Association between Negatively Charged Low-Density Lipoprotein L5 and Subclinical Atherosclerosis in Rheumatoid Arthritis Patients




 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population.
2.2. Determination of Plasma Lipid Profiles and Atherogenic index (AI)
2.3. Measurement of 10-Year Risk of CVD (QRISK-2 Score)
2.4. Isolation and Fractionation of LDL-C
2.5. Anion-Exchange Chromatography Purification of LDL-C Subfractions
2.6. Agarose Gel Electrophoresis of LDL-C Subfractions
2.7. Determination of Protein Expression with Immunoblotting
2.8. Cell Culture
2.9. LOX-1 and LDLR Protein Expression in THP-1 Cells Treated with L1 or L5
2.10. Ultrasound Vascular Imaging of Carotid Arteries
2.11. Statistical Analysis
3. Results
3.1. Clinical Characteristics of RA Patients
3.2. Comparison of Lipid Profiles, QRISK-2 Scores, and AI among RA Patients with or without Subclinical Atherosclerosis and Healthy Controls
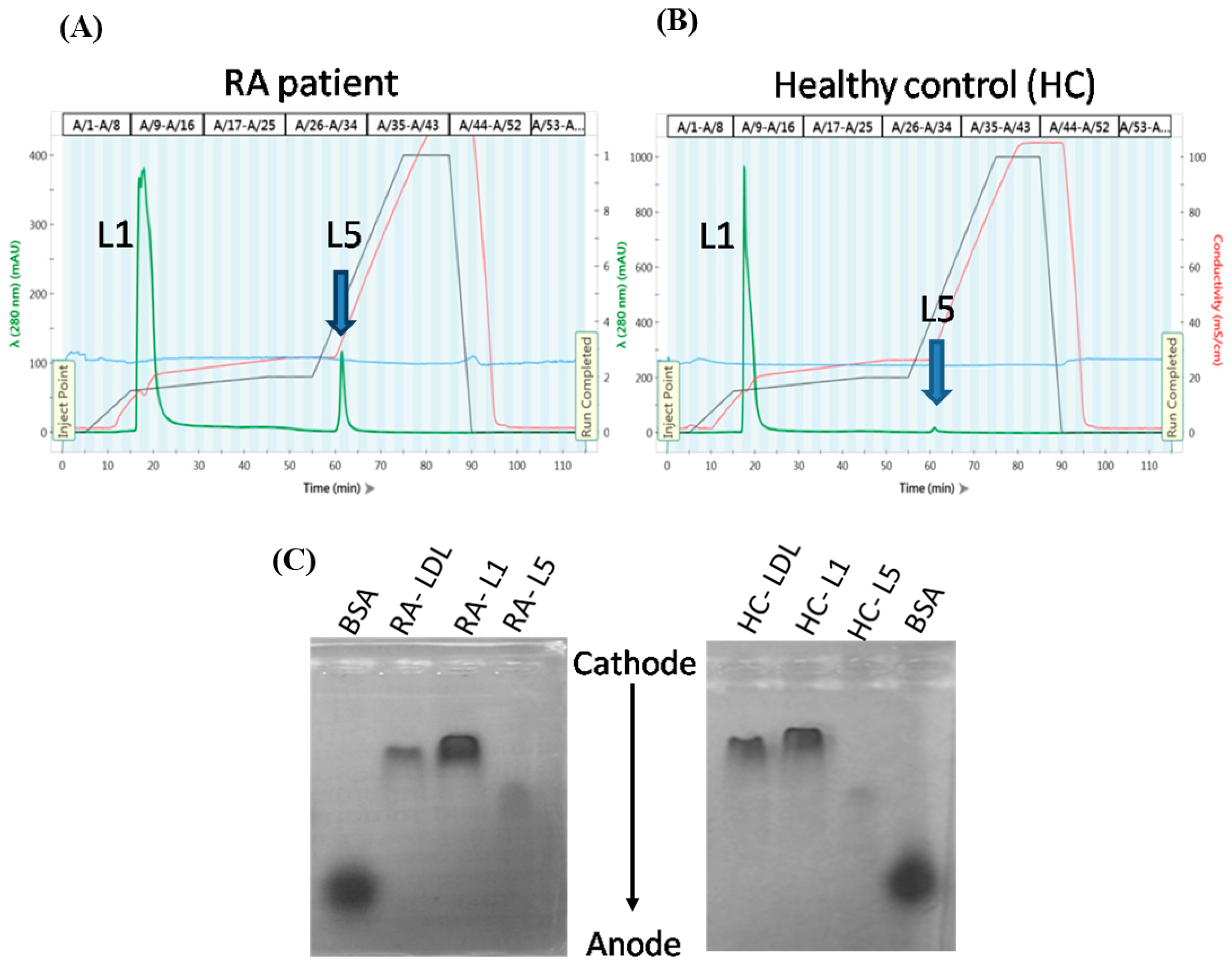
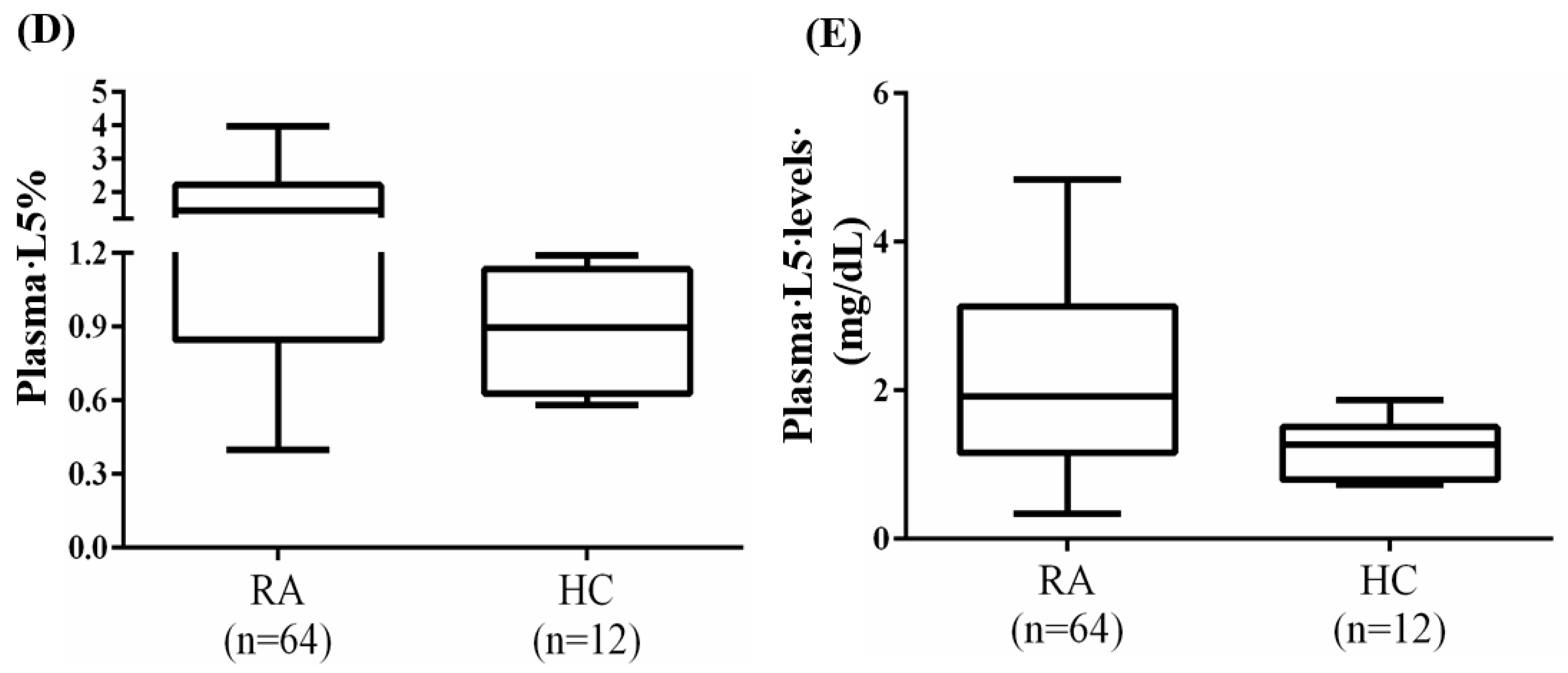
3.3. Increased Plasma L5% and L5 Levels in RA Patients
3.4. The Change of Plasma L5% and L5 Levels in RA Patients after 6-Month Therapy
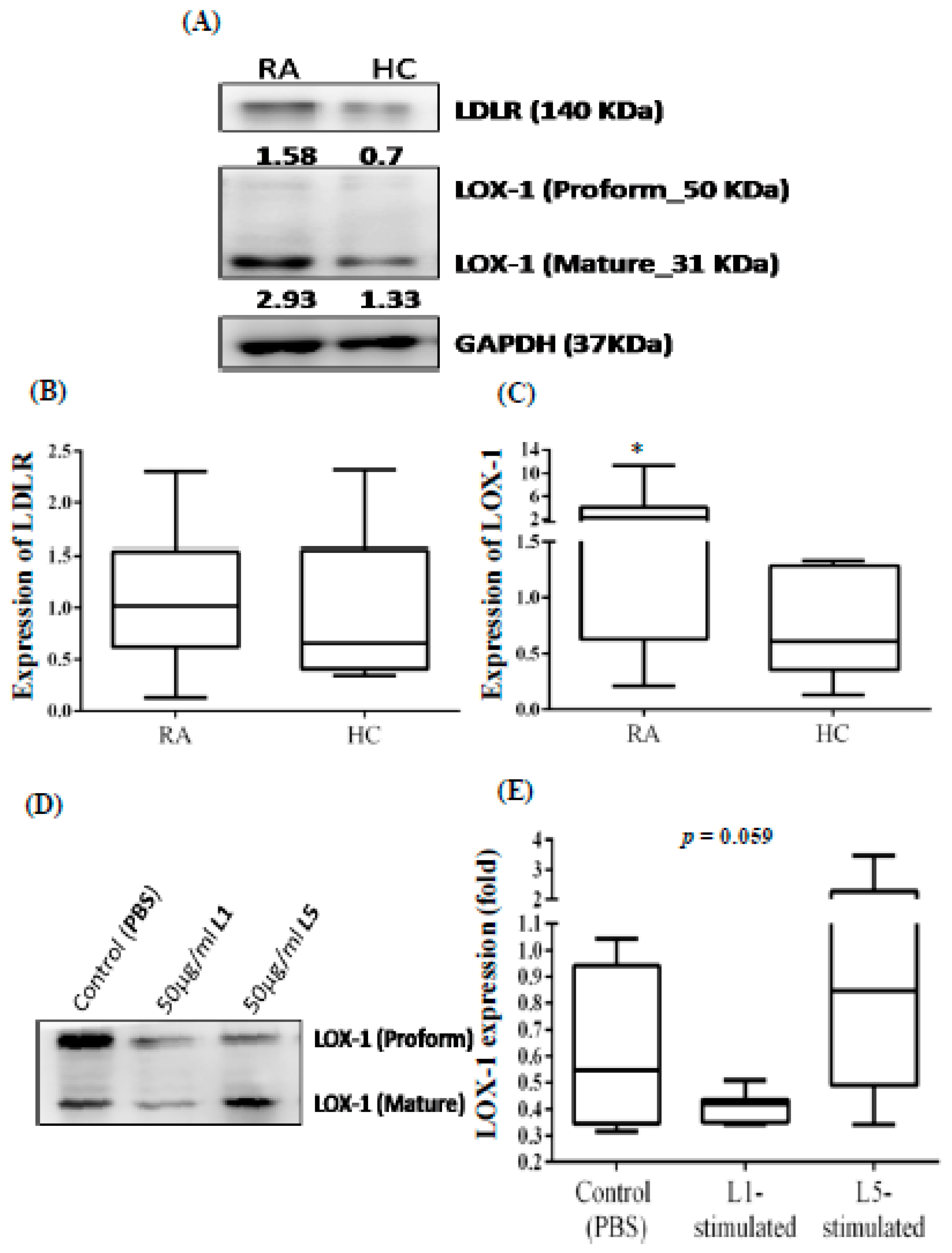
3.5. Increased Expression of LOX-1 in the PBMCs from RA Patients
3.6. Correlation of Plasma L5% and L5 Levels with the Extent of Atherosclerosis, LOX-1 Expression or RA Disease Activity
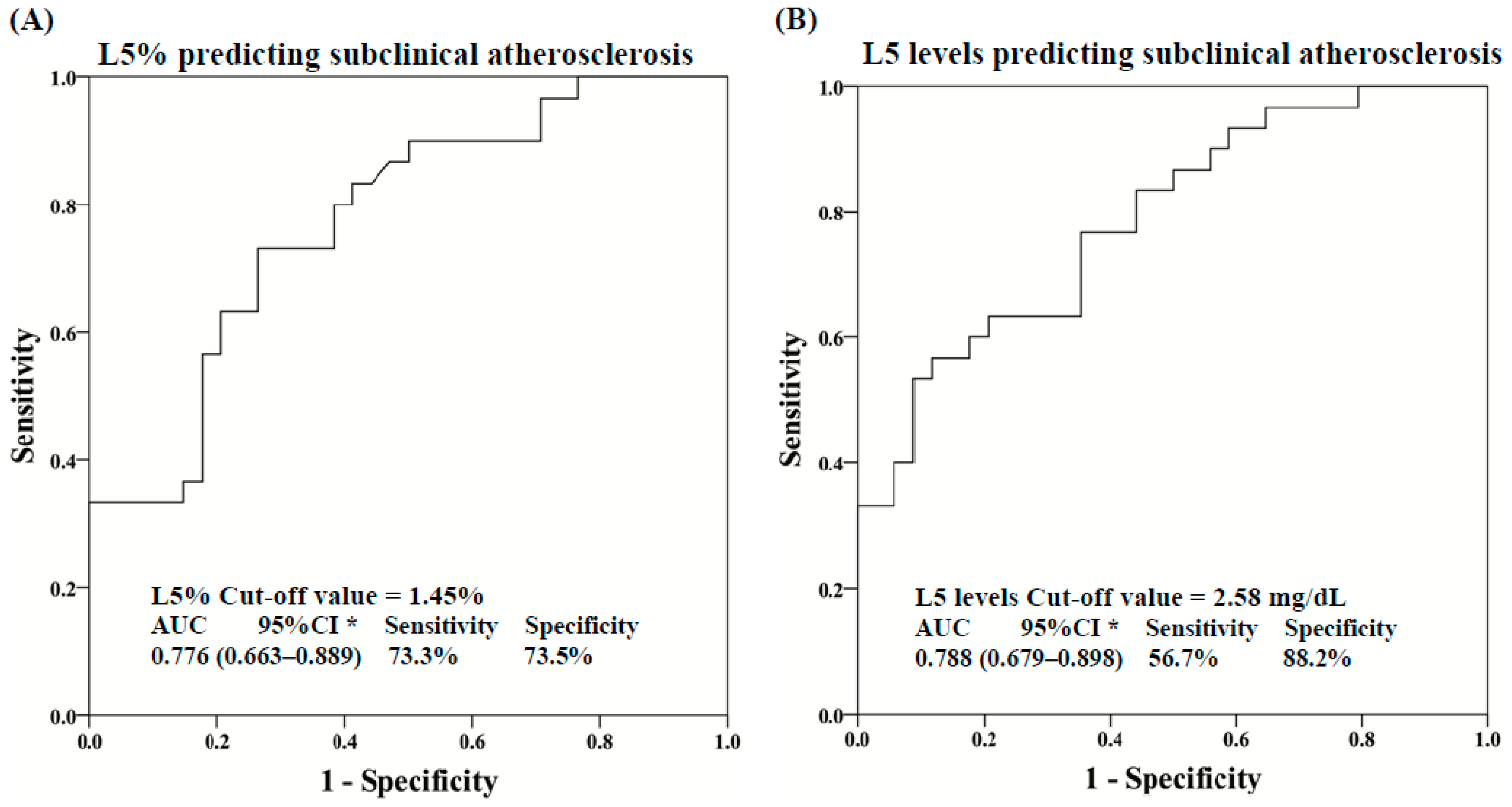
3.7. Multivariate Logistic Regression and ROC Curve Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Libby, P. Inflammation in atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2012, 32, 2045–2051. [Google Scholar] [CrossRef] [PubMed]
- Choy, E.H.; Panayi, G.S. Cytokine pathways and joint inflammation in rheumatoid arthritis. N. Engl. J. Med. 2001, 344, 907–916. [Google Scholar] [CrossRef] [PubMed]
- Firestein, G.S. Evolving concepts of rheumatoid arthritis. Nature 2003, 423, 356–361. [Google Scholar] [CrossRef] [PubMed]
- Avina-Zubieta, J.A.; Thomas, J.; Sadatsafavi, M.; Lehman, A.J.; Lacaille, D. Risk of incident cardiovascular events in patients with rheumatoid arthritis: a meta-analysis of observational studies. Ann. Rheum. Dis. 2012, 71, 1524–1529. [Google Scholar] [CrossRef] [PubMed]
- Symmons, D.P.; Gabriel, S.E. Epidemiology of CVD in rheumatic disease, with a focus on RA and SLE. Nat. Rev. Rheumatol. 2011, 7, 399–408. [Google Scholar] [CrossRef] [PubMed]
- Choy, E.; Ganeshalingam, K.; Semb, A.G.; Szekanecz, Z.; Nurmohamed, M. Cardiovascular risk in rheumatoid arthritis: recent advances in the understanding of the pivotal role of inflammation, risk predictors and the impact of treatment. Rheumatology 2014, 53, 2143–2154. [Google Scholar] [CrossRef] [Green Version]
- Im, C.H.; Kim, N.R.; Kang, J.W.; Kim, J.H.; Kang, J.Y.; Bae, G.B.; Nam, E.J.; Kang, Y.M. Inflammatory burden interacts with conventional cardiovascular risk factors for carotid plaque formation in rheumatoid arthritis. Rheumatology 2015, 54, 808–815. [Google Scholar] [CrossRef]
- Myasoedova, E.; Crowson, C.S.; Kremers, H.M.; Roger, V.L.; Fitz-Gibbon, P.D.; Therneau, T.M.; Gabriel, S.E. Lipid paradox in rheumatoid arthritis: the impact of serum lipid measures and systemic inflammation on the risk of cardiovascular disease. Ann. Rheum. Dis. 2011, 70, 482–487. [Google Scholar] [CrossRef] [Green Version]
- Chen, D.Y.; Chen, Y.M.; Hsieh, T.Y.; Hsieh, C.W.; Lin, C.C.; Lan, J.L. Significant effects of biologic therapy on lipid profiles and insulin resistance in patients with rheumatoid arthritis. Arthritis. Res. Ther. 2015, 17, 52. [Google Scholar] [CrossRef]
- Avogaro, P.; Bon, G.B.; Cazzolato, G. Presence of a modified low density lipoprotein in humans. Arteriosclerosis 1988, 8, 79–87. [Google Scholar] [CrossRef]
- Niccoli, G.; Baca, M.; De Spirito, M.; Parasassi, T.; Cosentino, N.; Greco, G.; Conte, M.; Montone, R.A.; Arcovito, G.; Crea, F. Impact of electronegative low-density lipoprotein on angiographic coronary atherosclerotic burden. Atherosclerosis 2012, 223, 166–170. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.H.; Jiang, T.; Yang, J.H.; Jiang, W.; Lu, J.; Marathe, G.K.; Pownall, H.J.; Ballantyne, C.M.; McIntyre, T.M.; Henry, P.D.; et al. CY Low-density lipoprotein in hypercholesterolemic human plasma induces vascular endothelial cell apoptosis by inhibiting fibroblast growth factor 2 transcription. Circulation 2013, 107, 2102–2108. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Jiang, W.; Yang, J.H.; Chang, P.Y.; Walterscheid, J.P.; Chen, H.H.; Marcelli, M.; Tang, D.; Lee, Y.T.; Liao, W.S.; et al. Electronegative LDL impairs vascular endothelial cell integrity in diabetes by disrupting fibroblast growth factor 2 (FGF2) autoregulation. Diabetes 2008, 57, 158–166. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.Y.; Raya, J.L.; Chen, H.H.; Chen, C.H.; Abe, Y.; Pownall, H.J.; Taylor, A.A.; Smith, C.V. Isolation, characterization, and functional assessment of oxidatively modified subfractions of circulating low-density lipoproteins. Arterioscler. Thromb. Vasc. Biol. 2013, 23, 1083–1090. [Google Scholar] [CrossRef] [PubMed]
- Mello, A.P.; da Silva, I.T.; Abdalla, D.S.; Damasceno, N.R. Electronegative low-density lipoprotein: origin and impact on health and disease. Atherosclerosis 2011, 215, 257–265. [Google Scholar] [CrossRef]
- Sawamura, T.; Kume, N.; Aoyama, T.; Moriwaki, H.; Hoshikawa, H.; Aiba, Y.; Tanaka, T.; Miwa, S.; Katsura, Y.; Kita, T.; et al. An endothelial receptor for oxidized low-density lipoprotein. Nature 1997, 386, 73–77. [Google Scholar] [CrossRef]
- Lu, J.; Yang, J.H.; Burns, A.R.; Chen, H.H.; Tang, D.; Walterscheid, J.P.; Suzuki, S.; Yang, C.Y.; Sawamura, T.; Chen, C.H. Mediation of electronegative low-density lipoprotein signaling by LOX-1: a possible mechanism of endothelial apoptosis. Circ. Res. 2009, 104, 619–627. [Google Scholar] [CrossRef]
- Chen, C.Y.; Hsu, H.C.; Lee, A.S.; Tang, D.; Chow, L.P.; Yang, C.Y.; Chen, H.; Lee, Y.T.; Chen, C.H. The most negatively charged low-density lipoprotein L5 induces stress pathways in vascular endothelial cells. J. Vasc. Res. 2012, 49, 329–341. [Google Scholar] [CrossRef]
- Takanabe-Mori, R.; Ono, K.; Wada, H.; Takaya, T.; Ura, S.; Yamakage, H.; Satoh-Asahara, N.; Shimatsu, A.; Takahashi, Y.; Fujita, M.; Fujita, Y.; et al. Lectin-like oxidized low-density lipoprotein receptor-1 plays an important role in vascular inflammation in current smokers. J. Atheroscler. Thromb. 2013, 20, 585–590. [Google Scholar] [CrossRef]
- Ishino, S.; Mukai, T.; Kume, N.; Asano, D.; Ogawa, M.; Kuge, Y.; Minami, M.; Kita, T.; Shiomi, M.; Saji, H. Lectin-like oxidized LDL receptor-1 (LOX-1) expression is associated with atherosclerotic plaque instability--analysis in hypercholesterolemic rabbits. Atherosclerosis 2007, 195, 48–56. [Google Scholar] [CrossRef]
- Kataoka, H.; Kume, N.; Miyamoto, S.; Minami, M.; Moriwaki, H.; Murase, T.; Sawamura, T.; Masaki, T.; Hashimoto, N.; Kita, T. Expression of lectinlike oxidized low-density lipoprotein receptor-1 in human atherosclerotic lesions. Circulation 1999, 99, 3110–3117. [Google Scholar] [CrossRef] [PubMed]
- Mehta, J.L.; Sanada, N.; Hu, C.P.; Chen, J.; Dandapat, A.; Sugawara, F.; Satoh, H.; Inoue, K.; Kawase, Y.; Jishage, K.; et al. Deletion of LOX-1 reduces atherogenesis in LDLR knockout mice fed high cholesterol diet. Circ. Res. 2007, 100, 1634–1642. [Google Scholar] [CrossRef] [PubMed]
- Agca, R.; Heslinga, S.C.; Rollefstad, S.; Heslinga, M.; McInnes, I.B.; Peters, M.J.; Kvien, K.; Dougados, M.; Radner, H.; Atzeni, F.; et al. EULAR recommendations for cardiovascular disease risk management in patients with rheumatoid arthritis and other forms of inflammatory joint disorders: 2015/2016 update. Ann. Rheum. Dis. 2017, 76, 17–28. [Google Scholar] [CrossRef]
- Corrales, A.; Gonzalez-Juanatey, C.; Peiro, M.E.; Blanco, R.; Llorca, J.; Gonzalez-Gay, M.A. Carotid ultrasound is useful for the cardiovascular risk stratification of patients with rheumatoid arthritis: results of a population-based study. Ann. Rheum. Dis. 2014, 73, 722–727. [Google Scholar] [CrossRef]
- Evans, M.R.; Escalante, A.; Battafarano, D.F.; Freeman, G.L.; O’Leary, D.H.; del Rincon, I. Carotid atherosclerosis predicts incident acute coronary syndromes in rheumatoid arthritis. Arthritis Rheum. 2011, 63, 1211–1220. [Google Scholar] [CrossRef] [Green Version]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O., 3rd; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Ann. Rheum. Dis. 2010, 69, 1580–1588. [Google Scholar] [CrossRef] [PubMed]
- Prevoo, M.L.; van ’t Hof, M.A.; Kuper, H.H.; van Leeuwen, M.A.; van de Putte, L.B.; van Riel, P. Modified disease activity scores that include twenty-eight-joint counts. Development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheum. 1995, 38, 44–48. [Google Scholar] [CrossRef]
- Hippisley-Cox, J.; Coupland, C.; Vinogradova, Y.; Robson, J.; Minhas, R.; Sheikh, A.; Brindle, P. Predicting cardiovascular risk in England and Wales: prospective derivation and validation of QRISK2. BMJ 2008, 336, 1475–1482. [Google Scholar] [CrossRef] [Green Version]
- ClinRisk Ltd. Welcome to the QRISK®2-2017 risk calculator. 2007. Available online: https://www.qrisk.org (accessed on 1 May 2017).
- D’Agostino, R.B.S.; Vasan, R.S.; Pencina, M.J.; Wolf, P.A.; Cobain, M.; Massaro, J.M.; Kannel, W.B. General Cardiovascular Risk Profile for Use in Primary Care: The Framingham Heart Study. Circulation 2008, 117, 743–753. [Google Scholar] [CrossRef] [Green Version]
- Eric, J. Topol, Medscape 1994. Framingham 10 Year Risk of General Cardiovascular Disease (2008 paper). Available online: https://reference.medscape.com/calculator/framingham-cardiovascular-disease-risk (accessed on 16 June 2015).
- Bradford, M.M. A rapid and sensitive method for the quantitation of microgram quantities of protein utilizing the principle of protein-dye binding. Anal. Biochem. 1976, 72, 248–254. [Google Scholar] [CrossRef]
- Boyer, J.F.; Gourraud, P.A.; Cantagrel, A.; Davignon, J.L.; Constantin, A. Traditional cardiovascular risk factors in rheumatoid arthritis: A meta-analysis. Joint Bone Spine 2011, 78, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.T.; Wang, G.J.; Kuo, C.C.; Hsieh, J.Y.; Lee, A.S.; Chang, C.M.; Wang, C.C.; Shen, M.Y.; Huang, C.C.; Sawamura, T.; et al. Electronegative low-density lipoprotein increases coronary artery disease risk in uremia ratients on maintenance hemodialysis. Medicine 2016, 95, e2265. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Quesada, J.L.; Benitez, S.; Ordonez-Llanos, J. Electronegative low-density lipoprotein. Curr. Opin. Lipidol. 2004, 15, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Rigla, M.; Sánchez-Quesada, J.L.; Ordóñez-Llanos, J.; Prat, T.; Caixas, A.; Jorba, O.; Serra, J.R.; de Leiva, A.; Perez, A. Effect of physical exercise on lipoprotein(a) and low-density lipoprotein modifications in type 1 and type 2 diabetic patients. Metabolism 2000, 49, 640–647. [Google Scholar] [CrossRef]
- Lindhardsen, J.; Ahle, O.-O.; Gislason, G.H.; Madsen, O.R.; Olesen, J.B.; Torp-Pedersen, C.; Hansen, P.R. The risk of myocardial infarction in rheumatoid arthritis and diabetes mellitus: a Danish nationwide cohort study. Ann. Rheum. Dis. 2011, 70, 929–934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, C.P.; Giles, J.T.; Kronmal, R.A.; Post, W.S.; Gelber, A.C.; Petri, M.; Szklo, M.; Detrano, R.; Budoff, M.J.; Blumenthal, R.S.; et al. Progression of coronary artery atherosclerosis in rheumatoid arthritis: comparison with participants from the Multi-Ethnic Study of Atherosclerosis. Arthritis Res. Ther. 2013, 15, R134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, C.T.; Shen, M.Y.; Lee, A.S.; Wang, C.C.; Chen, W.Y.; Chang, C.M.; Chang, K.C.; Stancel, N.; Chen, C.H. Electronegative low-density lipoprotein increases the risk of ischemic lower-extremity peripheral artery disease in uremia patients on maintenance hemodialysis. Sci. Rep. 2017, 7, 4654. [Google Scholar] [CrossRef]
- Wagan, A.A.; Mahmud, T.E.; Rasheed, A.; Zafar, Z.A.; Rehman, A.U.; Ali, A. Cardiovascular risk score in rheumatoid arthritis. Pak. J. Med. Sci. 2016, 32, 534–538. [Google Scholar] [CrossRef]
- Ishikawa, M.; Ito, H.; Akiyoshi, M.; Kume, N.; Yoshitomi, H.; Mitsuoka, H.; Tanida, S.; Murata, K.; Shibuya, H.; Kasahara, T.; et al. Lectin-like oxidized low-density lipoprotein receptor 1 signal is a potent biomarker and therapeutic target for human rheumatoid arthritis. Arthritis Rheum. 2012, 64, 1024–1034. [Google Scholar] [CrossRef] [Green Version]
- Ke, L.Y.; Engler, D.A.; Lu, J.; Matsunami, R.K.; Chan, H.C.; Wang, G.J.; Yang, C.Y.; Chang, J.G.; Chen, C.H. Chemical composition-oriented receptor selectivity of L5, a naturally occurring atherogenic low-density lipoprotein. Pure Appl. Chem. 2011, 83. [Google Scholar] [CrossRef]
- Chu, C.S.; Ke, L.Y.; Chan, H.C.; Chen, C.C.; Cheng, K.H. Four statin benefit groups defined by the 2013 ACC/AHA new cholesterol guideline are characterized by increased plasma level of electronegative low-density lipoprotein. Acta Cardiol. Sin. 2016, 32, 667–675. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| RA with Subclinical Atherosclerosis (n = 30) | RA without Subclinical Atherosclerosis (n = 34) | Healthy Controls (n = 12) | |
|---|---|---|---|
| Median age at entry, years | 63.5 ± 9.1 b | 56.6 ± 11.5 | 55.1 ± 6.5 |
| Women | 23 (76.7%) | 27 (79.4%) | 9 (75.0%) |
| Duration of RA, months | 81.8 ± 20.5 | 72.3±22.6 | NA |
| Body mass index, kg/m2 | 23.0 ± 2.8 | 21.7 ± 3.0 | 21.4 ± 2.3 |
| RF positivity | 21 (70.0%) | 22 (64.7%) | NA |
| ACPA positivity | 19 (63.3%) | 21 (61.8%) | NA |
| ESR at entry, mm/1st hour | 18.0 ± 12.6 | 18.0 ± 20.2 | NA |
| CRP at entry, mg/dL | 0.52 ± 0.53 | 0.42 ± 0.67 | NA |
| DAS28 at entry | 3.50 ± 0.89 | 3.52 ± 1.29 | NA |
| Daily steroid dose, mg/day | 3.8 ± 1.6 | 4.0 ± 2.3 | NA |
| csDMARDs used at entry | NA | ||
| Methotrexate | 25 (83.3%) | 28 (82.4%) | NA |
| Sulfasalazine | 14 (46.7%) | 15 (44.1%) | NA |
| Hydroxychloroquine | 12 (40.0%) | 13 (38.2%) | NA |
| Biologics used at entry | |||
| TNF-α inhibitors | 10 (33.3%) | 12 (35.3%) | NA |
| IL-6 receptor inhibitor | 8 (26.7%) | 10 (29.4%) | NA |
| Rituximab | 2 (6.7%) | 2 (5.9%) | NA |
| Hypertension | 15 (50.0%) † | 7 (20.6%) | 1 (8.3%) |
| Diabetes mellitus | 5 (16.7%) | 2 (5.9%) | 0 (0.0%) |
| Current smoker | 4 (13.3%) | 4 (11.8%) | 1 (8.3%) |
| Total cholesterol, mg/dL | 219 (193–245) | 225 (201–247) | 208 (201–231) |
| HDL-C, mg/dL | 58.5 (48.0–66.0) | 72.5 (56.8–86.0) c | 59.0 (46.3–77.8) |
| Triglyceride, mg/dL | 123 (87–170) | 94 (67.5–145) | 90 (72.8–126) |
| LDL-C, mg/dL | 142 (111–168) | 148 (106–154) | 131 (120–155) |
| Atherogenic index | 3.8 (2.8–4.7) | 3.1 (2.6–3.9) | 3.5 (2.9–4.8) |
| QRISK-2 scores | 9.3 (5.5–14.0) d | 5.4 (2.3–8.7) | 3.8 (2.9–5.0) |
| Framingham score (%) | 13.4 (8.5–19.4) e | 5.4 (3.8–5.4) | 3.6 (2.5–5.0) |
| CVD events | 3 (10.0%) f | 0 (0.0%) | 0 (0.0%) |
| Plasma LDL-C Levels | LDLR Expression | Plasma L5% | Plasma L5 Levels | LOX-1 Expression | |
|---|---|---|---|---|---|
| Right ccIMT, mm | 0.217 | 0.150 | 0.537 b | 0.611 b | 0.457 b |
| Left ccIMT, mm | 0.245 | 0.223 | 0.457 b | 0.540 b | 0.507 b |
| QRISK-2 scores | 0.072 | 0.244 | 0.256 a | 0.278 a | 0.339 a |
| Framingham score (%) | 0.160 | 0.336a | 0.107 | 0.188 | 0.251 |
| Atherogenic index | 0.635 b | 0.294 a | −0.024 | 0.281 a | 0.318 a |
| LDL-C levels | - | 0.181 | −0.107 | 0.298 a | 0.117 |
| LDLR expression | 0.181 | - | 0.102 | 0.182 | 0.298 a |
| Plasma L5% | −0.107 | 0.102 | - | 0.895b | 0.497 b |
| Plasma L5 levels | 0.298 a | 0.182 | 0.895 b | - | 0.588 b |
| LOX-1 expression | 0.117 | 0.298 a | 0.497 b | 0.588 b | - |
| Body mass index | 0.056 | 0.108 | 0.300 a | 0.317 a | 0.458 b |
| DAS28 at entry | −0.225 | −0.015 | 0.361 b | 0.254 a | 0.166 |
| Risk Factors | Odds Ratio | 95% Confidence Interval | P Value |
|---|---|---|---|
| Univariate | |||
| Age | 1.07 | 1.01–1.14 | 0.017 |
| Sex (female) | 0.26 | 0.08–0.86 | 0.027 |
| Body mass index | 1.17 | 0.98–1.40 | 0.085 |
| Smoking | 1.15 | 0.26–5.08 | 0.850 |
| Hypertension | 3.86 | 1.29–11.55 | 0.016 |
| Diabetes mellitus | 3.20 | 0.57–17.89 | 0.185 |
| RA duration | 1.02 | 0.997–1.05 | 0.089 |
| Steroid daily dose | 0.94 | 0.74–1.21 | 0.656 |
| RF positivity | 1.27 | 0.44–3.64 | 0.653 |
| ACPA positivity | 1.07 | 0.39–2.95 | 0.897 |
| ESR | 1.00 | 0.97–1.03 | 0.994 |
| CRP | 1.30 | 0.58–3.03 | 0.505 |
| DAS28 score | 0.99 | 0.63–1.54 | 0.964 |
| Total cholesterol | 1.00 | 0.99–1.01 | 0.622 |
| Total triglyceride | 1.01 | 0.996–1.01 | 0.285 |
| HDL-C | 0.97 | 0.94–0.995 | 0.022 |
| LDL-C | 1.00 | 0.99–1.00 | 0.579 |
| L5% | 2.95 | 1.34–6.50 | 0.007 |
| L5 levels | 1.01 | 1.002–1.01 | 0.007 |
| QRISK-2 scores | 1.16 | 1.05–1.29 | 0.005 |
| Atherogenic index | 1.60 | 0.96–2.65 | 0.069 |
| Multivariate | |||
| Age | 1.27 | 1.04–1.55 | 0.021 |
| Sex (female) | 0.15 | 0.02–1.09 | 0.061 |
| RA duration | 1.01 | 0.97–1.05 | 0.580 |
| Hypertension | 5.21 | 0.84–32.32 | 0.076 |
| HDL-C | 0.96 | 0.91–1.01 | 0.120 |
| L5% | 4.94 | 1.48–16.48 | 0.009 |
| L5 levels | 1.01 | 1.001–1.02 | 0.010 |
| QRISK-2 scores | 0.96 | 0.92–1.01 | 0.120 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, C.-Y.; Chen, C.-H.; Chen, Y.-M.; Hsieh, T.-Y.; Li, J.-P.; Shen, M.-Y.; Lan, J.-L.; Chen, D.-Y. Association between Negatively Charged Low-Density Lipoprotein L5 and Subclinical Atherosclerosis in Rheumatoid Arthritis Patients. J. Clin. Med. 2019, 8, 177. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8020177
Chang C-Y, Chen C-H, Chen Y-M, Hsieh T-Y, Li J-P, Shen M-Y, Lan J-L, Chen D-Y. Association between Negatively Charged Low-Density Lipoprotein L5 and Subclinical Atherosclerosis in Rheumatoid Arthritis Patients. Journal of Clinical Medicine. 2019; 8(2):177. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8020177
Chicago/Turabian StyleChang, Chun-Yu, Chu-Huang Chen, Yi-Ming Chen, Tsu-Yi Hsieh, Ju-Pi Li, Ming-Yi Shen, Joung-Liang Lan, and Der-Yuan Chen. 2019. "Association between Negatively Charged Low-Density Lipoprotein L5 and Subclinical Atherosclerosis in Rheumatoid Arthritis Patients" Journal of Clinical Medicine 8, no. 2: 177. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8020177