Prophylactic Hyperthermic Intraperitoneal Chemotherapy (HIPEC) for Gastric Cancer—A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search Strategy
2.2. Study Selection Criteria
- Study type: Comparative studies.
- Study characteristics: Only articles written in English or Dutch were included. Papers for which no abstract or no full text was available were excluded. In case of multiple publications of a study, only the most recent version was included.
- Participants: Patients with primary cancer of the stomach without peritoneal or distant metastases who underwent radical resection were included. Peritoneal cytology positive for cancer cells is regarded as a proven metastatic disease in TNM-7, thus patients with positive peritoneal cytology were excluded [11].
- Intervention and comparison: Patients who underwent radical surgery in combination with prophylactic HIPEC formed the intervention group. The comparison group consisted of patients receiving surgery alone (SA). No selection was made based on the lymphadenectomy performed.
- Outcomes: The primary endpoint was overall survival. The secondary endpoints were 5-year survival, disease-free survival, peritoneal recurrence, post-operative morbidity and mortality and quality of life.
2.3. Assessment of Methodological Quality
3. Results
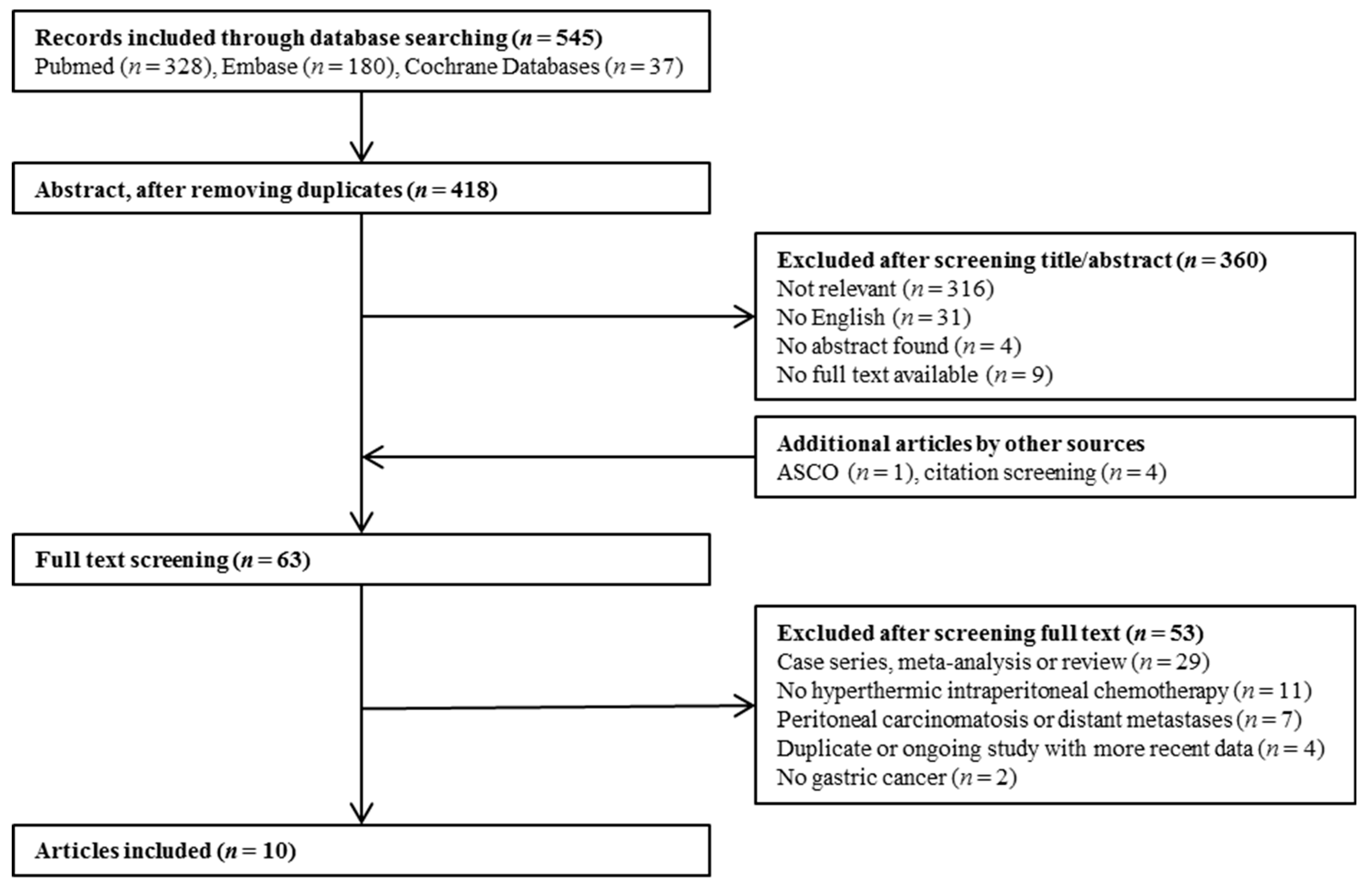
3.1. Literature Search
3.2. Assessment of Risk of Bias
3.3. Treatment
3.4. Morbidity and Mortality
3.5. Survival
3.6. Recurrence
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Ervik, M.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. GLOBOCAN 2012 v1.1, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11; International Agency for Research on Cancer: Lyon, France, 2014; Available online: http://globocan.iarc.fr (accessed on 12 December 2016).
- Al-Batran, S.E.; Homann, N.; Pauligk, C.; Goetze, T.O.; Meiler, J.; Kasper, S.; Kopp, H.G.; Mayer, F.; Haag, G.M.; Luley, K.; et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): A randomised, phase 2/3 trial. Lancet 2019, 393, 1948–1957. [Google Scholar] [PubMed]
- Thomassen, I.; Van Gestel, Y.R.; Van Ramshorst, B.; Luyer, M.D.; Bosscha, K.; Nienhuijs, S.W.; Lemmens, V.E.; De Hingh, I.H. Peritoneal carcinomatosis of gastric origin: A population-based study on incidence, survival and risk factors. Int. J. Cancer 2014, 134, 622–628. [Google Scholar] [CrossRef] [PubMed]
- Issels, R.D. Hyperthermia adds to chemotherapy. Eur. J. Cancer 2008, 44, 2546–2554. [Google Scholar] [CrossRef] [PubMed]
- Van der Speeten, K.; Stuart, O.A.; Sugarbaker, P.H. Using pharmacologic data to plan clinical treatments for patients with peritoneal surface malignancy. Curr. Drug Discov. Technol. 2009, 6, 72–81. [Google Scholar] [CrossRef] [PubMed]
- Yan, T.D.; Deraco, M.; Baratti, D.; Kusamura, S.; Elias, D.; Glehen, O.; Gilly, F.N.; Levine, E.A.; Shen, P.; Mohamed, F.; et al. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for malignant peritoneal mesothelioma: Multiinstitutional experience. J. Clin. Oncol. 2009, 27, 6237–6242. [Google Scholar] [CrossRef]
- Chua, T.C.; Moran, B.J.; Sugarbaker, P.H.; Levine, E.A.; Glehen, O.; Gilly, F.N.; Elias, D.; Baratti, D.; Deraco, M.; Sardi, A.; et al. Early and long-term outcome data on 2298 patients with pseudomyxoma peritonei of appendiceal origin treated by a strategy of cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. J. Clin. Oncol. 2012, 30, 2449–2456. [Google Scholar] [CrossRef]
- Verwaal, V.J.; van Ruth, S.; de Bree, E.; van Sloothen, G.W.; Van Tinteren, H.; Boot, H.; Zoetmulder, F.A. Randomized trial of cytoreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy and palliative surgery in patients with peritoneal carcinomatosis of colorectal cancer. J. Clin. Oncol. 2003, 21, 3737–3743. [Google Scholar] [CrossRef]
- Elias, D.; Goéré, D.; Dumont, F.; Honoré, C.; Dartigues, P.; Stoclin, A.; Malka, D.; Boige, V.; Ducreux, M. Role of hyperthermic intraoperative peritoneal chemotherapy in the management of peritoneal metastases. Eur. J. Cancer 2014, 50, 332–340. [Google Scholar] [CrossRef]
- Glehen, O.; Gilly, F.N.; Arvieux, C.; Cotte, E.; Boutitie, F.; Mansvelt, B.; Bereder, J.M.; Lorimier, G.; Quenet, F.; Elias, D. Peritoneal carcinomatosis from gastric cancer: A multi-institutional study of 159 patients treated by cytoreductive surgery combined with perioperative intraperitoneal chemotherapy. Ann. Surg. Oncol. 2010, 17, 2370–2377. [Google Scholar] [CrossRef]
- Kwon, S.J. Evaluation of the 7th UICC TNM Staging System of Gastric Cancer. J. Gastric Cancer 2011, 11, 78–85. [Google Scholar] [CrossRef]
- Higgins, J.P.; Sterne, J.A.; Savovic, J.; Page, M.J.; Hróbjartsson, A.; Boutron, I.; Reeves, B.; Eldridge, S. A revised tool for assessing risk of bias in randomized trials. Cochrane Database Syst. Rev. 2016, 10 (Suppl. 1), 29–31. [Google Scholar]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomized studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Koga, S.; Hamazoe, R.; Maeta, M.; Shimizu, N.; Murakami, A.; Wakatsuki, T. Prophylactic therapy for peritoneal recurrence of gastric cancer by continuous hyperthermic peritoneal perfusion with mitomycin C. Cancer 1988, 61, 232–237. [Google Scholar] [CrossRef]
- Kaibara, N.; Hamazoe, R.; Iitsuka, Y.; Maeta, M.; Koga, S. Hyperthermic peritoneal perfusion combined with anticancer chemotherapy as prophylactic treatment of peritoneal recurrence of gastric cancer. Hepatogastroenterology 1989, 36, 75–78. [Google Scholar]
- Yonemura, Y.; Ninomiya, I.; Kaji, M.; Sugiyama, K.; Fujimura, K.; Sawa, T.; Katayama, K.; Tanaka, S.; Hirono, Y.; Miwa, K.; et al. Prophylaxis with intraoperative chemohyperthermia against peritoneal recurrence of serosal invasion-positive gastric cancer. World J. Surg. 1995, 19, 450–454. [Google Scholar] [CrossRef]
- Hirose, K.; Katayama, K.; Iida, A.; Yamaguchi, A.; Nakagawara, G.; Umeda, S.; Kusaka, Y. Efficacy of continuous hyperthermic peritoneal perfusion for the prophylaxis and treatment of peritoneal metastasis of advanced gastric cancer: Evaluation by multivariate regression analysis. Oncology 1999, 57, 106–114. [Google Scholar] [CrossRef]
- Kim, J.Y.; Bae, H.S. A controlled clinical study of serosa-invasive gastric carcinoma patients who underwent surgery plus intraperitoneal hyperthermo-chemo-perfusion (IHCP). Gastric Cancer 2001, 4, 27–33. [Google Scholar] [CrossRef]
- Kunisaki, C.; Shimada, H.; Nomura, M.; Akiyama, H.; Takahashi, M.; Matsuda, G. Lack of efficacy of prophylactic continuous hyperthermic peritoneal perfusion on subsequent peritoneal recurrence and survival in patients with advanced gastric cancer. Surgery 2002, 131, 521–528. [Google Scholar] [CrossRef]
- Kunisaki, C.; Shimada, H.; Nomura, M.; Matsuda, G.; Otsuka, Y.; Ono, H.; Akiyama, H. Therapeutic strategy for scirrhous type gastric cancer. Hepatogastroenterology 2005, 52, 314–318. [Google Scholar]
- Coccolini, F.; Celotti, A.; Ceresoli, M.; Montori, G.; Marini, M.; Catena, F.; Ansaloni, L. Hyperthermic intraperitoneal chemotherapy (HIPEC) and neoadjuvant chemotherapy as prophylaxis of peritoneal carcinosis from advanced gastric cancer-effects on overall and disease free survival. J. Gastrointest. Oncol. 2016, 7, 523–529. [Google Scholar] [CrossRef]
- Murata, S.; Kaida, S.; Kodama, H.; Yamamoto, H.; Yamaguchi, T.; Ohtake, R.; Tani, M. A propensity-matched analysis comparing hepatic recurrence after curative gastrectomy followed by adjuvant HIPEC to surgery alone for advanced gastric cancer. J. Clin. Oncol. 2016, 34 (Suppl. 15), 4056. [Google Scholar] [CrossRef]
- Yonemura, Y.; Fujimura, T.; Fushida, S.; Katayama, K.; Bandou, E.; Sugiyama, K.; Kawamura, T.; Kinoshita, K.; Endou, Y.; Sasaki, T.; et al. Intraoperative chemohyperthermic peritoneal perfusion as an adjuvant to gastric cancer: Final results of a randomized controlled study. Hepatogastroenterology 2001, 48, 1776–1782. [Google Scholar] [PubMed]
- Mi, D.H.; Li, Z.; Yang, K.H.; Cao, N.; Lethaby, A.; Tian, J.H.; Santesso, N.; Ma, B.; Chen, Y.L.; Liu, Y.L. Surgery combined with intraoperative hyperthermic intraperitoneal chemotherapy (IHIC) for gastric cancer: A systematic review and meta-analysis of randomised controlled trials. Int. J. Hyperth. 2013, 29, 156–167. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Song, Y.; Wang, Z.; Gao, P.; Chen, X.; Xu, Y.; Liang, J.; Xu, H. Benefits of hyperthermic intraperitoneal chemotherapy for patients with serosal invasion in gastric cancer: A meta-analysis of the randomized controlled trials. BMC Cancer 2012, 12, 526. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.Y.; Xu, Y.Y.; Sun, Z.; Zhu, Z.; Song, Y.X.; Guo, P.T.; You, Y.; Xu, H.M. Comparison different methods of intraoperative and intraperitoneal chemotherapy for patients with gastric cancer: A meta-analysis. Asian Pac. J. Cancer Prev. 2012, 13, 4379–4385. [Google Scholar] [CrossRef]
- Yan, T.D.; Black, D.; Sugarbaker, P.H.; Zhu, J.; Yonemura, Y.; Petrou, G.; Morris, D.L. A systematic review and meta-analysis of the randomized controlled trials on adjuvant intraperitoneal chemotherapy for resectable gastric cancer. Ann. Surg. Oncol. 2007, 14, 2702–2713. [Google Scholar] [CrossRef]
- Xu, D.Z.; Zhan, Y.Q.; Sun, X.W.; Cao, S.M.; Geng, Q.R. Meta-analysis of intraperitoneal chemotherapy for gastric cancer. World J. Gastroenterol. 2004, 10, 2727–2730. [Google Scholar] [CrossRef]
- Bentrem, D.; Wilton, A.; Mazumdar, M.; Brennan, M.; Coit, D. The value of peritoneal cytology as a preoperative predictor in patients with gastric carcinoma undergoing a curative resection. Ann. Surg. Oncol. 2005, 12, 347–353. [Google Scholar] [CrossRef]
- Cunningham, D.; Allum, W.H.; Stenning, S.P.; Thompson, J.N.; Van de Velde, C.J.; Nicolson, M.; Scarffe, J.H.; Lofts, F.J.; Falk, S.J.; Iveson, T.J.; et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N. Engl. J. Med. 2006, 355, 11–20. [Google Scholar] [CrossRef]
- Baratti, D.; Kusamura, S.; Laterza, B.; Balestra, M.R.; Deraco, M. Early and long-term postoperative management following cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. World J. Gastrointest. Oncol. 2010, 2, 36–43. [Google Scholar] [CrossRef]
- Klaver, C.E.; Wisselink, D.D.; Punt, C.J.; Snaebjornsson, P.; Crezee, J.; Aalbers, A.G.; Brandt, A.; Bremers, A.J.; Burger, J.W.; Fabry, H.F.; et al. Adjuvant hyperthermic intraperitoneal chemotherapy in patients with locally advanced colon cancer (COLOPEC): A multicentre, open-label, randomised trial. Lancet Gastroenterol. Hepatol. 2019, 4, 761–770. [Google Scholar] [CrossRef]
- Gill, S.; Shah, A.; Le, N.; Cook, E.F.; Yoshida, E.M. Asian ethnicity-related differences in gastric cancer presentation and outcome among patients treated at a canadian cancer center. J. Clin. Oncol. 2003, 21, 2070–2076. [Google Scholar] [CrossRef] [PubMed]
- Glehen, O.; Passot, G.; Villeneuve, L.; Vaudoyer, D.; Bin-Dorel, S.; Boschetti, G.; Piaton, E.; Garofalo, A. GASTRICHIP: D2 resection and hyperthermic intraperitoneal chemotherapy in locally advanced gastric carcinoma: A randomized and multicenter phase III study. BMC Cancer 2014, 14, 183. [Google Scholar] [CrossRef] [PubMed]
- Dodson, R.M.; McQuellon, R.P.; Mogal, H.D.; Duckworth, K.E.; Russell, G.B.; Votanopoulos, K.I.; Shen, P.; Levine, E.A. Quality-of-Life Evaluation After Cytoreductive Surgery with Hyperthermic Intraperitoneal Chemotherapy. Ann. Surg. Oncol. 2016, 23 (Suppl. 5), 772. [Google Scholar] [CrossRef]


{kind=link}
| Author | Pub. Year | Total Number of Participants | Randomisation | Deviations from Intended Interventions | Missing Outcome Data | Measurement of Outcomes | Reported Result | Overall Risk of Bias |
|---|---|---|---|---|---|---|---|---|
| Koga et al. [14] | 1988 | 60 | Some concerns | High | Low | Low | Low | High |
| Kaibara et al. [15] | 1989 | 82 | Some concerns | Low | Low | Low | Low | Some concerns |
| Author | Pub. Year | Total No. of Participants | Confounding | Selection of Participants | Classification of Interventions | Deviations fromIntended Interventions | Missing Outcome Data | Measurement of Outcomes | Reported Result | Overall Risk of Bias |
|---|---|---|---|---|---|---|---|---|---|---|
| Koga et al. [14] | 1988 | 137 | Serious | Serious | Low | Low | Low | Moderate | Low | Serious |
| Yonemura et al. [16] | 1995 | 160 | Serious | Low | Low | Low | Low | Moderate | Moderate | Serious |
| Hirose et al. [17] | 1999 | 55 | Serious | Low | Low | Low | Low | Low | Moderate | Serious |
| Kim et al. [18] | 2001 | 65 | Serious | Moderate | Low | Low | Low | Moderate | Low | Serious |
| Kunisaki et al. [19] | 2002 | 124 | Serious | Low | Low | Low | Low | Moderate | Low | Serious |
| Kunisaki et al. [20] | 2005 | 61 | Serious | Low | Low | Low | Low | Moderate | Low | Serious |
| Coccolini et al. [21] | 2016 | 34 | Critical | Low | Low | Low | Low | Moderate | Low | Critical |
| Murata et al. [22] | 2016 | 186 | NI | NI | NI | NI | NI | NI | NI | NI |
| Author | Year | Country | Tumor Characteristics | No. of Participants | Therapy Regimen | Overall Survival | 5-Year Survival | Peritoneal Recurrence | Morbidity and Mortality | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HIPEC | SA | HIPEC | SA | HIPEC | SA | HIPEC | SA | HIPEC | SA | HIPEC | SA | HIPEC | SA | |||
| Koga et al. [14] | 1988 | Japan | cT3-4, | cT3-4 | 32 | 28 | CHPP: MMC 8–10 mg/L, total dose 64–100 mg. Temperature: in 44–45 °C, out 40–42 °C. Time: 50–60 min. No CTx. | Surgery alone | NA | NA | NA | NA | NA | NA | Morbidity: NA Mortality: 3.1% | Morbidity: NA Mortality: 0% |
| Kaibara et al. [15] | 1989 | Japan | cT3-4 | cT3-4 | 42 | 40 | CHPP: MMC 10 mg/L, total dose 20 mg. Temperature: in 44–45 °C, out 40–42 °C. Time: 50–60 min. No CTx. | Surgery alone | NA | NA | 71.5% | 59.7% | 11.9% | 20% | Morbidity: 0% | Morbidity: 0% |
| Yonemura et al. [23] | 2001 | Japan | T3-4 | T3-4 | 48 | 47 | CHPP: MMC 30 mg + cisplatin 300 mg. Temperature: 42–43.5 °C. Time: 60 min. No CTx. | Surgery alone | HR 0.42 (95% CI 0.20–0.90) | 61% | 42% | 12.5% | 14.9% | Morbidity: NA | Morbidity: NA Mortality: 4.3% | |
| Author | Year | Country | Tumor Characteristics | No. of Participants | Therapy Regimen | Median Disease Free Survival | Overall Survival | 5-Year Survival | Morbidity and Mortality | Peritoneal Recurrence | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HIPEC | SA | HIPEC | SA | HIPEC | SA | HIPEC | SA | HIPEC | SA | HIPEC | SA | HIPEC | SA | HIPEC | SA | |||
| Koga et al. [14] | 1988 | Japan | cT3-4 | cT3-4 | 59 | 78 | CHPP: MMC 8–10 mg/L, total dose 64–100 mg. Temperature: in 44–45 °C, out 40–42 °C. Time: 50–60 min. | Surgery alone | NA | NA | NA | NA | 63.0% | 43.0% | Mortality: 15.6% Morbidity: NA | Mortality: 9.8% Morbidity: NA | 6.8% (4/59) in 4 years | 14.1% (1/78) in 4 years |
| Yonemura et al. [16] | 1995 | Japan | cT3-T4 | cT3-T4 | 79 | 81 | CHPP: 30 mg MMC + 300 mg CDDP. Temperature: 41.5–43.5 °C. Time: 60 min. Adj. CTx.: 2–3 weeks 400 mg UFT p/o. | Surgery + Adj. CTx.: 2–3 weeks 400 mg UFT p/o. | NA | NA | NA | NA | NA | NA | Mortality: 3.8% | Mortality: 2.5% | NA | NA |
| Hirose et al. [17] | 1999 | Japan | cT3-4 | cT3-4 | 15 | 40 | CHPP: CDDP 100 mg + MMC 20 mg + etoposide 100 mg. Temperature: 41–44.5 °C. Time: 50 min. Adj. CTx: MMC and 5FU | Surgery + Adj. CTx.: MMC and 5FU | NA | NA | 33 m | 22 m | 39.1% | 17.3% | Mortality: 0%. Morbidity: 60% | Mortality: 5%. Morbidity: 42,5% | 26.7% | 45% |
| Kim et al. [18] | 2001 | Korea | pT3-4 | pT3-4 | 29 | 36 | Before closure: MMC 10 µg/mL, 40 mg in total. Temperature: 42–44 °C. Time: 120 min. Adj. CTx.: >6 cycles 5-FU or 5-FU + MMC | Surgery + Adj. CTx.: >6 cycles 5-FU or 5-FU + MMC | NA | NA | NA | NA | 58.5% | 44.4% | NA | NA | ||
| Kunisaki et al. [19] | 2002 | Japan | T3-4 | T3-4 | 45 | 79 | CHPP: 15 mg MMC + 150 mg CDDP + 150 mg etoposide. Temperature.: 42–43 °C. Time: 40 min. Adj. CTx. | Surgery + Some patients adj. CTx. | NA | NA | NA | NA | 48.5% | 55.1% | Morbidity: NA | Morbidity: NA Mortality: 1.3% | 24.4% | 26.6% |
| Kunisaki et al. [20] | 2005 | Japan | cT3-4, linitis plastica | pT2-4, linitis plastica | 6 | 55 | CHPP: 15 mg MMC + 150 mg CDDP + 150 mg etoposide. Temperature.: 42–43 °C. Time: 40 min. Adj. CTx. | Surgery + Some patients adj. CTx. | NA | NA | 32 m | 24 m | NA | NA | NA | NA | NA | NA |
| Coccolini et al. [21] | 2016 | Italy | pT4 | pT3-4 | 6 | 28 | Neoadj. CTx. Before reconstruction open HIPEC: CDDP 100 mg/m2 + paclitaxel 75 mg/m2. Temperature: 40–41 °C. Time: 90 min | Neoadj. CTx. + Surgery | 34.5 m | 24.7 m | 34.6 m | 27.7 m | NA | NA | Morbidity: 16.7% | Morbidity: 16.4% | NA | NA |
| Murata et al. [22] | 2016 | Japan | pT3-4 | pT3-4 | 186 in total | MMC + CDDP +/− 5-FU. Temperature: 42–43 °C. Time: 30 min | Surgery alone | NA | NA | NA | NA | 86.8% | 53.4% | NA | NA | HR: 0.20 (95% CI: 0.068–0.61, p: 0.005) | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brenkman, H.J.F.; Päeva, M.; van Hillegersberg, R.; Ruurda, J.P.; Haj Mohammad, N. Prophylactic Hyperthermic Intraperitoneal Chemotherapy (HIPEC) for Gastric Cancer—A Systematic Review. J. Clin. Med. 2019, 8, 1685. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8101685
Brenkman HJF, Päeva M, van Hillegersberg R, Ruurda JP, Haj Mohammad N. Prophylactic Hyperthermic Intraperitoneal Chemotherapy (HIPEC) for Gastric Cancer—A Systematic Review. Journal of Clinical Medicine. 2019; 8(10):1685. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8101685
Chicago/Turabian StyleBrenkman, H. J. F., M. Päeva, R. van Hillegersberg, J. P. Ruurda, and N. Haj Mohammad. 2019. "Prophylactic Hyperthermic Intraperitoneal Chemotherapy (HIPEC) for Gastric Cancer—A Systematic Review" Journal of Clinical Medicine 8, no. 10: 1685. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8101685