

Salivary Complaints in Burning Mouth Syndrome: A Cross Sectional Study on 500 Patients

 ,
,  ,
,  , , ,
, , ,  , , ,
, , ,  and
and
Abstract
:1. Introduction
- -
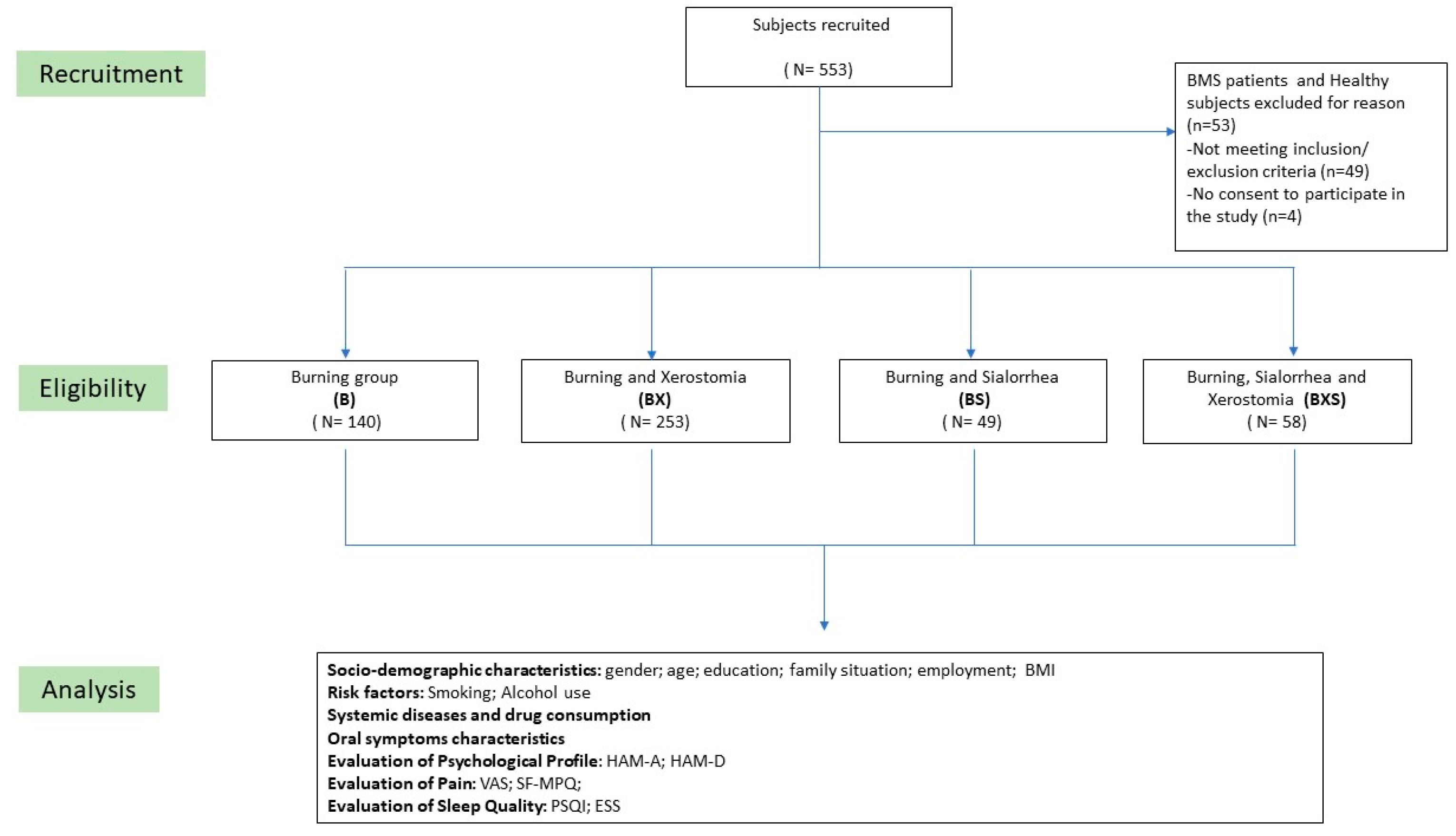
- to investigate the interplay between xerostomia, the subjective sensation of sialorrhea, and the sensation of burning in a large sample of 500 BMS patients.
- -
- to identify potential predictors of xerostomia and subjective sensation of sialorrhea in BMS patients, shedding light on the underlying factors contributing to these complex symptoms.
2. Materials and Methods
2.1. Patients Enrolment
2.2. Inclusion and Exclusion Criteria
2.3. Clinical Assessment
2.4. Salivary Flow Evaluation
2.5. Salivary Glands Imaging
2.6. Neurological Assessment
2.7. Data Analysis
3. Results
3.1. Demographic and Clinical Data
3.2. Systemic Evaluation and Symptoms Characteristics
3.3. Regression Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pedersen, A.M.L.; Sørensen, C.E.; Proctor, G.B.; Carpenter, G.H.; Ekström, J. Salivary Secretion in Health and Disease. J. Oral Rehabil. 2018, 45, 730–746. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, M. Science behind Human Saliva. J. Nat. Sci. Biol. Med. 2011, 2, 53–58. [Google Scholar] [CrossRef]
- Iorgulescu, G. Saliva between Normal and Pathological. Important factors in determining systemic and oral health. J. Med. Life 2009, 2, 303–307. [Google Scholar] [PubMed]
- Kubala, E.; Strzelecka, P.; Grzegocka, M.; Lietz-Kijak, D.; Gronwald, H.; Skomro, P.; Kijak, E. A Review of Selected Studies That Determine the Physical and Chemical Properties of Saliva in the Field of Dental Treatment. Biomed Res. Int. 2018, 2018, 6572381. [Google Scholar] [CrossRef] [PubMed]
- Miranda-Rius, J.; Brunet-Llobet, L.; Lahor-Soler, E.; Farré, M. Salivary Secretory Disorders, Inducing Drugs, and Clinical Management. Int. J. Med. Sci. 2015, 12, 811–824. [Google Scholar] [CrossRef] [PubMed]
- Tschoppe, P.; Wolgin, M.; Pischon, N.; Kielbassa, A.M. Etiologic Factors of Hyposalivation and Consequences for Oral Health. Quintessence Int. 2010, 41, 321–333. [Google Scholar]
- Thakkar, J.P.; Lane, C.J. Hyposalivation and Xerostomia and Burning Mouth Syndrome: Medical Management. Oral Maxillofac. Surg. Clin. N. Am. 2022, 34, 135–146. [Google Scholar] [CrossRef]
- Nederfors, T. Xerostomia and Hyposalivation. Adv. Dent. Res. 2000, 14, 48–56. [Google Scholar] [CrossRef]
- Silva, L.A.; Siqueira, J.T.T.; Teixeira, M.J.; Siqueira, S.R.D.T. The Role of Xerostomia in Burning Mouth Syndrome: A Case-Control Study. Arq. Neuropsiquiatr. 2014, 72, 91–98. [Google Scholar] [CrossRef]
- Gulati, A.; Kidane, J.; Chang, J.L. Patient Reported Outcome Measures for Salivary Function: A Systematic Review. Laryngoscope 2023, 133, 1796–1805. [Google Scholar] [CrossRef]
- Lakraj, A.A.; Moghimi, N.; Jabbari, B. Sialorrhea: Anatomy, Pathophysiology and Treatment with Emphasis on the Role of Botulinum Toxins. Toxins 2013, 5, 1010–1031. [Google Scholar] [CrossRef] [PubMed]
- Paine, C.C.; Snider, J.W. When Saliva Becomes a Problem: The Challenges and Palliative Care for Patients with Sialorrhea. Ann. Palliat. Med. 2020, 9, 1333–1339. [Google Scholar] [CrossRef] [PubMed]
- Boyce, H.W.; Bakheet, M.R. Sialorrhea: A Review of a Vexing, Often Unrecognized Sign of Oropharyngeal and Esophageal Disease. J. Clin. Gastroenterol. 2005, 39, 89–97. [Google Scholar] [PubMed]
- Lee, Y.; Hong, I.; Na, S.; Eun, Y. Evaluation of Salivary Function in Patients with Burning Mouth Syndrome. Oral Dis. 2015, 21, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Simcić, D.; Pezelj-Ribarić, S.; Grzić, R.; Horvat, J.; Brumini, G.; Muhvić-Urek, M. Detection of Salivary Interleukin 2 and Interleukin 6 in Patients with Burning Mouth Syndrome. Mediat. Inflamm. 2006, 2006, 54632. [Google Scholar] [CrossRef] [PubMed]
- Adamo, D.; Calabria, E.; Canfora, F.; Coppola, N.; Pecoraro, G.; D’Aniello, L.; Aria, M.; Mignogna, M.D.; Leuci, S. Burning Mouth Syndrome: Analysis of Diagnostic Delay in 500 Patients. Oral Dis. 2023. [Google Scholar] [CrossRef]
- International Classification of Orofacial Pain, 1st Edition (ICOP). Cephalalgia 2020, 40, 129–221. [CrossRef]
- Alsabbagh, R.; Ouanounou, A. Burning Mouth Syndrome: Etiology, Clinical Presentations, and Treatment Alternatives. Dent. Rev. 2022, 2, 100036. [Google Scholar] [CrossRef]
- Aringhieri, G.; Izzetti, R.; Vitali, S.; Ferro, F.; Gabriele, M.; Baldini, C.; Caramella, D. Ultra-High Frequency Ultrasound (UHFUS) Applications in Sjogren Syndrome: Narrative Review and Current Concepts. Gland. Surg. 2020, 9, 2248–2259. [Google Scholar] [CrossRef]
- Currie, C.C.; Ohrbach, R.; De Leeuw, R.; Forssell, H.; Imamura, Y.; Jääskeläinen, S.K.; Koutris, M.; Nasri-Heir, C.; Huann, T.; Renton, T.; et al. Developing a Research Diagnostic Criteria for Burning Mouth Syndrome: Results from an International Delphi Process. J. Oral Rehabil. 2021, 48, 308–331. [Google Scholar] [CrossRef]
- Veenbergen, S.; Kozmar, A.; van Daele, P.L.A.; Schreurs, M.W.J. Autoantibodies in Sjögren’s Syndrome and Its Classification Criteria. J. Transl. Autoimmun. 2021, 5, 100138. [Google Scholar] [CrossRef] [PubMed]
- Begaud, B. Standardized Assessment of Adverse Drug Reactions: The Method Used in France Special Workshop Clinical. Drug Inf. J. 1984, 18, 275–281. [Google Scholar] [CrossRef]
- Adamo, D.; Celentano, A.; Ruoppo, E.; Cucciniello, C.; Pecoraro, G.; Aria, M.; Mignogna, M.D. The Relationship Between Sociodemographic Characteristics and Clinical Features in Burning Mouth Syndrome. Pain Med. 2015, 16, 2171–2179. [Google Scholar] [CrossRef]
- Adamo, D.; Pecoraro, G.; Aria, M.; Favia, G.; Mignogna, M.D. Vortioxetine in the Treatment of Mood Disorders Associated with Burning Mouth Syndrome: Results of an Open-Label, Flexible-Dose Pilot Study. Pain Med. 2019, 21, 185–194. [Google Scholar] [CrossRef]
- Braud, A.; Touré, B.; Agbo-Godeau, S.; Descroix, V.; Boucher, Y. Characteristics of Pain Assessed with Visual Analog Scale and Questionnaire in Burning Mouth Syndrome Patients: A Pilot Study. J. Orofac. Pain 2013, 27, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Melzack, R. The Short-Form McGill Pain Questionnaire. Pain 1987, 30, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of Adult Pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthr. Care Res. 2011, 63 (Suppl. S11), S240–S252. [Google Scholar] [CrossRef]
- Hamilton, M. A Rating Scale for Depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef]
- Hamilton, M. The Assessment of Anxiety States by Rating. Br. J. Med. Psychol. 1959, 32, 50–55. [Google Scholar] [CrossRef]
- Morriss, R.; Leese, M.; Chatwin, J.; Baldwin, D.; THREAD Study Group. Inter-Rater Reliability of the Hamilton Depression Rating Scale as a Diagnostic and Outcome Measure of Depression in Primary Care. J. Affect. Disord. 2008, 111, 204–213. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A New Instrument for Psychiatric Practice and Research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef] [PubMed]
- Johns, M.W. A New Method for Measuring Daytime Sleepiness: The Epworth Sleepiness Scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [PubMed]
- Curcio, G.; Tempesta, D.; Scarlata, S.; Marzano, C.; Moroni, F.; Rossini, P.M.; Ferrara, M.; De Gennaro, L. Validity of the Italian Version of the Pittsburgh Sleep Quality Index (PSQI). Neurol. Sci. 2013, 34, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Vignatelli, L.; Plazzi, G.; Barbato, A.; Ferini-Strambi, L.; Manni, R.; Pompei, F.; D’Alessandro, R.; GINSEN (Gruppo Italiano Narcolessia Studio Epidemiologico Nazionale. Italian Version of the Epworth Sleepiness Scale: External Validity. Neurol. Sci. 2003, 23, 295–300. [Google Scholar] [CrossRef]
- Navazesh, M.; Kumar, S.K.S. University of Southern California School of Dentistry Measuring Salivary Flow: Challenges and Opportunities. J. Am. Dent. Assoc. 2008, 139 (Suppl. S2), 35S–40S. [Google Scholar] [CrossRef] [PubMed]
- Sreebny, L.M. Saliva in Health and Disease: An Appraisal and Update. Int. Dent. J. 2000, 50, 140–161. [Google Scholar] [CrossRef]
- Adamo, D.; Canfora, F.; Calabria, E.; Coppola, N.; Leuci, S.; Pecoraro, G.; Cuocolo, R.; Ugga, L.; D’Aniello, L.; Aria, M.; et al. White Matter Hyperintensities in Burning Mouth Syndrome Assessed According to the Age-Related White Matter Changes Scale. Front. Aging Neurosci. 2022, 14, 923720. [Google Scholar] [CrossRef]
- Verhoeff, M.C.; Koutris, M.; de Vries, R.; Berendse, H.W.; van Dijk, K.D.; Lobbezoo, F. Salivation in Parkinson’s Disease: A Scoping Review. Gerodontology 2023, 40, 26–38. [Google Scholar] [CrossRef]
- R: The R Project for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 1 July 2023).
- Forssell, H.; Teerijoki-Oksa, T.; Puukka, P.; Estlander, A.-M. Symptom Severity in Burning Mouth Syndrome Associates with Psychological Factors. J. Oral Rehabil. 2020, 47, 713–719. [Google Scholar] [CrossRef]
- Poon, R.; Su, N.; Ching, V.; Darling, M.; Grushka, M. Reduction in Unstimulated Salivary Flow Rate in Burning Mouth Syndrome. Br. Dent. J. 2014, 217, E14. [Google Scholar] [CrossRef]
- Werfalli, S.; Drangsholt, M.; Johnsen, J.M.; Jeffrey, S.K.; Dakhil, S.; Presland, R.B.; LeResche, L. Saliva Flow Rates and Clinical Characteristics of Patients with Burning Mouth Syndrome: A Case-Control Study. Int. J. Oral Maxillofac. Surg. 2021, 50, 1187–1194. [Google Scholar] [CrossRef]
- Lopez-Jornet, P.; Felipe, C.C.; Pardo-Marin, L.; Ceron, J.J.; Pons-Fuster, E.; Tvarijonaviciute, A. Salivary Biomarkers and Their Correlation with Pain and Stress in Patients with Burning Mouth Syndrome. J. Clin. Med. 2020, 9, 929. [Google Scholar] [CrossRef]
- Fernández-Agra, M.; González-Serrano, J.; de Pedro, M.; Virto, L.; Caponio, V.C.A.; Ibáñez-Prieto, E.; Hernández, G.; López-Pintor, R.M. Salivary Biomarkers in Burning Mouth Syndrome: A Systematic Review and Meta-Analysis. Oral Dis. 2022. Advance Online Publication. [Google Scholar] [CrossRef]
- Soares, M.S.M.; Chimenos-Küstner, E.; Subirá-Pifarrè, C.; Rodríguez de Rivera-Campillo, M.E.; López-López, J. Association of Burning Mouth Syndrome with Xerostomia and Medicines. Med. Oral Patol. Oral Cir. Bucal 2005, 10, 301–308. [Google Scholar] [PubMed]
- Pajukoski, H.; Meurman, J.H.; Halonen, P.; Sulkava, R. Prevalence of Subjective Dry Mouth and Burning Mouth in Hospitalized Elderly Patients and Outpatients in Relation to Saliva, Medication, and Systemic Diseases. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2001, 92, 641–649. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, Z.; Egbuniwe, O.; Renton, T. The Detection of Small-Fiber Neuropathies in Burning Mouth Syndrome and Iatrogenic Lingual Nerve Injuries: Use of Quantitative Sensory Testing. J. Oral Facial Pain. Headache 2016, 30, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Shaik, M.R.; Shaik, N.A.; Mikdashi, J. Autoimmune Dysphagia Related to Rheumatologic Disorders: A Focused Review on Diagnosis and Treatment. Cureus 2023, 15, e41883. [Google Scholar] [CrossRef]
- Talha, B.; Swarnkar, S.A. Xerostomia. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Bakkers, M.; Faber, C.G.; Hoeijmakers, J.G.J.; Lauria, G.; Merkies, I.S.J. Small Fibers, Large Impact: Quality of Life in Small-Fiber Neuropathy. Muscle Nerve 2014, 49, 329–336. [Google Scholar] [CrossRef]
- Grushka, M.; Epstein, J.B.; Gorsky, M. Burning Mouth Syndrome and Other Oral Sensory Disorders: A Unifying Hypothesis. Pain. Res. Manag. 2003, 8, 133–135. [Google Scholar] [CrossRef]
- Tu, T.T.H.; Takenoshita, M.; Matsuoka, H.; Watanabe, T.; Suga, T.; Aota, Y.; Abiko, Y.; Toyofuku, A. Current Management Strategies for the Pain of Elderly Patients with Burning Mouth Syndrome: A Critical Review. Biopsychosoc. Med. 2019, 13, 1. [Google Scholar] [CrossRef]
- Monteserín-Matesanz, M.; Domínguez-Gordillo, A.A.; Esparza-Gómez, G.C.; Jiménez-Ortega, L.; Cerero-Lapiedra, R. Central Sensitization in Burning Mouth Syndrome: A Practical Approach Using Questionnaires. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2022, 133, 292–300. [Google Scholar] [CrossRef]
- Navazesh, M.; Brightman, V.J.; Pogoda, J.M. Relationship of Medical Status, Medications, and Salivary Flow Rates in Adults of Different Ages. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1996, 81, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Ramírez, L.; Sánchez, I.; Muñoz, M.; Martínez-Acitores, M.L.; Garrido, E.; Hernández, G.; López-Pintor, R.M. Risk Factors Associated with Xerostomia and Reduced Salivary Flow in Hypertensive Patients. Oral Dis. 2023, 29, 1299–1311. [Google Scholar] [CrossRef] [PubMed]
- Ito, K.; Izumi, N.; Funayama, S.; Nohno, K.; Katsura, K.; Kaneko, N.; Inoue, M. Characteristics of Medication-Induced Xerostomia and Effect of Treatment. PLoS ONE 2023, 18, e0280224. [Google Scholar] [CrossRef] [PubMed]
- Moster, M.; Bolliger, D. Perioperative Guidelines on Antiplatelet and Anticoagulant Agents: 2022 Update. Curr. Anesthesiol. Rep. 2022, 12, 286–296. [Google Scholar] [CrossRef]
- Shah, S.; Urtecho, M.; Firwana, M.; Nayfeh, T.; Hasan, B.; Nanaa, A.; Saadi, S.; Flynn, D.N.; Abd-Rabu, R.; Seisa, M.O.; et al. Perioperative Management of Antiplatelet Therapy: A Systematic Review and Meta-Analysis. Mayo Clin. Proc. Innov. Qual. Outcomes 2022, 6, 564–573. [Google Scholar] [CrossRef]
- Hughes, A.; Lambert, E.M. Drooling and Aspiration of Saliva. Otolaryngol. Clin. N. Am. 2022, 55, 1181–1194. [Google Scholar] [CrossRef]
- Merello, M. Sialorrhoea and Drooling in Patients with Parkinson’s Disease: Epidemiology and Management. Drugs Aging 2008, 25, 1007–1019. [Google Scholar] [CrossRef]
- Seiler, A.; Nöth, U.; Hok, P.; Reiländer, A.; Maiworm, M.; Baudrexel, S.; Meuth, S.; Rosenow, F.; Steinmetz, H.; Wagner, M.; et al. Multiparametric Quantitative MRI in Neurological Diseases. Front. Neurol. 2021, 12, 640239. [Google Scholar] [CrossRef]
- Gholami, N.; Hosseini Sabzvari, B.; Razzaghi, A.; Salah, S. Effect of Stress, Anxiety and Depression on Unstimulated Salivary Flow Rate and Xerostomia. J. Dent. Res. Dent. Clin. Dent. Prospect. 2017, 11, 247–252. [Google Scholar] [CrossRef]
- Silvestre-Rangil, J.; Silvestre, F.-J.; Puente-Sandoval, A.; Requeni-Bernal, J.; Simó-Ruiz, J.-M. Clinical-Therapeutic Management of Drooling: Review and Update. Med. Oral Patol. Oral Cir. Bucal 2011, 16, e763–e766. [Google Scholar] [CrossRef] [PubMed]
- Meningaud, J.-P.; Pitak-Arnnop, P.; Chikhani, L.; Bertrand, J.-C. Drooling of Saliva: A Review of the Etiology and Management Options. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Jafari, A.; Alaee, A.; Ghods, K. The Etiologies and Considerations of Dysgeusia: A Review of Literature. J. Oral Biosci. 2021, 63, 319–326. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Demographic Variables | B (140) | BX (253) | BS (49) | BXS (58) | p-Value |
| Frequency % | Frequency % | Frequency % | Frequency % | ||
| Gender - Male - Female | 39 (27.9) 101 (72.1) | 3 (24.9) 190 (75.1) | 18 (36.7) 31 (63.3) | 9 (15.5) 49 (84.5) | 0.082 |
| Employment - Employed - Unemployed - Retired | 30 (21.4) 71 (50.7) 39 (27.9) | 58 (22.9) 110 (43.5) 85 (33.6) | 14 (28.6) 16 (32.7) 19 (38.8) | 17 (29.3) 20 (34.5) 21 (36.2) | 0.447 |
| Family situation - Single - Married - Divorced - Widowed | 10 (7.1) 114 (81.4) 7 (5) 9 (6.4) | 17 (6.7) 188 (74.3) 9 (3.6) 39 (15.4) | 8 (16.3) 34 (69.4) 4 (8.2) 3 (6.1) | 2 (3.4) 45 (77.6) 4 (6.9) 7 (12.1) | 0.038 * |
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | p-value | |
| Age (in years) | 64 ± 12.7 | 65.4 ± 12.5 | 61.3 ± 15.4 | 64 ± 12.9 | 0.193 |
| Education (in years) | 9.33 ± 4.70 | 9.07 ± 4.51 | 9.43 ± 4.37 | 9.28 ± 4.59 | 0.929 |
| Body Mass Index | 27.4 ± 3.38 | 26.7 ± 3.53 | 26.3 ± 2.61 | 26.1 ± 4.16 | 0.059 |
| Risk factors | Frequency (%) | Frequency (%) | Frequency (%) | Frequency (%) | p-value |
| Smoker - cigarettes < 5 - cigar. 5–10 - cigar. 10–15 - cigar. >15 - Not smoker | 5 (3.6) 6 (4.3) 10 (7.1) 7 (5) 112 (80) | 12 (4.7) 11 (4.3) 16 (6.3) 25 (9.9) 189 (74.7) | 3 (6.1) 0 (0) 4 (8.2) 11 (22.4) 31 (63.3) | 1 (1.7) 3 (5.2) 10 (17.2) 6 (10.3) 38 (65.5) | 0.148 |
| Alcohol use - 1–2 units - 2–3 units - >3 units - No Alcohol | 15 (10.7) 4 (2.9) 2 (1.4) 119 (85) | 27 (10.7) 12 (4.7) 4 (1.6) 210 (83) | 6 (12.2) 1 (2) 0 (0) 42 (85.7) | 3 (5.2) 0 (0) 0 (0) 55 (94.8) | 0.755 |
| B | BX | BS | BXS | p-Value | |
| Comorbidities | Frequency (%) | Frequency (%) | Frequency (%) | Frequency (%) | |
| Total | 107 (76.4) | 219 (86.6) | 45 (91.8) | 49 (84.5) | 0.029 |
| Hypertension | 65 (46.4) | 131 (51.8) | 26 (53.1) | 27 (46.6) | 0.683 |
| Hypercholesterolemia | 56 (40) | 95 (37.5) | 20 (40.8) | 22 (37.9) | 0.949 |
| Myocardial infarction | 6 (4.3) | 10 (4) | 2 (4.1) | 2 (3.4) | 1.000 |
| Other Cardiovascular diseases | 8 (5.7) | 23 (9.1) | 5 (10.2) | 5 (8.6) | 0.604 |
| Respiratory diseases | 3 (2.1) | 12 (4.7) | 2 (4.1) | 0 (0) | 0.245 |
| Gastrointestinal diseases | 23 (16.4) | 49 (19.4) | 8 (16.3) | 10 (17.2) | 0.900 |
| Endocrine diseases | 0 (0) | 4 (1.6) | 3 (6.1) | 0 (0) | 0.025 |
| Prostatic Hypertrophy | 4 (2.9) | 17 (6.7) | 2 (4.1) | 3 (5.2) | 0.433 |
| Hypothyroidism | 14 (10) | 42 (16.6) | 7 (14.3) | 5 (8.6) | 0.207 |
| Hyperthyroidism | 3 (2.1) | 0 (0) | 1 (2) | 1 (1.7) | 0.047 |
| HCV infection | 3 (2.1) | 4 (1.6) | 2 (4.1) | 0 (0) | 0.400 |
| HBV infection | 1 (0.7) | 2 (0.8) | 0 (0) | 0 (0) | 1.000 |
| Neoplastic disease | 7 (5) | 16 (6.3) | 1 (2) | 6 (10.3) | 0.341 |
| Neurological disease | 5 (3.6) | 2 (0.8) | 1 (2) | 0 (0) | 0.146 |
| Others | 16 (11.4) | 60 (23.7) | 6 (12.2) | 14 (24.1) | 0.009 |
| Medications | Frequency (%) | Frequency (%) | Frequency (%) | Frequency (%) | p-value |
| Total Drugs intake | 85 (60.7) | 193 (76.3) | 32 (65.3) | 38 (65.5) | 0.009 |
| ACE-inhibitors | 19 (13.6) | 33 (13) | 4 (8.2) | 6 (10.3) | 0.793 |
| Calcium Channel blockers | 12 (8.6) | 25 (9.9) | 1 (2) | 7 (12.1) | 0.244 |
| Angiotensin II receptor antagonists | 23 (16.4) | 40 (15.8) | 12 (24.5) | 9 (15.5) | 0.508 |
| Thiazide Diuretics | 10 (7.1) | 41 (16.2) | 7 (14.3) | 5 (8.6) | 0.049 |
| Beta blockers | 21 (15) | 45 (17.8) | 5 (10.2) | 9 (15.5) | 0.620 |
| Statins | 36 (25.7) | 66 (26.1) | 11 (22.4) | 12 (20.7) | 0.845 |
| Ezetimibe | 0 (0) | 9 (3.6) | 1 (2) | 0 (0) | 0.057 |
| Antiplatelets | 40 (28.6) | 76 (30) | 14 (28.6) | 15 (25.9) | 0.944 |
| Blood thinners | 2 (1.4) | 22 (8.7) | 0 (0) | 1 (1.7) | 0.002 ** |
| Bisphosphonates | 4 (2.9) | 5 (2) | 1 (2) | 1 (1.7) | 0.960 |
| Levothyroxin sodium | 12 (8.6) | 33 (13) | 5 (10.2) | 8 (13.8) | 0.545 |
| Steroids | 2 (1.4) | 7 (2.8) | 0 (0) | 3 (5.2) | 0.291 |
| Proton Pump inhibitors | 29 (20.7) | 65 (25.7) | 10 (20.4) | 17 (29.3) | 0.491 |
| Others | 16 (11.4) | 39 (15.4) | 4 (8.2) | 7 (12.1) | 0.515 |
| B | BX | BS | BXS | p-Value | |
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | ||
| Disease onset (months) | 26.4 ± 47.9 | 32.6 ± 49.6 | 34.5 ± 53.2 | 20.8 ± 21.8 | 0.236 |
| Symptoms pattern | Frequency (%) | Frequency (%) | Frequency (%) | Frequency (%) | |
| Worst in the morning | 3 (2.1) | 12 (4.7) | 1 (2) | 1 (1.7) | 0.583 |
| Worst in the afternoon/evening | 55 (39.3) | 104 (41.1) | 17 (34.7) | 29 (50) | 0.412 |
| Same morning/afternoon/evening | 79 (56.4) | 134 (53) | 30 (61.2) | 28 (48.3) | 0.527 |
| Continuous | 90 (64.3) | 152 (60.1) | 32 (65.3) | 33 (56.9) | 0.690 |
| Intermittent | 49 (35) | 92 (36.4) | 16 (32.7) | 25 (43.1) | 0.677 |
| Improvement during eating | 26 (18.6) | 58 (22.9) | 15 (30.6) | 24 (41.4) | 0.006 ** |
| Topical Therapy | Frequency (%) | Frequency (%) | Frequency (%) | Frequency (%) | |
| Topical Clonazepam | 86 (61.4) | 194 (76.7) | 30 (61.2) | 37 (63.8) | 0.004 ** |
| Improvement with topical treatment | 15 (10.7) | 43 (17) | 10 (20.4) | 9 (15.5) | 0.262 |
| B | BX | BS | BXS | p-Value | |
| Oral Symptoms | Frequency (%) | Frequency (%) | Frequency (%) | Frequency (%) | |
| Burning | 140 (100) | 253 (100) | 49 (100) | 58 (100) | - |
| Dysgeusia | 45 (32.1) | 118 (46.6) | 28 (57.1) | 34 (58.6) | 0.001 ** |
| Globus | 32 (22.9) | 109 (43.1) | 19 (38.8) | 23 (39.7) | 0.001 ** |
| Itching | 16 (11.4) | 28 (11.1) | 10 (20.4) | 7 (12.1) | 0.339 |
| Intraoral foreign body sensation | 27 (19.3) | 50 (19.8) | 13 (26.5) | 16 (27.6) | 0.392 |
| Subjective Halitosis | 5 (3.6) | 17 (6.7) | 4 (8.2) | 4 (6.9) | 0.449 |
| Tingling | 10 (7.1) | 29 (11.5) | 14 (28.6) | 5 (8.6) | 0.002 ** |
| Occlusal Dysesthesia | 7 (5) | 19 (7.5) | 11 (22.4) | 4 (6.9) | 0.006 |
| Change in tongue morphology | 20 (14.3) | 58 (22.9) | 16 (32.7) | 14 (24.1) | 0.033 |
| Oral Dyskinesia | 7 (5) | 20 (7.9) | 8 (16.3) | 4 (6.9) | 0.109 |
| Dysosmia | 2 (1.4) | 12 (4.7) | 6 (12.2) | 5 (8.6) | 0.009 |
| Location of Pain/Burning | Frequency (%) | Frequency (%) | Frequency (%) | Frequency (%) | p-value |
| Generalized | 35 (25%) | 135 (53.4%) | 22 (44.9%) | 36 (62.1%) | <0.001 ** |
| Gums | 61 (43.6) | 159 (62.8) | 33 (67.3) | 42 (72.4) | <0.001 ** |
| Lips | 56 (40) | 180 (71.1) | 30 (61.2) | 45 (77.6) | <0.001 ** |
| Cheeks | 43 (30.7) | 157 (62.3) | 25 (51) | 40 (69) | <0.001 ** |
| Tongue | 119 (85) | 241 (95.3) | 43 (87.8) | 53 (91.4) | 0.004 ** |
| Floor of the mouth | 42 (30) | 140 (55.3) | 25 (51) | 35 (60.3) | <0.001 ** |
| Palate | 63 (45) | 175 (69.2) | 25 (51) | 42 (72.4) | <0.001 ** |
| Trigone | 37 (26.4) | 131 (51.8) | 19 (38.8) | 40 (69) | <0.001 ** |
| B | BX | BS | BXS | p-Value | |
|---|---|---|---|---|---|
| Median (IQR) | Median (IQR) | Median (IQR) | Median (IQR) | Median (IQR) | |
| VAS | 10 [8.75–10] | 10 [9–10] | 10 [9–10] | 10 [9.25–10] | 0.288 |
| SF-MPQ | 10.5 [7.75–12] | 10 [7–12] | 9 [7–13] | 11 [9–12] | 0.168 |
| HAM-A | 16.5 [15–20] | 18 [15–20] | 17 [15–21] | 18 [16–21] | 0.276 |
| HAM-D | 16 [14–19] | 17 [14–20] | 17 [14–20] | 16.5 [14–21.75] | 0.785 |
| PSQI | 8 [8–10] | 8 [7–10] | 8 [8–10] | 8 [8–10] | 0.968 |
| ESS | 7 [5–9] | 7 [5–9] | 8 [5–9] | 7 [5–9] | 0.337 |
| BURNING (B) | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | p-Value | OR | p-Value | OR | p-Value | OR | p-Value | OR | p-Value | OR | p-Value | ||||||
| Age | 1.01 | 0.292 | 1.01 | 0.219 | 1.01 | 0.272 | 1.01 | 0.289 | 1.01 | 0.290 | 1.01 | 0.188 | |||||
| Gender: Male | 0.89 | 0.625 | 0.99 | 0.976 | 0.87 | 0.552 | 0.89 | 0.608 | 0.88 | 0.584 | 0.95 | 0.838 | |||||
| Years of education | 0.99 | 0.719 | 0.99 | 0.715 | 1.00 | 0.888 | 0.99 | 0.734 | 0.99 | 0.813 | 1.00 | 0.924 | |||||
| Marital status: Married | 0.69 | 0.136 | 0.65 | 0.095 | 0.70 | 0.153 | 0.69 | 0.138 | 0.69 | 0.147 | 0.64 | 0.092 | |||||
| Job: Occupied | 1.19 | 0.529 | 1.25 | 0.434 | 1.20 | 0.514 | 1.19 | 0.530 | 1.24 | 0.449 | 1.30 | 0.368 | |||||
| Smoker | 1.66 | 0.043 * | 1.53 | 0.098 | 1.65 | 0.045 * | 1.64 | 0.049 * | 1.60 | 0.059 | 1.48 | 0.130 | |||||
| Alcohol | 0.89 | 0.687 | 0.86 | 0.628 | 0.88 | 0.678 | 0.90 | 0.715 | 0.94 | 0.827 | 0.91 | 0.756 | |||||
| BMI | 0.94 | 0.024 * | 0.94 | 0.027 * | 0.93 | 0.018 * | 0.93 | 0.020 * | 0.94 | 0.032 * | 0.93 | 0.021 * | |||||
| Dysgeusia | 1.87 | 0.004 ** | 1.84 | 0.006 ** | |||||||||||||
| Globus | 2.17 | 0.001 ** | 2.12 | 0.002 ** | |||||||||||||
| Tingling | 1.67 | 0.178 | 2.02 | 0.077 | |||||||||||||
| VAS | 1.17 | 0.061 | 1.17 | 0.073 | |||||||||||||
| SF-MPQ | 1.01 | 0.579 | 1.00 | 0.907 | |||||||||||||
| HAM-A | 1.02 | 0.492 | 1.03 | 0.404 | |||||||||||||
| HAM-D | 0.99 | 0.705 | 0.97 | 0.362 | |||||||||||||
| PSQI | 1.04 | 0.378 | 1.03 | 0.554 | |||||||||||||
| ESS | 0.94 | 0.096 | 0.94 | 0.109 | |||||||||||||
| R2 (%) | 2.3 | 0.086 | 6.9 | <0.001 ** | 3 | 0.059 | 2.4 | 0.157 | 2.9 | 0.076 | 8.1 | <0.001 ** | |||||
| R2 change (%) | 4.6 | <0.001 ** | 0.7 | 0.140 | 0.1 | 0.773 | 0.6 | 0.217 | 5.8 | <0.001 ** | |||||||
| BURN + XEROSTOMIA (BX) | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 | Model 7 | ||||||||||
| OR | p-value | OR | p-value | OR | p-value | OR | p-value | OR | p-value | OR | p-value | OR | p-value | ||||
| Age | 1.45 | 0.128 | 0.99 | 0.098 | 0.99 | 0.278 | 0.99 | 0.139 | 0.99 | 0.117 | 0.99 | 0.117 | 0.99 | 0.209 | |||
| Gender: Male | 1.19 | 0.414 | 1.12 | 0.614 | 1.30 | 0.230 | 1.21 | 0.367 | 1.20 | 0.384 | 1.20 | 0.405 | 1.26 | 0.296 | |||
| Years of education | 1.00 | 0.824 | 1.00 | 0.873 | 1.01 | 0.752 | 1.00 | 0.984 | 1.01 | 0.784 | 1.00 | 0.915 | 1.00 | 0.978 | |||
| Marital status: Married | 1.21 | 0.362 | 1.27 | 0.272 | 1.23 | 0.346 | 1.23 | 0.338 | 1.22 | 0.357 | 1.21 | 0.378 | 1.31 | 0.227 | |||
| Job: Occupied | 0.86 | 0.540 | 0.83 | 0.471 | 0.80 | 0.384 | 0.84 | 0.492 | 0.87 | 0.577 | 0.84 | 0.481 | 0.76 | 0.294 | |||
| Smoker | 1.03 | 0.878 | 1.10 | 0.670 | 0.99 | 0.944 | 1.05 | 0.826 | 1.03 | 0.884 | 1.07 | 0.751 | 1.09 | 0.694 | |||
| Alcohol | 0.71 | 0.204 | 0.72 | 0.212 | 0.75 | 0.301 | 0.70 | 0.187 | 0.71 | 0.197 | 0.68 | 0.153 | 0.71 | 0.226 | |||
| BMI | 1.01 | 0.733 | 1.01 | 0.736 | 1.01 | 0.714 | 1.01 | 0.702 | 1.01 | 0.627 | 1.00 | 0.851 | 1.01 | 0.702 | |||
| Disgeusia | 0.97 | 0.849 | 0.98 | 0.908 | |||||||||||||
| Globus | 0.53 | 0.002 ** | 0.54 | 0.002 ** | |||||||||||||
| Tingling | 1.18 | 0.576 | 1.11 | 0.739 | |||||||||||||
| Blood thinners | 0.13 | 0.001 ** | 0.14 | 0.002 ** | |||||||||||||
| VAS | 0.91 | 0.219 | 0.92 | 0.341 | |||||||||||||
| SF-MPQ | 1.01 | 0.416 | 1.02 | 0.223 | |||||||||||||
| HAM-A | 0.97 | 0.229 | 0.97 | 0.289 | |||||||||||||
| HAM-D | 1.04 | 0.204 | 1.04 | 0.160 | |||||||||||||
| PSQI | 0.98 | 0.605 | 0.97 | 0.533 | |||||||||||||
| ESS | 1.07 | 0.041 * | 1.07 | 0.065 | |||||||||||||
| R2 (%) | 0.9 | 0.583 | 2.5 | 0.100 | 3.2 | 0.009 ** | 1.2 | 0.567 | 1.2 | 0.595 | 1.6 | 0.373 | 5.7 | 0.003 ** | |||
| R2 change (%) | 1.6 | 0.013 * | 2.3 | <0.001 ** | 0.3 | 0.356 | 0.3 | 0.411 | 0.7 | 0.120 | 4.8 | <0.001 ** | |||||
| BURN + SIALORRHEA (BS) | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 | |||||||||||
| OR | p-value | OR | p-value | OR | p-value | OR | p-value | OR | p-value | OR | p-value | ||||||
| Age | 1.02 | 0.174 | 1.02 | 0.190 | 1.02 | 0.173 | 1.02 | 0.165 | 1.02 | 0.165 | 1.02 | 0.181 | |||||
| Gender: Male | 0.51 | 0.047 * | 0.49 | 0.036 | 0.53 | 0.056 | 0.51 | 0.042 * | 0.51 | 0.047 * | 0.51 | 0.049 * | |||||
| Years of education | 1.01 | 0.758 | 1.02 | 0.685 | 1.01 | 0.838 | 1.01 | 0.741 | 1.01 | 0.737 | 1.01 | 0.762 | |||||
| Marital status: Married | 1.42 | 0.302 | 1.40 | 0.336 | 1.41 | 0.306 | 1.41 | 0.306 | 1.42 | 0.301 | 1.39 | 0.343 | |||||
| Job: Occupied | 1.05 | 0.908 | 1.04 | 0.931 | 1.02 | 0.950 | 1.03 | 0.936 | 1.05 | 0.910 | 0.98 | 0.964 | |||||
| Smoker | 0.62 | 0.142 | 0.64 | 0.197 | 0.62 | 0.144 | 0.61 | 0.131 | 0.61 | 0.135 | 0.62 | 0.161 | |||||
| Alcohol | 1.23 | 0.654 | 1.18 | 0.717 | 1.21 | 0.678 | 1.23 | 0.647 | 1.23 | 0.646 | 1.15 | 0.761 | |||||
| BMI | 1.05 | 0.310 | 1.06 | 0.255 | 1.05 | 0.288 | 1.04 | 0.367 | 1.05 | 0.299 | 1.06 | 0.261 | |||||
| Disgeusia | 0.57 | 0.079 | 0.58 | 0.094 | |||||||||||||
| Globus | 1.25 | 0.512 | 1.22 | 0.556 | |||||||||||||
| Tingling | 0.26 | <0.001 ** | 0.24 | <0.001 ** | |||||||||||||
| VAS | 0.88 | 0.386 | 0.82 | 0.213 | |||||||||||||
| SF-MPQ | 1.00 | 0.965 | 1.01 | 0.772 | |||||||||||||
| HAM-A | 1.06 | 0.281 | 1.04 | 0.429 | |||||||||||||
| HAM-D | 0.96 | 0.421 | 0.99 | 0.827 | |||||||||||||
| PSQI | 1.00 | 0.984 | 0.99 | 0.885 | |||||||||||||
| ESS | 0.97 | 0.638 | 0.97 | 0.648 | |||||||||||||
| R2 (%) | 3.5 | 0.196 | 8.1 | 0.007 ** | 3.7 | 0.290 | 3.8 | 0.267 | 3.5 | 0.331 | 8.9 | 0.038 * | |||||
| R2 change (%) | 4.6 | 0.002 ** | 0.2 | 0.664 | 0.3 | 0.554 | 0.0 | 0.886 | 5.4 | 0.041 * | |||||||
| BURN + XERO + SIAL (BXS) | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 | |||||||||||
| OR | p-value | OR | p-value | OR | p-value | OR | p-value | OR | p-value | OR | p-value | ||||||
| Age | 0.99 | 0.562 | 0.99 | 0.598 | 0.99 | 0.502 | 0.99 | 0.615 | 0.99 | 0.583 | 0.99 | 0.600 | |||||
| Gender: Male | 1.68 | 0.183 | 1.69 | 0.181 | 1.64 | 0.205 | 1.69 | 0.178 | 1.70 | 0.175 | 1.67 | 0.196 | |||||
| Years of education | 0.99 | 0.829 | 0.99 | 0.781 | 1.00 | 0.909 | 0.99 | 0.749 | 0.99 | 0.817 | 0.99 | 0.840 | |||||
| Marital status: Married | 0.88 | 0.706 | 0.89 | 0.728 | 0.85 | 0.629 | 0.88 | 0.698 | 0.88 | 0.702 | 0.85 | 0.648 | |||||
| Job: Occupied | 0.97 | 0.928 | 0.94 | 0.868 | 1.02 | 0.954 | 0.94 | 0.876 | 0.97 | 0.928 | 0.99 | 0.987 | |||||
| Smoker | 0.61 | 0.11 | 0.59 | 0.092 | 0.58 | 0.087 | 0.64 | 0.155 | 0.60 | 0.108 | 0.58 | 0.090 | |||||
| Alcohol | 3.52 | 0.042 * | 3.48 | 0.044 * | 3.70 | 0.035 * | 3.42 | 0.047 * | 3.52 | 0.043 * | 3.65 | 0.039 * | |||||
| BMI | 1.07 | 0.096 | 1.07 | 0.120 | 1.08 | 0.079 | 1.07 | 0.101 | 1.08 | 0.090 | 1.08 | 0.103 | |||||
| Dysgeusia | 0.53 | 0.031 * | 0.56 | 0.052 | |||||||||||||
| Globus | 1.01 | 0.977 | 1.02 | 0.941 | |||||||||||||
| Tingling | 1.56 | 0.377 | 1.85 | 0.239 | |||||||||||||
| VAS | 1.00 | 0.973 | 1.05 | 0.733 | |||||||||||||
| SF-MPQ | 0.95 | 0.045 * | 0.95 | 0.049 * | |||||||||||||
| HAM-A | 0.99 | 0.862 | 1.00 | 0.927 | |||||||||||||
| HAM-D | 0.97 | 0.548 | 0.97 | 0.428 | |||||||||||||
| PSQI | 0.98 | 0.751 | 1.01 | 0.861 | |||||||||||||
| ESS | 0.97 | 0.537 | 0.96 | 0.468 | |||||||||||||
| R2 (%) | 4.0 | 0.076 | 5.5 | 0.049 * | 5.0 | 0.054 | 4.3 | 0.118 | 4.1 | 0.139 | 7.0 | 0.093 | |||||
| R2 change (%) | 1.5 | 0.136 | 1.0 | 0.148 | 0.3 | 0.554 | 0.1 | 0.740 | 3.0 | 0.282 | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Canfora, F.; Calabria, E.; Spagnuolo, G.; Coppola, N.; Armogida, N.G.; Mazzaccara, C.; Solari, D.; D’Aniello, L.; Aria, M.; Pecoraro, G.; et al. Salivary Complaints in Burning Mouth Syndrome: A Cross Sectional Study on 500 Patients. J. Clin. Med. 2023, 12, 5561. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12175561
Canfora F, Calabria E, Spagnuolo G, Coppola N, Armogida NG, Mazzaccara C, Solari D, D’Aniello L, Aria M, Pecoraro G, et al. Salivary Complaints in Burning Mouth Syndrome: A Cross Sectional Study on 500 Patients. Journal of Clinical Medicine. 2023; 12(17):5561. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12175561
Chicago/Turabian StyleCanfora, Federica, Elena Calabria, Gianrico Spagnuolo, Noemi Coppola, Niccolò Giuseppe Armogida, Cristina Mazzaccara, Domenico Solari, Luca D’Aniello, Massimo Aria, Giuseppe Pecoraro, and et al. 2023. "Salivary Complaints in Burning Mouth Syndrome: A Cross Sectional Study on 500 Patients" Journal of Clinical Medicine 12, no. 17: 5561. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12175561