Lower Plasma Magnesium, Measured by Nuclear Magnetic Resonance Spectroscopy, is Associated with Increased Risk of Developing Type 2 Diabetes Mellitus in Women: Results from a Dutch Prospective Cohort Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
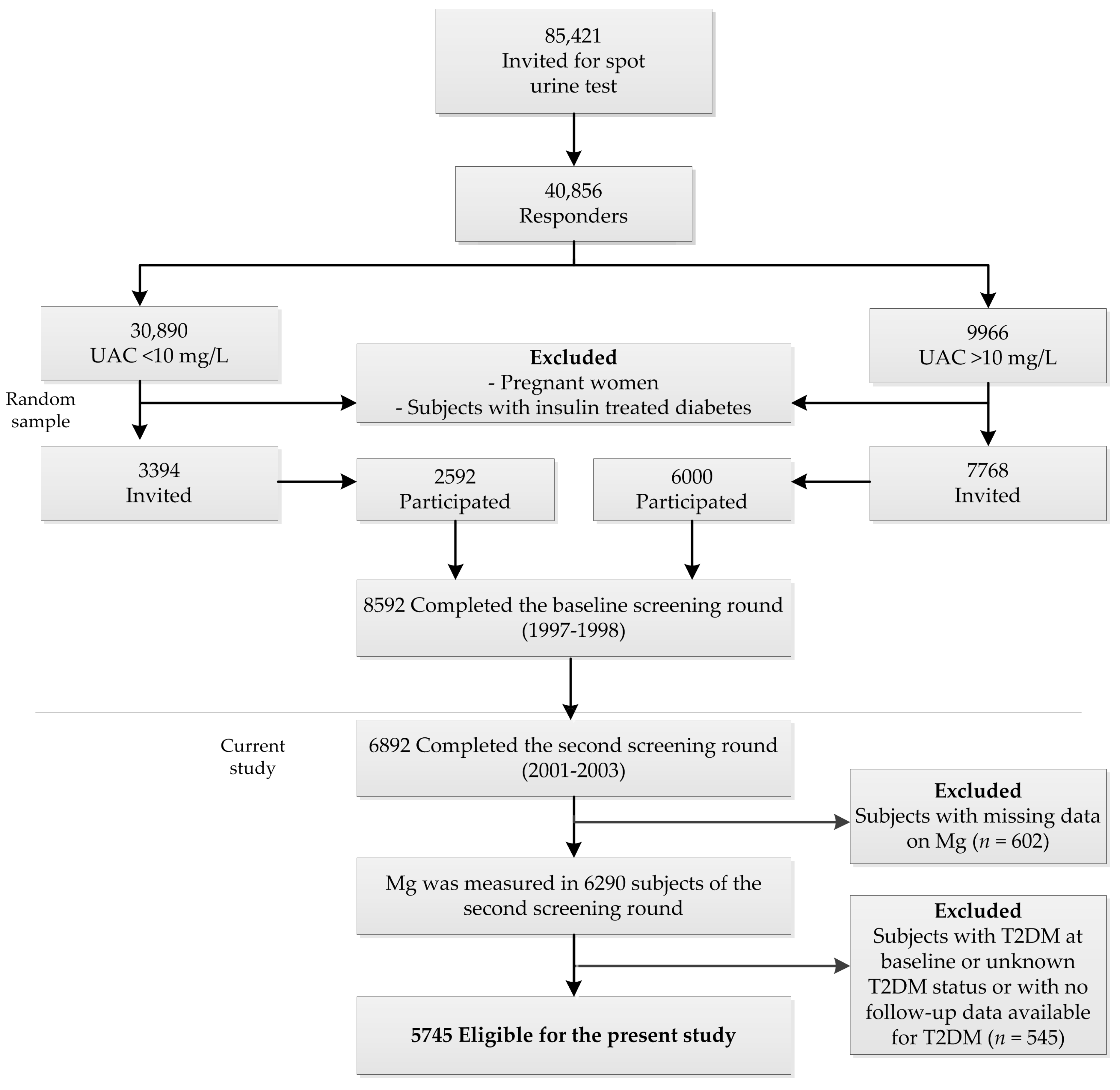
2.1. Study Design
2.2. Laboratory Analysis
2.3. NMR-Based Ionized Mg Assay
2.4. Roche Modular Total Mg Assay and Assay Comparison
2.5. Assessment of Covariates
2.6. Assessment of T2DM Risk
2.7. Statistical Analysis
3. Results
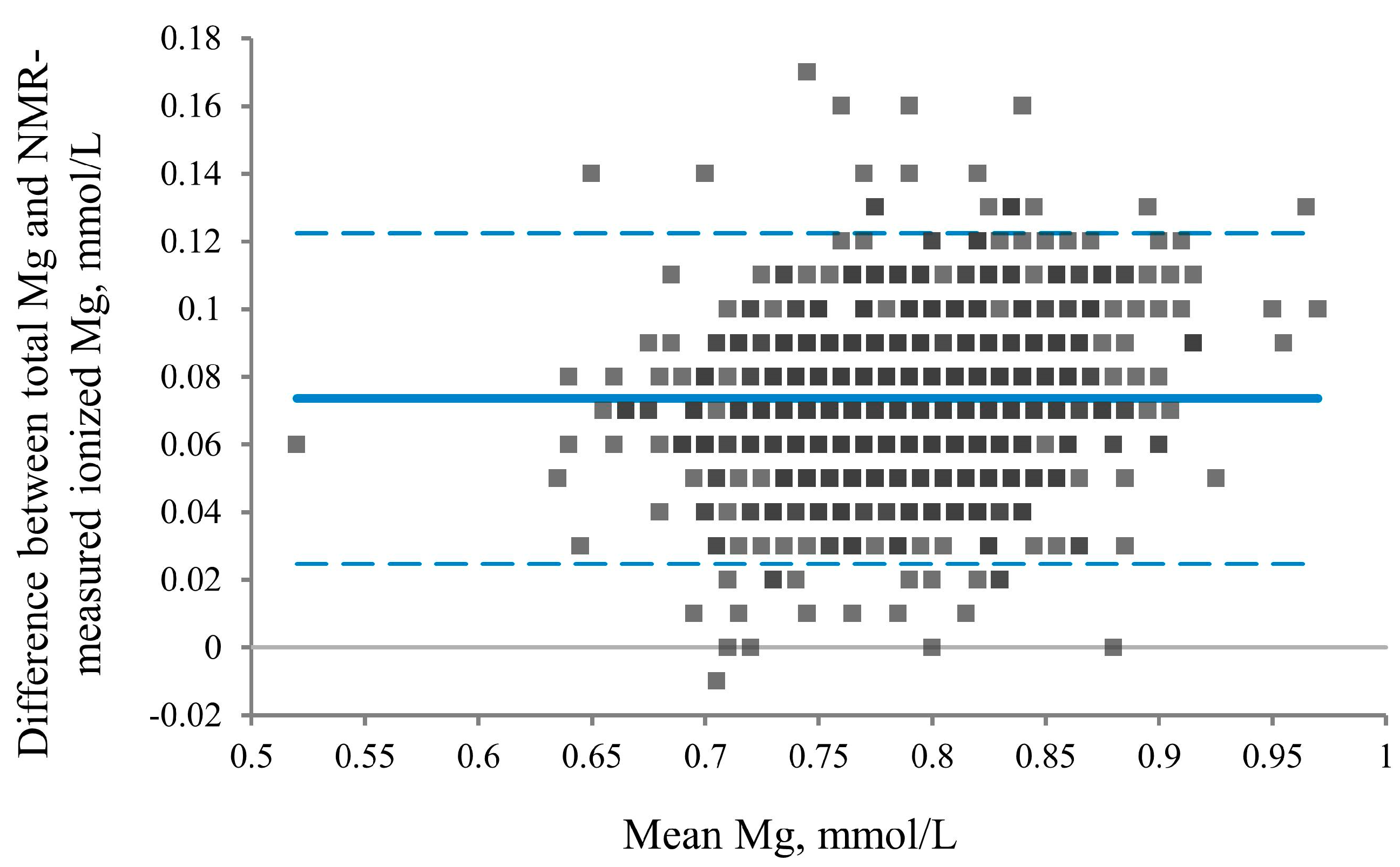
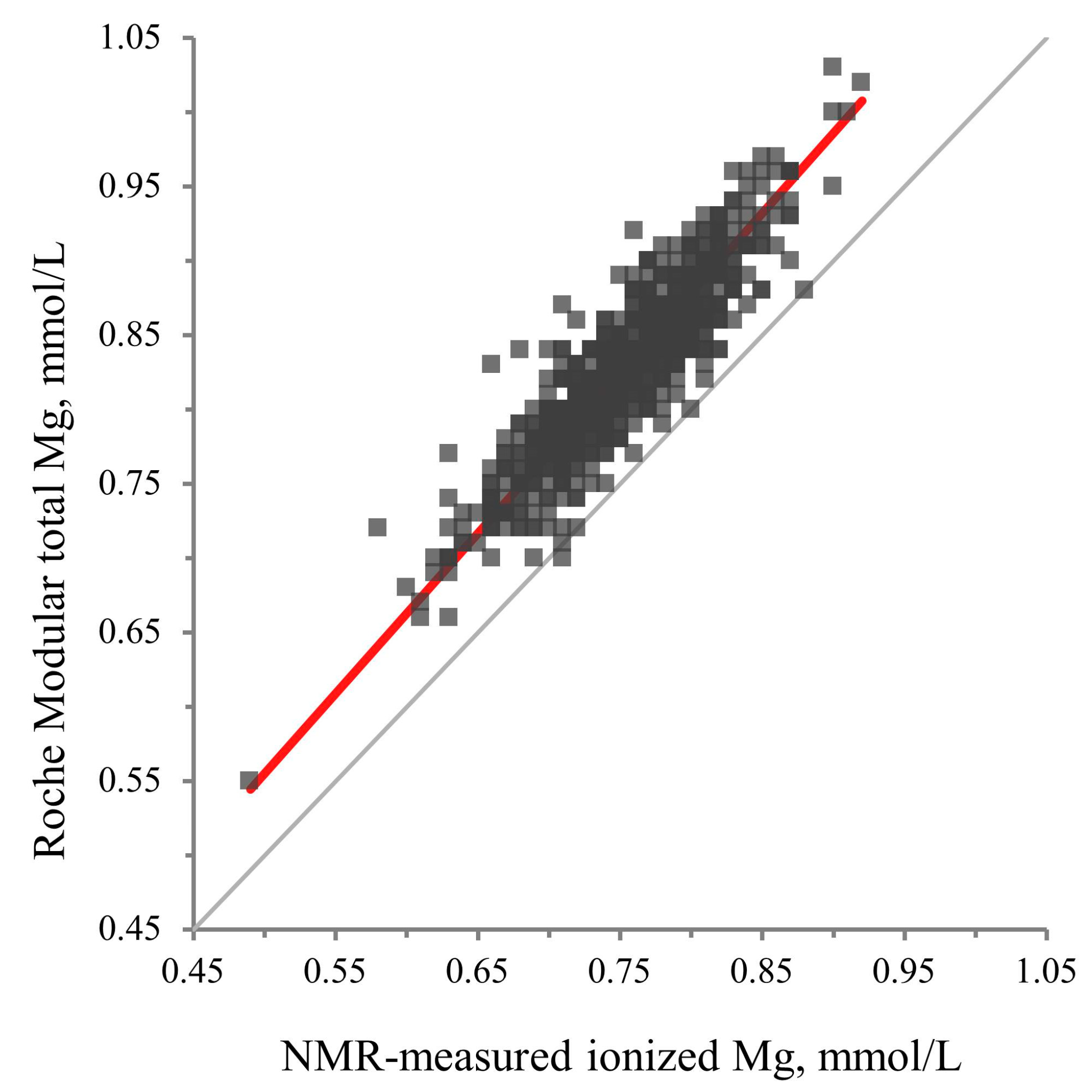
3.1. Analytical Performance of the NMR-Measured Ionized Mg Assay
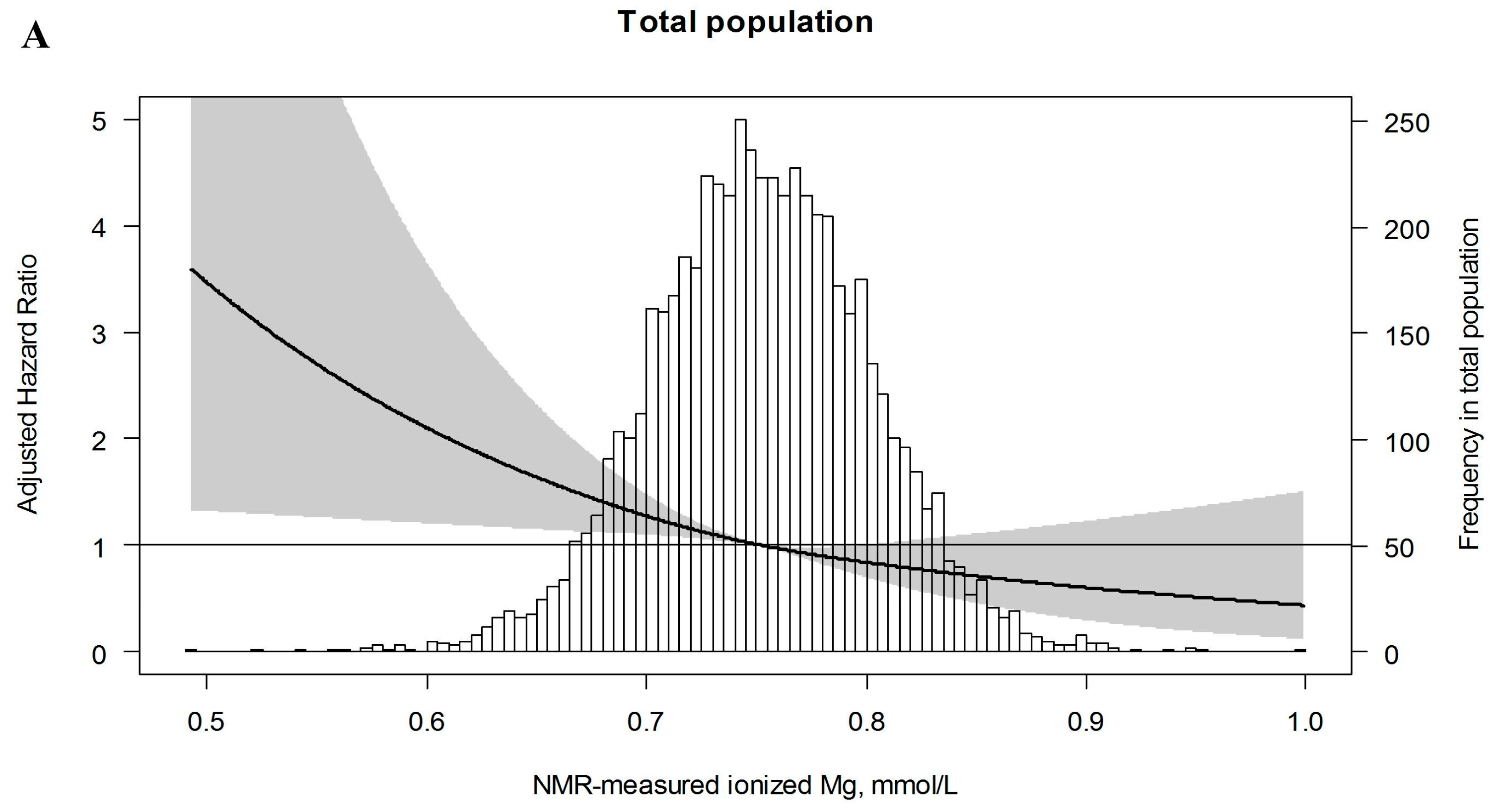
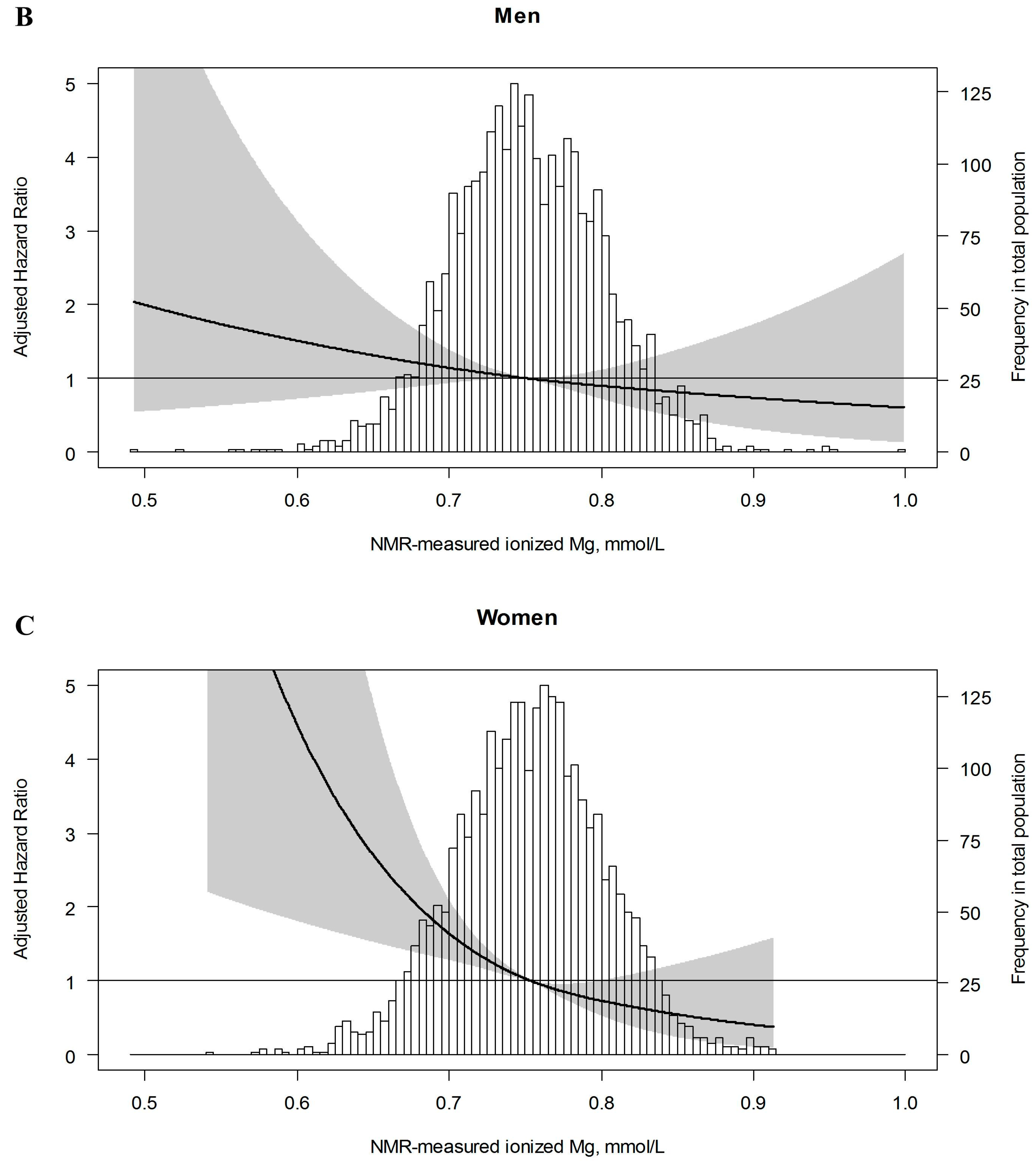
3.2. Association of Ionized Mg with the Risk of Developing T2DM
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Wild, S.; Roglic, G.; Green, A.; Sicree, R.; King, H. Global prevalence of diabetes: Estimates for the year 2000 and projections for 2030. Diabetes Care 2004, 27, 1047–1053. [Google Scholar] [CrossRef] [PubMed]
- Bonora, E.; Kiechl, S.; Willeit, J.; Oberhollenzer, F.; Egger, G.; Meigs, J.B.; Bonadonna, R.C.; Muggeo, M. Population-based incidence rates and risk factors for type 2 diabetes in white individuals: The Bruneck study. Diabetes 2004, 53, 1782–1789. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Xu, Q.; Park, Y.; Hollenbeck, A.; Schatzkin, A.; Chen, H. Multivitamins, individual vitamin and mineral supplements, and risk of diabetes among older U.S. adults. Diabetes Care 2011, 34, 108–114. [Google Scholar] [CrossRef]
- Paolisso, G.; Barbagallo, M. Hypertension, diabetes mellitus, and insulin resistance: The role of intracellular magnesium. Am. J. Hypertens. 1997, 10, 346–355. [Google Scholar] [CrossRef]
- Song, Y.; Li, T.Y.; van Dam, R.M.; Manson, J.E.; Hu, F.B. Magnesium intake and plasma concentrations of markers of systemic inflammation and endothelial dysfunction in women. Am. J. Clin. Nutr. 2007, 85, 1068–1074. [Google Scholar] [CrossRef]
- Chacko, S.A.; Song, Y.; Nathan, L.; Tinker, L.; de Boer, I.H.; Tylavsky, F.; Wallace, R.; Liu, S. Relations of dietary magnesium intake to biomarkers of inflammation and endothelial dysfunction in an ethnically diverse cohort of postmenopausal women. Diabetes Care 2010, 33, 304–310. [Google Scholar] [CrossRef]
- Joosten, M.M.; Gansevoort, R.T.; Mukamal, K.J.; van der Harst, P.; Geleijnse, J.M.; Feskens, E.J.M.; Navis, G.; Bakker, S.J. Urinary and plasma magnesium and risk of ischemic heart disease. Am. J. Clin. Nutr. 2013, 97, 1299–1306. [Google Scholar] [CrossRef] [PubMed]
- Joosten, M.M.; Gansevoort, R.T.; Mukamal, K.J.; Kootstra-Ros, J.E.; Feskens, E.J.M.; Geleijnse, J.M.; Navis, G.; Bakker, S.J. Urinary magnesium excretion and risk of hypertension: The prevention of renal and vascular end-stage disease study. Hypertension 2013, 61, 1161–1167. [Google Scholar] [CrossRef]
- Zhang, X.; Li, Y.; Del Gobbo, L.C.; Rosanoff, A.; Wang, J.; Zhang, W.; Song, Y. Effects of Magnesium Supplementation on Blood Pressure: A Meta-Analysis of Randomized Double-Blind Placebo-Controlled Trials. Hypertension 2016, 68, 324–333. [Google Scholar] [CrossRef] [PubMed]
- Gommers, L.M.M.; Hoenderop, J.G.J.; Bindels, R.J.M.; de Baaij, J.H.F. Hypomagnesemia in Type 2 Diabetes: A Vicious Circle? Diabetes 2016, 65, 3–13. [Google Scholar] [CrossRef]
- Fang, X.; Wang, K.; Han, D.; He, X.; Wei, J.; Zhao, L.; Imam, M.U.; Ping, Z.; Li, Y.; Xu, Y.; et al. Dietary magnesium intake and the risk of cardiovascular disease, type 2 diabetes, and all-cause mortality: A dose-response meta-analysis of prospective cohort studies. BMC Med. 2016, 14, 210. [Google Scholar] [CrossRef] [PubMed]
- Dong, J.Y.; Xun, P.; He, K.; Qin, L.Q. Magnesium intake and risk of type 2 diabetes: Meta-analysis of prospective cohort studies. Diabetes Care 2011, 34, 2116–2122. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Xun, P.; Tang, Q.; Cai, W.; He, K. Circulating magnesium levels and incidence of coronary heart diseases, hypertension, and type 2 diabetes mellitus: A meta-analysis of prospective cohort studies. Nutr. J. 2017, 19, 60. [Google Scholar] [CrossRef]
- Elin, R.J. Assessment of magnesium status. Clin. Chem. 1987, 33, 1965–1970. [Google Scholar] [PubMed]
- Saris, N.E.; Mervaala, E.; Karppanen, H.; Khawaja, J.A.; Lewenstam, A. Magnesium. An update on physiological, clinical and analytical aspects. Clin. Chim. Acta 2000, 294, 1–26. [Google Scholar] [CrossRef]
- Matyus, S.P.; Braun, P.J.; Wolak-Dinsmore, J.; Jeyarajah, E.J.; Shalaurova, I.; Xu, Y.; Warner, S.M.; Clement, T.S.; Connelly, M.A.; Fischer, T.J. NMR measurement of LDL particle number using the Vantera Clinical Analyzer. Clin. Biochem. 2014, 47, 203–210. [Google Scholar] [CrossRef]
- Otvos, J.D.; Shalaurova, I.; Wolak-Dinsmore, J.; Connelly, M.A.; Mackey, R.H.; Stein, J.H.; Tracy, R.P. GlycA: A Composite Nuclear Magnetic Resonance Biomarker of Systemic Inflammation. Clin. Chem. 2015, 61, 714–723. [Google Scholar] [CrossRef] [PubMed]
- Garcia, E.; Wolak-Dinsmore, J.; Wang, Z.; Li, X.S.; Bennett, D.W.; Connelly, M.A.; Otvos, J.D.; Hazen, S.L.; Jeyarajah, E.J. NMR quantification of trimethylamine-N-oxide in human serum and plasma in the clinical laboratory setting. Clin. Biochem. 2017, 50, 947–955. [Google Scholar] [CrossRef] [PubMed]
- Wolak-Dinsmore, J.; Gruppen, E.G.; Shalaurova, I.; Matyus, S.P.; Grant, R.P.; Gegen, R.; Bakker, S.J.L.; Otvos, J.D.; Connelly, M.A.; Dullaart, R.P.F. A novel NMR-based assay to measure circulating concentrations of branched-chain amino acids: Elevation in subjects with type 2 diabetes mellitus and association with carotid intima media thickness. Clin. Biochem. 2018, 54, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Hillege, H.L.; Janssen, W.M.; Bak, A.A.; Diercks, G.F.; Grobbee, D.E.; Crijns, H.J.; Van Gilst, W.H.; De Zeeuw, D.; De Jong, P.E. Microalbuminuria is common, also in a nondiabetic, nonhypertensive population, and an independent indicator of cardiovascular risk factors and cardiovascular morbidity. J. Intern. Med. 2001, 249, 519–526. [Google Scholar] [CrossRef] [PubMed]
- Jeyarajah, E.J.; Cromwell, W.C.; Otvos, J.D. Lipoprotein particle analysis by nuclear magnetic resonance spectroscopy. Clin. Lab. Med. 2006, 26, 847–870. [Google Scholar] [CrossRef]
- Eisenga, M.F.; Wouters, H.J.C.M.; Kieneker, L.M.; van der Klauw, M.M.; van der Meer, P.; Wolffenbuttel, B.H.R.; Gaillard, C.A.J.M.; Kootstra-Ros, J.E.; Touw, D.J.; Huls, G.; et al. Active smoking and macrocytosis in the general population: Two population-based cohort studies. Am. J. Hematol. 2019, 94, E45–E48. [Google Scholar] [CrossRef] [PubMed]
- Visser, S.T.; Schuiling-Veninga, C.C.; Bos, J.H.; de Jong-van den Berg, L.T.; Postma, M.J. The population-based prescription database IADB.nl: Its development, usefulness in outcomes research and challenges. Expert. Rev. Pharmacoecon. Outcomes Res. 2013, 13, 285–292. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Oterdoom, L.H.; Gansevoort, R.T.; Schouten, J.P.; de Jong, P.E.; Gans, R.O.B.; Bakker, S.J.L. Urinary creatinine excretion, an indirect measure of muscle mass, is an independent predictor of cardiovascular disease and mortality in the general population. Atherosclerosis 2009, 207, 534–540. [Google Scholar] [CrossRef] [PubMed]
- Verhave, J.C.; Hillege, H.L.; Burgerhof, J.G.M.; Janssen, W.M.T.; Gansevoort, R.T.; Navis, G.J.; de Zeeuw, D.; de Jong, P.E. Sodium intake affects urinary albumin excretion especially in overweight subjects. J. Intern. Med. 2004, 256, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Gruppen, E.G.; Connelly, M.A.; Vart, P.; Otvos, J.D.; Bakker, S.J.; Dullaart, R.P. GlycA, a novel proinflammatory glycoprotein biomarker, and high-sensitivity C-reactive protein are inversely associated with sodium intake after controlling for adiposity: The Prevention of Renal and Vascular End-Stage Disease study. Am. J. Clin. Nutr. 2016, 104, 415–422. [Google Scholar] [CrossRef]
- Connelly, M.A.; Gruppen, E.G.; Wolak-Dinsmore, J.; Matyus, S.P.; Riphagen, I.J.; Shalaurova, I.; Bakker, S.J.; Otvos, J.D.; Dullaart, R.P. GlycA, a marker of acute phase glycoproteins, and the risk of incident type 2 diabetes mellitus: PREVEND study. Clin. Chim. Acta 2016, 452, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, A.; Corpeleijn, E.; Postmus, D.; Gansevoort, R.T.; De Jong, P.E.; Gans, R.O.B.; Struck, J.; Hillege, H.L.; Stolk, R.P.; Navis, G.; et al. Plasma procalcitonin and risk of type 2 diabetes in the general population. Diabetologia 2011, 54, 2463–2465. [Google Scholar] [CrossRef]
- Schafer, J.L.; Graham, J.W. Missing data: Our view of the state of the art. Psychol. Methods 2002, 7, 147–177. [Google Scholar] [CrossRef] [PubMed]
- Koch, S.M.; Warters, R.D.; Mehlhorn, U. The simultaneous measurement of ionized and total calcium and ionized and total magnesium in intensive care unit patients. J. Crit. Care 2002, 17, 203–205. [Google Scholar] [CrossRef] [PubMed]
- Van Genugten, R.E.; Utzschneider, K.M.; Tong, J.; Gerchman, F.; Zraika, S.; Udayasankar, J.; Boyko, E.J.; Fujimoto, W.Y.; Kahn, S.E. Effects of sex and hormone replacement therapy use on the prevalence of isolated impaired fasting glucose and isolated impaired glucose tolerance in subjects with a family history of type 2 diabetes. Diabetes 2006, 55, 3529–3535. [Google Scholar] [CrossRef] [PubMed]
- Groenestege, W.M.T.; Hoenderop, J.G.; van den Heuvel, L.; Knoers, N.; Bindels, R.J. The Epithelial Mg2 Channel Transient Receptor Potential Melastatin 6 Is Regulated by Dietary Mg2 Content and Estrogens. J. Am. Soc. Nephrol. 2006, 17, 1035–1043. [Google Scholar] [CrossRef] [PubMed]
- Van der Wijst, J.; Hoenderop, J.G.J.; Bindels, R.J.M. Epithelial Mg2+ channel TRPM6: Insight into the molecular regulation. Magn. Res. 2009, 22, 127–132. [Google Scholar] [CrossRef]
- Grochans, E.; Karakiewicz, B.; Kozielec, T.; Brodowska, A.; Brodowski, J.; Starczewski, A.; Laszczynska, M.; Nocen, I.; Grzywacz, A.; Samochowiec, A.; et al. Serum Mg and Zn levels in postmenopausal women. Magn. Res. 2011, 24, 209–214. [Google Scholar] [CrossRef]
- Muneyyirci-Delale, O.; Nacharaju, V.L.; Altura, B.M.; Altura, B.T. Sex steroid hormones modulate serum ionized magnesium and calcium levels throughout the menstrual cycle in women. Fertil. Steril. 1998, 69, 958–962. [Google Scholar] [CrossRef]
- Bertinato, J.; Wu Xiao, C.; Ratnayake, W.M.; Fernandez, L.; Lavergne, C.; Wood, C.; Swist, E. Lower serum magnesium concentration is associated with diabetes, insulin resistance, and obesity in South Asian and white Canadian women but not men. Food Nutr. Res. 2015, 59. [Google Scholar] [CrossRef]
- Brown, I.R.; McBain, A.S.; Chalmers, J.; Campbell, I.W.; Brown, E.R.; Lewis, M.J. Sex difference in the relationship of calcium and magnesium excretion to glycaemic control in type 1 diabetes mellitus. Clin. Chim. Acta 1999, 283, 119–128. [Google Scholar] [CrossRef]
- Xu, T.; Sun, Y.; Xu, T.; Zhang, Y. Magnesium intake and cardiovascular disease mortality: A meta-analysis of prospective cohort studies. Int. J. Cardiol. 2013, 167, 3044–3047. [Google Scholar] [CrossRef]
- Velat, I.; Culić, V. Magnesium, sex and cardiovascular mortality. Int. J. Cardiol. 2013, 168, 4437–4438. [Google Scholar] [CrossRef]
- Ye, H.; Cao, P.; Zhang, X.; Lin, J.; Guo, Q.; Mao, H.; Yu, X.; Yang, X. Serum magnesium and cardiovascular mortality in peritoneal dialysis patients: A 5-year prospective cohort study. Br. J. Nutr. 2018, 120, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Kao, W.H.; Folsom, A.R.; Nieto, F.J.; Mo, J.P.; Watson, R.L.; Brancati, F.L. Serum and dietary magnesium and the risk for type 2 diabetes mellitus: The Atherosclerosis Risk in Communities Study. Arch. Intern. Med. 1999, 159, 2151–2159. [Google Scholar] [CrossRef] [PubMed]
- Everett, C.J.; King, D.E. Serum magnesium and the development of diabetes. Nutrition 2006, 22, 679. [Google Scholar] [CrossRef] [PubMed]
- Kieboom, B.C.T.; Ligthart, S.; Dehghan, A.; Kurstjens, S.; de Baaij, J.H.F.; Franco, O.H.; Hofman, A.; Zietse, R.; Stricker, B.H.; Hoorn, E.J. Serum magnesium and the risk of prediabetes: A population-based cohort study. Diabetologia 2017, 60, 843–853. [Google Scholar] [CrossRef]
- Veronese, N.; Watutantrige-Fernando, S.; Luchini, C.; Solmi, M.; Sartore, G.; Sergi, G.; Manzato, E.; Barbagallo, M.; Maggi, S.; Stubbs, B. Effect of magnesium supplementation on glucose metabolism in people with or at risk of diabetes: A systematic review and meta-analysis of double-blind randomized controlled trials. Eur. J. Clin. Nutr. 2016, 70, 1354–1359. [Google Scholar] [CrossRef]
- Wang, X.; Bao, W.; Liu, J.; Ouyang, Y.Y.; Wang, D.; Rong, S.; Xiao, X.; Shan, Z.L.; Zhang, Y.; Yao, P.; et al. Inflammatory markers and risk of type 2 diabetes: A systematic review and meta-analysis. Diabetes Care 2013, 36, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Jin, X.; Liu, J.; Sun, T.; Xie, M.; Bao, W.; Yu, X.; Yang, X.; Zhang, Y.; Zhang, H.; et al. Association of Plasma Magnesium with Prediabetes and Type 2 Diabetes Mellitus in Adults. Sci. Rep. 2017, 7, 12763. [Google Scholar] [CrossRef]
- Simental-Mendia, L.E.; Sahebkar, A.; Rodriguez-Moran, M.; Zambrano-Galvan, G.; Guerrero-Romero, F. Effect of Magnesium Supplementation on Plasma C-reactive Protein Concentrations: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Curr. Pharm. Des. 2017, 23, 4678–4686. [Google Scholar] [CrossRef]
- Ishimura, E.; Okuno, S.; Yamakawa, T.; Inaba, M.; Nishizawa, Y. Serum magnesium concentration is a significant predictor of mortality in maintenance hemodialysis patients. Magn. Res. 2007, 20, 237–244. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Within-Lab | NMR-Measured Mg (mmol/L) | |
|---|---|---|
| Low | High | |
| Mean | 0.489 | 0.892 |
| SD | 0.035 | 0.041 |
| CV | 7.1% | 4.6% |
| Tertiles of NMR-Measured Mg, mmol/L | P Trend | |||
|---|---|---|---|---|
| 1 (<0.73) | 2 (0.73–0.77) | 3 (>0.77) | ||
| Participants, n | 1919 | 1900 | 1928 | - |
| Age, years | 52.3 ± 11.8 | 52.2 ± 11.7 | 54.4 ± 12.0 | <0.001 |
| Female, % | 48.7 | 52.1 | 50.5 | 0.27 |
| Race, whites, % | 96.2 | 95.9 | 96.0 | 0.65 |
| Body mass index, kg/m2 | 26.9 ± 4.3 | 26.5 ± 4.3 | 26.1 ± 3.9 | <0.001 |
| Smoking status, % | <0.001 | |||
| Never | 25.9 | 29.3 | 30.9 | |
| Former | 42.2 | 43.1 | 43.2 | |
| Current | 31.9 | 27.6 | 25.9 | |
| Alcohol consumption, % | 0.82 | |||
| None | 24.1 | 23.8 | 23.5 | |
| 1–4 drinks per month | 16.1 | 17.7 | 17.4 | |
| 2–7 drinks per week | 31.9 | 32.6 | 31.4 | |
| 1–3 drinks per day | 21.7 | 21.9 | 22.3 | |
| 4 or more drinks per day | 5.3 | 3.3 | 4.2 | |
| Education, % | 0.17 | |||
| Low | 43.3 | 41.6 | 42.4 | |
| Middle | 26.4 | 27.2 | 24.3 | |
| High | 30.4 | 31.2 | 33.3 | |
| Glucose, mmol/L | 4.89 ± 0.66 | 4.82 ± 0.65 | 4.81 ± 0.63 | <0.001 |
| Parental history of T2DM, % | 14.0 | 14.6 | 14.6 | 0.61 |
| Blood pressure, mm Hg | ||||
| Systolic | 125.7 ± 18.2 | 124.0 ± 17.2 | 126.2 ± 19.2 | 0.43 |
| Diastolic | 73.4 ± 9.1 | 72.7 ± 8.9 | 73.3 ± 9.1 | 0.87 |
| Hypertension, yes, % | 33.1 | 28.1 | 32.9 | 0.90 |
| Use of antihypertensive drugs | ||||
| ACEi, % | 6.2 | 5.5 | 5.2 | 0.41 |
| ARB, % | 2.1 | 1.5 | 2.0 | 0.36 |
| Diuretics, % | 6.0 | 5.3 | 5.4 | 0.59 |
| Beta blockers, % | 11.1 | 8.8 | 8.5 | 0.01 |
| Total cholesterol, mmol/L | 5.40 ± 1.04 | 5.40 ± 1.03 | 5.50 ± 1.03 | 0.004 |
| HDL-cholesterol, mmol/L | 1.23 ± 0.29 | 1.26 ± 0.30 | 1.30 ± 0.25 | <0.001 |
| Triglycerides, mmol/L | 1.13 (0.83–1.66) | 1.09 (0.78–1.54) | 1.08 (0.79–1.55) | 0.001 |
| Triglyeride:HDL-cholesterol ratio | 2.19 (1.40–3.46) | 2.00 (1.33–3.18) | 1.93 (1.24–3.17) | <0.001 |
| Use of lipid lowering drugs, yes, % | 6.5 | 7.3 | 7.6 | 0.03 |
| CRP, mg/L | 1.41 (0.64–3.14) | 1.26 (0.58–2.77) | 1.26 (0.60–2.86) | 0.02 |
| Creatinine, μmol/L | 70.0 (61.0–79.0) | 71.0 (62.0–80.0) | 72.0 (64.0–81.0) | <0.001 |
| Cystatine C, mg/L | 0.87 (0.78–0.98) | 0.86 (0.78–0.96) | 0.89 (0.80–0.99) | <0.001 |
| Estimated GFR, mL/min/1.732 | 93.6 ± 17.0 | 94.1 ± 16.2 | 90.3 ± 17.0 | <0.001 |
| Plasma levels of | ||||
| Albumin, g/L | 43.3 ± 2.8 | 43.8 ± 2.6 | 44.2 ± 2.9 | <0.001 |
| Sodium, mmol/L | 140.5 ± 2.0 | 140.7 ± 2.0 | 140.9 ± 2.1 | <0.001 |
| Potassium, mmol/L | 4.20 ± 0.28 | 4.22 ± 0.26 | 4.25 ± 0.29 | <0.001 |
| Calcium, mmol/L | 2.30 ± 0.12 | 2.30 ± 0.10 | 2.30 ± 0.11 | 0.06 |
| Urinary excretions of | ||||
| Albumin, mg/24-h | 9.0 (6.1–17.3) | 8.2 (5.9–14.0) | 8.3 (6.0–13.5) | <0.001 |
| Sodium, mmol/24-h | 148.5 ± 56.3 | 144.3 ± 55.3 | 139.9 ± 53.5 | <0.001 |
| Urea, mmol/24-h | 365.6 ± 112.8 | 367.8 ± 115.0 | 359.2 ± 110.8 | 0.07 |
| Creatinine, mmol/24-h | 12.7 ± 3.4 | 12.4 ± 3.3 | 12.2 ± 3.4 | <0.001 |
| Continuous, per 0.1 mmol/L Decrease | Tertiles of NMR-Measured Mg, mmol/L | |||
|---|---|---|---|---|
| 1 | 2 | 3 | ||
| Total (n = 5747) | ||||
| Events, n (%) | 289 (5.0) | 108 (5.6) | 99 (5.2) | 82 (4.3) |
| Crude analysis | 1.50 (1.19–1.89) | 1.36 (1.02–1.82) | 1.23 (1.02–1.82) | 1.00 (reference) |
| Age and sex adjusted | 1.54 (1.23–1.92) | 1.46 (1.09–1.94) | 1.36 (1.01–1.82) | 1.00 (reference) |
| Model 1 | 1.27 (1.00–1.61) | 1.17 (0.87–1.56) | 1.19 (0.89–1.60) | 1.00 (reference) |
| Model 2 | 1.32 (1.04–1.67) | 1.20 (0.89–1.61) | 1.20 (0.89–1.62) | 1.00 (reference) |
| Model 3 | 1.16 (0.91–1.47) | 1.09 (0.81–1.47) | 1.23 (0.91–1.65) | 1.00 (reference) |
| Men (n = 2848) | ||||
| Events, n (%) | 186 (6.5) | 66 (6.7) | 66 (7.3) | 54 (5.7) |
| Crude analysis | 1.25 (0.94–1.67) | 1.21 (0.84–1.73) | 1.31 (0.91–1.87) | 1.00 (reference) |
| Age adjusted | 1.27 (0.96–1.69) | 1.26 (0.88–1.80) | 1.41 (0.98–2.02) | 1.00 (reference) |
| Model 1 | 1.04 (0.78–1.40) | 1.01 (0.70–1.45) | 1.31 (0.92–1.89) | 1.00 (reference) |
| Model 2 | 1.04 (0.78–1.40) | 1.01 (0.70–1.45) | 1.31 (0.91–1.89) | 1.00 (reference) |
| Model 3 | 0.90 (0.67–1.21) | 0.85 (0.58–1.24) | 1.26 (0.88–1.81) | 1.00 (reference) |
| Women (n = 2899) | ||||
| Events, n (%) | 103 (3.6) | 42 (4.5) | 33 (3.3) | 28 (2.9) |
| Crude analysis | 2.02 (1.37–2.99) | 1.65 (1.02–2.66) | 1.15 (0.70–1.91) | 1.00 (reference) |
| Age adjusted | 2.33 (1.58–3.42) | 1.99 (1.23–3.22) | 1.28 (0.78–2.13) | 1.00 (reference) |
| Model 1 | 1.66 (1.11–2.47) | 1.45 (0.88–2.39) | 1.13 (0.68–1.89) | 1.00 (reference) |
| Model 2 | 1.88 (1.26–2.79) | 1.67 (1.01–2.77) | 1.23 (0.73–2.08) | 1.00 (reference) |
| Model 3 | 1.80 (1.20–2.70) | 1.72 (1.03–2.86) | 1.30 (0.76–2.20) | 1.00 (reference) |
| Continuous, per 0.1 mmol/L decrease | Tertiles of NMR-Measured Mg, mmol/L | |||
|---|---|---|---|---|
| 1 | 2 | 3 | ||
| Total (n = 5747) | ||||
| Events, n (%) | 289 (5.0) | 108 (5.6) | 99 (5.2) | 82 (4.3) |
| Crude analysis | 1.50 (1.19–1.89) | 1.36 (1.02–1.82) | 1.23 (1.02–1.82) | 1.00 (reference) |
| Age and sex adjusted | 1.54 (1.23–1.92) | 1.46 (1.09–1.94) | 1.36 (1.01–1.82) | 1.00 (reference) |
| Model 1 | 1.32 (1.04–1.67) | 1.21 (0.90–1.62) | 1.18 (0.90–1.62) | 1.00 (reference) |
| Model 2 | 1.37 (1.08–1.74) | 1.26 (0.93–1.69) | 1.20 (0.89–1.62) | 1.00 (reference) |
| Model 3 | 1.19 (0.94–1.51) | 1.12 (0.83–1.51) | 1.21 (0.90–1.63) | 1.00 (reference) |
| Men (n = 2848) | ||||
| Events, n (%) | 186 (6.5) | 66 (6.7) | 66 (7.3) | 54 (5.7) |
| Crude analysis | 1.25 (0.94–1.67) | 1.21 (0.84–1.73) | 1.31 (0.91–1.87) | 1.00 (reference) |
| Age adjusted | 1.27 (0.96–1.69) | 1.26 (0.88–1.80) | 1.41 (0.98–2.02) | 1.00 (reference) |
| Model 1 | 1.05 (0.78–1.40) | 1.01 (0.70–1.45) | 1.32 (0.92–1.90) | 1.00 (reference) |
| Model 2 | 1.04 (0.78–1.41) | 1.01 (0.70–1.45) | 1.32 (0.92–1.89) | 1.00 (reference) |
| Model 3 | 0.89 (0.67–1.20) | 0.84 (0.58–1.22) | 1.26 (0.87–1.81) | 1.00 (reference) |
| Women (n = 2899) | ||||
| Events, n (%) | 103 (3.6) | 42 (4.5) | 33 (3.3) | 28 (2.9) |
| Crude analysis | 2.02 (1.37–2.99) | 1.65 (1.02–2.66) | 1.15 (0.70–1.91) | 1.00 (reference) |
| Age adjusted | 2.33 (1.58–3.42) | 1.99 (1.23–3.22) | 1.28 (0.78–2.13) | 1.00 (reference) |
| Model 1 | 1.70 (1.14–2.52) | 1.52 (0.92–2.49) | 1.12 (0.67–1.87) | 1.00 (reference) |
| Model 2 | 1.89 (1.27–2.81) | 1.71 (1.04–2.83) | 1.18 (0.70–1.99) | 1.00 (reference) |
| Model 3 | 1.81 (1.22–2.69) | 1.75 (1.06–2.89) | 1.29 (1.06–2.17) | 1.00 (reference) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schutten, J.C.; Gomes-Neto, A.W.; Navis, G.; Gansevoort, R.T.; Dullaart, R.P.F.; Kootstra-Ros, J.E.; Danel, R.M.; Goorman, F.; Gans, R.O.B.; de Borst, M.H.; et al. Lower Plasma Magnesium, Measured by Nuclear Magnetic Resonance Spectroscopy, is Associated with Increased Risk of Developing Type 2 Diabetes Mellitus in Women: Results from a Dutch Prospective Cohort Study. J. Clin. Med. 2019, 8, 169. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8020169
Schutten JC, Gomes-Neto AW, Navis G, Gansevoort RT, Dullaart RPF, Kootstra-Ros JE, Danel RM, Goorman F, Gans ROB, de Borst MH, et al. Lower Plasma Magnesium, Measured by Nuclear Magnetic Resonance Spectroscopy, is Associated with Increased Risk of Developing Type 2 Diabetes Mellitus in Women: Results from a Dutch Prospective Cohort Study. Journal of Clinical Medicine. 2019; 8(2):169. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8020169
Chicago/Turabian StyleSchutten, Joëlle C., António W. Gomes-Neto, Gerjan Navis, Ron T. Gansevoort, Robin P. F. Dullaart, Jenny E. Kootstra-Ros, Richard M. Danel, Frans Goorman, Rijk O. B. Gans, Martin H. de Borst, and et al. 2019. "Lower Plasma Magnesium, Measured by Nuclear Magnetic Resonance Spectroscopy, is Associated with Increased Risk of Developing Type 2 Diabetes Mellitus in Women: Results from a Dutch Prospective Cohort Study" Journal of Clinical Medicine 8, no. 2: 169. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8020169