Quadriceps Neuromuscular Impairments after Arthroscopic Knee Surgery: Comparison between Procedures

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Surgical Procedures and Rehabilitation
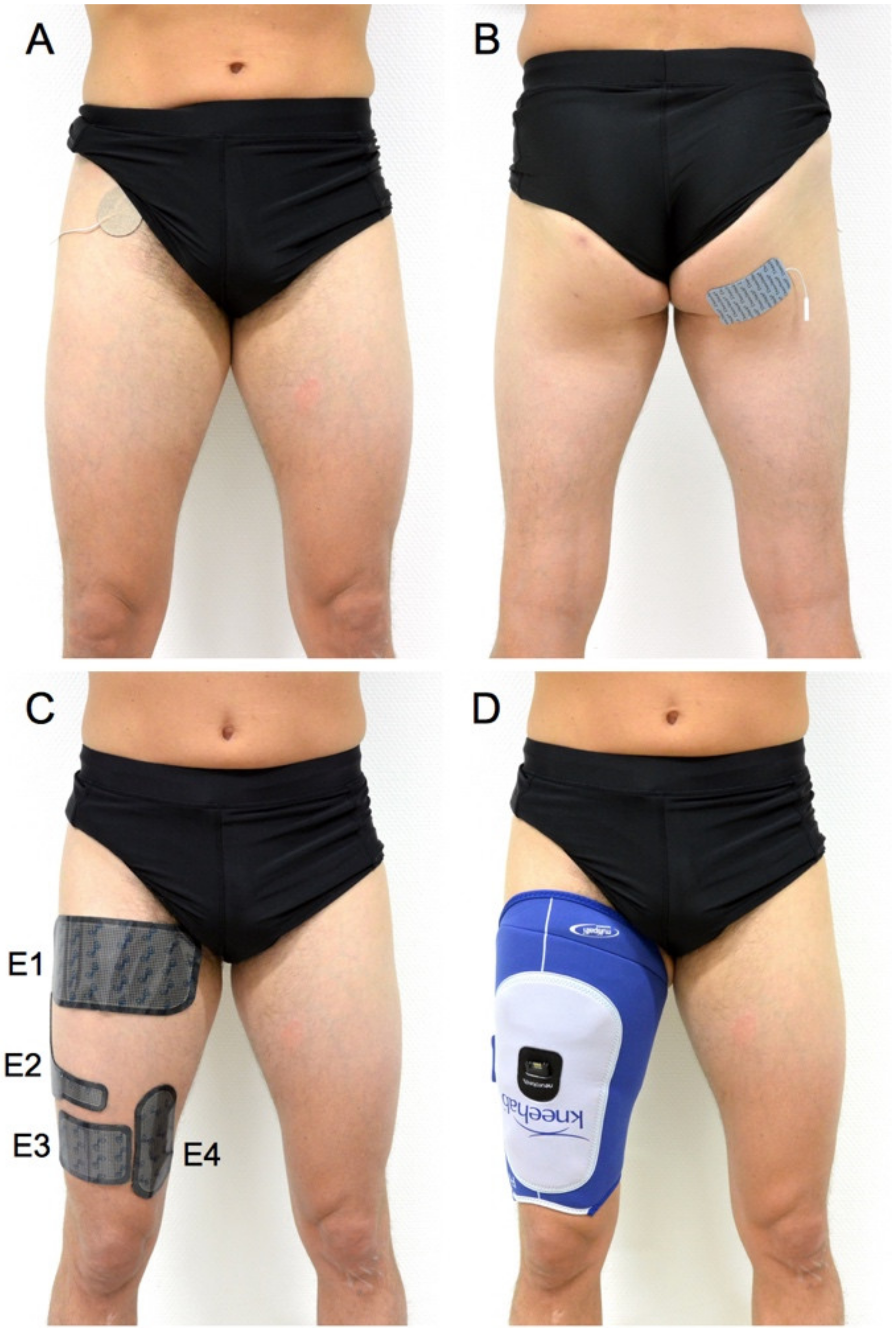
2.3. Experimental Procedure
2.4. Self-Reported Questionnaires
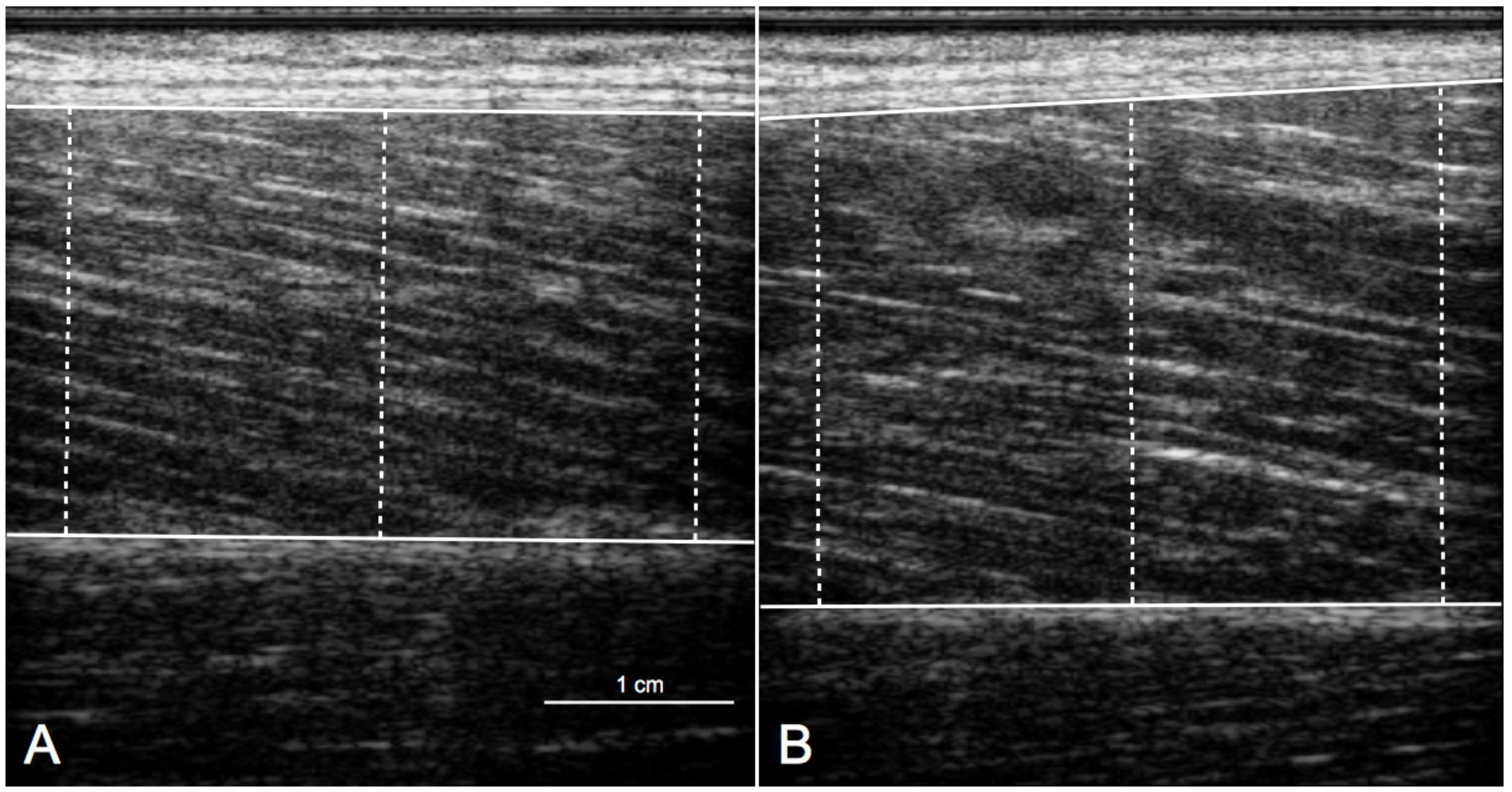
2.5. Neuromuscular Parameters
2.6. Statistics
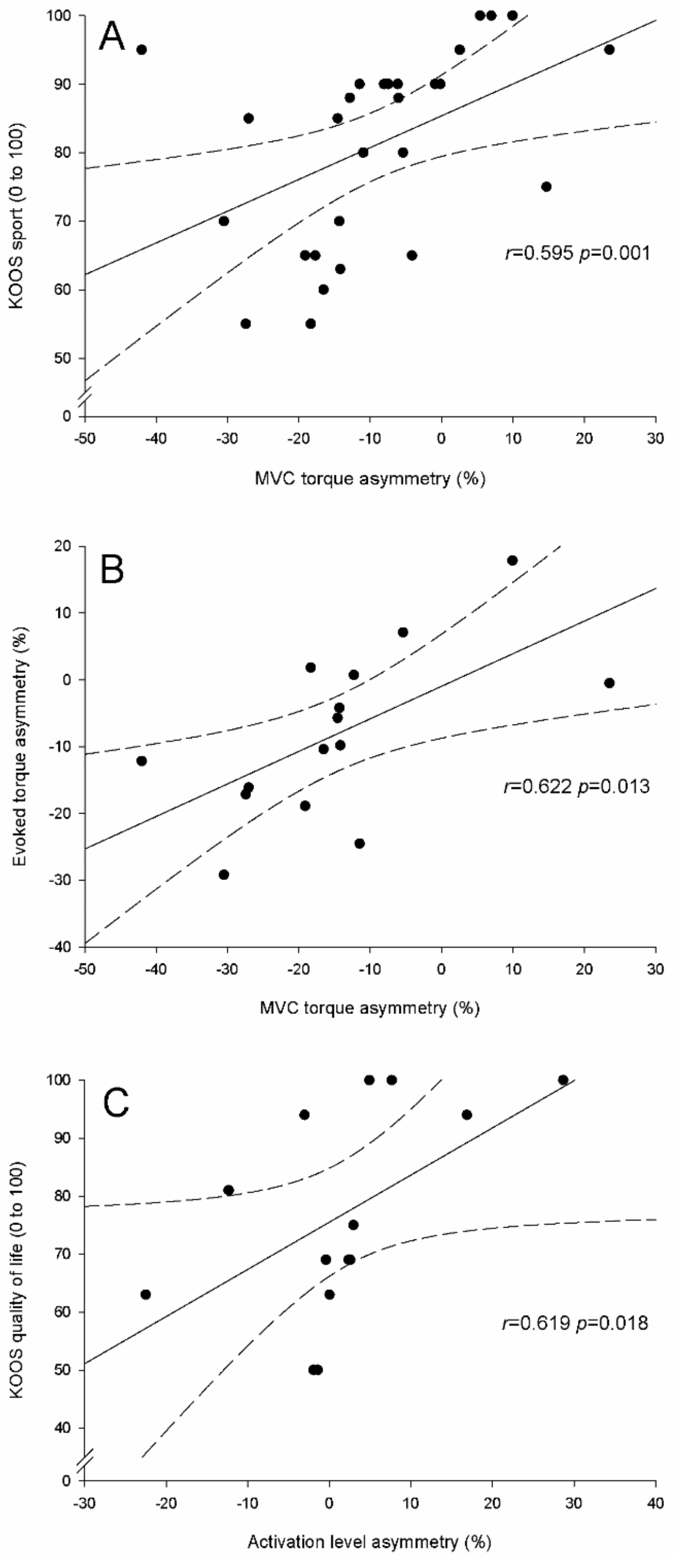
3. Results
4. Discussion
4.1. Strengths and Limitations
4.2. Quadriceps Muscle Weakness in ACL and Meniscus Patients
4.3. Neuromuscular Impairments in ACL Patients
4.4. Neuromuscular Impairments in Meniscus Patients
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Lohmander, L.S.; Englund, P.M.; Dahl, L.L.; Roos, E.M. The long-term consequence of anterior cruciate ligament and meniscus injuries: Osteoarthritis. Am. J. Sports Med. 2007, 35, 1756–1769. [Google Scholar] [CrossRef]
- Arangio, G.A.; Chen, C.; Kalady, M.; Reed, J.F., 3rd. Thigh muscle size and strength after anterior cruciate ligament reconstruction and rehabilitation. J. Orthop. Sports Phys. 1997, 26, 238–243. [Google Scholar] [CrossRef]
- Keays, S.L.; Bullock-Saxton, J.; Keays, A.C.; Newcombe, P. Muscle strength and function before and after anterior cruciate ligament reconstruction using semitendonosus and gracilis. Knee 2001, 8, 229–234. [Google Scholar] [CrossRef]
- Ericsson, Y.B.; Roos, E.M.; Dahlberg, L. Muscle strength, functional performance, and self-reported outcomes four years after arthroscopic partial meniscectomy in middle-aged patients. Arthritis Rheum. 2006, 55, 946–952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glatthorn, J.F.; Berendts, A.M.; Bizzini, M.; Munzinger, U.; Maffiuletti, N.A. Neuromuscular function after arthroscopic partial meniscectomy. Clin. Orthop. Relat. Res. 2010, 468, 1336–1343. [Google Scholar] [CrossRef] [PubMed]
- Pietrosimone, B.; Blackburn, J.T.; Harkey, M.S.; Luc, B.A.; Pamukoff, D.N.; Hart, J.M. Clinical strategies for addressing muscle weakness following knee injury. Clin. Sports Med. 2015, 34, 285–300. [Google Scholar] [CrossRef] [PubMed]
- Brandt, K.D. Is a strong quadriceps muscle bad for a patient with knee osteoarthritis? Ann. Intern. Med. 2003, 138, 678–679. [Google Scholar] [CrossRef] [PubMed]
- Maffiuletti, N.A. Assessment of hip and knee muscle function in orthopaedic practice and research. J. Bone Joint Surg. Am. 2010, 92, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Cobian, D.G.; Koch, C.M.; Amendola, A.; Williams, G.N. Knee extensor rate of torque development before and after arthroscopic partial meniscectomy, with analysis of neuromuscular mechanisms. J. Orthop. Sports Phys. 2017, 47, 945–956. [Google Scholar] [CrossRef] [PubMed]
- Rice, D.A.; McNair, P.J. Quadriceps arthrogenic muscle inhibition: Neural mechanisms and treatment perspectives. Semin. Arthritis Rheum. 2010, 40, 250–266. [Google Scholar] [CrossRef]
- Thomas, A.C.; Wojtys, E.M.; Brandon, C.; Palmieri-Smith, R.M. Muscle atrophy contributes to quadriceps weakness after anterior cruciate ligament reconstruction. J. Sci. Med. Sport 2016, 19, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Lepley, A.S.; Grooms, D.R.; Burland, J.P.; Davi, S.M.; Kinsella-Shaw, J.M.; Lepley, L.K. Quadriceps muscle function following anterior cruciate ligament reconstruction: Systemic differences in neural and morphological characteristics. Exp. Brain Res. 2019, 237, 1267–1278. [Google Scholar] [CrossRef] [PubMed]
- Place, N.; Maffiuletti, N.A.; Martin, A.; Lepers, R. Assessment of the reliability of central and peripheral fatigue after sustained maximal voluntary contraction of the quadriceps muscle. Muscle Nerve 2007, 35, 486–495. [Google Scholar] [CrossRef] [PubMed]
- Roos, E.M.; Lohmander, L.S. The Knee injury and Osteoarthritis Outcome Score (KOOS): From joint injury to osteoarthritis. Health Qual. Life Outcomes 2003, 1, 64. [Google Scholar] [CrossRef] [PubMed]
- Aagaard, P.; Andersen, J.L.; Dyhre-Poulsen, P.; Leffers, A.M.; Wagner, A.; Magnusson, S.P.; Halkjaer-Kristensen, J.; Simonsen, E.B. A mechanism for increased contractile strength of human pennate muscle in response to strength training: Changes in muscle architecture. J. Physiol. 2001, 534, 613–623. [Google Scholar] [CrossRef] [PubMed]
- Fukunaga, T.; Ichinose, Y.; Ito, M.; Kawakami, Y.; Fukashiro, S. Determination of fascicle length and pennation in a contracting human muscle in vivo. J. Appl. Physiol. (1985) 1997, 82, 354–358. [Google Scholar] [CrossRef]
- Wellauer, V.; Morf, C.; Minetto, M.A.; Place, N.; Maffiuletti, N.A. Assessment of quadriceps muscle inactivation with a new electrical stimulation paradigm. Muscle Nerve 2015, 51, 117–124. [Google Scholar] [CrossRef]
- Rodriguez-Falces, J.; Maffiuletti, N.A.; Place, N. Twitch and M-wave potentiation induced by intermittent maximal voluntary quadriceps contractions: Differences between direct quadriceps and femoral nerve stimulation. Muscle Nerve 2013, 48, 920–929. [Google Scholar] [CrossRef]
- Allen, G.M.; McKenzie, D.K.; Gandevia, S.C. Twitch interpolation of the elbow flexor muscles at high forces. Muscle Nerve 1998, 21, 318–328. [Google Scholar] [CrossRef]
- Akima, H.; Hioki, M.; Furukawa, T. Effect of arthroscopic partial meniscectomy on the function of quadriceps femoris. Knee Surg. Sports Traumatol. Arthrosc. 2008, 16, 1017–1025. [Google Scholar] [CrossRef]
- Urbach, D.; Awiszus, F. Impaired ability of voluntary quadriceps activation bilaterally interferes with function testing after knee injuries. A twitch interpolation study. Int. J. Sports Med. 2002, 23, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Roos, E.M.; Roos, H.P.; Ryd, L.; Lohmander, L.S. Substantial disability 3 months after arthroscopic partial meniscectomy: A prospective study of patient-relevant outcomes. Arthroscopy 2000, 16, 619–626. [Google Scholar] [CrossRef] [PubMed]
- Behrens, M.; Brown, N.; Bollinger, R.; Bubeck, D.; Mau-Moeller, A.; Weippert, M.; Zschorlich, V.; Bruhn, S.; Alt, W. Relationship between muscle volume and contractile properties of the human knee extensors. Appl. Physiol. Nutr. Metab. 2016, 41, 110–113. [Google Scholar] [CrossRef] [PubMed]
- Fry, C.S.; Johnson, D.L.; Ireland, M.L.; Noehren, B. ACL injury reduces satellite cell abundance and promotes fibrogenic cell expansion within skeletal muscle. J. Orthop. Res. 2016, 35, 1876–1885. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Mean ± SD / Number | Mean Difference / Relative Risk (95% CI) | p Value | |||
|---|---|---|---|---|---|
| All brk (n = 30) | M brk (n = 15) | ACL + M brk (n = 15) | |||
| Gender (women / men) | 4 / 26 | 1 / 14 | 3 / 12 | 1.62 (0.81 to 3.28) | 0.598 |
| Age (years) | 32 ± 9 | 35 ± 10 | 29 ± 7 | 6 (−1 to 13) | 0.077 |
| Body mass (kg) | 74 ± 10 | 76 ± 7 | 73 ± 11 | 3 (−4 to 10) | 0.386 |
| Height (cm) | 176 ± 8 | 178 ± 7 | 174 ± 9 | 4 (−2 to 10) | 0.190 |
| BMI (kg/m2) | 24 ± 2 | 24 ± 2 | 24 ± 2 | 0 (−1 to 1) | 0.909 |
| Number | Relative Risk (95% CI) | p Value | |||
|---|---|---|---|---|---|
| All brk (n = 30) | M brk (n = 15) | ACL + M brk (n = 15) | |||
| Partial meniscectomy | 17 | 9 | 8 | 0.87 (0.42 to 1.82) | 0.713 |
| Meniscal repair | 7 | 3 | 4 | 1.22 (0.47 to 3.12) | 1.000 |
| Partial meniscectomy and repair | 3 | 2 | 1 | 0.72 (0.30 to 1.76) | 1.000 |
| Meniscal debridement | 3 | 1 | 2 | 1.56 (0.30 to 8.03) | 1.000 |
| Operated Knee | Non-Operated Knee | p Value | Side-to-Side Asymmetry (%) | p Value | ||
|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean Difference (95%CI) | ||||
| MVC torque (Nm/kg) | ||||||
| All (n = 30) | 3.16 ± 0.61 | 3.54 ± 0.66 | <0.001 | −10 ± 14 | ||
| M (n = 15) | 3.47 ± 0.49 | 3.68 ± 0.64 | 0.052 | −5 ±10 | 10 (0 to 20) | 0.049 |
| ACL + M (n = 15) | 2.85 ± 0.57 | 3.40 ± 0.68 | 0.001 | −15 ± 16 | ||
| Vastus lateralis thickness (cm) | ||||||
| All (n = 30) | 2.53 ± 0.34 | 2.62 ± 0.33 | 0.032 | −3 ± 8 | ||
| M (n = 15) | 2.60 ± 0.25 | 2.60 ± 0.27 | 0.953 | 0 ± 7 | 6 (1 to 12) | 0.021 |
| ACL + M (n = 15) | 2.47 ± 0.41 | 2.64 ± 0.40 | 0.009 | −6 ± 8 | ||
| Activation level (%) | ||||||
| All (n = 30) | 91 ± 8 | 92 ± 8 | 0.654 | 0 ± 9 | ||
| M (n = 15) | 91 ± 9 | 91 ± 9 | 0.754 | 2 ± 11 | 4 (-3 to 10) | 0.292 |
| ACL + M (n = 15) | 91 ± 8 | 93 ± 7 | 0.203 | −2 ± 6 | ||
| Evoked torque (Nm/kg) | ||||||
| All (n = 30) | 1.10 ± 0.27 | 1.16 ± 0.28 | 0.013 | −5 ± 12 | ||
| M (n = 15) | 1.23 ± 0.20 | 1.27 ± 0.22 | 0.329 | −2 ± 11 | 6 (-3 to 15) | 0.188 |
| ACL + M (n = 15) | 0.97 ± 0.26 | 1.06 ± 0.30 | 0.014 | −8 ± 12 | ||
| Median (25th to 75th Percentile) | p Value | |||
|---|---|---|---|---|
| All brk (n = 28) | M brk (n = 14) | ACL + M brk (n = 14) | ||
| KOOS pain (0 to 100) | 92 (83 to 96) | 94 (85 to 100) | 89 (78 to 92) | 0.020 |
| KOOS symptoms (0 to 100) | 89 (79 to 95) | 91 (86 to 97) | 83 (68 to 90) | 0.014 |
| KOOS ADL (0 to 100) | 99 (96 to 100) | 100 (96 to 100) | 99 (95 to 100) | 0.645 |
| KOOS sport (0 to 100) | 87 (66 to 90) | 90 (79 to 91) | 75 (62 to 91) | 0.087 |
| KOOS quality of life (0 to 100) | 69 (52 to 81) | 72 (63 to 96) | 63 (49 to 75) | 0.042 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casartelli, N.C.; Item-Glatthorn, J.F.; Friesenbichler, B.; Bizzini, M.; Salzmann, G.M.; Maffiuletti, N.A. Quadriceps Neuromuscular Impairments after Arthroscopic Knee Surgery: Comparison between Procedures. J. Clin. Med. 2019, 8, 1881. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8111881
Casartelli NC, Item-Glatthorn JF, Friesenbichler B, Bizzini M, Salzmann GM, Maffiuletti NA. Quadriceps Neuromuscular Impairments after Arthroscopic Knee Surgery: Comparison between Procedures. Journal of Clinical Medicine. 2019; 8(11):1881. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8111881
Chicago/Turabian StyleCasartelli, Nicola C., Julia F. Item-Glatthorn, Bernd Friesenbichler, Mario Bizzini, Gian M. Salzmann, and Nicola A. Maffiuletti. 2019. "Quadriceps Neuromuscular Impairments after Arthroscopic Knee Surgery: Comparison between Procedures" Journal of Clinical Medicine 8, no. 11: 1881. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8111881