Use of Secukinumab in a Cohort of Erythrodermic Psoriatic Patients: A Pilot Study

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Experimental Section
3. Results
3.1. Study Population
3.2. Drug History
3.3. Drug Abuses and Comorbidities
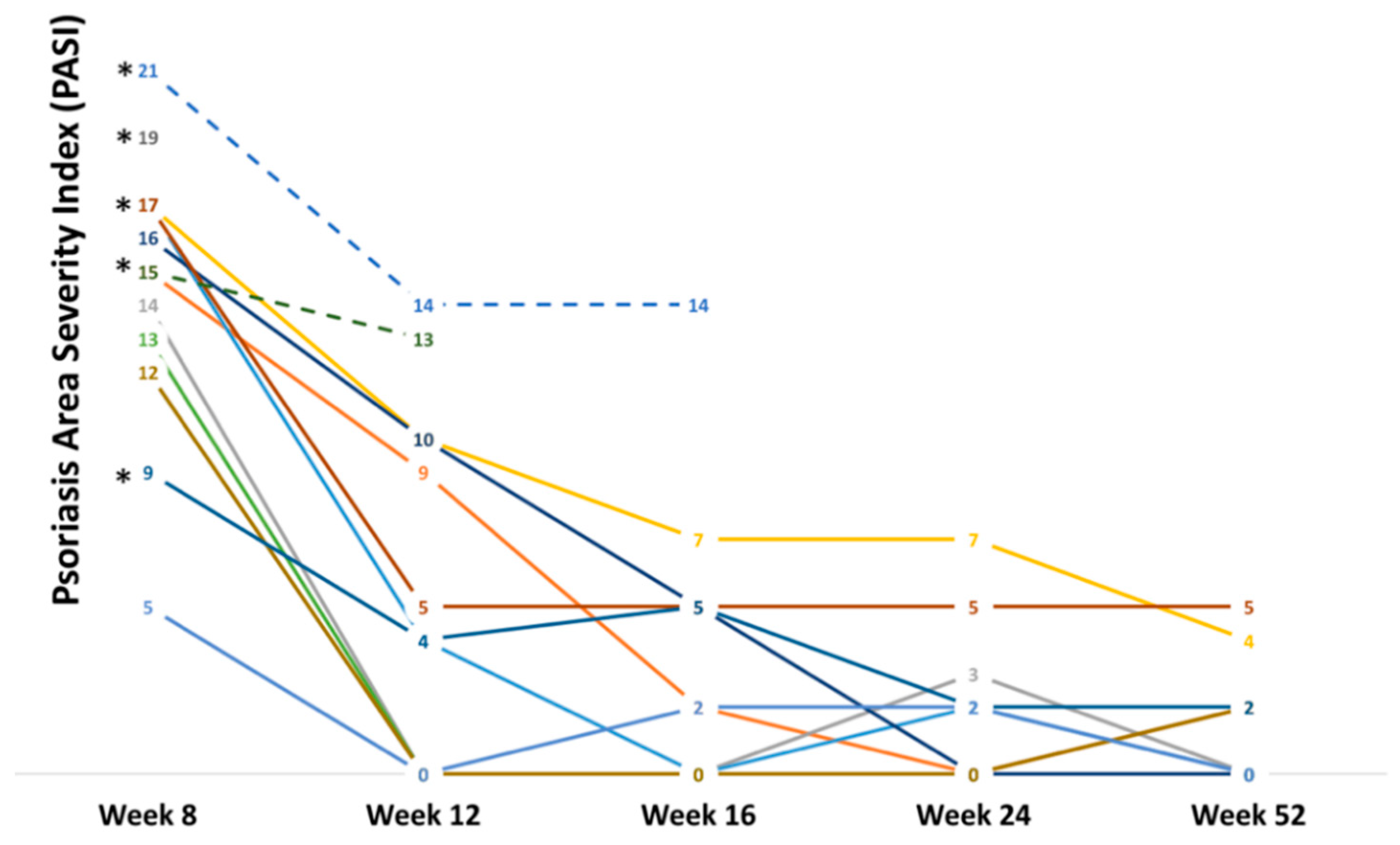
3.4. Clinical Response to Secukinumab
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Singh, R.K.; Lee, K.M.; Ucmak, D.; Brodsky, M.; Atanelov, Z.; Farahnik, B.; Abrouk, M.; Nakamura, M.; Zhu, T.H.; Liao, W. Erythrodermic psoriasis: Pathophysiology and current treatment perspectives. Psoriasis (Auckl) 2016, 6, 93–104. [Google Scholar]
- Rosenbach, M.; Hsu, S.; Korman, N.J.; Lebwohl, M.G.; Young, M.; Bebo, B.F., Jr.; Van Voorhees, A.S.; National Psoriasis Foundation Medical Board. Treatment of erythrodermic psoriasis: From the medical board of the National Psoriasis Foundation. J. Am. Acad. Dermatol. 2010, 62, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Nast, A.; Gisondi, P.; Ormerod, A.D.; Saiag, P.; Smith, C.; Spuls, P.I.; Arenberger, P.; Bachelez, H.; Barker, J.; Dauden, E.; et al. European S3-Guidelines on the systemic treatment of psoriasis vulgaris--Update 2015--Short version--EDF in cooperation with EADV and IPC. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 2277–2294. [Google Scholar] [CrossRef] [PubMed]
- Mateu-Puchades, A.; Santos-Alarcón, S.; Martorell-Calatayud, A.; Pujol-Marco, C.; Sánchez-Carazo, J.L. Erythrodermic psoriasis and secukinumab: Our clinical experience. Dermatol. Ther. 2018, 31, e12607. [Google Scholar] [CrossRef] [PubMed]
- Weng, H.J.; Wang, T.S.; Tsai, T.F. Clinical experience of secukinumab in the treatment of erythrodermic psoriasis: A case series. Br. J. Dermatol. 2018, 178, 1439–1440. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Han, J.; Qureshi, A.A. Smoking and risk of incident psoriatic arthritis in US women. Ann. Rheum. Dis. 2012, 71, 804–808. [Google Scholar] [CrossRef]
- Hojgaard, P.; Glintborg, B.; Hetland, M.L.; Hansen, T.H.; Lage-Hansen, P.R.; Petersen, M.H.; Holland-Fischer, M.; Nilsson, C.; Loft, A.G.; Andersen, B.N.; et al. Association between tobacco smoking and response to tumour necrosis factor alpha inhibitor treatment in psoriatic arthritis: Results from the DANBIO registry. Ann. Rheum. Dis. 2015, 74, 2130–2136. [Google Scholar] [CrossRef]
- Qureshi, A.A.; Dominguez, P.L.; Choi, H.; Han, J.; Curhan, G. Alcohol intake and risk of incident psoriasis in US women: A prospective study. Arch. Dermatol. 2010, 146, 1364–1369. [Google Scholar] [CrossRef] [PubMed]
- Farkas, A.; Kemeny, L. Alcohol, liver, systemic inflammation and skin: A focus on patients with psoriasis. Skin Pharmacol. Physiol. 2013, 26, 119–126. [Google Scholar] [CrossRef]
- Poikolainen, K.; Reunala, T.; Karvonen, J.; Lauharanta, J.; Kärkkäinen, P. Alcohol intake: A risk factor for psoriasis in young and middle aged men? BMJ 1990, 300, 780–783. [Google Scholar] [CrossRef] [PubMed]
- Katz-Talmor, D.; Katz, I.; Porat-Katz, B.S.; Shoenfeld, Y. Cannabinoids for the treatment of rheumatic diseases—Where do we stand? Nat. Rev. Rheumatol. 2018, 14, 488–498. [Google Scholar] [CrossRef]
- Galluzzo, M.; Talamonti, M.; De Simone, C.; D’Adamio, S.; Moretta, G.; Tambone, S.; Caldarola, G.; Fargnoli, M.C.; Peris, K.; Bianchi, L. Secukinumab in moderate-to-severe plaque psoriasis: A multi-center, retrospective, real-life study up to 52 weeks observation. Expert Opin. Biol. Ther. 2018, 18, 727–735. [Google Scholar] [CrossRef]
- Damiani, G.; Conic, R.R.Z.; de Vita, V.; Costanzo, A.; Regazzini, R.; Pigatto, P.D.M.; Bragazzi, N.L.; Pacifico, A.; Malagoli, P. When IL-17 inhibitors fail: Real-life evidence to switch from secukinumab to adalimumab or ustekinumab. Dermatol. Ther. 2018, e12793. [Google Scholar] [CrossRef]
- van Vugt, L.J.; van den Reek, J.M.P.A.; Hannink, G.; Coenen, M.J.H.; de Jong, E.M.G.J. Association of HLA-C*06:02 Status with Differential Response to Ustekinumab in Patients With Psoriasis: A Systematic Review and Meta-analysis. JAMA Dermatol. 2019. [Google Scholar] [CrossRef]
- Zaba, L.C.; Suárez-Fariñas, M.; Fuentes-Duculan, J.; Nograles, K.E.; Guttman-Yassky, E.; Cardinale, I.; Lowes, M.A.; Krueger, J.G. Effective treatment of psoriasis with etanercept is linked to suppression of IL-17 signaling, not immediate response TNF genes. J. Allergy Clin. Immunol. 2009, 124, 1022–1030.e395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong, E.J.; Harskamp, C.T.; Dhillon, J.S.; Armstrong, A.W. Psoriasis and smoking: A systematic review and meta-analysis. Br. J. Dermatol. 2014, 170, 304–314. [Google Scholar] [CrossRef] [PubMed]
- Brenaut, E.; Horreau, C.; Pouplard, C.; Barnetche, T.; Paul, C.; Richard, M.A.; Joly, P.; Le Maître, M.; Aractingi, S.; Aubin, F.; et al. Alcohol consumption and psoriasis: A systematic literature review. J. Eur. Acad. Dermatol. Venereol. 2013, 27, 30–35. [Google Scholar] [CrossRef]
- Fortes, C.; Mastroeni, S.; Leffondré, K.; Sampogna, F.; Melchi, F.; Mazzotti, E.; Pasquini, P.; Abeni, D. Relationship between smoking and the clinical severity of psoriasis. Arch. Dermatol. 2005, 141, 1580–1584. [Google Scholar] [CrossRef] [PubMed]
- Richer, V.; Roubille, C.; Fleming, P.; Starnino, T.; McCourt, C.; McFarlane, A.; Siu, S.; Kraft, J.; Lynde, C.; Pope, J.E.; et al. Psoriasis and smoking: A systematic literature review and meta-analysis with qualitative analysis of effect of smoking on psoriasis severity. J. Cutan. Med. Surg. 2016, 20, 221–227. [Google Scholar] [CrossRef]
- Armstrong, A.W.; Armstrong, E.J.; Fuller, E.N.; Sockolov, M.E.; Voyles, S.V. Smoking and pathogenesis of psoriasis: A review of oxidative, inflammatory and genetic mechanisms. Br. J. Dermatol. 2011, 165, 1162–1168. [Google Scholar] [CrossRef]
- Wilkinson, J.D.; Williamson, E.M. Cannabinoids inhibit human keratinocyte proliferation through a non-CB1/CB2 mechanism and have a potential therapeutic value in the treatment of psoriasis. J. Dermatol. Sci. 2007, 45, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Kozela, E.; Juknat, A.; Kaushansky, N.; Rimmerman, N.; Ben-Nun, A.; Vogel, Z. Cannabinoids decrease the th17 inflammatory autoimmune phenotype. J. Neuroimmune Pharmacol. 2013, 8, 1265–1276. [Google Scholar] [CrossRef] [PubMed]
- Dhadwal, G.; Kirchhof, M.G. The Risks and Benefits of Cannabis in the Dermatology Clinic. J. Cutan. Med. Surg. 2018, 22, 194–199. [Google Scholar] [CrossRef]
- Russo, E.B. Taming THC: Potential cannabis synergy and phytocannabinoid-terpenoid entourage effects. Br. J. Pharmacol. 2011, 163, 1344–1364. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | EP (n = 13) |
|---|---|
| Last anti-psoriatic therapy (N (%)) | |
| Methotrexate | 1 (7.7) |
| Phototherapy | 1 (7.7) |
| Adalimumab | 4 (30.8) |
| Etanercept | 2 (15.4) |
| Ustekinumab | 2 (15.4) |
| Apremilast | 1 (7.7) |
| Combination therapy (MTX + Etanercept) | 3 (23.1) |
| Biologics naïve (N (%)) | 3 (23.1) |
| Biologics switching (N (%)) | 10 (76.9) |
| 1 | 2 (20.0) |
| 2 | 5 (50.0) |
| 3 | 1 (10.0) |
| >3 | 2 (20.0) |
| Other drugs capable to aggravate psoriasis (N (%)) | |
| Beta-blockers | 4 (30.8) |
| ACE inhibitors | 2 (15.4) |
| ARBs | 3 (23.1) |
| Thiazides diuretics | 1 (7.7) |
| Addictions | EP (n = 13) |
|---|---|
| Smokers (N (%)) | 7 (53.8) |
| Pack/year (median (IQR)) | 295 (190–365) |
| AUDIT test (median ± SD) | 9 (4–14) |
| Zone I (0–7 points) (N (%)) | 6 (46.2) |
| Zone II (8–15 points) (N (%)) | 6 (46.2) |
| Zone III (16–19 points) (N (%)) | 1 (7.7) |
| Zone IV (20–40 points) (N (%)) | 0 (0.0) |
| Cannabis use (N (%)) | 3 (23.1) |
| Variables | EP (n = 13) |
|---|---|
| Last control PASI (median (IQR)) | 10 (7–15) |
| Secukinumab responders (N (%)) | 10 (76.9) |
| Secukinumab non-responders (N (%)) | 3 (23.1) |
| Previous erythroderma episodes (N (%)) | 8 (61.5) |
| 1 | 2 (25.0) |
| 2 | 3 (37.5) |
| 3 | 1 (12.5) |
| >3 | 2 (25.0) |
| Erythroderma clearing time (median (IQR), weeks) | 3 (1–5.3) |
| PASI (median (IQR)) | |
| Week 8 | 15 (13–17) |
| PASI 75 (N (%)) | 4 (30.8) |
| PASI 90 (N (%)) | 0 (0.0) |
| PASI 100 (N (%)) | 0 (0.0) |
| Week 12 | 4.5 (0–10) |
| PASI 75 (N (%)) | 5 (38.5) |
| PASI 90 (N (%)) | 3 (23.1) |
| PASI 100 (N (%)) | 4 (30.8) |
| Week 16 | 2 (0–5) |
| PASI 75 (N (%)) | 1 (7.7) |
| PASI 90 (N (%)) | 5 (38.5) |
| PASI 100 (N (%)) | 4 (30.8) |
| Week 24 | 2 (0–2.75) |
| PASI 75 (N (%)) | 1 (7.7) |
| PASI 90 (N (%)) | 5 (38.5) |
| PASI 100 (N (%)) | 4 (30.8) |
| DLQI (median (IQR)) | |
| Week 8 | 17 (13–22) |
| Week 12 | 12 (9–17) |
| Week 16 | 11 (7–16) |
| Week 24 | 8 (6–12) |
| Week 52 | 8 (5–12) |
| Side effects (N (%)) | 5 (38.5) |
| Recurrent oral candidiasis | 1 (20.0) |
| Urticaria | 1 (20.0) |
| Injection-site pain | 3 (60.0) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Damiani, G.; Pacifico, A.; Russo, F.; Pigatto, P.D.M.; Bragazzi, N.L.; Bonifati, C.; Morrone, A.; Watad, A.; Adawi, M. Use of Secukinumab in a Cohort of Erythrodermic Psoriatic Patients: A Pilot Study. J. Clin. Med. 2019, 8, 770. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8060770
Damiani G, Pacifico A, Russo F, Pigatto PDM, Bragazzi NL, Bonifati C, Morrone A, Watad A, Adawi M. Use of Secukinumab in a Cohort of Erythrodermic Psoriatic Patients: A Pilot Study. Journal of Clinical Medicine. 2019; 8(6):770. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8060770
Chicago/Turabian StyleDamiani, Giovanni, Alessia Pacifico, Filomena Russo, Paolo Daniele Maria Pigatto, Nicola Luigi Bragazzi, Claudio Bonifati, Aldo Morrone, Abdulla Watad, and Mohammad Adawi. 2019. "Use of Secukinumab in a Cohort of Erythrodermic Psoriatic Patients: A Pilot Study" Journal of Clinical Medicine 8, no. 6: 770. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8060770