
Placenta Accreta Spectrum Prophylactic Therapy for Hyperfibrinolysis with Tranexamic Acid

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Planned EM, Failed
3.2. Planned EM, Successful
3.3. Uplanned EM, Successful
3.4. Follow-Up during EM (n = 25)
3.5. Hyperfibrinolysis Management
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Poder, L.; Weinstein, S.; Maturen, K.E.; Feldstein, V.A.; Mackenzie, D.C.; Oliver, E.R.; Shipp, T.D.; Strachowski, L.M.; Sussman, B.L.; Wang, E.Y.; et al. ACR Appropriateness Criteria® Placenta Accreta Spectrum Disorder. J. Am. Coll. Radiol. 2020, 17, S207–S214. [Google Scholar] [CrossRef] [PubMed]
- Sentilhes, L.; Kayem, G.; Chandraharan, E.; Palacios-Jaraquemada, J.; Jauniaux, E. FIGO Placenta Accreta Diagnosis and Management Expert Consensus Panel FIGO Consensus Guidelines on Placenta Accreta Spectrum Disorders: Conservative Management. Int. J. Gynecol. Obstet. 2018, 140, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Silver, R.M.; Barbour, K.D. Placenta Accreta Spectrum. Obstet. Gynecol. Clin. N. Am. 2015, 42, 381–402. [Google Scholar] [CrossRef] [PubMed]
- Jauniaux, E.; Chantraine, F.; Silver, R.M.; Langhoff-Roos, J. FIGO Placenta Accreta Diagnosis and Management Expert Consensus Panel FIGO Consensus Guidelines on Placenta Accreta Spectrum Disorders: Epidemiology. Int. J. Gynecol. Obstet. 2018, 140, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Jauniaux, E.; Collins, S.; Burton, G.J. Placenta Accreta Spectrum: Pathophysiology and Evidence-Based Anatomy for Prenatal Ultrasound Imaging. Am. J. Obstet. Gynecol. 2018, 218, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Jauniaux, E.; Jurkovic, D. Placenta Accreta: Pathogenesis of a 20th Century Iatrogenic Uterine Disease. Placenta 2012, 33, 244–251. [Google Scholar] [CrossRef]
- Parra-Herran, C.; Djordjevic, B. Histopathology of Placenta Creta: Chorionic Villi Intrusion into Myometrial Vascular Spaces and Extravillous Trophoblast Proliferation Are Frequent and Specific Findings with Implications for Diagnosis and Pathogenesis. Int. J. Gynecol. Pathol. 2016, 35, 497–508. [Google Scholar] [CrossRef]
- Jauniaux, E.; Alfirevic, Z.; Bhide, A.; Belfort, M.; Burton, G.; Collins, S.; Dornan, S.; Jurkovic, D.; Kayem, G.; Kingdom, J.; et al. Placenta Praevia and Placenta Accreta: Diagnosis and Management: Green-top Guideline No. 27a. BJOG 2019, 126, E1–E48. [Google Scholar] [CrossRef]
- Eshkoli, T.; Weintraub, A.Y.; Sergienko, R.; Sheiner, E. Placenta Accreta: Risk Factors, Perinatal Outcomes, and Consequences for Subsequent Births. Am. J. Obstet. Gynecol. 2013, 208, 219.e1–219.e7. [Google Scholar] [CrossRef]
- Solheim, K.N.; Esakoff, T.F.; Little, S.E.; Cheng, Y.W.; Sparks, T.N.; Caughey, A.B. The Effect of Cesarean Delivery Rates on the Future Incidence of Placenta Previa, Placenta Accreta, and Maternal Mortality. J. Matern.-Fetal Neonatal Med. 2011, 24, 1341–1346. [Google Scholar] [CrossRef]
- Nikolajsen, S.; Løkkegaard, E.C.L.; Bergholt, T. Reoccurrence of Retained Placenta at Vaginal Delivery: An Observational Study. Acta Obstet. Gynecol. Scand. 2013, 92, 421–425. [Google Scholar] [CrossRef] [PubMed]
- Cahill, A.G.; Beigi, R.; Heine, R.P.; Silver, R.M.; Wax, J.R. Placenta Accreta Spectrum. Am. J. Obstet. Gynecol. 2018, 219, B2–B16. [Google Scholar] [CrossRef] [PubMed]
- Sandall, J.; Tribe, R.M.; Avery, L.; Mola, G.; Visser, G.H.; Homer, C.S.; Gibbons, D.; Kelly, N.M.; Kennedy, H.P.; Kidanto, H.; et al. Short-Term and Long-Term Effects of Caesarean Section on the Health of Women and Children. Lancet 2018, 392, 1349–1357. [Google Scholar] [CrossRef] [PubMed]
- Silver, R.M.; Landon, M.B.; Rouse, D.J.; Leveno, K.J.; Spong, C.Y.; Thom, E.A.; Moawad, A.H.; Caritis, S.N.; Harper, M.; Wapner, R.J.; et al. Maternal Morbidity Associated With Multiple Repeat Cesarean Deliveries. Obstet. Gynecol. 2006, 107, 1226–1232. [Google Scholar] [CrossRef] [PubMed]
- Fox, K.A.; Shamshirsaz, A.A.; Carusi, D.; Secord, A.A.; Lee, P.; Turan, O.M.; Huls, C.; Abuhamad, A.; Simhan, H.; Barton, J.; et al. Conservative Management of Morbidly Adherent Placenta: Expert Review. Am. J. Obstet. Gynecol. 2015, 213, 755–760. [Google Scholar] [CrossRef]
- Kingdom, J.C.; Hobson, S.R.; Murji, A.; Allen, L.; Windrim, R.C.; Lockhart, E.; Collins, S.L.; Soleymani Majd, H.; Alazzam, M.; Naaisa, F.; et al. Minimizing Surgical Blood Loss at Cesarean Hysterectomy for Placenta Previa with Evidence of Placenta Increta or Placenta Percreta: The State of Play in 2020. Am. J. Obstet. Gynecol. 2020, 223, 322–329. [Google Scholar] [CrossRef]
- Allen, L.; Jauniaux, E.; Hobson, S.; Papillon-Smith, J.; Belfort, M.A.; Tikkanen, M. FIGO Placenta Accreta Diagnosis and Management Expert Consensus Panel FIGO Consensus Guidelines on Placenta Accreta Spectrum Disorders: Nonconservative Surgical Management. Int. J. Gynecol. Obstet. 2018, 140, 281–290. [Google Scholar] [CrossRef]
- Tan, S.G.; Jobling, T.W.; Wallace, E.M.; Mcneilage, L.J.; Manolitsas, T.; Hodges, R.J. Surgical Management of Placenta Accreta: A 10-year Experience. Acta Obstet. Gynecol. Scand. 2013, 92, 445–450. [Google Scholar] [CrossRef]
- Sentilhes, L.; Goffinet, F.; Kayem, G. Management of Placenta Accreta. Acta Obstet. Gynecol. Scand. 2013, 92, 1125–1134. [Google Scholar] [CrossRef]
- Fitzpatrick, K.; Sellers, S.; Spark, P.; Kurinczuk, J.; Brocklehurst, P.; Knight, M. The Management and Outcomes of Placenta Accreta, Increta, and Percreta in the UK : A Population-based Descriptive Study. BJOG 2014, 121, 62–71. [Google Scholar] [CrossRef]
- Kayem, G.; Davy, C.; Goffinet, F.; Thomas, C.; Clément, D.; Cabrol, D. Conservative Versus Extirpative Management in Cases of Placenta Accreta. Obstet. Gynecol. 2004, 104, 531–536. [Google Scholar] [CrossRef] [PubMed]
- Timmermans, S.; Van Hof, A.C.; Duvekot, J.J. Conservative Management of Abnormally Invasive Placentation. Obstet. Gynecol. Surv. 2007, 62, 529–539. [Google Scholar] [CrossRef] [PubMed]
- Sentilhes, L.; Ambroselli, C.; Kayem, G.; Provansal, M.; Fernandez, H.; Perrotin, F.; Winer, N.; Pierre, F.; Benachi, A.; Dreyfus, M.; et al. Maternal Outcome After Conservative Treatment of Placenta Accreta. Obstet. Gynecol. 2010, 115, 526–534. [Google Scholar] [CrossRef] [PubMed]
- Sentilhes, L.; Kayem, G.; Ambroselli, C.; Provansal, M.; Fernandez, H.; Perrotin, F.; Winer, N.; Pierre, F.; Benachi, A.; Dreyfus, M.; et al. Fertility and Pregnancy Outcomes Following Conservative Treatment for Placenta Accreta. Hum. Reprod. 2010, 25, 2803–2810. [Google Scholar] [CrossRef] [PubMed]
- Clausen, C.; Lönn, L.; Langhoff-Roos, J. Management of Placenta Percreta: A Review of Published Cases. Acta Obstet. Gynecol. Scand. 2014, 93, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Pather, S.; Strockyj, S.; Richards, A.; Campbell, N.; De Vries, B.; Ogle, R. Maternal Outcome after Conservative Management of Placenta Percreta at Caesarean Section: A Report of Three Cases and a Review of the Literature. Aust. N. Z. J. Obstet. Gynaecol. 2014, 54, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Kayem, G.; Deneux-Tharaux, C.; Sentilhes, L. The PACCRETA group PACCRETA: Clinical Situations at High Risk of Placenta ACCRETA/Percreta: Impact of Diagnostic Methods and Management on Maternal Morbidity. Acta Obstet. Gynecol. Scand. 2013, 92, 476–482. [Google Scholar] [CrossRef]
- Bretelle, F.; Courbière, B.; Mazouni, C.; Agostini, A.; Cravello, L.; Boubli, L.; Gamerre, M.; D’Ercole, C. Management of Placenta Accreta: Morbidity and Outcome. Eur. J. Obstet. Gynecol. Reprod. Biol. 2007, 133, 34–39. [Google Scholar] [CrossRef]
- Matsuzaki, S.; Yoshino, K.; Endo, M.; Tomimatsu, T.; Takiuchi, T.; Mimura, K.; Kumasawa, K.; Ueda, Y.; Kimura, T. Successful Anticoagulant Therapy for Disseminated Intravascular Coagulation during Conservative Management of Placenta Percreta: A Case Report and Literature Review. BMC Pregnancy Childbirth 2017, 17, 443. [Google Scholar] [CrossRef]
- Biele, C.; Kaufner, L.; Schwickert, A.; Nonnenmacher, A.; Von Weizsäcker, K.; Muallem, M.Z.; Henrich, W.; Braun, T. Conservative Management of Abnormally Invasive Placenta Complicated by Local Hyperfibrinolysis and Beginning Disseminated Intravascular Coagulation. Arch. Gynecol. Obstet. 2021, 303, 61–68. [Google Scholar] [CrossRef]
- Schröder, L.; Pötzsch, B.; Rühl, H.; Gembruch, U.; Merz, W.M. Tranexamic Acid for Hyperfibrinolytic Hemorrhage During Conservative Management of Placenta Percreta. Obstet. Gynecol. 2015, 126, 1012–1015. [Google Scholar] [CrossRef] [PubMed]
- Levi, M.; Ten Cate, H. Disseminated Intravascular Coagulation. N. Engl. J. Med. 1999, 341, 586–592. [Google Scholar] [CrossRef] [PubMed]
- McCormack, P.L. Tranexamic Acid: A Review of Its Use in the Treatment of Hyperfibrinolysis. Drugs 2012, 72, 585–617. [Google Scholar] [CrossRef] [PubMed]
- Welz, J.; Keyver-Paik, M.-D.; Gembruch, U.; Merz, W.M. Self-Reported Physical, Mental, and Reproductive Sequelae after Treatment of Abnormally Invasive Placenta: A Single-Center Observational Study. Arch. Gynecol. Obstet. 2019, 300, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Merz, W.; Van De Vondel, P.; Strunk, H.; Geipel, A.; Gembruch, U. Diagnosis, Treatment and Application of Color Doppler in Conservative Management of Abnormally Adherent Placenta. Ultraschall Med. 2008, 30, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Jauniaux, E.; D’Antonio, F.; Bhide, A.; Prefumo, F.; Silver, R.M.; Hussein, A.M.; Shainker, S.A.; Chantraine, F.; Alfirevic, Z. Delphi consensus expert panel Modified Delphi Study of Ultrasound Signs Associated with Placenta Accreta Spectrum. Ultrasound Obstet. Gynecol. 2023, 61, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Comstock, C.H. Antenatal Diagnosis of Placenta Accreta: A Review: Antenatal Diagnosis of Placenta Accreta. Ultrasound Obstet. Gynecol. 2005, 26, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Collins, S.L.; Ashcroft, A.; Braun, T.; Calda, P.; Langhoff-Roos, J.; Morel, O.; Stefanovic, V.; Tutschek, B.; Chantraine, F.; on behalf of the European Working Group on Abnormally Invasive Placenta (EW-AIP). Proposal for Standardized Ultrasound Descriptors of Abnormally Invasive Placenta (AIP). Ultrasound Obstet. Gynecol. 2016, 47, 271–275. [Google Scholar] [CrossRef]
- Shukunami, K.; Hattori, K.; Nishijima, K.; Kotsuji, F. Transverse Fundal Uterine Incision in a Patient with Placenta Increta. J. Matern.-Fetal Neonatal Med. 2004, 16, 355–356. [Google Scholar] [CrossRef]
- Matsubara, S. Measures for Peripartum Hysterectomy for Placenta Previa Accreta: Avoiding Uterotonic Agents and “Double Distal Edge Pickup” Mass Ligation. Arch. Gynecol. Obstet. 2012, 285, 1765–1767. [Google Scholar] [CrossRef]
- Youssefzadeh, A.C.; Matsuzaki, S.; Mandelbaum, R.S.; Sangara, R.N.; Bainvoll, L.; Matsushima, K.; Ouzounian, J.G.; Matsuo, K. Trends, Characteristics, and Outcomes of Conservative Management for Placenta Percreta. Arch. Gynecol. Obstet. 2022, 306, 913–920. [Google Scholar] [CrossRef] [PubMed]
- Van Beekhuizen, H.J.; Stefanovic, V.; Schwickert, A.; Henrich, W.; Fox, K.A.; MHallem Gziri, M.; Sentilhes, L.; Gronbeck, L.; Chantraine, F.; Morel, O.; et al. A Multicenter Observational Survey of Management Strategies in 442 Pregnancies with Suspected Placenta Accreta Spectrum. Acta Obstet. Gynecol. Scand. 2021, 100, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Judy, A.E.; Lyell, D.J.; Druzin, M.L.; Dorigo, O. Disseminated Intravascular Coagulation Complicating the Conservative Management of Placenta Percreta. Obstet. Gynecol. 2015, 126, 1016–1018. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total number of patients | 35 |
| Maternal age, mean (range) | 32.8 (21–41) |
| Gravidity, mean (range) | 3.6 (1–13) |
| Parity, mean (range) | 2.2 (0–11) |
| Timing of diagnosis, n (%) | |
| antepartum | 32/35 (91.4%) |
| Intrapartum | 3/35 (8.6%) |
| Type of PAS | |
| increta | 17/35 (48.6%) |
| percreta | 14/35 (40%) |
| increta/percreta and membranacea | 4/35 (11.4%) |
| Placenta previa in current pregnancy | 26/35 (74.3%) |
| total | 24/35 (68.6%) |
| Partial | 2/35 (5.7%) |
| GA at diagnosis (weeks), mean (range) | 28 + 4 (9 + 2–36 + 3) |
| GA at delivery (weeks), mean (range) | 35 + 0 (27 + 2–37 + 1) |
| Risk factors, n (%) (multiple risk factors possible) | |
| Previous CS | 30/35 (85.7%) |
| 1 CS | 18/30 (60%) |
| 2 CS | 5/30 (16.7%) |
| 3 CS | 3/30 (10%) |
| >3 CS | 4/30 (13.3%) |
| Number of patients without previous CS | 5/35 (14.3%) |
| Curettages | 2/5 (40%) |
| Placenta previa in current pregnancy | 1/5 (20%) |
| History of placenta increta | 1/5 (20%) |
| Smoking | 1/5 (20%) |
| Curettages (number of curettages) | 11(1–5)/35 (31.4%) |
| Uterus bicornis/arcuatus | 3/35 (8.6%) |
| History of endomyometritis | 1/35 (2.9%) |
| Asherman syndrome | 1/35 (2.9%) |
| History of intrauterine device | 1/35 (2.9%) |
| History of placenta increta | 2/35 (5.7%) |
| Assisted reproduction by IVF/ICSI | 2/35 (5.7%) |
| Smoking | 4/35 (11.4%) |
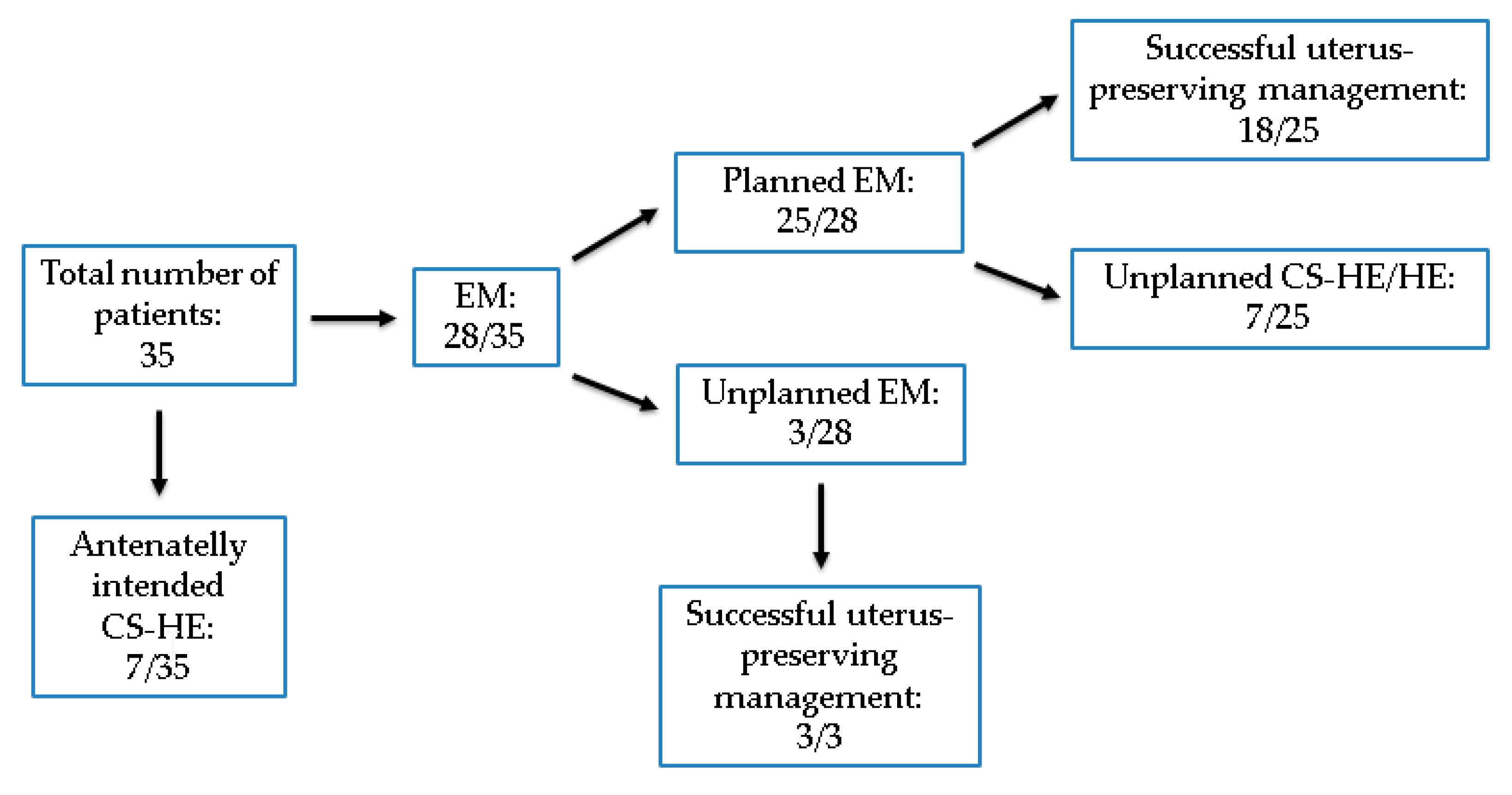
| EM | 28/35 (80%) |
| Planned EM | 25/28 (89%) |
| Intrapartum diagnosis (unplanned), managed with EM | 3/28 (11%) |
| Successful uterus-preserving management | 21/35 (60%) |
| Successful uterus-preserving management in planned EM | 18/25 (72%) |
| Antenataelly intended CS-HE | 7/35 (20%) |
| Unplanned CS-HE/HE | 7/25 (28%) |
| EM n (%) | 28 |
| Mean duration of EM (days) | 107 (8–589) |
| Planned EM | 25/28 (89.3%) |
| Complete placental absorption | 2/25 (8%) |
| Planned curettage | 14/25 (56%) |
| Emergency curettage due to bleeding | 1/25 (4%) |
| Intraoperative placental detachment, complete removal during CS | 2/25 (8%) |
| HE | 7/25 (28%) |
| HE during CS | 1/25 (4%) |
| Unplanned HE | 4/25 (16%) |
| Planned HE | 2/25 (8%) |
| Unplanned EM (one vaginal delivery, one operative vagianal delivery, one CS) | 3/28 (10.7%) |
| Complete placental absorption | 3/3 (100%) |
| Complications following planned EM, n (%) (multiple possible) | 25 |
| Abnormal coagulation screening | 11/25 (44%) |
| Infection | 11/25 (44%) |
| Abdominal pain | 6/25 (24%) |
| Nausea | 1/25 (4%) |
| Gingival bleeding | 1/25 (4%) |
| Dysuria | 1/25 (4%) |
| Blood transfusions (2–26 units) | 11/25 (44%) |
| During HE (8–26 units) | 5/7 (71.4%) |
| During curettage (2–11 units) | 4/14 (28.6%) |
| During CS (4 units) | 2/2 (100%) |
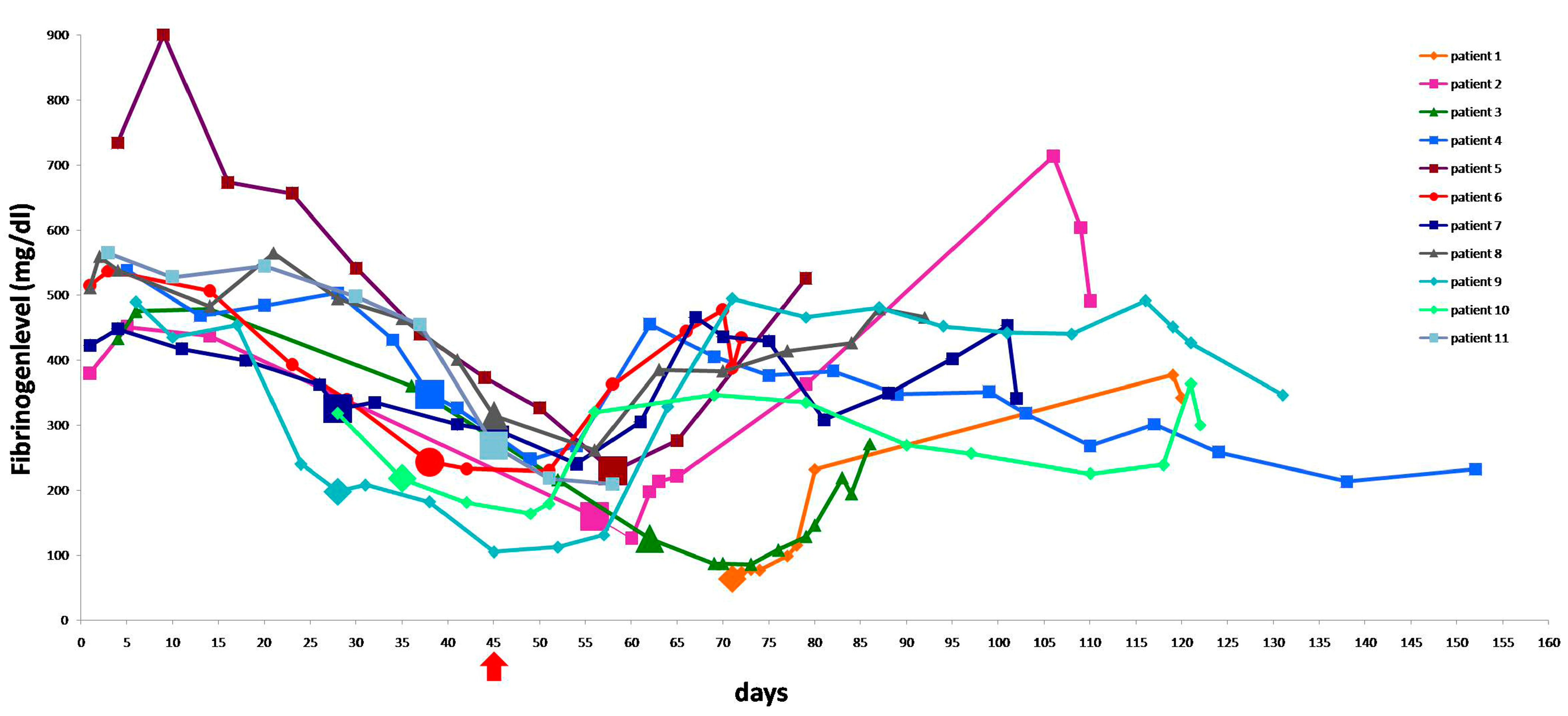
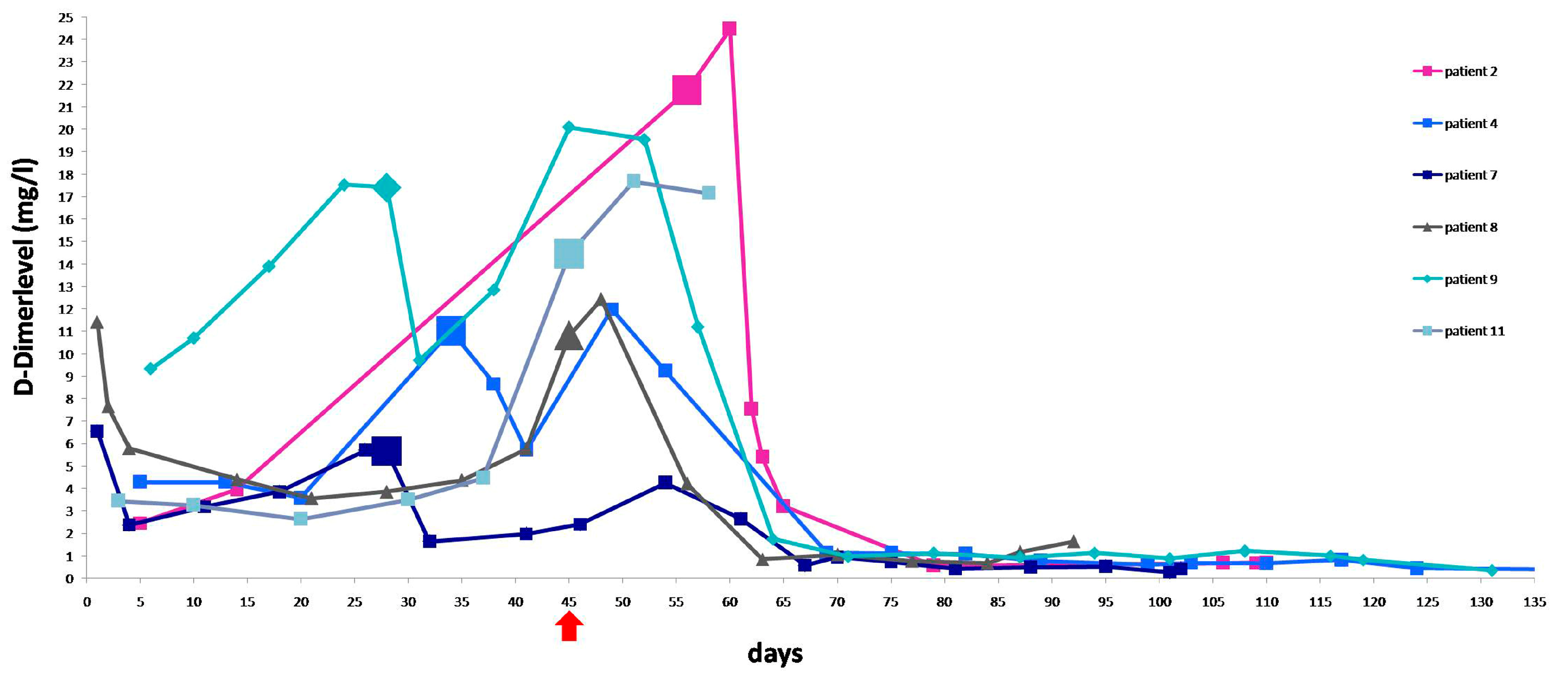
| Pat. | Start of TXA (Day) | Fibrinogen (mg/dL) at Start of TXA (Previous Value), Normal Range 180–355 mg/dL | D-Dimer (mg/L) at Start of TXA (Previous Value), Normal Range: 0–0.5 mg/L | Therapy Outcome | Duration of EM (Days) |
|---|---|---|---|---|---|
| 1 | 71 | 64 (ND) | ND | Curettage | 119 |
| 2 | 56 | 159 (437) | 21.75 (3.9) | Curettage | 109 |
| 3 | 52 | 216 (360) | ND | HE due to infection and perforation with injury of bladder during curettage (24 PRC transfusion) | 86 |
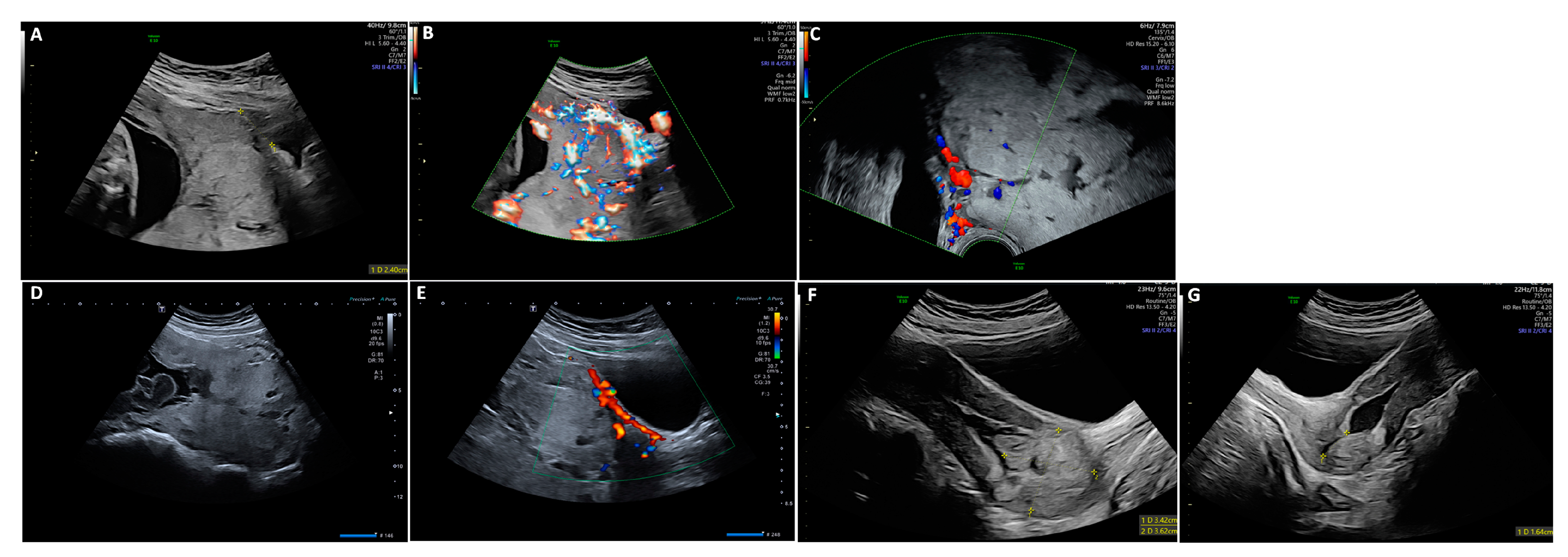
| 4 | 34 | 431 (503) | 11.02 (3.6) | Complete absorption (Figure 1) | 152 |
| 5 | 58 | 229 (326) | ND | Curettage | 82 |
| 6 | 38 | 243 (339) | ND | Curettage, laparotomy due to perforation and injury of bladder without HE | 71 |
| 7 | 28 | 325 (362) | 5.66 (3.86) | Curettage (two PRC transfusion) | 102 |
| 8 | 45 | 315 (401) | 10.83 (5.77) | Curettage | 91 |
| 9 | 28 | 198 (240) | 17.41 (13.89) | Curettage, but residual placenta | 116 |
| 10 | 35 | 218 (318) | ND | Elective HE due to large area of placenta previa et percreta near the cervix | 121 |
| 11 | 45 | 268 (454) | 14.45 (4.46) | Elective HE due to completed family planning | 59 |
| Mean | 45 (28–71) | 242.4 (64–431) mean % drop: 29.7% | 13.5 (5.7–21.7) mean % rise: 273.7% | 101 (59–152) |
| Suggested Follow Up |
|---|
| Weekly follow-up in the first two month, thereafter every two-four weeks |
| Clinical examination |
| Ultrasound |
| Laboratory tests |
| (for detailed algorithm for coagulation screening we refer to Schröder et al., 2015 [31]) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ayub, T.H.; Strizek, B.; Poetzsch, B.; Kosian, P.; Gembruch, U.; Merz, W.M. Placenta Accreta Spectrum Prophylactic Therapy for Hyperfibrinolysis with Tranexamic Acid. J. Clin. Med. 2024, 13, 135. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13010135
Ayub TH, Strizek B, Poetzsch B, Kosian P, Gembruch U, Merz WM. Placenta Accreta Spectrum Prophylactic Therapy for Hyperfibrinolysis with Tranexamic Acid. Journal of Clinical Medicine. 2024; 13(1):135. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13010135
Chicago/Turabian StyleAyub, Tiyasha Hosne, Brigitte Strizek, Bernd Poetzsch, Philipp Kosian, Ulrich Gembruch, and Waltraut M. Merz. 2024. "Placenta Accreta Spectrum Prophylactic Therapy for Hyperfibrinolysis with Tranexamic Acid" Journal of Clinical Medicine 13, no. 1: 135. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13010135