Psoriasis and Psoriatic Arthritis Cardiovascular Disease Endotypes Identified by Red Blood Cell Distribution Width and Mean Platelet Volume

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Experimental Section
2.1. Study Design
2.2. Explorys
2.3. University Hospitals Cleveland Medical Center Data
2.4. Statistical Analysis
3. Results
3.1. Demographics
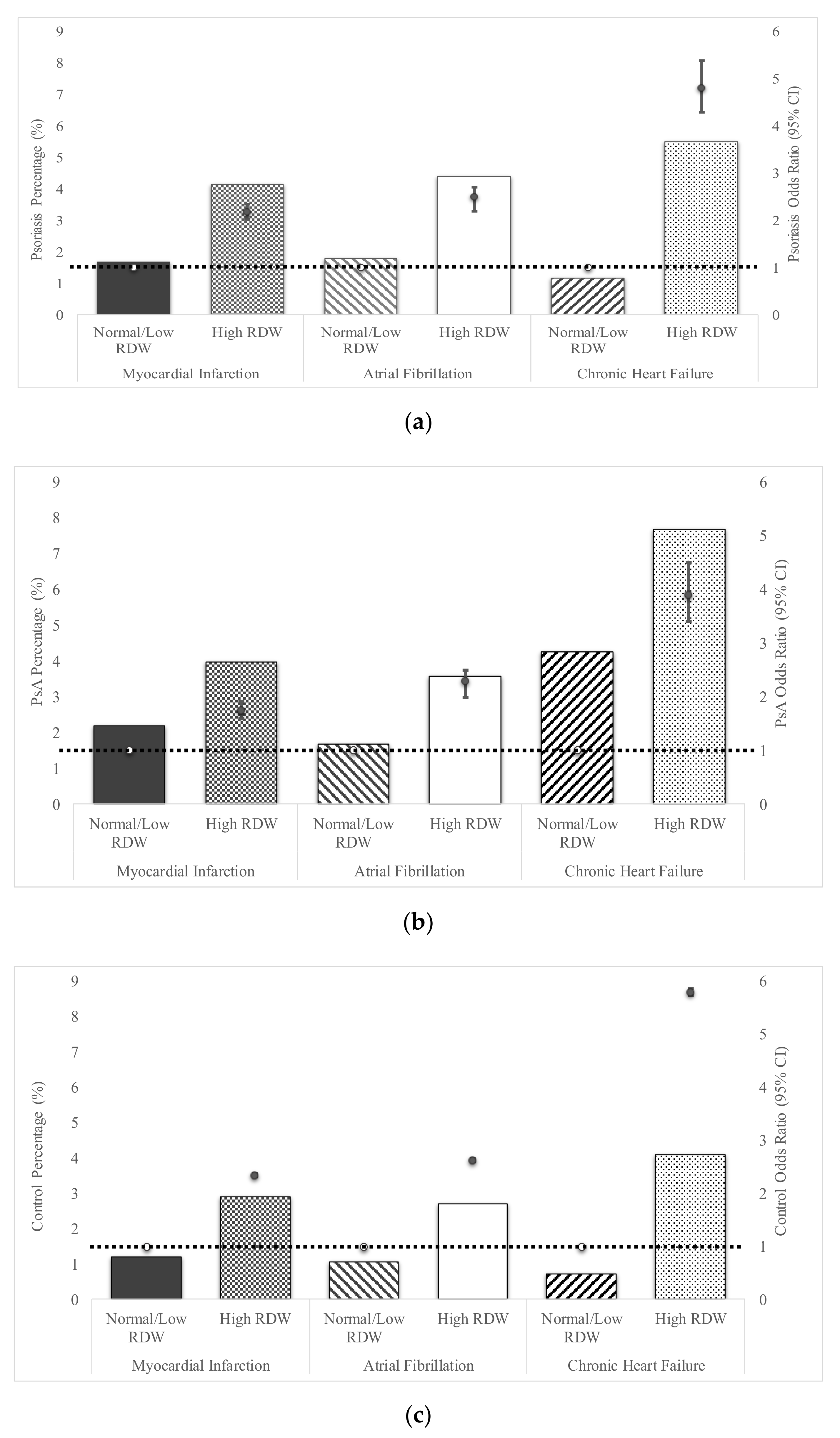
3.2. Erythrocyte Distribution Width and Cardiovascular Disease
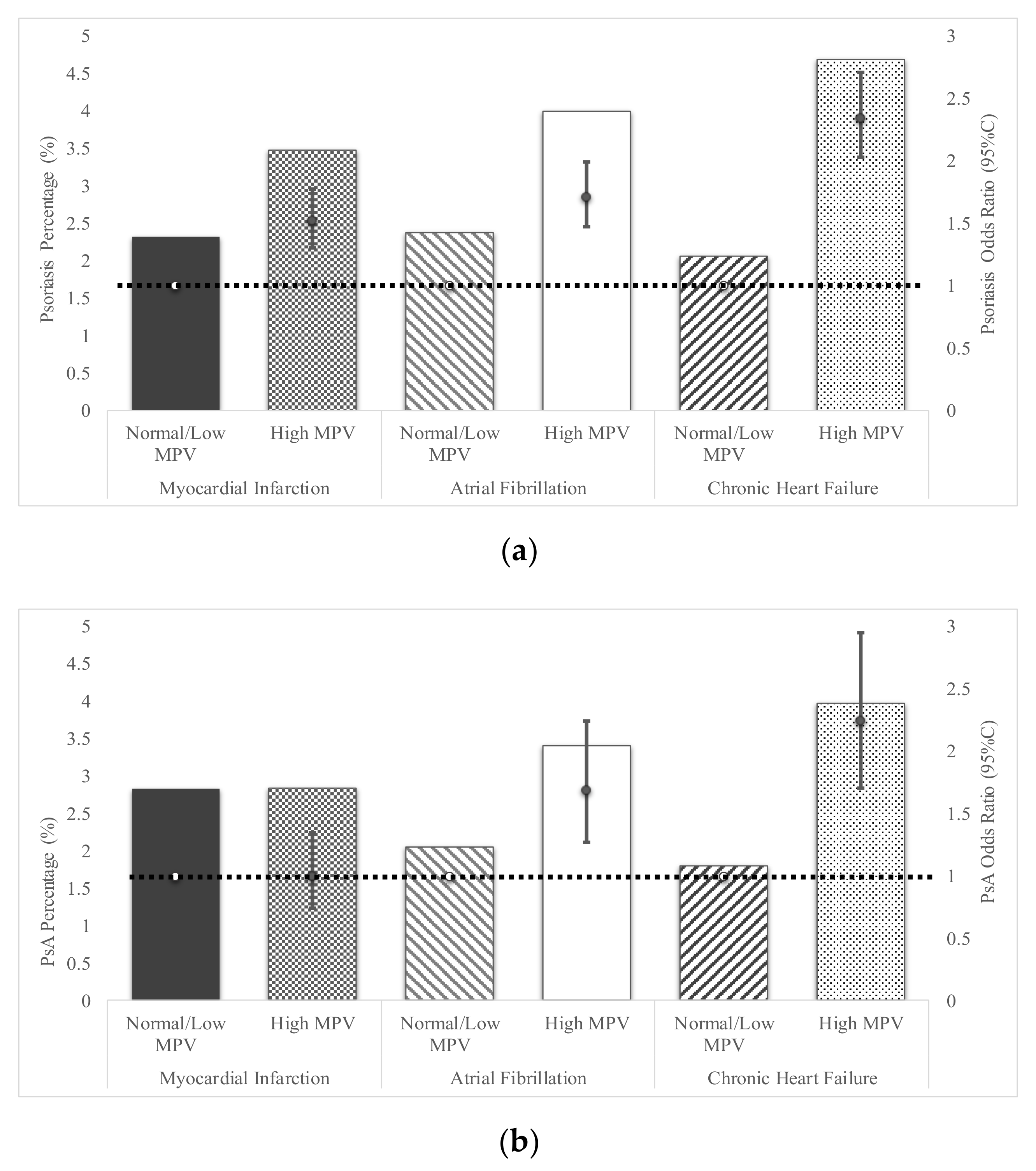
3.3. Mean Platelet Volume and Cardiovascular Disease
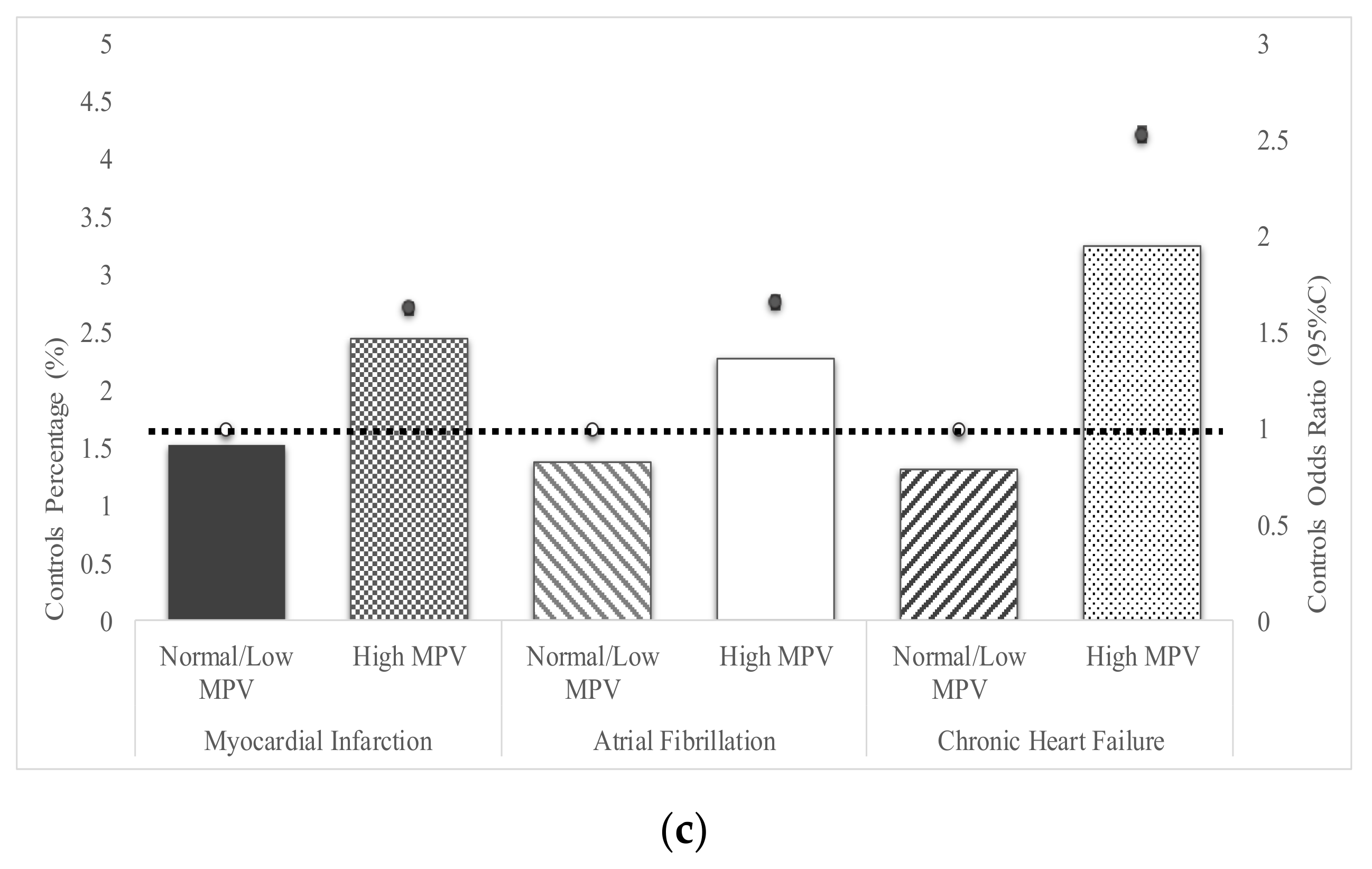
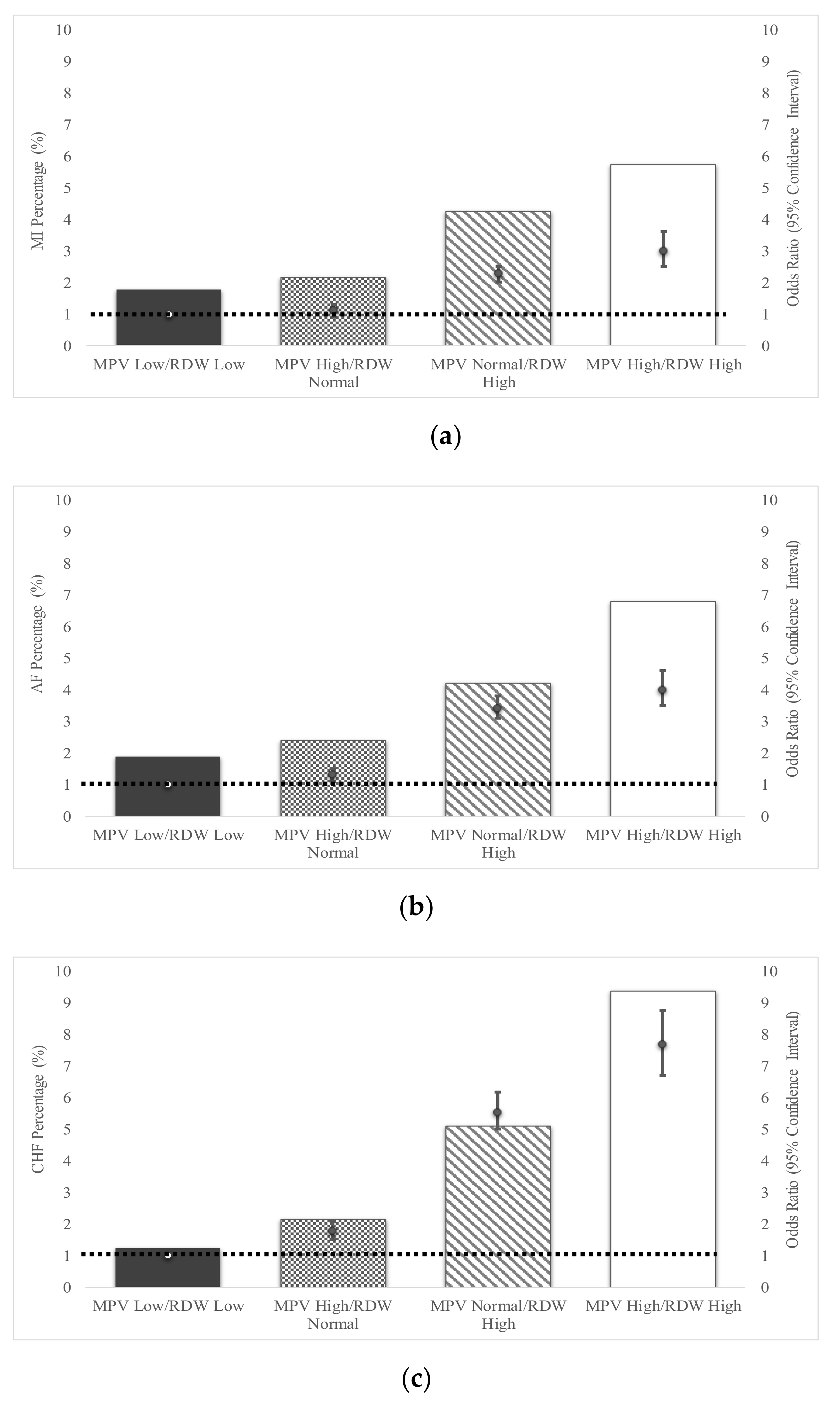
3.4. Combination of MPV and RDW in Assessment of Cardiovascular Disease Risk
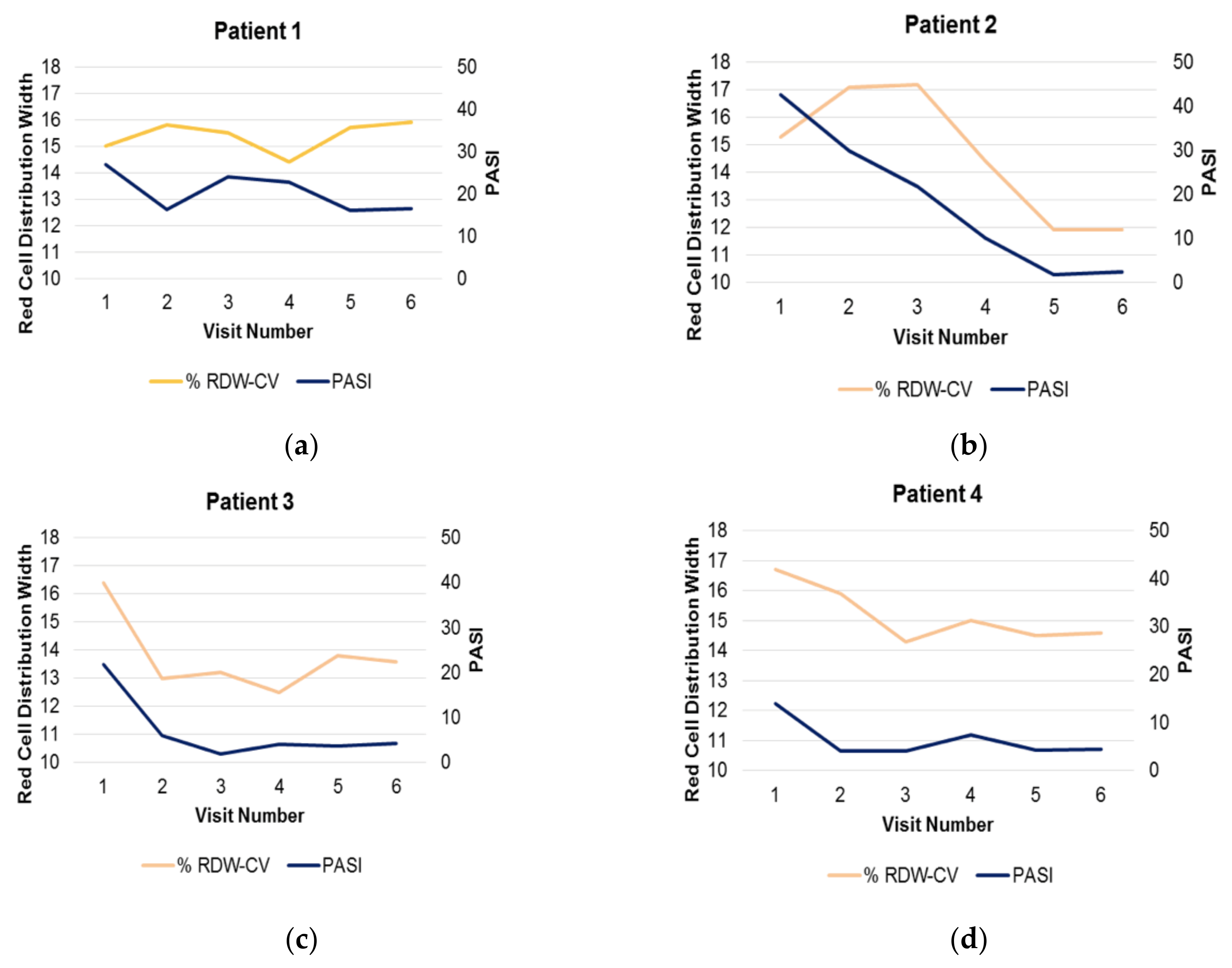
3.5. Responsiveness of High RDW to Therapy
3.6. Regional Organ Response Compared to Distant Organ Response
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Gelfand, J.M.; Neimann, A.L.; Shin, D.B.; Wang, X.; Margolis, D.J.; Troxel, A.B. Risk of myocardial infarction in patients with psoriasis. JAMA 2006, 296, 1735–1741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeung, H.; Takeshita, J.; Mehta, N.N.; Kimmel, S.E.; Ogdie, A.; Margolis, D.J.; Shin, D.B.; Attor, R.; Troxel, A.B.; Gelfand, J.M. Psoriasis severity and the prevalence of major medical comorbidity: A population-based study. JAMA Dermatol. 2013, 149, 1173–1179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.J.; Joshi, A.A.; Reddy, S.P.; Batech, M.; Egeberg, A.; Ahlehoff, O.; Mehta, N.N. Anti-inflammatory therapy with tumour necrosis factor inhibitors is associated with reduced risk of major adverse cardiovascular events in psoriasis. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 1320–1326. [Google Scholar] [CrossRef] [PubMed]
- Bissonnette, R.; Kerdel, F.; Naldi, L.; Papp, K.; Galindo, C.; Langholff, W.; Tang, K.L.; Szapary, P.; Fakharzadeh, S.; Srivastava, B.; et al. Evaluation of Risk of Major Adverse Cardiovascular Events With Biologic Therapy in Patients With Psoriasis. J. Drugs Dermatol. 2017, 16, 1002–1013. [Google Scholar] [PubMed]
- Ogdie, A.; Yu, Y.; Haynes, K.; Love, T.J.; Maliha, S.; Jiang, Y.; Troxel, A.B.; Hennessy, S.; Kimmel, S.E.; Margolis, D.J.; et al. Risk of major cardiovascular events in patients with psoriatic arthritis, psoriasis and rheumatoid arthritis: A population-based cohort study. Ann. Rheum. Dis. 2015, 74, 326–332. [Google Scholar] [CrossRef] [Green Version]
- Santilli, S.; Kast, D.R.; Grozdev, I.; Cao, L.; Feig, R.L.; Golden, J.B.; Debanne, S.M.; Gilkeson, R.C.; Orringer, C.E.; McCormick, T.S.; et al. Visualization of atherosclerosis as detected by coronary artery calcium and carotid intima-media thickness reveals significant atherosclerosis in a cross-sectional study of psoriasis patients in a tertiary care center. J. Transl. Med. 2016, 14, 217. [Google Scholar] [CrossRef] [Green Version]
- Takeshita, J.; Grewal, S.; Langan, S.M.; Mehta, N.N.; Ogdie, A.; Van Voorhees, A.S.; Gelfand, J.M. Psoriasis and comorbid diseases: Epidemiology. J. Am. Acad. Dermatol. 2017, 76, 377–390. [Google Scholar] [CrossRef] [Green Version]
- Traghella, I.; Mastorci, F.; Alessia, P.; Pingitore, A.; Vassalle, C. Nontraditional Cardiovascular Biomarkers and Risk Factors: Rationale and Future Perspectives. Biomolecules 2018, 8, 40. [Google Scholar] [CrossRef] [Green Version]
- Hou, H.; Sun, T.; Li, C.; Li, Y.; Guo, Z.; Wang, W.; Li, D. An overall and dose-response meta-analysis of red blood cell distribution width and CVD outcomes. Sci. Rep. 2017, 7, 43420. [Google Scholar] [CrossRef] [Green Version]
- Choi, D.H.; Kang, S.H.; Song, H. Mean platelet volume: a potential biomarker of the risk and prognosis of heart disease. Korean J. Intern. Med. 2016, 31, 1009–1017. [Google Scholar] [CrossRef] [Green Version]
- Al-Kindi, S.G.; ElAmm, C.; Ginwalla, M.; Mehanna, E.; Zacharias, M.; Benatti, R.; Oliveira, G.H.; Longenecker, C.T. Heart failure in patients with human immunodeficiency virus infection: Epidemiology and management disparities. Int. J. Cardiol. 2018, 218, 43–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niu, X.; Liu, G.; Huo, L.; Zhang, J.; Bai, M.; Peng, Y.; Zhang, Z. Risk stratification based on components of the complete blood count in patients with acute coronary syndrome: A classification and regression tree analysis. Sci. Rep. 2018, 8, 2838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turcato, G.; Serafini, V.; Dilda, A.; Bovo, C.; Caruso, B.; Ricci, G.; Lippi, G. Red blood cell distribution width independently predicts medium-term mortality and major adverse cardiac events after an acute coronary syndrome. Ann. Transl. Med. 2016, 4, 254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dogan, S.; Atakan, N. Red Blood Cell Distribution Width is a Reliable Marker of Inflammation in Plaque Psoriasis. Acta Dermatovenerol. Croat. 2015, 25, 26–31. [Google Scholar]
- Kim, D.S.; Shin, D.; Jee, H.; Kim, T.G.; Kim, S.H.; Kim, D.Y.; Kim, S.M.; Lee, M.G. Red blood cell distribution width is increased in patients with psoriasis vulgaris: A retrospective study on 261 patients. J. Dermatol. 2015, 42, 567–571. [Google Scholar] [CrossRef]
- Raghavan, V.; Radha, R.K.N.; Rao, R.K.; Kuberan, A. A Correlative Study between Platelet Count, Mean Platelet Volume and Red Cell Distribution Width with the Disease Severity Index in Psoriasis Patients. J. Clin. Diagn. Res. 2017, 11, EC13–EC16. [Google Scholar] [CrossRef]
- Damiani, G.; Berti, E.; Pigatto, P.D.M.; Franchi, C.; Asa’ad, F. Benchmarking Stem Cells and Transplantation in Psoriasis. J. Stem Cell Res. Ther. 2018, 8, 416. [Google Scholar]
- Hou, R.; Liu, R.; Niu, X.; Chang, W.; Yan, X.; Wang, C.; Li, J.; An, P.; Li, X.; Yin, G.; et al. Biological characteristics and gene expression pattern of bone marrow mesenchymal stem cells in patients with psoriasis. Exp. Dermatol. 2014, 23, 521–523. [Google Scholar] [CrossRef] [Green Version]
- Liu, R.F.; Li, J.Q.; Hou, R.X.; Wang, R.; Zhang, K.M. Impact of BMMSCs from different sources on proliferation of CD34(+) cells. Genet. Mol. Res. 2015, 14, 474–482. [Google Scholar] [CrossRef]
- Zhang, K.; Liu, R.; Yin, G.; Li, X.; Li, J.; Zhang, J. Differential cytokine secretion of cultured bone marrow stromal cells from patients with psoriasis and healthy volunteers. Eur. J. Dermatol. 2009, 20, 49–53. [Google Scholar] [CrossRef]
- Anatoliotakis, N.; Deftereos, S.; Bouras, G.; Giannopoulos, G.; Tsounis, D.; Angelidis, C.; Kaoukis, A.; Stefanadis, C. Myeloperoxidase: expressing inflammation and oxidative stress in cardiovascular disease. Curr. Top. Med. Chem. 2013, 13, 115–138. [Google Scholar] [CrossRef] [PubMed]
- Bai, F.; Zheng, W.; Dong, Y.; Wang, J.; Garstka, M.A.; Li, R.; An, J.; Ma, H. Serum levels of adipokines and cytokines in psoriasis patients: A systematic review and meta-analysis. Oncotarget 2018, 9, 1266–1278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bokarewa, M.; Nagaev, I.; Dahlberg, L.; Smith, U.; Tarkowski, A. Resistin, an adipokine with potent proinflammatory properties. J. Immunol. 2005, 174, 5789–5795. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.Y.; Soler, D.C.; Debanne, S.M.; Grozdev, I.; Rodriguez, M.E.; Feig, R.L.; Carman, T.L.; Gilkeson, R.C.; Orringer, C.E.; Kern, E.F.; et al. Psoriasis and cardiovascular risk factors: Increased serum myeloperoxidase and corresponding immunocellular overexpression by Cd11b(+) CD68(+) macrophages in skin lesions. Am. J. Transl. Res. 2013, 6, 16–27. [Google Scholar]
- Sabry, H.H.; Sabry, J.H.; Daifalla, A.E.H.; Akl, E.M.; Hamed, A.M.; Torky, A.A.A. Serum markers for asymptomatic atherosclerosis in Egyptian psoriatic patients: Study controlled by Doppler estimation of carotid intima-media thickness. Vasc. Health Risk Manag. 2018, 14, 145–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Wilde, K.; Martens, A.; Lambrecht, S.; Jacques, P.; Drennan, M.B.; Debusschere, K.; Govindarajan, S.; Coudenys, J.; Verheugen, E.; Windels, F.; et al. A20 inhibition of STAT1 expression in myeloid cells: A novel endogenous regulatory mechanism preventing development of enthesitis. Ann. Rheum. Dis. 2016, 76, 585–592. [Google Scholar] [CrossRef]
- Golden, J.B.; Groft, S.G.; Squeri, M.V.; Debanne, S.M.; Ward, N.L.; McCormick, T.S.; Cooper, K.D. Chronic Psoriatic Skin Inflammation Leads to Increased Monocyte Adhesion and Aggregation. J. Immunol. 2015, 195, 2006–2018. [Google Scholar] [CrossRef] [Green Version]
- Huang, T.; Gao, Z.; Zhang, Y.; Fan, K.; Wang, F.; Li, Y.; Zhong, J.; Fan, H.Y.; Cao, Q.; Zhou, J.; et al. CRL4(DCAF2) negatively regulates IL-23 production in dendritic cells and limits the development of psoriasis. J. Exp. Med. 2018, 215, 1999–2017. [Google Scholar] [CrossRef] [Green Version]
- Johnson-Huang, L.M.; Pensabene, C.A.; Shah, K.R.; Pierson, K.C.; Kikuchi, T.; Lentini, T.; Gilleaudeau, P.; Sullivan-Whalen, M.; Cueto, I.; Khatcherian, A.; et al. Post-therapeutic relapse of psoriasis after CD11a blockade is associated with T cells and inflammatory myeloid DCs. PLoS ONE 2012, 7, e30308. [Google Scholar] [CrossRef] [Green Version]
- Khasawneh, A.; Barath, S.; Medgyesi, B.; Béke, G.; Dajnoki, Z.; Gáspár, K.; Jenei, A.; Pogácsás, L.; Pázmándi, K.; Gaál, J.; et al. Myeloid but not plasmacytoid blood DCs possess Th1 polarizing and Th1/Th17 recruiting capacity in psoriasis. Immunol. Lett. 2017, 189, 109–113. [Google Scholar] [CrossRef] [Green Version]
- Soler, D.C.; McCormick, T.S. Expanding the List of Dysregulated Immunosuppressive Cells in Psoriasis. J. Investig. Dermatol. 2016, 136, 1749–1751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soler, D.C.; Young, A.B.; Fiessinger, L.; Galimberti, F.; Debanne, S.; Groft, S.; McCormick, T.S.; Cooper, K.D. Increased, but Functionally Impaired, CD14(+) HLA-DR(-/low) Myeloid-Derived Suppressor Cells in Psoriasis: A Mechanism of Dysregulated T Cells. J. Invest. Dermatol. 2016, 136, 798–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xanthopoulos, A.; Giamouzis, G.; Melidonis, A.; Kitai, T.; Paraskevopoulou, E.; Paraskevopoulou, P.; Patsilinakos, S.; Triposkiadis, F.; Skoularigis, J. Red blood cell distribution width as a prognostic marker in patients with heart failure and diabetes mellitus. Cardiovasc. Diabetol. 2017, 16, 81. [Google Scholar] [CrossRef] [PubMed]
- Al Taii, H.; Yaqoob, Z.; Al-Kindi, S.G. Red cell distribution width (RDW) is associated with cardiovascular disease risk in Crohn’s disease. Clin. Res. Hepatol. Gastroenterol. 2017, 41, 490–492. [Google Scholar] [CrossRef] [PubMed]
- Hassan, S.; Antonelli, M.; Ballou, S. Red cell distribution width: a measure of cardiovascular risk in rheumatoid arthritis patients? Clin. Rheumatol. 2015, 34, 1053–1057. [Google Scholar] [CrossRef] [PubMed]
- Ai, L.; Mu, S.; Hu, Y. Prognostic role of RDW in hematological malignancies: A systematic review and meta-analysis. Cancer Cell Int. 2018, 18, 61. [Google Scholar] [CrossRef] [PubMed]
- Felker, G.M.; Allen, L.A.; Pocock, S.J.; Shaw, L.K.; McMurray, J.J.; Pfeffer, M.A.; Swedberg, K.; Wang, D.; Yusuf, S.; Michelson, E.L.; et al. Red cell distribution width as a novel prognostic marker in heart failure: data from the CHARM Program and the Duke Databank. J. Am. Coll. Cardiol. 2007, 50, 40–47. [Google Scholar] [CrossRef] [Green Version]
- Löfvendahl, S.; Theander, E.; Svensson, Å.; Carlsson, K.S.; Englund, M.; Petersson, I.F. Validity of diagnostic codes and prevalence of physician-diagnosed psoriasis and psoriatic arthritis in southern Sweden—A population-based register study. PLoS ONE 2014, 9, e98024. [Google Scholar]
- Ye, Z.; Smith, C.; Kullo, I.J. Usefullness of red cell distribution width to predict mortality in patients with peripheral artery disease. Am. J. Cardiol. 2011, 107, 1241–1245. [Google Scholar] [CrossRef] [Green Version]
- Fredriksson, T.; Pettersson, U. Severe psoriasis—Oral therapy with a new retinoid. Dermatologica 1978, 157, 238–244. [Google Scholar] [CrossRef]
- R Development Core Team, R. A Language and environment for statistical computing; R Foundation for Statistical Computing: Wien, Austria, 2017. [Google Scholar]
- Chiang, C.C.; Cheng, W.J.; Korinek, M.; Lin, C.Y.; Hwang, T.L. Neutrophils in Psoriasis. Front Immunol. 2019, 10, 2376. [Google Scholar] [CrossRef] [PubMed]
- Lowes, M.A.; Suárez-Fariñas, M.; Krueger, J.G. Immunology of psoriasis. Annu. Rev. Immunol. 2014, 32, 227–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lowes, M.A.; Russell, C.B.; Martin, D.A.; Towne, J.E.; Krueger, J.G. The IL-23/T17 pathogenic axis in psoriasis is amplified by keratinocyte responses. Trends Immunol. 2013, 34, 174–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucijanic, M.; Mitrovic, Z.; Cicic, D.; Prka, Z.; Pejsa, V.; Livun, A.; Stoos-Veic, T.; Romic, Z.; Zivkovic, M.; Lucijanic, I.; et al. Increased mean platelet volume (MPV) is an independent predictor of inferior survival in patients with primary and secondary myelofibrosis. Int. J. Hematol. 2017, 107, 166–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kenney, M.J.; Ganta, C.K. Autonomic nervous system and immune system interactions. Compr. Physiol. 2014, 4, 1177–1200. [Google Scholar] [PubMed] [Green Version]
- Li, N.; Zhou, H.; Tang, Q. Red Blood Cell Distribution Width: A Novel Predictive Indicator for Cardiovascular and Cerebrovascular Diseases. Dis. Markers 2017, 2017, 7089493. [Google Scholar] [CrossRef] [Green Version]
- Hall, J.M.; Cruser, D.; Podawiltz, A.; Mummert, D.I.; Jones, H.; Mummert, M.E. Psychological Stress and the Cutaneous Immune Response: Roles of the HPA Axis and the Sympathetic Nervous System in Atopic Dermatitis and Psoriasis. Dermatol. Res. Pract. 2012, 2012, 403908. [Google Scholar] [CrossRef]
- Vizioli, L.; Muscari, S.; Muscari, A. The relationship of mean platelet volume with the risk and prognosis of cardiovascular diseases. Int. J. Clin. Pract. 2009, 63, 1509–1515. [Google Scholar] [CrossRef]
- Schena, D.; Chieregato, G.C.; de Gironcoli, M.; Girelli, D.; Olivieri, O.; Stanzial, A.M.; Corrocher, R.; Bassi, A.; Ferrari, S.; Perazzoli, P. Increased erythrocyte membrane arachidonate and platelet malondialdehyde (MDA) production in psoriasis: normalization after fish-oil. Acta Derm. Venereol. Suppl. 1989, 146, 42–44. [Google Scholar]
- Baba, Y.; Saito, B.; Shimada, S.; Sasaki, Y.; Murai, S.; Abe, M.; Fujiwara, S.; Arai, N.; Kawaguchi, Y.; Kabasawa, N.; et al. Association of red cell distribution width with clinical outcomes in myelodysplastic syndrome. Leuk. Res. 2018, 67, 56–59. [Google Scholar] [CrossRef]
- Sousa, R.; Gonçalves, C.; Guerra, I.C.; Costa, E.; Fernandes, A.; do Bom Sucesso, M.; Azevedo, J.; Rodriguez, A.; Rius, R.; Seabra, C.; et al. Increased red cell distribution width in Fanconi anemia: A novel marker of stress erythropoiesis. Orphanet J. Rare Dis. 2016, 11, 102. [Google Scholar]
- Kang, S.; Chemaly, E.R.; Hajjar, R.J.; Lebeche, D. Resistin promotes cardiac hypertrophy via the AMP-activated protein kinase/mammalian target of rapamycin (AMPK/mTOR) and c-Jun N-terminal kinase/insulin receptor substrate 1 (JNK/IRS1) pathways. J. Biol. Chem. 2011, 286, 18465–18473. [Google Scholar] [CrossRef] [Green Version]
- Luo, Z.; Zhang, Y.; Li, F.; He, J.; Ding, H.; Yan, L.; Cheng, H. Resistin induces insulin resistance by both AMPK-dependent and AMPK-independent mechanisms in HepG2 cells. Endocrine 2009, 36, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Ou, H.C.; Lee, W.J.; Wu, C.M.; Chen, J.F.; Sheu, W.H. Aspirin prevents resistin-induced endothelial dysfunction by modulating AMPK, ROS, and Akt/eNOS signaling. J. Vasc. Surg. 2012, 55, 1104–1115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steppan, C.M.; Lazar, M.A. The current biology of resistin. J. Intern. Med. 2004, 255, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Rungapiromnan, W.; Mason, K.J.; Lunt, M.; McElhone, K.; Burden, A.D.; Rutter, M.K.; Warren, R.B.; Griffiths, C.E.M.; Ashcroft, D.M.; BADBIR Study Group. Risk of major cardiovascular events in patients with psoriasis receiving biologic therapies: a prospective cohort study. J. Eur. Acad. Dermatol. Venereol. 2019. [Epub ahead of print]. [Google Scholar] [CrossRef] [PubMed]
- Kaur, S.; Kingo, K.; Zilmer, M. Psoriasis and Cardiovascular Risk-Do Promising New Biomarkers Have Clinical Impact? Mediators Inflamm. 2017, 2017, 7279818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019, 74, 1376–1414. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Psoriasis (n = 91,190 (%)) | Psoriatic Arthritis (n = 22,220 (%)) | Control (n = 10,633,910 (%)) | |
|---|---|---|---|
| Age (years) | |||
| <40 | 23,010 (25.23) | 3320 (14.94) | 4,801,560 (45.15) |
| 40–49 | 21,270 (23.32) | 5420 (24.39) | 2,275,540 (21.4) |
| 50–59 | 28,750 (31.53) | 8520 (38.34) | 2,395,360 (22.53) |
| 60–65 | 18,160 (19.91) | 4960 (22.32) | 1,161,450 (10.92) |
| Gender | |||
| Male | 43,720 (47.94) | 11,550 (51.98) | 4,360,730 (41.01) |
| Female | 47,470 (52.06) | 10,670 (48.02) | 6,271,350 (58.98) |
| Not Recorded | 0 (0) | 0 (0) | 1830 (0.02) |
| Race | |||
| Caucasian | 76,940 (84.37) | 17,180 (77.32) | 7,405,980 (69.64) |
| African-American | 5370 (5.89) | 1480 (6.66) | 1,481,020 (13.93) |
| Other | 8880 (9.74) | 3560 (16.02) | 1,746,910 (16.43) |
| BMI (kg/m2) | |||
| Underweight (<18.5) | 3540 (3.88) | 500 (2.25) | 731,070 (6.87) |
| Normal (18.5–24.99) | 12,610 (13.83) | 2310 (10.4) | 3,079,670 (28.96) |
| Overweight (25–29.99) | 23,570 (25.85) | 4840 (21.78) | 2,412,230 (22.68) |
| Obese (>30) | 28,200 (30.92) | 10,070 (45.32) | 3,567,680 (33.55) |
| Not Recorded | 23,270 (25.52) | 4500 (20.25) | 843,260 (7.93) |
| Smokers | 24,720 (27.11) | 4560 (20.52) | 1,634,230 (15.37) |
| Blood pressure (mmHg) | |||
| Normal (<120 systolic, <80 diastolic) | 4770 (5.23) | 4530 (20.39) | 1,169,620 (11) |
| Prehypertension (120–139 systolic, 80–89 diastolic) | 25,360 (27.81) | 4890 (22.01) | 3,144,250 (29.57) |
| Stage 1 Hypertension (140–159 systolic, 90–99 diastolic) | 30,300 (33.23) | 6680 (30.06) | 2,540,710 (23.89) |
| Stage 2 Hypertension (>160 systolic, >100 diastolic | 23,780 (26.08) | 5190 (23.36) | 1,548,290 (14.56) |
| Not Recorded | 6980 (7.65) | 910 (4.1) | 2,231,040 (20.98) |
| RDW (%) | |||
| High (>14.5) | 19,480 (21.36) | 5210 (23.45) | 1,943,130 (18.27) |
| Normal/Low (≤14.5) | 69,670 (76.4) | 16,660 (74.98) | 8,311,460 (78.16) |
| No RDW Data Available | 2040 (2.24) | 350 (1.58) | 379,320 (3.57) |
| MPV (fL) | |||
| High (>12.3) | 7900 (8.66) | 1850 (8.33) | 747,140 (7.03) |
| Normal/low (≤12.3) | 64,180 (70.38) | 17,780 (80) | 5,921,370 (55.68) |
| No MPV Data Available | 7110 (21.02) | 2590 (11.68) | 9,965,400 (37.29) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conic, R.R.; Damiani, G.; Schrom, K.P.; Ramser, A.E.; Zheng, C.; Xu, R.; McCormick, T.S.; Cooper, K.D. Psoriasis and Psoriatic Arthritis Cardiovascular Disease Endotypes Identified by Red Blood Cell Distribution Width and Mean Platelet Volume. J. Clin. Med. 2020, 9, 186. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9010186
Conic RR, Damiani G, Schrom KP, Ramser AE, Zheng C, Xu R, McCormick TS, Cooper KD. Psoriasis and Psoriatic Arthritis Cardiovascular Disease Endotypes Identified by Red Blood Cell Distribution Width and Mean Platelet Volume. Journal of Clinical Medicine. 2020; 9(1):186. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9010186
Chicago/Turabian StyleConic, Rosalynn RZ, Giovanni Damiani, Kory P. Schrom, Amy E. Ramser, Chunlei Zheng, Rong Xu, Thomas S. McCormick, and Kevin D. Cooper. 2020. "Psoriasis and Psoriatic Arthritis Cardiovascular Disease Endotypes Identified by Red Blood Cell Distribution Width and Mean Platelet Volume" Journal of Clinical Medicine 9, no. 1: 186. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9010186