
Right Atrial Phasic Function in Heart Failure with Preserved Ejection Fraction: Cardiac Magnetic Resonance Feature Tracking and Outcomes
 , , , ,
, , , ,  , ,
, , 
Abstract
:1. Introduction
- (1)
- The impact of phasic RA volumes und function on cardiovascular outcomes for HFpEF patients in SR;
- (2)
- The correlation of phasic RA volumes and function with markers of cardiovascular and pulmonary vascular performance;
- (3)
- The impact of RA volumes and ejection fraction on cardiovascular outcome for HFpEF patients in persistent AF;
- (4)
- The correlation of RA volumes and ejection fraction with markers of cardiovascular and pulmonary vascular performance.
2. Materials and Methods
2.1. Study Design
2.2. Clinical Definitions
2.3. Outcome Measures
2.4. Assessment Techniques
2.4.1. Exercise Capacity
2.4.2. Transthoracic Echocardiography
2.4.3. Invasive Hemodynamic Assessment
2.4.4. Cardiac Magnetic Resonance Imaging
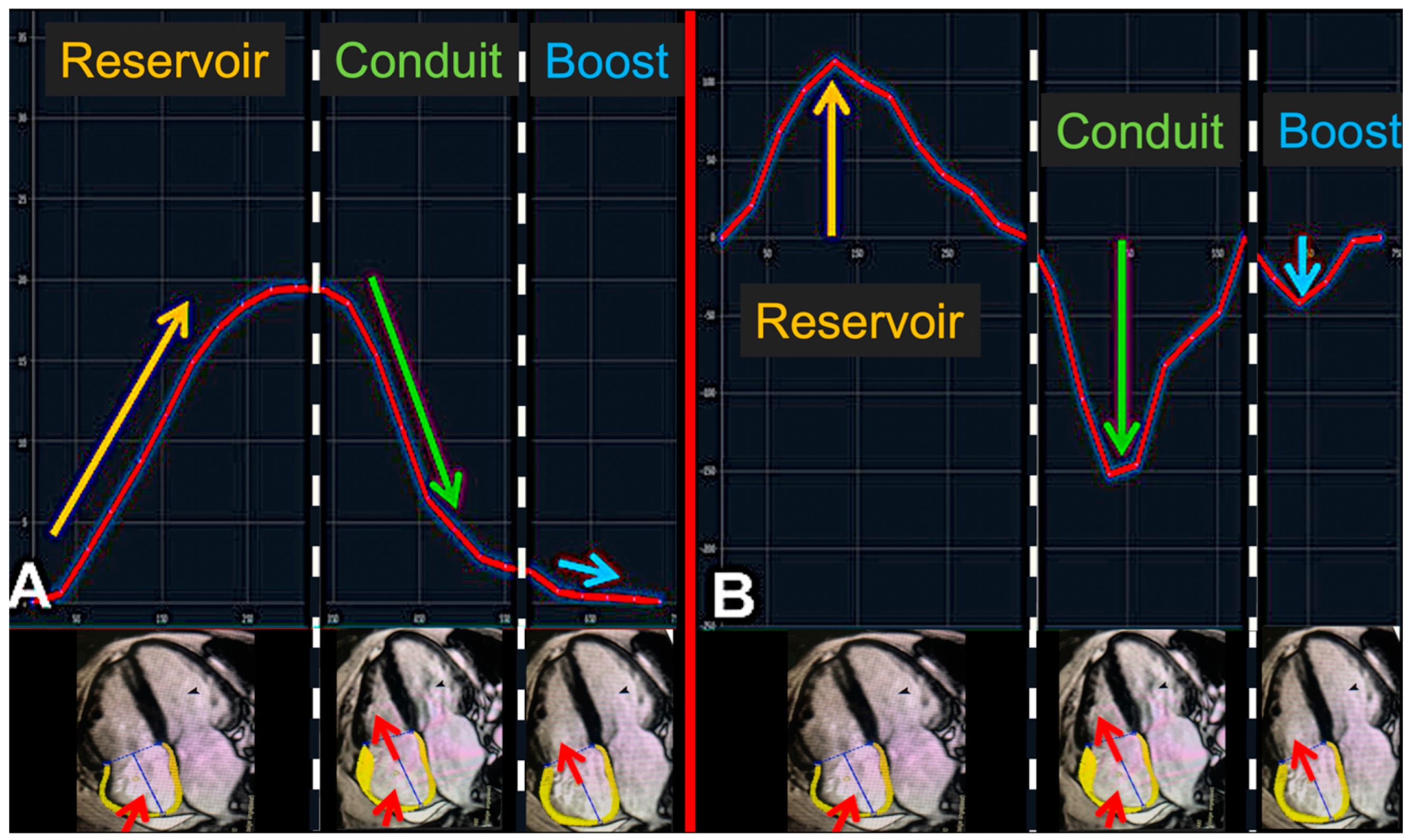
Right Atrial Chamber Evaluation
- (1)
- Reservoir function: atrial diastole during ventricular systole.
- (2)
- Conduit function: subsequent passive atrial emptying starts with the opening of the atrio-ventricular valves.
- (3)
- Booster pump function: active atrial emptying (which is lost in AF).
2.5. Statistical Analysis
3. Results
3.1. Study Population
3.2. Right Atrial Function and Cardiovascular Outcome in Sinus Rhythm and Atrial Fibrillation
3.3. Right Atrial Function in Correlation to Functional Capacity, NT-proBNP Levels, and Pulmonary Vascular Function
4. Discussion
- (1)
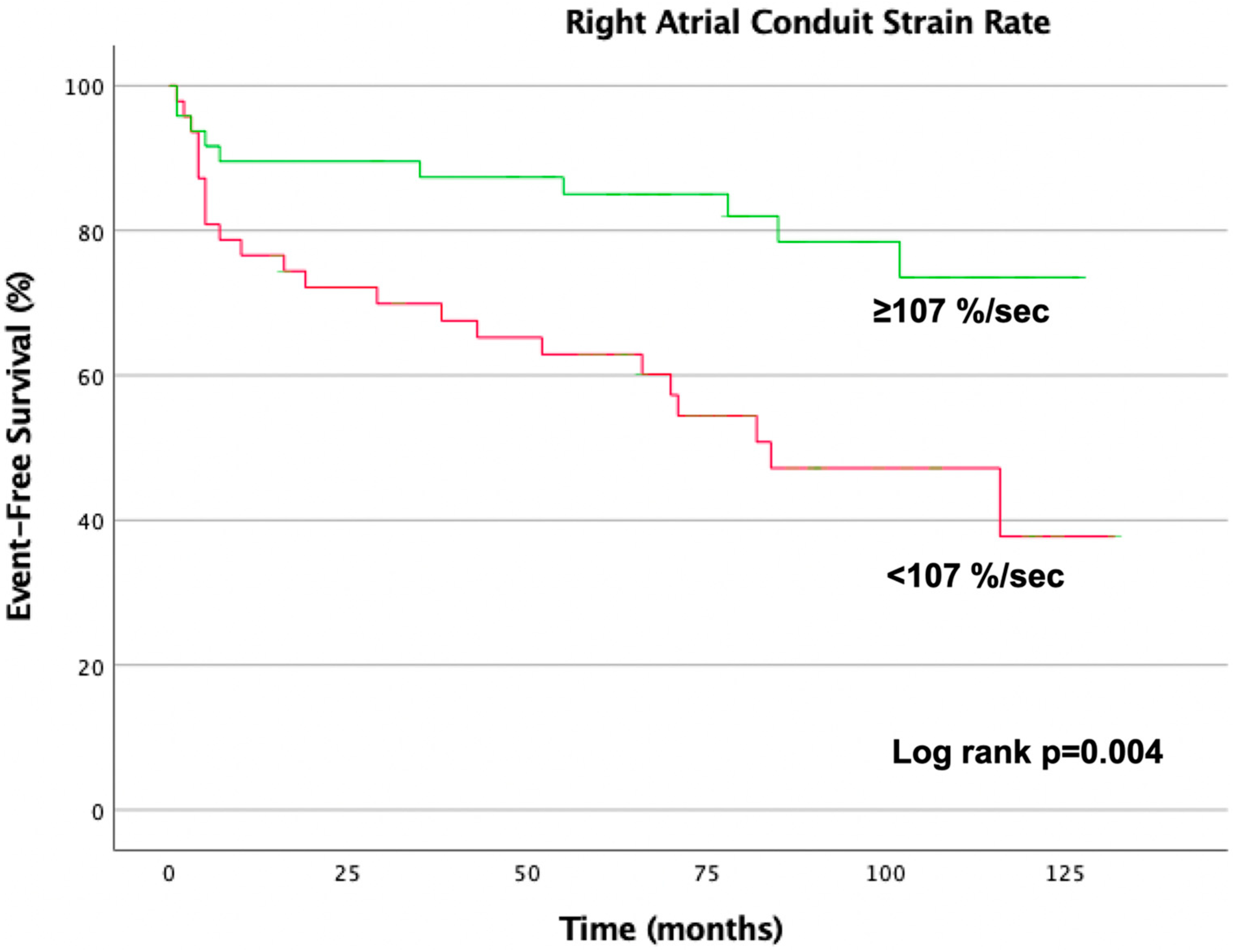
- For patients in SR, parameters of the RA reservoir and conduit function show (in contrast to booster pump function) a robust relation to cardiovascular outcome, even after adjustment for well-known risk factors in HFpEF.
- (2)
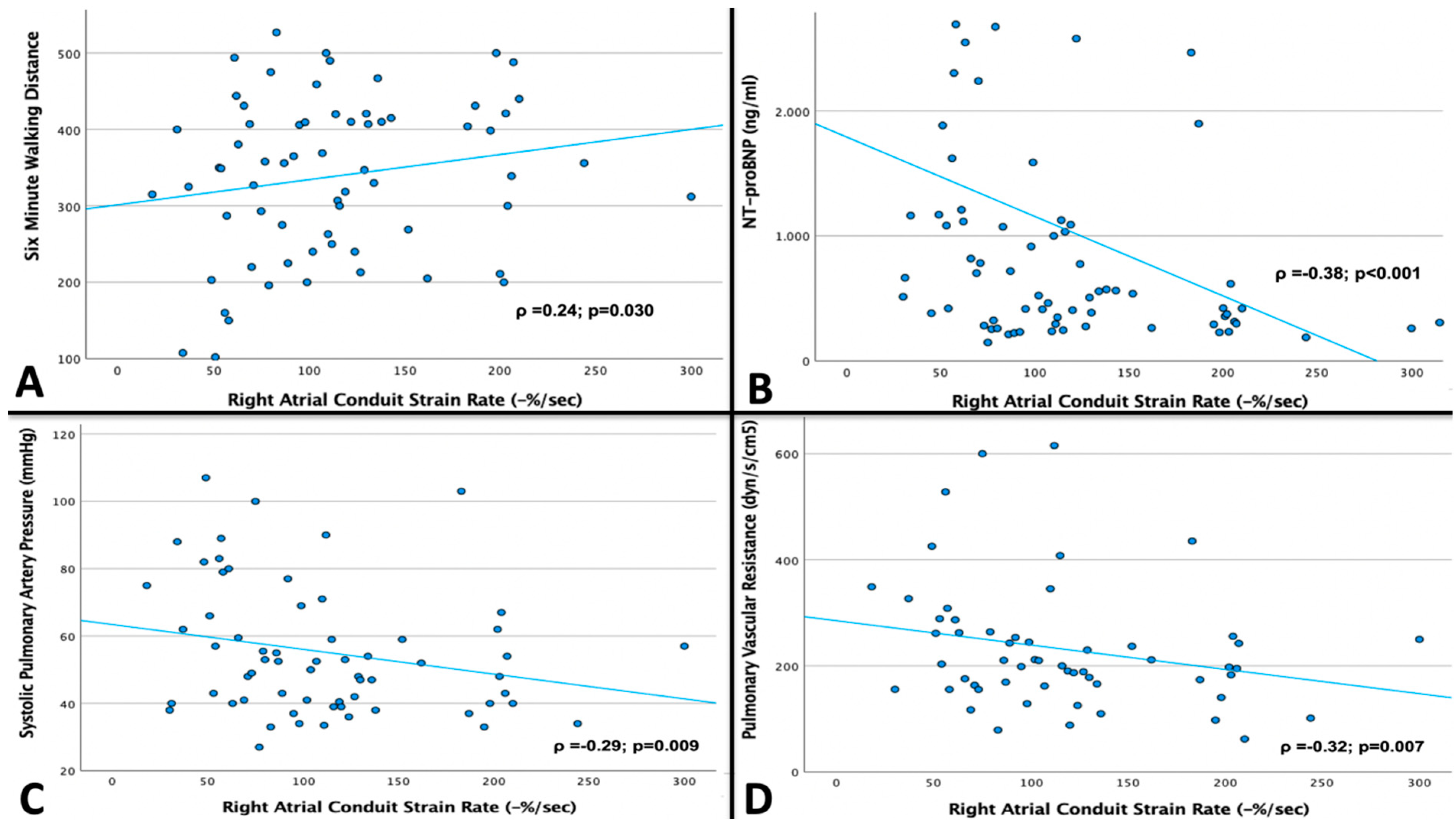
- An impaired RA conduit function shows a significant association with an impaired exercise capacity (6MWD, NT-proBNP) and an impaired pulmonary vascular function (sPAP, PVR).
- (3)
- Regarding baseline characteristics, patients with persistent AF showed markers of pronounced disease progression. However, parameters of RA function did not relate to cardiovascular outcome, nor did they correlate to parameters of exercise capacity and pulmonary vascular function in this patient population.
4.1. Prognostic Value of Right Atrial Volume and Function
4.2. Right Atrial Phasic Function and Its Relation with Exercise Capacity and Pulmonary Vascular Function
4.3. Prognostic Impact of Right Atrial Function in Heart Failure with Preserved Ejection Fraction and Atrial Fibrillation
5. Clinical Implications
6. Conclusions
7. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Kittleson, M.M.; Panjrath, G.S.; Amancherla, K.; Davis, L.L.; Deswal, A.; Dixon, D.L.; Januzzi, J.L.; Yancy, C.W. 2023 ACC Expert Consensus Decision Pathway on Management of Heart Failure with Preserved Ejection Fraction: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2023, 81, 1835–1878. [Google Scholar] [CrossRef] [PubMed]
- Redfield, M.M. Heart Failure with Preserved Ejection Fraction. N. Engl. J. Med. 2016, 375, 1868–1877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paulus, W.J.; Tschöpe, C. A novel paradigm for heart failure with preserved ejection fraction: Comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J. Am. Coll. Cardiol. 2013, 62, 263–271. [Google Scholar] [CrossRef] [Green Version]
- Zakeri, R.; Moulay, G.; Chai, Q.; Ogut, O.; Hussain, S.; Takahama, H.; Lu, T.; Wang, X.-L.; Linke, W.A.; Lee, H.-C.; et al. Left Atrial Remodeling and Atrioventricular Coupling in a Canine Model of Early Heart Failure with Preserved Ejection Fraction. Circ. Heart Fail. 2016, 9, e003238. [Google Scholar] [CrossRef] [Green Version]
- Melenovsky, V.; Hwang, S.-J.; Redfield, M.M.; Zakeri, R.; Lin, G.; Borlaug, B.A. Left atrial remodeling and function in advanced heart failure with preserved or reduced ejection fraction. Circ. Heart Fail. 2015, 8, 295–303. [Google Scholar] [CrossRef] [Green Version]
- Schönbauer, R.; Kammerlander, A.A.; Duca, F.; Aschauer, S.; Koschutnik, M.; Dona, C.; Nitsche, C.; Loewe, C.; Hengstenberg, C.; Mascherbauer, J. Prognostic impact of left atrial function in heart failure with preserved ejection fraction in sinus rhythm vs. persistent atrial fibrillation. ESC Hear. Fail. 2022, 9, 465–475. [Google Scholar] [CrossRef]
- Schönbauer, R.; Kammerlander, A.A.; Duca, F.; Aschauer, S.; Binder, C.; Zotter-Tufaro, C.; Nitsche, C.; Fiedler, L.; Roithinger, F.X.; Loewe, C.; et al. Impact of Left Atrial Phasic Function in Heart Failure with Preserved Ejection Fraction. JACC Cardiovasc Imaging 2020, 13, 2254–2255. [Google Scholar] [CrossRef]
- Aschauer, S.; Kammerlander, A.A.; Zotter-Tufaro, C.; Ristl, R.; Pfaffenberger, S.; Bachmann, A.; Duca, F.; Marzluf, B.A.; Bonderman, D.; Mascherbauer, J. The right heart in heart failure with preserved ejection fraction: Insights from cardiac magnetic resonance imaging and invasive haemodynamics. Eur. J. Heart Fail. 2016, 18, 71–80. [Google Scholar] [CrossRef]
- Guazzi, M. Pulmonary hypertension in heart failure with preserved ejection fraction: Prevalence, pathophysiology, and clinical perspectives. Circ. Heart Fail. 2014, 7, 367–377. [Google Scholar] [CrossRef] [Green Version]
- Jain, S.; Kuriakose, D.; Edelstein, I.; Ansari, B.; Oldland, G.; Gaddam, S.; Javaid, K.; Manaktala, P.; Lee, J.; Miller, R.; et al. Right Atrial Phasic Function in Heart Failure with Preserved and Reduced Ejection Fraction. JACC Cardiovasc. Imaging 2019, 12, 1460–1470. [Google Scholar] [CrossRef] [PubMed]
- von Roeder, M.; Kowallick, J.T.; Rommel, K.-P.; Blazek, S.; Besler, C.; Fengler, K.; Lotz, J.; Hasenfuß, G.; Lücke, C.; Gutberlet, M.; et al. Right atrial–right ventricular coupling in heart failure with preserved ejection fraction. Clin. Res. Cardiol. 2020, 109, 54–66. [Google Scholar] [CrossRef] [PubMed]
- Schönbauer, R.; Duca, F.; Kammerlander, A.A.; Aschauer, S.; Binder, C.; Zotter-Tufaro, C.; Koschutnik, M.; Fiedler, L.; Roithinger, F.X.; Loewe, C.; et al. Persistent atrial fibrillation in heart failure with preserved ejection fraction: Prognostic relevance and association with clinical, imaging and invasive haemodynamic parameters. Eur. J. Clin. Investig. 2020, 50, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Agner, B.F.R.; Kühl, J.T.; Linde, J.J.; Kofoed, K.F.; Åkeson, P.; Rasmussen, B.V.; Jensen, G.B.; Dixen, U. Assessment of left atrial volume and function in patients with permanent atrial fibrillation: Comparison of cardiac magnetic resonance imaging, 320-slice multi-detector computed tomography, and transthoracic echocardiography. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 532–540. [Google Scholar] [CrossRef] [Green Version]
- Maceira, A.M.; Cosin-Sales, J.; Prasad, S.K.; Pennell, D.J. Characterization of left and right atrial function in healthy volunteers by cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2016, 18, 64. [Google Scholar] [CrossRef] [Green Version]
- McMurray, J.J.V.; Adamopoulos, S.; Anker, S.D.; Auricchio, A.; Böhm, M.; Dickstein, K.; Falk, V.; Filippatos, G.; Fonseca, C.; Gomez-Sanchez, M.A.; et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart. Eur. Heart J. 2012, 33, 1787–1847. [Google Scholar] [CrossRef]
- Bonderman, D.; Agis, H.; Kain, R.; Mascherbauer, J. Amyloid in the heart: An under-recognized threat at the interface of cardiology, haematology, and pathology. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 978–980. [Google Scholar] [CrossRef]
- Enright, P.L.; Sherrill, D.L. Reference equations for the six-minute walk in healthy adults. Am. J. Respir. Crit. Care Med. 1998, 158, 1384–1387. [Google Scholar] [CrossRef] [Green Version]
- Kramer, C.M.; Barkhausen, J.; Flamm, S.D.; Kim, R.J.; Nagel, E.; Protocols S for CMRB of TTF on, S. Standardized cardiovascular magnetic resonance (CMR) protocols 2013 update. J. Cardiovasc. Magn. Reson. 2013, 15, 91. [Google Scholar] [CrossRef] [Green Version]
- Messroghli, D.R.; Moon, J.C.; Ferreira, V.M.; Grosse-Wortmann, L.; He, T.; Kellman, P.; Mascherbauer, J.; Nezafat, R.; Salerno, M.; Schelbert, E.B.; et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J. Cardiovasc. Magn. Reson. 2017, 19, 75. [Google Scholar] [CrossRef] [Green Version]
- Krittanawong, C.; Maitra, N.S.; Virk, H.U.H.; Farrell, A.; Hamzeh, I.; Arya, B.; Pressman, G.S.; Wang, Z.; Marwick, T.H. Normal Ranges of Right Atrial Strain: A Systematic Review and Meta-Analysis. Cardiovasc. Imaging 2022, 16, 282–294. [Google Scholar] [CrossRef]
- Sallach, J.A.; Tang, W.W.; Borowski, A.G.; Tong, W.; Porter, T.; Martin, M.G.; Jasper, S.E.; Shrestha, K.; Troughton, R.W.; Klein, A.L. Right atrial volume index in chronic systolic heart failure and prognosis. JACC Cardiovasc. Imaging 2009, 2, 527–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ivanov, A.; Mohamed, A.; Asfour, A.; Ho, J.; Khan, S.A.; Chen, O.; Klem, I.; Ramasubbu, K.; Brener, S.J.; Heitner, J.F. Right atrial volume by cardiovascular magnetic resonance predicts mortality in patients with heart failure with reduced ejection fraction. PLoS ONE 2017, 12, e0173245. [Google Scholar] [CrossRef] [PubMed]
- Maurer, M.S.; Packer, M. Impaired systemic venous capacitance: The neglected mechanism in patients with heart failure and a preserved ejection fraction? Eur. J. Heart Fail. 2020, 22, 173–176. [Google Scholar] [CrossRef]
- Kotecha, D.; Lam, C.S.P.; Van Veldhuisen, D.J.; Van Gelder, I.C.; Voors, A.A.; Rienstra, M. Heart Failure with Preserved Ejection Fraction and Atrial Fibrillation. J. Am. Coll. Cardiol. 2016, 68, 2217–2228. [Google Scholar] [CrossRef]
- Solomon, S.D.; McMurray, J.J.V.; Anand, I.S.; Junbo Ge, D.P.; Lam, C.S.P.; Maggioni, A.P.; Martinez, F.; Packer, M.; Pfeffer, M.A.; Pieske, B.; et al. Angiotensin–Neprilysin Inhibition in Heart Failure with Preserved Ejection Fraction. N. Engl. J. Med. 2019, 381, 1609–1620. [Google Scholar] [CrossRef] [Green Version]
- Anker, S.D.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Bocchi, E.; Böhm, M.; Brunner–La Rocca, H.-P.; Choi, D.-J.; Chopra, V.; Chuquiure-Valenzuela, E.; et al. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N. Engl. J. Med. 2021, 385, 1451–1461. [Google Scholar] [CrossRef]
- Solomon, S.D.; McMurray, J.J.V.; Claggett, B.; de Boer, R.A.; DeMets, D.; Hernandez, A.F.; Inzucchi, S.E.; Kosiborod, M.N.; Lam, C.S.P.; Martinez, F.; et al. Dapagliflozin in Heart Failure with Mildly Reduced or Preserved Ejection Fraction. N. Engl. J. Med. 2022, 387, 1089–1098. [Google Scholar] [CrossRef]
- Fudim, M.; Fail, P.S.; Litwin, S.E.; Shaburishvili, T.; Goyal, P.; Hummel, S.L.; Borlaug, B.A.; Mohan, R.C.; Patel, R.B.; Mitter, S.S.; et al. Endovascular ablation of the right greater splanchnic nerve in heart failure with preserved ejection fraction: Early results of the REBALANCE-HF trial roll-in cohort. Eur. J. Heart Fail. 2022, 24, 1410–1414. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable |
Sinus Rhythm (n = 96) |
AF (n = 92) | p-Value |
|---|---|---|---|
| Clinical parameters | |||
| Age, y | 69 ± 9 | 72 ± 8 | 0.023 |
| Female sex, n (%) | 75 (78) | 58 (63) | 0.026 |
| Body mass index, kg/m2 | 31 ± 6 | 30 ± 6 | 0.432 |
| Paroxysmal AF (%) | 30 (31) | 0 (0) | <0.001 |
| Persistent AF (%) | 0 (0) | 92 (100) | <0.001 |
| Diabetes mellitus type II, n (%) | 37 (39) | 30 (33) | 0.446 |
| Hyperlipidemia, n (%) | 56 (58) | 44 (48) | 0.144 |
| Arterial hypertension, n (%) | 89 (93) | 89 (97) | 0.497 |
| Heart rate, (beats/min) | 69 ± 14 | 73 ± 13 | 0.010 |
| 6MWD, m | 344 ± 112 | 318 ± 120 | 0.109 |
| Sleep apnea, n (%) | 8 (8) | 12 (13) | 0.350 |
| COPD, n (%) | 26 (27) | 32 (35) | 0.190 |
| NYHA functional class, n (%) | 0.003 | ||
| II | 45 (47) | 26 (28) | |
| III | 49 (51) | 58 (63) | |
| IV | 2 (2) | 8 (9) | |
| NT-proBNP, ng/mL | 0.52 (0.32 to 1.16) | 1.60 (1.04 to 2.42) | <0.001 |
| Glycated hemoglobin, % | 6.1 ± 1.3 | 6.1 ± 0.7 | 0.470 |
| eGFR, mL/min/1.73 m2 | 60 ± 18 | 62 ± 19 | 0.719 |
| Gamma-Glutamyl-Transferase, U/L | 27 (19 to 41) | 47 (29 to 94) | <0.001 |
| HMG-CoA reductase inhibitor, n (%) | 48 (50) | 36 (39) | 0.106 |
| Betablocker, n (%) | 67 (70) | 66 (72) | 1.000 |
| Diuretics, n (%) | 69 (72) | 72 (78) | 0.605 |
| ACE inhibitor, n (%) | 21 (22) | 31 (34) | 0.104 |
| AT II receptor antagonist, n (%) | 41 (43) | 33 (36) | 0.296 |
| Cardiac magnetic resonance imaging parameters | |||
| LV end-diastolic diameter, mm | 47 ± 6 | 47 ± 6 | 0.565 |
| RV end-diastolic diameter, mm | 39 ± 7 | 43 ± 8 | <0.001 |
| Interventricular septum, mm | 11 ± 2 | 11 ± 2 | 0.754 |
| LA diameter, mm | 68 ± 8 | 75 ± 10 | <0.001 |
| LA area, cm2 | 30 ± 7 | 37 ± 9 | <0.001 |
| RA diameter, mm | 61 ± 7 | 70 ± 10 | <0.001 |
| RA area, cm2 | 25 ± 5 | 35 ± 11 | <0.001 |
| LV ejection fraction, % | 68 ± 9 | 61 ± 6 | <0.001 |
| LV end-diastolic volume, mL | 129 ± 45 | 123 ± 42 | 0.793 |
| Cardiac output, L/min | 5.6 ± 1.9 | 5.1 ± 2.9 | 0.072 |
| RV ejection fraction, % | 56 ± 11 | 47 ± 10 | <0.001 |
| RV end-diastolic volume, mL | 144 ± 46 | 162 ± 65 | 0.053 |
| MOLLI-ECV | 28.0 ± 3.2 | 31.2 ± 4.8 | <0.001 |
| Invasive hemodynamics | |||
| Systolic PAP, mmHg | 53 ± 20 | 54 ± 18 | 0.589 |
| Diastolic PAP, mmHg | 21 ± 8 | 23 ± 7 | 0.112 |
| Mean PAP, mmHg | 33 ± 11 | 35 ± 10 | 0.379 |
| PAWP, mmHg | 19 ± 6 | 20 ± 6 | 0.154 |
| LV end-diastolic pressure, mmHg | 21 ± 7 | 20 ± 6 | 0.439 |
| TPG, mmHg | 14 ± 7 | 14 ± 7 | 0.860 |
| Diastolic pressure gradient, mmHg | 2.0 (−1.0 to 5.0) | 2.0 (−2.0 to 6.0) | 0.634 |
| CO thermodilution, L/min | 5.5 ± 1.4 | 5.0 ± 1.2 | 0.028 |
| PVR, dyn-s-cm−5 | 202 (155 to 254) | 205 (138 to 289) | 0.628 |
| Variable |
Sinus Rhythm (n = 96) |
AF (n = 92) | p-Value |
|---|---|---|---|
| Right Atrial Cardiac Magnetic Resonance Imaging Parameters | |||
| RA Volumetric Analyses | |||
| Vi max., mL/m2 | 46 ± 15 | 85 ± 35 | <0.001 |
| Vi pre A-wave, mL/m2 | 40 ± 14 | / | |
| Vi min., mL/m2 | 27 ± 11 | 77 ± 34 | <0.001 |
| Conduit EF, % | 13 ± 9 | / | |
| Booster pump EF, % | 28 ± 9 | / | |
| Total EF, % | 41 ± 10 | 11 ± 10 | <0.001 |
| RA Strain Analyses | |||
| Reservoir strain, % | 28 ± 12 | / | |
| Conduit strain, -% | 15 ± 9 | / | |
| Booster strain, -% | 13 ± 5 | / | |
| Reservoir strain rate, %/s | 134 ± 63 | / | |
| Conduit strain rate, -%/s | 115 ± 67 | / | |
| Booster strain rate, -%/s | 148 ± 54 | / | |
| Univariate | ||||
|---|---|---|---|---|
| Variable | No Event | Event | Hazard Ratio (95% CI) | p-Value |
| Right atrial magnetic resonance imaging parameters in sinus rhythm | ||||
| (n = 62) | (n = 34) | |||
| RA Volumetric Analyses | ||||
| Maximum Vi, mL/m2 | 47 ± 16 | 44 ± 14 | 0.99 (0.97–1.02) | 0.662 |
| Vi pre A-wave, mL/m2 | 40 ± 14 | 39 ± 13 | 1.00 (0.98–1.03) | 0.887 |
| Minimum Vi, mL/m2 | 28 ± 11 | 26 ± 12 | 1.00 (0.97–1.03) | 0.998 |
| Conduit EF, % | 14 ± 10 | 11 ± 7 | 0.97 (0.94–1.01) | 0.174 |
| Booster EF, % | 28 ± 9 | 30 ± 9 | 1.02 (0.98–1.06) | 0.310 |
| Total EF, % | 41 ± 10 | 41 ± 11 | 0.99 (0.96–1.03) | 0.707 |
| RA Strain Analyses | ||||
| Reservoir strain, % | 30 ± 12 | 24 ± 11 | 0.96 (0.93–0.99) | 0.034 |
| Conduit strain, -% | 16 ± 9 | 12 ± 8 | 0.94 (0.89–0.99) | 0.023 |
| Booster strain, -% | 13 ± 5 | 13 ± 6 | 0.98 (0.92–1.05) | 0.549 |
| Reservoir strain rate,%/s | 143 ± 64 | 117 ± 58 | 0.99 (0.98–0.99) | 0.049 |
| Conduit strain rate, -%/s | 127 ± 71 | 94 ± 53 | 0.99 (0.98–0.99) | 0.014 |
| Booster strain rate, -%/s | 155 ± 53 | 134 ± 54 | 0.99 (0.99–1.00) | 0.063 |
| Adjusted analysis for age, NT-proBNP level, RV EF and NYHA class | ||||
| Reservoir strain | 0.95 (0.91–0.99) | 0.016 | ||
| Reservoir strain rate | 0.99 (0.98–0.99) | 0.028 | ||
| Conduit strain | 0.93 (0.88–0.99) | 0.019 | ||
| Conduit strain rate | 0.99 (0.98–0.99) | 0.011 | ||
| Right atrial magnetic resonance imaging parameters in atrial fibrillation | ||||
| (n = 41) | (n = 51) | |||
| RA Volumetric Analyses | ||||
| Maximum Vi, mL/m2 | 88 ± 32 | 83 ± 37 | 0.99 (0.99–1.01) | 0.516 |
| Minimum Vi, mL/m2 | 78 ± 33 | 76 ± 35 | 0.99 (0.99–1.01) | 0.862 |
| Total EF, % | 15 ± 13 | 10 ± 8 | 0.97 (0.94–0.99) | 0.026 |
| 6MWD m | NT-proBNP ng/mL | sPAP mmHg | PVR dyn-s-cm−5 | |
|---|---|---|---|---|
| ρ | ρ | ρ | ρ | |
| Sinus Rhythm | ||||
| RA conduit function | ||||
| Conduit EF, % | 0.26 * | −0.19 | −0.20 | −0.36 ** |
| Conduit strain, -% | 0.18 | −0.39 ** | −0.32 ** | −0.28 * |
| Conduit SR, -%/s | 0.24 * | −0.38 ** | −0.29 ** | −0.32 ** |
| RA booster pump function | ||||
| Booster pump EF,% | −0.17 | −0.14 | 0.12 | 0.07 |
| Booster strain, -% | −0.19 | −0.17 | 0.02 | −0.16 |
| Booster SR, -%/s | −0.56 | −0.19 | 0.02 | −0.15 |
| RA total EF, % | 0.07 | −0.26 * | −0.10 | −0.27 * |
| RA reservoir function | ||||
| Reservoir strain, % | 0.05 | −0.37 ** | −0.23 * | −0.31 ** |
| Reservoir SR, %/s | 0.04 | −0.43 ** | −0.08 | −0.19 |
| RA volumetric measurements | ||||
| RAVi endsyst., mL/m2 | 0.05 | 0.26 * | 0.13 | −0.05 |
| RAVi pre A, mL/m2 | −0.01 | 0.27 ** | 0.18 | 0.02 |
| RAVi enddiast.mL/m2 | 0.01 | 0.32 ** | 0.13 | 0.04 |
| Atrial Fibrillation | ||||
| RA total EF, % | 0.13 | −0.20 | −0.17 | −0.18 |
| RAVi endsyst., mL/m2 | 0.07 | 0.03 | −0.01 | −0.13 |
| RAVi enddiast.mL/m2 | 0.04 | 0.09 | 0.09 | −0.10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schönbauer, R.; Hana, F.; Duca, F.; Koschutnik, M.; Donà, C.; Nitsche, C.; Sponder, M.; Lenz, M.; Lee, J.; Loewe, C.; et al. Right Atrial Phasic Function in Heart Failure with Preserved Ejection Fraction: Cardiac Magnetic Resonance Feature Tracking and Outcomes. J. Clin. Med. 2023, 12, 5179. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12165179
Schönbauer R, Hana F, Duca F, Koschutnik M, Donà C, Nitsche C, Sponder M, Lenz M, Lee J, Loewe C, et al. Right Atrial Phasic Function in Heart Failure with Preserved Ejection Fraction: Cardiac Magnetic Resonance Feature Tracking and Outcomes. Journal of Clinical Medicine. 2023; 12(16):5179. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12165179
Chicago/Turabian StyleSchönbauer, Robert, Fiona Hana, Franz Duca, Matthias Koschutnik, Carolina Donà, Christian Nitsche, Michael Sponder, Max Lenz, Jonghui Lee, Christian Loewe, and et al. 2023. "Right Atrial Phasic Function in Heart Failure with Preserved Ejection Fraction: Cardiac Magnetic Resonance Feature Tracking and Outcomes" Journal of Clinical Medicine 12, no. 16: 5179. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12165179