The Effects of Hyperuricemia on the Prognosis of IgA Nephropathy are More Potent in Females

 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
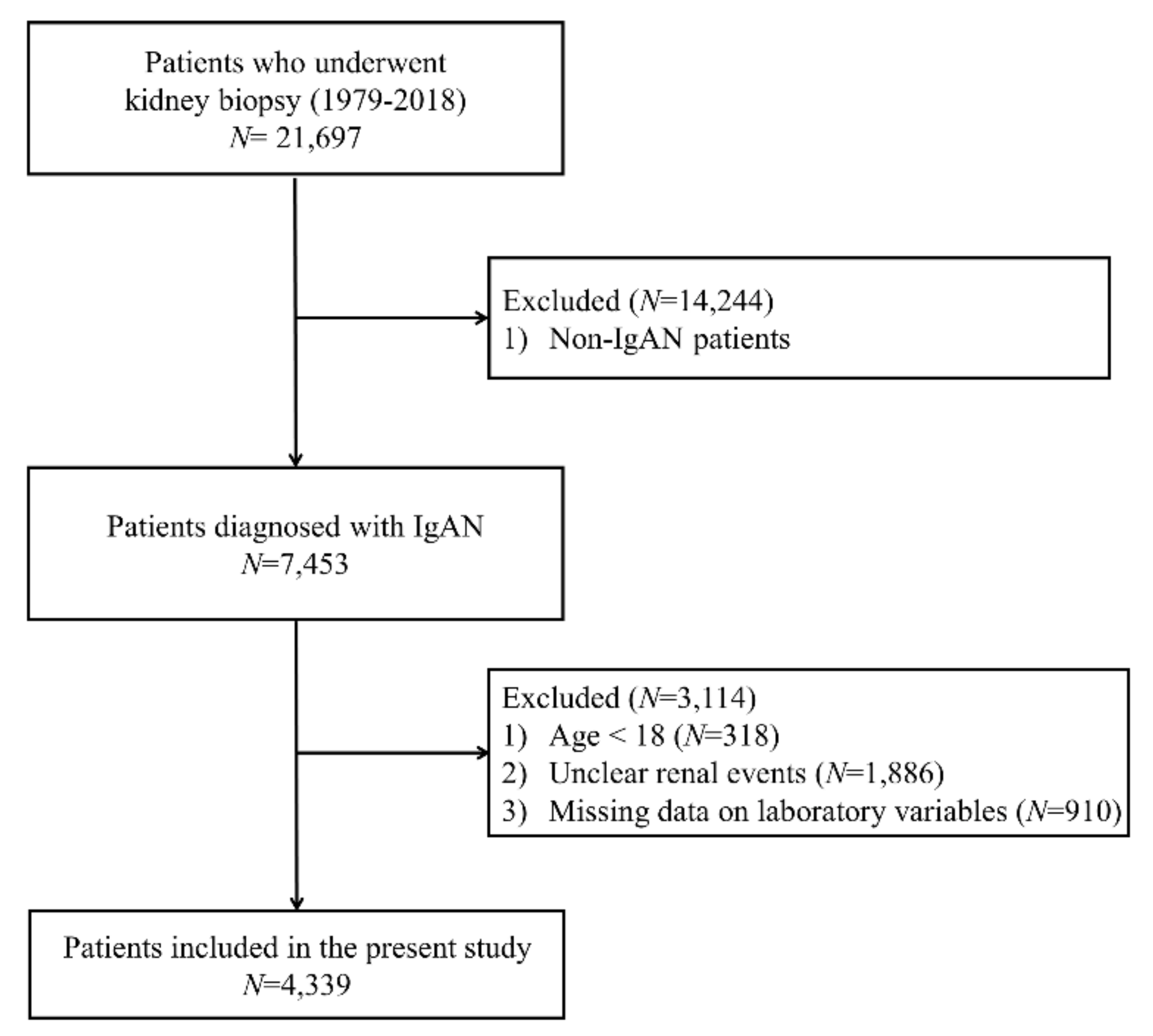
2.1. Data Source and Study Population
2.2. Study End Point, Definitions, and Measurements
2.3. Statistical Analyses
2.4. Ethics Approval and Consent to Participate
3. Results
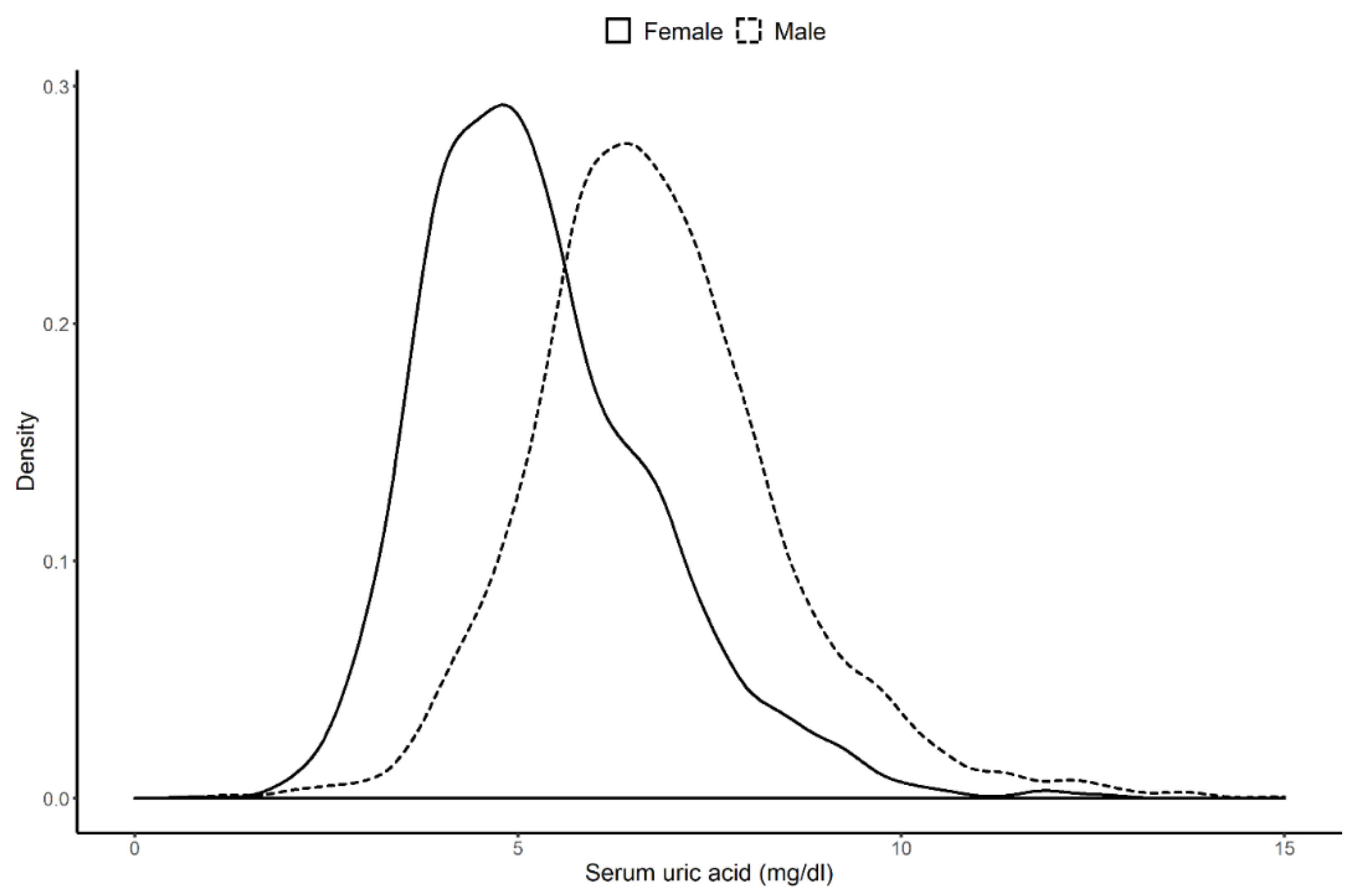
3.1. Clinical Characteristics of the Study Population
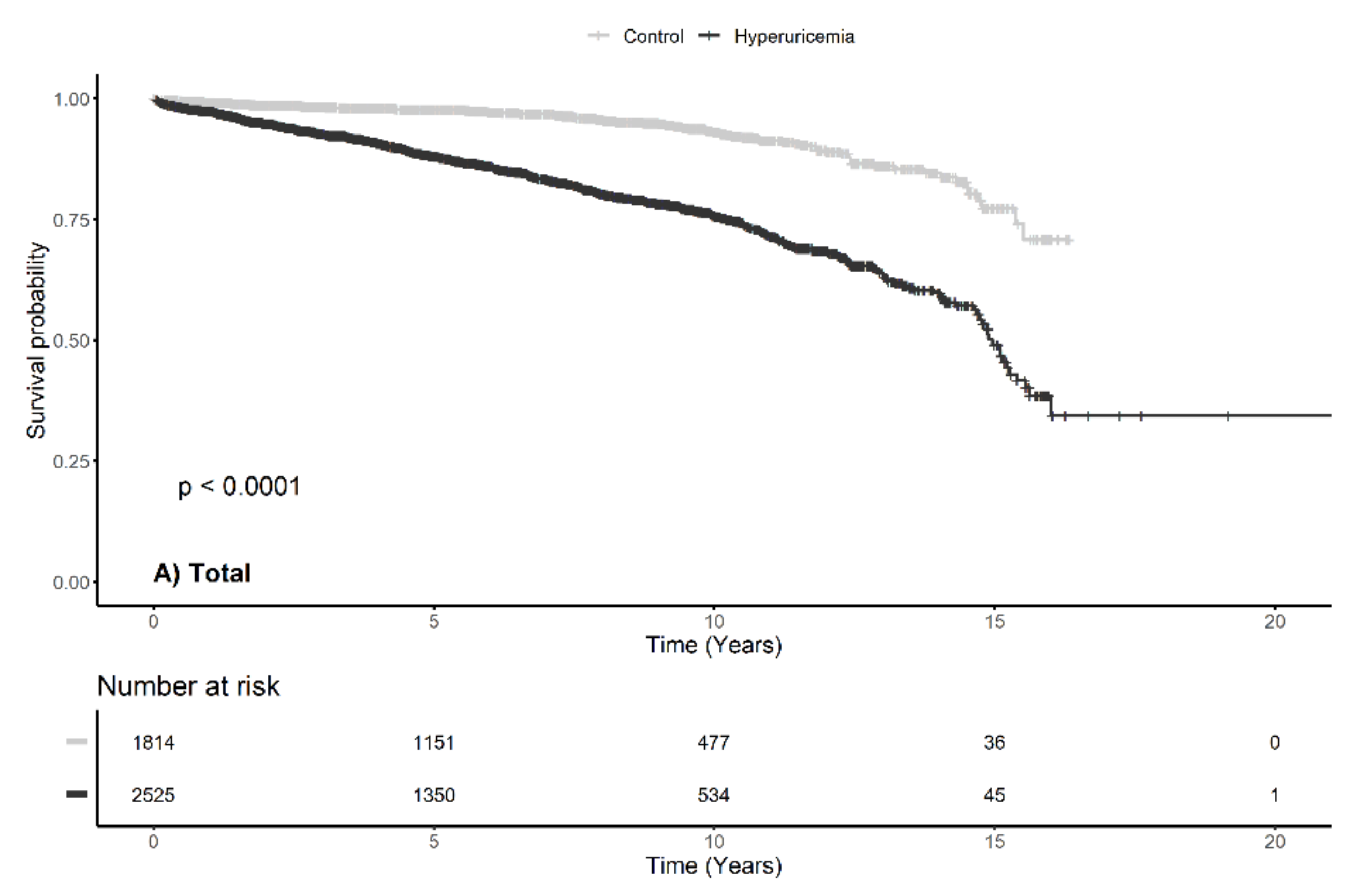
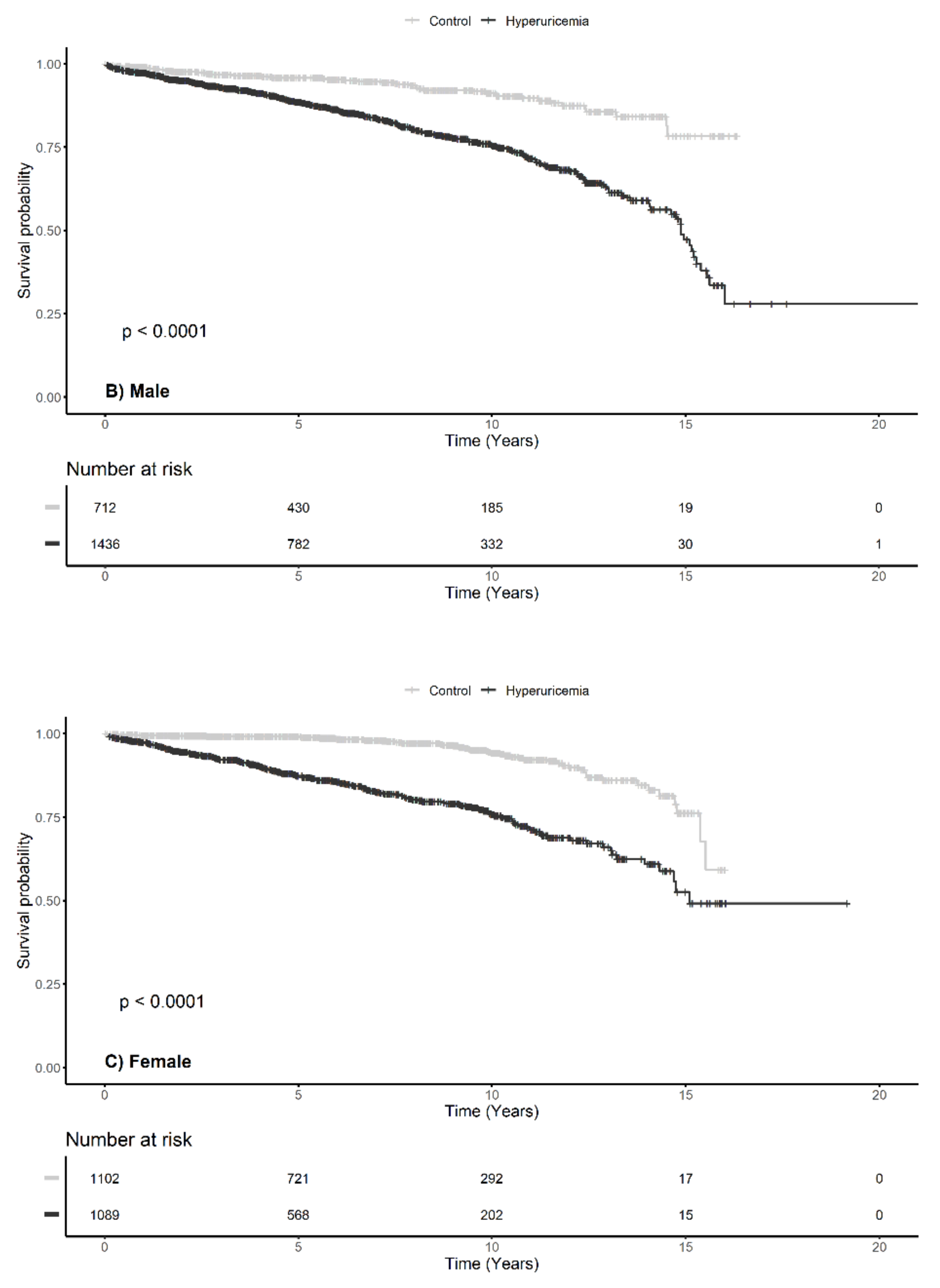
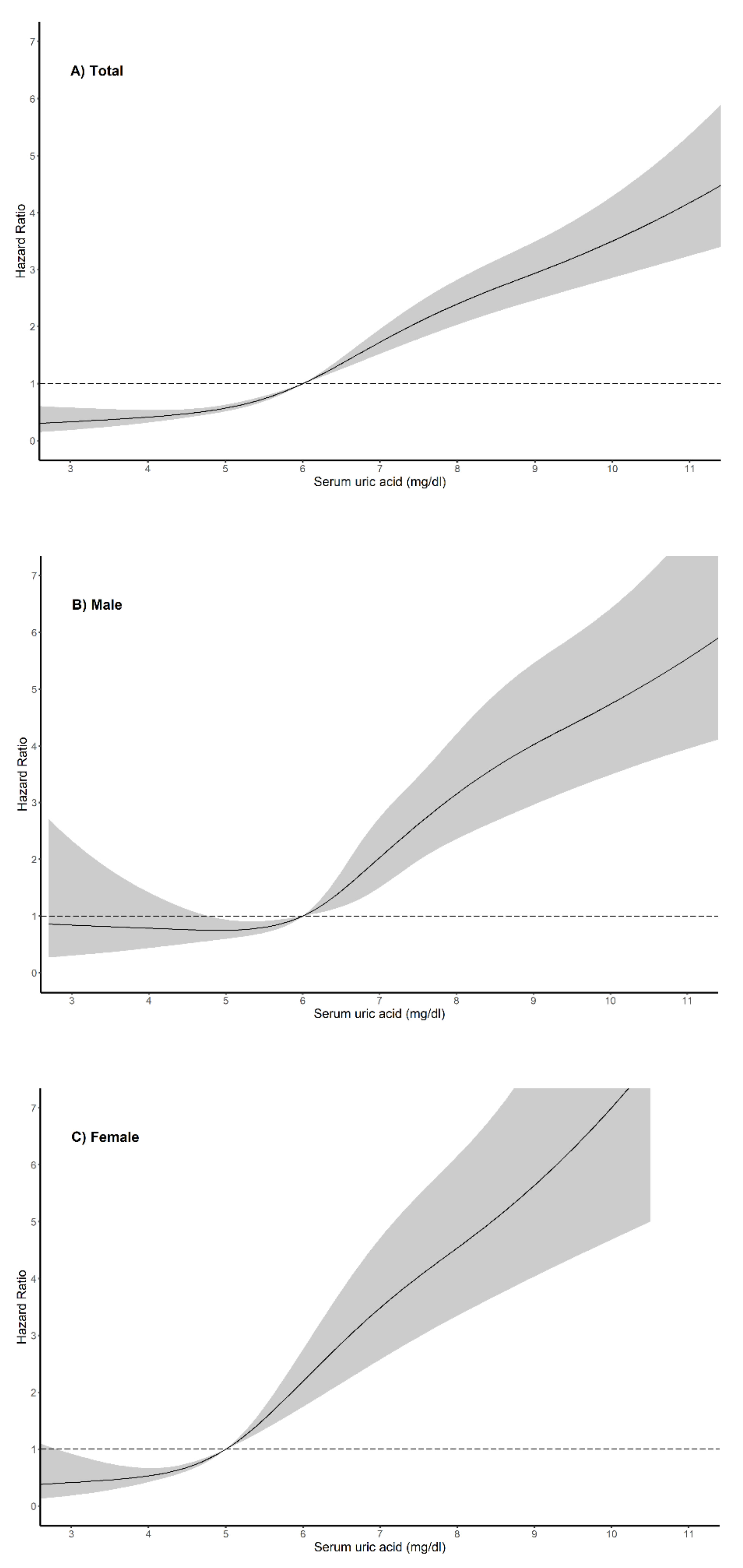
3.2. Crude Analysis of the Association Between the Serum Uric Acid Levels and the Progression of Immunoglobulin A Nephropathy
3.3. Independent Risk Factors Associated with the Progression of Immunoglobulin A Nephropathy
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Jin, D.C.; Han, J.S. Renal replacement therapy in Korea, 2012. Kidney Res. Clin. Pract. 2014, 33, 9–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunsicker, L.G. The consequences and costs of chronic kidney disease before ESRD. J. Am. Soc. Nephrol. JASN 2004, 15, 1363–1364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, J.H.; Kim, D.K.; Kim, H.W.; Park, S.Y.; Yoo, T.H.; Kim, B.S.; Kang, S.W.; Choi, K.H.; Han, D.S.; Jeong, H.J.; et al. Changing prevalence of glomerular diseases in Korean adults: A review of 20 years of experience. Nephrol. Dial. Transplant. 2009, 24, 2406–2410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moriyama, T.; Tanaka, K.; Iwasaki, C.; Oshima, Y.; Ochi, A.; Kataoka, H.; Itabashi, M.; Takei, T.; Uchida, K.; Nitta, K. Prognosis in IgA nephropathy: 30-year analysis of 1,012 patients at a single center in Japan. PLoS ONE 2014, 9, e91756. [Google Scholar] [CrossRef]
- Wakai, K.; Kawamura, T.; Endoh, M.; Kojima, M.; Tomino, Y.; Tamakoshi, A.; Ohno, Y.; Inaba, Y.; Sakai, H. A scoring system to predict renal outcome in IgA nephropathy: From a nationwide prospective study. Nephrol. Dial. Transplant. 2006, 21, 2800–2808. [Google Scholar] [CrossRef]
- Yamamoto, R.; Nagasawa, Y.; Shoji, T.; Iwatani, H.; Hamano, T.; Kawada, N.; Inoue, K.; Uehata, T.; Kaneko, T.; Okada, N.; et al. Cigarette smoking and progression of IgA nephropathy. Am. J. Kidney Dis. 2010, 56, 313–324. [Google Scholar] [CrossRef]
- Syrjanen, J.; Mustonen, J.; Pasternack, A. Hypertriglyceridaemia and hyperuricaemia are risk factors for progression of IgA nephropathy. Nephrol. Dial. Transplant. 2000, 15, 34–42. [Google Scholar] [CrossRef]
- Kiryluk, K.; Novak, J.; Gharavi, A.G. Pathogenesis of immunoglobulin A nephropathy: Recent insight from genetic studies. Annu. Rev. Med. 2013, 64, 339–356. [Google Scholar] [CrossRef] [Green Version]
- Kiryluk, K.; Li, Y.; Sanna-Cherchi, S.; Rohanizadegan, M.; Suzuki, H.; Eitner, F.; Snyder, H.J.; Choi, M.; Hou, P.; Scolari, F.; et al. Geographic differences in genetic susceptibility to IgA nephropathy: GWAS replication study and geospatial risk analysis. PLoS Genet. 2012, 8, e1002765. [Google Scholar] [CrossRef]
- Li, M.; Hou, W.; Zhang, X.; Hu, L.; Tang, Z. Hyperuricemia and risk of stroke: A systematic review and meta-analysis of prospective studies. Atherosclerosis 2014, 232, 265–270. [Google Scholar] [CrossRef]
- Gustafsson, D.; Unwin, R. The pathophysiology of hyperuricaemia and its possible relationship to cardiovascular disease, morbidity and mortality. BMC Nephrol. 2013, 14, 164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazzali, M.; Hughes, J.; Kim, Y.G.; Jefferson, J.A.; Kang, D.H.; Gordon, K.L.; Lan, H.Y.; Kivlighn, S.; Johnson, R.J. Elevated uric acid increases blood pressure in the rat by a novel crystal-independent mechanism. Hypertension 2001, 38, 1101–1106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feig, D.I.; Kang, D.H.; Johnson, R.J. Uric acid and cardiovascular risk. N. Engl. J. Med. 2008, 359, 1811–1821. [Google Scholar] [CrossRef] [PubMed]
- Oh, T.R.; Choi, H.S.; Kim, C.S.; Bae, E.H.; Ma, S.K.; Sung, S.A.; Kim, Y.S.; Oh, K.H.; Ahn, C.; Kim, S.W. Hyperuricemia has increased the risk of progression of chronic kidney disease: Propensity score matching analysis from the KNOW-CKD study. Sci. Rep. 2019, 9, 6681. [Google Scholar] [CrossRef] [PubMed]
- Bakan, A.; Oral, A.; Elcioglu, O.C.; Takir, M.; Kostek, O.; Ozkok, A.; Basci, S.; Sumnu, A.; Ozturk, S.; Sipahioglu, M.; et al. Hyperuricemia is associated with progression of IgA nephropathy. Int. Urol. Nephrol. 2015, 47, 673–678. [Google Scholar] [CrossRef] [PubMed]
- Fan, S.; Zhang, P.; Wang, A.Y.; Wang, X.; Wang, L.; Li, G.; Hong, D. Hyperuricemia and its related histopathological features on renal biopsy. BMC Nephrol. 2019, 20, 95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsukuma, Y.; Masutani, K.; Tanaka, S.; Tsuchimoto, A.; Fujisaki, K.; Torisu, K.; Katafuchi, R.; Hirakata, H.; Tsuruya, K.; Kitazono, T. A J-shaped association between serum uric acid levels and poor renal survival in female patients with IgA nephropathy. Hypertens. Res. 2017, 40, 291–297. [Google Scholar] [CrossRef]
- Nagasawa, Y.; Yamamoto, R.; Shoji, T.; Shinzawa, M.; Hasuike, Y.; Nagatoya, K.; Yamauchi, A.; Hayashi, T.; Kuragano, T.; Moriyama, T.; et al. Serum Uric Acid Level Predicts Progression of IgA Nephropathy in Females but Not in Males. PLoS ONE 2016, 11, e0160828. [Google Scholar] [CrossRef]
- Nutritional Anaemias: Report of a WHO Scientific Group; Technical Report Series, No. 405; World Health Organization: Geneva, Sitzerland, 1968; pp. 5–37.
- Levey, A.S.; Bosch, J.P.; Lewis, J.B.; Greene, T.; Rogers, N.; Roth, D. A more accurate method to estimate glomerular filtration rate from serum creatinine: A new prediction equation. Modification of Diet in Renal Disease Study Group. Ann. Int. Med. 1999, 130, 461–470. [Google Scholar] [CrossRef]
- A Language and Environment for Statistical Computing. 2018. Available online: http://www.R-project.org/ (accessed on 6 January 2020).
- Becker, B.F. Towards the physiological function of uric acid. Free Radic. Boil. Med. 1993, 14, 615–631. [Google Scholar] [CrossRef]
- Ames, B.N.; Cathcart, R.; Schwiers, E.; Hochstein, P. Uric acid provides an antioxidant defense in humans against oxidant- and radical-caused aging and cancer: A hypothesis. Proc. Natl. Acad. Sci. USA 1981, 78, 6858–6862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Justicia, C.; Salas-Perdomo, A.; Perez-de-Puig, I.; Deddens, L.H.; van Tilborg, G.A.F.; Castellvi, C.; Dijkhuizen, R.M.; Chamorro, A.; Planas, A.M. Uric Acid Is Protective After Cerebral Ischemia/Reperfusion in Hyperglycemic Mice. Transl. Stroke Res. 2017, 8, 294–305. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Evans, J.E.; Rock, K.L. Molecular identification of a danger signal that alerts the immune system to dying cells. Nature 2003, 425, 516–521. [Google Scholar] [CrossRef] [PubMed]
- Roncal, C.A.; Mu, W.; Croker, B.; Reungjui, S.; Ouyang, X.; Tabah-Fisch, I.; Johnson, R.J.; Ejaz, A.A. Effect of elevated serum uric acid on cisplatin-induced acute renal failure. Am. J. Physiol. Ren. Physiol. 2007, 292, F116–F122. [Google Scholar] [CrossRef] [PubMed]
- Cannon, P.J.; Stason, W.B.; Demartini, F.E.; Sommers, S.C.; Laragh, J.H. Hyperuricemia in primary and renal hypertension. N. Engl. J. Med. 1966, 275, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.H.; Park, S.K.; Lee, I.K.; Johnson, R.J. Uric acid-induced C-reactive protein expression: Implication on cell proliferation and nitric oxide production of human vascular cells. J. Am. Soc. Nephrol. JASN 2005, 16, 3553–3562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romi, M.M.; Arfian, N.; Tranggono, U.; Setyaningsih, W.A.W.; Sari, D.C.R. Uric acid causes kidney injury through inducing fibroblast expansion, Endothelin-1 expression, and inflammation. BMC Nephrol. 2017, 18, 326. [Google Scholar] [CrossRef] [Green Version]
- Messerli, F.H.; Frohlich, E.D.; Dreslinski, G.R.; Suarez, D.H.; Aristimuno, G.G. Serum uric acid in essential hypertension: An indicator of renal vascular involvement. Ann. Int. Med. 1980, 93, 817–821. [Google Scholar] [CrossRef]
- Ohno, I.; Hosoya, T.; Gomi, H.; Ichida, K.; Okabe, H.; Hikita, M. Serum uric acid and renal prognosis in patients with IgA nephropathy. Nephron 2001, 87, 333–339. [Google Scholar] [CrossRef]
- Shi, Y.; Chen, W.; Jalal, D.; Li, Z.; Chen, W.; Mao, H.; Yang, Q.; Johnson, R.J.; Yu, X. Clinical outcome of hyperuricemia in IgA nephropathy: A retrospective cohort study and randomized controlled trial. Kidney Blood Press. Res. 2012, 35, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Ben-Dov, I.Z.; Kark, J.D. Serum uric acid is a GFR-independent long-term predictor of acute and chronic renal insufficiency: The Jerusalem Lipid Research Clinic cohort study. Nephrol. Dial. Transplant. 2011, 26, 2558–2566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbieri, L.; Verdoia, M.; Schaffer, A.; Marino, P.; Suryapranata, H.; De Luca, G. Impact of sex on uric acid levels and its relationship with the extent of coronary artery disease: A single-centre study. Atherosclerosis 2015, 241, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Zhang, H.; Tian, W.; Shi, L.; Chen, L.; Li, J.; Zhao, S.; Qi, G. Association between serum uric acid levels and coronary artery disease in different age and gender: A cross-sectional study. Aging Clin. Exp. Res. 2019, 31, 1783–1790. [Google Scholar] [CrossRef] [PubMed]
- Akasaka, H.; Yoshida, H.; Takizawa, H.; Hanawa, N.; Tobisawa, T.; Tanaka, M.; Moniwa, N.; Togashi, N.; Yamashita, T.; Kuroda, S.; et al. The impact of elevation of serum uric acid level on the natural history of glomerular filtration rate (GFR) and its sex difference. Nephrol. Dial. Transplant. 2014, 29, 1932–1939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshitomi, R.; Fukui, A.; Nakayama, M.; Ura, Y.; Ikeda, H.; Oniki, H.; Tsuchihashi, T.; Tsuruya, K.; Kitazono, T. Sex differences in the association between serum uric acid levels and cardiac hypertrophy in patients with chronic kidney disease. Hypertens. Res. 2014, 37, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Takiue, Y.; Hosoyamada, M.; Kimura, M.; Saito, H. The effect of female hormones upon urate transport systems in the mouse kidney. Nucleosides Nucleotides Nucleic Acids 2011, 30, 113–119. [Google Scholar] [CrossRef]
- Hak, A.E.; Choi, H.K. Menopause, postmenopausal hormone use and serum uric acid levels in US women--the Third National Health and Nutrition Examination Survey. Arthritis Res. Ther. 2008, 10, R116. [Google Scholar] [CrossRef] [Green Version]
- Sciacqua, A.; Perticone, M.; Tassone, E.J.; Cimellaro, A.; Miceli, S.; Maio, R.; Sesti, G.; Perticone, F. Uric acid is an independent predictor of cardiovascular events in post-menopausal women. Int. J. Cardiol. 2015, 197, 271–275. [Google Scholar] [CrossRef]
- Prasad, M.; Matteson, E.L.; Herrmann, J.; Gulati, R.; Rihal, C.S.; Lerman, L.O.; Lerman, A. Uric Acid Is Associated with Inflammation, Coronary Microvascular Dysfunction, and Adverse Outcomes in Postmenopausal Women. Hypertension 2017, 69, 236–242. [Google Scholar] [CrossRef] [Green Version]
- Kohagura, K.; Kochi, M.; Miyagi, T.; Kinjyo, T.; Maehara, Y.; Nagahama, K.; Sakima, A.; Iseki, K.; Ohya, Y. An association between uric acid levels and renal arteriolopathy in chronic kidney disease: A biopsy-based study. Hypertens. Res. 2013, 36, 43–49. [Google Scholar] [CrossRef]
- Doring, A.; Gieger, C.; Mehta, D.; Gohlke, H.; Prokisch, H.; Coassin, S.; Fischer, G.; Henke, K.; Klopp, N.; Kronenberg, F.; et al. SLC2A9 influences uric acid concentrations with pronounced sex-specific effects. Nat. Genet. 2008, 40, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Dehghan, A.; Kottgen, A.; Yang, Q.; Hwang, S.J.; Kao, W.L.; Rivadeneira, F.; Boerwinkle, E.; Levy, D.; Hofman, A.; Astor, B.C.; et al. Association of three genetic loci with uric acid concentration and risk of gout: A genome-wide association study. Lancet 2008, 372, 1953–1961. [Google Scholar] [CrossRef] [Green Version]
- Vitart, V.; Rudan, I.; Hayward, C.; Gray, N.K.; Floyd, J.; Palmer, C.N.; Knott, S.A.; Kolcic, I.; Polasek, O.; Graessler, J.; et al. SLC2A9 is a newly identified urate transporter influencing serum urate concentration, urate excretion and gout. Nat. Genet. 2008, 40, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Sanna, S.; Maschio, A.; Busonero, F.; Usala, G.; Mulas, A.; Lai, S.; Dei, M.; Orru, M.; Albai, G.; et al. The GLUT9 gene is associated with serum uric acid levels in Sardinia and Chianti cohorts. PLoS Genet. 2007, 3, e194. [Google Scholar] [CrossRef] [PubMed]
- Caulfield, M.J.; Munroe, P.B.; O’Neill, D.; Witkowska, K.; Charchar, F.J.; Doblado, M.; Evans, S.; Eyheramendy, S.; Onipinla, A.; Howard, P.; et al. SLC2A9 is a high-capacity urate transporter in humans. PLoS Med. 2008, 5, e197. [Google Scholar] [CrossRef] [PubMed]
- Greene, T. Randomized and observational studies in nephrology: How strong is the evidence? Am. J. Kidney Dis. 2009, 53, 377–388. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Missing Data (n (%)) | All Subjects (n = 4339) | Control (n = 1814) | Hyperuricemia (n = 2525) | p-Value |
|---|---|---|---|---|---|
| Age (year) | 0 (0) | 39.3 ± 14.1 | 37.9 ± 13.4 | 40.4 ± 14.5 | <0.001 |
| Male (%) | 0 (0) | 2148 (49.5) | 712 (39.3%) | 1436 (56.9) | <0.001 |
| Height (cm) | 341 (7.9) | 164.9 [158.0; 172.0] | 163.0 [157.4; 170.0] | 166.0 [158.9; 173.0] | <0.001 |
| Weight (kg) | 193 (4.4) | 63.6 [55.8; 72.5] | 60.0 [53.6; 68.5] | 66.1 [58.0; 75.0] | <0.001 |
| Body mass index | 355 (8.2) | 23.4 [21.1; 26.0] | 22.6 [20.7; 24.8] | 24.0 [21.7; 26.6] | <0.001 |
| Diabetes mellitus (%) | 6 (0.1) | 329 (7.6) | 110 (6.1) | 219 (8.7) | 0.002 |
| Systolic blood pressure (mmHg) | 240 (5.5) | 123.9 ± 16.5 | 120.4 ± 14.7 | 126.5 ± 17.2 | <0.001 |
| Diastolic blood pressure (mmHg) | 241 (5.6) | 77.4 ± 11.5 | 75.4 ± 10.8 | 78.9 ± 11.8 | <0.001 |
| Serum uric acid (mg/dl) | 0 (0) | 6.0 ± 1.8 | 4.5 ± 0.9 | 7.1 ± 1.4 | <0.001 |
| Hemoglobin (g/dl) | 12 (0.3) | 13.0 ± 1.9 | 12.9 ± 1.7 | 13.0 ± 2.0 | 0.301 |
| Serum albumin (mg/dl) | 18 (0.4) | 3.9 [3.6; 4.2] | 4.0 [3.7; 4.3] | 3.9 [3.5; 4.2] | <0.001 |
| Creatinine (mg/dl) | 6 (0.1) | 1.00 [0.80; 1.30] | 0.84 [0.70; 1.00] | 1.10 [0.90; 1.50] | <0.001 |
| eGFR (ml/min/1.73 m2) | 6 (0.1) | 75.1 [54.4; 95.8] | 86.4 [70.4; 104.5] | 64.4 [44.4; 86.1] | <0.001 |
| Total cholesterol (mg/dl) | 242 (5.6) | 184.0 [157.0; 215.0] | 178.0 [155.0; 206.0] | 189.0 [160.0; 220.0] | <0.001 |
| Urine protein creatinine ratio (g/g Creatinine) | 790 (18.2) | 1.0 [0.5; 2.1] | 0.8 [0.4; 1.6] | 1.2 [0.6; 2.4] | <0.001 |
| Follow-up duration (year) | 0 (0) | 6.1 [2.7; 9.8] | 6.9 [3.2; 10.1] | 5.5 [2.5; 9.4] | <0.001 |
| Total Subjects | Male | Female | ||||
|---|---|---|---|---|---|---|
| HR [95% CI] | p-Value | HR [95% CI] | p-Value | HR [95% CI] | p-Value | |
| Crude | 1.376 [1.329; 1.425] | <0.001 | 1.346 [1.283; 1.413] | <0.001 | 1.514 [1.427; 1.606] | <0.001 |
| Model 1 | 1.398 [1.343; 1.447] | <0.001 | 1.338 [1.274; 1.404] | <0.001 | 1.507 [1.419; 1.600] | <0.001 |
| Model 2 | 1.288 [1.227; 1.352] | <0.001 | 1.211 [1.134; 1.293] | <0.001 | 1.415 [1.316; 1.522] | <0.001 |
| Model 3 | 1.260 [1.191; 1.332] | <0.001 | 1.188 [1.104; 1.279] | <0.001 | 1.381 [1.259; 1.513] | <0.001 |
| Constraints | Total Subjects | Male | Female | |||
|---|---|---|---|---|---|---|
| HR [95% CI] | p-Value | HR [95% CI] | p-Value | HR [95% CI] | p-Value | |
| Exclude first 1-year follow-up period † | ||||||
| Serum uric acid | 1.298 [1.225; 1.377] | <0.001 | 1.235 [1.143; 1.333] | <0.001 | 1.405 [1.274; 1.550] | <0.001 |
| Include urine protein creatinine ratio ‡ | ||||||
| Serum uric acid | 1.228 [1.155; 1.306] | <0.001 | 1.151 [1.065; 1.245] | <0.001 | 1.380 [1.240; 1.533] | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, T.R.; Choi, H.S.; Kim, C.S.; Kang, K.P.; Kwon, Y.J.; Kim, S.G.; Ma, S.K.; Kim, S.W.; Bae, E.H. The Effects of Hyperuricemia on the Prognosis of IgA Nephropathy are More Potent in Females. J. Clin. Med. 2020, 9, 176. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9010176
Oh TR, Choi HS, Kim CS, Kang KP, Kwon YJ, Kim SG, Ma SK, Kim SW, Bae EH. The Effects of Hyperuricemia on the Prognosis of IgA Nephropathy are More Potent in Females. Journal of Clinical Medicine. 2020; 9(1):176. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9010176
Chicago/Turabian StyleOh, Tae Ryom, Hong Sang Choi, Chang Seong Kim, Kyung Pyo Kang, Young Joo Kwon, Sung Gyun Kim, Seong Kwon Ma, Soo Wan Kim, and Eun Hui Bae. 2020. "The Effects of Hyperuricemia on the Prognosis of IgA Nephropathy are More Potent in Females" Journal of Clinical Medicine 9, no. 1: 176. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9010176