
Evolution of Coronary Stent Platforms: A Brief Overview of Currently Used Drug-Eluting Stents
 , , , ,
, , , ,
Abstract
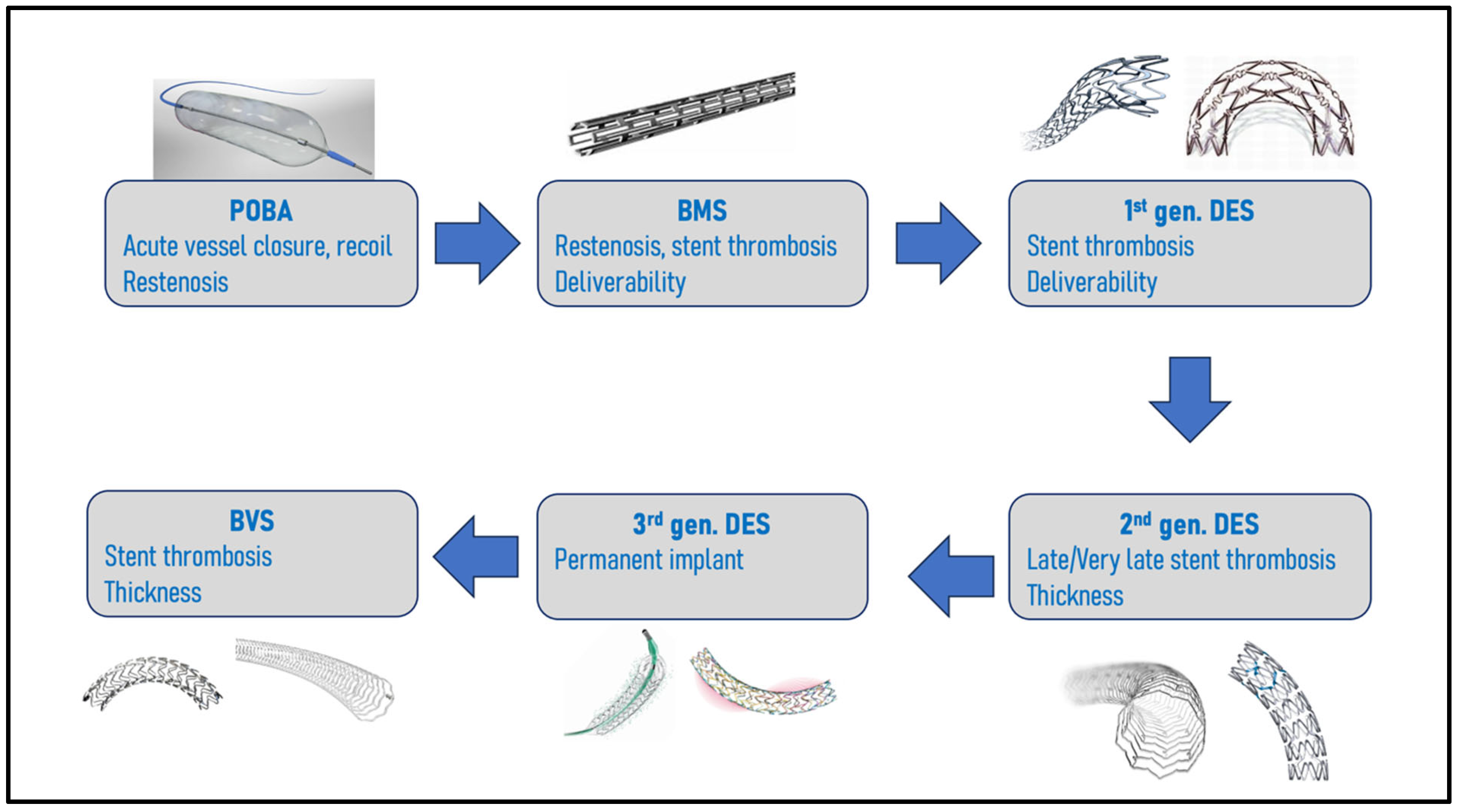
:1. Introduction
2. First and Second-Generation DESs
3. Third Generation DESs
3.1. Durable Polymer DESs
3.1.1. Xience Skypoint™ (Abbott Vascular)
3.1.2. Resolute Onyx™ (Medtronic)
3.2. Biodegradable Polymer DESs
3.2.1. Synergy™ XD (Boston Scientific)
3.2.2. Orsiro® Mission (Biotronik)
3.2.3. Biomatrix Alpha (Biosensors International)
3.2.4. Ultimaster Nagomi™ (Terumo)
3.3. Polymer-Free Drug-Coated Stents
3.3.1. Coroflex® Isar Neo (B. Braun)
3.3.2. Biofreedom Ultra™ (Biosensors)
4. Leaving Nothing Behind
4.1. Bioabsorbable Vascular Scaffolds
4.2. The Future of DESs
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Seldinger, S.I. Catheter replacement of the needle in percutaneous arteriography: A new technique. Acta Radiol. 1953, 39, 368–376. [Google Scholar] [CrossRef] [PubMed]
- Mason Sones, F. Cine-Cardio-Angiography. Pediatr. Clin. N. Am. 1958, 5, 945–979. [Google Scholar] [CrossRef]
- Grüntzig, A.R.; Senning, A.; Siegenthaler, W.E. Nonoperative dilatation of coronary-artery stenosis: Percutaneous transluminal coronary angioplasty. N. Engl. J. Med. 1979, 301, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Bonzel, T.; Wollschläger, H.; Kasper, W.; Meinertz, T.; Just, H. The sliding rail system (monorail): Description of a new technique for intravascular instrumentation and its application to coronary angioplasty. Z. Kardiol. 1987, 76 (Suppl. 6), 119–122. [Google Scholar]
- Picard, F.; Pighi, M.; Marquis-Gravel, G.; Labinaz, M.; Cohen, E.A.; Tanguay, J.F. The Ongoing Saga of the Evolution of Percutaneous Coronary Intervention: From Balloon Angioplasty to Recent Innovations to Future Prospects. Can. J. Cardiol. 2022, 38, S30–S41. [Google Scholar] [CrossRef]
- McKavanagh, P.; Zawadowski, G.; Ahmed, N.; Kutryk, M. The evolution of coronary stents. Expert Rev. Cardiovasc. Ther. 2018, 16, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Serruys, P.W.; de Jaegere, P.; Kiemeneij, F.; Macaya, C.; Rutsch, W.; Heyndrickx, G.; Emanuelsson, H.; Marco, J.; Legrand, V.; Materne, P.; et al. A Comparison of Balloon-Expandable-Stent Implantation with Balloon Angioplasty in Patients with Coronary Artery Disease. N. Engl. J. Med. 1994, 331, 489–495. [Google Scholar] [CrossRef]
- Fischman, D.L.; Leon, M.B.; Baim, D.S.; Schatz, R.A.; Savage, M.P.; Penn, I.; Detre, K.; Veltri, L.; Ricci, D.; Nobuyoshi, M.; et al. A Randomized Comparison of Coronary-Stent Placement and Balloon Angioplasty in the Treatment of Coronary Artery Disease. N. Engl. J. Med. 1994, 331, 496–501. [Google Scholar] [CrossRef] [PubMed]
- Schömig, A.; Neumann, F.J.; Kastrati, A.; Schühlen, H.; Blasini, R.; Hadamitzky, M.; Walter, H.; Zitzmann-Roth, E.M.; Richardt, G.; Alt, E.; et al. A Randomized Comparison of Antiplatelet and Anticoagulant Therapy after the Placement of Coronary-Artery Stents. N. Engl. J. Med. 1996, 334, 1084–1089. [Google Scholar] [CrossRef]
- Morice, M.C.; Hayashi, E.B.; Guagliumi, G. A Randomized Comparison of a Sirolimus-Eluting Stent with a Standard Stent for Coronary Revascularization. N. Engl. J. Med. 2002, 346, 1773–1780. [Google Scholar] [CrossRef]
- Moses, J.W.; Holmes, D.R.; Williams, D.O. Sirolimus-Eluting Stents versus Standard Stents in Patients with Stenosis in a Native Coronary Artery. N. Engl. J. Med. 2003, 349, 1315–1323. [Google Scholar] [CrossRef] [PubMed]
- Stone, G.W.; Ellis, S.G.; Cannon, L.; Mann, J.T.; Greenberg, J.D.; Spriggs, D.; O’Shaughnessy, C.D.; DeMaio, S.; Hall, P.; Popma, J.; et al. Comparison of a Polymer-Based Paclitaxel-Eluting Stent with a Bare Metal Stent in Patients with Complex Coronary Artery Disease A Randomized Controlled Trial. JAMA 2005, 294, 1215–1223. [Google Scholar] [CrossRef] [PubMed]
- Morice, M.C.; Colombo, A.; Meier, B.; Serruys, P.; Tamburino, C.; Guagliumi, G.; Sousa, E.; Stoll, H.-P. Sirolimus- vs Paclitaxel-Eluting Stents in De Novo Coronary Artery Lesions The REALITY Trial: A Randomized Controlled Trial. JAMA 2006, 295, 895–904. [Google Scholar] [CrossRef] [PubMed]
- Kastrati, A.; Mehilli, J.; Von Beckerath, N.; Dibra, A.; Hausleiter, J.; Pache, J.; Schühlen, J.; Schmitt, C.; Dirschinger, J.; Schömig, A.; et al. Sirolimus-Eluting Stent or Paclitaxel-Eluting Stent vs Balloon Angioplasty for Prevention of Recurrences in Patients with Coronary In-Stent Restenosis: A Randomized Controlled Trial. JAMA 2005, 293, 165–171. [Google Scholar] [CrossRef] [PubMed]
- McFadden, E.P.; Stabile, E.; Regar, E.; Cheneau, E.; Ong, A.T.L.; Kinnaird, T.; O Suddath, W.; Weissman, N.J.; Torguson, R.; Kent, K.M.; et al. Late thrombosis in drug-eluting coronary stents after discontinuation of antiplatelet therapy. Cardiology 2004, 364, 1519–1521. [Google Scholar]
- Stone, G.W.; Ellis, S.G.; Colombo, A.; Grube, E.; Popma, J.J.; Uchida, T.; Bleuit, J.S.; Dawkins, K.D.; Russell, M.E. Long-Term Safety and Efficacy of Paclitaxel-Eluting Stents. JACC Cardiovasc. Interv. 2011, 4, 530–542. [Google Scholar] [CrossRef]
- Joner, M.; Finn, A.V.; Farb, A.; Mont, E.K.; Kolodgie, F.D.; Ladich, E.; Kutys, R.; Skorija, K.; Gold, H.K.; Virmani, R. Pathology of Drug-Eluting Stents in Humans. J. Am. Coll. Cardiol. 2006, 48, 193–202. [Google Scholar] [CrossRef]
- Kastrati, A.; Mehilli, J.; Dirschinger, J.; Dotzer, F.; Schühlen, H.; Neumann, F.J.; Fleckenstein, M.; Pfafferott, C.; Seyfarth, M.; Schömig, A. Intracoronary Stenting and Angiographic Results: Strut Thickness Effect on Restenosis Outcome (ISAR-STEREO) Trial. Circulation 2001, 103, 2816–2821. [Google Scholar] [CrossRef]
- Pache, J.; Kastrati, A.; Mehilli, J.; Schühlen, H.; Dotzer, F.; Hausleiter, J.; Fleckenstein, M.; Neumann, F.J.; Sattelberger, U.; Schmitt, C.; et al. Intracoronary stenting and angiographic results: Strut thickness effect on restenosis outcome (ISAR-STEREO-2) trial. J. Am. Coll. Cardiol. 2003, 41, 1283–1288. [Google Scholar] [CrossRef]
- Iglesias, J.F.; Heg, D.; Roffi, M.; Tüller, D.; Noble, S.; Muller, O.; Moarof, I.; Cook, S.; Weilenmann, D.; Kaiser, C.; et al. Long-Term Effect of Ultrathin-Strut Versus Thin-Strut Drug-Eluting Stents in Patients with Small Vessel Coronary Artery Disease Undergoing Percutaneous Coronary Intervention: A Subgroup Analysis of the BIOSCIENCE Randomized Trial. Circ. Cardiovasc. Interv. 2019, 12, e008024. [Google Scholar] [CrossRef]
- Iantorno, M.; Lipinski, M.J.; Garcia-Garcia, H.M.; Forrestal, B.J.; Rogers, T.; Gajanana, D.; Buchanan, K.D.; Torguson, R.; Weintraub, W.S.; Waksman, R. Meta-Analysis of the Impact of Strut Thickness on Outcomes in Patients with Drug-Eluting Stents in a Coronary Artery. Am. J. Cardiol. 2018, 122, 1652–1660. [Google Scholar] [PubMed]
- Joshi, A.; Allocco, D.; Joshi, A. Everolimus-eluting stents: Update on current clinical studies. Med. Devices Evid. Res. 2011, 91, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Burke, S.E.; Kuntz, R.E.; Schwartz, L.B. Zotarolimus (ABT-578) eluting stents. Adv. Drug Deliv. Rev. 2006, 58, 437–446. [Google Scholar] [PubMed]
- Nakazawa, G.; Finn, A.V.; John, M.C.; Kolodgie, F.D.; Virmani, R. The Significance of Preclinical Evaluation of Sirolimus-, Paclitaxel-, and Zotarolimus-Eluting Stents. Am. J. Cardiol. 2007, 100, S36–S44. [Google Scholar] [CrossRef]
- Choi, H.H.; Kim, J.S.; Yoon, D.H.; Hong, K.S.; Kim, T.H.; Kim, B.K.; Ko, Y.G.; Choi, D.; Jang, Y.; Hong, M.K. Favorable neointimal coverage in everolimus-eluting stent at 9 months after stent implantation: Comparison with sirolimus-eluting stent using optical coherence tomography. Int. J. Cardiovasc. Imaging. 2012, 28, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Kandzari, D.E.; Mauri, L.; Popma, J.J.; Turco, M.A.; Gurbel, P.A.; Fitzgerald, P.J.; Leon, M.B. Late-Term Clinical Outcomes with Zotarolimus- and Sirolimus-Eluting Stents. JACC Cardiovasc. Interv. 2011, 4, 543–550. [Google Scholar] [PubMed]
- Onuma, Y.; Miquel-Hebert, K.; Serruys, P.W. Five-year long-term clinical follow-up of the XIENCE V everolimus-eluting coronary stent system in the treatment of patients with de novo coronary artery disease: The SPIRIT II trial. EuroIntervention 2013, 8, 1047–1051. [Google Scholar] [CrossRef] [PubMed]
- Kelly, C.R.; Teirstein, P.S.; Meredith, I.T.; Farah, B.; Dubois, C.L.; Feldman, R.L.; Dens, J.; Hagiwara, N.; Rabinowitz, A.; Carrié, D.; et al. Long-Term Safety and Efficacy of Platinum Chromium Everolimus-Eluting Stents in Coronary Artery Disease. JACC Cardiovasc. Interv. 2017, 10, 2392–2400. [Google Scholar]
- Palmerini, T.; Sangiorgi, D.; Valgimigli, M.; Biondi-Zoccai, G.; Feres, F.; Abizaid, A.; Costa, R.A.; Hong, M.K.; Kim, B.K.; Jang, Y.; et al. Short- Versus Long-Term Dual Antiplatelet Therapy after Drug-Eluting Stent Implantation. J. Am. Coll. Cardiol. 2015, 65, 1092–1102. [Google Scholar]
- Bravo Baptista, S. The third generation of drug-eluting stents: Reassuring data while we wait for the next one. Rev. Port. Cardiol. 2021, 40, 77–80. [Google Scholar]
- Serruys, P.W.; Ruygrok, P.; Neuzner, J.; Piek, J.J.; Seth, A.; Schofer, J.J.; Richardt, G.; Wiemer, M.; Carrié, D.; Thuesen, L.; et al. A randomised comparison of an everolimus-eluting coronary stent with a paclitaxel-eluting coronary stent:the SPIRIT II trial. EuroIntervention J. Eur. Collab. Work Group Interv. Cardiol. Eur. Soc. Cardiol. 2006, 2, 286–294. [Google Scholar]
- Okkels Jensen, L.; Thayssen, P.; Hansen, H.S.; Christiansen, E.H.; Tilsted, H.H.; Krusell, L.R.; Villadsen, A.B.; Junker, A.; Hansen, K.N.; Kaltoft, A.; et al. Randomized Comparison of Everolimus-Eluting and Sirolimus-Eluting Stents in Patients Treated with Percutaneous Coronary Intervention: The Scandinavian Organization for Randomized Trials with Clinical Outcome IV (SORT OUT IV). Circulation 2012, 125, 1246–1255. [Google Scholar] [CrossRef] [PubMed]
- Saito, S.; Toelg, R.; Witzenbichler, B.; Haude, M.; Masotti, M.; Salmeron, R.; Witkowski, A.; Uematsu, M.; Takahashi, A.; Waksman, R.; et al. BIOFLOW-IV, a randomised, intercontinental, multicentre study to assess the safety and effectiveness of the Orsiro sirolimus-eluting stent in the treatment of subjects with de novo coronary artery lesions: Primary outcome target vessel failure at 12 months. EuroIntervention 2019, 15, e1006–e1013. [Google Scholar] [CrossRef] [PubMed]
- Van der Sangen, N.; Kikkert, W.J.; Henriques, J.P.; Claessen, B.E. XIENCE Implantation Followed By Short Dual Antiplatelet Therapy: ‘The New Normal’? Heart Int. 2021, 15, 65. [Google Scholar] [CrossRef] [PubMed]
- Von Birgelen, C.; Sen, H.; Lam, M.K.; Danse, P.W.; Jessurun, G.A.J.; Hautvast, R.W.M.; van Houwelingen, G.K.; Schramm, A.R.; Tjon Joe Gin, R.M.; Louwerenburg, J.W.; et al. Third-generation zotarolimus-eluting and everolimus-eluting stents in all-comer patients requiring a percutaneous coronary intervention (DUTCH PEERS): A randomised, single-blind, multicentre, non-inferiority trial. Lancet 2014, 383, 413–423. [Google Scholar] [CrossRef]
- Von Birgelen, C.; Basalus, M.W.Z.; Tandjung, K.; Van Houwelingen, K.G.; Stoel, M.G.; Louwerenburg, J.W.; Linssen, G.C.M.; Saïd, S.A.M.; Kleijne, M.A.W.J.; Sen, H.; et al. A Randomized Controlled Trial in Second-Generation Zotarolimus-Eluting Resolute Stents Versus Everolimus-Eluting Xience V Stents in Real-World Patients. J. Am. Coll. Cardiol. 2012, 59, 1350–1361. [Google Scholar] [CrossRef]
- Raungaard, B.; Jensen, L.O.; Tilsted, H.H.; Christiansen, E.H.; Maeng, M.; Terkelsen, C.J.; Krusell, L.R.; Kaltoft, A.; Kristensen, S.D.; Bøtker, H.E.; et al. Zotarolimus-eluting durable-polymer-coated stent versus a biolimus-eluting biodegradable-polymer-coated stent in unselected patients undergoing percutaneous coronary intervention (SORT OUT VI): A randomised non-inferiority trial. Lancet 2015, 385, 1527–1535. [Google Scholar]
- Yeh, R.W.; Silber, S.; Chen, L.; Chen, S.; Hiremath, S.; Neumann, F.J.; Qiao, S.; Saito, S.; Xu, B.; Yang, Y.; et al. 5-Year Safety and Efficacy of Resolute Zotarolimus-Eluting Stent. JACC Cardiovasc. Interv. 2017, 10, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Price, M.J.; Shlofmitz, R.A.; Spriggs, D.J.; Haldis, T.A.; Myers, P.; Popma Almonacid, A.; Maehara, A.; Dauler, M.; Peng, Y.; Mehran, R. Safety and efficacy of the next generation Resolute Onyx zotarolimus-eluting stent: Primary outcome of the RESOLUTE ONYX core trial. Catheter. Cardiovasc. Interv. 2018, 92, 253–259. [Google Scholar] [PubMed]
- Windecker, S.; Latib, A.; Kedhi, E.; Kirtane, A.J.; Kandzari, D.E.; Mehran, R.; Price, M.J.; Abizaid, A.; Simon, D.I.; Worthley, S.G.; et al. Polymer-based or Polymer-free Stents in Patients at High Bleeding Risk. N. Engl. J. Med. 2020, 382, 1208–1218. [Google Scholar] [CrossRef]
- Von Birgelen, C.; Kok, M.M.; van der Heijden, L.C.; Danse, P.W.; Schotborgh, C.E.; Scholte, M.; Tjon Joe Gin, R.M.; Somi, S.; van Houwelingen, K.G.; Stoel, M.G.; et al. Very thin strut biodegradable polymer everolimus-eluting and sirolimus-eluting stents versus durable polymer zotarolimus-eluting stents in allcomers with coronary artery disease (BIO-RESORT): A three-arm, randomised, non-inferiority trial. Lancet 2016, 388, 2607–2617. [Google Scholar] [CrossRef] [PubMed]
- Meredith, I.T.; Verheye, S.; Dubois, C.L.; Dens, J.; Fajadet, J.; Carrié, D.; Walsh, S.; Oldroyd, K.G.; Varenne, O.; El-Jack, S.; et al. Primary Endpoint Results of the EVOLVE Trial. J. Am. Coll. Cardiol. 2012, 59, 1362–1370. [Google Scholar] [CrossRef] [PubMed]
- Kereiakes, D.J.; Meredith, I.T.; Windecker, S.; Lee Jobe, R.; Mehta, S.R.; Sarembock, I.J.; Feldman, R.L.; Stein, B.; Dubois, C.; Grady, T.; et al. Efficacy and Safety of a Novel Bioabsorbable Polymer-Coated, Everolimus-Eluting Coronary Stent: The EVOLVE II Randomized Trial. Circ. Cardiovasc. Interv. 2015, 8, e002372. [Google Scholar] [CrossRef] [PubMed]
- Kereiakes, D.J.; Windecker, S.; Jobe, R.; Mehta, S.R.; Sarembock, I.J.; Feldman, R.; Stein, B.; Dubois, C.; Grady, T.; Saito, S.; et al. Final 5-year outcomes of the evolve ii trial: A prospective randomized investigation of a novel bioabsorbable polymer-coated, everolimus-eluting synergy stent. J. Am. Coll. Cardiol. 2019, 73, 1029. [Google Scholar] [CrossRef]
- Kirtane, A.J.; Stoler, R.; Feldman, R.; Neumann, F.J.; Boutis, L.; Tahirkheli, N.; Toelg, R.; Othman, I.; Stein, B.; Choi, J.W.; et al. Primary Results of the EVOLVE Short DAPT Study: Evaluation of 3-Month Dual Antiplatelet Therapy in High Bleeding Risk Patients Treated with a Bioabsorbable Polymer-Coated Everolimus-Eluting Stent. Circ. Cardiovasc. Interv. 2021, 14, e010144. [Google Scholar] [CrossRef]
- Sarno, G.; Lagerqvist, B.; Olivecrona, G.; Varenhorst, C.; Danielewicz, M.; Hambraeus, K.; Lindholm, D.; Råmunddal, T.; Witt, N.; James, S. Real-life clinical outcomes with everolimus eluting platinum chromium stent with an abluminal biodegradable polymer in patients from the Swedish Coronary Angiography Angioplasty Registry (SCAAR): Everolimus Bioabsorbable Polymer Stent in, S.C.A.A.R. Catheter Cardiovasc. Interv. 2017, 90, 881–887. [Google Scholar] [CrossRef]
- Pilgrim, T.; Heg, D.; Roffi, M.; Tüller, D.; Muller, O.; Vuilliomenet, A.; Cook, S.; Weilenmann, D.; Kaiser, C.; Jamshidi, P.; et al. Ultrathin strut biodegradable polymer sirolimus-eluting stent versus durable polymer everolimus-eluting stent for percutaneous coronary revascularisation (BIOSCIENCE): A randomised, single-blind, non-inferiority trial. Lancet 2014, 384, 2111–2122. [Google Scholar] [CrossRef]
- Kandzari, D.E.; Mauri, L.; Koolen, J.J.; Massaro, J.M.; Doros, G.; Garcia-Garcia, H.M.; Bennett, J.; Roguin, A.; Gharib, E.G.; Cutlip, D.E.; et al. Ultrathin, bioresorbable polymer sirolimus-eluting stents versus thin, durable polymer everolimus-eluting stents in patients undergoing coronary revascularisation (BIOFLOW V): A randomised trial. Lancet 2017, 390, 1843–1852. [Google Scholar] [CrossRef]
- Kandzari, D.E.; Koolen, J.J.; Doros, G.; Garcia-Garcia, H.M.; Bennett, J.; Roguin, A.; Gharib, E.G.; Cutlip, D.E.; Waksman, R.; BIOFLOW V Investigators. Ultrathin Bioresorbable Polymer Sirolimus-Eluting Stents Versus Durable Polymer Everolimus-Eluting Stents. JACC Cardiovasc. Interv. 2022, 15, 1852–1860. [Google Scholar] [CrossRef]
- Iglesias, J.F.; Muller, O.; Heg, D.; Roffi, M.; Kurz, D.J.; Moarof, I.; Weilenmann, D.; Kaiser, C.; Tapponnier, M.; Stortecky, S.; et al. Biodegradable polymer sirolimus-eluting stents versus durable polymer everolimus-eluting stents in patients with ST-segment elevation myocardial infarction (BIOSTEMI): A single-blind, prospective, randomised superiority trial. Lancet 2019, 394, 1243–1253. [Google Scholar] [CrossRef]
- Pilgrim, T.; Muller, O.; Heg, D.; Roffi, M.; Kurz, D.J.; Moarof, I.; Weilenmann, D.; Kaiser, C.; Tapponnier, M.; Losdat, S.; et al. Biodegradable- Versus Durable-Polymer Drug-Eluting Stents for STEMI. JACC Cardiovasc. Interv. 2021, 14, 639–648. [Google Scholar] [CrossRef] [PubMed]
- Von Birgelen, C.; Zocca, P.; Buiten, R.A.; Jessurun, G.A.J.; Schotborgh, C.E.; Roguin, A.; Danse, P.W.; Benit, E.; Aminian, A.; van Houwelingen, K.G.; et al. Thin composite wire strut, durable polymer-coated (Resolute Onyx) versus ultrathin cobalt–chromium strut, bioresorbable polymer-coated (Orsiro) drug-eluting stents in allcomers with coronary artery disease (BIONYX): An international, single-blind, randomised non-inferiority trial. Lancet 2018, 392, 1235–1245. [Google Scholar]
- Windecker, S.; Serruys, P.W.; Wandel, S.; Buszman, P.; Trznadel, S.; Linke, A.; Lenk, K.; Ischinger, T.; Klauss, V.; Eberli, F.; et al. Biolimus-eluting stent with biodegradable polymer versus sirolimus-eluting stent with durable polymer for coronary revascularisation (LEADERS): A randomised non-inferiority trial. Lancet 2008, 372, 1163–1173. [Google Scholar] [CrossRef] [PubMed]
- Serruys, P.W.; Farooq, V.; Kalesan, B.; de Vries, T.; Buszman, P.; Linke, A.; Ischinger, T.; Klauss, V.; Eberli, F.; Wijns, W.; et al. Improved Safety and Reduction in Stent Thrombosis Associated with Biodegradable Polymer-Based Biolimus-Eluting Stents Versus Durable Polymer-Based Sirolimus-Eluting Stents in Patients with Coronary Artery Disease. JACC Cardiovasc. Interv. 2013, 6, 777–789. [Google Scholar] [CrossRef]
- Maeng, M.; Christiansen, E.H.; Raungaard, B.; Kahlert, J.; Terkelsen, C.J.; Kristensen, S.D.; Carstensen, S.; Aarøe, J.; Jensen, S.E.; Villadsen, A.B.; et al. Everolimus-Eluting Versus Biolimus-Eluting Stents with Biodegradable Polymers in Unselected Patients Undergoing Percutaneous Coronary Intervention. JACC Cardiovasc. Interv. 2019, 12, 624–633. [Google Scholar] [CrossRef]
- Yoon, C.H.; Choi, Y.J.; Park, J.J.; Kang, S.H.; Kim, S.H.; Suh, J.W.; Cho, Y.S.; Youn, T.J.; Kim, M.K.; Cha, K.S.; et al. BioMatrix versus Orsiro biodegradable polymer stents in all-comer patients with coronary artery disease: The multicentre, randomised BIODEGRADE trial. EuroIntervention 2021, 16, 1404–1412. [Google Scholar] [CrossRef]
- Menown, I.B.A.; Mamas, M.A.; Cotton, J.M.; Hildick-Smith, D.; Eberli, F.R.; Leibundgut, G.; Tresukosol, D.; Macaya, C.; Copt, S.; Slama, S.S.; et al. First clinical evidence characterizing safety and efficacy of the new CoCr Biolimus-A9 eluting stent: The Biomatrix AlphaTM registry. Int. J. Cardiol. Heart Vasc. 2020, 26, 100472. [Google Scholar] [CrossRef] [PubMed]
- Saito, S.; Valdes-Chavarri, M.; Richardt, G.; Moreno, R.; Iniguez Romo, A.; Barbato, E.; Carrie, D.; Ando, K.; Merkely, B.; Kornowski, R.; et al. A randomized, prospective, intercontinental evaluation of a bioresorbable polymer sirolimus-eluting coronary stent system: The CENTURY II (Clinical Evaluation of New Terumo Drug-Eluting Coronary Stent System in the Treatment of Patients with Coronary Artery Disease) trial. Eur. Heart J. 2014, 35, 2021–2031. [Google Scholar]
- Williams, T.; Mittal, A.; Karageorgiev, D.; Iniguez Romo, A.; Aminian, A.; Fernandez Portalese, J.; Kharrat, E.; Gómez-Hospital, J.A.; Firman, D.; Trillo Nouche, R.; et al. Complete revascularization optimizes patient outcomes in multivessel coronary artery disease: Data from the e-Ultimaster registry. Catheter. Cardiovasc. Interv. 2022, 99, 961–967. [Google Scholar] [CrossRef]
- Valgimigli, M.; Frigoli, E.; Heg, D.; Tijssen, J.; Jüni, P.; Vranckx, P.; Ozaki, Y.; Morice, M.C.; Chevalier, B.; Onuma, Y.; et al. Dual Antiplatelet Therapy after PCI in Patients at High Bleeding Risk. N. Engl. J. Med. 2021, 385, 1643–1655. [Google Scholar] [CrossRef]
- Massberg, S.; Byrne, R.A.; Kastrati, A.; Schulz, S.; Pache, J.; Hausleiter, J.; Ibrahim, T.; Fusaro, M.; Ott, I.; Schömig, A.; et al. Polymer-Free Sirolimus- and Probucol-Eluting Versus New Generation Zotarolimus-Eluting Stents in Coronary Artery Disease: The Intracoronary Stenting and Angiographic Results: Test Efficacy of Sirolimus- and Probucol-Eluting Versus Zotarolimus-Eluting Stents (ISAR-TEST 5) Trial. Circulation 2011, 124, 624–632. [Google Scholar]
- Kufner, S.; Ernst, M.; Cassese, S.; Joner, M.; Mayer, K.; Colleran, R.; Koppara, T.; Xhepa, E.; Koch, T.; Wiebe, J.; et al. 10-Year Outcomes From a Randomized Trial of Polymer-Free Versus Durable Polymer Drug-Eluting Coronary Stents. J. Am. Coll. Cardiol. 2020, 76, 146–158. [Google Scholar] [CrossRef]
- Mahmood Zuhdi, A.S.; Krackhardt, F.; Waliszewski, M.W.; Ismail, M.D.; Boxberger, M.; Wan Ahmad, W.A. Efficacy and Safety of Polymer-Free Ultrathin Strut Sirolimus-Probucol Coated Drug-Eluting Stents for Chronic Total Occlusions: Insights from the Coroflex® ISAR 2000 Worldwide Registry. Cardiol. Res. Pract. 2018, 2018, 8053168. [Google Scholar] [CrossRef] [PubMed]
- Urban, P.; Meredith, I.T.; Abizaid, A.; Pocock, S.J.; Carrié, D.; Naber, C.; Lipiecki, J.; Richardt, G.; Iñiguez, A.; Brunel, P.; et al. Polymer-free Drug-Coated Coronary Stents in Patients at High Bleeding Risk. N. Engl. J. Med. 2015, 373, 2038–2047. [Google Scholar] [CrossRef] [PubMed]
- Jensen, L.O.; Maeng, M.; Raungaard, B.; Kahlert, J.; Ellert, J.; Jakobsen, L.; Villadsen, A.B.; Veien, K.T.; Kristensen, S.D.; Ahlehoff, O.; et al. Randomized Comparison of the Polymer-Free Biolimus-Coated Biofreedom Stent with the Ultrathin Strut Biodegradable Polymer Sirolimus-Eluting Orsiro Stent in an All-Comers Population Treated With Percutaneous Coronary Intervention: The SORT OUT IX Trial. Circulation 2020, 141, 2052–2063. [Google Scholar]
- Sabaté, M.; Okkels Jensen, L.; Tilsted, H.H.; Moreno, R.; García Del Blanco, B.; Macaya, C.; Pérez de Prado, A.; Cequier, À.; Pérez-Fuentes, P.; Schütte, D.; et al. Thin- versus thick-strut polymer-free biolimus-eluting stents: The Biofreedom QCA randomised trial. EuroIntervention 2021, 17, 233–239. [Google Scholar] [CrossRef]
- Oberhauser, J.P.; Hossainy, S.; Rapoza, R.J. Design principles and performance of bioresorbable polymeric vascular scaffolds. EuroIntervention 2009, 5, F15–F22. [Google Scholar] [CrossRef] [PubMed]
- Waksman, R. Biodegradable stents: They do their job and disappear. J. Invasive Cardiol. 2006, 18, 70–74. [Google Scholar]
- Gogas, B.D. Bioresorbable scaffolds for percutaneous coronary interventions. Glob. Cardiol. Sci. Pract. 2014, 2014, 55. [Google Scholar] [CrossRef]
- Jeżewski, M.P.; Kubisa, M.J.; Eyileten, C.; De Rosa, S.; Christ, G.; Lesiak, M.; Indolfi, C.; Toma, A.; Siller-Matula, J.M.; Postuła, M. Bioresorbable Vascular Scaffolds—Dead End or Still a Rough Diamond? J. Clin. Med. 2019, 8, 2167. [Google Scholar] [CrossRef]
- Otsuka, F.; Pacheco, E.; Perkins, L.E.L.; Lane, J.P.; Wang, Q.; Kamberi, M.; Frie, M.; Wang, J.; Sakakura, K.; Yahagi, K.; et al. Long-Term Safety of an Everolimus-Eluting Bioresorbable Vascular Scaffold and the Cobalt-Chromium XIENCE V Stent in a Porcine Coronary Artery Model. Circ. Cardiovasc. Interv. 2014, 7, 330–342. [Google Scholar] [CrossRef]
- Garcia-Garcia, H.M.; Haude, M.; Kuku, K.; Hideo-Kajita, A.; Ince, H.; Abizaid, A.; Tölg, R.; Lemos, P.A.; von Birgelen, C.; Christiansen, E.H.; et al. In vivo serial invasive imaging of the second-generation drug-eluting absorbable metal scaffold (Magmaris—DREAMS 2G) in de novo coronary lesions: Insights from the BIOSOLVE-II First-In-Man Trial. Int. J. Cardiol. 2018, 255, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Wykrzykowska, J.J.; Kraak, R.P.; Hofma, S.H.; Van Der Schaaf, R.J.; Arkenbout, E.K.; IJsselmuiden, A.J.; Elias, J.; van Dongen, I.M.; Tijssen, R.Y.G.; Koch, K.T.; et al. Bioresorbable Scaffolds versus Metallic Stents in Routine, P.C.I. N. Engl. J. Med. 2017, 376, 2319–2328. [Google Scholar] [CrossRef]
- Kereiakes, D.J.; Ellis, S.G.; Metzger, C.; Caputo, R.P.; Rizik, D.G.; Teirstein, P.S.; Litt, M.R.; Kini, A.; Kabour, A.; Marx, S.O.; et al. 3-Year Clinical Outcomes with Everolimus-Eluting Bioresorbable Coronary Scaffolds. J. Am. Coll. Cardiol. 2017, 70, 2852–2862. [Google Scholar] [CrossRef]
- De Pommereau, A.; De Hemptinne, Q.; Varenne, O.; Picard, F. Bioresorbable vascular scaffolds: Time to absorb past lessons or fade away? Arch. Cardiovasc. Dis. 2018, 111, 229–232. [Google Scholar] [CrossRef]
- Cherian, A.M.; Nair, S.V.; Maniyal, V.; Menon, D. Surface engineering at the nanoscale: A way forward to improve coronary stent efficacy. APL Bioeng. 2021, 5, 021508. [Google Scholar] [CrossRef] [PubMed]
- Vishnu, J.; Manivasagam, G. Perspectives on smart stents with sensors: From conventional permanent to novel bioabsorbable smart stent technologies. Med. Devices Sens. 2020, 3, e10116. [Google Scholar] [CrossRef]
- Bassous, N.; Cooke, J.P.; Webster, T.J. Enhancing Stent Effectiveness with Nanofeatures. Methodist DeBakey Cardiovasc. J. 2016, 12, 163. [Google Scholar] [CrossRef]
- Lee, D.H.; de la Torre Hernandez, J.M. Cardiology Service, Interventional Cardiology Unit, University Hospital Marques de Valdecilla, Santander, Spain. The Newest Generation of Drug-eluting Stents and Beyond. Eur. Cardiol. Rev. 2018, 13, 54. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
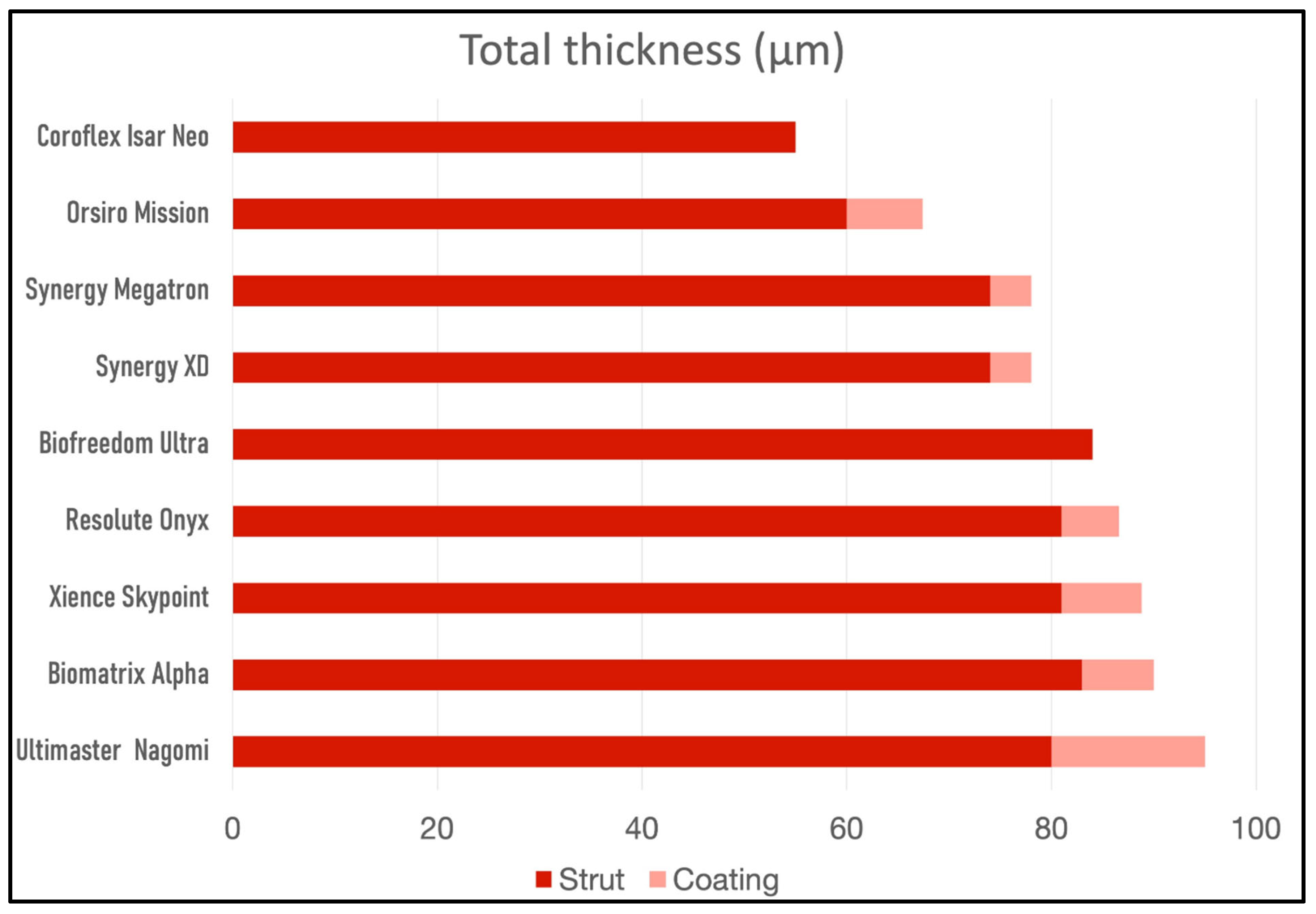
| Stent Platform | Synergy XD™ | Synergy Megatron™ | Xience Skypoint™ | Orsiro® Mission | Resolute Onyx™ | Biomatrix Alpha | Ultimaster Nagomi™ | Coroflex® Isar Neo | Biofreedom Ultra™ |
|---|---|---|---|---|---|---|---|---|---|
| Metal alloy | platinum–chromium | platinum–chromium | cobalt–chromium | cobalt–chromium | cobalt–chromium | cobalt–chromium | cobalt–chromium | cobalt–chromium | cobalt–chromium |
| Active drug | everolimus | everolimus | everolimus | sirolimus | zotarolimus | biolimus A9 | sirolimus | Sirolimus /probucol | biolimus A9 |
| Strut thickness | Ø 2.25–2.75: 74 µm Ø 3.0–3.5: 79 µm Ø 4.0–5.0: 81 µm | 89 µm | 81 µm | Ø ≤ 3.0: 60 µm Ø ≥ 3.5: 80 µm | 81 µm | 83 µm | 80 µm | Ø ≤ 3.0: 55 µm Ø ≥ 3.5: 65 µm | Ø ≤ 3.0: 84 µm Ø ≥ 3.5: 88 µm |
| Polymer composition | PLGA | PLGA | Fluorinated Copolymer | Poly-L-lactic Acid | BioLinx™ | Polylactic Acid | PDLLA | na | na |
| Polymer type | Biodegradable | Biodegradable | Durable | Biodegradable | Durable | Biodegradable | Biodegradable | No polymer | No polymer |
| Polymer thickness | 4 µm | 4 µm | 7.8 μm | 3.5 µm (abluminal) 7.4 µm (rest) | 5.6 µm | 8–11 µm | 15 µm | na | na |
| Polymer degradation delay | 4 months | 4 months | na | 12–24 months | na | 6–9 months | 3–4 months | na | na |
| Coating | Abluminal | Abluminal | Circumferential | Circumferential | Circumferential | Abluminal | Abluminal | Abluminal | Abluminal |
| Stent expansion capacity | Ø 2.25–2.75: 3.5 mm Ø 3.0–3.5: 4.25 mm Ø ≥ 4.0: 5.75 mm | Ø ≥ 3.5: 6.0 mm | Ø ≤ 3.0: 3.75 mm Ø ≥ 3.5: 5.75 mm | Ø ≤ 3.0: 3.5 mm Ø ≥ 3.5: 4.5 mm | Ø 2.25–2.5: 3.5 mm Ø 2.75–3.0: 4.0 mm Ø 3.5–4.0: 5.0 mm Ø 4.5–5.0: 6.0 mm | Ø ≤ 3.0: 3.5 mm Ø ≥ 3.5: 4.5 mm | Ø ≤ 2.5: 3.5 mm Ø 2.75–3.0: 4.5 mm Ø ≥ 3.5: 6.25 mm | Ø ≤ 3.0: 3.5 mm Ø ≥ 3.5: 4.5 mm | Ø ≤ 3.0: 4.76 mm Ø ≥ 3.5: 5.95 mm |
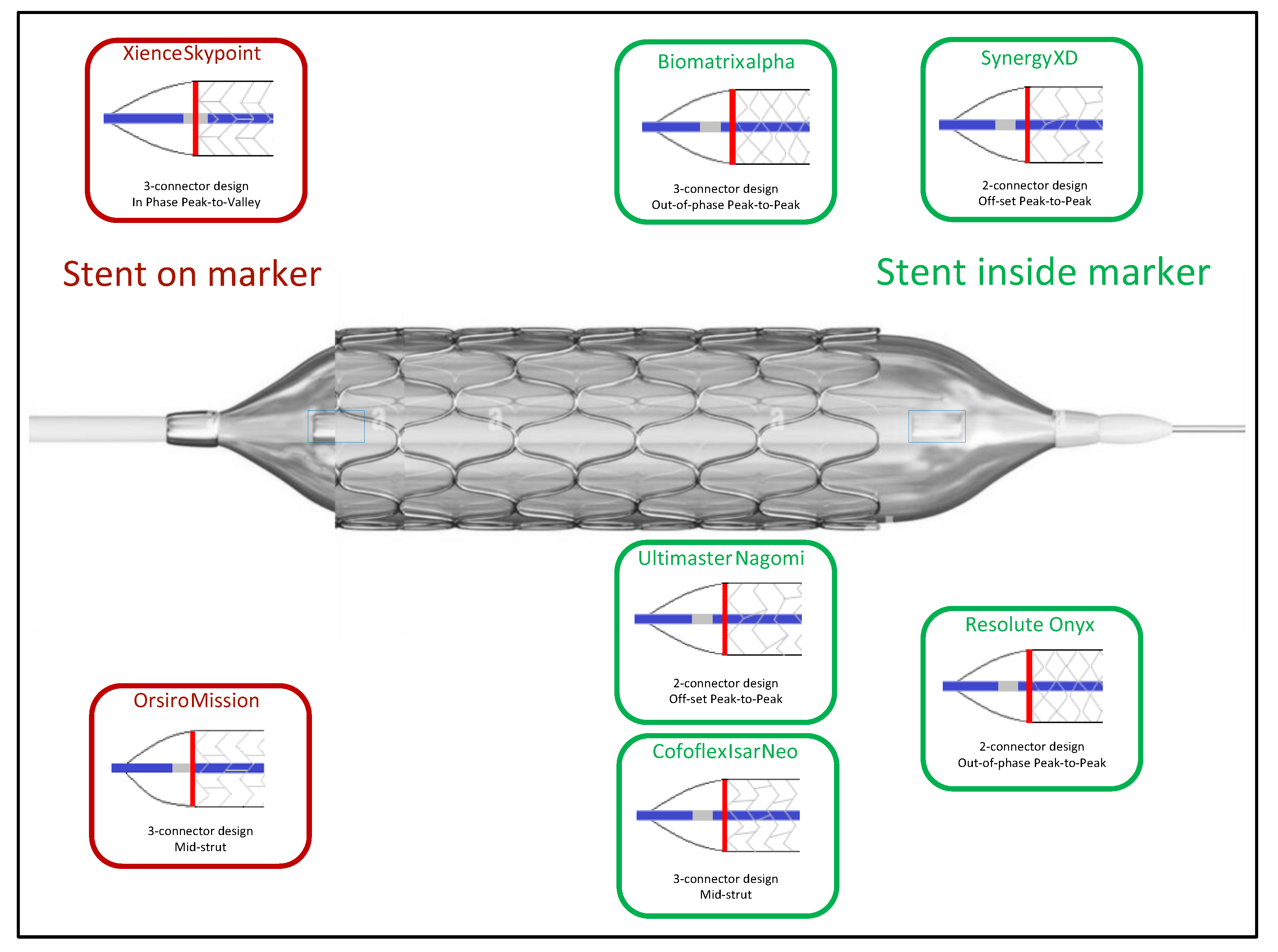
| Radiopaque Marker position |  |  |  |  |  |  |  |  |  |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brami, P.; Fischer, Q.; Pham, V.; Seret, G.; Varenne, O.; Picard, F. Evolution of Coronary Stent Platforms: A Brief Overview of Currently Used Drug-Eluting Stents. J. Clin. Med. 2023, 12, 6711. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12216711
Brami P, Fischer Q, Pham V, Seret G, Varenne O, Picard F. Evolution of Coronary Stent Platforms: A Brief Overview of Currently Used Drug-Eluting Stents. Journal of Clinical Medicine. 2023; 12(21):6711. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12216711
Chicago/Turabian StyleBrami, Pierre, Quentin Fischer, Vincent Pham, Gabriel Seret, Olivier Varenne, and Fabien Picard. 2023. "Evolution of Coronary Stent Platforms: A Brief Overview of Currently Used Drug-Eluting Stents" Journal of Clinical Medicine 12, no. 21: 6711. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12216711