Congenital Heart Defects in Monochorionic Twins: A Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Methods
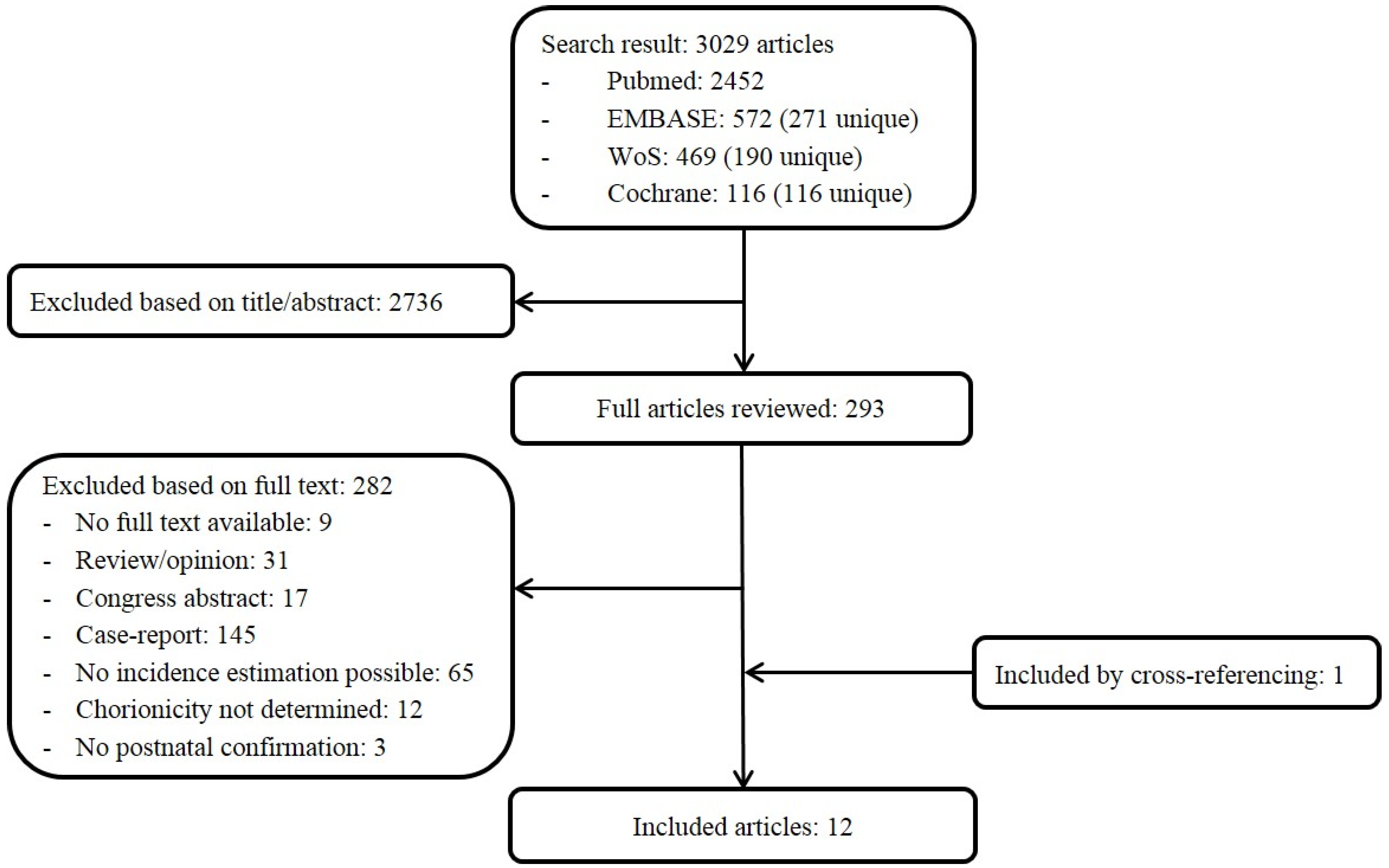
2.1. Search Strategy
2.2. Quality Assessment
2.3. Data Extraction
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Van der Linde, D.; Konings, E.E.; Slager, M.A.; Witsenburg, M.; Helbing, W.A.; Takkenberg, J.J.; Roos-Hesselink, J.W. Birth prevalence of congenital heart disease worldwide: A systematic review and meta-analysis. J. Am. Coll. Cardiol. 2011, 58, 2241–2247. [Google Scholar] [CrossRef]
- Best, K.E.; Rankin, J. Increased risk of congenital heart disease in twins in the North of England between 1998 and 2010. Heart 2015, 101, 1807–1812. [Google Scholar] [CrossRef] [Green Version]
- Bahtiyar, M.O.; Dulay, A.T.; Weeks, B.P.; Friedman, A.H.; Copel, J.A. Prevalence of congenital heart defects in monochorionic/diamniotic twin gestations: A systematic literature review. J. Ultrasound Med. 2007, 26, 1491–1498. [Google Scholar] [CrossRef]
- Michelfelder, E.; Tan, X.; Cnota, J.; Divanovic, A.; Statile, C.; Lim, F.Y.; Crombleholme, T. Prevalence, Spectrum, and Outcome of Right Ventricular Outflow Tract Abnormalities in Twin-twin Transfusion Syndrome: A Large, Single-center Experience. Congenit. Heart Dis. 2015, 10, 209–218. [Google Scholar] [CrossRef]
- Lopriore, E.; Vandenbussche, F.P.; Tiersma, E.S.; de Beaufort, A.J.; de Leeuw, J.P. Twin-to-twin transfusion syndrome: New perspectives. J. Pediatr. 1995, 127, 675–680. [Google Scholar] [CrossRef]
- Huber, A.; Hecher, K. How can we diagnose and manage twin-twin transfusion syndrome? Best Pract. Res. Clin. Obstet. Gynaecol. 2004, 18, 543–556. [Google Scholar] [CrossRef]
- Hecher, K.; Gardiner, H.M.; Diemert, A.; Bartmann, P. Long-term outcomes for monochorionic twins after laser therapy in twin-to-twin transfusion syndrome. Lancet Child Adolesc. Health 2018, 2, 525–535. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Hayden, J.A.; van der Windt, D.A.; Cartwright, J.L.; Cote, P.; Bombardier, C. Assessing bias in studies of prognostic factors. Ann. Intern. Med. 2013, 158, 280–286. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Cincotta, R.; Oldham, J.; Sampson, A. Antepartum and postpartum complications of twin-twin transfusion. Aust. N. Z. J. Obstet. Gynaecol. 1996, 36, 303–308. [Google Scholar] [CrossRef]
- Eschbach, S.J.; Boons, L.; Van Zwet, E.; Middeldorp, J.M.; Klumper, F.; Lopriore, E.; Teunissen, A.K.K.; Rijlaarsdam, M.E.; Oepkes, D.; Ten Harkel, A.D.J.; et al. Right ventricular outflow tract obstruction in complicated monochorionic twin pregnancy. Ultrasound Obstet. Gynecol. 2017, 49, 737–743. [Google Scholar] [CrossRef]
- Hack, K.E.; Derks, J.B.; Schaap, A.H.; Lopriore, E.; Elias, S.G.; Arabin, B.; Eggink, A.J.; Sollie, K.M.; Mol, B.W.J.; Duvekot, H.J.; et al. Perinatal outcome of monoamniotic twin pregnancies. Obstet. Gynecol. 2009, 113, 353–360. [Google Scholar] [CrossRef]
- Herberg, U.; Gross, W.; Bartmann, P.; Banek, C.S.; Hecher, K.; Breuer, J. Long term cardiac follow up of severe twin to twin transfusion syndrome after intrauterine laser coagulation. Heart 2006, 92, 95–100. [Google Scholar] [CrossRef] [Green Version]
- Hidaka, N.; Tsukimori, K.; Chiba, Y.; Hara, T.; Wake, N. Monochorionic twins in which at least one fetus has a congenital heart disease with or without twin-twin transfusion syndrome. J. Perinat. Med. 2007, 35, 425–430. [Google Scholar] [CrossRef]
- Karatza, A.A.; Wolfenden, J.L.; Taylor, M.J.; Wee, L.; Fisk, N.M.; Gardiner, H.M. Influence of twin-twin transfusion syndrome on fetal cardiovascular structure and function: Prospective case-control study of 136 monochorionic twin pregnancies. Heart 2002, 88, 271–277. [Google Scholar] [CrossRef]
- Lopriore, E.; Bokenkamp, R.; Rijlaarsdam, M.; Sueters, M.; Vandenbussche, F.P.; Walther, F.J. Congenital heart disease in twin-to-twin transfusion syndrome treated with fetoscopic laser surgery. Congenit. Heart Dis. 2007, 2, 38–43. [Google Scholar] [CrossRef]
- Lougheed, J.; Sinclair, B.G.; Fung Kee Fung, K.; Bigras, J.L.; Ryan, G.; Smallhorn, J.F.; Hornberger, L.K. Acquired right ventricular outflow tract obstruction in the recipient twin in twin-twin transfusion syndrome. J. Am. Coll. Cardiol. 2001, 38, 1533–1538. [Google Scholar] [CrossRef]
- Pettit, K.E.; Merchant, M.; Machin, G.A.; Tacy, T.A.; Norton, M.E. Congenital heart defects in a large, unselected cohort of monochorionic twins. J. Perinatol. 2013, 33, 457–461. [Google Scholar] [CrossRef]
- Pruetz, J.D.; Sklansky, M.; Detterich, J.; Korst, L.M.; Llanes, A.; Chmait, R.H. Twin-twin transfusion syndrome treated with laser surgery: Postnatal prevalence of congenital heart disease in surviving recipients and donors. Prenat. Diagn. 2011, 31, 973–977. [Google Scholar] [CrossRef]
- Simpson, L.L.; Marx, G.R.; Elkadry, E.A.; D’Alton, M.E. Cardiac dysfunction in twin-twin transfusion syndrome: A prospective, longitudinal study. Obstet. Gynecol. 1998, 92, 557–562. [Google Scholar] [CrossRef]
- Springer, S.; Mlczoch, E.; Krampl-Bettelheim, E.; Mailath-Pokorny, M.; Ulm, B.; Worda, C.; Worda, K. Congenital heart disease in monochorionic twins with and without twin-to-twin transfusion syndrome. Prenat. Diagn. 2014, 34, 994–999. [Google Scholar] [CrossRef]
- Quintero, R.A.; Morales, W.J.; Allen, M.H.; Bornick, P.W.; Johnson, P.K.; Kruger, M. Staging of twin-twin transfusion syndrome. J. Perinatol. 1999, 19, 550–555. [Google Scholar] [CrossRef]
- Wren, C.; Richmond, S.; Donaldson, L. Temporal variability in birth prevalence of cardiovascular malformations. Heart 2000, 83, 414–419. [Google Scholar] [CrossRef] [Green Version]
- Ferencz, C. On the birth prevalence of congenital heart disease. J. Am. Coll. Cardiol. 1990, 16, 1701–1702. [Google Scholar] [CrossRef] [Green Version]
- Blondel, B.; Kaminski, M. Trends in the occurrence, determinants, and consequences of multiple births. Semin. Perinatol. 2002, 26, 239–249. [Google Scholar] [CrossRef]
- Martin, J.A.; Hamilton, B.E.; Osterman, M.J. Three Decades of Twin Births in the United States, 1980–2009; NCHS Data Brief; U.S. Department of Health & Human Services: Washington, DC, USA, 2012; pp. 1–8.
- Burn, J.; Corney, G. Congenital heart defects and twinning. Acta Genet. Med. Gemellol. (Roma) 1984, 33, 61–69. [Google Scholar] [CrossRef]
- Giorgione, V.; Parazzini, F.; Fesslova, V.; Cipriani, S.; Candiani, M.; Inversetti, A.; Sigismondi, C.; Tiberio, F.; Cavoretto, P. Congenital heart defects in IVF/ICSI pregnancy: Systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2018, 51, 33–42. [Google Scholar] [CrossRef]
- Panagiotopoulou, O.; Fouzas, S.; Sinopidis, X.; Mantagos, S.P.; Dimitriou, G.; Karatza, A.A. Congenital heart disease in twins: The contribution of type of conception and chorionicity. Int. J. Cardiol. 2016, 218, 144–149. [Google Scholar] [CrossRef]
- Michelfelder, E.; Gottliebson, W.; Border, W.; Kinsel, M.; Polzin, W.; Livingston, J.; Khoury, P.; Crombleholme, T. Early manifestations and spectrum of recipient twin cardiomyopathy in twin-twin transfusion syndrome: Relation to Quintero stage. Ultrasound Obstet. Gynecol. 2007, 30, 965–971. [Google Scholar] [CrossRef]
- Barrea, C.; Alkazaleh, F.; Ryan, G.; McCrindle, B.W.; Roberts, A.; Bigras, J.L.; Barrett, J.; Seaward, G.P.; Smallhorn, J.F.; Hornberger, L.K. Prenatal cardiovascular manifestations in the twin-to-twin transfusion syndrome recipients and the impact of therapeutic amnioreduction. Am. J. Obstet. Gynecol. 2005, 192, 892–902. [Google Scholar] [CrossRef]
- Moon-Grady, A.J.; Rand, L.; Lemley, B.; Gosnell, K.; Hornberger, L.K.; Lee, H. Effect of selective fetoscopic laser photocoagulation therapy for twin-twin transfusion syndrome on pulmonary valve pathology in recipient twins. Ultrasound Obstet. Gynecol. 2011, 37, 27–33. [Google Scholar] [CrossRef]
- Sueters, M.; Middeldorp, J.M.; Vandenbussche, F.P.; Teunissen, K.A.; Lopriore, E.; Kanhai, H.H.; Le Cessie, S.; Oepkes, D. The effect of fetoscopic laser therapy on fetal cardiac size in twin-twin transfusion syndrome. Ultrasound Obstet. Gynecol. 2008, 31, 158–163. [Google Scholar] [CrossRef]
- Barrea, C.; Hornberger, L.K.; Alkazaleh, F.; McCrindle, B.W.; Roberts, A.; Berezovska, O.; Windrim, R.; Seaward, P.G.; Smallhorn, J.F.; Ryan, G. Impact of selective laser ablation of placental anastomoses on the cardiovascular pathology of the recipient twin in severe twin-twin transfusion syndrome. Am. J. Obstet. Gynecol. 2006, 195, 1388–1395. [Google Scholar] [CrossRef]
- Van Mieghem, T.; Martin, A.M.; Weber, R.; Barrea, C.; Windrim, R.; Hornberger, L.K.; Jaeggi, E.; Ryan, G. Fetal cardiac function in recipient twins undergoing fetoscopic laser ablation of placental anastomoses for Stage IV twin-twin transfusion syndrome. Ultrasound Obstet. Gynecol. 2013, 42, 64–69. [Google Scholar] [CrossRef] [Green Version]
- van den Boom, J.; Battin, M.; Hornung, T. Twin-twin transfusion syndrome, coarctation of the aorta and hypoplastic aortic arch: A case series report. J. Paediatr. Child Health 2010, 46, 76–79. [Google Scholar] [CrossRef]
- Buyens, A.; Gyselaers, W.; Coumans, A.; Al Nasiry, S.; Willekes, C.; Boshoff, D.; Frijns, J.P.; Witters, I. Difficult prenatal diagnosis: Fetal coarctation. Facts Views Vis. ObGyn 2012, 4, 230–236. [Google Scholar]
- Rudolph, A.M.; Heymann, M.A.; Spitznas, U. Hemodynamic considerations in the development of narrowing of the aorta. Am. J. Cardiol. 1972, 30, 514–525. [Google Scholar] [CrossRef]
- Paladini, D.; Vassallo, M.; Sglavo, G.; Russo, M.G.; Martinelli, P. Diagnosis and outcome of congenital heart disease in fetuses from multiple pregnancies. Prenat. Diagn. 2005, 25, 403–406. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Year | Author | Country | Time Period | Design | Chorionicity Determination | Study Population | Number of Liveborn Twins (n TTTS) | Number of CHDs | |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 1996 | Cincotta | UK | 1994–1995 | P | TTTS diagnosis | 14 TTTS pregnancies | 22 | 2/10 recipients RVOTO, donors 0 |
| 2 | 1998 | Simpson | USA | 1992–1997 | P | Examination placenta postpartum | 12 TTTS pregnancies | 22 | 3/10 recipients RVOTO, donors 0 |
| 3 | 2001 | Lougheed | Canada | 1994–1998 | R | TTTS diagnosis | 73 TTTS pregnancies | 146 | 6/73 recipients RVOTO, donors 0 |
| 4 | 2002 | Karatza | UK | 1997–2000 | P | Examination placenta postpartum | 136 MC twin pregnancies (47 TTTS) | 226 (60) | 9/226 MC twins, no-TTTS 4/166, TTTS 5/60 |
| 5 | 2006 | Herberg | Germany | 1995–1997 | P | TTTS diagnosis, treated with FLS | 73 TTTS pregnancies | 89 | 10/89 TTTS twins |
| 6 | 2007 | Hidaka | Japan | 2000–2006 | P | Examination placenta postpartum | 87 MC twin pregnancies (1 TTTS) | 174 (2) | 11/174 MC twins |
| 7 | 2007 | Lopriore | Netherlands | 2002–2005 | P | Examination placenta postpartum | 101 MC twin pregnancies (46 TTTS) | 161 (74) | 6/161 MC twins, no-TTTS 2/87, TTTS 4/74 |
| 8 | 2009 | Hack | Netherlands | 2000–2007 | R | First trimester ultrasound scan and/or examination placenta postpartum | 98 MCMA twin pregnancies (6 TTTS) | 164 (unknown) | 7/164 MC twins |
| 9 | 2011 | Pruetz | USA | 2009–2010 | P | TTTS diagnosis, all treated with FLS | 50 TTTS pregnancies | 84 | 13/84 TTTS twins |
| 10 | 2013 | Pettit | USA | 1996–2003 | R | Examination placenta postpartum | 482 MC twin pregnancies (48 TTTS) | 926 (83) | 69/926 MC twins, no-TTTS 55/843, TTTS 14/83 |
| 11 | 2014 | Springer | Austria | 2002–2012 | R | First trimester scan, TTTS treated with FLS | 381 MC twin pregnancies (70 TTTS) | 754 (135) | 39/754 MC twins, no-TTTS 27/619, TTTS 12/135 |
| 12 | 2016 | Eschbach | Netherlands | 2004–2015 | P | TTTS diagnosis, majority treated with FLS | 485 TTTS pregnancies | 368 (368 recipients) | 11/368 recipients RVOTO |
| Variable/Study | Study Participation | Study Attrition | Prognostic Factor Measurement | Outcome Measurement | Study Confounding | Statistical Analysis and Reporting | |
|---|---|---|---|---|---|---|---|
| 1 | Cincotta | Moderate | Moderate | High | Moderate | Low | Low |
| 2 | Simpson | Low | Low | Low | Moderate | Low | Low |
| 3 | Lougheed | Moderate | Moderate | High | Low | Low | Moderate |
| 4 | Karatza | Low | Low | Low | Low | Low | Moderate |
| 5 | Herberg | Low | Low | Low | Low | Low | Low |
| 6 | Hidaka | Moderate | Low | Moderate | Moderate | Low | Low |
| 7 | Lopriore | Low | Low | Low | Low | Low | Low |
| 8 | Hack | Low | High | Moderate | High | Low | Moderate |
| 9 | Pruetz | Low | Low | Moderate | Low | Low | Low |
| 10 | Pettit | Low | Low | Moderate | Low | Low | Low |
| 11 | Springer | Low | Moderate | Low | Moderate | Low | Moderate |
| 12 | Eschbach | Low | Moderate | Low | Moderate | Low | Low |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gijtenbeek, M.; Shirzada, M.R.; Ten Harkel, A.D.J.; Oepkes, D.; C. Haak, M. Congenital Heart Defects in Monochorionic Twins: A Systematic Review and Meta-Analysis. J. Clin. Med. 2019, 8, 902. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8060902
Gijtenbeek M, Shirzada MR, Ten Harkel ADJ, Oepkes D, C. Haak M. Congenital Heart Defects in Monochorionic Twins: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2019; 8(6):902. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8060902
Chicago/Turabian StyleGijtenbeek, Manon, Maryam R. Shirzada, Arend D. J. Ten Harkel, Dick Oepkes, and Monique C. Haak. 2019. "Congenital Heart Defects in Monochorionic Twins: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 8, no. 6: 902. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8060902