The Effect of Gamification through a Virtual Reality on Preoperative Anxiety in Pediatric Patients Undergoing General Anesthesia: A Prospective, Randomized, and Controlled Trial

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
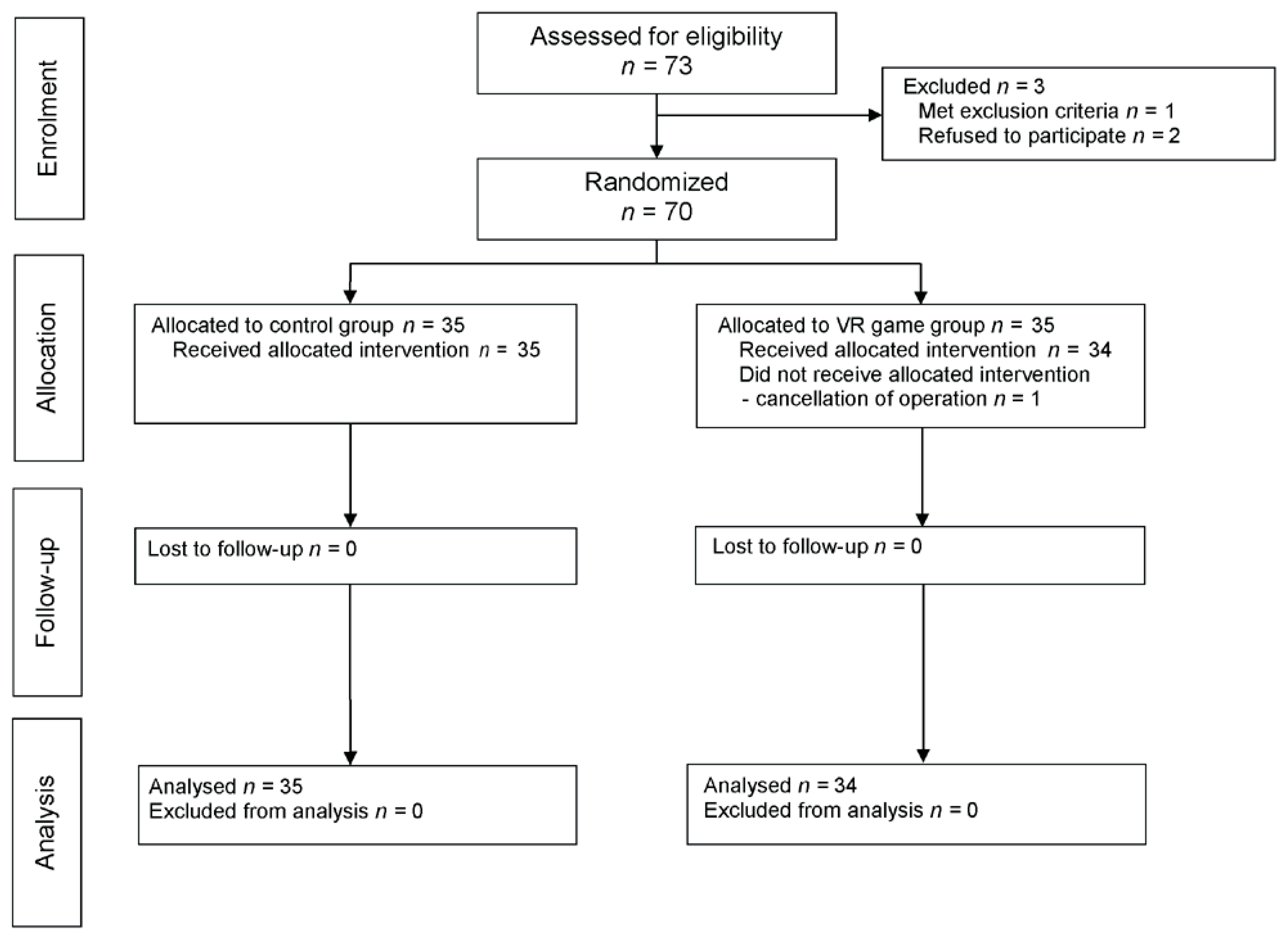
2.1. Study
2.2. Patients
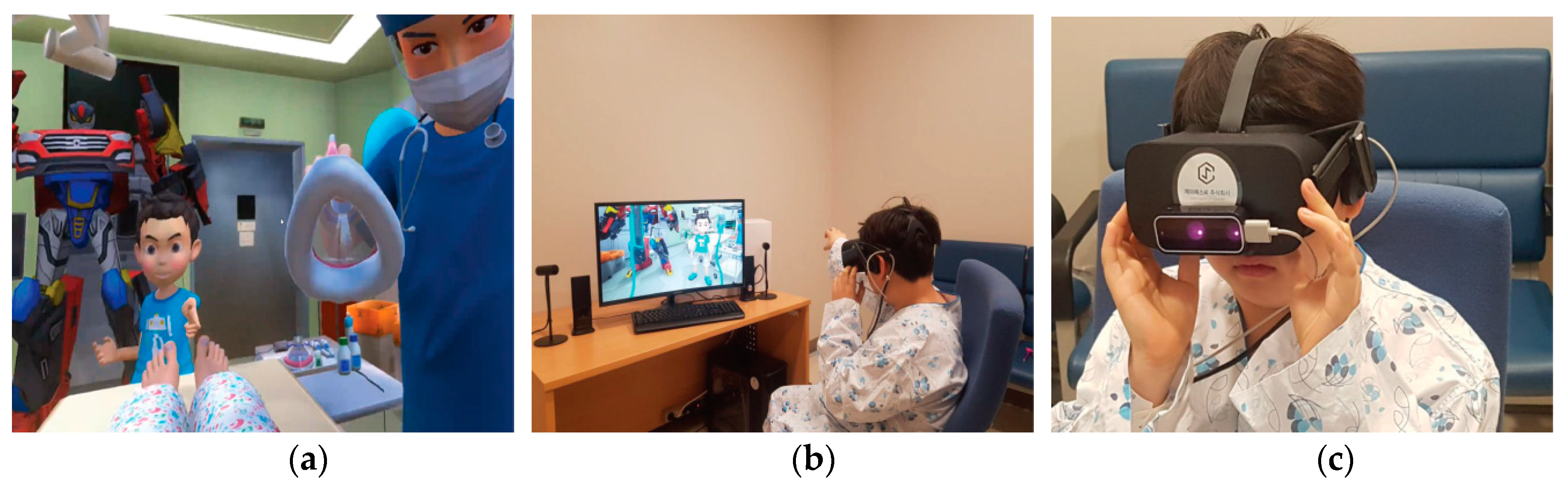
2.3. VR Game
2.4. Intervention
2.5. Anesthesia
2.6. Study Outcomes
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- King, D.; Greaves, F.; Exeter, C.; Darzi, A. ‘Gamification’: Influencing health behaviours with games. J. R. Soc. Med. 2013, 106, 76–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCoy, L.; Lewis, J.H.; Dalton, D. Gamification and multimedia for medical education: A landscape review. J. Am. Osteopath. Assoc. 2016, 116, 22–34. [Google Scholar] [CrossRef] [PubMed]
- Theng, Y.L.; Lee, J.W.; Patinadan, P.V.; Foo, S.S. The use of videogames, gamification, and virtual environments in the self-management of diabetes: A systematic review of evidence. Games Health J. 2015, 4, 352–361. [Google Scholar] [CrossRef] [PubMed]
- Primack, B.A.; Carroll, M.V.; McNamara, M.; Klem, M.L.; King, B.; Rich, M.; Chan, C.W.; Nayak, S. Role of video games in improving health-related outcomes: A systematic review. Am. J. Prev. Med. 2012, 42, 630–638. [Google Scholar] [CrossRef] [PubMed]
- Bekelis, K.; Calnan, D.; Simmons, N.; MacKenzie, T.A.; Kakoulides, G. Effect of an immersive preoperative virtual reality experience on patient reported outcomes: A randomized controlled trial. Ann. Surg. 2017, 265, 1068–1073. [Google Scholar] [CrossRef] [PubMed]
- Ryu, J.H.; Park, S.J.; Park, J.W.; Kim, J.W.; Yoo, H.J.; Kim, T.W.; Hong, J.S.; Han, S.H. Randomized clinical trial of immersive virtual reality tour of the operating theatre in children before anaesthesia. Br. J. Surg. 2017, 104, 1628–1633. [Google Scholar] [CrossRef] [PubMed]
- Willaert, W.I.; Aggarwal, R.; Van Herzeele, I.; Cheshire, N.J.; Vermassen, F.E. Recent advancements in medical simulation: Patient-specific virtual reality simulation. World J. Surg. 2012, 36, 1703–1712. [Google Scholar] [CrossRef] [PubMed]
- Ling, Y.; Nefs, H.T.; Morina, N.; Heynderickx, I.; Brinkman, W.P. A meta-analysis on the relationship between self-reported presence and anxiety in virtual reality exposure therapy for anxiety disorders. PLoS ONE 2014, 9, e96144. [Google Scholar] [CrossRef] [PubMed]
- Kothgassner, O.D.; Felnhofer, A.; Hlavacs, H.; Beutl, L.; Palme, R.; Kryspin-Exner, I.; Glenk, L.M. Salivary cortisol and cardiovascular reactivity to a public speaking task in a virtual and real-life environment. Comput. Hum. Behav. 2016, 62, 124–135. [Google Scholar] [CrossRef]
- Banchs, R.J.; Lerman, J. Preoperative anxiety management, emergence delirium, and postoperative behavior. Anesthesiol. Clin. 2014, 32, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Aouad, M.T.; Nasr, V.G. Emergence agitation in children: An update. Curr. Opin. Anaesthesiol. 2005, 18, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Kain, Z.N.; Mayes, L.C.; Caldwell-Andrews, A.A.; Karas, D.E.; McClain, B.C. Preoperative anxiety, postoperative pain, and behavioral recovery in young children undergoing surgery. Pediatrics 2006, 118, 651–658. [Google Scholar] [CrossRef] [PubMed]
- Litke, J.; Pikulska, A.; Wegner, T. Management of perioperative stress in children and parents. Part 1–The preoperative period. Anaesthesiol. Intensive Ther. 2012, 44, 165–169. [Google Scholar] [PubMed]
- Jung, K.; Im, M.H.; Hwang, J.M.; Oh, A.Y.; Park, M.S.; Jeong, W.J.; Kim, S.C.; Jung, S.W.; Sohn, H.; Yoon, M.O.; et al. Reliability and validity of korean version of modified: Yale preoperative anxiety scale. Ann. Surg. Treat. Res. 2016, 90, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Kain, Z.N.; Mayes, L.C.; Wang, S.M.; Caramico, L.A.; Hofstadter, M.B. Parental presence during induction of anesthesia versus sedative premedication: Which intervention is more effective? Anesthesiology 1998, 89, 1147–1156. [Google Scholar] [CrossRef] [PubMed]
- Blount, R.L.; Loiselle, K.A. Behavioural assessment of pediatric pain. Pain Res. Manag. 2009, 14, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Moura, L.A.; Dias, I.M.; Pereira, L.V. Prevalence and factors associated with preoperative anxiety in children aged 5–12 years. Rev. Lat. Am. Enfermagem. 2016, 24. [Google Scholar] [CrossRef] [PubMed]
- De Leo, G.; Diggs, L.A.; Radici, E.; Mastaglio, T.W. Measuring sense of presence and user characteristics to predict effective training in an online simulated virtual environment. Simul. Healthc. 2014, 9, 1–6. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Control Group (n = 35) | Gamification Group (n = 34) | p Value | |
|---|---|---|---|
| Age (year) | 6 (5−8) | 5 (5−7) | 0.170 |
| Height (cm) | 116.7 (109.8–127.3) | 114.7 (108.7–125.7) | 0.618 |
| Weight (kg) | 21.3 (18.9–28.6) | 20.9 (18.4–28.9) | 0.529 |
| BMI (kg/m2) | 16.8 (15.7–17.6) | 16.3 (15.2–17.3) | 0.400 |
| Gender (M/F) | 22 (63)/13 (37) | 18 (53)/16 (47) | 0.469 |
| ASA physical class (I/II) | 34 (97)/1 (3) | 33 (97)/1 (3) | >0.999 |
| Induction time (min) | 6 (4.5–8) | 6 (5–7.8) | 0.789 |
| Anesthesia time (min) | 40 (35–50) | 42.5 (35–50) | 0.479 |
| Operation time (min) | 20 (17.5–25) | 20 (15–30) | 0.997 |
| Type of surgery | 0.569 | ||
| Otolaryngeal | 12 (34) | 17 (50) | |
| Ophthalmic | 14 (40) | 12 (35) | |
| Dental | 4 (11) | 2 (6) | |
| Others | 5 (15) | 3 (9) |
| Control Group (n = 35) | Gamification Group (n = 34) | p Value | ||
|---|---|---|---|---|
| m-YPAS | baseline | 50.0 (43.3–65) | 51.7 (46.7−67.5) | 0.389 |
| preanesthetic | 46.7 (31.7–51.7) | 28.3 (23.3−36.7) | <0.001 | |
| difference | 0 (−20–4.2) | −22.5 (−29.6–−14.2) | 0.002 | |
| ICC score | perfect (0) | 19 (54) | 27 (79) | 0.038 |
| moderate (1–3) | 13 (37) | 7 (21) | ||
| poor (>4) | 3 (9) | 0 (0) | ||
| PBRS score | 1 (0–2) | 0 (0–1) | 0.092 | |
| Satisfaction Score (101 NRS) | 100 (90–100) | 100 (90–100) | 0.268 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ryu, J.-H.; Park, J.-W.; Nahm, F.S.; Jeon, Y.-T.; Oh, A.-Y.; Lee, H.J.; Kim, J.-H.; Han, S.-H. The Effect of Gamification through a Virtual Reality on Preoperative Anxiety in Pediatric Patients Undergoing General Anesthesia: A Prospective, Randomized, and Controlled Trial. J. Clin. Med. 2018, 7, 284. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm7090284
Ryu J-H, Park J-W, Nahm FS, Jeon Y-T, Oh A-Y, Lee HJ, Kim J-H, Han S-H. The Effect of Gamification through a Virtual Reality on Preoperative Anxiety in Pediatric Patients Undergoing General Anesthesia: A Prospective, Randomized, and Controlled Trial. Journal of Clinical Medicine. 2018; 7(9):284. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm7090284
Chicago/Turabian StyleRyu, Jung-Hee, Jin-Woo Park, Francis Sahngun Nahm, Young-Tae Jeon, Ah-Young Oh, Hak Jong Lee, Jin-Hee Kim, and Sung-Hee Han. 2018. "The Effect of Gamification through a Virtual Reality on Preoperative Anxiety in Pediatric Patients Undergoing General Anesthesia: A Prospective, Randomized, and Controlled Trial" Journal of Clinical Medicine 7, no. 9: 284. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm7090284