Prenatal and Postnatal Hair Steroid Levels Predict Post-Partum Depression 12 Weeks after Delivery

 , and
, and 
Abstract
:1. Introduction
1.1. Plasma Cortisol in Healthy Pregnant Women
1.2. Salivary, Blood and Urine Cortisol in Pregnant Women with Major Depressive Disorders
1.3. Hair Cortisol in Women with Post-Partum Depression
1.4. Other Steroids during Pregnancy and after Delivery
1.5. Hypotheses of the Current Study
2. Methods
2.1. Procedure
2.2. Sample
2.3. Sample Size Calculation
2.4. Tools
Self-Ratings of Symptoms of Depression
Edinburgh Postnatal Depression Scale (EPDS)
Beck Depression Inventory (BDI)
Symptoms of Depression in the Past
2.5. Apgar Score
2.6. Hair Strands Sampling
2.7. Assessment of Hair Steroids
2.8. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Hair Steroids, Separately for Participants with (n = 48) and without (n = 50) Post-Partum Depression, and Separately for Prenatal and Postnatal Hair Segments
3.3. Correlations between Symptoms of Depression and Steroid Levels (Prenatal and Postnatal Stage)
3.4. Current Post-Partum Depression and Issues of Depression before Pregnancy
3.5. Predicting Postnatal Depression Levels (Edinburgh Depression Rating Scale) Based on Prenatal Hair Steroids
3.6. Predicting Postnatal Depression Status on the Basis of Prenatal and Postnatal Hair Steroid Levels
4. Discussion
Clinical Implications
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- O’Hara, M.W.; McCabe, J.E. Postpartum depression: Current status and future directions. Annu. Rev. Clin. Psychol. 2013, 9, 379–407. [Google Scholar] [CrossRef] [PubMed]
- O’Hara, M.W.; Wisner, K.L. Perinatal mental illness: Definition, description and aetiology. Best Pract. Res. Clin. Obs. Gynaecol. 2014, 28, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Brummelte, S.; Galea, L.A. Postpartum depression: Etiology, treatment and consequences for maternal care. Horm. Behav. 2016, 77, 153–166. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; DSM 5; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Heron, J.; O’Connor, T.G.; Evans, J.; Golding, J.; Glover, V. The course of anxiety and depression through pregnancy and the postpartum in a community sample. J. Affect. Disord. 2004, 80, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Brüne, M. Textbook of Evolutionary Psychiatry and Psychosomatic Medicine. The Origins of Psychopathology; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Buss, D.M. Evoutionary Psychology: The New Science of the Mind, 6th ed.; Taylor & Francis: New York, NY, USA, 2019. [Google Scholar]
- Stevens, A.; Price, J. Evolutionary Psychiatry: A New Beginning, 2nd ed.; Routledge: London, UK, 2000. [Google Scholar]
- McGuire, M.T.; Troisi, A. Darwinian Psychiatry; Oxford University Press: New York, NY, USA, 1998. [Google Scholar] [CrossRef]
- Wikenius, E.; Moe, V.; Kjellevold, M.; Smith, L.; Lyle, R.; Waagbo, R.; Page, C.M.; Myhre, A.M. The Association between Hair Cortisol and Self-Reported Symptoms of Depression in Pregnant Women. PLoS ONE 2016, 11, e0161804. [Google Scholar] [CrossRef] [PubMed]
- Tsubouchi, H.; Nakai, Y.; Toda, M.; Morimoto, K.; Chang, Y.S.; Ushioda, N.; Kaku, S.; Nakamura, T.; Kimura, T.; Shimoya, K. Change of salivary stress marker concentrations during pregnancy: Maternal depressive status suppress changes of those levels. J. Obstet. Gynaecol. Res. 2011, 37, 1004–1009. [Google Scholar] [CrossRef] [PubMed]
- Yim, I.S.; Stapleton, L.R.T.; Guardino, C.M.; Hahn-Holbrook, J.; Schetter, C.D. Biological and Psychosocial Predictors of Postpartum Depression: Systematic Review and Call for Integration. Annu. Rev. Clin. Psychol. 2015, 11, 99–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seth, S.; Lewis, A.J.; Galbally, M. Perinatal maternal depression and cortisol function in pregnancy and the postpartum period: A systematic literature review. BMC Pregnancy Childbirth 2016, 16, 124. [Google Scholar] [CrossRef] [PubMed]
- Holsboer, F.; Ising, M. Stress hormone regulation: Biological role and translation into therapy. Annu. Rev. Psychol. 2010, 61, 81–109. [Google Scholar] [CrossRef] [PubMed]
- Yehuda, R. Biology of posttraumatic stress disorder. J. Clin. Psychiatry 2001, 62 (Suppl. S17), 41–46. [Google Scholar] [PubMed]
- Miller, G.E.; Chen, E.; Zhou, E.S. If it goes up, must it come down? Chronic stress and the hypothalamic-pituitary-adrenocortical axis in humans. Psychol. Bull. 2007, 133, 25–45. [Google Scholar] [CrossRef] [PubMed]
- Wosu, A.C.; Valdimarsdottir, U.; Shields, A.E.; Williams, D.R.; Williams, M.A. Correlates of cortisol in human hair: Implications for epidemiologic studies on health effects of chronic stress. Ann. Epidemiol. 2013, 23, 797–811.e792. [Google Scholar] [CrossRef] [PubMed]
- Braig, S.; Grabher, F.; Ntomchukwu, C.; Reister, F.; Stalder, T.; Kirschbaum, C.; Genuneit, J.; Rothenbacher, D. Determinants of maternal hair cortisol concentrations at delivery reflecting the last trimester of pregnancy. Psychoneuroendocrinology 2015, 52, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Stalder, T.; Steudte-Schmiedgen, S.; Alexander, N.; Klucken, T.; Vater, A.; Wichmann, S.; Kirschbaum, C.; Miller, R. Stress-related and basic determinants of hair cortisol in humans: A meta-analysis. Psychoneuroendocrinology 2017, 77, 261–274. [Google Scholar] [CrossRef] [PubMed]
- Stalder, T.; Kirschbaum, C. Analysis of cortisol in hair – State of the art and future directions. Brain Behav. Immun. 2012, 26, 1019–1029. [Google Scholar] [CrossRef] [PubMed]
- Jung, C.; Ho, J.T.; Torpy, D.J.; Rogers, A.; Doogue, M.; Lewis, J.G.; Czajko, R.J.; Inder, W.J. A longitudinal study of plasma and urinary cortisol in pregnancy and postpartum. J. Clin. Endocrinol. Metab. 2011, 96, 1533–1540. [Google Scholar] [CrossRef] [PubMed]
- Glynn, L.M.; Davis, E.P.; Sandman, C.A. New insights into the role of perinatal HPA-axis dysregulation in postpartum depression. Neuropeptides 2013, 47, 363–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yehuda, R.; Seckl, J. Minireview: Stress-Related Psychiatric Disorders with Low Cortisol Levels: A Metabolic Hypothesis. Endocrinology 2011, 152, 4496–4503. [Google Scholar] [CrossRef] [Green Version]
- Serati, M.; Redaelli, M.; Buoli, M.; Altamura, A.C. Perinatal Major Depression Biomarkers: A systematic review. J. Affect. Disord. 2016, 193, 391–404. [Google Scholar] [CrossRef]
- Szpunar, M.J.; Parry, B.L. A systematic review of cortisol, thyroid-stimulating hormone, and prolactin in peripartum women with major depression. Arch. Womens Ment. Health 2018, 21, 149–161. [Google Scholar] [CrossRef]
- Field, T.; Hernandez-Reif, M.; Diego, M.; Schanberg, S.; Kuhn, C. Stability of mood states and biochemistry across pregnancy. Infant Behav. Dev. 2006, 29, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Field, T.; Diego, M.; Hernandez-Reif, M.; Figueiredo, B.; Schanberg, S.; Kuhn, C.; Deeds, O.; Contogeorgos, J.; Ascencio, A. Chronic prenatal depression and neonatal outcome. Int. J. Neurosci. 2008, 118, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Field, T.; Diego, M.; Hernandez-Reif, M.; Figueiredo, B.; Deeds, O.; Ascencio, A.; Schanberg, S.; Kuhn, C. Comorbid depression and anxiety effects on pregnancy and neonatal outcome. Infant Behav. Dev. 2010, 33, 23–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duthie, L.; Reynolds, R.M. Changes in the maternal hypothalamic-pituitary-adrenal axis in pregnancy and postpartum: Influences on maternal and fetal outcomes. Neuroendocrinology 2013, 98, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Bergman, K.; Sarkar, P.; Glover, V.; O’Connor, T.G. Maternal prenatal cortisol and infant cognitive development: Moderation by infant-mother attachment. Biol. Psychiatry 2010, 67, 1026–1032. [Google Scholar] [CrossRef] [PubMed]
- de Rezende, M.G.; Garcia-Leal, C.; de Figueiredo, F.P.; Cavalli Rde, C.; Spanghero, M.S.; Barbieri, M.A.; Bettiol, H.; de Castro, M.; Del-Ben, C.M. Altered functioning of the HPA axis in depressed postpartum women. J. Affect. Disord. 2016, 193, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Greff, M.J.E.; Levine, J.M.; Abuzgaia, A.M.; Elzagallaai, A.A.; Rieder, M.J.; van Uum, S.H.M. Hair cortisol analysis: An update on methodological considerations and clinical applications. Clin. Biochem. 2019, 63, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Braig, S.; Grabher, F.; Ntomchukwu, C.; Reister, F.; Stalder, T.; Kirschbaum, C.; Rothenbacher, D.; Genuneit, J. The Association of Hair Cortisol with Self-Reported Chronic Psychosocial Stress and Symptoms of Anxiety and Depression in Women Shortly after Delivery. Paediatr. Perinat. Epidemiol. 2016, 30, 97–104. [Google Scholar] [CrossRef]
- Caparros-Gonzalez, R.A.; Romero-Gonzalez, B.; Strivens-Vilchez, H.; Gonzalez-Perez, R.; Martinez-Augustin, O.; Peralta-Ramirez, M.I. Hair cortisol levels, psychological stress and psychopathological symptoms as predictors of postpartum depression. PLoS ONE 2017, 12, e0182817. [Google Scholar] [CrossRef]
- Kalra, S.; Einarson, A.; Karaskov, T.; Van Uum, S.; Koren, G. The relationship between stress and hair cortisol in healthy pregnant women. Clin. Investig. Med. 2007, 30, E103–E107. [Google Scholar] [CrossRef]
- Orta, O.R.; Tworoger, S.S.; Terry, K.L.; Coull, B.A.; Gelaye, B.; Kirschbaum, C.; Sanchez, S.E.; Williams, M.A. Stress and hair cortisol concentrations from preconception to the third trimester. Stress 2019, 22, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Wester, V.L.; van Rossum, E.F. Clinical applications of cortisol measurements in hair. Eur. J. Endocrinol. 2015, 173, M1–M10. [Google Scholar] [CrossRef] [PubMed]
- Dettenborn, L.; Muhtz, C.; Skoluda, N.; Stalder, T.; Steudte, S.; Hinkelmann, K.; Kirschbaum, C.; Otte, C. Introducing a novel method to assess cumulative steroid concentrations: Increased hair cortisol concentrations over 6 months in medicated patients with depression. Stress 2012, 15, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Dettenborn, L.; Tietze, A.; Kirschbaum, C.; Stalder, T. The assessment of cortisol in human hair: Associations with sociodemographic variables and potential confounders. Stress 2012, 15, 578–588. [Google Scholar] [CrossRef] [PubMed]
- Hinkelmann, K.; Muhtz, C.; Dettenborn, L.; Agorastos, A.; Wingenfeld, K.; Spitzer, C.; Gao, W.; Kirschbaum, C.; Wiedemann, K.; Otte, C. Association between childhood trauma and low hair cortisol in depressed patients and healthy control subjects. Biol. Psychiatry 2013, 74, e15–e17. [Google Scholar] [CrossRef] [PubMed]
- Steudte, S.; Kirschbaum, C.; Gao, W.; Alexander, N.; Schonfeld, S.; Hoyer, J.; Stalder, T. Hair cortisol as a biomarker of traumatization in healthy individuals and posttraumatic stress disorder patients. Biol. Psychiatry 2013, 74, 639–646. [Google Scholar] [CrossRef] [PubMed]
- Steudte, S.; Kolassa, I.T.; Stalder, T.; Pfeiffer, A.; Kirschbaum, C.; Elbert, T. Increased cortisol concentrations in hair of severely traumatized Ugandan individuals with PTSD. Psychoneuroendocrinology 2011, 36, 1193–1200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dajani, R.; Hadfield, K.; van Uum, S.; Greff, M.; Panter-Brick, C. Hair cortisol concentrations in war-affected adolescents: A prospective intervention trial. Psychoneuroendocrinology 2018, 89, 138–146. [Google Scholar] [CrossRef]
- Pacella, M.L.; Hruska, B.; Steudte-Schmiedgen, S.; George, R.L.; Delahanty, D.L. The utility of hair cortisol concentrations in the prediction of PTSD symptoms following traumatic physical injury. Soc. Sci. Med. (1982) 2017, 175, 228–234. [Google Scholar] [CrossRef]
- Sierau, S.; Glaesmer, H.; Klucken, T.; Stalder, T. Hair cortisol, lifetime traumatic experiences and psychopathology in unaccompanied refugee minors. Psychoneuroendocrinology 2019, 104, 191–194. [Google Scholar] [CrossRef]
- van den Heuvel, L.L.; Wright, S.; Suliman, S.; Stalder, T.; Kirschbaum, C.; Seedat, S. Cortisol levels in different tissue samples in posttraumatic stress disorder patients versus controls: A systematic review and meta-analysis protocol. Syst. Rev. 2019, 8. [Google Scholar] [CrossRef] [PubMed]
- D’Anna-Hernandez, K.L.; Ross, R.G.; Natvig, C.L.; Laudenslager, M.L. Hair cortisol levels as a retrospective marker of hypothalamic-pituitary axis activity throughout pregnancy: Comparison to salivary cortisol. Physiol. Behav. 2011, 104, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Schiller, C.E.; Meltzer-Brody, S.; Rubinow, D.R. The role of reproductive hormones in postpartum depression. CNS Spectr. 2015, 20, 48–59. [Google Scholar] [CrossRef] [PubMed]
- Finocchi, C.; Ferrari, M. Female reproductive steroids and neuronal excitability. Neurol. Sci. 2011, 32, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Guintivano, J.; Sullivan, P.F.; Stuebe, A.M.; Penders, T.; Thorp, J.; Rubinow, D.R.; Meltzer-Brody, S. Adverse life events, psychiatric history, and biological predictors of postpartum depression in an ethnically diverse sample of postpartum women. Psychol. Med. 2018, 48, 1190–1200. [Google Scholar] [CrossRef] [PubMed]
- Turkcapar, A.F.; Kadioglu, N.; Aslan, E.; Tunc, S.; Zayifoglu, M.; Mollamahmutoglu, L. Sociodemographic and clinical features of postpartum depression among Turkish women: A prospective study. BMC Pregnancy Childbirth 2015, 15, 108. [Google Scholar] [CrossRef] [PubMed]
- Suhitharan, T.; Pham, T.P.; Chen, H.; Assam, P.N.; Sultana, R.; Han, N.L.; Tan, E.C.; Sng, B.L. Investigating analgesic and psychological factors associated with risk of postpartum depression development: A case-control study. Neuropsychiatr. Dis. Treat. 2016, 12, 1333–1339. [Google Scholar] [CrossRef] [PubMed]
- Vliegen, N.; Casalin, S.; Luyten, P. The course of postpartum depression: A review of longitudinal studies. Harv. Rev. Psychiatry 2014, 22, 1–22. [Google Scholar] [CrossRef]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59 (Suppl. S20), 22–33; quiz 34–57. [Google Scholar]
- Ross, L.E.; Grigoriadis, S.; Mamisashvili, L.; Koren, G.; Steiner, M.; Dennis, C.L.; Cheung, A.; Mousmanis, P. Quality assessment of observational studies in psychiatry: An example from perinatal psychiatric research. Int. J. Methods Psychiatr. Res. 2011, 20, 224–234. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Knights, J.E.; Salvatore, M.L.; Simpkins, G.; Hunter, K.; Khandelwal, M. In search of best practice for postpartum depression screening: is once enough? Eur. J. Obstet. Gynecol. Reprod. Boil. 2016, 206, 99–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry J. Ment. Sci. 1987, 150, 782–786. [Google Scholar] [CrossRef] [PubMed]
- Matthey, S.; Henshaw, C.; Elliott, S.; Barnett, B. Variability in use of cut-off scores and formats on the Edinburgh Postnatal Depression Scale—implications for clinical and research practice. Arch. Women’s Ment. Heal. 2006, 9, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [PubMed]
- Ghassemzadeh, H.; Mojtabai, R.; Karamghadiri, N.; Ebrahimkhani, N. Psychometric properties of a Persian-language version of the Beck Depression Inventory - Second edition: BDI-II-PERSIAN. Depression Anxiety 2005, 21, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Eslami, Z.; Falah, R. Evaluation of the Apgar score and its related factors in neonates born in hospitals of Yazd (Persian). J. Shahid Sadoughi Unversity Med. Sci. 2009, 16, 40–45. [Google Scholar]
- Kirschbaum, C.; Tietze, A.; Skoluda, N.; Dettenborn, L. Hair as a retrospective calendar of cortisol production-Increased cortisol incorporation into hair in the third trimester of pregnancy. Psychoneuroendocrinology 2009, 34, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Colledge, F.; Brand, S.; Zimmerer, S.; Puhse, U.; Holsboer-Trachsler, E.; Gerber, M. In Individuals Following Aneurysmal Subarachnoid Haemorrhage, Hair Cortisol Concentrations Are Higher and More Strongly Associated with Psychological Functioning and Sleep Complaints than in Healthy Controls. Neuropsychobiology 2017, 75, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Gerber, M.; Jonsdottir, I.H.; Kalak, N.; Elliot, C.; Puhse, U.; Holsboer-Trachsler, E.; Brand, S. Objectively assessed physical activity is associated with increased hair cortisol content in young adults. Stress 2013, 16, 593–599. [Google Scholar] [CrossRef]
- Gerber, M.; Kalak, N.; Elliot, C.; Holsboer-Trachsler, E.; Puhse, U.; Brand, S. Both hair cortisol levels and perceived stress predict increased symptoms of depression: An exploratory study in young adults. Neuropsychobiology 2013, 68, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Gao, W.; Stalder, T.; Foley, P.; Rauh, M.; Deng, H.; Kirschbaum, C. Quantitative analysis of steroid hormones in human hair using a column-switching LC-APCI-MS/MS assay. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2013, 928, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Mastorakos, G.; Ilias, I. Maternal and fetal hypothalamic-pituitary-adrenal axes during pregnancy and postpartum. Ann. N. Y. Acad. Sci. 2003, 997, 136–149. [Google Scholar] [CrossRef] [PubMed]
- Scheyer, K.; Urizar, G.G., Jr. Altered stress patterns and increased risk for postpartum depression among low-income pregnant women. Arch. Women’s Ment. Health 2016, 19, 317–328. [Google Scholar] [CrossRef] [PubMed]
- Harris, L.; The Lancet. Screening for perinatal depression: A missed opportunity. Lancet 2016, 387, 505. [Google Scholar] [CrossRef]
- Hagen, E.H. The Functions of Postpartum Depression. Evol. Hum. Behav. 1999, 20, 325–359. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Group | Statistics | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| With PPD | Healthy Controls | |||||||||||
| N | 48 | 48 | 50 | 50 | ||||||||
| Time period of steroid levels | Prenatal | Postnatal | d | Prenatal | Postnatal | d | ||||||
| Hair steroids | M (SD) | M (SD) | M (SD) | M (SD) | Time | Group | Time × Group interaction | |||||
| F | ηp2 | F | ηp2 | F | ηp2 | |||||||
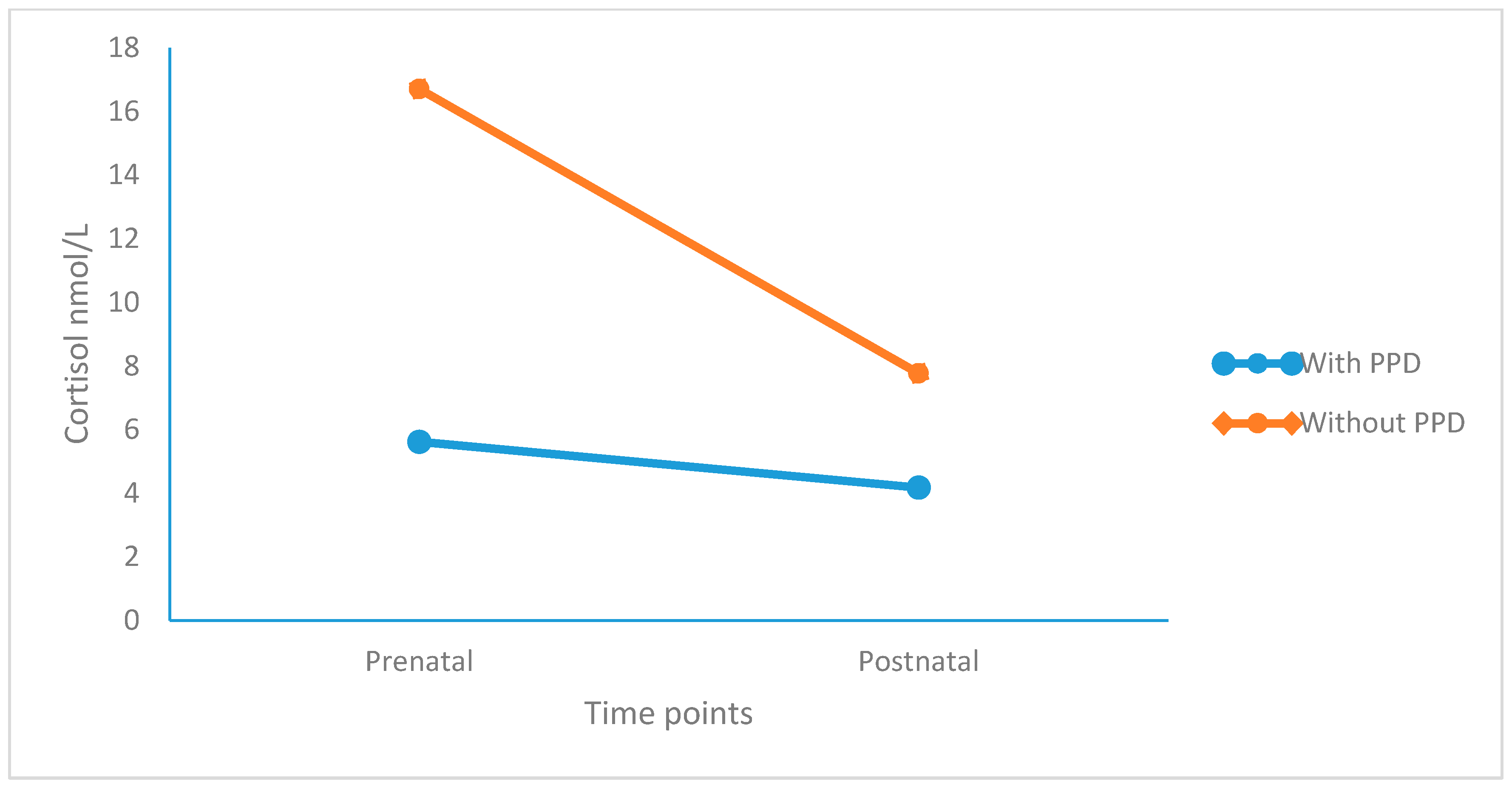
| Cortisol | 5.62 (3.98) | 4.18 (2.59) | 0.43 (S) | 16.71 (9.51) | 7.77 (5.47) | 1.15 (L) | 40.43 *** | 0.296 (L) | 10.47 *** | 0.373 (M) | 21.08 *** | 0.180 (L) |
| Cortisone | 12.48 (7.57) | 6.14 (3.50) | 1.08 (L) | 48.49 (26.35) | 17.94 (12.83) | 1.47 (L) | 59.44 *** | 0.282 (L) | 17.97 *** | 0.158 (L) | 25.63 *** | 0.211 (L) |
| Testosterone | 0.34 (0.53) | 0.42 (0.45) | 0.16 (T) | 0.58 (0.79) | 0.82 (0.95) | 0.27 (S) | 1.00 | 0.010 (S) | 1.52 | 0.016 (S) | 0.79 | 0.008 (S) |
| Progesterone | 30.66 (26.44) | 40.58 (25.37) | 0.38 (S) | 107.59 (45.03) | 86.91 (51.55) | 0.42 (S) | 0.60 | 0.006 (S) | 19.13 *** | 0.166 (L) | 4.80 * | 0.049 (S) |
| DHEA | 7.74 (4.56) | 6.34 (5.37) | 0.28 (S) | 3.93 (2.97) | 2.95 (2.64) | 0.34 (S) | 3.53 (*) | 0.035 (S) | 7.48 ** | 0.072 (M) | 0.11 | 0.001 (S) |
| Groups | Statistics | |||
|---|---|---|---|---|
| Individuals with PPD | Individuals without PPD | |||
| N | 48 | 50 | ||
| n (%) | n (%) | X2-test | ||
| Depressive episode in life (yes/no) | 21/27 | 1/49 | X2 (N = 98, df = 1) = 24.52 *** | |
| M (SD) | M (SD) | t-tests | Cohen’s d | |
| Age (years) | 25.88 (4.28) | 25.22 (4.88) | t(96) = 0.71 | 0.14 (S) |
| Beck Depression Inventory | 28.08 (9.19) | 4.30 (3.13) | t(96) = 17.28 *** | 3.49 (L) |
| Edinburgh Postnatal Depression Scale | 15.69 (3.47) | 3.82 (2.76) | t(96) = 18.77 *** | 3.78 (L) |
| Gestational age (days) | 270.23 (12.79) | 274.04 (11.92) | t(96) = 1.53 | 0.00 (-) |
| Apgar score at delivery | 8.81 (0.70) | 9.98 (0.25) | t(96) = 1.58 | 2.23 (L) |
| Apgar score 10′ after delivery | 9.85 (0.50) | 9.96 (0.20) | t(96) = 1.38 | 0.29 (S) |
| Dimensions | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | ||
| 1 | BDI | - | 0.90 *** | −0.28 ** | −0.13 | −0.36 *** | −0.23 * | −0.14 | −0.08 | −0.40 *** | −0.23 * | 0.21 * | 0.21 * |
| 2 | EPDS | - | −0.23 ** | −0.15 | −0.35 ** | −0.24 * | −0.16 | −0.14 | −0.40 *** | −0.22 * | 0.19 (*) | 0.20 * | |
| 3 | Cortisol pre | - | 0.91 *** | 0.94 *** | 0.86 *** | −0.12 | −0.04 | 0.04 | −0.02 | 0.07 | 0.11 | ||
| 4 | Cortisol post | - | 0.86 *** | 0.04 *** | −0.09 | −0.03 | −0.01 | −0.03 | 0.07 | 0.17 | |||
| 5 | Cortisone pre | - | 0.91 *** | −0.15 | −0.07 | 0.03 | −0.03 | 0.00 | 0.09 | ||||
| 6 | Cortisone post | - | −0.11 | −0.08 | −0.02 | −0.03 | 0.00 | 0.11 | |||||
| 7 | Testosterone pre | - | 0.90 *** | 0.61 *** | 0.22 * | 0.01 | 0.00 | ||||||
| 8 | Testosterone post | - | 0.05 | −0.05 | −0.04 | −0.02 | |||||||
| 9 | Progesterone pre | - | 0.65 *** | −0.16 | −0.14 | ||||||||
| 10 | Progesterone post | - | −0.15 | −0.10 | |||||||||
| 11 | DHEA pre | - | 0.65 ** | ||||||||||
| 12 | DHEA post | - | |||||||||||
| Dimension | Variables | Coefficient | Standard Error | Coefficient β | t | p | R | R2 | Durbin-Watson Coefficient |
|---|---|---|---|---|---|---|---|---|---|
| Edinburgh Postnatal Depression Scale | Intercept | 12.69 | 1.038 | - | 12.22 | 0.001 | 0.552 | 0.30 | 1.78 |
| Antenatal cortisol | 0.152 | 0.111 | 0.127 | 1.373 | 0.173 | ||||
| Antenatal cortisone | −0.105 | 0.041 | −0.664 | −2.548 | 0.012 | ||||
| Antenatal testosterone | 0.219 | 1.112 | 0.022 | 0.197 | 0.884 | ||||
| Antenatal progesterone | −0.032 | 0.009 | −0.393 | −3.453 | 0.001 | ||||
| Antenatal DHEA | 0.099 | 0.085 | 0.1.06 | 1.164 | 0.248 |
| Dimension | Variables | Coefficient | Standard Error | Wald | p | Nagelkerke R2 |
|---|---|---|---|---|---|---|
| Depression (yes vs. no) | Intercept | 2.99 | 1.074 | 7.729 | 0.003 | 0.924 |
| Cortisol prenatal | −0.526 | 0.150 | 12.366 | 0.000 | ||
| Cortisol postnatal | 1.083 | 0.307 | 12.471 | 0.001 | ||
| Cortisone postnatal | −0.304 | 0.131 | 5.440 | 0.020 | ||
| Progesterone prenatal | −0.019 | 0.007 | 7.043 | 0.008 | ||
| Progesterone postnatal | −0.024 | 0.011 | 4.759 | 0.029 | ||
| DHEA prenatal | 0.211 | 0.099 | 4.525 | 0.033 | ||
| Excluded variables | Cortisone prenatal, testosterone prenatal, testosterone postnatal, DHEA postnatal, (all Wald’s < 1.8, all p’s > 0.10). | |||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jahangard, L.; Mikoteit, T.; Bahiraei, S.; Zamanibonab, M.; Haghighi, M.; Sadeghi Bahmani, D.; Brand, S. Prenatal and Postnatal Hair Steroid Levels Predict Post-Partum Depression 12 Weeks after Delivery. J. Clin. Med. 2019, 8, 1290. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8091290
Jahangard L, Mikoteit T, Bahiraei S, Zamanibonab M, Haghighi M, Sadeghi Bahmani D, Brand S. Prenatal and Postnatal Hair Steroid Levels Predict Post-Partum Depression 12 Weeks after Delivery. Journal of Clinical Medicine. 2019; 8(9):1290. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8091290
Chicago/Turabian StyleJahangard, Leila, Thorsten Mikoteit, Saman Bahiraei, Mehrangiz Zamanibonab, Mohammad Haghighi, Dena Sadeghi Bahmani, and Serge Brand. 2019. "Prenatal and Postnatal Hair Steroid Levels Predict Post-Partum Depression 12 Weeks after Delivery" Journal of Clinical Medicine 8, no. 9: 1290. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8091290