PD-L1 Expression and Tumor-Infiltrating Lymphocytes in Thymic Epithelial Neoplasms

 , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Patients
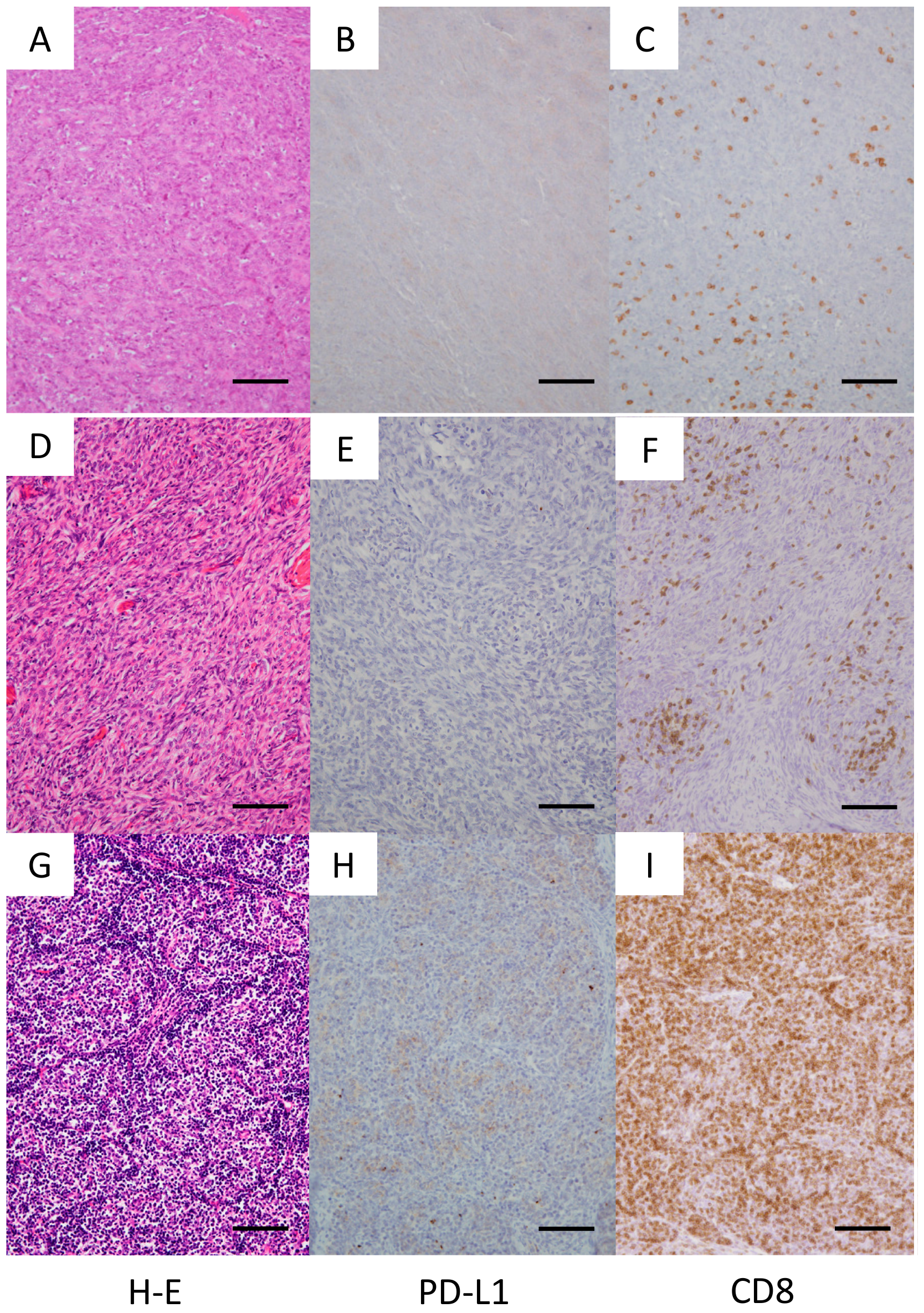
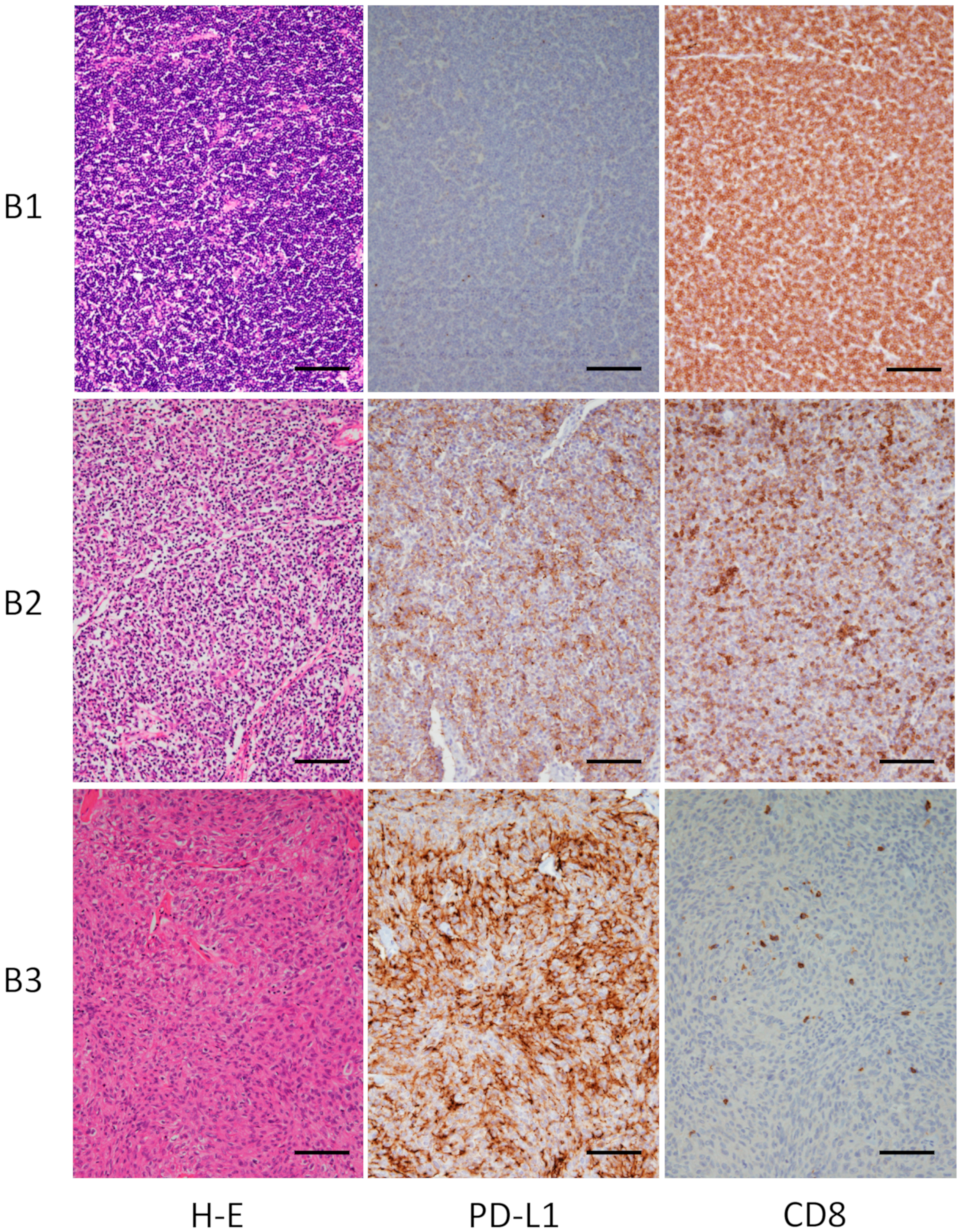
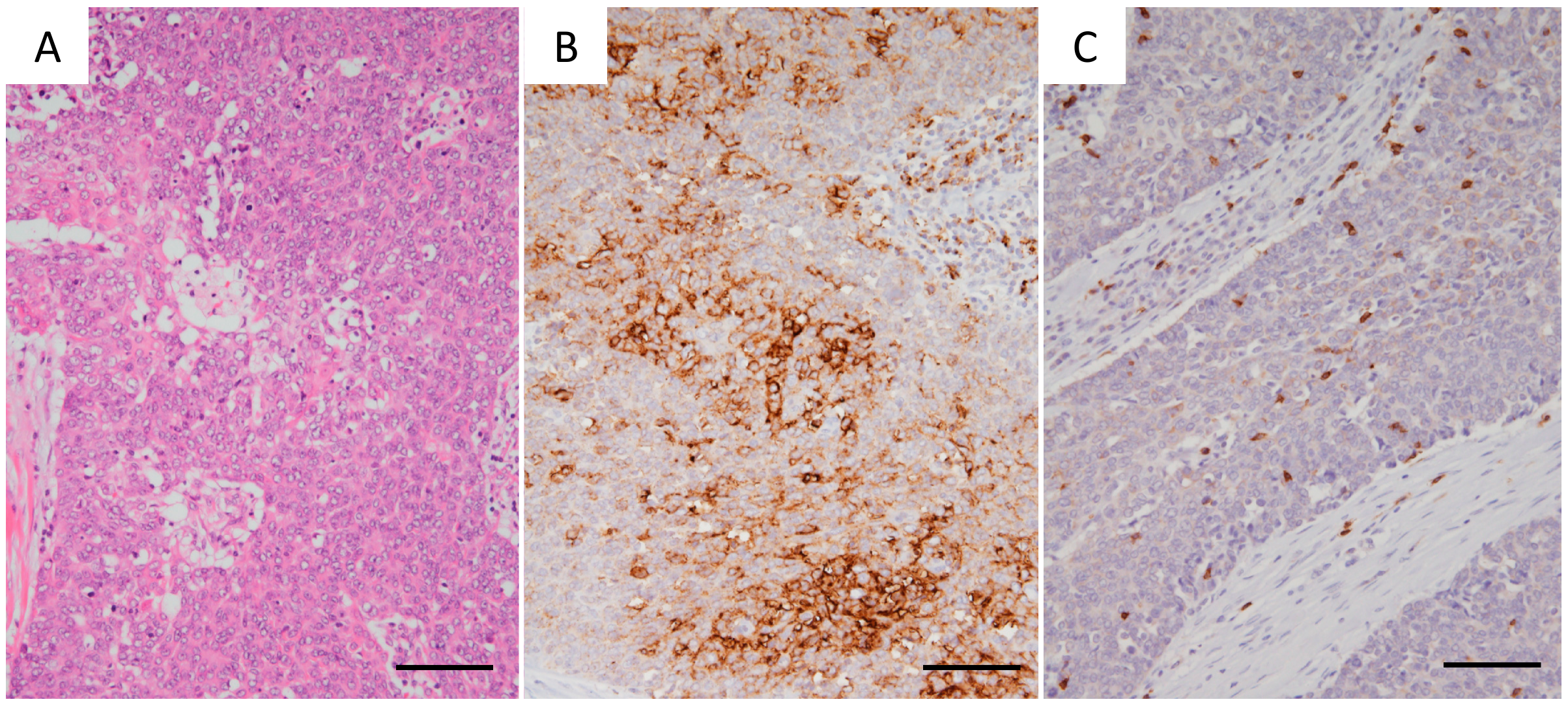
2.2. Immunohistochemistry for PD-L1 and TILs
2.3. mRNA Expression and Quantitative Real-Time PCR Analyses
2.4. Statistical Analyses
3. Results
3.1. Patient Characteristics
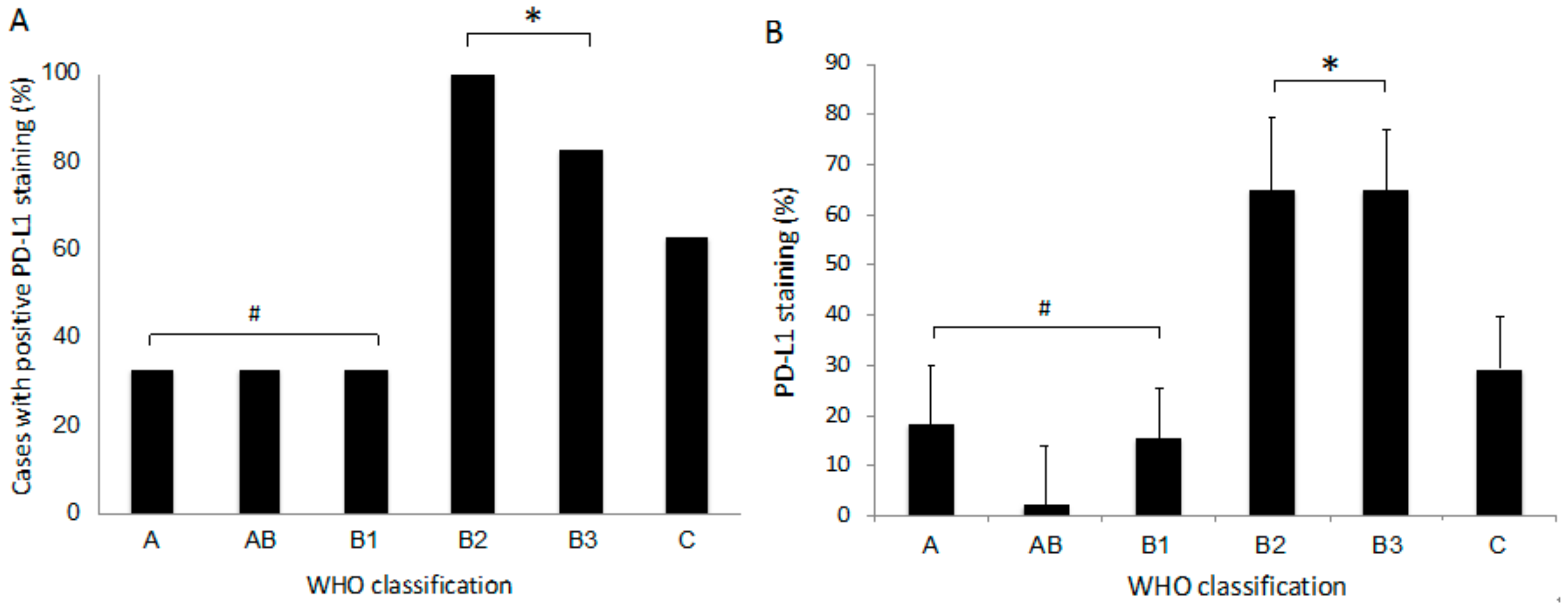
3.2. Expression of PD-L1 in Tumor Cells
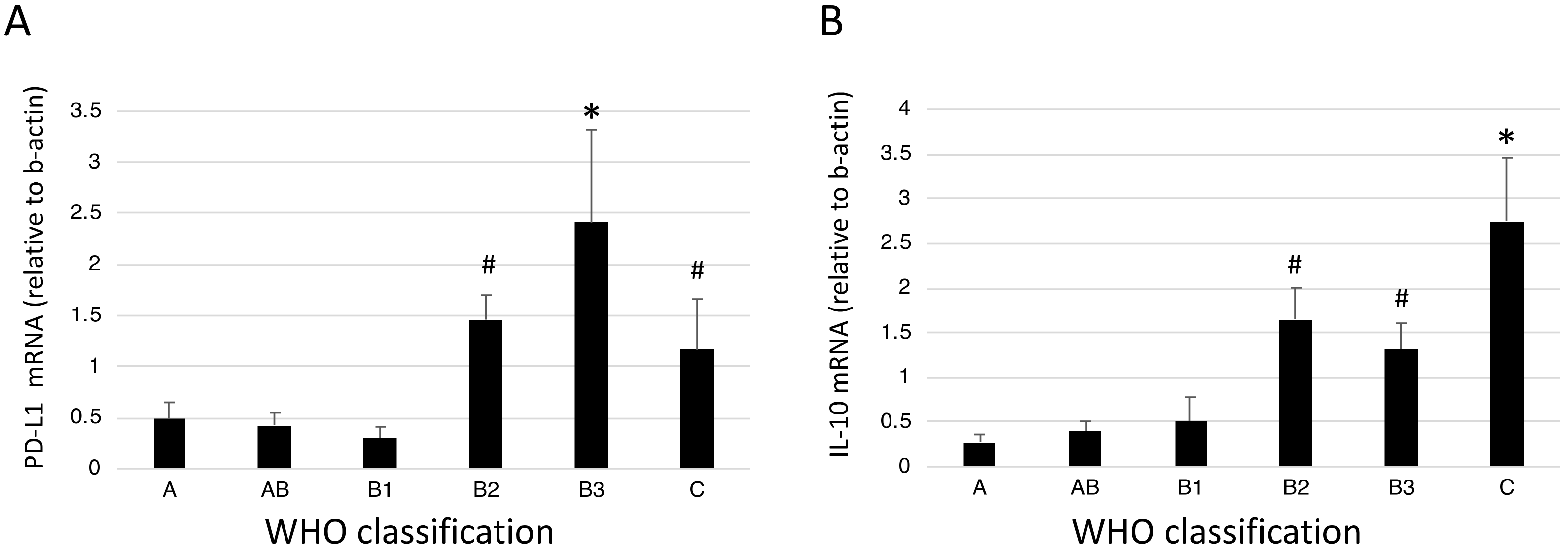
3.3. mRNA Expression of PD-L1 and IL-10 in Tumor Tissues
3.4. CD8 Expression in Lymphocytes
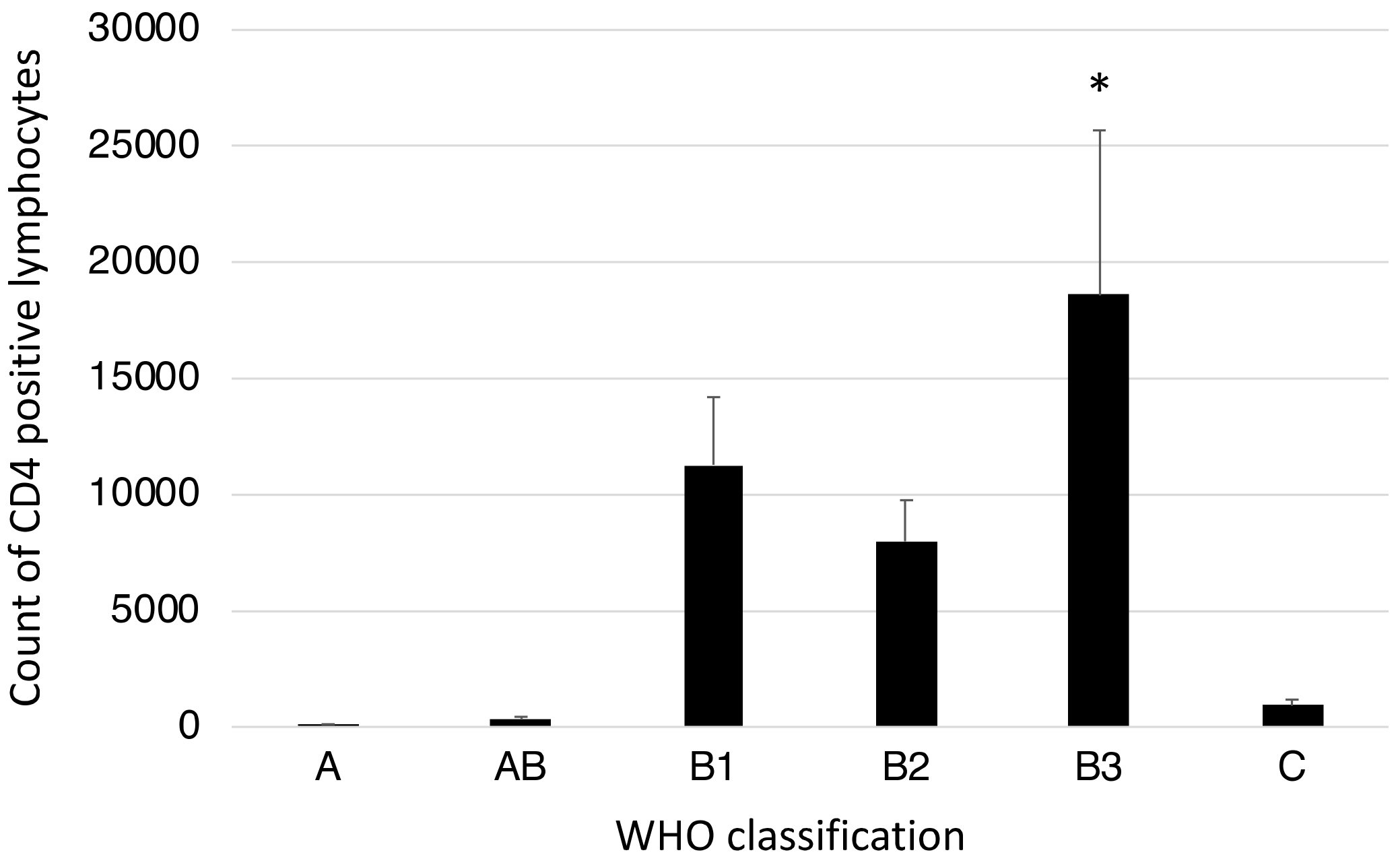
3.5. CD4-Positive Lymphocytes in Tumor Tissues
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Engels, E.A. Epidemiology of thymoma and associated malignancies. J. Thorac. Oncol. 2010, 5, S260–S265. [Google Scholar] [CrossRef]
- Venuta, F.; Anile, M.; Diso, D.; Vitolo, D.; Rendina, E.A.; De Giacomo, T.; Francioni, F.; Coloni, G.F. Thymoma and thymic carcinoma. Eur. J. Cardiothorac. Surg. 2010, 37, 13–25. [Google Scholar] [CrossRef] [Green Version]
- Kondo, K.; Yoshizawa, K.; Tsuyuguchi, M.; Kimura, S.; Sumitomo, M.; Morita, J.; Miyoshi, T.; Sakiyama, S.; Mukai, K.; Monden, Y. Who histologic classification is a prognostic indicator in thymoma. Ann. Thorac. Surg. 2004, 77, 1183–1188. [Google Scholar] [CrossRef] [PubMed]
- Marx, A.; Chan, J.K.; Coindre, J.M.; Detterbeck, F.; Girard, N.; Harris, N.L.; Jaffe, E.S.; Kurrer, M.O.; Marom, E.M.; Moreira, A.L.; et al. The 2015 world health organization classification of tumors of the thymus: Continuity and changes. J. Thorac. Oncol. 2015, 10, 1383–1395. [Google Scholar] [CrossRef] [PubMed]
- Marx, A.; Strobel, P.; Badve, S.S.; Chalabreysse, L.; Chan, J.K.; Chen, G.; de Leval, L.; Detterbeck, F.; Girard, N.; Huang, J.; et al. Itmig consensus statement on the use of the who histological classification of thymoma and thymic carcinoma: Refined definitions, histological criteria, and reporting. J. Thorac. Oncol. 2014, 9, 596–611. [Google Scholar] [CrossRef] [PubMed]
- Moon, J.W.; Lee, K.S.; Shin, M.H.; Kim, S.; Woo, S.Y.; Lee, G.; Han, J.; Shim, Y.M.; Choi, Y.S. Thymic epithelial tumors: Prognostic determinants among clinical, histopathologic, and computed tomography findings. Ann. Thorac. Surg. 2015, 99, 462–470. [Google Scholar] [CrossRef] [PubMed]
- Detterbeck, F.C.; Parsons, A.M. Management of stage i and ii thymoma. Thorac. Surg. Clin. 2011, 21, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Litvak, A.M.; Woo, K.; Hayes, S.; Huang, J.; Rimner, A.; Sima, C.S.; Moreira, A.L.; Tsukazan, M.; Riely, G.J. Clinical characteristics and outcomes for patients with thymic carcinoma: Evaluation of masaoka staging. J. Thorac. Oncol. 2014, 9, 1810–1815. [Google Scholar] [CrossRef]
- Zhao, Y.; Shi, J.; Fan, L.; Hu, D.; Yang, J.; Zhao, H. Surgical treatment of thymoma: An 11-year experience with 761 patients. Eur. J. Cardiothorac. Surg. 2016, 49, 1144–1149. [Google Scholar] [CrossRef]
- Girard, N.; Lal, R.; Wakelee, H.; Riely, G.J.; Loehrer, P.J. Chemotherapy definitions and policies for thymic malignancies. J. Thorac. Oncol. 2011, 6, S1749–S1755. [Google Scholar] [CrossRef]
- Schmitt, J.; Loehrer, P.J., Sr. The role of chemotherapy in advanced thymoma. J. Thorac. Oncol. 2010, 5, S357–S360. [Google Scholar] [CrossRef] [PubMed]
- Liang, S.C.; Latchman, Y.E.; Buhlmann, J.E.; Tomczak, M.F.; Horwitz, B.H.; Freeman, G.J.; Sharpe, A.H. Regulation of pd-1, pd-l1, and pd-l2 expression during normal and autoimmune responses. Eur. J. Immunol. 2003, 33, 2706–2716. [Google Scholar] [CrossRef] [PubMed]
- Dong, H.; Zhu, G.; Tamada, K.; Chen, L. B7-h1, a third member of the b7 family, co-stimulates t-cell proliferation and interleukin-10 secretion. Nat. Med. 1999, 5, 1365–1369. [Google Scholar] [CrossRef] [PubMed]
- Pardoll, D.M. The blockade of immune checkpoints in cancer immunotherapy. Nat. Rev. Cancer 2012, 12, 252–264. [Google Scholar] [CrossRef] [Green Version]
- Philips, G.K.; Atkins, M. Therapeutic uses of anti-pd-1 and anti-pd-l1 antibodies. Int. Immunol. 2015, 27, 39–46. [Google Scholar] [CrossRef]
- Wang, X.; Teng, F.; Kong, L.; Yu, J. Pd-l1 expression in human cancers and its association with clinical outcomes. OncoTargets Ther. 2016, 9, 5023–5039. [Google Scholar]
- Ferris, R.L.; Blumenschein, G., Jr.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.; Kasper, S.; Vokes, E.E.; Even, C.; et al. Nivolumab for recurrent squamous-cell carcinoma of the head and neck. N. Engl. J. Med. 2016, 375, 1856–1867. [Google Scholar] [CrossRef]
- Motzer, R.J.; Escudier, B.; McDermott, D.F.; George, S.; Hammers, H.J.; Srinivas, S.; Tykodi, S.S.; Sosman, J.A.; Procopio, G.; Plimack, E.R.; et al. Nivolumab versus everolimus in advanced renal-cell carcinoma. N. Engl. J. Med. 2015, 373, 1803–1813. [Google Scholar] [CrossRef]
- Reck, M.; Rodriguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csoszi, T.; Fulop, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus chemotherapy for pd-l1-positive non-small-cell lung cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef]
- Gunturi, A.; McDermott, D.F. Potential of new therapies like anti-pd1 in kidney cancer. Curr. Treat. Options Oncol. 2014, 15, 137–146. [Google Scholar] [CrossRef]
- Brahmer, J.R.; Tykodi, S.S.; Chow, L.Q.; Hwu, W.J.; Topalian, S.L.; Hwu, P.; Drake, C.G.; Camacho, L.H.; Kauh, J.; Odunsi, K.; et al. Safety and activity of anti-pd-l1 antibody in patients with advanced cancer. N. Engl. J. Med. 2012, 366, 2455–2465. [Google Scholar] [CrossRef] [PubMed]
- Rotte, A.; D’Orazi, G.; Bhandaru, M. Nobel committee honors tumor immunologists. J. Exp. Clin. Cancer Res. 2018, 37, 262. [Google Scholar] [CrossRef] [PubMed]
- Topalian, S.L.; Sznol, M.; McDermott, D.F.; Kluger, H.M.; Carvajal, R.D.; Sharfman, W.H.; Brahmer, J.R.; Lawrence, D.P.; Atkins, M.B.; Powderly, J.D.; et al. Survival, durable tumor remission, and long-term safety in patients with advanced melanoma receiving nivolumab. J. Clin. Oncol. 2014, 32, 1020–1030. [Google Scholar] [CrossRef] [PubMed]
- Xu, F.; Jin, T.; Zhu, Y.; Dai, C. Immune checkpoint therapy in liver cancer. J. Exp. Clin. Cancer Res. 2018, 37, 110. [Google Scholar] [CrossRef] [PubMed]
- Giaccone, G.; Kim, C.; Thompson, J.; McGuire, C.; Kallakury, B.; Chahine, J.J.; Manning, M.; Mogg, R.; Blumenschein, W.M.; Tan, M.T.; et al. Pembrolizumab in patients with thymic carcinoma: A single-arm, single-centre, phase 2 study. Lancet Oncol. 2018, 19, 347–355. [Google Scholar] [CrossRef]
- Merveilleux du Vignaux, C.; Maury, J.M.; Girard, N. Novel agents in the treatment of thymic malignancies. Curr. Treat. Options Oncol. 2017, 18, 52. [Google Scholar] [CrossRef] [PubMed]
- Travis, W.D.; Brambilla, E.; Nicholson, A.G.; Yatabe, Y.; Austin, J.H.M.; Beasley, M.B.; Chirieac, L.R.; Dacic, S.; Duhig, E.; Flieder, D.B.; et al. The 2015 world health organization classification of lung tumors: Impact of genetic, clinical and radiologic advances since the 2004 classification. J. Thorac. Oncol. 2015, 10, 1243–1260. [Google Scholar] [CrossRef]
- Cermakova, P.; Melichar, B.; Tomsova, M.; Zoul, Z.; Kalabova, H.; Spacek, J.; Dolezel, M. Prognostic significance of cd3+ tumor-infiltrating lymphocytes in patients with endometrial carcinoma. Anticancer Res. 2014, 34, 5555–5561. [Google Scholar]
- Hu, X.; Li, Y.Q.; Li, Q.G.; Ma, Y.L.; Peng, J.J.; Cai, S.J. Itgae defines cd8+ tumor-infiltrating lymphocytes predicting a better prognostic survival in colorectal cancer. EBioMedicine 2018, 35, 178–188. [Google Scholar] [CrossRef]
- Yu, A.; Mansure, J.J.; Solanki, S.; Siemens, D.R.; Koti, M.; Dias, A.B.T.; Burnier, M.M.; Brimo, F.; Kassouf, W. Presence of lymphocytic infiltrate cytotoxic t lymphocyte cd3+, cd8+, and immunoscore as prognostic marker in patients after radical cystectomy. PLoS ONE 2018, 13, e0205746. [Google Scholar] [CrossRef]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef] [PubMed]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.J.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Dummer, R.; Smylie, M.; Rutkowski, P.; et al. Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N. Engl. J. Med. 2015, 373, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Arbour, K.C.; Naidoo, J.; Steele, K.E.; Ni, A.; Moreira, A.L.; Rekhtman, N.; Robbins, P.B.; Karakunnel, J.; Rimner, A.; Huang, J.; et al. Expression of pd-l1 and other immunotherapeutic targets in thymic epithelial tumors. PLoS ONE 2017, 12, e0182665. [Google Scholar] [CrossRef] [PubMed]
- Marchevsky, A.M.; Walts, A.E. Pd-l1, pd-1, cd4, and cd8 expression in neoplastic and nonneoplastic thymus. Hum. Pathol. 2017, 60, 16–23. [Google Scholar] [CrossRef]
- Yang, Y.; Ding, L.; Wang, P. Dramatic response to anti-pd-1 therapy in a patient of squamous cell carcinoma of thymus with multiple lung metastases. J. Thorac. Dis. 2016, 8, E535–E537. [Google Scholar] [CrossRef]
- Zander, T.; Aebi, S.; Rast, A.C.; Zander, A.; Winterhalder, R.; Brand, C.; Diebold, J.; Gautschi, O. Response to pembrolizumab in a patient with relapsing thymoma. J. Thorac. Oncol. 2016, 11, e147–e149. [Google Scholar] [CrossRef]
- Heery, C.R.; O’Sullivan-Coyne, G.; Madan, R.A.; Cordes, L.; Rajan, A.; Rauckhorst, M.; Lamping, E.; Oyelakin, I.; Marte, J.L.; Lepone, L.M.; et al. Avelumab for metastatic or locally advanced previously treated solid tumours (javelin solid tumor): A phase 1a, multicohort, dose-escalation trial. Lancet Oncol. 2017, 18, 587–598. [Google Scholar] [CrossRef]
- Yamamoto, N.; Nokihara, H.; Yamada, Y.; Shibata, T.; Tamura, Y.; Seki, Y.; Honda, K.; Tanabe, Y.; Wakui, H.; Tamura, T. Phase i study of nivolumab, an anti-pd-1 antibody, in patients with malignant solid tumors. Invest. New Drugs 2017, 35, 207–216. [Google Scholar] [CrossRef]
- Cho, J.; Kim, H.S.; Ku, B.M.; Choi, Y.L.; Cristescu, R.; Han, J.; Sun, J.M.; Lee, S.H.; Ahn, J.S.; Park, K.; et al. Pembrolizumab for patients with refractory or relapsed thymic epithelial tumor: An open-label phase ii trial. J. Clin. Oncol. 2019, 37, 2162–2170. [Google Scholar] [CrossRef]
- Brown, J.A.; Dorfman, D.M.; Ma, F.R.; Sullivan, E.L.; Munoz, O.; Wood, C.R.; Greenfield, E.A.; Freeman, G.J. Blockade of programmed death-1 ligands on dendritic cells enhances t cell activation and cytokine production. J. Immunol. 2003, 170, 1257–1266. [Google Scholar] [CrossRef]
- Chen, Y.; Zhang, Y.; Chai, X.; Gao, J.; Chen, G.; Zhang, W.; Zhang, Y. Correlation between the expression of pd-l1 and clinicopathological features in patients with thymic epithelial tumors. Biomed. Res. Int. 2018, 2018. [Google Scholar] [CrossRef] [PubMed]
- Enkner, F.; Pichlhofer, B.; Zaharie, A.T.; Krunic, M.; Holper, T.M.; Janik, S.; Moser, B.; Schlangen, K.; Neudert, B.; Walter, K.; et al. Molecular profiling of thymoma and thymic carcinoma: Genetic differences and potential novel therapeutic targets. Pathol. Oncol. Res. 2017, 23, 551–564. [Google Scholar] [CrossRef] [PubMed]
- Guleria, P.; Husain, N.; Shukla, S.; Kumar, S.; Parshad, R.; Jain, D. Pd-l1 immuno-expression assay in thymomas: Study of 84 cases and review of literature. Ann. Diagn. Pathol. 2018, 34, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Hakiri, S.; Fukui, T.; Mori, S.; Kawaguchi, K.; Nakamura, S.; Ozeki, N.; Kato, T.; Goto, M.; Yatabe, Y.; Yokoi, K. Clinicopathologic features of thymoma with the expression of programmed death ligand 1. Ann. Thorac. Surg. 2019, 107, 418–424. [Google Scholar] [CrossRef]
- Katsuya, Y.; Fujita, Y.; Horinouchi, H.; Ohe, Y.; Watanabe, S.; Tsuta, K. Immunohistochemical status of pd-l1 in thymoma and thymic carcinoma. Lung Cancer 2015, 88, 154–159. [Google Scholar] [CrossRef]
- Owen, D.; Chu, B.; Lehman, A.M.; Annamalai, L.; Yearley, J.H.; Shilo, K.; Otterson, G.A. Expression patterns, prognostic value, and intratumoral heterogeneity of pd-l1 and pd-1 in thymoma and thymic carcinoma. J. Thorac. Oncol. 2018, 13, 1204–1212. [Google Scholar] [CrossRef]
- Padda, S.K.; Riess, J.W.; Schwartz, E.J.; Tian, L.; Kohrt, H.E.; Neal, J.W.; West, R.B.; Wakelee, H.A. Diffuse high intensity pd-l1 staining in thymic epithelial tumors. J. Thorac. Oncol. 2015, 10, 500–508. [Google Scholar] [CrossRef]
- Tiseo, M.; Damato, A.; Longo, L.; Barbieri, F.; Bertolini, F.; Stefani, A.; Migaldi, M.; Gnetti, L.; Camisa, R.; Bordi, P.; et al. Analysis of a panel of druggable gene mutations and of alk and pd-l1 expression in a series of thymic epithelial tumors (tets). Lung Cancer 2017, 104, 24–30. [Google Scholar] [CrossRef]
- Weissferdt, A.; Fujimoto, J.; Kalhor, N.; Rodriguez, J.; Bassett, R.; Wistuba, I.I.; Moran, C.A. Expression of pd-1 and pd-l1 in thymic epithelial neoplasms. Mod. Pathol. 2017, 30, 826–833. [Google Scholar] [CrossRef]
- Yokoyama, S.; Miyoshi, H.; Nishi, T.; Hashiguchi, T.; Mitsuoka, M.; Takamori, S.; Akagi, Y.; Kakuma, T.; Ohshima, K. Clinicopathologic and prognostic implications of programmed death ligand 1 expression in thymoma. Ann. Thorac. Surg. 2016, 101, 1361–1369. [Google Scholar] [CrossRef]
- Petrini, I.; Meltzer, P.S.; Kim, I.K.; Lucchi, M.; Park, K.S.; Fontanini, G.; Gao, J.; Zucali, P.A.; Calabrese, F.; Favaretto, A.; et al. A specific missense mutation in gtf2i occurs at high frequency in thymic epithelial tumors. Nat. Genet. 2014, 46, 844–849. [Google Scholar] [CrossRef] [PubMed]
- Radovich, M.; Pickering, C.R.; Felau, I.; Ha, G.; Zhang, H.; Jo, H.; Hoadley, K.A.; Anur, P.; Zhang, J.; McLellan, M.; et al. The integrated genomic landscape of thymic epithelial tumors. Cancer Cell 2018, 33, 244–258. [Google Scholar] [CrossRef] [PubMed]
- Golstein, P.; Griffiths, G.M. An early history of t cell-mediated cytotoxicity. Nat. Rev. Immunol. 2018, 18, 527–535. [Google Scholar] [CrossRef] [PubMed]
- Khalil, D.N.; Smith, E.L.; Brentjens, R.J.; Wolchok, J.D. The future of cancer treatment: Immunomodulation, cars and combination immunotherapy. Nat. Rev. Clin. Oncol. 2016, 13, 273–290. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Green, M.; Choi, J.E.; Gijon, M.; Kennedy, P.D.; Johnson, J.K.; Liao, P.; Lang, X.; Kryczek, I.; Sell, A.; et al. Cd8(+) t cells regulate tumour ferroptosis during cancer immunotherapy. Nature 2019, 569, 270–274. [Google Scholar] [CrossRef] [PubMed]
- Zou, W.; Wolchok, J.D.; Chen, L. Pd-l1 (b7-h1) and pd-1 pathway blockade for cancer therapy: Mechanisms, response biomarkers, and combinations. Sci. Transl. Med. 2016, 8, 328rv. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pathology | Case No. | PD-L1 Expression | CD8/CD3 |
|---|---|---|---|
| A (n = 6) | 1 | (-) | 90% |
| 2 | 80% | 90% | |
| 3 | (-) | 90% | |
| 4 | (-) | 90% | |
| 5 | (-) | 90% | |
| 6 | 30% | 90% | |
| AB (n = 6) | 7 | (-) | 90% |
| 8 | (-) | 90% | |
| 9 | (-) | 90% | |
| 10 | A(-)/B:3% | 90% | |
| 11 | (-) | 90% | |
| 12 | A(-)/B:10% | 90% | |
| B1 (n = 9) | 13 | (-) | 70% |
| 14 | 70% | 90% | |
| 15 | (-) | 90% | |
| 16 | (-) | 50% | |
| 17 | 70% | 90% | |
| 18 | (-) | 90% | |
| 19 | 1% | 90% | |
| 20 | (-) | 95% | |
| 21 | (-) | 90% | |
| B2 (n = 4) | 22 | 70% | 90% |
| 23 | 70% | 90% | |
| 24 | 50% | 90% | |
| 25 | 70% | 90% | |
| B3 (n = 6) | 26 | (-) | 90% |
| 27 | 70% | 70% | |
| 28 | 80% | 40% | |
| 29 | 60% | 90% | |
| 30 | 90% | 5% | |
| 31 | 90% | 90% | |
| Ca (n = 8) | 32 | 40% | 40% |
| 33 | (-) | 90% | |
| 34 | 90% | 90% | |
| 35 | (-) | 90% | |
| 36 | (-) | 90% | |
| 37 | 30% | 90% | |
| 38 | 70% | 70% | |
| 39 | 5% | 90% |
| No. | Author/Year | No. of Thymoma/Thymic Ca Cases | Sex Ratio (M/F) | MG | Clone of PD-L1 (Dilution) | Criteria for Positivity: Cut-Off | Percent Positivity | Most Common Histologies with PD-L1 Positivity |
|---|---|---|---|---|---|---|---|---|
| 1 | Brown et al. [40]/2003 | 26/8 | NA | NA | 29E.2A3, 29E.5A9 | Not defined | Thymoma: 81%, Ca: 88% | Not defined |
| 2 | Padda et al. [47]/2015 | 65/4 | 1.1:1 | 16 | 5H1 murine mAb (1:100) 15 rabbit mAb (1:1000) | Intensity of staining (score 0–3): score 3 | Thymoma: 68%, Ca: 75% | B2, Ca |
| 3 | Katsuya et al. [45]/2015 | 102/37 | 0.6:1 | NA | E1L3N (1:800) | H-score (staining intensity (0–3) × % of positive cells (0%–100%)): score 3 | Thymoma: 23% Ca: 70% | Ca |
| 4 | Yokoyama et al. [50]/2016 | 82/0 | 0.6:1 | 18 | EPR1161 (1:200) | Youden’s index: > 38% | Thymoma: 53.7% Ca: Not available | B2 and B3 |
| 5 | Enkner et al. [42]/2017 | 37/35 | NA | NA | E1L3N | H-score (cut-off not defined) | Thymoma: 76% in B3, 13% in A Ca: 53% | B3, Ca |
| 6 | Tiseo et al. [48]/2017 | 87/20 | 1.2:1 | 26 | E1L3N (1:500) | H-score: Score 3 | Thymoma: 18% Ca: 65% | Ca |
| 7 | Marchevsky et al. [34]/2017 | 38/8 | NA | NA | SP142 (1:250) | Membranous expression ≥ 6% tumor cells | Thymoma: 92% Ca: 50% | B2, B3 |
| 8 | Weissferdt et al. [49]/2017 | 74/26 | 1.3:1 | 19 | EPR4877 (1:250) | Strong membranous staining: > 5% tumor cells | Thymoma: 64% Ca: 54% | B3 |
| 9 | Arbour et al. [33]/2017 | 12/11 | 1.3:1 | 2 | E1L3N | Membranous expression > 25% tumor cells | Thymoma: 92% Ca: 36% | B2, B3 |
| 10 | Owen et al. [46]/2018 | 32/3 | 1.1:1 | NA | 22C3 | Intensity of staining (score 0–5): Score 1 | Thymoma: 81% Ca: 100% | Not associated |
| 11 | Chen et al. [41]/2018 | 50/20 | 0.8:1 | 1 | SP142 | Membranous expression ≥ 5% tumor cells | Thymoma: 48% Ca: 70% | B3, Ca |
| 12 | Guleria et al. [43]/2018 | 84/0 | 1.5:1 | 28 | SP263 | Membranous expression > 25% tumor cells | Thymoma: 82% | B1, B2, B3 |
| 13 | Hakiri et al. [44]/2019 | 81/0 | 1:1 | 17 | SP142 (1:50) | Membranous expression ≥ 1% tumor cells | Thymoma: 27% | B2, B3 |
| 14 | Present study | 31/8 | 1.2:1 | 1 | 28–8 | Membranous expression ≥ 1% tumor cells | Thymoma: 51.6% Ca: 62.5% | B2, B3 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Higuchi, R.; Goto, T.; Hirotsu, Y.; Nakagomi, T.; Yokoyama, Y.; Otake, S.; Amemiya, K.; Oyama, T.; Omata, M. PD-L1 Expression and Tumor-Infiltrating Lymphocytes in Thymic Epithelial Neoplasms. J. Clin. Med. 2019, 8, 1833. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8111833
Higuchi R, Goto T, Hirotsu Y, Nakagomi T, Yokoyama Y, Otake S, Amemiya K, Oyama T, Omata M. PD-L1 Expression and Tumor-Infiltrating Lymphocytes in Thymic Epithelial Neoplasms. Journal of Clinical Medicine. 2019; 8(11):1833. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8111833
Chicago/Turabian StyleHiguchi, Rumi, Taichiro Goto, Yosuke Hirotsu, Takahiro Nakagomi, Yujiro Yokoyama, Sotaro Otake, Kenji Amemiya, Toshio Oyama, and Masao Omata. 2019. "PD-L1 Expression and Tumor-Infiltrating Lymphocytes in Thymic Epithelial Neoplasms" Journal of Clinical Medicine 8, no. 11: 1833. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8111833