study. Ann. Intern. Med. 2022, 175, 362–370. [Google Scholar] [CrossRef] [PubMed]
- Le Vu, S.; Bertrand, M.; Jabagi, M.J.; Botton, J.; Drouin, J.; Baricault, B.; Weill, A.; Dray-Spira, R.; Zureik, M. Age and sex-specific risks of myocarditis and pericarditis following COVID-19 messenger RNA vaccines. Nat. Commun. 2022, 13, 3633. [Google Scholar] [CrossRef] [PubMed]
- Husby, A.; Hansen, J.V.; Fosbøl, E.; Thiesson, E.M.; Madsen, M.; Thomsen, R.W.; Sørensen, H.T.; Andersen, M.; Wohlfahrt, J.; Gislason, G. SARS-CoV-2 vaccination and myocarditis or myopericarditis: Population based cohort study. BMJ 2021, 375, e068665. [Google Scholar] [CrossRef]
- Patone, M.; Mei, X.W.; Handunnetthi, L.; Dixon, S.; Zaccardi, F.; Shankar-Hari, M.; Watkinson, P.; Khunti, K.; Harnden, A.; Coupland, C.A.C.; et al. Risks of myocarditis, pericarditis, and cardiac arrhythmias associated with COVID-19 vaccination or SARS-CoV-2 infection. Nat. Med. 2022, 28, 410–422. [Google Scholar] [CrossRef] [PubMed]
- Ab Rahman, N.; Lim, M.T.; Lee, F.Y.; Lee, S.C.; Ramli, A.; Saharudin, S.N.; King, T.L.; Anak Jam, E.B.; Ayub, N.A.; Sevalingam, R.K.; et al. Risk of serious adverse events after the BNT162b2, CoronaVac, and ChAdOx1 vaccines in Malaysia: A self-controlled case series study. Vaccine 2022, 40, 4394–4402. [Google Scholar] [CrossRef]
- Massari, M.; Spila Alegiani, S.; Morciano, C.; Spuri, M.; Marchione, P.; Felicetti, P.; Belleudi, V.; Poggi, F.R.; Lazzeretti, M.; Ercolanoni, M.; et al. Postmarketing active surveillance of myocarditis and pericarditis following vaccination with COVID-19 mRNA vaccines in persons aged 12 to 39 years in Italy: A multi-database, self-controlled case series study. PLoS Med. 2022, 19, e1004056. [Google Scholar] [CrossRef]
- Witberg, G.; Barda, N.; Hoss, S.; Richter, I.; Wiessman, M.; Aviv, Y.; Grinberg, T.; Auster, O.; Dagan, N.; Balicer, R.D. Myocarditis after COVID-19 vaccination in a large health care organization. N. Engl. J. Med. 2021, 385, 2132–2139. [Google Scholar] [CrossRef]
- Barda, N.; Dagan, N.; Ben-Shlomo, Y.; Kepten, E.; Waxman, J.; Ohana, R.; Hernán, M.A.; Lipsitch, M.; Kohane, I.; Netzer, D.; et al. Safety of the BNT162b2 mRNA COVID-19 Vaccine in a Nationwide Setting. N. Engl. J. Med. 2021, 385, 1078–1090. [Google Scholar] [CrossRef]
- Mansanguan, S.; Charunwatthana, P.; Piyaphanee, W.; Dechkhajorn, W.; Poolcharoen, A.; Mansanguan, C. Cardiovascular Manifestation of the BNT162b2 mRNA COVID-19 Vaccine in Adolescents. Trop. Med. Infect. Dis. 2022, 7, 196. [Google Scholar] [CrossRef]
- Ling, R.R.; Ramanathan, K.; Tan, F.L.; Tai, B.C.; Somani, J.; Fisher, D.; MacLaren, G. Myopericarditis following COVID-19 vaccination and non-COVID-19 vaccination: A systematic review and meta-analysis. Lancet Respir. Med. 2022, 10, 679–688. [Google Scholar] [CrossRef]
- Su, J.R.; McNeil, M.M.; Welsh, K.J.; Marquez, P.L.; Ng, C.; Yan, M.; Cano, M.V. Myopericarditis after vaccination, vaccine adverse event reporting system (VAERS), 1990–2018. Vaccine 2021, 39, 839–845. [Google Scholar] [CrossRef]
- Engler, R.J.M.; Nelson, M.R.; Collins, L.C., Jr.; Spooner, C.; Hemann, B.A.; Gibbs, B.T.; Atwood, J.E.; Howard, R.S.; Chang, A.S.; Cruser, D.L.; et al. A Prospective Study of the Incidence of Myocarditis/Pericarditis and New Onset Cardiac Symptoms following Smallpox and Influenza Vaccination. PLoS ONE 2015, 10, e0118283. [Google Scholar] [CrossRef]
- McMahon, A.W.; Zinderman, C.; Ball, R.; Gupta, G.; Braun, M.M. Comparison of military and civilian reporting rates for smallpox vaccine adverse events. Pharmacoepidemiol. Drug Saf. 2007, 16, 597–604. [Google Scholar] [CrossRef]
- Weiss, S.R. Myocarditis Cases After mRNA-Based COVID-19 Vaccination in the US. JAMA 2022, 327, 2019–2020. [Google Scholar] [CrossRef]
- L’Angiocola, P.D. Myocarditis, COVID-19 and Anti-Sarscov2 Vaccines in Adolescents: Are We Really. Ital. J. Prev. Diagn. Ther. Med. 2021, 4, 8–12. [Google Scholar]
- Dancea, A.B. Myocarditis in infants and children: A review for the paediatrician. Paediatr. Child Health 2001, 6, 543–545. [Google Scholar] [CrossRef]
- Power, J.R.; Keyt, L.K.; Adler, E.D. Myocarditis following COVID-19 vaccination: Incidence, mechanisms, and clinical considerations. Expert Rev. Cardiovasc. Ther. 2022, 20, 241–251. [Google Scholar] [CrossRef]
- Patrignani, A.; Palmieri, G.; Ciampani, N.; Moretti, V.; Mariani, A.; Racca, L. Under-reporting of adverse drug reactions, a problem that also involves medicines subject to additional monitoring. Preliminary data from a single-center experience on novel oral anticoagulants. G. Ital. Cardiol. (2006) 2018, 19, 54–61. [Google Scholar]
- Segec, A.; Slattery, J.; Morales, D.R.; Januskiene, J.; Kurz, X.; Arlett, P. Does additional monitoring status increase the reporting of adverse drug reaction s? An interrupted time series analysis of EudraVigilance data. Pharmacoepidemiol. Drug Saf. 2021, 30, 350–359. [Google Scholar] [CrossRef] [PubMed]
- Hazell, L.; Shakir, S.A. Under-reporting of adverse drug reactions: A systematic review. Drug Saf. 2006, 29, 385–396. [Google Scholar] [CrossRef]
- Danova, J.; Kocourkova, A.; Celko, A.M. Active surveillance study of adverse events following immunisation of children in the Czech Republic. BMC Public Health 2017, 17, 167. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, N.; Crescioli, G.; Bettiol, A.; Marconi, E.; Vitiello, A.; Bonaiuti, R.; Calvani, A.M.; Masi, S.; Lucenteforte, E.; Mugelli, A.; et al. Characterization of serious adverse drug reactions as cause of emergency department visit in children: A 5-years active pharmacovigilance study. BMC Pharmacol. Toxicol. 2018, 19, 16. [Google Scholar]
- Patrignani, A.; Palmieri, G.; Ciampani, N.; Moretti, V.; Maracchini, G.; Mariani, A.; Racca, L. Under-Reporting of Adverse Events Following Immunization Observed in a Single Hospital Setting in Italy. G. Ital. Farm. Farm. 2019, 11, 19–28. [Google Scholar]
- Chua, G.T.; Tsao, S.; Kwan, M.Y.W.; Yu, T.C.; Leung, A.S.Y.; Li, K.W.; Chow, C.C.K.; Ku, W.H.; Kwok, J.; To, K.K.W.; et al. Medium-term outcomes of myocarditis and pericarditis following BNT162b2 vaccination among adolescents in Hong Kong. Emerg. Microbes Infect. 2022, 11, 2466–2473. [Google Scholar] [CrossRef]
- Kracalik, I.; Oster, M.E.; Broder, K.R.; Cortese, M.M.; Glover, M.; Shields, K.; Creech, C.B.; Romanson, B.; Novosad, S.; Soslow, J.; et al. Outcomes at least 90 days since onset of myocarditis after mRNA COVID-19 vaccination in adolescents and young adults in the USA: A follow-up surveillance study. Lancet Child Adolesc. Health 2022, 6, 788–798. [Google Scholar] [CrossRef]
- Voleti, N.; Reddy, S.P.; Ssentongo, P. Myocarditis in SARS-CoV-2 infection vs. COVID-19 vaccination: A systematic review and meta-analysis. Front. Cardiovasc. Med. 2022, 9, 2059. [Google Scholar]
- Abecasis, F. The benefits of COVID-19 vaccination programmes for children may not outweigh the risks. Acta Paediatr. 2022, 111, 1843–1845. [Google Scholar] [CrossRef]
- Ellenberg, S.S.; Foulkes, M.A.; Midthun, K.; Goldenthal, K.L. Evaluating the safety of new vaccines: Summary of a workshop. Am. J. Public Health 2005, 95, 800–807. [Google Scholar] [CrossRef]
- Ellenberg, S.S.; Chen, R.T. The complicated task of monitoring vaccine safety. Public Health Rep. 1997, 112, 10. [Google Scholar] [PubMed]
- Stephenson, W.P.; Hauben, M. Data mining for signals in spontaneous reporting databases: Proceed with caution. Pharmacoepidemiol. Drug Saf. 2007, 16, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Bahri, P.; Rägo, L. CIOMS Guide To Vaccine Safety Communication–Executive summary. Vaccine 2019, 37, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Iskander, J.K.; Miller, E.R.; Chen, R.T. The Role of the Vaccine Adverse Event Reporting System (VAERS) in Monitoring Vaccine Safety. Pediatr. Ann. 2004, 33, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Xu, E.; Bowe, B.; Al-Aly, Z. Long-term cardiovascular outcomes of COVID-19. Nat. Med. 2022, 28, 583–590. [Google Scholar] [CrossRef]
- Tuvali, O.; Tshori, S.; Derazne, E.; Hannuna, R.R.; Afek, A.; Haberman, D.; Sella, G.; George, J. The Incidence of Myocarditis and Pericarditis in Post COVID-19 Unvaccinated Patients—A Large Population-Based Study. J. Clin. Med. 2022, 11, 2219. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pfizer-BioNTech (Excluding Moderna Vaccine Reports) | Moderna (Excluding Pfizer-BioNTech Vaccine Reports) | All mRNA Combined | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Vaccine Dose Number | Cases | PRR (PRR025, PRR975) | IC (IC025, IC975) | Cases | PRR (PRR025, PRR975) | IC (IC025, IC975) | Cases | PRR (PRR025, PRR975) | IC (IC025, IC975) |
| Dose 1 | 736 | 2.0 (1.75, 2.29) | 0.36 (0.24, 0.45) | 524 | 1.21 (1.05, 1.40) | 0.11 (−0.04, 0.21) | 1260 | 1.58 (1.39, 1.79) | 0.15 (0.06, 0.22) |
| Dose 2 | 1509 | 4.39 (3.87, 4.98) | 0.63 (0.55, 0.69) | 716 | 2.62 (2.29, 3.0) | 0.56 (0.43, 0.64) | 2225 | 3.61 (3.19, 4.07) | 0.38 (0.31, 0.43) |
| Dose 3 | 308 | 3.47 (2.29, 4.07) | 1.14 (0.95, 1.27) | 187 | 2.05 (2.08, 3.0) | 0.94 (0.69, 1.11) | 495 | 3.03 (2.62, 3.50) | 0.81 (0.66, 0.92) |
| Dose 4 | 13 | 1.07 (0.61, 1.86) | 0.09 (−0.84, 0.74) | 10 | 0.87 (0.46, 1.63) | −0.20 (−1.27, 0.53) | 23 | 0.97 (0.64, 1.49) | −0.04 (−0.74, 0.45) |
| Dose 5 | 2 | N/A | N/A | 0 | N/A | NR | 2 | N/A | N/A |
| Adverse Event Following Immunization | mRNA Vaccine Dose Number | Age Groups: | Infants, Toddlers, and Preschoolers (6 Months to 4 Years) | Middle Childhood (5 to 11 Years) | Young Teens and Adolescents (12 to 17 Years) | Young Adults (18 to 24 Years) | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Sex: | F | M | F | M | F | M | F | M | ||
| Myo/pericarditis | 1st dose | Cases | 0 | 0 | 2 | 7 | 21 | 110 | 41 | 141 |
| PRR (PRR025, PRR975) | N/A | N/A | N/A | 4.8 (2.3, 10.0) | 7.8 (1.1, 58.3) | 4.1 (2.1, 8.1) | 2.9 (1.1, 7.3) | 3.3 (2.1, 5.2) | ||
| IC (IC025, IC975) | N/A | N/A | N/A | 0.8 (−0.6, 1.6) | 0.4 (−0.3, 1) | 0.3 (−0.1, 0.5) | 0.3 (−0.3, 0.6) | 0.4 (0.1, 0.6) | ||
| 2nd dose | Cases | 1 | 1 | 1 | 11 | 45 | 363 | 66 | 367 | |
| PRR (PRR025, PRR975) | N/A | N/A | N/A | 12.2 (6.7, 21.9) | 25.2 (3.5, 183.1) | 15 (7.8, 29.1) | 6.6 (2.7, 16.5) | 11.7 (7.7, 17.8) | ||
| IC (IC025, IC975) | N/A | N/A | N/A | 1.1(0.1, 1.8) | 0.6 (0.1, 1) | 0.4 (0.3, 0.6) | 0.5 (0.1, 0.8) | 0.7 (0.5, 0.8) | ||
| Chest pain | 1st dose | Cases | 6 | 4 | 32 | 58 | 149 | 285 | 434 | 326 |
| PRR (PRR025, PRR975) | 12.8 (3.2, 51.2) | 5.7 (1.7, 18.9) | 7 (2.1, 22.7) | 3.6 (1.9, 6.9) | 3.5 (2.1, 5.8) | 4 (2.6, 6) | 1.6 (1.3, 2) | 1.9 (1.5, 2.4) | ||
| IC (IC025, IC975) | 2.3 (0.9, 3.2) | 2.1 (0.3, 3.1) | 0.6 (0, 1) | 0.5 (0.1, 0.8) | 0.3 (0, 0.5) | 0.3 (0.1, 0.4) | 0.1 (0, 0.3) | 0.3 (0.1, 0.4) | ||
| 2nd dose | Cases | 5 | 5 | 27 | 40 | 216 | 667 | 380 | 517 | |
| PRR (PRR025, PRR975) | 30 (7.2, 125.3) | 31.6 (10.4, 95.9) | 9.5 (2.9, 31.3) | 4 (2.1, 7.8) | 7.6 (4.6, 12.6) | 10.4 (6.9, 15.6) | 2 (1.6, 2.5) | 4.1 (3.3, 5.1) | ||
| IC (IC025, IC975) | 3.6 (2, 4.6) | 4.3 (2.7, 5.3) | 0.9 (0.2, 1.3) | 0.7 (0.2, 1.1) | 0.5 (0.3, 0.7) | 0.4 (0.3, 0.5) | 0.3 (0.1, 0.4) | 0.6 (0.4, 0.7) | ||
| Dyspnea | 1st dose | Cases | 27 | 15 | 41 | 39 | 249 | 184 | 754 | 324 |
| PRR (PRR025, PRR975) | 7.2 (4.2, 12.5) | 6.6 (3.5, 12.4) | 0.9 (0.6, 1.5) | 1.7 (0.9, 3) | 1.8 (1.3, 2.4) | 2.7 (1.7, 4.1) | 1.3 (1.1, 1.5) | 1.3 (1, 1.5) | ||
| IC (IC025, IC975) | 2 (1.3, 2.4) | 2.2 (1.3, 2.8) | 0 (−0.6, 0.3) | 0.3 (−0.3, 0.6) | 0.2 (0, 0.3) | 0.2 (0, 0.4) | 0.1 (0, 0.2) | 0.1 (−0.1, 0.2) | ||
| 2nd dose | Cases | 11 | 8 | 22 | 29 | 205 | 232 | 514 | 281 | |
| PRR (PRR025, PRR975) | 8.2 (4.1, 16.8) | 15.5 (7.1,34) | 0.8 (0.5, 1.4) | 2 (1.1, 3.7) | 2.2 (1.6, 3) | 3.8 (2.5, 5.8) | 1.3 (1.1, 1.5) | 1.5 (1.2, 1.8) | ||
| IC (IC025, IC975) | 2.6 (1.6, 3.3) | 3.6 (2.4, 4.4) | −0.2 (−0.9, 0.3) | 0.4 (−0.2, 0.9) | 0.3 (0.1, 0.5) | 0.3 (0.1, 0.5) | 0.1 (0, 0.2) | 0.2 (0, 0.4) | ||
| Palpitation | 1st dose | Cases | 9 | 2 | 4 | 13 | 46 | 57 | 211 | 113 |
| PRR (PRR025, PRR975) | 28.8 (6.2, 133.4) | N/A | 0.2 (0.1, 0.7) | 8.9 (1.2, 68) | 1.1 (0.6, 1.9) | 2.1 (1.1, 4.3) | 1.3 (1, 1.7) | 1.8 (1.2, 2.6) | ||
| IC (IC025, IC975) | 2.6 (1.5, 3.4) | N/A | −1.3 (−3, −0.2) | 0.6 (−0.3, 1.3) | 0 (−0.5, 0.4) | 0.2 (−0.2, 0.5) | 0.1 (−0.1, 0.3) | 0.2 (−0.1, 0.5) | ||
| 2nd dose | Cases | 3 | 0 | 7 | 6 | 50 | 70 | 145 | 94 | |
| PRR (PRR025, PRR975) | 27 (4.5, 161.3) | N/A | 0.6 (0.2, 1.6) | 6.6 (0.8, 55) | 1.8 (1, 3.1) | 2.9 (1.4, 5.8) | 1.3 (0.9, 1.7) | 2 (1.4, 3) | ||
| IC (IC025, IC975) | 3.5 (1.4, 4.7) | N/A | −0.4 (−1.7, 0.5) | 0.9 (−0.6, 1.8) | 0.2 (−0.2, 0.6) | 0.3 (−0.1, 0.6) | 0.1 (−0.2, 0.3) | 0.3 (0, 0.6) | ||
| Tachycardia | 1st dose | Cases | 7 | 1 | 6 | 12 | 40 | 30 | 155 | 45 |
| PRR (PRR025, PRR975) | 3.5 (1.4, 8.6) | N/A | 3.9 (0.5, 32.5) | 2.1 (0.7, 6.4) | 0.8 (0.5, 1.4) | 3.4 (1, 11) | 1.7 (1.2, 2.5) | 1.2 (0.7, 1.9) | ||
| IC (IC025, IC975) | 1.4 (0.1, 2.2) | N/A | 0.5 (−0.9, 1.4) | 0.3 (−0.6, 1) | −0.1 (−0.6, 0.3) | 0.3 (−0.3, 0.7) | 0.2 (−0.1, 0.4) | 0.1 (−0.4, 0.4) | ||
| 2nd dose | Cases | 2 | 1 | 6 | 5 | 36 | 27 | 114 | 46 | |
| PRR (PRR025, PRR975) | N/A | N/A | 6.3 (0.7, 52.6) | 1.4 (0.4, 5.1) | 1.1 (0.6, 1.9) | 3.4 (1, 11.1) | 1.8 (1.2, 2.7) | 1.6 (1, 2.7) | ||
| IC (IC025, IC975) | N/A | N/A | 0.8 (−0.6, 1.7) | 0.2 (−1.3, 1.2) | 0.1 (−0.5, 0.4) | 0.3 (−0.3, 0.8) | 0.2 (−0.1, 0.5) | 0.2 (−0.2, 0.6) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alami, A.; Villeneuve, P.J.; Farrell, P.J.; Mattison, D.; Farhat, N.; Haddad, N.; Wilson, K.; Gravel, C.A.; Crispo, J.A.G.; Perez-Lloret, S.; et al. Myocarditis and Pericarditis Post-mRNA COVID-19 Vaccination: Insights from a Pharmacovigilance Perspective. J. Clin. Med. 2023, 12, 4971. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12154971
Alami A, Villeneuve PJ, Farrell PJ, Mattison D, Farhat N, Haddad N, Wilson K, Gravel CA, Crispo JAG, Perez-Lloret S, et al. Myocarditis and Pericarditis Post-mRNA COVID-19 Vaccination: Insights from a Pharmacovigilance Perspective. Journal of Clinical Medicine. 2023; 12(15):4971. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12154971
Chicago/Turabian StyleAlami, Abdallah, Paul J. Villeneuve, Patrick J. Farrell, Donald Mattison, Nawal Farhat, Nisrine Haddad, Kumanan Wilson, Christopher A. Gravel, James A. G. Crispo, Santiago Perez-Lloret, and et al. 2023. "Myocarditis and Pericarditis Post-mRNA COVID-19 Vaccination: Insights from a Pharmacovigilance Perspective" Journal of Clinical Medicine 12, no. 15: 4971. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12154971