Three-Dimensional Analysis of Initial Brace Correction in the Setting of Adolescent Idiopathic Scoliosis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
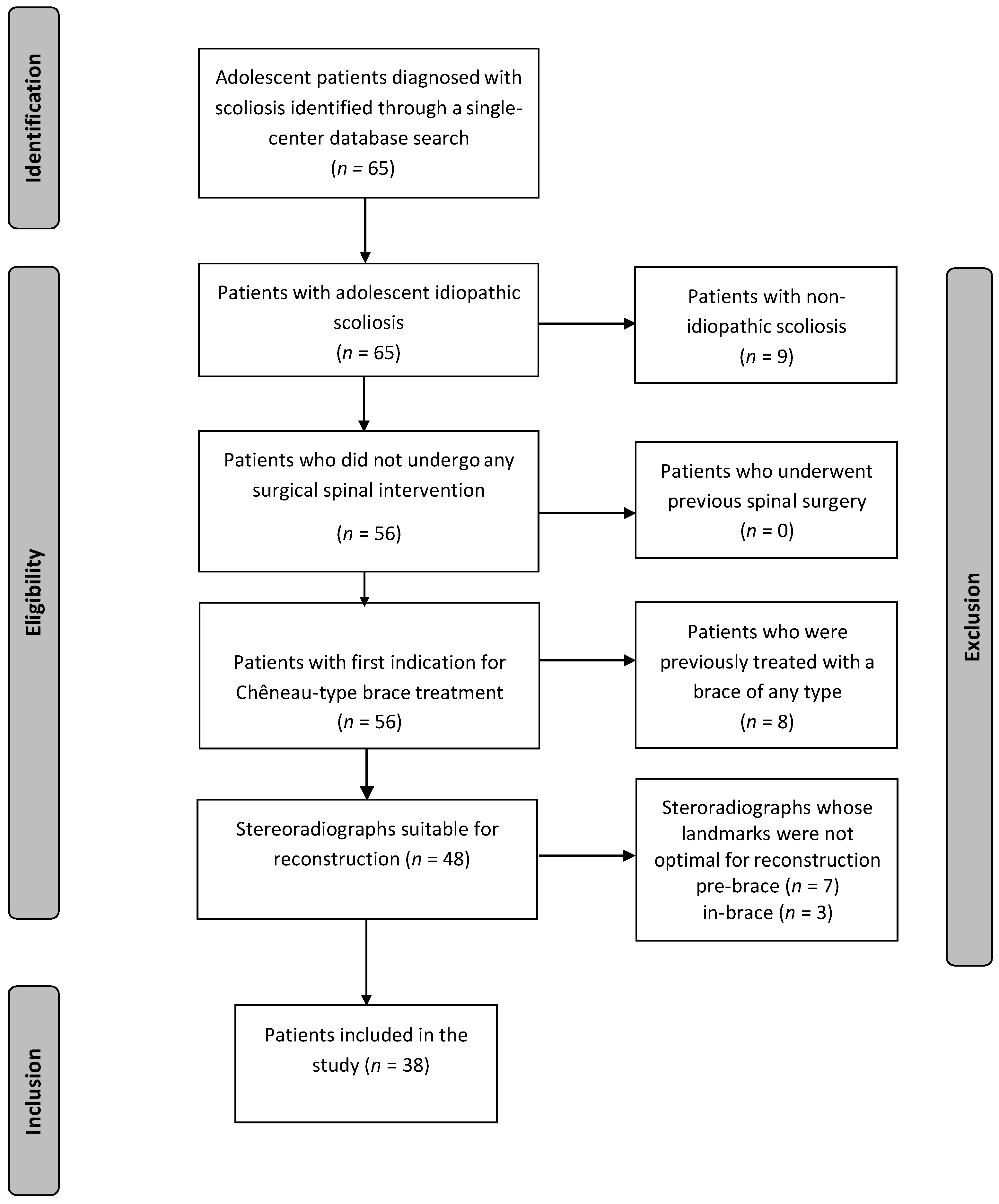
2.1. Inclusion/Exclusion of the Patient Population
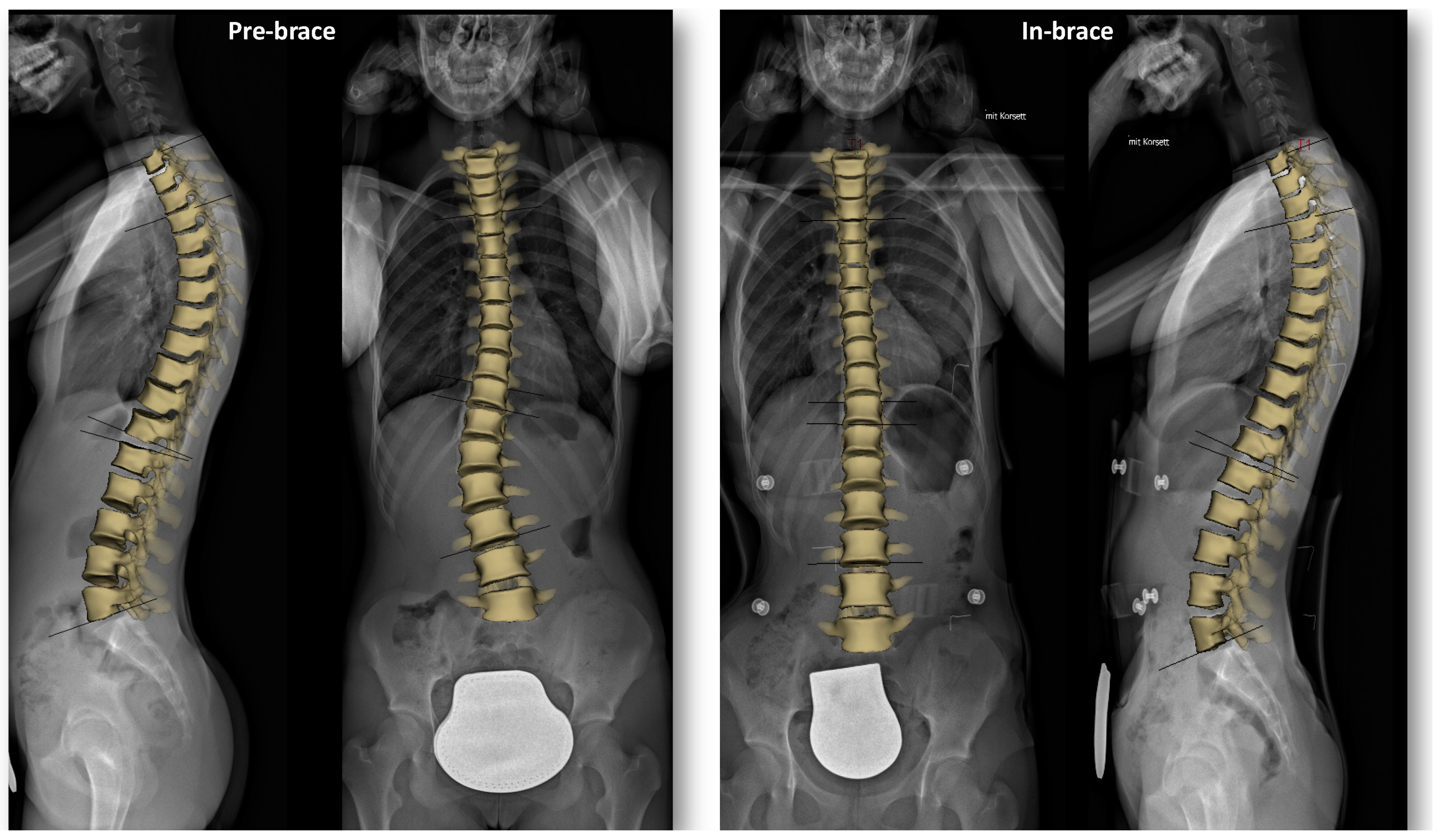
2.2. Radiographic Acquisition and Tridimensional Reconstruction
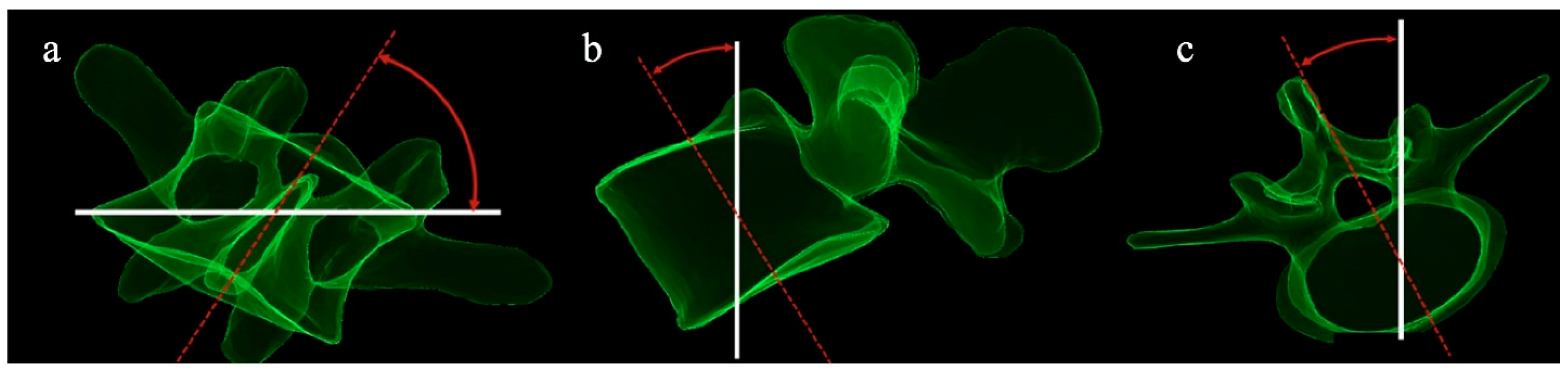
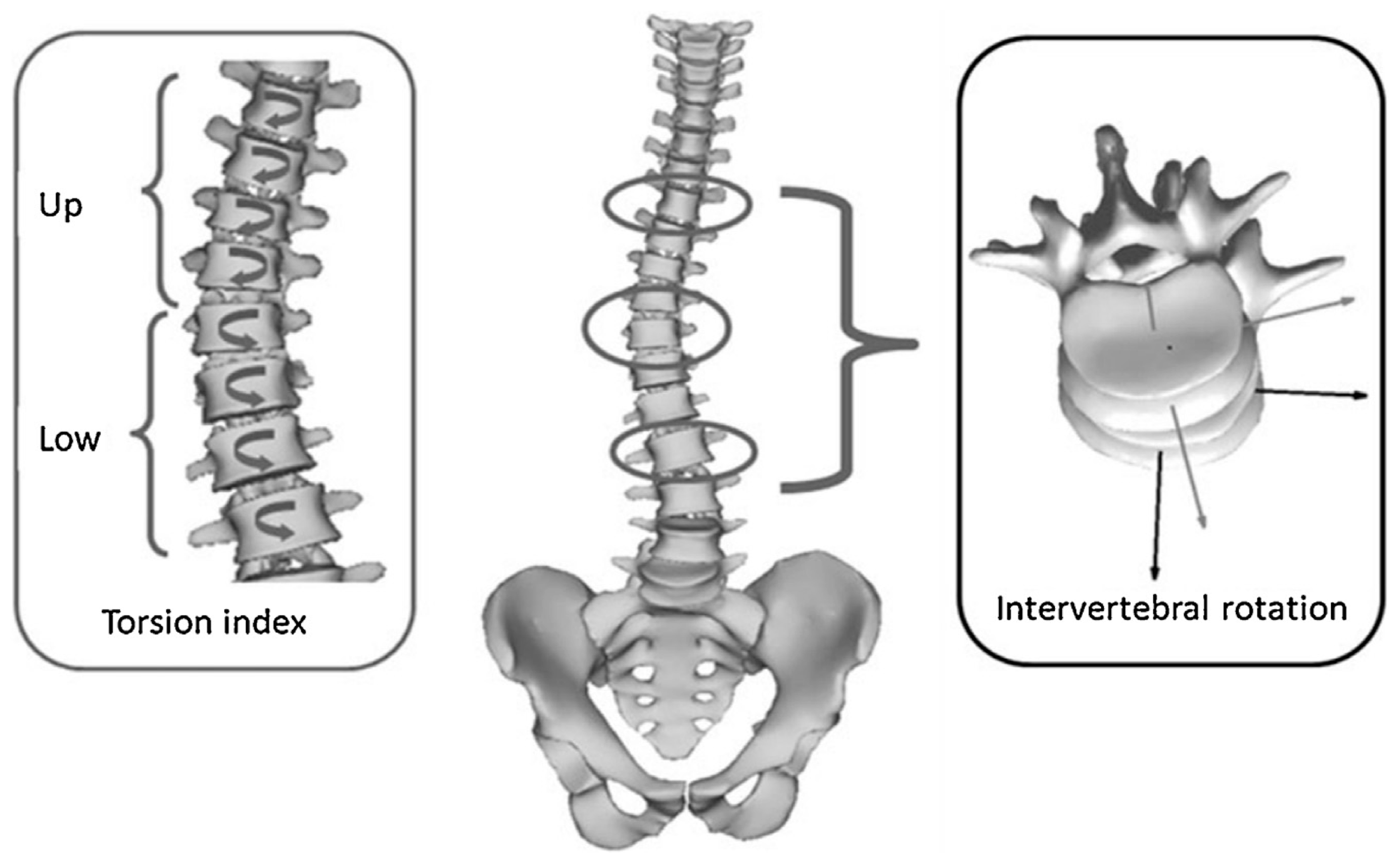
2.3. Anthropometric Outcome Measures and Radiographic Analysis
2.4. Patient Stratification
2.5. Statistical Analysis
3. Results
3.1. Global Analysis
3.2. Sub-Analysis by Curve Type
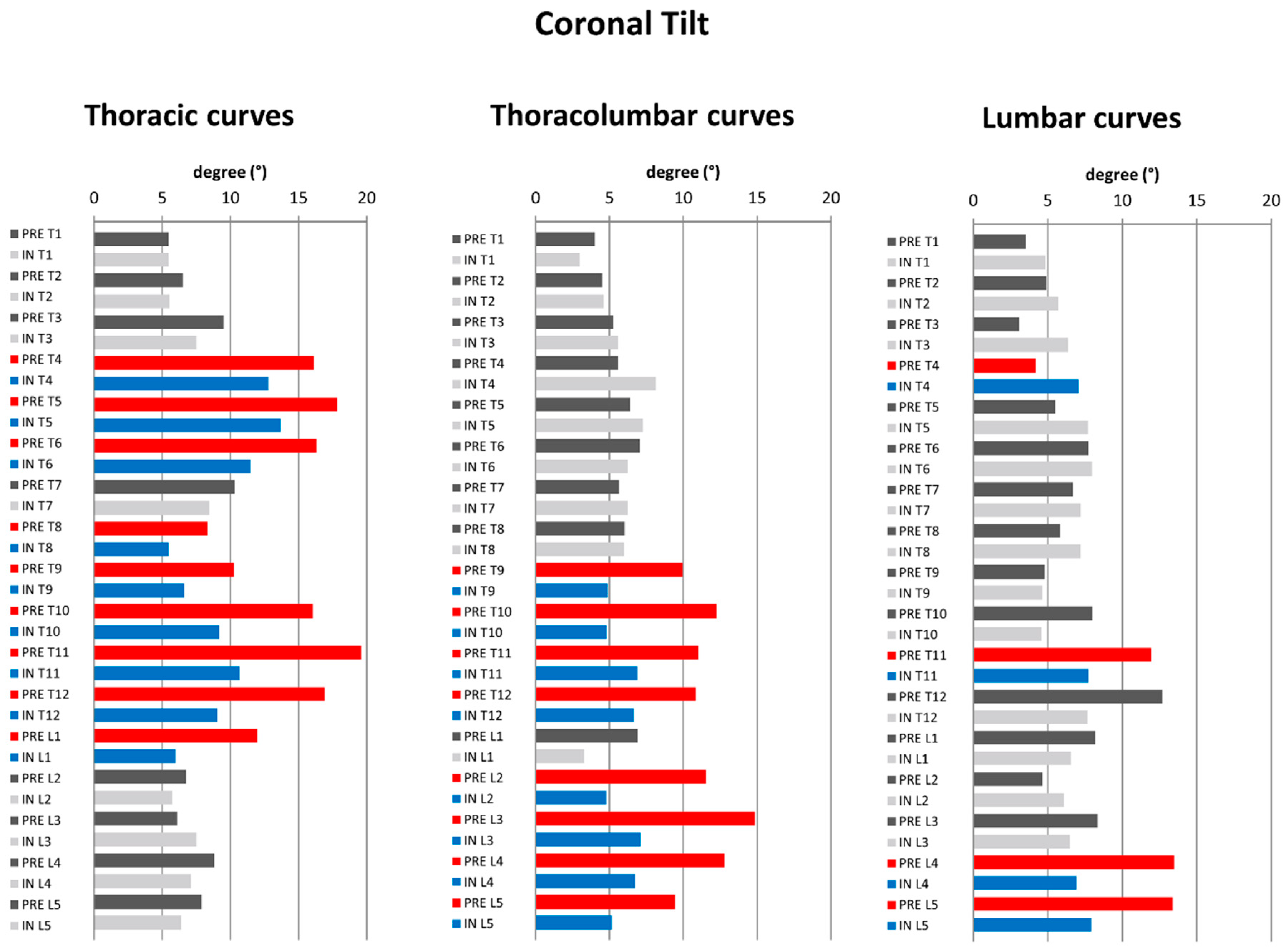
3.2.1. Coronal Plane
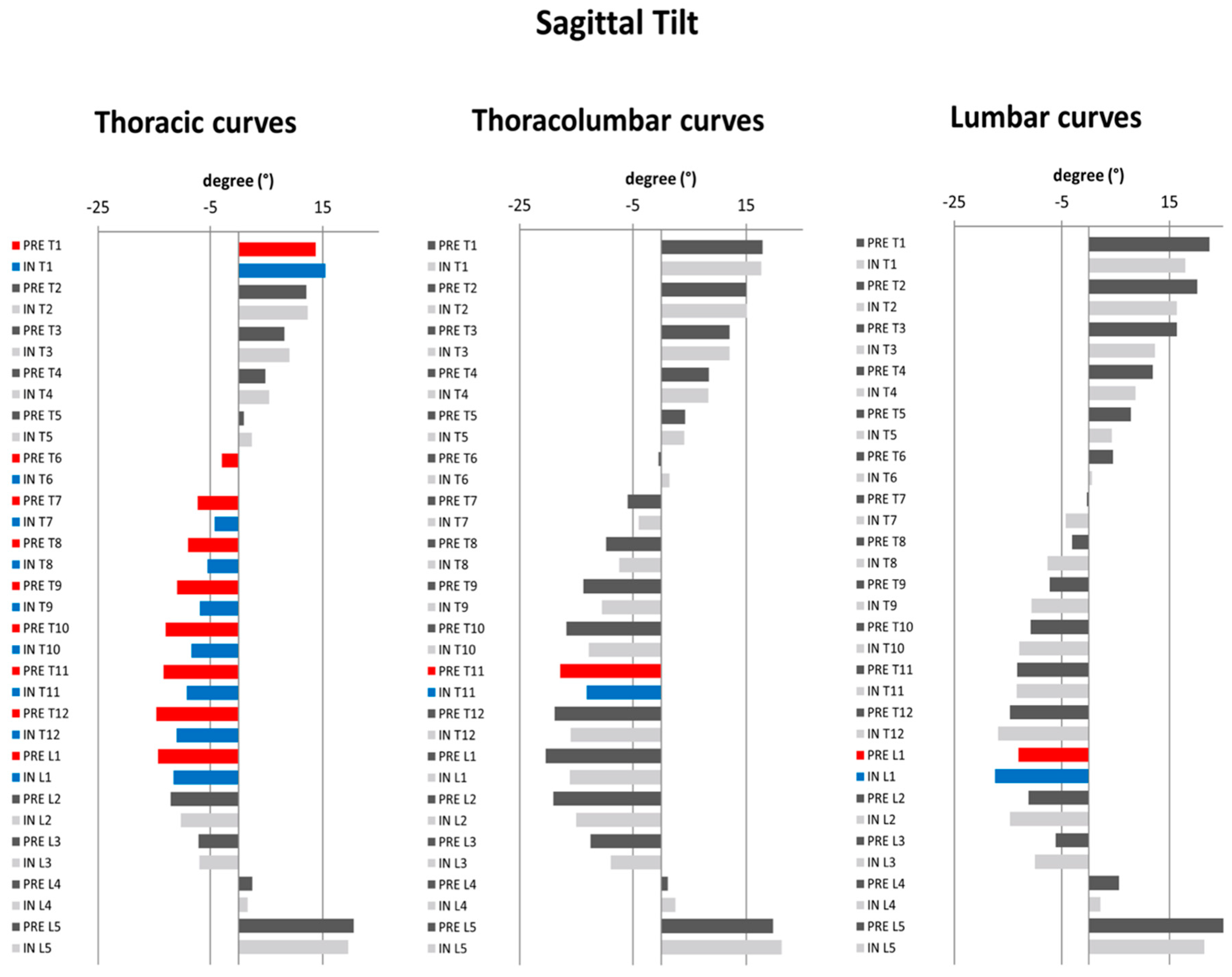
3.2.2. Regional and Global Sagittal Profile
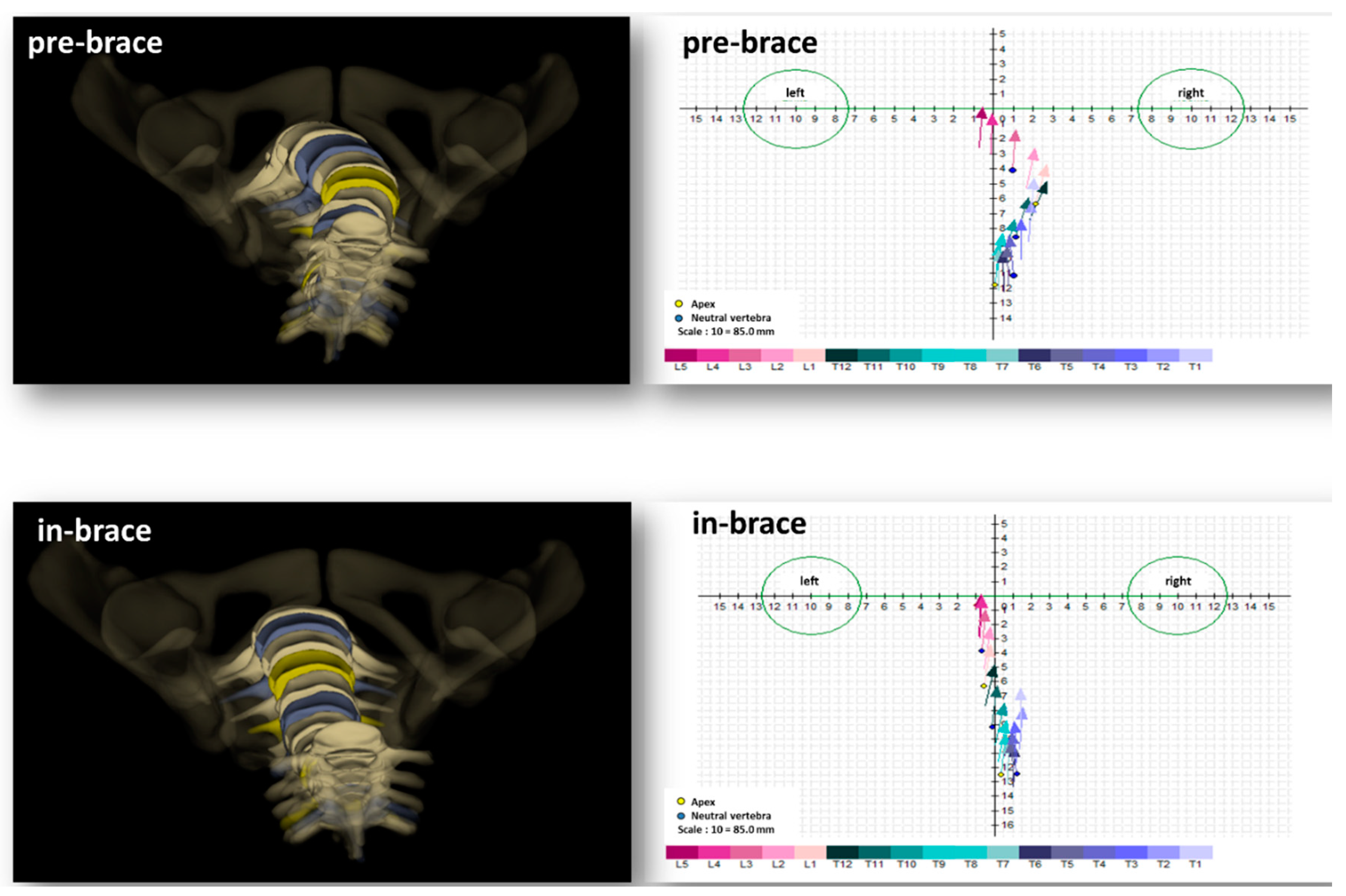
3.2.3. Transverse Plane Parameters (Figure 3)
4. Discussion
4.1. In-Brace Spinopelvic Sagittal Changes
4.2. In-Brace Behavior of Transverse Plane Parameters
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Weinstein, S.L.; Dolan, L.A.; Wright, J.G.; Dobbs, M.B. Design of the Bracing in Adolescent Idiopathic Scoliosis Trial (BrAIST). Spine 2013, 38, 1832–1841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perdriolle, R.; Vidal, J. A study of scoliotic curve. The importance of extension and vertebral rotation (author’s transl). Rev. Chir. Orthopédique Réparatrice Appar. Mot. 1981, 67, 25–34. [Google Scholar]
- Courvoisier, A. Letter to the Editor: The Chêneau brace. J. Neurosurg. Spine 2016, 25, 138–139. [Google Scholar] [CrossRef] [PubMed]
- Fang, M.-Q.; Wang, C.; Xiang, G.-H.; Lou, C.; Tian, N.-F.; Xu, H.-Z. Long-term effects of the Chêneau brace on coronal and sagittal alignment in adolescent idiopathic scoliosis. J. Neurosurg. Spine 2015, 23, 505–509. [Google Scholar] [CrossRef] [PubMed]
- Negrini, S.; Minozzi, S.; Bettany-Saltikov, J.; Chockalingam, N.; Grivas, T.B.; Kotwicki, T.; Maruyama, T.; Romano, M.; Zaina, F. Braces for idiopathic scoliosis in adolescents. Cochrane Database Syst. Rev. 2015, 6, CD006850. [Google Scholar] [CrossRef] [PubMed]
- De Giorgi, S.; Piazzolla, A.; Tafuri, S.; Borracci, C.; Martucci, A.; De Giorgi, G. Chêneau brace for adolescent idiopathic scoliosis: Long–term results. Can it prevent surgery? Eur. Spine J. 2013, 22, 815–822. [Google Scholar] [CrossRef] [PubMed]
- Rigo, M.; Negrini, S.; Weiss, H.R.; Grivas, T.; Maruyama, T.; Kotwicki, T. SOSORT consensus paper on brace action: TLSO biomechanics of correction (investigating the rationale for force vector selection). Scoliosis 2006, 1, 11. [Google Scholar] [CrossRef]
- Kuroki, H. Brace Treatment for Adolescent Idiopathic Scoliosis. J. Clin. Med. 2018, 7, 136. [Google Scholar] [CrossRef]
- Moe, J.H. Moe’s Textbook of Scoliosis and Other Spinal Deformities; Saunders: Philadelphia, PA, USA, 1995. [Google Scholar]
- MacLean, W.E., Jr.; Green, N.E.; Pierre, C.B.; Ray, D.C. Stress and coping with scoliosis: Psychological effects on adolescents and their families. J. Pediatric Orthop. 1989, 9, 257–261. [Google Scholar] [CrossRef]
- Matsunaga, S.; Hayashi, K.; Naruo, T.; Nozoe, S.-I.; Komiya, S. Psychologic management of brace therapy for patients with idiopathic scoliosis. Spine 2005, 30, 547–550. [Google Scholar] [CrossRef]
- Rivett, L.; Rothberg, A.; Stewart, A.; Berkowitz, R. The relationship between quality of life and compliance to a brace protocol in adolescents with idiopathic scoliosis: A comparative study. BMC Musculoskelet. Disord. 2009, 10, 5. [Google Scholar] [CrossRef] [PubMed]
- Mac–Thiong, J.M.; Labelle, H.; Charlebois, M.; Huot, M.P.; de Guise, J.A. Sagittal plane analysis of the spine and pelvis in adolescent idiopathic scoliosis according to the coronal curve type. Spine 2003, 28, 1404–1409. [Google Scholar] [CrossRef] [PubMed]
- Upasani, V.V.; Tis, J.; Bastrom, T.; Pawelek, J.; Marks, M.; Lonner, B.; Crawford, A.; Newton, P.O. Analysis of sagittal alignment in thoracic and thoracolumbar curves in adolescent idiopathic scoliosis: How do these two curve types differ? Spine 2007, 32, 1355–1359. [Google Scholar] [CrossRef]
- Nault, M.L.; Mac-Thiong, J.M.; Roy-Beaudry, M.; Turgeon, I.; Deguise, J.; Labelle, H.; Parent, S. Three–dimensional spinal morphology can differentiate between progressive and Non–progressive patients with adolescent idiopathic scoliosis at the initial presentation. Spine 2014, 39, E601–E606. [Google Scholar] [CrossRef] [PubMed]
- Labelle, H.; Aubin, C.E.; Jackson, R.; Lenke, L.; Newton, P.; Parent, S. Seeing the spine in 3D: How will it change what we do? J. Pediatr. Orthop. 2011, 31, S37–S45. [Google Scholar] [CrossRef] [PubMed]
- Negrini, S.; Donzelli, S.; Aulisa, A.G.; Czaprowski, D.; Schreiber, S.; de Mauroy, J.C.; Diers, H.; Grivas, T.B.; Knott, P.; Kotwicki, T.; et al. 2016 SOSORT guidelines: Orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis Spinal Disord. 2018, 13, 3. [Google Scholar] [CrossRef] [PubMed]
- Rigo, M.; Jelačić, M. Brace technology thematic series: The 3D Rigo Chêneau-type brace. Scoliosis Spinal Disord. 2017, 12, 10. [Google Scholar] [CrossRef]
- Negrini, S.; Hresko, T.M.; O’Brien, J.P.; Price, N.; Boards, S.; SRS Non-Operative Committee. Recommendations for research studies on treatment of idiopathic scoliosis: Consensus 2014 between SOSORT and SRS non-operative management committee. Scoliosis 2015, 10, 8. [Google Scholar] [CrossRef]
- Almansour, H.; Pepke, W.; Rehm, J.; Bruckner, T.; Spira, D.; Akbar, M. Interrater reliability of three-dimensional reconstruction of the spine: Low-dose stereoradiography for evaluating bracing in adolescent idiopathic scoliosis. Orthopäde 2019. [Google Scholar] [CrossRef]
- Dubousset, J.; Charpak, G.; Dorion, I.; Skalli, W.; Lavaste, F.; DeGuise, J.; Kalifa, G.; Ferey, S. A new 2D and 3D imaging approach to musculoskeletal physiology and pathology with low-dose radiation and the standing position: The EOS system. Bull. Acad. Natl. Med. 2005, 189, 287–297. [Google Scholar]
- Ferrero, E.; Lafage, R.; Challier, V.; Diebo, B.; Guigui, P.; Mazda, K.; Schwab, F.; Skalli, W.; Lafage, V. Clinical and stereoradiographic analysis of adult spinal deformity with and without rotatory subluxation. Orthop. Traumatol. Surg. Res. 2015, 101, 613–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Humbert, L.; De Guise, J.; Aubert, B.; Godbout, B.; Skalli, W.; De Guise, J. 3D reconstruction of the spine from biplanar X-rays using parametric models based on transversal and longitudinal inferences. Med. Eng. Phys. 2009, 31, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Sangole, A.; Aubin, C.E.; Labelle, H.; Lenke, L.; Jackson, R.; Newton, P.; Stokes, I.A.; Scoliosis Research Society 3D Scoliosis Committee. The central hip vertical axis: A reference axis for the Scoliosis Research Society three–dimensional classification of idiopathic scoliosis. Spine 2010, 35, E530–E534. [Google Scholar] [CrossRef] [PubMed]
- Courvoisier, A.; Drevelle, X.; Vialle, R.; Dubousset, J.; Skalli, W. 3D analysis of brace treatment in idiopathic scoliosis. Eur. Spine J. 2013, 22, 2449–2455. [Google Scholar] [CrossRef] [Green Version]
- Steib, J.P.; Dumas, R.; Mitton, D.; Skalli, W. Surgical correction of scoliosis by in situ contouring: A detorsion analysis. Spine 2004, 29, 193–199. [Google Scholar] [CrossRef]
- Courvoisier, A.; Drevelle, X.; Dubousset, J.; Skalli, W. Transverse plane 3D analysis of mild scoliosis. Eur. Spine J. 2013, 22, 2427–2432. [Google Scholar] [CrossRef] [Green Version]
- Donzelli, S.; Zaina, F.; Lusini, M.; Minnella, S.; Respizzi, S.; Balzarini, L.; Poma, S.; Negrini, S. The three dimensional analysis of the Sforzesco brace correction. Scoliosis Spinal Disord. 2016, 11, 34. [Google Scholar] [CrossRef]
- Mac–Thiong, J.M.; Labelle, H.; Berthonnaud, E.; Betz, R.R.; Roussouly, P. Sagittal spinopelvic balance in normal children and adolescents. Eur. Spine J. 2007, 16, 227–234. [Google Scholar] [CrossRef]
- Clin, J.; Aubin, C.É.; Sangole, A.; Labelle, H.; Parent, S. Correlation between immediate in–brace correction and biomechanical effectiveness of brace treatment in adolescent idiopathic scoliosis. Spine 2010, 35, 1706–1713. [Google Scholar] [CrossRef]
- Roussouly, P.; Pinheiro-Franco, J.L. Biomechanical analysis of the spino-pelvic organization and adaptation in pathology. Eur. Spine J. 2011, 20, 609–618. [Google Scholar] [CrossRef] [Green Version]
- Pepke, W.; Almansour, H.; Lafage, R.; Diebo, B.G.; Wiedenhöfer, B.; Schwab, F.; Lafage, V.; Akbar, M. Cervical spine alignment following surgery for adolescent idiopathic scoliosis (AIS): A pre-to-post analysis of 81 patients. BMC Surg. 2019, 19, 7. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Yang, C.; Chen, Z.; Wei, X.; Chen, Y.; Zhao, J.; Shao, J.; Zhu, X.; Li, M. Lumbar lordosis minus thoracic kyphosis: Remain constant in adolescent idiopathic scoliosis patients before and after correction surgery. Spine 2016, 41, E359–E363. [Google Scholar] [CrossRef] [PubMed]
- Ilharreborde, B. Sagittal balance and idiopathic scoliosis: Does final sagittal alignment influence outcomes, degeneration rate or failure rate? Eur. Spine J. 2018, 27, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Labelle, H.; Dansereau, J.; Bellefleur, C.; Poitras, B. Three–dimensional effect of the Boston brace on the thoracic spine and rib cage. Spine 1996, 21, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Illés, T.; Tunyogi–Csapó, M.; Somoskeöy, S. Breakthrough in three–dimensional scoliosis diagnosis: Significance of horizontal plane view and vertebra vectors. Eur. Spine J. 2011, 20, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Lebel, D.E.; Al-Aubaidi, Z.; Shin, E.-J.; Howard, A.; Zeller, R. Three dimensional analysis of brace biomechanical efficacy for patients with AIS. Eur. Spine J. 2013, 22, 2445–2448. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Global Changes of Sagittal Parameter | |||||
|---|---|---|---|---|---|
| Before Brace | In Brace | Mean Difference | p | Absolute Mean Difference | |
| TK (T1/T12) | 33.2 ± 11.5 | 30.9 ± 11.3 | 2.3 ± 8.3 | 0.095 | 2.3 ± 8.3 |
| TK (T4/T12) | 24.8 ± 12.6 | 22.2 ± 12.4 | 2.6 ± 6.3 | 0.017 | 2.6 ± 6.3 |
| LL (L1/L5) | 43.9 ± 10.4 | 41.3 ± 11.0 | 2.6 ± 6.7 | 0.020 | 2.6 ± 6.7 |
| LL (L1/S1) | 55.7 ± 10.8 | 52.0 ± 12.1 | 3.8 ± 7.5 | 0.004 | 3.8 ± 7.5 |
| PT | 6.7 ± 8.0 | 8.3 ± 7.8 | −1.6 ± 4.9 | 0.057 | 3.6 ± 3.7 |
| PI | 48.3 ± 12.0 | 46.6 ± 12.8 | 1.7 ± 6.3 | 0.109 | 1.7 ± 6.3 |
| SS | 41.6 ± 9.6 | 38.3 ± 10.0 | 3.3 ± 6.5 | 0.004 | 3.3 ± 6.5 |
| Pelvic Obliquity (mm) | 4.4 ± 2.7 | 4.1 ± 3.1 | 0.3 ± 2.5 | 0.446 | 0.3 ± 2.5 |
| SVA (mm) | −8.3 ± 28.8 | −6.7 ± 25.1 | −1.6 ± 31.6 | 0.752 | 23.6 ± 20.6 |
| SSA | 132.7 ± 9.8 | 130.2 ± 9.7 | 2.4 ± 6.2 | 0.019 | 2.4 ± 6.2 |
| T1SPi | 4.0 ± 3.9 | 4.0 ± 3.6 | −0.06 ± 4.0 | 0.921 | 3 ± 2.6 |
| T9SPi | 7.4 ± 5.0 | 7.3 ± 4.5 | 0.07 ± 4.7 | 0.930 | 3.4 ± 3.3 |
| TK (TK1/TK12) = thoracic kyphosis measured from TK 1 to TK 12, TK (TK4/TK12) = thoracic kyphosis measured from TK 4 to TK 12, LL-L5 (L1/L5) = lumbar lordosis measured from L1 to L5, LL-S1 (L1/S1) = lumbar lordosis measured from L1 to S1, PT = pelvic tilt, PI = Pelvic incidence, SS = sacral slope, SVA = sagittal vertical axis (mm), SSA = spinosacral angle, T1SPi = T1 spinopelvic inclination, T9SPi = T9 spinopelvic inclination. Bold denotes statistical significance. All angles are given with °. | |||||
| Stratification by Scoliosis Type | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Thoracic | Thoracolumbar | Lumbar | ||||||||||
| Before Brace | In Brace | Mean Difference | p | Before Brace | In Brace | Mean Difference | p | Before Brace | In Brace | Mean Difference | p | |
| Cobb angle | 34.2 ± 5.6 | 23.5 ± 8.0 | 10.6 ± 6.0 | 0.000 | 29.4 ± 6.4 | 12.9 ± 8.1 | 16.5 ± 5.5 | 0.000 | 27.6 ± 6.2 | 15.6 ± 4.3 | 12.4 ± 6.7 | 0.000 |
| TK (T1/T12) | 29.0 ± 11.6 | 27.0 ± 11.1 | 1.9 ± 6.3 | 0.196 | 37.8 ± 7.4 | 33.8 ± 13.4 | 4.0 ± 10.3 | 0.276 | 36.9 ± 12.2 | 35.5 ± 7.6 | 1.5 ± 10.1 | 0.660 |
| TK (T4/T12) | 20.8 ± 14.5 | 17.7 ± 12.1 | 3.1 ± 5.3 | 0.021 | 29.3 ± 8.4 | 26.2 ± 13.2 | 3.2 ± 7.8 | 0.261 | 28.4 ± 9.7 | 27.4 ± 9.5 | 1.0 ± 7.2 | 0.658 |
| LL–L5 (L1/L5) | 42.2 ± 10.8 | 38.1 ± 12.0 | 4.1 ± 5.7 | 0.006 | 46.2 ± 7.4 | 42.7 ± 9.3 | 3.5 ± 7.2 | 0.183 | 45.0 ± 12.2 | 46.0 ± 9.4 | −0.1 ± 7.2 | 0.672 |
| LL–S1 (L1/S1) | 53.0 ± 10.4 | 47.6 ± 12.6 | 5.4 ± 5.6 | 0.001 | 59.6 ± 9.5 | 52.2 ± 9.8 | 7.5 ± 8.6 | 0.032 | 57.3 ± 12.2 | 60.1 ± 8.9 | −2.7 ± 6.0 | 0.186 |
| PT | 7.3 ± 8.7 | 8.4 ± 8.6 | –1.2 ± 4.4 | 0.256 | 4.3 ± 7.2 | 5.8 ± 5.0 | −1.5 ± 5.6 | 0.450 | 8.2 ± 7.8 | 10.0 ± 7.9 | −1.8 ± 4.3 | 0.211 |
| PI | 47.3 ± 12.6 | 44.5 ± 14.1 | 2.8 ± 8.0 | 0.142 | 44.7 ± 7.8 | 43.6 ± 8.6 | 1.1 ± 4.1 | 0.433 | 53.3 ± 13.0 | 53.5 ± 12.3 | −0.2 ± 4.0 | 0.882 |
| SS | 40.0 ± 10.7 | 36.0 ± 11.3 | 4.0 ± 6.2 | 0.011 | 40.4 ± 6.3 | 37.8 ± 6.7 | 2.6 ± 6.4 | 0.255 | 45.2 ± 9.5 | 43.6 ± 8.8 | 1.7 ± 5.7 | 0.379 |
| Pelvic Obliquity (mm) | 4.0 ± 2.3 | 4.3 ± 3.2 | −0.4 ± 2.7 | 0.530 | 5.2 ± 2.7 | 4.4 ± 3.0 | 0.8 ± 2.3 | 0.336 | 4.8 ± 3.5 | 3.8 ± 3.2 | 1.0 ± 2.5 | 0.224 |
| SVA (mm) | −11.1 ± 15.3 | 0.1 ± 22.7 | −11.2 ± 20.7 | 0.030 | −28.1 ± 29.5 | −17.6 ± 32.2 | −10.6 ± 39.0 | 0.441 | 15.0 ± 34.1 | −9.9 ± 28.9 | 24.8 ± 28.9 | 0.024 |
| SSA | 132.3 ± 10.8 | 127.9 ± 11.2 | 4.4 ± 5.1 | 0.001 | 134.0 ± 8.1 | 129.9 ± 7.6 | 4.1 ± 3.5 | 0.007 | 132.1 ± 9.9 | 134.9 ± 7.2 | −2.8 ± 7.2 | 0.249 |
| T1SPi | 4.3 ± 2.6 | 3.5 ± 3.6 | 0.7 ± 2.8 | 0.266 | 5.9 ± 4.0 | 4.4 ± 3.2 | 1.5 ± 5.3 | 0.432 | 1.7 ± 4.9 | 4.6 ± 4.0 | −2.9 ± 3.7 | 0.036 |
| T9SPi | 6.9 ± 4.8 | 6.5 ± 5.1 | 0.4 ± 3.1 | 0.556 | 10.0 ± 4.6 | 7.8 ± 3.9 | 2.2 ± 6.6 | 0.351 | 5.9 ± 5.2 | 8.4 ± 3.6 | −2.5 ± 4.8 | 0.135 |
| AVR | 8.1 ± 5.2 | 7.4 ± 4.4 | 0.7 ± 5.1 | 0.586 | 14.5 ± 8.6 | 10.2 ± 7.0 | 4.4 ± 4.2 | 0.014 | 10.6 ± 4.4 | 10.1 ± 4.2 | 0.6 ± 6.9 | 0.796 |
| Upper IAR | 8 ± 6.7 | 6.3 ± 4.7 | 1.7 ± 5.4 | 0.188 | 7.9 ± 4.3 | 4.1 ± 3.5 | 3.8 ± 3.8 | 0.018 | 5.6 ± 4.7 | 4.4 ± 3.8 | 1.3 ± 2.8 | 0.186 |
| Lower IAR | 7.4 ± 6.6 | 8.4 ± 5.2 | 0.9 ± 5.5 | 0.471 | 5.9 ± 3.9 | 3.7 ± 3.2 | 2.2 ± 3.8 | 0.117 | 4.4 ± 3.1 | 3.5 ± 2.9 | 0.8 ± 2.7 | 0.383 |
| Ti | 7.7 ± 6.1 | 7.3 ± 4.3 | 0.4 ± 5.1 | 0.744 | 6.9 ± 3.0 | 3.9 ± 3.2 | 3.0 ± 2.9 | 0.016 | 5.0 ± 2.6 | 3.9 ± 1.6 | 1.0 ± 1.7 | 0.092 |
| TK (TK1/TK12) = thoracic kyphosis measured from TK 1 to TK 12, TK (TK4/TK12) = thoracic kyphosis measured from TK 4 to TK 12, LL (L1/L5) = lumbar lordosis measured from L1 to L5, LL (L1/S1) = lumbar lordosis measured from L1 to S1, PT = pelvic tilt, PI = pelvic incidence, SS = sacral slope, SVA = sagittal vertical axis (mm), SSA = spinosacral angle, T1SPi = T1 spinopelvic inclination, T9SPi = T9 spinopelvic inclination; AVR = axial rotation of the apical vertebra; IAR = intervertebral axial rotation; Ti = torsion index. Data expressed as mean ± standard deviation; Bold denotes statistical significance, p ≤ 0.05. | ||||||||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almansour, H.; Pepke, W.; Bruckner, T.; Diebo, B.G.; Akbar, M. Three-Dimensional Analysis of Initial Brace Correction in the Setting of Adolescent Idiopathic Scoliosis. J. Clin. Med. 2019, 8, 1804. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8111804
Almansour H, Pepke W, Bruckner T, Diebo BG, Akbar M. Three-Dimensional Analysis of Initial Brace Correction in the Setting of Adolescent Idiopathic Scoliosis. Journal of Clinical Medicine. 2019; 8(11):1804. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8111804
Chicago/Turabian StyleAlmansour, Haidara, Wojciech Pepke, Thomas Bruckner, Bassel G. Diebo, and Michael Akbar. 2019. "Three-Dimensional Analysis of Initial Brace Correction in the Setting of Adolescent Idiopathic Scoliosis" Journal of Clinical Medicine 8, no. 11: 1804. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8111804