Comparative Volume Analysis of Alveolar Defects by 3D Simulation
_周(Chou).jpg)
 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Material and Methods
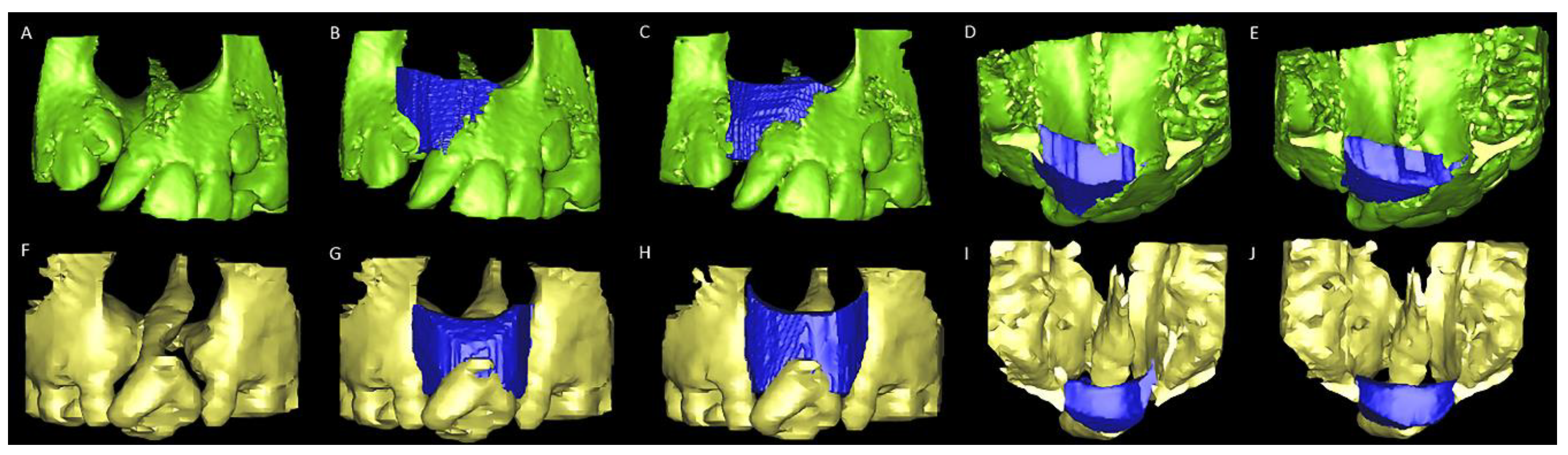
2.1. Alveolar Cleft Surgery Simulation Tools
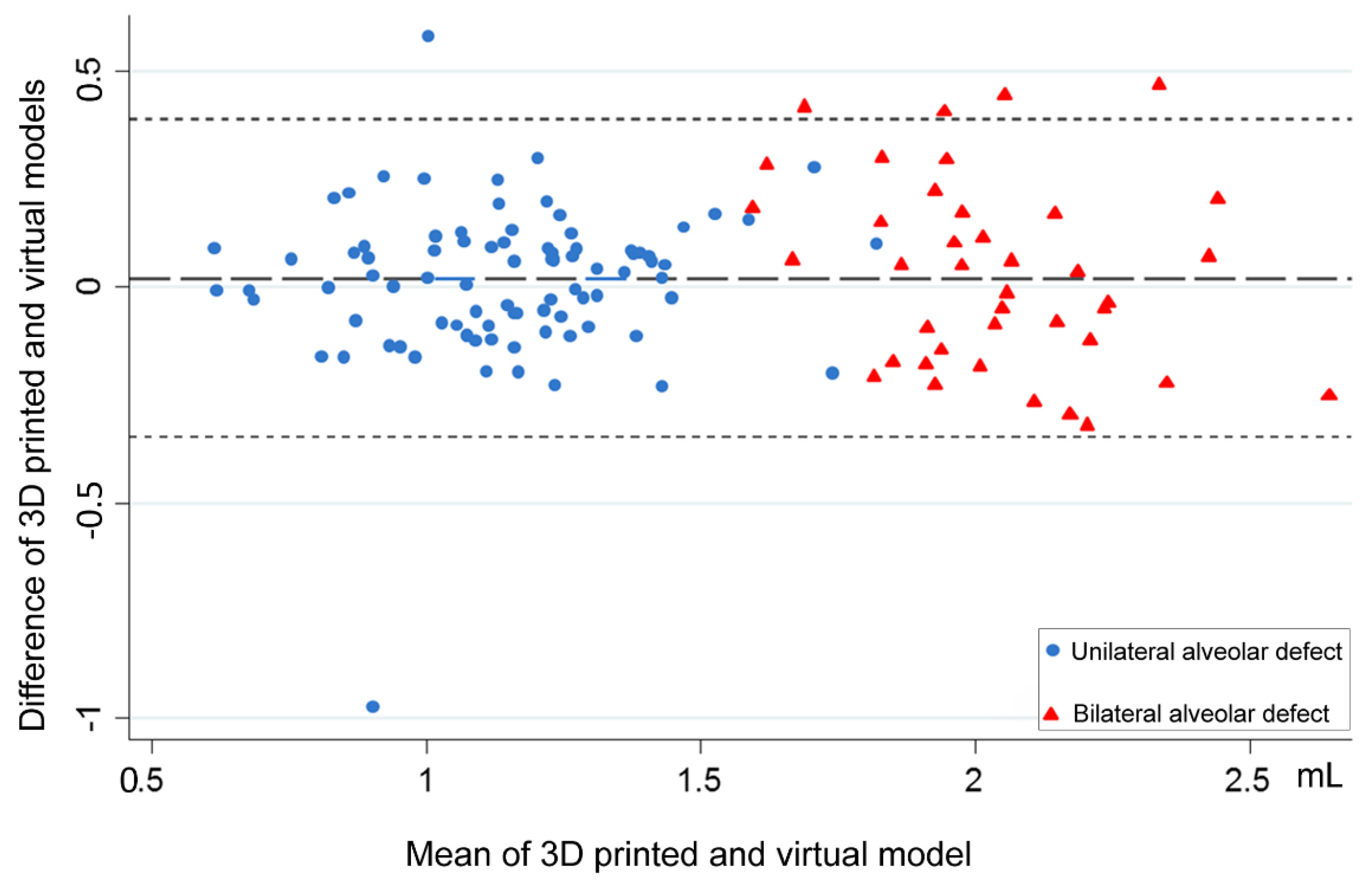
2.2. Statistical Analysis
3. Results
D-Based Alveolar Cleft Volume
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Semb, G. Alveolar bone grafting. Front. Oral Biol. 2012, 16, 124–136. [Google Scholar]
- Weissler, E.H.; Paine, K.M.; Ahmed, M.K.; Taub, P.J. Alveolar Bone Grafting and Cleft Lip and Palate: A Review. Plast. Reconstr. Surg. 2016, 138, 1287–1295. [Google Scholar] [CrossRef]
- Witherow, H.; Cox, S.; Jones, E.; Carr, R.; Waterhouse, N. A new scale to assess radiographic success of secondary alveolar bone grafts. Cleft Palate Craniofacial J. 2002, 39, 255–260. [Google Scholar] [CrossRef]
- Liao, Y.F.; Huang, C.S. Presurgical and postsurgical orthodontics are associated with superior secondary alveolar bone grafting outcomes. J. Cranio Maxillofac. Surg. 2015, 43, 717–723. [Google Scholar] [CrossRef]
- Lo, L.J.; Marsh, J.L.; Vannier, M.W.; Patel, V.V. Craniofacial computer-assisted surgical planning and simulation. Clin. Plast. Surg. 1994, 21, 501–516. [Google Scholar]
- Lo, L.J.; Chen, Y.R. Three-dimensional computed tomography imaging in craniofacial surgery: Morphological study and clinical applications. Chang. Gung Med. J. 2003, 26, 1–11. [Google Scholar]
- De Mulder, D.; Cadenas de Llano-Pérula, M.; Jacobs, R.; Verdonck, A.; Willems, G. Three-dimensional radiological evaluation of secondary alveolar bone grafting in cleft lip and palate patients: A systematic review. Dentomaxillofac. Radiol. 2018, 48, 20180047. [Google Scholar] [CrossRef]
- Stasiak, M.; Wojtaszek-Słomińska, A.; Racka-Pilszak, B. Current methods for secondary alveolar bone grafting assessment in cleft lip and palate patients—A systematic review. J. Cranio Maxillofac. Surg. 2019, 47, 578–585. [Google Scholar] [CrossRef]
- Krille, L.; Zeeb, H.; Jahnen, A.; Mildenberger, P.; Seidenbusch, M.; Schneider, K.; Weisser, G.; Hammer, G.; Scholz, P.; Blettner, M. Computed tomographies and cancer risk in children: A literature overview of CT practices, risk estimations and an epidemiologic cohort study proposal. Radiat. Environ. Biophys. 2012, 51, 103–111. [Google Scholar] [CrossRef]
- Sheppard, J.P.; Nguyen, T.; Alkhalid, Y.; Beckett, J.S.; Salamon, N.; Yang, I. Risk of brain tumor induction from pediatric head CT Procedures: A systematic literature review. Brain Tumor Res. Treat. 2018, 6, 1–7. [Google Scholar] [CrossRef]
- Eufinger, H.; Leppänen, H. Iliac crest donor site morbidity following open and closed methods of bone harvest for alveolar cleft osteoplasty. J. Cranio Maxillofac. Surg. 2000, 28, 31–38. [Google Scholar] [CrossRef]
- Loeffler, B.J.; Kellam, J.F.; Sims, S.H.; Bosse, M.J. Prospective observational study of donor-site morbidity following anterior iliac crest bone-grafting in orthopaedic trauma reconstruction patients. J. Bone Jt. Surg. Am. 2012, 94, 1649–1654. [Google Scholar] [CrossRef]
- Canady, J.W.; Zeitler, D.P.; Thompson, S.A.; Nicholas, C.D. Suitability of the iliac crest as a site for harvest of autogenous bone grafts. Cleft Palate Craniofacial J. 1993, 30, 579–581. [Google Scholar] [CrossRef]
- Mossey, P.A.; Shaw, W.C.; Munger, R.G.; Murray, J.C.; Murthy, J.; Little, J. Global oral health inequalities: Challenges in the prevention and management of orofacial clefts and potential solutions. Adv. Dent. Res. 2011, 23, 247–258. [Google Scholar] [CrossRef]
- Long, R.E.; Wilson-Genderson, M.; Grayson, B.H.; Flores, R.; Broder, H.L. Oral health-related quality of life and self-rated speech in children with existing fistulas in mid-childhood and adolescence. Cleft Palate Craniofacial J. 2016, 53, 664–669. [Google Scholar] [CrossRef]
- Chang, C.S.; Wallace, C.G.; Hsiao, Y.C.; Lu, T.C.; Chen, S.H.; Chan, F.C.; Chen, P.K.; Chen, J.P.; Chang, C.J.; Noordhoff, M.S. Patient and parent reported outcome measures in cleft lip and palate patients before and after secondary alveolar bone grafting. Medicine 2017, 96, e9541. [Google Scholar] [CrossRef]
- Franceschi, R.T. Biological approaches to bone regeneration by gene therapy. J. Dent. Res. 2005, 84, 1093–1103. [Google Scholar] [CrossRef]
- Mao, J.J.; Giannobile, W.V.; Helms, J.A.; Hollister, S.J.; Krebsbach, P.H.; Longaker, M.T.; Shi, S. Craniofacial tissue engineering by stem cells. J. Dent. Res. 2006, 85, 966–979. [Google Scholar] [CrossRef]
- Lonic, D.; Yamaguchi, K.; Chien-Jung Pai, B.; Lo, L.J. Reinforcing the mucoperiosteal pocket with the scarpa fascia graft in secondary alveolar bone grafting: A retrospective controlled outcome study. Plast. Reconstr. Surg. 2017, 140, 568e–578e. [Google Scholar] [CrossRef]
- Pai, B.C.J.; Hung, Y.T.; Wang, R.S.H.; Lo, L.J. Outcome of patients with complete unilateral cleft lip and palate: 20-year follow-up of a treatment protocol. Plast. Reconstr. Surg. 2019, 143, 359e–367e. [Google Scholar] [CrossRef]
- Linderup, B.W.; Küseler, A.; Jensen, J.; Cattaneo, P.M. A novel semiautomatic technique for volumetric assessment of the alveolar bone defect using cone beam computed tomography. Cleft Palate Craniofacial J. 2015, 52, e47–e55. [Google Scholar] [CrossRef]
- Angelopoulos, C. Cone beam tomographic imaging anatomy of the maxillofacial region. Dent. Clin. N. Am. 2008, 52, 731–752. [Google Scholar] [CrossRef]
- Schlicher, W.; Nielsen, I.; Huang, J.C.; Maki, K.; Hatcher, D.C.; Miller, A.J. Consistency and precision of landmark identification in three- dimensional cone beam computed tomography scans. Eur. J. Orthod. 2012, 34, 263–275. [Google Scholar] [CrossRef]
- Zamora, N.; Llamas, J.M.; Cibrian, R.; Gandia, J.L.; Paredes, V. A study on the reproducibility of cephalometric landmarks when undertaking a three-dimensional (3D) cephalometric analysis. Med. Oral Patol. Oral Cir. Bucal 2012, 17, e678–e688. [Google Scholar] [CrossRef] [Green Version]
- Roth, D.A.; Gosain, A.K.; McCarthy, J.G.; Stracher, M.A.; Lefton, D.R.; Grayson, B.H. A CT scan technique for quantitative volumetric assessment of the mandible after distraction osteogenesis. Plast. Reconstr. Surg. 1997, 99, 1237–1247. [Google Scholar] [CrossRef]
- Johansson, B.; Grepe, A.; Wannfors, K.; Aberg, P.; Hirsch, J.M. Volumetry of simulated bone grafts in the edentulous maxilla by computed tomography: An experimental study. Dentomaxillofac. Radiol. 2001, 30, 153–156. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- Oberoi, S.; Chigurupati, R.; Gill, P.; Hoffman, W.Y.; Vargervik, K. Volumetric assessment of secondary alveolar bone grafting using cone beam computed tomography. Cleft Palate Craniofacial J. 2009, 46, 503–511. [Google Scholar] [CrossRef]
- Amirlak, B.; Tang, C.J.; Becker, D.; Palomo, J.M.; Gosain, A.K. Volumetric analysis of simulated alveolar cleft defects and bone grafts using cone beam computed tomography. Plast. Reconstr. Surg. 2013, 131, 854–859. [Google Scholar] [CrossRef]
- Zhou, W.N.; Xu, Y.B.; Jiang, H.B.; Wan, L.; Du, Y.F. Accurate evaluation of cone-beam computed tomography to volumetrically assess bone grafting in alveolar cleft patients. J. Craniofacial Surg. 2015, 26, e535–e539. [Google Scholar] [CrossRef]
- Du, F.; Li, B.; Yin, N.; Cao, Y.; Wang, Y. Volumetric analysis of alveolar bone defect using three-dimensional-printed models versus computer-aided engineering. J. Craniofacial Surg. 2017, 28, 383–386. [Google Scholar] [CrossRef]
- Feng, B.; Jiang, M.; Xu, X.; Li, J. A new method of volumetric assessment of alveolar bone grafting for cleft patients using cone beam computed tomography. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2017, 124, e171–e182. [Google Scholar] [CrossRef]
- Janssen, N.G.; Schreurs, R.; Bittermann, G.K.P.; Borstlap, W.A.; Koole, R.; Meijer, G.J.; Maal, T.J.J. A novel semi-automatic segmentation protocol for volumetric assessment of alveolar cleft grafting procedures. J. Cranio Maxillofac. Surg. 2017, 45, 685–689. [Google Scholar] [CrossRef]
- Kasaven, C.P.; McIntyre, G.T.; Mossey, P.A. Accuracy of both virtual and printed 3-dimensional models for volumetric measurement of alveolar clefts before grafting with alveolar bone compared with a validated algorithm: A preliminary investigation. Br. J. Oral Maxillofac. Surg. 2017, 55, 31–36. [Google Scholar] [CrossRef]
- Chen, G.C.; Sun, M.; Yin, N.B.; Li, H.D. A novel method to calculate the volume of alveolar cleft defect before surgery. J. Craniofacial Surg. 2018, 29, 342–346. [Google Scholar] [CrossRef]
- Pauwels, R.; Jacobs, R.; Singer, S.R.; Mupparapu, M. CBCT-based bone quality assessment: Are Hounsfield units applicable? Dentomaxillofac. Radiol. 2015, 44, 20140238. [Google Scholar] [CrossRef]
- Molteni, R. Prospects and challenges of rendering tissue density in Hounsfield units for cone beam computed tomography. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 116, 105–119. [Google Scholar] [CrossRef]
- Mah, P.; Reeves, T.E.; McDavid, W.D. Deriving Hounsfield units using grey levels in cone beam computed tomography. Dentomaxillofac. Radiol. 2010, 39, 323–335. [Google Scholar] [CrossRef]
- Mossey, P.A.; Modell, B. Epidemiology of oral clefts 2012: An international perspective. Front. Oral Biol. 2012, 16, 1–18. [Google Scholar] [CrossRef]
- Mossey, P.A.; Little, J.; Munger, R.G.; Dixon, M.J.; Shaw, W.C. Cleft lip and palate. Lancet 2009, 374, 1773–1785. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | 3D Printed Model | Virtual Model | p-Value |
|---|---|---|---|
| Unilateral alveolar cleft volume, mL | |||
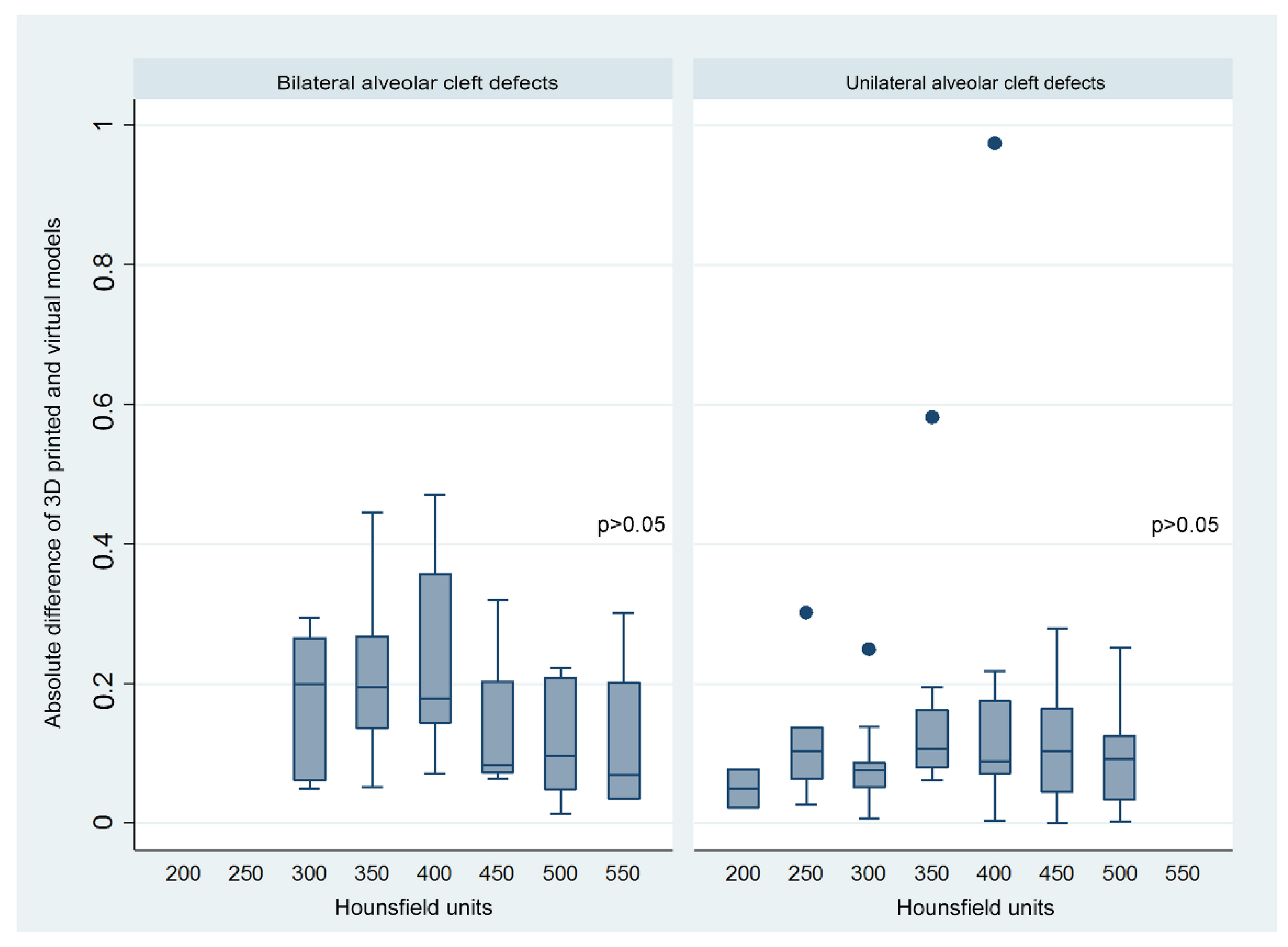
| HU1 400 (p25 = 300, p75 = 450) | 1.07 ± 0.25 | 1.05 ± 0.27 | >0.05 |
| HU2 375 (p25 = 350, p75 = 462.5) | 1.11 ± 0.23 | 1.14 ± 0.23 | >0.05 |
| Total | 1.09 ± 0.24 | 1.09 ± 0.25 | >0.05 |
| Bilateral alveolar cleft volume, mL | |||
| HU1 350 (p25 = 300, p75 = 350) | 2.07 ± 0.24 | 2.03 ± 0.29 | >0.05 |
| HU2 400 (p25 = 350, p75 = 400) | 2.02 ± 0.20 | 2.00 ± 0.25 | >0.05 |
| Total | 2.05 ± 0.22 | 2.02 ± 0.27 | >0.05 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chou, P.-Y.; Denadai, R.; Hallac, R.R.; Dumrongwongsiri, S.; Hsieh, W.-C.; Pai, B.C.; Lo, L.-J. Comparative Volume Analysis of Alveolar Defects by 3D Simulation. J. Clin. Med. 2019, 8, 1401. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8091401
Chou P-Y, Denadai R, Hallac RR, Dumrongwongsiri S, Hsieh W-C, Pai BC, Lo L-J. Comparative Volume Analysis of Alveolar Defects by 3D Simulation. Journal of Clinical Medicine. 2019; 8(9):1401. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8091401
Chicago/Turabian StyleChou, Pang-Yun, Rafael Denadai, Rami R. Hallac, Sarayuth Dumrongwongsiri, Wei-Chuan Hsieh, Betty CJ Pai, and Lun-Jou Lo. 2019. "Comparative Volume Analysis of Alveolar Defects by 3D Simulation" Journal of Clinical Medicine 8, no. 9: 1401. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8091401