
Management and Prognosis of Acute Stroke in Atrial Fibrillation
by
 , and
, and
Mette F. Hindsholm
1,2,*,
Dorte Damgaard
1,
M. Edip Gurol
3,4,
David Gaist
5 and
Claus Z. Simonsen
1,2 1
Department of Neurology, Aarhus University Hospital, 8200 Aarhus, Denmark
2
Department of Clinical Medicine, Aarhus University, 8200 Aarhus, Denmark
3
Department of Neurology, Massachusetts General Hospital, Boston, MA 02114, USA
4
Harvard Medical School, Boston, MA 02115, USA
5
Research Unit for Neurology, Odense University Hospital, University of Southern Denmark, 5000 Odense, Denmark
*
Author to whom correspondence should be addressed.
J. Clin. Med. 2023, 12(17), 5752; https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12175752
Submission received: 14 July 2023
/
Revised: 25 August 2023
/
Accepted: 1 September 2023
/
Published: 4 September 2023
(This article belongs to the Special Issue New Trends for Stroke Prevention in Atrial Fibrillation)
Abstract
:Atrial fibrillation (AF) is an important risk factor for ischemic stroke (IS). Oral anticoagulation (OAC) significantly reduces the risk of IS in AF but also increases the risk of systemic bleeding, including intracerebral hemorrhage (ICH). AF-related strokes are associated with greater disability and mortality compared to non-AF strokes. The management of patients with AF-related strokes is challenging, and it involves weighing individual risks and benefits in the acute treatment and preventive strategies of these patients. This review summarizes the current knowledge of the acute management of ischemic and hemorrhagic stroke in patients with AF, and the prognosis and potential implications for management both in the acute and long-term setting.
1. Introduction
Stroke is a severe and devastating disease affecting more than 12 million people worldwide every year [1]. One of the main risk factors for ischemic stroke (IS) is atrial fibrillation (AF). AF is the most common chronic cardiac arrhythmia, affecting 2–3% of the population in Europe and the USA [2]. AF-related IS are associated with increased mortality, poorer functional outcomes, and increased recurrence rates compared to non-AF-related IS [3].
To prevent IS in patients with AF, clinical guidelines recommend long-term oral anticoagulant (OAC) therapy in selected patients [4,5]. OAC therapy reduces the risk of IS by approximately two-thirds [6,7]. However, despite proven efficacy and good compliance, patients with AF may still suffer an IS even when treated with OAC therapy. In addition, long-term OAC treatment also confers an increased risk of hemorrhagic stroke.
In this review, we summarize the current knowledge in the field of acute stroke in patients with AF regarding stroke characteristics, acute management, and prognosis.
2. Ischemic Stroke
Stroke is a clinical diagnosis defined as the acute onset of focal neurological symptoms of presumed vascular origin. Patients with a stroke can be identified by the typical clinical presentation (sudden hemiparesis, anesthesia, anopia, and loss of function in speech and balance). The scale most often used to evaluate neurologic deficits in the acute setting is the National Institutes of Health Stroke Scale (NIHSS). The NIHSS is composed of 11 items with a score of 0 to 42 (a higher score indicating greater stroke severity) [8].
Of all strokes, 85% are ischemic and 15% are hemorrhagic (comprising spontaneous intracerebral hemorrhage (ICH) and atraumatic subarachnoid hemorrhage (SAH)). The clinical presentation is similar among patients with IS and ICH, and brain imaging is needed to distinguish between the two. Brain CT is the imaging modality most commonly used in the acute setting. Here, an ICH will be visualized as a hyperdense, parenchymatous lesion. As brain ischemia may be difficult to visualize acutely on CT; IS is often diagnosed as a combination of a typical clinical syndrome and the absence of bleeding on CT. MRI is superior to CT for providing imaging evidence of brain ischemia and is particularly useful in certain situations, e.g., wake-up stroke and atypical presentations. However, the availability of MRI (and imaging modalities other than CT) is highly setting-dependent, while CT is universally available and can be performed rapidly, including in patients where acute MRI is contraindicated (e.g., patients with pacemakers) or not possible to perform.
The etiology of an IS has implications for prognosis and long-term management. All patients suffering an IS should be evaluated with brain and neurovascular imaging, cardiac evaluation (rhythm monitoring), and relevant blood tests to establish the etiology of the stroke.
A system for classifying IS according to the underlying stroke etiology has been developed in the Trial of Org 10,172 in Acute Stroke Treatment (TOAST [9]). The TOAST criteria categorize IS into five subtypes based on diagnostic evaluation of brain imaging (CT/MRI), cardiac evaluation (ECG and echocardiography), vascular imaging of cerebral arteries, the results of blood tests, and, in some cases, additional assessments (Table 1).
Since the cause of IS affects the choice of management, categorizing the stroke etiology according to the TOAST classification is an important step in reducing future risk of stroke. One of the leading pathophysiologic causes of IS is cardioembolism (CE), often secondary to AF.
3. Acute Reperfusion Therapy in Ischemic Stroke
The primary goal in the acute management of IS, no matter the etiology of the stroke, is to minimize brain injury by reestablishing blood flow to the parts of the brain that are ischemic but not yet infarcted. This is achieved through reperfusion therapy. The benefit of reperfusion therapy is time-dependent, and the effect decreases over time. In general, the earlier the treatment is initiated, the better the outcome.
There are two main options for reperfusion therapy for acute ischemic stroke (AIS): intravenous thrombolysis (IVT) and endovascular treatment (EVT).
3.1. Intravenous Thrombolysis (IVT)
The cornerstone of reperfusion therapy for AIS is IVT with alteplase (a recombinant tissue plasminogen activator, rt-PA) [10]. Alteplase converts plasminogen to plasmin, inducing fibrinolysis of the thrombus [11]. Ten percent of the alteplase dose is administered as an intravenous bolus over one minute, and the rest is infused over one hour, often administered on a pump.
Randomized controlled trials (RCTs) have shown treatment with alteplase to improve functional outcomes at three months when administered within 4.5 h from stroke onset [12,13,14]. However, treatment with alteplase is associated with a significantly increased risk of hemorrhagic complications, including ICH. The risk of symptomatic ICH (sICH) varies in studies depending on population and definitions, but generally ranges from 2% to 7% in alteplase-treated patients [14,15]. The vast majority of sICH occurs within the first 24 h after IVT administration [16].
The sooner IVT is initiated, the greater the benefit. When administered beyond 4.5 h, harm may exceed the benefit. Hence, it is critical to treat eligible patients as quickly as possible.
Recently, the drug tenecteplase, an established treatment for acute myocardial infarction, was proven noninferior to alteplase in AIS treatment [17,18,19,20]. Tenecteplase is a modified rt-PA administered as an intravenous bolus with no need for continuous infusion. Bolus administration of tenecteplase seems more advantageous in the setting of AIS management with faster door-to-needle times. For patients with a large vessel occlusion (LVO) who need transfer for EVT at a comprehensive stroke center, work flow and transfer time are greatly improved with tenecteplase. In case of LVO, recent studies have shown treatment with tenecteplase to be associated with increased rates of successful recanalization before initiation of EVT and a better functional outcome at three months compared with patients treated with alteplase [21,22]. This has led most guidelines [23] to recognize tenecteplase 0.25 mg/kg (maximum dose of 25 mg) as an appropriate first-line treatment, preferable to alteplase, in patients eligible for IVT and EVT.
3.2. Endovascular Treatment (EVT)
One in three patients presenting with AIS has an LVO, a blockage of one of the major brain arteries. Different mechanisms may cause LVO: occlusion secondary to intracranial atherosclerosis, artery-to-artery embolization (extracranial atherosclerotic embolism resulting in intracranial occlusion), cardioembolic occlusion (e.g., due to AF), or cryptogenic causes [24].
LVO is associated with severe deficits and poor outcomes [25,26]. EVT is indicated in patients with AIS and concomitant LVO. The procedure involves physical extraction of the thrombus through a catheter. Guidelines recommend EVT in patients with LVO presenting within 24 h of stroke onset based on large RCTs [27,28,29,30,31,32,33]. Patients should, if eligible, be treated with IVT even when EVT is considered [34].
4. Ischemic Stroke in Atrial Fibrillation
Patients with AF have a five-fold-increased risk of stroke, and approximately one-third of all stroke events are attributable to AF [35,36]. An IS may occur in patients with AF either as the first manifestation of AF (2–4% of patients with AF present with an IS or a transient ischemic attack (TIA)) or despite appropriate OAC treatment. Randomized trials and observational studies report the residual risk of IS in patients treated with OAC to be between 1.4% and 8.9% per year [6,37].
AF-related IS often presents with a distinct radiologic pattern indicating embolic stroke, i.e., a typical wedge-shaped cortical-subcortical infarct [38] (Figure 1). AF-related IS can affect any vascular territory, and multiple vascular territories can be affected [39].
IS in patients with AF has no specific or characteristic clinical features. However, AF-related strokes are often more severe than non-AF-related strokes (i.e., higher NIHSS at admission), presumably due to embolization of larger thrombi [40]. Consequently, patients with AF suffering an IS have worse outcomes compared to patients with sinus rhythm and are at an increased risk of stroke recurrence. This was shown in the Copenhagen Stroke Study [41]: AF-related strokes were associated with higher mortality rates (odds ratio (OR) 1.7; 95% CI, 1.2–2.5), longer hospital stays (50 days vs. 40 days, p < 0.001), and lower discharge rates to patients’ own homes versus care facilities (OR 0.60; 95% CI, 0.44–0.85). The Framingham Study showed a similar increase in 30-day mortality in AF-related strokes (OR 1.84; 95% CI, 1.04–3.27) and an increased risk of recurrent stroke during one-year follow-up [42]. These results were exclusively explained by initially more severe strokes and larger infarcts in patients with AF.
Treatment with OAC therapy reduces the risk of IS by 60–70% [43]. OAC therapy has also been shown to reduce stroke severity (lower NIHSS at hospitalization) [44,45], lower the rates of LVO, and result in better functional outcomes at three months after an IS on OAC, compared with AF-related IS in patients not on OAC [46]. For most patients, guidelines recommend the use of direct oral anticoagulant therapy (DOACs, i.e., apixaban, rivaroxaban, edoxaban, or dabigatran) to prevent IS in patients with non-valvular AF (NVAF) rather than vitamin K antagonists (VKA, i.e., warfarin). DOACs perform similarly to warfarin in the prevention of IS, while the risk of treatment-related hemorrhagic stroke is lower when using a DOAC, resulting in decreased mortality [6,47,48,49,50].
5. Acute Treatment of Ischemic Stroke in Atrial Fibrillation
5.1. Use of Intravenous Thrombolysis in Atrial Fibrillation
The initial acute evaluation of patients with AF suffering an IS is similar to the evaluation of non-AF patients. However, the acute management of patients treated with OAC differs from the guidelines described above depending on OAC subtype (Figure 2).
Recent studies have shown that about 10% of all patients presenting with an AIS are treated with an OAC, with the majority being on a DOAC [51]. Hence, stroke neurologists are often faced with patients with AIS treated with OAC who could be candidates for acute reperfusion therapy. Treatment with OAC therapy is a relative contraindication for IVT. International guidelines recommend that patients treated with VKA and who are otherwise eligible for IVT may be treated with IVT if the INR is 1.7 or less [52,53]. This recommendation is based on register-based observational studies indicating that use of IVT in patients on VKA with an INR of 1.7 or less is not associated with an increased risk of ICH, a decrease in functional outcome, or higher mortality rates at three months [54,55].
Recommendations regarding the use of IVT in DOAC patients vary between countries based on different patient selection strategies [56]. The inconsistencies in guidelines on IVT treatment in DOAC patients are the result of current uncertainty regarding monitoring of drug effects in DOAC-treated patients.
Guidelines recommend against the use of IVT in patients with DOAC intake within 48 h (representing approximately four half-lives of the drugs). This contraindication is based on the presumption of a potential increased risk of ICH. However, data regarding the safety and outcomes of patients treated with IVT while on DOAC to support this presumption are lacking [57].
Information about time since DOAC intake is not always available in the acute setting, and selection of patients based on time since last DOAC intake may lead to the exclusion of IVT-eligible patients who could potentially benefit from this treatment. It is currently debated whether patients can be selected for IVT treatment based on laboratory test results of drug-specific coagulation assays (i.e., anti-Xa activity for Xa inhibitors, thrombin time for dabigatran, or DOAC blood concentrations). In centers with rapid access to calibrated anti-Xa activity levels, selection strategies based on predefined plasma drug-level cut-offs have been adopted [58]. However, several factors complicate the use of such selection strategies, including test availability, turn-around time (analysis time, which varies between 30 and 90 min), a lack of clear cut-off values, and test variability [59]. According to the European Stroke Organisation guideline (ESO, 2021), even with relevant specific anticoagulation tests, there is insufficient evidence to make evidence-based recommendations for this group of patients [52].
Another approach for selecting patients on DOAC for IVT is to use reversal agents. There are currently two specific reversal agents (antidotes) approved for DOACs. Only one of them, idarucizumab, is approved prior to IVT. Idarucizumab is approved for the reversal of the anticoagulant effect of dabigatran based on the RE-VERSE AD study [59,60]. Idarucizumab is a humanized monoclonal antibody fragment that binds dabigatran with a high affinity and rapidly neutralizes its anticlotting effect without procoagulant effects. It is quickly administered and, therefore, suitable for use prior to IVT without delaying treatment significantly. Observational studies have found treatment with idarucizumab prior to IVT to be safe and to have similar clinical outcomes and mortality rates as compared to routinely IVT-treated patients, despite an observed delay in door-to-needle time of 22 min in patients treated with the reversal agent [61,62]. According to guidelines, there is still a lack of evidence to make recommendations for or against the combination of idarucizumab and IVT, but several stroke experts recommend this approach [52]. To date, there are no specific reversal agents approved for apixaban, rivaroxaban, or edoxaban prior to IVT treatment.
Currently, treatment with IVT in DOAC patients is generally withheld due to concerns about treatment safety and the current limited knowledge on the subject. An observational study found that DOAC patients had a five-fold lower rate of IVT treatment than controls not treated with DOACs [46].
5.2. Use of EVT in Atrial Fibrillation
Approximately half of LVOs are CE, with the majority due to AF [65,66]. The most common sites of occlusion in EVT-eligible patients are the proximal middle cerebral artery (MCA, M1), followed by the more distal part of the MCA (M2) or the intracranial segment of the carotid artery (IC-ICA) [67]. Occlusion of the extracranial segment of the ICA also occurs with or without distal migration of thromboemboli to the IC-ICA segment or M1/M2 segments (artery-to-artery embolization). An observational study found that occlusion of IC-ICA or M1 was associated with AF, higher age, and female sex, whereas tandem occlusion (due to atherosclerosis) was associated with smoking, male sex, and lower age [68].
Treatment with OAC is not a contraindication for EVT. Similar rates of EVT have been reported in VKA, DOAC, and non-anticoagulated patients, with no significant time delay in symptom onset to groin puncture in VKA and DOAC patients compared to controls [46]. Current guidelines recommend treatment with IVT prior to EVT in eligible patients. However, a meta-analysis comparing direct EVT to IVT followed by EVT has shown similar safety and functional outcomes in the two groups [69]. Hence, DOAC patients with a concomitant LVO presenting directly to an EVT center should preferably bypass IVT evaluation and start EVT directly to minimize delay.
Only very few anticoagulated patients participated in randomized trials of EVT [32,33], and data regarding the safety and efficacy of EVT in OAC-treated patients rely mainly on observational studies. These studies have shown similar rates of recanalization in anticoagulated as in non-anticoagulated (OAC-naïve) patients, and OAC status has not been associated with ICH [70,71,72]. Current guidelines do not distinguish between VKA or DOAC prior to EVT. However, two large meta-analyses from 2020 and 2022 found VKA treatment associated with a higher risk of sICH and mortality after EVT compared to OAC-naïve patients [73,74]. This association was not found in DOAC patients. A newly published register-based study found recent use of VKA to significantly increase the risk of sICH (8.3%) after EVT if INR was higher than 1.7, compared with OAC-naïve patients [75]. DOAC treatment has also been associated with increased rates of successful reperfusion and better functional outcomes after EVT compared to VKA [76].
Some thrombi are easier to retrieve during EVT than others, and successful reperfusion is achieved in 44% to 88% of cases [77]. The reasons for the differences in reperfusion rates are multifaceted. Thrombus composition may influence the efficacy of EVT. Studies indicate that red blood cell-rich thrombi are associated with higher recanalization rates compared to fibrin-rich thrombi, which have a higher friction and therefore stronger interaction with the vessel wall [78,79]. Histopathological differences in thrombi composition have also been described as being associated with stroke etiology [66]; however, whether this is the case is highly debated.
CE-caused LVOs have been associated with higher EVT efficacy due to faster and higher rates of successful reperfusion, potentially leading to better clinical outcomes compared to large artery atherosclerotic (LAA) LVOs [66,68,80]. LAA LVOs have also been found to have higher mortality rates, probably due to the complexity of the procedure and higher rates of re-occlusion in this group of patients [81]. These findings might be related to thrombus composition and etiologic differences in the extent of atherosclerosis and vessel elongation/tortuosity, factors that may impede access to the occlusion. However, other studies did not find any differences in rates of successful reperfusion or clinical outcomes in CE LVOs compared to other etiologies [81]; some even described worse outcomes in CE LVOs [82].
6. Determining the Cause of Ischemic Stroke in OAC-Treated Patients
IS despite OAC, often referred to as “OAC failure”, comprises heterogeneous etiologies. OAC failure may be caused by non-compliance, insufficient anticoagulation (off-label low DOAC dose or subtherapeutic VKA dosage), CE stroke despite OAC (due to advanced or other cardiac disease), or other stroke mechanisms (e.g., large vessel atherosclerosis, small vessel disease, malignancy). A recent analysis of 1674 patients with IS despite OAC therapy found stroke etiology in patients on DOAC/VKA to be CE in 49%/37%, poor adherence or insufficient dose in 23%/43%, and a competing mechanism in 28%/20%, respectively [83]. The RENo study, comparing patients with AF who suffered an IS while on DOAC versus those who did not, found off-label low DOAC dose, atrial enlargement, hyperlipidemia, high CHA2DS2-VASc score, and increased AF burden to be associated with IS despite OAC treatment [84]. Hence, all patients with AF who suffer an IS while treated with OAC should have a thorough workup to determine the most likely stroke mechanism.
In 20–30% of OAC failures, a competing stroke mechanism is identified. Generally, OAC failures require life-long OAC therapy even when other etiologies, such as large or small vessel disease, are identified. However, some more rare causes of IS indicate specific antithrombotic strategies (i.e., antiphospholipid antibody syndrome, hypercoagulability (malignancy), or infective endocarditis) [58].
7. Restarting OAC after Ischemic Stroke
OAC treatment is initially withheld after admission to reduce the risk of hemorrhagic transformation (HT), a potential complication of AIS often occurring within the first few days after stroke onset [85]. Symptomatic HT has been reported in 2% to 20% of patients in RCTs [86], and it is associated with increased stroke mortality and morbidity.
Risk factors for HT include stroke severity (large infarct size), reperfusion treatment (both IVT and EVT), hypertension, hyperglycemia, prior OAC treatment, and age [87]. Due to the concern of a possible association between early initiation of anticoagulation and an increased risk of HT, OAC therapy is withheld for days to weeks after IS in AF patients. But the risk of recurrent IS is also increased within the first few days to weeks after an IS. An observational study of AF-related IS reported the risk of recurrent IS to vary between 0.5% and 1.3% per day within 14 days of admission [88]. The clinical conundrum is when to (re)start OAC to balance these risks.
In patients treated with IVT, guidelines recommend withholding anticoagulants and antiplatelet agents for at least 24 h after treatment and until repeated neuroimaging confirms no bleeding to mitigate the risk of hemorrhagic complications. Guideline recommendations regarding timing OAC after an IS have varied due to the dearth of high-quality evidence on the subject. OAC initiation has generally been guided by the size of the infarct; the more severe the stroke, the later the initiation of OAC. The 1–6–12 day rule, introduced in 2013 by the European Heart Rhythm Association of the European Society of Cardiology (EHRA-ESC) [89], has been the most prevailing strategy regarding OAC initiation after IS. The severity of the stroke is based on the NIHSS score; the higher the score, the more severe the stroke. This strategy has been adopted in various associations, including the European Stroke Organisation guideline [90], with small variations (3–4 days after mild stroke, 7 days after moderate stroke, and 14 days after major infarcts). The 2021 AHA/ASA guideline [90] recommends delaying initiation of OAC beyond 14 days in patients at high risk of HT to reduce the risk of ICH, whereas patients at low risk of HT may initiate OAC after 2 to 14 days to reduce the risk of recurrent IS. These recommendations are based on expert opinions, not RCT data.
Treatment with DOAC is recommended in preference to VKA in patients with NVAF and previous IS/TIA [90,91].
The ELAN trial, an RCT published in 2023, investigated the effect of early initiation (within 48 h after mild or moderate strokes and 6–7 days after major strokes) versus later initiation (according to current guidelines: 3–4 days after minor stroke, 6–7 after moderate stroke, and 12–14 after major stroke) of DOAC in patients with AF and IS [92]. The study used imaging-based classification of stroke severity (i.e., minor, moderate, or major), and not NIHSS score as in current guidelines and did not include patients with OAC use prior to their IS.
The study found the incidence of recurrent IS within 30 days to be 1.4% in the early-treatment group vs. 2.5% in the later-treatment group (OR 0.57; 95% CI, 0.29–1.07), while ICH occurred at the same rate in both arms (0.2%). The similar TIMING trial, published in 2022, found early initiation (within 4 days) noninferior to delayed start (within 5–10 days) of DOACs after IS, with no ICH in any of the groups [93]. The results of these studies, along with the promising results of observational studies of DOAC initiation after IS [94,95,96], indicate that early DOAC initiation is not associated with any safety concerns. The decision making regarding the timing of OAC initiation after an IS always has to be individually assessed based on risk factors, but according to the ELAN results, early treatment with DOAC should be considered for secondary prevention in AF after an IS (Figure 3).
8. Prognosis
OAC failure is associated with an increased mortality rate. An analysis based on combined data from the pivotal DOAC randomized trials (the COMBINE AF dataset [97]) found all-cause mortality particularly high in the early time period following IS (cumulative incidence of 12.4% (95% CI, 10.5–14.4%) at three months and 18.1% (95% CI, 15.7–20.4%) at one year [98]). The observed one-year post-stroke mortality rate in OAC failures was higher than the baseline mortality rate of patients treated with OAC in the individual trials.
The risk of stroke recurrence (ischemic or hemorrhagic) in AF patients suffering an IS is associated with high CHA2DS2-VASc score, high NIHSS score at admission, large infarct size, and type of anticoagulation used after index IS (i.e., higher for VKA than DOAC) [99].
Prior IS or TIA seems to be one of the strongest prognostic factors for future IS. Results from subgroup analysis from five major DOAC trials in AF (RE-LY [100], AVERROES [101], ROCKET AF [102], ARISTOTLE [103], and ENGAGE AF-TIME [104]) suggest that the risk of recurrent IS is doubled in patients with prior IS or TIA (relative risk (RR) 1.8–2.9 per 100 patient years in patients with prior IS/TIA vs. 0.7–1.4 per 100 patient years in patients with no prior IS/TIA) [98]. Hence, prior IS or TIA is a central component in stroke-risk scoring systems of AF patients and confers a strong recommendation for lifelong OAC therapy for secondary stroke prevention (a CHA2DS2-VASc score of at least two).
An analysis based on combined data from the pivotal DOAC randomized trials (the COMBINE AF dataset [97]) found the risk of recurrent IS to be particularly high in OAC-failure patients [98]. The cumulative incidence of recurrent IS in OAC failures was 7.0% (95% CI, 5.2–8.7%) at one year and 10.3% (95% CI, 7.8–2.8%) at two years. The incidence was particularly high within the first months (3.0% (95% CI, 1.9–4.0%) at 3 months). An Asian observational study reported similar rates (cumulative incidence of 5.3% in patients with OAC failure vs. 2.9% in patients without prior OAC treatment (HR 1.50 (95% CI, 1.02–2.21)) [105]. Observational studies are in line with these findings [37,106]. These results indicate that OAC-failure patients might have unknown risk factors that increase their future risk of recurrent IS.
Management of OAC failure is challenging, and there are currently limited data on how to guide treatment of this group of patients. Strategies include strict risk factor control (e.g., hypertension, diabetes mellitus, and dyslipidemia) and continuous OAC treatment. Data on the effect of switching anticoagulant type (VKA to DOAC, DOAC to VKA, or between DOACs) to reduce the future risk of recurrent IS is limited. Most observational studies have not found switching between OACs to be associated with a lower risk of recurrent IS [37,106]. One study found a treatment with DOAC after index IS to be associated with lower odds for recurrent IS compared to VKA [83]. However, there are no data from randomized trials to support the strategy of switching between OACs.
There is no proven benefit in the reduction of recurrent IS or death from adding platelet inhibitors on top of OAC therapy, but only an increased risk of bleeding complications, including ICH [83,107,108].
Whether left atrial appendage occlusion (LAAO) plus OAC treatment could be beneficial in patients with AF-related IS despite OAC treatment is currently unknown. The LAAOS III trial, where patients with AF and OAC treatment were randomized to LAAO or no LAAO during open cardiac surgery, found a 30% lower rate of stroke or systemic embolisms in the occlusion group compared to the no-occlusion group (4.8% vs. 7.0%, HR 0.67; 95% CI, 0.53–0.85) [109]. Whether these results are transferable to percutaneous LAAO is uncertain. In patients with prior IS or TIA and an absolute contraindication to OAC, LAAO may be considered according to guidelines [110].
9. Hemorrhagic Stroke
ICH is the second most common cause of stroke, accounting for approximately 10% of all strokes but 50% of stroke mortality. It is associated with a 30-day mortality rate of 40–50%, and only about 30% of ICH patients gain functional independence after 90 days [111].
The most common cause of ICH is small vessel disease due to hypertension or cerebral amyloid angiopathy (CAA), a neurodegenerative age-dependent disorder characterized by amyloid deposition in the small cortical and leptomeningeal arteries, with an increased risk of IS and ICH [112]. Other causes include hemorrhage due to sinus thrombosis, rupture of vascular malformations (i.e., arteriovenous malformations, cavernous angiomas, and cerebral aneurysms), or neoplasms [113]. The location of ICH is associated with its etiology. In spontaneous (non-traumatic) ICH, lobar hematoma location may be indicative of underlying CAA, whereas non-lobar hemorrhages (basal ganglia, thalamus, and pontine) are almost always caused by hypertensive arteriopathy (Figure 4).
Risk factors for ICH include increasing age (incidence rate of 0.1% in people below age 45 vs. 9.6% for people over age 85 [114]), hypertension (which doubles the risk of ICH [115,116]), and use of OAC.
The majority of patients suffering an ICH present with elevated blood pressure (BP) caused by pain, increased intracranial pressure (ICP), or untreated baseline hypertension. Clinically, ICH presents with similar symptoms as IS. However, some symptoms may indicate the presence of ICH rather than IS. These include progressive worsening of symptoms, severely elevated blood pressure, seizures, and signs of elevated intracranial pressure (ICP) (headache, nausea, vomiting, and decreased level of consciousness).
10. Intracerebral Hemorrhage in Atrial Fibrillation
ICH is the most feared and devastating complication in AF patients treated with OAC. Warfarin is associated with a two- to five-fold increased risk of ICH, whereas the risk is lower in DOAC therapy (relative risk reduction of about 50% compared to warfarin [117]).
11. Acute Treatment of ICH
The acute treatment of ICH consists of BP lowering, reversion of possible hypercoagulable state, possible surgery, and general stroke care. A recent RCT showed that implementation of a care bundle protocol including early intensive systolic BP (SBP) lowering (<140 mmHg), strict glucose control, antipyretic treatment, and reversal of warfarin-related anticoagulation within one hour improved functional outcomes in ICH patients [122].
11.1. Medical Treatment
Guidelines recommend lowering systolic BP to a target of 140 mmHg (130–150 mmHg) in the acute phase [123,124]. This recommendation is based on two large RCTs of BP-lowering strategies in patients with acute ICH (INTERACT2 [125] and ATACH-II [126]). A pooled analysis from these studies found that each reduction in systolic BP of 10 mmHg within the first 24 h was associated with a 10% increase in odds of a better functional outcome (down to a threshold of 120 to 130 mmHg) [127]. Lowering BP too much (i.e., below 130 mmHg) or too fast may be associated with a worse outcome [128] and increases the risk of adverse events like cerebral hypoperfusion and kidney injury. Elevated BP should be treated with drugs with short half-lives (such as labetalol or nicardipine) for better BP control and to avoid hypotension.
11.2. Surgical Treatment
The role of surgical treatment in patients with ICH has been intensively debated over the years. There is still a lack of evidence regarding which patients might benefit from surgical treatment, the appropriate surgical technique, and the optimal timing of intervention. Overall, RCTs evaluating the neurosurgical evacuation of hematomas have not shown improved functional outcomes of surgery compared with standard medical treatment [129,130]. However, some patients with signs of elevated ICP (neurologic deterioration), especially patients with fossa posterior hemorrhages, may benefit from surgical treatment, and in certain cases, guidelines recommend surgery to reduce mortality [123].
A recent study (ENRICH [131], ClinicalTrials.gov NTC02880878), results not yet published, comparing early minimally invasive surgery (MIPS) and standard medical management in primary, supratentorial ICH is the first RCT to demonstrate a positive effect on mortality and functional outcome in patients treated with early surgery. There are currently several ongoing trials investigating this correlation.
11.3. Treatment in Anticoagulated Patients
Treatment of OAC-related ICH in AF includes discontinuation of anticoagulation and immediate reversal of anticoagulation to reduce the risk of hematoma expansion. The choice of reversal strategy depends on the OAC type (Figure 5).
VKAs are recommended to be reversed with a 4-factor (factor II, VII, IX, and X) prothrombin complex concentrate (4F-PCC). Since the half-life of 4F-PCC is shorter than the half-life of VKA, it is recommended to also administer intravenous vitamin K. If not available, fresh frozen plasma (FFP) may be administered instead of 4F-PCC. This recommendation is based on the INCH trial, which showed faster INR normalization and smaller hematoma expansion with 4F-PCC compared to FFP [132]. However, despite effective reversal of warfarin in the acute setting, mortality is still high in warfarin-related ICH patients (up to 42% in-hospital mortality has been reported [133]).
There is only limited data on the efficacy of specific and unspecific approaches to reverse DOACs, and RCTs in DOAC-related ICH are lacking. Guidelines recommend the use of specific reversal agents (i.e., idarucizumab and andexanet alfa) for the reversal of DOACs if available, and PCC is recommended when not available [134].
In patients treated with dabigatran, idarucizumab should preferably be administered to reverse the anticoagulant effect. Based on the REVERSE-AD study, idarucizumab seems safe and has a fast reversal effect, according to coagulation tests [60]. However, data are lacking to evaluate the effect of idarucizumab on clinical outcomes.
Andexanet alfa has been shown to reverse the anticoagulant activity of factor Xa inhibitors [135,136]. It is approved for the reversal of rivaroxaban and apixaban in patients with uncontrolled, life-threatening bleeding. Andexanet alfa is a modified recombinant factor Xa that binds factor Xa inhibitors, reducing their anticoagulant effects [137]. It is administered as a bolus followed by a two-hour infusion. Serial plasma concentration measurement is recommended after administration to observe for potential rebound effects [110]. Most recently, a phase IV RCT, ANNEXA-I, was stopped early. It showed superior hemostatic efficacy of andexanet alfa compared to usual care in limiting expansion of ICH (results not yet published, ClinicalTrials.gov NCT03661528). Data on the safety and clinical outcomes of andexanet alfa treatment are awaited, and guidelines recommend randomizing into trials if possible [134].
12. Restarting Anticoagulation Therapy in Atrial Fibrillation after Intracerebral Hemorrhage
Optimal timing of OAC resumption after ICH in NVAF is often a clinical dilemma. The decision requires balancing future hemorrhagic and thromboembolic risks at an individual level. Guidelines recommend enrollment in ongoing randomized trials investigating optimal therapeutic management after ICH in AF patients.
The risk of IS often exceeds the risk of re-ICH in AF patients, with risk–benefit analyses favoring resumption of OAC therapy after bleeding has resolved [138]. Resumption of OAC has been associated with a lower risk of thromboembolic events, lower rates of mortality, and no increase in re-ICH risk in meta-analyses of OAC-related ICH [139,140,141]. In a large meta-analysis of AF patients, the association of OAC resumption with decreased mortality and all-cause stroke was also observed regardless of hematoma location (lobar vs. non-lobar) [142]. A 2023 Cochrane review on antithrombotic treatment after ICH in patients with AF found OAC initiation after ICH to reduce IS events but probably to increase the risk of ICH (based on three RCTs) [143].
The risk of ICH and re-ICH is increased in CAA patients [144]. This has often led clinicians to abstain from OAC treatment in AF patients with concomitant CAA to mitigate ICH risk. However, the presence of AF might confer an even higher risk of IS and mortality that outweighs the risk of re-ICH in this group of patients. The evidence and knowledge on CAA-related ICH and resumption of OAC are limited. OAC therapy may be indicated in CAA-related lobar hemorrhages depending on imaging findings (presence of hemorrhagic MRI markers on blood-sensitive sequences: cerebral microbleeds (CMBs) and degree of cortical superficial siderosis (cSS)) and in patients with well-controlled BP [110].
Individual decision-making regarding resumption of OAC treatment after ICH should include an evaluation of the following risk factors: BP control, age, ICH location, burden of small vessel disease (CMBs, leukoaraiosis, and cSS), and indication of antiplatelets. Data suggestive of individual factors favoring OAC resumption may include younger age, deep ICH location, and well-controlled hypertension [110]. The available evidence regarding risk factors in OAC resumption is scarce, highlighting the necessity of identifying sub-groups for whom resuming OAC therapy may be more beneficial or harmful in future studies.
In the absence of randomized data, the optimal time to resume OAC treatment is unknown. Timing depends on OAC indication and individual risk–benefit analyses. In general, restarting OAC in patients with NVAF seems safe within four to eight weeks after index ICH [110]. An observational study, limited by selection bias, found OAC initiation within seven to eight weeks after index ICH to optimize treatment benefit and minimize risks [145]. Treatment with DOAC therapy is preferred over VKA in ICH survivors with NVAF due to DOAC’s reduced risk of bleeding.
In OAC-related ICH, patients with especially high bleeding risks or other contraindications to OAC treatment may be considered for LAAO [123].
13. Prognosis and Risk of Recurrent ICH
Less than 50% of patients suffering an ICH are alive within one year, and only 30% within five years [146]. Increasing age, low GCS, large ICH volume, presence of intraventricular hemorrhage, and deep or infratentorial ICH are all factors associated with increased mortality.
The risk of recurrent ICH is especially high within the first 12 months. A meta-analysis investigating the long-term prognosis of ICH found the annual risk of re-ICH to vary between 1.3% and 7.4% [146].
Hypertension is consistently the primary risk factor associated with an increased risk of re-ICH and predisposes to both lobar and non-lobar bleeding [147]. Thus, aggressive management of BP is essential in the prevention of re-ICH [148,149].
The location and etiology of ICH are associated with a higher risk of re-ICH, probably due to the underlying arteriopathy [144]. The risk of recurrent bleeding is higher in lobar bleedings (suggestive of CAA), with an annual risk of 3.7% to 5.1%, compared to non-lobar bleedings (associated with hypertension), with an annual risk of 1.2% to 1.8% [150,151].
The presence of CMBs, a radiologic biomarker of small vessel disease in the brain visible on MRI blood-sensitive sequences (SWI or T2*) as small, black dots (accumulation of blood products), has also been related to the risk of re-ICH. CMBs are more often present in patients with re-ICH compared to patients with first-ever ICH (83% vs. 52% [152]), and their presence may predict an increased risk of ICH [144]. The location of CMBs may indicate the underlying arteriopathy: deep CMBs are related to hypertensive arteriopathy, whereas strictly lobar CMBs are more likely associated with CAA [153] (Figure 6). As the risk of re-ICH is significantly higher in lobar CAA-related ICH, lobar CMBs indicative of CAA may be a stronger ICH predictor than deep (hypertensive) CMBs [153].
The presence of cSS, the deposition of iron on the brain surface with characteristic curvilinear low signal on MRI (SWI and T2* sequences) along the cerebral convexities due to prior bleeding, is an MRI biomarker of CAA [154] (Figure 6). The presence of cSS has been shown to increase the risk of recurrent ICH [155]. It may be the most potent independent marker of increased risk for CAA-related ICH, especially if disseminated (involving more than three sulci) [110,156]. A cohort study evaluating patients with CAA-related ICH reported increased re-ICH rates with increasing degree of cSS [157].
14. Conclusions
Stroke in atrial fibrillation is a common and severe condition. OAC therapy reduces the risk of IS, but in spite of relevant OAC treatment, patients with AF may still suffer an IS. OAC patients are also at an increased risk of ICH, a condition more severe than ICH off OAC. Both acute and long-term treatment of patients with AF and IS or ICH represents a common clinical challenge.
Future studies including robust clinical trials regarding the use and safety of IVT in DOAC patients, reversal strategies of DOAC in the acute setting of stroke (ischemic and hemorrhagic), optimal timing of OAC after IS and ICH, identification of high-risk stroke patients, and optimal treatment of OAC failures are needed.
Author Contributions
Conceptualization and original draft preparation, M.F.H. and C.Z.S.; review and editing, D.G., M.E.G. and D.D. All authors have read and agreed to the published version of the manuscript.
Funding
This Work is supported by a grant from C. B. Holding Århus ApS/Claus Brændstrup and wife.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
Simonsen reports a research grant from the Novo Nordisk Foundation and Health Research Foundation of Central Denmark Region outside the submitted work. Gaist reports receiving a speaker honorarium from Bristol-Myers Squibb and Pfizer outside the submitted work.
Abbreviations
| AF | Atrial fibrillation |
| AIS | Acute ischemic stroke |
| BP | Blood pressure |
| CAA | Cerebral amyloid angiopathy |
| CE | Cardioembolism |
| CMB | Cerebral microbleed |
| cSS | Cortical superficial siderosis |
| DOAC | Direct oral anticoagulants |
| EVT | Endovascular treatment |
| HT | Hemorrhagic transformation |
| ICH | Intracerebral hemorrhage |
| IS | Ischemic stroke |
| IVT | Intravenous thrombolysis |
| LAAO | Left atrial appendage occlusion |
| LVO | Large vessel occlusion |
| NIHSS | National Institutes of Health Stroke Scale |
| NVAF | Non-valvular atrial fibrillation |
| OAC | Oral anticoagulation |
| rt-PA | Recombinant tissue plasminogen activator |
| SAH | Subarachnoid hemorrhage |
| sICH | Symptomatic intracerebral hemorrhage |
| TIA | Transient ischemic attack |
| VKA | Vitamin K agonist |
References
- World Stroke Organization (WSO). Global Stroke Fact Sheet 2022.pdf. Available online: https://www.dropbox.com/s/wm12nosylzkk5ea/World%20Stroke%20Organization%20%28WSO%29-%20Global%20Stroke%20Fact%20Sheet%202022.pdf?dl=0 (accessed on 18 April 2023).
- Kirchhof, P. The Future of Atrial Fibrillation Management: Integrated Care and Stratified Therapy. Lancet 2017, 390, 1873–1887. [Google Scholar] [CrossRef] [PubMed]
- Freedman, B.; Potpara, T.S.; Lip, G.Y.H. Stroke Prevention in Atrial Fibrillation. Lancet 2016, 388, 806–817. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the Diagnosis and Management of Atrial Fibrillation Developed in Collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the Diagnosis and Management of Atrial Fibrillation of the European Society of Cardiology (ESC) Developed with the Special Contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- January, C.T.; Wann, L.S.; Calkins, H.; Chen, L.Y.; Cigarroa, J.E.; Cleveland, J.C.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; Furie, K.L.; et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in Collaboration With the Society of Thoracic Surgeons. Circulation 2019, 140, e125–e151. [Google Scholar] [CrossRef] [PubMed]
- Ruff, C.T.; Giugliano, R.P.; Braunwald, E.; Hoffman, E.B.; Deenadayalu, N.; Ezekowitz, M.D.; Camm, A.J.; Weitz, J.I.; Lewis, B.S.; Parkhomenko, A.; et al. Comparison of the Efficacy and Safety of New Oral Anticoagulants with Warfarin in Patients with Atrial Fibrillation: A Meta-Analysis of Randomised Trials. Lancet 2014, 383, 955–962. [Google Scholar] [CrossRef] [PubMed]
- Hart, R.G.; Pearce, L.A.; Aguilar, M.I. Meta-Analysis: Antithrombotic Therapy to Prevent Stroke in Patients Who Have Nonvalvular Atrial Fibrillation. Ann. Intern. Med. 2007, 146, 857–867. [Google Scholar] [CrossRef] [PubMed]
- NIH Stroke Scale. Available online: https://www.ninds.nih.gov/health-information/public-education/know-stroke/health-professionals/nih-stroke-scale (accessed on 21 June 2023).
- Adams, H.P.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E. Classification of Subtype of Acute Ischemic Stroke. Definitions for Use in a Multicenter Clinical Trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef]
- Stemer, A.; Lyden, P. Evolution of the Thrombolytic Treatment Window for Acute Ischemic Stroke. Curr. Neurol. Neurosci. Rep. 2010, 10, 29–33. [Google Scholar] [CrossRef]
- Alteplase. In Essential Neuropharmacology: The Prescriber’s Guide; Marmura, M.J., Silberstein, S.D., Eds.; Cambridge University Press: Cambridge, UK, 2010; pp. 8–10. ISBN 978-1-139-66952-8. [Google Scholar]
- Tissue Plasminogen Activator for Acute Ischemic Stroke. N. Engl. J. Med. 1995, 333, 1581–1588. [CrossRef]
- Hacke, W.; Kaste, M.; Bluhmki, E.; Brozman, M.; Dávalos, A.; Guidetti, D.; Larrue, V.; Lees, K.R.; Medeghri, Z.; Machnig, T.; et al. Thrombolysis with Alteplase 3 to 4.5 Hours after Acute Ischemic Stroke. N. Engl. J. Med. 2008, 359, 1317–1329. [Google Scholar] [CrossRef]
- Emberson, J.; Lees, K.R.; Lyden, P.; Blackwell, L.; Albers, G.; Bluhmki, E.; Brott, T.; Cohen, G.; Davis, S.; Donnan, G.; et al. Effect of Treatment Delay, Age, and Stroke Severity on the Effects of Intravenous Thrombolysis with Alteplase for Acute Ischaemic Stroke: A Meta-Analysis of Individual Patient Data from Randomised Trials. Lancet 2014, 384, 1929–1935. [Google Scholar] [CrossRef] [PubMed]
- Yaghi, S.; Willey, J.Z.; Cucchiara, B.; Goldstein, J.N.; Gonzales, N.R.; Khatri, P.; Kim, L.J.; Mayer, S.A.; Sheth, K.N.; Schwamm, L.H. Treatment and Outcome of Hemorrhagic Transformation After Intravenous Alteplase in Acute Ischemic Stroke: A Scientific Statement for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2017, 48, e343–e361. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.; Cao, Y.; Yan, J.; Zhang, Z.; Ye, Z.; Huang, X.; Cheng, Z.; Han, Z. Risk Factors for Early Intracerebral Hemorrhage after Intravenous Thrombolysis with Alteplase. J. Atheroscler. Thromb. 2020, 27, 1176–1182. [Google Scholar] [CrossRef] [PubMed]
- Tsivgoulis, G.; Katsanos, A.H.; Christogiannis, C.; Faouzi, B.; Mavridis, D.; Dixit, A.K.; Palaiodimou, L.; Khurana, D.; Petruzzellis, M.; Psychogios, K.; et al. Intravenous Thrombolysis with Tenecteplase for the Treatment of Acute Ischemic Stroke. Ann. Neurol. 2022, 92, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Menon, B.K.; Buck, B.H.; Singh, N.; Deschaintre, Y.; Almekhlafi, M.A.; Coutts, S.B.; Thirunavukkarasu, S.; Khosravani, H.; Appireddy, R.; Moreau, F.; et al. Intravenous Tenecteplase Compared with Alteplase for Acute Ischaemic Stroke in Canada (AcT): A Pragmatic, Multicentre, Open-Label, Registry-Linked, Randomised, Controlled, Non-Inferiority Trial. Lancet 2022, 400, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Bivard, A.; Zhao, H.; Churilov, L.; Campbell, B.C.V.; Coote, S.; Yassi, N.; Yan, B.; Valente, M.; Sharobeam, A.; Balabanski, A.H.; et al. Comparison of Tenecteplase with Alteplase for the Early Treatment of Ischaemic Stroke in the Melbourne Mobile Stroke Unit (TASTE-A): A Phase 2, Randomised, Open-Label Trial. Lancet Neurol. 2022, 21, 520–527. [Google Scholar] [CrossRef]
- Burgos, A.M.; Saver, J.L. Evidence That Tenecteplase Is Noninferior to Alteplase for Acute Ischemic Stroke. Stroke 2019, 50, 2156–2162. [Google Scholar] [CrossRef] [PubMed]
- Campbell, B.C.V.; Mitchell, P.J.; Churilov, L.; Yassi, N.; Kleinig, T.J.; Dowling, R.J.; Yan, B.; Bush, S.J.; Dewey, H.M.; Thijs, V.; et al. Tenecteplase versus Alteplase before Thrombectomy for Ischemic Stroke. N. Engl. J. Med. 2018, 378, 1573–1582. [Google Scholar] [CrossRef]
- Katsanos, A.H.; Safouris, A.; Sarraj, A.; Magoufis, G.; Leker, R.R.; Khatri, P.; Cordonnier, C.; Leys, D.; Shoamanesh, A.; Ahmed, N.; et al. Intravenous Thrombolysis With Tenecteplase in Patients With Large Vessel Occlusions: Systematic Review and Meta-Analysis. Stroke 2021, 52, 308–312. [Google Scholar] [CrossRef]
- Alamowitch, S.; Turc, G.; Palaiodimou, L.; Bivard, A.; Cameron, A.; De Marchis, G.M.; Fromm, A.; Kõrv, J.; Roaldsen, M.B.; Katsanos, A.H.; et al. European Stroke Organisation (ESO) Expedited Recommendation on Tenecteplase for Acute Ischaemic Stroke. Eur. Stroke J. 2023, 8, 8–54. [Google Scholar] [CrossRef]
- Rennert, R.C.; Wali, A.R.; Steinberg, J.A.; Santiago-Dieppa, D.R.; Olson, S.E.; Pannell, J.S.; Khalessi, A.A. Epidemiology, Natural History, and Clinical Presentation of Large Vessel Ischemic Stroke. Neurosurgery 2019, 85, S4–S8. [Google Scholar] [CrossRef] [PubMed]
- Cougo-Pinto, P.T.; Chandra, R.V.; Simonsen, C.Z.; Hirsch, J.A.; Leslie-Mazwi, T. Intra-Arterial Therapy for Acute Ischemic Stroke: A Golden Age. Curr. Treat Options Neurol. 2015, 17, 30. [Google Scholar] [CrossRef] [PubMed]
- Lakomkin, N.; Dhamoon, M.; Carroll, K.; Singh, I.P.; Tuhrim, S.; Lee, J.; Fifi, J.T.; Mocco, J. Prevalence of Large Vessel Occlusion in Patients Presenting with Acute Ischemic Stroke: A 10-Year Systematic Review of the Literature. J. NeuroIntervent. Surg. 2019, 11, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Berkhemer, O.A.; Fransen, P.S.S.; Beumer, D.; van den Berg, L.A.; Lingsma, H.F.; Yoo, A.J.; Schonewille, W.J.; Vos, J.A.; Nederkoorn, P.J.; Wermer, M.J.H.; et al. A Randomized Trial of Intraarterial Treatment for Acute Ischemic Stroke. N. Engl. J. Med. 2015, 372, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Goyal, M.; Demchuk, A.M.; Menon, B.K.; Eesa, M.; Rempel, J.L.; Thornton, J.; Roy, D.; Jovin, T.G.; Willinsky, R.A.; Sapkota, B.L.; et al. Randomized Assessment of Rapid Endovascular Treatment of Ischemic Stroke. N. Engl. J. Med. 2015, 372, 1019–1030. [Google Scholar] [CrossRef] [PubMed]
- Saver, J.L.; Goyal, M.; Bonafe, A.; Diener, H.-C.; Levy, E.I.; Pereira, V.M.; Albers, G.W.; Cognard, C.; Cohen, D.J.; Hacke, W.; et al. Stent-Retriever Thrombectomy after Intravenous t-PA vs. t-PA Alone in Stroke. N. Engl. J. Med. 2015, 372, 2285–2295. [Google Scholar] [CrossRef]
- Campbell, B.C.V.; Mitchell, P.J.; Kleinig, T.J.; Dewey, H.M.; Churilov, L.; Yassi, N.; Yan, B.; Dowling, R.J.; Parsons, M.W.; Oxley, T.J.; et al. Endovascular Therapy for Ischemic Stroke with Perfusion-Imaging Selection. N. Engl. J. Med. 2015, 372, 1009–1018. [Google Scholar] [CrossRef]
- Jovin, T.G.; Chamorro, A.; Cobo, E.; de Miquel, M.A.; Molina, C.A.; Rovira, A.; San Román, L.; Serena, J.; Abilleira, S.; Ribó, M.; et al. Thrombectomy within 8 Hours after Symptom Onset in Ischemic Stroke. N. Engl. J. Med. 2015, 372, 2296–2306. [Google Scholar] [CrossRef]
- Nogueira, R.G.; Jadhav, A.P.; Haussen, D.C.; Bonafe, A.; Budzik, R.F.; Bhuva, P.; Yavagal, D.R.; Ribo, M.; Cognard, C.; Hanel, R.A.; et al. Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct. N. Engl. J. Med. 2018, 378, 11–21. [Google Scholar] [CrossRef]
- Albers, G.W.; Marks, M.P.; Kemp, S.; Christensen, S.; Tsai, J.P.; Ortega-Gutierrez, S.; McTaggart, R.A.; Torbey, M.T.; Kim-Tenser, M.; Leslie-Mazwi, T.; et al. Thrombectomy for Stroke at 6 to 16 Hours with Selection by Perfusion Imaging. N. Engl. J. Med. 2018, 378, 708–718. [Google Scholar] [CrossRef]
- Turc, G.; Bhogal, P.; Fischer, U.; Khatri, P.; Lobotesis, K.; Mazighi, M.; Schellinger, P.D.; Toni, D.; de Vries, J.; White, P.; et al. European Stroke Organisation (ESO)—European Society for Minimally Invasive Neurological Therapy (ESMINT) Guidelines on Mechanical Thrombectomy in Acute Ischaemic StrokeEndorsed by Stroke Alliance for Europe (SAFE). Eur. Stroke J. 2019, 4, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics—2020 Update: A Report From the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef] [PubMed]
- García Rodríguez, L.A.; Cea Soriano, L.; Munk Hald, S.; Hallas, J.; Balabanova, Y.; Brobert, G.; Vora, P.; Sharma, M.; Gaist, D. Discontinuation of Oral Anticoagulation in Atrial Fibrillation and Risk of Ischaemic Stroke. Heart 2020, 107, 542–548. [Google Scholar] [CrossRef] [PubMed]
- Seiffge, D.J.; De Marchis, G.M.; Koga, M.; Paciaroni, M.; Wilson, D.; Cappellari, M.; Macha, M.D.K.; Tsivgoulis, G.; Ambler, G.; Arihiro, S.; et al. Ischemic Stroke despite Oral Anticoagulant Therapy in Patients with Atrial Fibrillation. Ann. Neurol. 2020, 87, 677–687. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.-W.; Chalela, J.A.; Ezzeddine, M.A.; Warach, S. Association of Ischemic Lesion Patterns on Early Diffusion-Weighted Imaging With TOAST Stroke Subtypes. Arch. Neurol. 2003, 60, 1730–1734. [Google Scholar] [CrossRef] [PubMed]
- Wessels, T.; Wessels, C.; Ellsiepen, A.; Reuter, I.; Trittmacher, S.; Stolz, E.; Jauss, M. Contribution of Diffusion-Weighted Imaging in Determination of Stroke Etiology. AJNR Am. J. Neuroradiol. 2006, 27, 35–39. [Google Scholar] [PubMed]
- Kimura, K.; Minematsu, K.; Yamaguchi, T. Atrial Fibrillation as a Predictive Factor for Severe Stroke and Early Death in 15,831 Patients with Acute Ischaemic Stroke. J. Neurol. Neurosurg. Psychiatry 2005, 76, 679–683. [Google Scholar] [CrossRef]
- Jørgensen, H.S.; Nakayama, H.; Reith, J.; Raaschou, H.O.; Olsen, T.S. Acute Stroke with Atrial Fibrillation. The Copenhagen Stroke Study. Stroke 1996, 27, 1765–1769. [Google Scholar] [CrossRef]
- Lin, H.J.; Wolf, P.A.; Kelly-Hayes, M.; Beiser, A.S.; Kase, C.S.; Benjamin, E.J.; D’Agostino, R.B. Stroke Severity in Atrial Fibrillation. The Framingham Study. Stroke 1996, 27, 1760–1764. [Google Scholar] [CrossRef]
- Paciaroni, M.; Caso, V.; Agnelli, G.; Mosconi, M.G.; Giustozzi, M.; Seiffge, D.J.; Engelter, S.T.; Lyrer, P.; Polymeris, A.A.; Kriemler, L.; et al. Recurrent Ischemic Stroke and Bleeding in Patients With Atrial Fibrillation Who Suffered an Acute Stroke While on Treatment With Nonvitamin K Antagonist Oral Anticoagulants: The RENO-EXTEND Study. Stroke 2022, 53, 2620–2627. [Google Scholar] [CrossRef]
- Macha, K.; Marsch, A.; Siedler, G.; Breuer, L.; Strasser, E.F.; Engelhorn, T.; Schwab, S.; Kallmünzer, B. Cerebral Ischemia in Patients on Direct Oral Anticoagulants. Stroke 2019, 50, 873–879. [Google Scholar] [CrossRef] [PubMed]
- Xian, Y.; O’Brien, E.C.; Liang, L.; Xu, H.; Schwamm, L.H.; Fonarow, G.C.; Bhatt, D.L.; Smith, E.E.; Olson, D.M.; Maisch, L.; et al. Association of Preceding Antithrombotic Treatment With Acute Ischemic Stroke Severity and In-Hospital Outcomes Among Patients With Atrial Fibrillation. JAMA 2017, 317, 1057–1067. [Google Scholar] [CrossRef] [PubMed]
- Meinel, T.R.; Branca, M.; De Marchis, G.M.; Nedeltchev, K.; Kahles, T.; Bonati, L.; Arnold, M.; Heldner, M.R.; Jung, S.; Carrera, E.; et al. Prior Anticoagulation in Patients with Ischemic Stroke and Atrial Fibrillation. Ann. Neurol. 2021, 89, 42–53. [Google Scholar] [CrossRef] [PubMed]
- Giugliano, R.P.; Ruff, C.T.; Braunwald, E.; Murphy, S.A.; Wiviott, S.D.; Halperin, J.L.; Waldo, A.L.; Ezekowitz, M.D.; Weitz, J.I.; Špinar, J.; et al. Edoxaban versus Warfarin in Patients with Atrial Fibrillation. N. Engl. J. Med. 2013, 369, 2093–2104. [Google Scholar] [CrossRef] [PubMed]
- Connolly, S.J.; Ezekowitz, M.D.; Yusuf, S.; Eikelboom, J.; Oldgren, J.; Parekh, A.; Pogue, J.; Reilly, P.A.; Themeles, E.; Varrone, J.; et al. Dabigatran versus Warfarin in Patients with Atrial Fibrillation. N. Engl. J. Med. 2009, 361, 1139–1151. [Google Scholar] [CrossRef] [PubMed]
- Granger, C.B.; Alexander, J.H.; McMurray, J.J.V.; Lopes, R.D.; Hylek, E.M.; Hanna, M.; Al-Khalidi, H.R.; Ansell, J.; Atar, D.; Avezum, A.; et al. Apixaban versus Warfarin in Patients with Atrial Fibrillation. N. Engl. J. Med. 2011, 365, 981–992. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.R.; Mahaffey, K.W.; Garg, J.; Pan, G.; Singer, D.E.; Hacke, W.; Breithardt, G.; Halperin, J.L.; Hankey, G.J.; Piccini, J.P.; et al. Rivaroxaban versus Warfarin in Nonvalvular Atrial Fibrillation. N. Engl. J. Med. 2011, 365, 883–891. [Google Scholar] [CrossRef]
- Auer, E.; Frey, S.; Kaesmacher, J.; Hakim, A.; Seiffge, D.J.; Goeldlin, M.; Arnold, M.; Fischer, U.; Jung, S.; Meinel, T.R. Stroke Severity in Patients with Preceding Direct Oral Anticoagulant Therapy as Compared to Vitamin K Antagonists. J. Neurol. 2019, 266, 2263–2272. [Google Scholar] [CrossRef]
- Berge, E.; Whiteley, W.; Audebert, H.; De Marchis, G.M.; Fonseca, A.C.; Padiglioni, C.; de la Ossa, N.P.; Strbian, D.; Tsivgoulis, G.; Turc, G. European Stroke Organisation (ESO) Guidelines on Intravenous Thrombolysis for Acute Ischaemic Stroke. Eur. Stroke J. 2021, 6, I–LXII. [Google Scholar] [CrossRef]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. 2018 Guidelines for the Early Management of Patients With Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2018, 49, e46–e99. [Google Scholar] [CrossRef]
- Mazya, M.; Egido, J.A.; Ford, G.A.; Lees, K.R.; Mikulik, R.; Toni, D.; Wahlgren, N.; Ahmed, N. Predicting the Risk of Symptomatic Intracerebral Hemorrhage in Ischemic Stroke Treated With Intravenous Alteplase. Stroke 2012, 43, 1524–1531. [Google Scholar] [CrossRef]
- Xian, Y.; Liang, L.; Smith, E.E.; Schwamm, L.H.; Reeves, M.J.; Olson, D.M.; Hernandez, A.F.; Fonarow, G.C.; Peterson, E.D. Risks of Intracranial Hemorrhage Among Patients With Acute Ischemic Stroke Receiving Warfarin and Treated With Intravenous Tissue Plasminogen Activator. JAMA 2012, 307, 2600–2608. [Google Scholar] [CrossRef] [PubMed]
- Sedghi, A.; Heubner, L.; Klimova, A.; Tiebel, O.; Pietsch, J.; Mirus, M.; Barlinn, K.; Minx, T.; Beyer-Westendorf, J.; Puetz, V.; et al. Point-of-Care Assessment of Direct Oral Anticoagulation in Acute Ischemic Stroke: Protocol for a Prospective Observational Diagnostic Accuracy Study. Thromb. Haemost. 2022, 122, 1954–1962. [Google Scholar] [CrossRef] [PubMed]
- Meinel, T.R.; Wilson, D.; Gensicke, H.; Scheitz, J.F.; Ringleb, P.; Goganau, I.; Kaesmacher, J.; Bae, H.-J.; Kim, D.Y.; Kermer, P.; et al. Intravenous Thrombolysis in Patients With Ischemic Stroke and Recent Ingestion of Direct Oral Anticoagulants. JAMA Neurol. 2023, 80, 233–243. [Google Scholar] [CrossRef] [PubMed]
- Stretz, C.; Wu, T.Y.; Wilson, D.; Seiffge, D.J.; Smith, E.E.; Gurol, M.E.; Yaghi, S. Ischaemic Stroke in Anticoagulated Patients with Atrial Fibrillation. J. Neurol. Neurosurg. Psychiatry 2021, 92, 1164–1172. [Google Scholar] [CrossRef]
- Seiffge, D.J.; Meinel, T.; Purrucker, J.C.; Kaesmacher, J.; Fischer, U.; Wilson, D.; Wu, T.Y. Recanalisation Therapies for Acute Ischaemic Stroke in Patients on Direct Oral Anticoagulants. J. Neurol. Neurosurg. Psychiatry 2021, 92, 534–541. [Google Scholar] [CrossRef] [PubMed]
- Pollack, C.V.; Reilly, P.A.; van Ryn, J.; Eikelboom, J.W.; Glund, S.; Bernstein, R.A.; Dubiel, R.; Huisman, M.V.; Hylek, E.M.; Kam, C.-W.; et al. Idarucizumab for Dabigatran Reversal—Full Cohort Analysis. N. Engl. J. Med. 2017, 377, 431–441. [Google Scholar] [CrossRef]
- Barber, P.A.; Wu, T.Y.; Ranta, A. Stroke Reperfusion Therapy Following Dabigatran Reversal with Idarucizumab in a National Cohort. Neurology 2020, 94, e1968–e1972. [Google Scholar] [CrossRef]
- Kermer, P.; Eschenfelder, C.C.; Diener, H.-C.; Grond, M.; Abdalla, Y.; Abraham, A.; Althaus, K.; Becks, G.; Berrouschot, J.; Berthel, J.; et al. Antagonizing Dabigatran by Idarucizumab in Cases of Ischemic Stroke or Intracranial Hemorrhage in Germany-Updated Series of 120 Cases. Int. J. Stroke 2020, 15, 609–618. [Google Scholar] [CrossRef]
- Shahjouei, S.; Tsivgoulis, G.; Goyal, N.; Sadighi, A.; Mowla, A.; Wang, M.; Seiffge, D.J.; Zand, R. Safety of Intravenous Thrombolysis Among Patients Taking Direct Oral Anticoagulants. Stroke 2020, 51, 533–541. [Google Scholar] [CrossRef]
- Kam, W.; Holmes, D.N.; Hernandez, A.F.; Saver, J.L.; Fonarow, G.C.; Smith, E.E.; Bhatt, D.L.; Schwamm, L.H.; Reeves, M.J.; Matsouaka, R.A.; et al. Association of Recent Use of Non–Vitamin K Antagonist Oral Anticoagulants With Intracranial Hemorrhage Among Patients With Acute Ischemic Stroke Treated With Alteplase. JAMA 2022, 327, 760–771. [Google Scholar] [CrossRef]
- Binning, M.J.; Bartolini, B.; Baxter, B.; Budzik, R.; English, J.; Gupta, R.; Hedayat, H.; Krajina, A.; Liebeskind, D.; Nogueira, R.G.; et al. Trevo 2000: Results of a Large Real-World Registry for Stent Retriever for Acute Ischemic Stroke. J. Am. Heart Assoc. 2018, 7, e010867. [Google Scholar] [CrossRef] [PubMed]
- Tiedt, S.; Herzberg, M.; Küpper, C.; Feil, K.; Kellert, L.; Dorn, F.; Liebig, T.; Alegiani, A.; Dichgans, M.; Wollenweber, F.A.; et al. Stroke Etiology Modifies the Effect of Endovascular Treatment in Acute Stroke. Stroke 2020, 51, 1014–1016. [Google Scholar] [CrossRef]
- Bernsen, M.L.E.; Goldhoorn, R.-J.B.; Lingsma, H.F.; van Oostenbrugge, R.J.; van Zwam, W.H.; Uyttenboogaart, M.; Roos, Y.B.W.E.M.; Martens, J.M.; Hofmeijer, J.; Dippel, D.W.J.; et al. Importance of Occlusion Site for Thrombectomy Technique in Stroke. Stroke 2021, 52, 80–90. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, M.M.; Leslie-Mazwi, T.M.; Jensen, J.; Valentin, J.B.; Simonsen, C.Z. Endovascular Therapy of Tandem Occlusions: Baseline Characteristics and Outcomes Compared With Intracranial Occlusion. Stroke Vasc. Interv. Neurol. 2023, 3, e000466. [Google Scholar] [CrossRef]
- Podlasek, A.; Dhillon, P.S.; Butt, W.; Grunwald, I.Q.; England, T.J. Direct Mechanical Thrombectomy without Intravenous Thrombolysis versus Bridging Therapy for Acute Ischemic Stroke: A Meta-Analysis of Randomized Controlled Trials. Int. J. Stroke 2021, 16, 621–631. [Google Scholar] [CrossRef] [PubMed]
- Küpper, C.; Feil, K.; Wollenweber, F.A.; Tiedt, S.; Herzberg, M.; Dorn, F.; Liebig, T.; Dieterich, M.; Kellert, L. Endovascular Stroke Treatment in Orally Anticoagulated Patients: An Analysis from the German Stroke Registry-Endovascular Treatment. J. Neurol. 2021, 268, 1762–1769. [Google Scholar] [CrossRef] [PubMed]
- Kurowski, D.; Jonczak, K.; Shah, Q.; Yaghi, S.; Marshall, R.S.; Ahmad, H.; McKinney, J.; Torres, J.; Ishida, K.; Cucchiara, B. Safety of Endovascular Intervention for Stroke on Therapeutic Anticoagulation: Multicenter Cohort Study and Meta-Analysis. J. Stroke Cerebrovasc. Dis. 2017, 26, 1104–1109. [Google Scholar] [CrossRef]
- Goldhoorn, R.-J.B.; van de Graaf, R.A.; van Rees, J.M.; Lingsma, H.F.; Dippel, D.W.J.; Hinsenveld, W.H.; Postma, A.; van den Wijngaard, I.; van Zwam, W.H.; van Oostenbrugge, R.J.; et al. Endovascular Treatment for Acute Ischemic Stroke in Patients on Oral Anticoagulants: Results From the MR CLEAN Registry. Stroke 2020, 51, 1781–1789. [Google Scholar] [CrossRef]
- Meinel, T.R.; Kniepert, J.U.; Seiffge, D.J.; Gralla, J.; Jung, S.; Auer, E.; Frey, S.; Goeldlin, M.; Mordasini, P.; Mosimann, P.J.; et al. Endovascular Stroke Treatment and Risk of Intracranial Hemorrhage in Anticoagulated Patients. Stroke 2020, 51, 892–898. [Google Scholar] [CrossRef]
- Chen, J.-H.; Hong, C.-T.; Chung, C.-C.; Kuan, Y.-C.; Chan, L. Safety and Efficacy of Endovascular Thrombectomy in Acute Ischemic Stroke Treated with Anticoagulants: A Systematic Review and Meta-Analysis. Thromb. J. 2022, 20, 35. [Google Scholar] [CrossRef] [PubMed]
- Mac Grory, B.; Holmes, D.N.; Matsouaka, R.A.; Shah, S.; Chang, C.W.J.; Rison, R.; Jindal, J.; Holmstedt, C.; Logan, W.R.; Corral, C.; et al. Recent Vitamin K Antagonist Use and Intracranial Hemorrhage After Endovascular Thrombectomy for Acute Ischemic Stroke. JAMA 2023, 329, 2038–2049. [Google Scholar] [CrossRef] [PubMed]
- L’Allinec, V.; Sibon, I.; Mazighi, M.; Labreuche, J.; Kyheng, M.; Boissier, E.; Roy, M.; Gory, B.; Dargazanli, C.; Desal, H.; et al. MT in Anticoagulated Patients: Direct Oral Anticoagulants versus Vitamin K Antagonists. Neurology 2020, 94, e842–e850. [Google Scholar] [CrossRef] [PubMed]
- Yoo, A.J.; Andersson, T. Thrombectomy in Acute Ischemic Stroke: Challenges to Procedural Success. J. Stroke 2017, 19, 121–130. [Google Scholar] [CrossRef]
- Fitzgerald, S.; Mereuta, O.M.; Doyle, K.M.; Dai, D.; Kadirvel, R.; Kallmes, D.F.; Brinjikji, W. Correlation of Imaging and Histopathology of Thrombi in Acute Ischemic Stroke with Etiology and Outcome. J. Neurointerv. Surg. 2017, 9, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Patil, S.; Darcourt, J.; Messina, P.; Bozsak, F.; Cognard, C.; Doyle, K. Characterising Acute Ischaemic Stroke Thrombi: Insights from Histology, Imaging and Emerging Impedance-Based Technologies. Stroke Vasc. Neurol. 2022, 7, 353–363. [Google Scholar] [CrossRef] [PubMed]
- Matusevicius, M.; Cooray, C.; Rand, V.-M.; Nunes, A.P.; Moreira, T.; Tassi, R.; Egido, J.A.; Ollikainen, J.; Bigliardi, G.; Holmin, S.; et al. Stroke Etiology and Outcomes after Endovascular Thrombectomy: Results from the SITS Registry and a Meta-Analysis. J. Stroke 2021, 23, 388–400. [Google Scholar] [CrossRef]
- Deniz, C.; Kula, A.Y.; Altunan, B.; Asil, T. Effects of Stroke Etiology on Angiographic Success in Patients Undergoing Mechanical Thrombectomy. Neurol. Sci. 2022, 43, 3737–3745. [Google Scholar] [CrossRef]
- Boeckh-Behrens, T.; Kleine, J.F.; Zimmer, C.; Neff, F.; Scheipl, F.; Pelisek, J.; Schirmer, L.; Nguyen, K.; Karatas, D.; Poppert, H. Thrombus Histology Suggests Cardioembolic Cause in Cryptogenic Stroke. Stroke 2016, 47, 1864–1871. [Google Scholar] [CrossRef]
- Polymeris, A.A.; Meinel, T.R.; Oehler, H.; Hölscher, K.; Zietz, A.; Scheitz, J.F.; Nolte, C.H.; Stretz, C.; Yaghi, S.; Stoll, S.; et al. Aetiology, Secondary Prevention Strategies and Outcomes of Ischaemic Stroke despite Oral Anticoagulant Therapy in Patients with Atrial Fibrillation. J. Neurol. Neurosurg. Psychiatry 2022, 93, 588–598. [Google Scholar] [CrossRef]
- Paciaroni, M.; Agnelli, G.; Caso, V.; Silvestrelli, G.; Seiffge, D.J.; Engelter, S.; De Marchis, G.M.; Polymeris, A.; Zedde, M.L.; Yaghi, S.; et al. Causes and Risk Factors of Cerebral Ischemic Events in Patients With Atrial Fibrillation Treated With Non-Vitamin K Antagonist Oral Anticoagulants for Stroke Prevention. Stroke 2019, 50, 2168–2174. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.M.; Kim, D.S.; Kim, M. Hemorrhagic Transformation After Ischemic Stroke: Mechanisms and Management. Front. Neurol. 2021, 12, 703258. [Google Scholar] [CrossRef] [PubMed]
- Sussman, E.S.; Connolly, E.S. Hemorrhagic Transformation: A Review of the Rate of Hemorrhage in the Major Clinical Trials of Acute Ischemic Stroke. Front. Neurol. 2013, 4, 69. [Google Scholar] [CrossRef]
- Spronk, E.; Sykes, G.; Falcione, S.; Munsterman, D.; Joy, T.; Kamtchum-Tatuene, J.; Jickling, G.C. Hemorrhagic Transformation in Ischemic Stroke and the Role of Inflammation. Front. Neurol. 2021, 12, 661955. [Google Scholar] [CrossRef] [PubMed]
- Hart, R.G.; Coull, B.M.; Hart, D. Early Recurrent Embolism Associated with Nonvalvular Atrial Fibrillation: A Retrospective Study. Stroke 1983, 14, 688–693. [Google Scholar] [CrossRef]
- Heidbuchel, H.; Verhamme, P.; Alings, M.; Antz, M.; Hacke, W.; Oldgren, J.; Sinnaeve, P.; Camm, A.J.; Kirchhof, P. EHRA Practical Guide on the Use of New Oral Anticoagulants in Patients with Non-Valvular Atrial Fibrillation: Executive Summary†. Eur. Heart J. 2013, 34, 2094–2106. [Google Scholar] [CrossRef] [PubMed]
- Klijn, C.J.; Paciaroni, M.; Berge, E.; Korompoki, E.; Kõrv, J.; Lal, A.; Putaala, J.; Werring, D.J. Antithrombotic Treatment for Secondary Prevention of Stroke and Other Thromboembolic Events in Patients with Stroke or Transient Ischemic Attack and Non-Valvular Atrial Fibrillation: A European Stroke Organisation Guideline. Eur. Stroke J. 2019, 4, 198–223. [Google Scholar] [CrossRef]
- Kleindorfer, D.O.; Towfighi, A.; Chaturvedi, S.; Cockroft, K.M.; Gutierrez, J.; Lombardi-Hill, D.; Kamel, H.; Kernan, W.N.; Kittner, S.J.; Leira, E.C.; et al. 2021 Guideline for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack: A Guideline From the American Heart Association/American Stroke Association. Stroke 2021, 52, e364–e467. [Google Scholar] [CrossRef]
- Fischer, U.; Koga, M.; Strbian, D.; Branca, M.; Abend, S.; Trelle, S.; Paciaroni, M.; Thomalla, G.; Michel, P.; Nedeltchev, K.; et al. Early versus Later Anticoagulation for Stroke with Atrial Fibrillation. N. Engl. J. Med. 2023, 388, 2411–2421. [Google Scholar] [CrossRef]
- Oldgren, J.; Åsberg, S.; Hijazi, Z.; Wester, P.; Bertilsson, M.; Norrving, B. Early Versus Delayed Non–Vitamin K Antagonist Oral Anticoagulant Therapy After Acute Ischemic Stroke in Atrial Fibrillation (TIMING): A Registry-Based Randomized Controlled Noninferiority Study. Circulation 2022, 146, 1056–1066. [Google Scholar] [CrossRef]
- Seiffge, D.J.; Traenka, C.; Polymeris, A.; Hert, L.; Peters, N.; Lyrer, P.; Engelter, S.T.; Bonati, L.H.; Marchis, G.M.D. Early Start of DOAC after Ischemic Stroke: Risk of Intracranial Hemorrhage and Recurrent Events. Neurology 2016, 87, 1856–1862. [Google Scholar] [CrossRef] [PubMed]
- Arihiro, S.; Todo, K.; Koga, M.; Furui, E.; Kinoshita, N.; Kimura, K.; Yamagami, H.; Terasaki, T.; Yoshimura, S.; Shiokawa, Y.; et al. Three-Month Risk-Benefit Profile of Anticoagulation after Stroke with Atrial Fibrillation: The SAMURAI-Nonvalvular Atrial Fibrillation (NVAF) Study. Int. J. Stroke 2016, 11, 565–574. [Google Scholar] [CrossRef] [PubMed]
- Paciaroni, M.; Agnelli, G.; Falocci, N.; Tsivgoulis, G.; Vadikolias, K.; Liantinioti, C.; Chondrogianni, M.; Bovi, P.; Carletti, M.; Cappellari, M.; et al. Early Recurrence and Major Bleeding in Patients With Acute Ischemic Stroke and Atrial Fibrillation Treated With Non-Vitamin-K Oral Anticoagulants (RAF-NOACs) Study. J. Am. Heart Assoc. 2017, 6, e007034. [Google Scholar] [CrossRef]
- Carnicelli, A.P.; Hong, H.; Giugliano, R.P.; Connolly, S.J.; Eikelboom, J.; Patel, M.R.; Wallentin, L.; Morrow, D.A.; Wojdyla, D.; Hua, K.; et al. Individual Patient Data from the Pivotal Randomized Controlled Trials of Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation (COMBINE AF): Design and Rationale: From the COMBINE AF (A Collaboration between Multiple Institutions to Better Investigate Non-Vitamin K Antagonist Oral Anticoagulant Use in Atrial Fibrillation) Investigators. Am. Heart J. 2021, 233, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Benz, A.P.; Hohnloser, S.H.; Eikelboom, J.W.; Carnicelli, A.P.; Giugliano, R.P.; Granger, C.B.; Harrington, J.; Hijazi, Z.; Morrow, D.A.; Patel, M.R.; et al. Outcomes of Patients with Atrial Fibrillation and Ischemic Stroke While on Oral Anticoagulation. Eur. Heart J. 2023, 44, 1807–1814. [Google Scholar] [CrossRef] [PubMed]
- Paciaroni, M.; Agnelli, G.; Falocci, N.; Caso, V.; Becattini, C.; Marcheselli, S.; Rueckert, C.; Pezzini, A.; Poli, L.; Padovani, A.; et al. Early Recurrence and Cerebral Bleeding in Patients With Acute Ischemic Stroke and Atrial Fibrillation. Stroke 2015, 46, 2175–2182. [Google Scholar] [CrossRef] [PubMed]
- Diener, H.-C.; Connolly, S.J.; Ezekowitz, M.D.; Wallentin, L.; Reilly, P.A.; Yang, S.; Xavier, D.; Di Pasquale, G.; Yusuf, S. RE-LY study group Dabigatran Compared with Warfarin in Patients with Atrial Fibrillation and Previous Transient Ischaemic Attack or Stroke: A Subgroup Analysis of the RE-LY Trial. Lancet Neurol. 2010, 9, 1157–1163. [Google Scholar] [CrossRef]
- Diener, H.-C.; Eikelboom, J.; Connolly, S.J.; Joyner, C.D.; Hart, R.G.; Lip, G.Y.H.; O’Donnell, M.; Hohnloser, S.H.; Hankey, G.J.; Shestakovska, O.; et al. Apixaban versus Aspirin in Patients with Atrial Fibrillation and Previous Stroke or Transient Ischaemic Attack: A Predefined Subgroup Analysis from AVERROES, a Randomised Trial. Lancet Neurol. 2012, 11, 225–231. [Google Scholar] [CrossRef]
- Hankey, G.J.; Patel, M.R.; Stevens, S.R.; Becker, R.C.; Breithardt, G.; Carolei, A.; Diener, H.-C.; Donnan, G.A.; Halperin, J.L.; Mahaffey, K.W.; et al. Rivaroxaban Compared with Warfarin in Patients with Atrial Fibrillation and Previous Stroke or Transient Ischaemic Attack: A Subgroup Analysis of ROCKET AF. Lancet Neurol. 2012, 11, 315–322. [Google Scholar] [CrossRef]
- Easton, J.D.; Lopes, R.D.; Bahit, M.C.; Wojdyla, D.M.; Granger, C.B.; Wallentin, L.; Alings, M.; Goto, S.; Lewis, B.S.; Rosenqvist, M.; et al. Apixaban Compared with Warfarin in Patients with Atrial Fibrillation and Previous Stroke or Transient Ischaemic Attack: A Subgroup Analysis of the ARISTOTLE Trial. Lancet Neurol. 2012, 11, 503–511. [Google Scholar] [CrossRef]
- Rost, N.S.; Giugliano, R.P.; Ruff, C.T.; Murphy, S.A.; Crompton, A.E.; Norden, A.D.; Silverman, S.; Singhal, A.B.; Nicolau, J.C.; SomaRaju, B.; et al. Outcomes With Edoxaban Versus Warfarin in Patients With Previous Cerebrovascular Events: Findings From ENGAGE AF-TIMI 48 (Effective Anticoagulation With Factor Xa Next Generation in Atrial Fibrillation-Thrombolysis in Myocardial Infarction 48). Stroke 2016, 47, 2075–2082. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, K.; Koga, M.; Lee, K.-J.; Kim, B.J.; Park, E.L.; Lee, J.; Mizoguchi, T.; Yoshimura, S.; Cha, J.-K.; Lee, B.-C.; et al. Atrial Fibrillation-Associated Ischemic Stroke Patients With Prior Anticoagulation Have Higher Risk for Recurrent Stroke. Stroke 2020, 51, 1150–1157. [Google Scholar] [CrossRef] [PubMed]
- Yaghi, S.; Henninger, N.; Giles, J.A.; Leon Guerrero, C.; Mistry, E.; Liberman, A.L.; Asad, D.; Liu, A.; Nagy, M.; Kaushal, A.; et al. Ischemic Stroke on Anticoagulation Therapy and Early Recurrence in Acute Cardioembolic Stroke: The IAC Study. J. Neurol. Neurosurg Psychiatry 2021, 92, 1062–1067. [Google Scholar] [CrossRef]
- Benz, A.P.; Johansson, I.; Dewilde, W.J.M.; Lopes, R.D.; Mehran, R.; Sartori, S.; Sarafoff, N.; Yasuda, S.; McIntyre, W.F.; Healey, J.S.; et al. Antiplatelet Therapy in Patients with Atrial Fibrillation: A Systematic Review and Meta-Analysis of Randomized Trials. Eur. Heart J. Cardiovasc. Pharmacother. 2022, 8, 648–659. [Google Scholar] [CrossRef] [PubMed]
- Eikelboom, J.W.; Connolly, S.J.; Bosch, J.; Dagenais, G.R.; Hart, R.G.; Shestakovska, O.; Diaz, R.; Alings, M.; Lonn, E.M.; Anand, S.S.; et al. Rivaroxaban with or without Aspirin in Stable Cardiovascular Disease. N. Engl. J. Med. 2017, 377, 1319–1330. [Google Scholar] [CrossRef] [PubMed]
- Whitlock, R.P.; Belley-Cote, E.P.; Paparella, D.; Healey, J.S.; Brady, K.; Sharma, M.; Reents, W.; Budera, P.; Baddour, A.J.; Fila, P.; et al. Left Atrial Appendage Occlusion during Cardiac Surgery to Prevent Stroke. N. Engl. J. Med. 2021, 384, 2081–2091. [Google Scholar] [CrossRef]
- Ahmed, N.; Audebert, H.; Turc, G.; Cordonnier, C.; Christensen, H.; Sacco, S.; Sandset, E.C.; Ntaios, G.; Charidimou, A.; Toni, D.; et al. Consensus Statements and Recommendations from the ESO-Karolinska Stroke Update Conference, Stockholm 11–13 November 2018. Eur. Stroke J. 2019, 4, 307–317. [Google Scholar] [CrossRef]
- Woo, D.; Comeau, M.E.; Venema, S.U.; Anderson, C.D.; Flaherty, M.; Testai, F.; Kittner, S.; Frankel, M.; James, M.L.; Sung, G.; et al. Risk Factors Associated With Mortality and Neurologic Disability After Intracerebral Hemorrhage in a Racially and Ethnically Diverse Cohort. JAMA Netw. Open 2022, 5, e221103. [Google Scholar] [CrossRef]
- Biessels, G.J. Cerebral Amyloid Angiopathy. Stroke 2020, 51, 3487–3488. [Google Scholar] [CrossRef]
- Rajashekar, D.; Liang, J.W. Intracerebral Hemorrhage. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- van Asch, C.J.; Luitse, M.J.; Rinkel, G.J.; van der Tweel, I.; Algra, A.; Klijn, C.J. Incidence, Case Fatality, and Functional Outcome of Intracerebral Haemorrhage over Time, According to Age, Sex, and Ethnic Origin: A Systematic Review and Meta-Analysis. Lancet Neurol. 2010, 9, 167–176. [Google Scholar] [CrossRef]
- Sturgeon, J.D.; Folsom, A.R.; Longstreth, W.T.; Shahar, E.; Rosamond, W.D.; Cushman, M. Risk Factors for Intracerebral Hemorrhage in a Pooled Prospective Study. Stroke 2007, 38, 2718–2725. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, M.J.; Xavier, D.; Liu, L.; Zhang, H.; Chin, S.L.; Rao-Melacini, P.; Rangarajan, S.; Islam, S.; Pais, P.; McQueen, M.J.; et al. Risk Factors for Ischaemic and Intracerebral Haemorrhagic Stroke in 22 Countries (the INTERSTROKE Study): A Case-Control Study. Lancet 2010, 376, 112–123. [Google Scholar] [CrossRef] [PubMed]
- López-López, J.A.; Sterne, J.A.C.; Thom, H.H.Z.; Higgins, J.P.T.; Hingorani, A.D.; Okoli, G.N.; Davies, P.A.; Bodalia, P.N.; Bryden, P.A.; Welton, N.J.; et al. Oral Anticoagulants for Prevention of Stroke in Atrial Fibrillation: Systematic Review, Network Meta-Analysis, and Cost Effectiveness Analysis. BMJ 2017, 359, j5058. [Google Scholar] [CrossRef] [PubMed]
- Reversal of Anticoagulation in Intracranial Hemorrhage—UpToDate. Available online: https://www.uptodate.com/contents/reversal-of-anticoagulation-in-intracranial-hemorrhage (accessed on 19 June 2023).
- Gokcal, E.; Pasi, M.; Fisher, M.; Gurol, M.E. Atrial Fibrillation for the Neurologist: Preventing Both Ischemic and Hemorrhagic Strokes. Curr. Neurol. Neurosci. Rep. 2018, 18, 6. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Sanchis-Gomar, F.; Cervellin, G. Global Epidemiology of Atrial Fibrillation: An Increasing Epidemic and Public Health Challenge. Int. J. Stroke 2021, 16, 217–221. [Google Scholar] [CrossRef] [PubMed]
- García Rodríguez, L.A.; Cea Soriano, L.; de Abajo, F.J.; Valent, F.; Hallas, J.; Gil, M.; Cattaruzzi, C.; Rodriguez-Martin, S.; Vora, P.; Soriano-Gabarró, M.; et al. Trends in the Use of Oral Anticoagulants, Antiplatelets and Statins in Four European Countries: A Population-Based Study. Eur. J. Clin. Pharmacol. 2022, 78, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Hu, X.; Song, L.; Chen, X.; Ouyang, M.; Billot, L.; Li, Q.; Malavera, A.; Li, X.; Muñoz-Venturelli, P.; et al. The Third Intensive Care Bundle with Blood Pressure Reduction in Acute Cerebral Haemorrhage Trial (INTERACT3): An International, Stepped Wedge Cluster Randomised Controlled Trial. Lancet 2023, 402, 27–40. [Google Scholar] [CrossRef]
- Greenberg, S.M.; Ziai, W.C.; Cordonnier, C.; Dowlatshahi, D.; Francis, B.; Goldstein, J.N.; Hemphill, J.C.; Johnson, R.; Keigher, K.M.; Mack, W.J.; et al. 2022 Guideline for the Management of Patients With Spontaneous Intracerebral Hemorrhage: A Guideline From the American Heart Association/American Stroke Association. Stroke 2022, 53, e282–e361. [Google Scholar] [CrossRef]
- Steiner, T.; Salman, R.A.-S.; Beer, R.; Christensen, H.; Cordonnier, C.; Csiba, L.; Forsting, M.; Harnof, S.; Klijn, C.J.M.; Krieger, D.; et al. European Stroke Organisation (ESO) Guidelines for the Management of Spontaneous Intracerebral Hemorrhage. Int. J. Stroke 2014, 9, 840–855. [Google Scholar] [CrossRef]
- Hill, M.D.; Muir, K.W. Interact-2. Stroke 2013, 44, 2951–2952. [Google Scholar] [CrossRef]
- Qureshi, A.I.; Palesch, Y.Y.; Barsan, W.G.; Hanley, D.F.; Hsu, C.Y.; Martin, R.L.; Moy, C.S.; Silbergleit, R.; Steiner, T.; Suarez, J.I.; et al. Intensive Blood-Pressure Lowering in Patients with Acute Cerebral Hemorrhage. N. Engl. J. Med. 2016, 375, 1033–1043. [Google Scholar] [CrossRef] [PubMed]
- Moullaali, T.J.; Wang, X.; Martin, R.H.; Shipes, V.B.; Robinson, T.G.; Chalmers, J.; Suarez, J.I.; Qureshi, A.I.; Palesch, Y.Y.; Anderson, C.S. Blood Pressure Control and Clinical Outcomes in Acute Intracerebral Haemorrhage: A Preplanned Pooled Analysis of Individual Participant Data. Lancet Neurol. 2019, 18, 857–864. [Google Scholar] [CrossRef] [PubMed]
- Rabinstein, A.A. Optimal Blood Pressure After Intracerebral Hemorrhage. Stroke 2018, 49, 275–276. [Google Scholar] [CrossRef] [PubMed]
- Dammers, R.; Beck, J.; Volovici, V.; Anderson, C.S.; Klijn, C.J.M. Advancing the Surgical Treatment of Intracerebral Hemorrhage: Study Design and Research Directions. World Neurosurg. 2022, 161, 367–375. [Google Scholar] [CrossRef] [PubMed]
- Kellner, C.P.; Schupper, A.J.; Mocco, J. Surgical Evacuation of Intracerebral Hemorrhage. Stroke 2021, 52, 3391–3398. [Google Scholar] [CrossRef] [PubMed]
- Ratcliff, J.J.; Hall, A.J.; Porto, E.; Saville, B.R.; Lewis, R.J.; Allen, J.W.; Frankel, M.; Wright, D.W.; Barrow, D.L.; Pradilla, G. Early Minimally Invasive Removal of Intracerebral Hemorrhage (ENRICH): Study Protocol for a Multi-Centered Two-Arm Randomized Adaptive Trial. Front. Neurol. 2023, 14, 1126958. [Google Scholar] [CrossRef] [PubMed]
- Steiner, T.; Poli, S.; Griebe, M.; Hüsing, J.; Hajda, J.; Freiberger, A.; Bendszus, M.; Bösel, J.; Christensen, H.; Dohmen, C.; et al. Fresh Frozen Plasma versus Prothrombin Complex Concentrate in Patients with Intracranial Haemorrhage Related to Vitamin K Antagonists (INCH): A Randomised Trial. Lancet Neurol. 2016, 15, 566–573. [Google Scholar] [CrossRef]
- Dowlatshahi, D.; Butcher, K.S.; Asdaghi, N.; Nahirniak, S.; Bernbaum, M.L.; Giulivi, A.; Wasserman, J.K.; Poon, M.-C.; Coutts, S.B. Poor Prognosis in Warfarin-Associated Intracranial Hemorrhage Despite Anticoagulation Reversal. Stroke 2012, 43, 1812–1817. [Google Scholar] [CrossRef]
- Christensen, H.; Cordonnier, C.; Kõrv, J.; Lal, A.; Ovesen, C.; Purrucker, J.C.; Toni, D.; Steiner, T. European Stroke Organisation Guideline on Reversal of Oral Anticoagulants in Acute Intracerebral Haemorrhage. Eur. Stroke J. 2019, 4, 294–306. [Google Scholar] [CrossRef]
- Connolly, S.J.; Crowther, M.; Eikelboom, J.W.; Gibson, C.M.; Curnutte, J.T.; Lawrence, J.H.; Yue, P.; Bronson, M.D.; Lu, G.; Conley, P.B.; et al. Full Study Report of Andexanet Alfa for Bleeding Associated with Factor Xa Inhibitors. N. Engl. J. Med. 2019, 380, 1326–1335. [Google Scholar] [CrossRef]
- Siegal, D.M.; Curnutte, J.T.; Connolly, S.J.; Lu, G.; Conley, P.B.; Wiens, B.L.; Mathur, V.S.; Castillo, J.; Bronson, M.D.; Leeds, J.M.; et al. Andexanet Alfa for the Reversal of Factor Xa Inhibitor Activity. N. Engl. J. Med. 2015, 373, 2413–2424. [Google Scholar] [CrossRef] [PubMed]
- Reed, M.; Tadi, P.; Nicolas, D. Andexanet Alfa. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Nielsen, P.B.; Melgaard, L.; Overvad, T.F.; Jensen, M.; Larsen, T.B.; Lip, G.Y.H.; Veltkamp, R.; Harvey, K.H.; Korompoki, E.; D’Anna, L.; et al. Risk of Cerebrovascular Events in Intracerebral Hemorrhage Survivors With Atrial Fibrillation: A Nationwide Cohort Study. Stroke 2022, 53, 2559–2568. [Google Scholar] [CrossRef] [PubMed]
- Ivany, E.; Ritchie, L.A.; Lip, G.Y.H.; Lotto, R.R.; Werring, D.J.; Lane, D.A. Effectiveness and Safety of Antithrombotic Medication in Patients With Atrial Fibrillation and Intracranial Hemorrhage: Systematic Review and Meta-Analysis. Stroke 2022, 53, 3035–3046. [Google Scholar] [CrossRef] [PubMed]
- Murthy, S.B.; Gupta, A.; Merkler, A.E.; Navi, B.B.; Mandava, P.; Iadecola, C.; Sheth, K.N.; Hanley, D.F.; Ziai, W.C.; Kamel, H. Restarting Anticoagulant Therapy After Intracranial Hemorrhage. Stroke 2017, 48, 1594–1600. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Yu, J.; Carcel, C.; Delcourt, C.; Jiehui, S.; Lindley, R.; Neal, B.; Anderson, C.; Hackett, M. Resuming Anticoagulants after Anticoagulation-Associated Intracranial Haemorrhage: Systematic Review and Meta-Analysis. BMJ Open 2018, 8, e019672. [Google Scholar] [CrossRef] [PubMed]
- Biffi, A.; Kuramatsu, J.B.; Leasure, A.; Kamel, H.; Kourkoulis, C.; Schwab, K.; Ayres, A.M.; Elm, J.; Gurol, M.E.; Greenberg, S.M.; et al. Oral Anticoagulation and Functional Outcome after Intracerebral Hemorrhage. Ann. Neurol. 2017, 82, 755–765. [Google Scholar] [CrossRef]
- Cochrane, A.; Chen, C.; Stephen, J.; Rønning, O.M.; Anderson, C.S.; Hankey, G.J.; Al-Shahi Salman, R. Antithrombotic Treatment after Stroke Due to Intracerebral Haemorrhage. Cochrane Database Syst. Rev. 2023, 1, CD012144. [Google Scholar] [CrossRef]
- Charidimou, A.; Imaizumi, T.; Moulin, S.; Biffi, A.; Samarasekera, N.; Yakushiji, Y.; Peeters, A.; Vandermeeren, Y.; Laloux, P.; Baron, J.-C.; et al. Brain Hemorrhage Recurrence, Small Vessel Disease Type, and Cerebral Microbleeds. Neurology 2017, 89, 820–829. [Google Scholar] [CrossRef]
- Pennlert, J.; Overholser, R.; Asplund, K.; Carlberg, B.; Van Rompaye, B.; Wiklund, P.-G.; Eriksson, M. Optimal Timing of Anticoagulant Treatment After Intracerebral Hemorrhage in Patients With Atrial Fibrillation. Stroke 2017, 48, 314–320. [Google Scholar] [CrossRef]
- Poon, M.T.C.; Fonville, A.F.; Salman, R.A.-S. Long-Term Prognosis after Intracerebral Haemorrhage: Systematic Review and Meta-Analysis. J. Neurol. Neurosurg. Psychiatry 2014, 85, 660–667. [Google Scholar] [CrossRef]
- Biffi, A.; Anderson, C.D.; Battey, T.W.K.; Ayres, A.M.; Greenberg, S.M.; Viswanathan, A.; Rosand, J. Association Between Blood Pressure Control and Risk of Recurrent Intracerebral Hemorrhage. JAMA 2015, 314, 904–912. [Google Scholar] [CrossRef] [PubMed]
- Arima, H.; Tzourio, C.; Butcher, K.; Anderson, C.; Bousser, M.-G.; Lees, K.R.; Reid, J.L.; Omae, T.; Woodward, M.; MacMahon, S.; et al. Prior Events Predict Cerebrovascular and Coronary Outcomes in the PROGRESS Trial. Stroke 2006, 37, 1497–1502. [Google Scholar] [CrossRef] [PubMed]
- Mullen, M.T.; Anderson, C.S. Review of Long-Term Blood Pressure Control After Intracerebral Hemorrhage: Challenges and Opportunities. Stroke 2022, 53, 2142–2151. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Poon, M.T.C.; Samarasekera, N.E.; Perry, L.A.; Moullaali, T.J.; Rodrigues, M.A.; Loan, J.J.M.; Stephen, J.; Lerpiniere, C.; Tuna, M.A.; et al. Risks of Recurrent Stroke and All Serious Vascular Events after Spontaneous Intracerebral Haemorrhage: Pooled Analyses of Two Population-Based Studies. Lancet Neurol. 2021, 20, 437–447. [Google Scholar] [CrossRef] [PubMed]
- Boe, N.J.; Hald, S.M.; Jensen, M.M.; Kristensen, L.M.B.; Bojsen, J.A.; Elhakim, M.T.; Clausen, A.; Möller, S.; Hallas, J.; García Rodríguez, L.A.; et al. Major Cardiovascular Events After Spontaneous Intracerebral Hemorrhage by Hematoma Location. JAMA Netw Open 2023, 6, e235882. [Google Scholar] [CrossRef] [PubMed]
- Cordonnier, C.; Al-Shahi Salman, R.; Wardlaw, J. Spontaneous Brain Microbleeds: Systematic Review, Subgroup Analyses and Standards for Study Design and Reporting. Brain 2007, 130, 1988–2003. [Google Scholar] [CrossRef] [PubMed]
- Charidimou, A.; Werring, D.J. Cerebral Microbleeds as a Predictor of Macrobleeds: What Is the Evidence? Int. J. Stroke 2014, 9, 457–459. [Google Scholar] [CrossRef]
- Pongpitakmetha, T.; Fotiadis, P.; Pasi, M.; Boulouis, G.; Xiong, L.; Warren, A.D.; Schwab, K.M.; Rosand, J.; Gurol, M.E.; Greenberg, S.M.; et al. Cortical Superficial Siderosis Progression in Cerebral Amyloid Angiopathy. Neurology 2020, 94, e1853–e1865. [Google Scholar] [CrossRef]
- Charidimou, A.; Linn, J.; Vernooij, M.W.; Opherk, C.; Akoudad, S.; Baron, J.-C.; Greenberg, S.M.; Jäger, H.R.; Werring, D.J. Cortical Superficial Siderosis: Detection and Clinical Significance in Cerebral Amyloid Angiopathy and Related Conditions. Brain 2015, 138, 2126–2139. [Google Scholar] [CrossRef]
- Charidimou, A.; Peeters, A.P.; Jäger, R.; Fox, Z.; Vandermeeren, Y.; Laloux, P.; Baron, J.-C.; Werring, D.J. Cortical Superficial Siderosis and Intracerebral Hemorrhage Risk in Cerebral Amyloid Angiopathy. Neurology 2013, 81, 1666–1673. [Google Scholar] [CrossRef]
- Charidimou, A.; Boulouis, G.; Roongpiboonsopit, D.; Auriel, E.; Pasi, M.; Haley, K.; van Etten, E.S.; Martinez-Ramirez, S.; Ayres, A.; Vashkevich, A.; et al. Cortical Superficial Siderosis Multifocality in Cerebral Amyloid Angiopathy: A Prospective Study. Neurology 2017, 89, 2128–2135. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Diffusion-weighted imaging (DWI). Case of cardioembolic infarct in left hemisphere (bright area).
Figure 1.
Diffusion-weighted imaging (DWI). Case of cardioembolic infarct in left hemisphere (bright area).

Figure 2.
Intravenous thrombolysis (IVT) in patients on oral anticoagulant (OAC) treatment. VKA, vitamin K antagonist; DOAC, direct oral anticoagulants; INR, international normalized ratio; dTT, dilute thrombin time; TT, thrombin time; aPTT, activated partial thromboplastin time; EVT, endovascular treatment.
Figure 2.
Intravenous thrombolysis (IVT) in patients on oral anticoagulant (OAC) treatment. VKA, vitamin K antagonist; DOAC, direct oral anticoagulants; INR, international normalized ratio; dTT, dilute thrombin time; TT, thrombin time; aPTT, activated partial thromboplastin time; EVT, endovascular treatment.

Figure 3.
Timing of initiation of oral anticoagulation (OAC) after ischemic stroke (IS) in patients with non-valvular atrial fibrillation (NVAF) according to the ELAN trial results [92]. IVT, intravenous thrombolysis; MCA, middle cerebral artery; ACA, anterior cerebral artery; PCA, posterior cerebral artery; DOAC, direct oral anticoagulants.
Figure 3.
Timing of initiation of oral anticoagulation (OAC) after ischemic stroke (IS) in patients with non-valvular atrial fibrillation (NVAF) according to the ELAN trial results [92]. IVT, intravenous thrombolysis; MCA, middle cerebral artery; ACA, anterior cerebral artery; PCA, posterior cerebral artery; DOAC, direct oral anticoagulants.

Figure 4.
Head CT of intracerebral hemorrhage (ICH). (A) Deep basal ganglia ICH in the left hemisphere with intraventricular hemorrhage (IVH) due to hypertension. (B) Lobar ICH in right occipital lobe with subarachnoid hemorrhage (SAH) probably due to cerebral amyloid angiopathy (CAA).
Figure 4.
Head CT of intracerebral hemorrhage (ICH). (A) Deep basal ganglia ICH in the left hemisphere with intraventricular hemorrhage (IVH) due to hypertension. (B) Lobar ICH in right occipital lobe with subarachnoid hemorrhage (SAH) probably due to cerebral amyloid angiopathy (CAA).

Figure 5.
Reversal of oral anticoagulation (OAC) in patients with intracerebral hemorrhage (ICH). VKA, vitamin K antagonist; 4F-PCC, f-factor prothrombin complex concentrate; BP, blood pressure; SBP, systolic blood pressure.
Figure 5.
Reversal of oral anticoagulation (OAC) in patients with intracerebral hemorrhage (ICH). VKA, vitamin K antagonist; 4F-PCC, f-factor prothrombin complex concentrate; BP, blood pressure; SBP, systolic blood pressure.

Figure 6.
Radiologic bleeding markers on susceptibility weighted imaging (SWI) on MRI. (A) Multiple lobar cerebral microbleeds (CMBs) in patient with cerebral amyloid angiopathy (CAA). (B) Deep CMBs related to hypertension. (C) Cortical superficial siderosis (cSS) in frontal left hemisphere and posterior right sulci in patient with CAA.
Figure 6.
Radiologic bleeding markers on susceptibility weighted imaging (SWI) on MRI. (A) Multiple lobar cerebral microbleeds (CMBs) in patient with cerebral amyloid angiopathy (CAA). (B) Deep CMBs related to hypertension. (C) Cortical superficial siderosis (cSS) in frontal left hemisphere and posterior right sulci in patient with CAA.


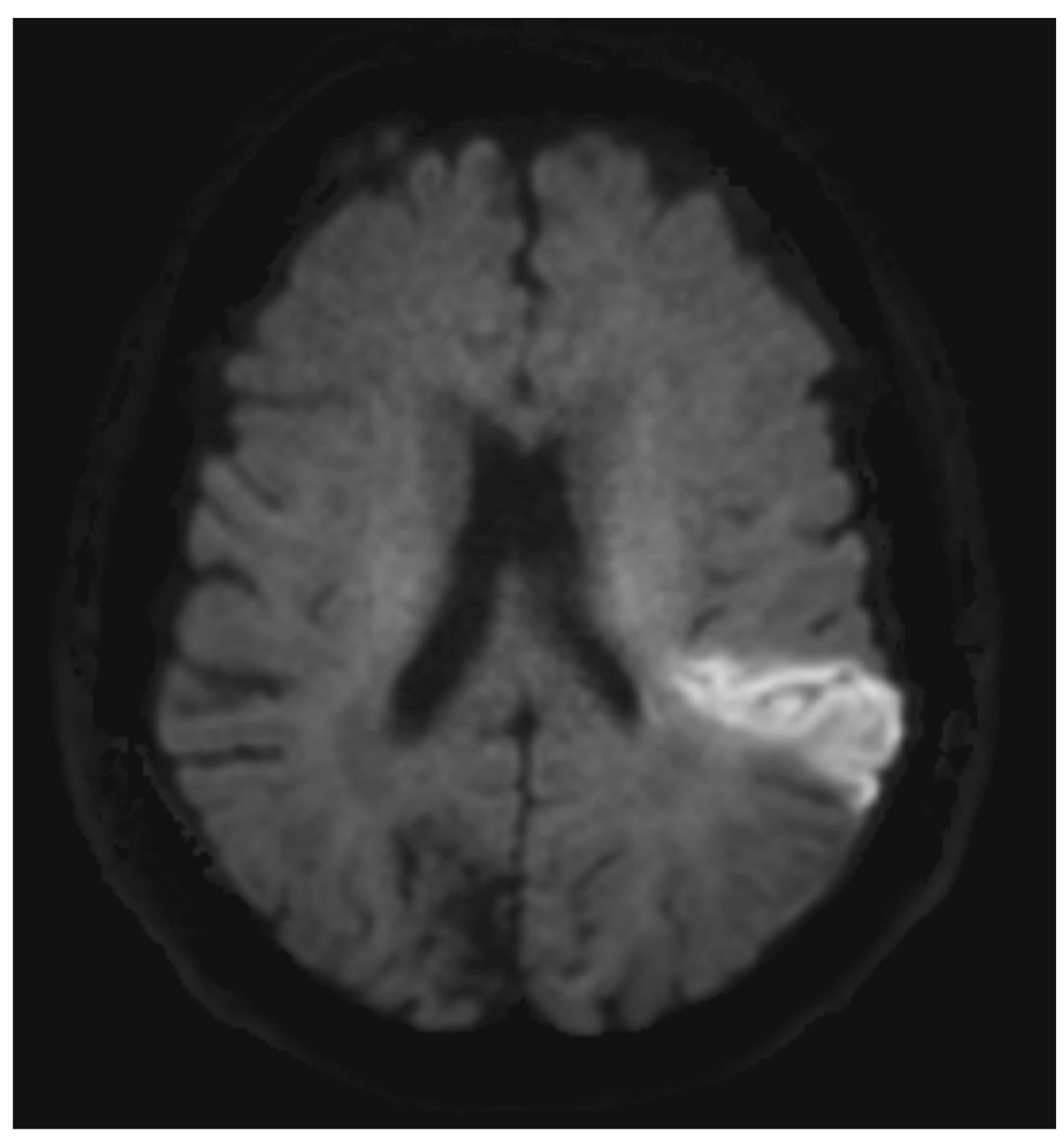{kind=link}
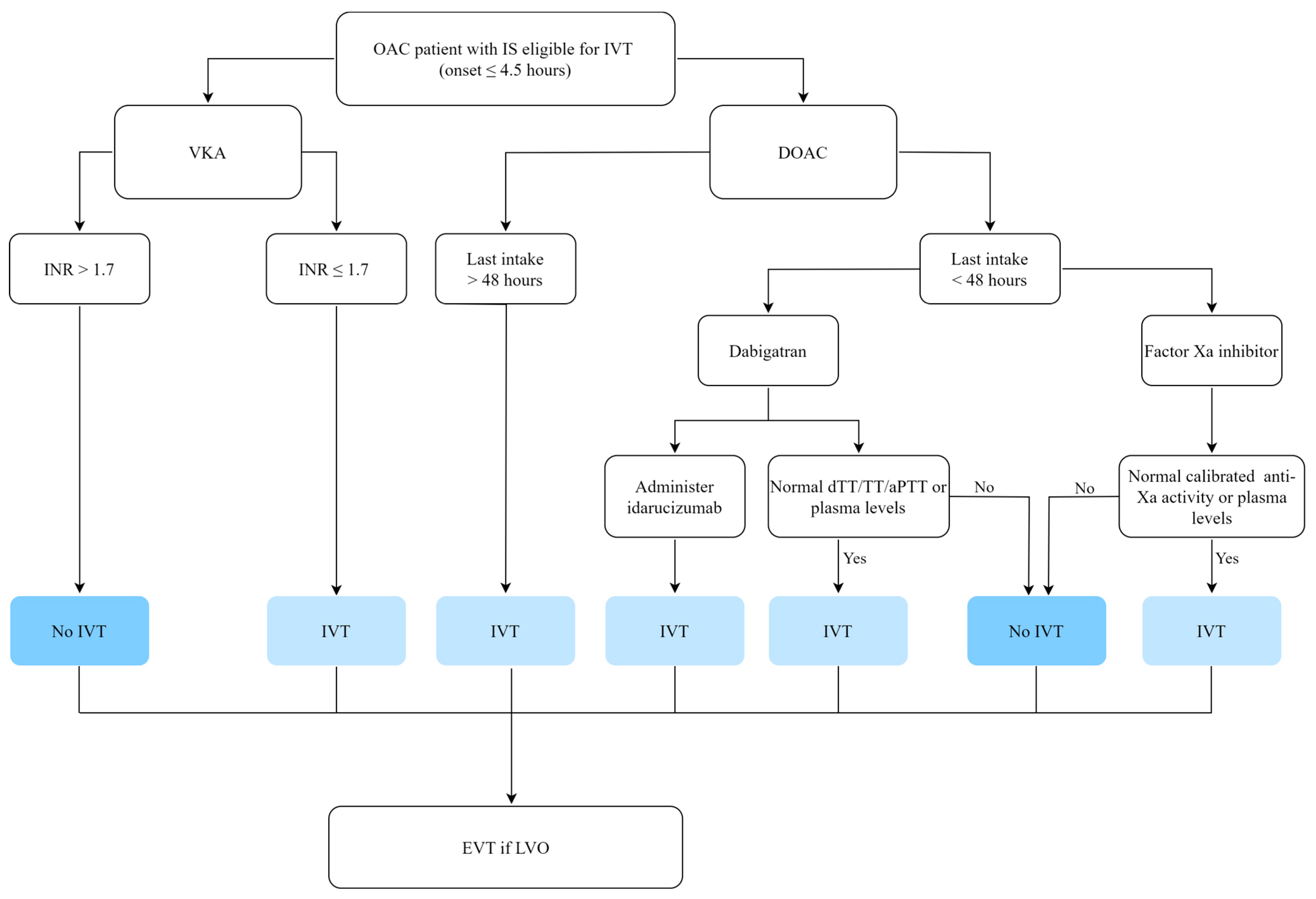{kind=link}
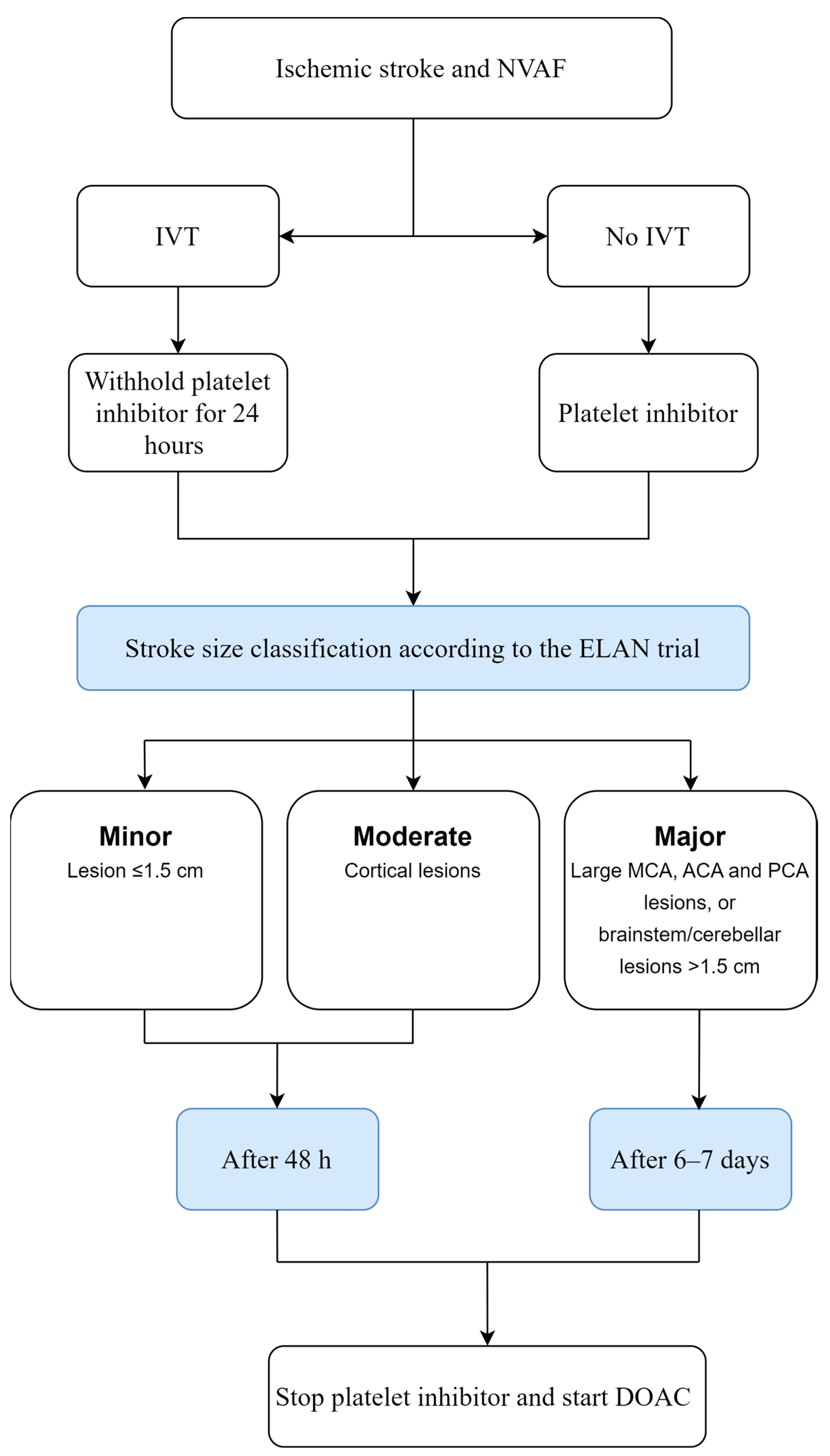{kind=link}
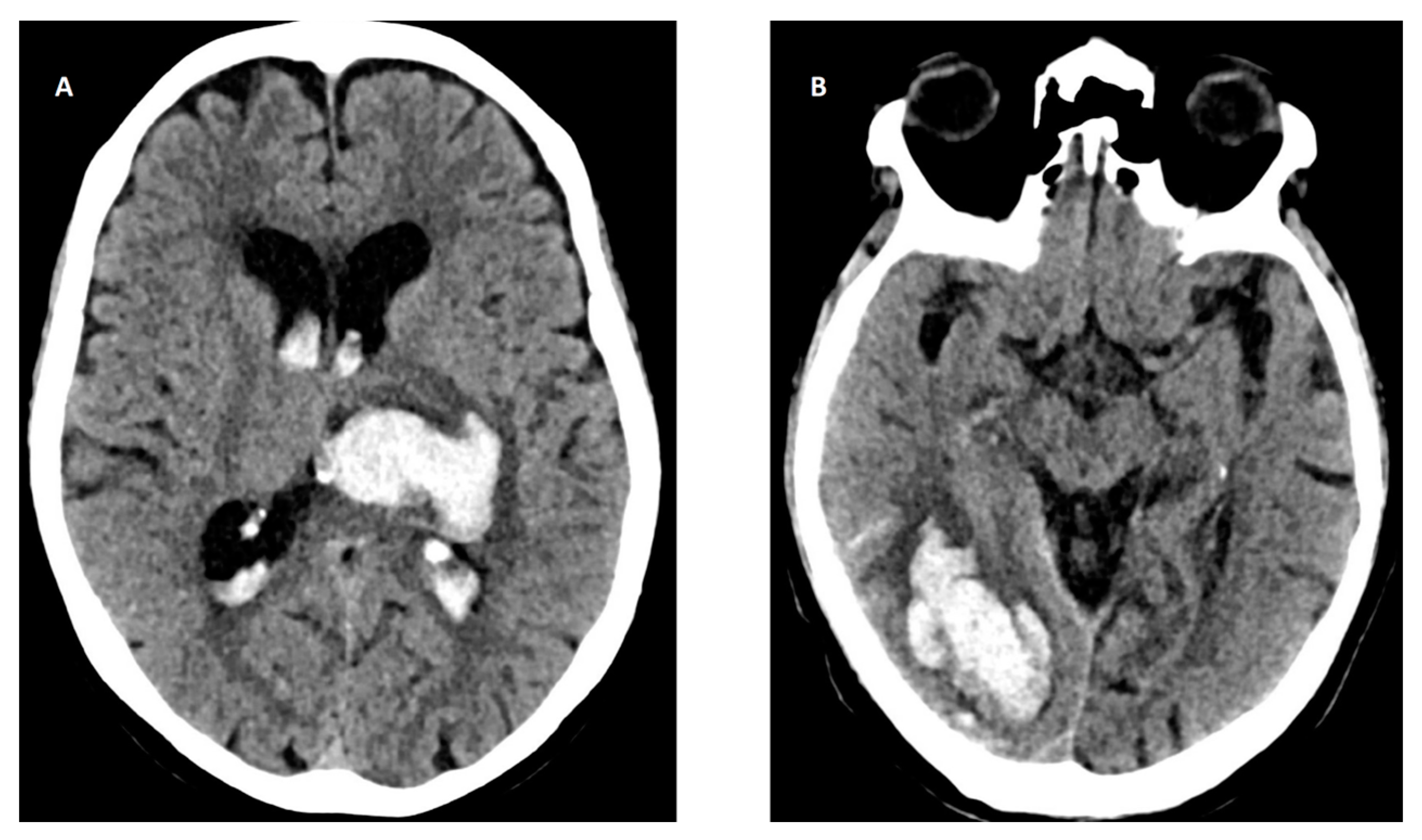{kind=link}
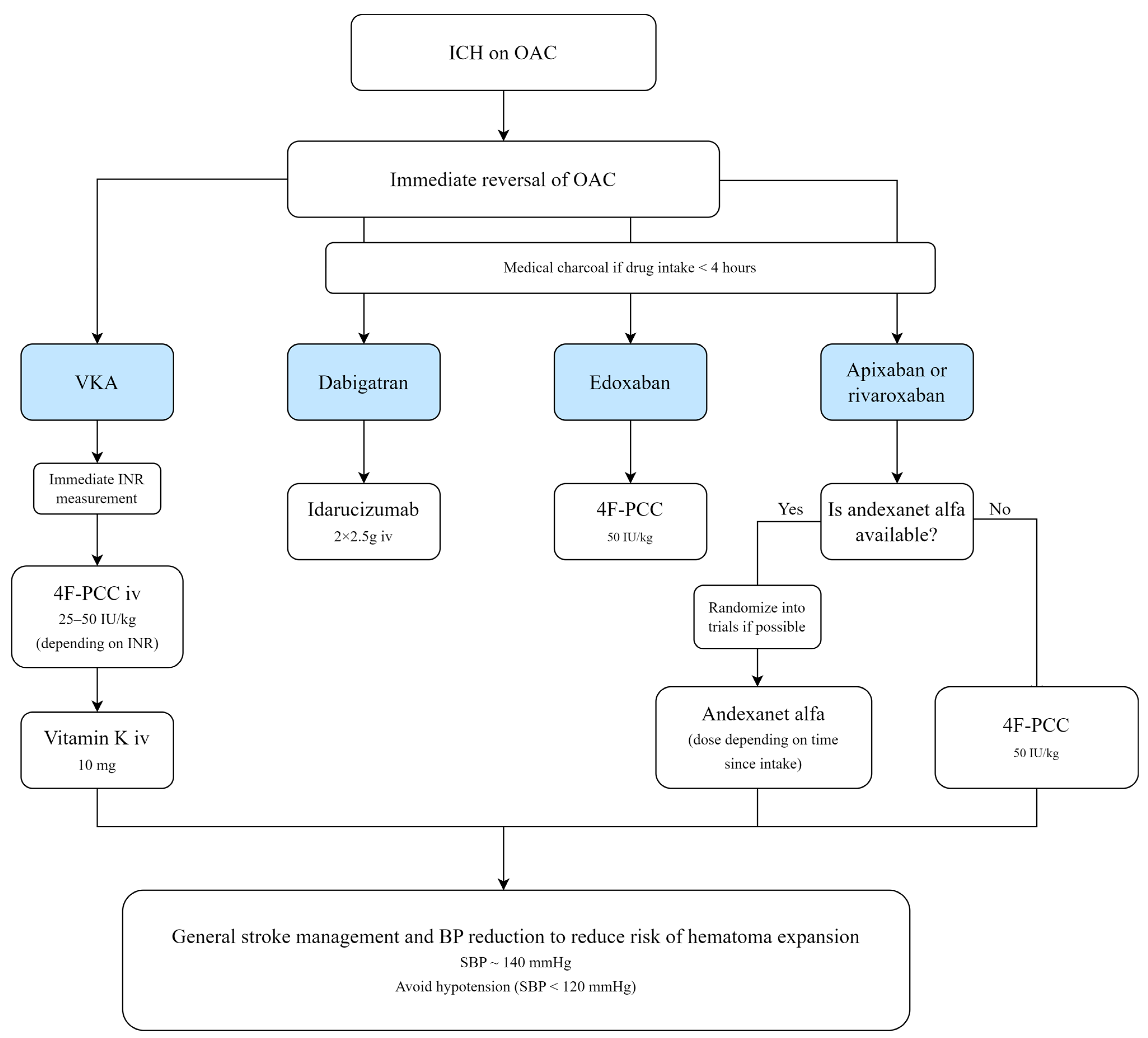{kind=link}
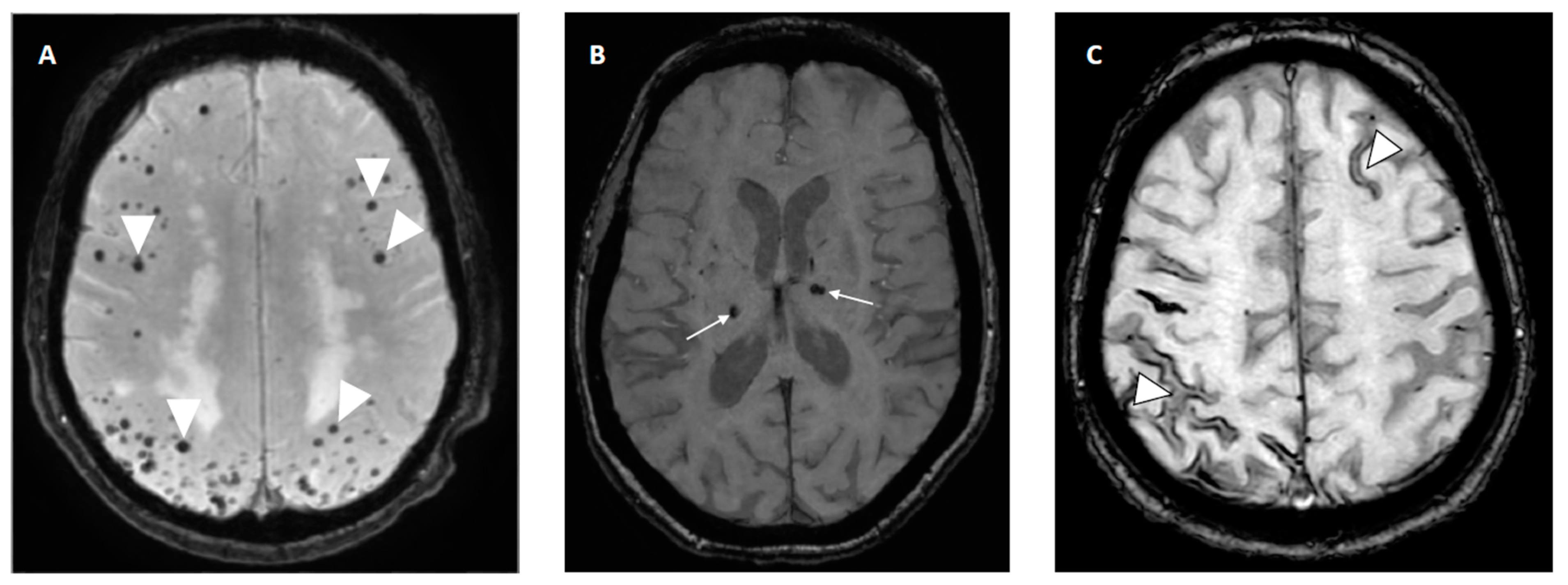{kind=link}
Table 1.
TOAST classification of subtype of ischemic stroke.
| Etiology | Definition | CT/MRI Scan |
|---|---|---|
| Large artery atherosclerosis (LAA) (embolus/thrombus) * | Imaging showing significant stenosis (>50%) of ipsilateral extra- or intracranial artery or occlusion of major brain artery or branch cortical artery due to atherosclerosis. | Cortical and cerebellar lesions, and brain stem and subcortical infarcts ≥ 1.5 cm in diameter. |
| Cardioembolism * | Identification of at least one cardiac high-risk/medium-risk ** source for embolism. | Cortical and cerebellar lesions, and brain stem and subcortical infarcts ≥ 1.5 cm in diameter. |
| Small-vessel occlusion (lacune) * | Clinical lacunar syndromes. Absence of LAA and cardioembolic source identified. Comorbidity of diabetes mellitus and hypertension supports etiology. | Brain stem and subcortical lesions ≤ 1.5 cm in diameter. OR No detectable lesion. |
| Stroke of other determined etiology * | Identification of rarer causes of stroke (vasculitis, hypercoagulable states, and hematologic disorders). | Visual infarct regardless of size and location. |
| Stroke of undetermined etiology | Not possible to determine cause of stroke with confidence due to: ≥2 causes are identified Negative evaluations Incomplete evaluations |
* Possible or probable. ** High-risk/medium-risk sources of cardioembolism are based on the evidence of their propensities for embolism [9].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Hindsholm, M.F.; Damgaard, D.; Gurol, M.E.; Gaist, D.; Simonsen, C.Z. Management and Prognosis of Acute Stroke in Atrial Fibrillation. J. Clin. Med. 2023, 12, 5752. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12175752
AMA Style
Hindsholm MF, Damgaard D, Gurol ME, Gaist D, Simonsen CZ. Management and Prognosis of Acute Stroke in Atrial Fibrillation. Journal of Clinical Medicine. 2023; 12(17):5752. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12175752
Chicago/Turabian StyleHindsholm, Mette F., Dorte Damgaard, M. Edip Gurol, David Gaist, and Claus Z. Simonsen. 2023. "Management and Prognosis of Acute Stroke in Atrial Fibrillation" Journal of Clinical Medicine 12, no. 17: 5752. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12175752
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.