Immunohistochemical BRAF V600E Expression and Intratumor BRAF V600E Heterogeneity in Acral Melanoma: Implication in Melanoma-Specific Survival

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Patients
2.3. Immunohistochemistry
2.4. Evaluation of VE1 IHC Staining
2.5. Statistical Analysis
3. Results
3.1. Patient Data
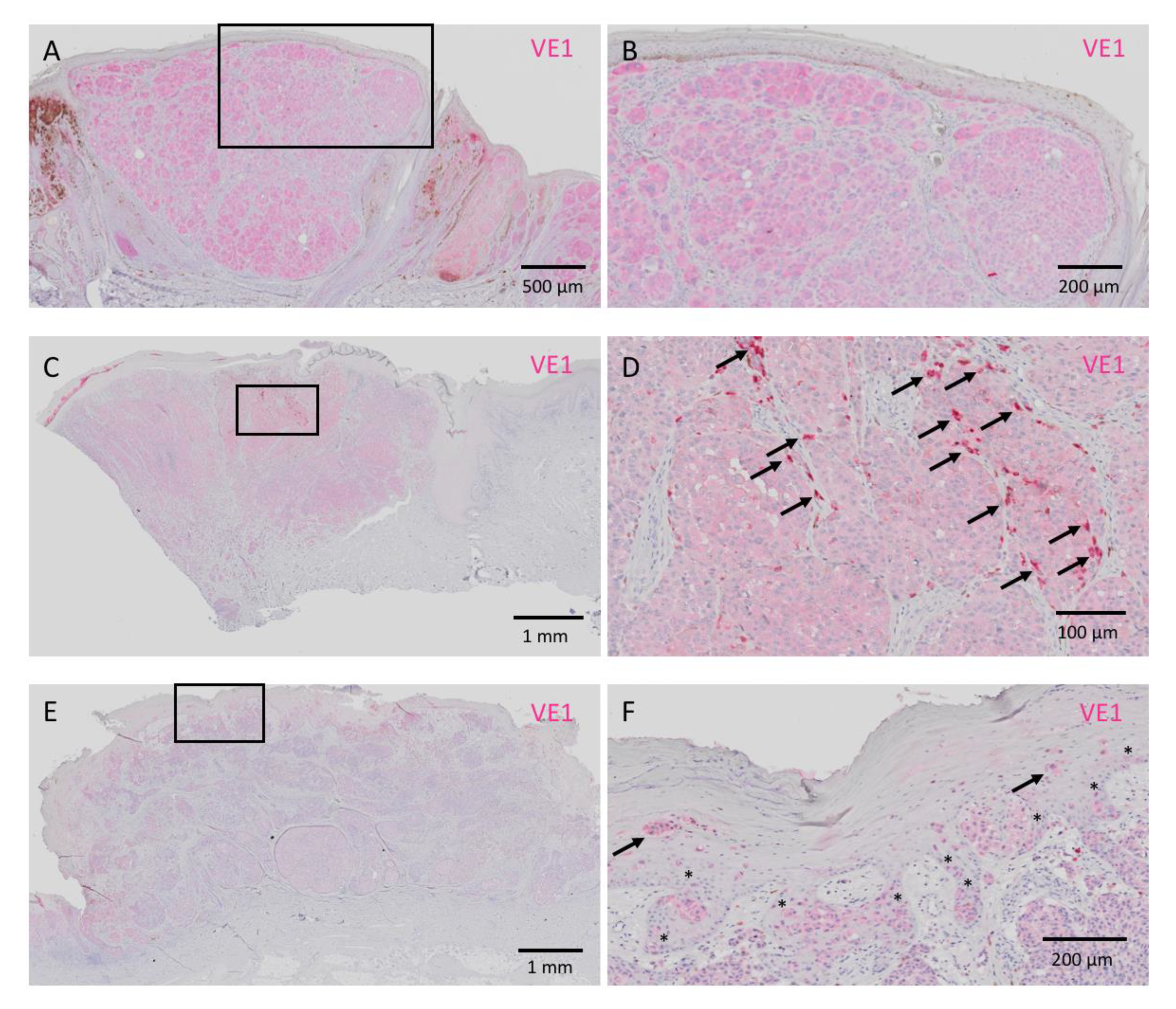
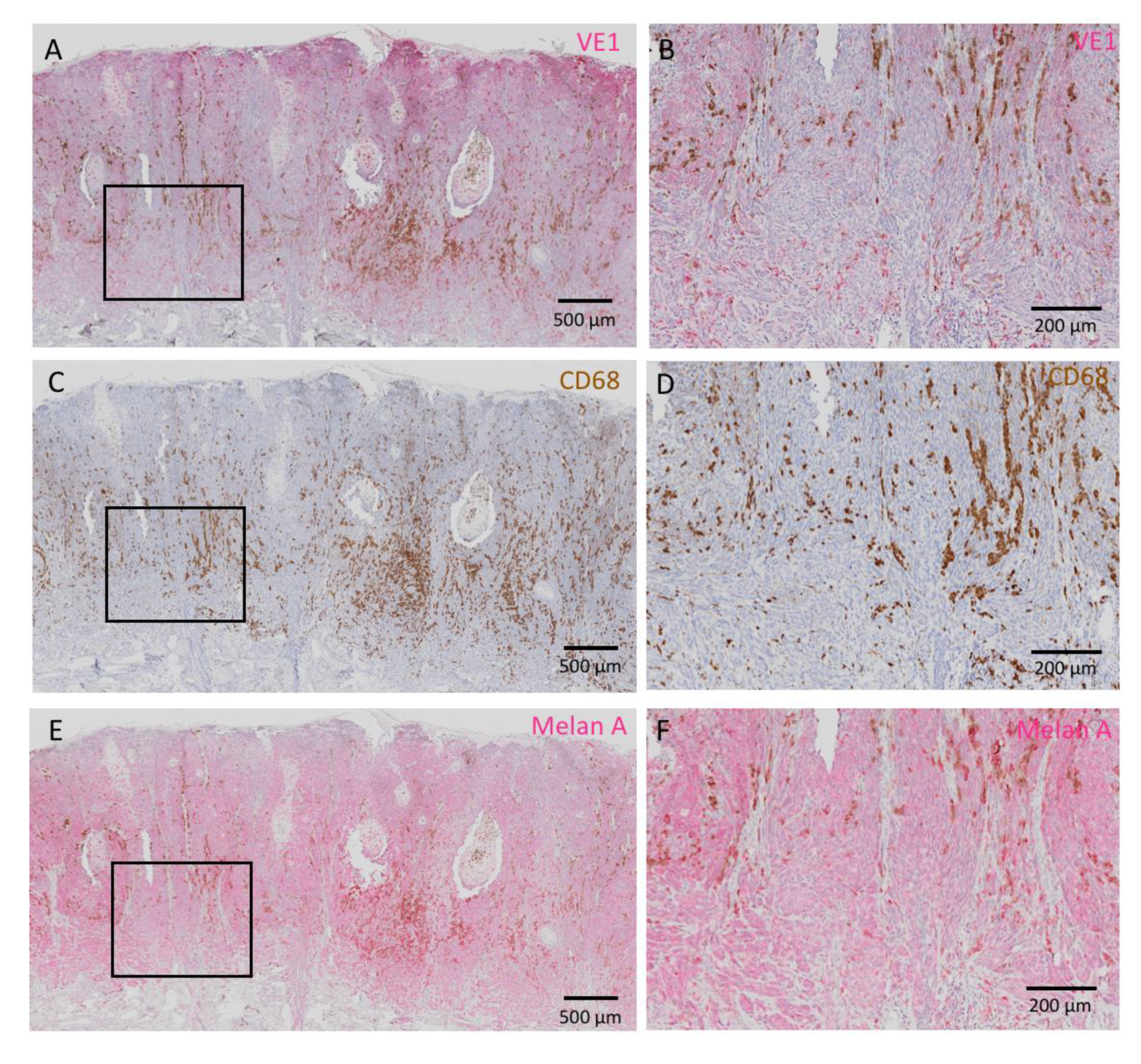
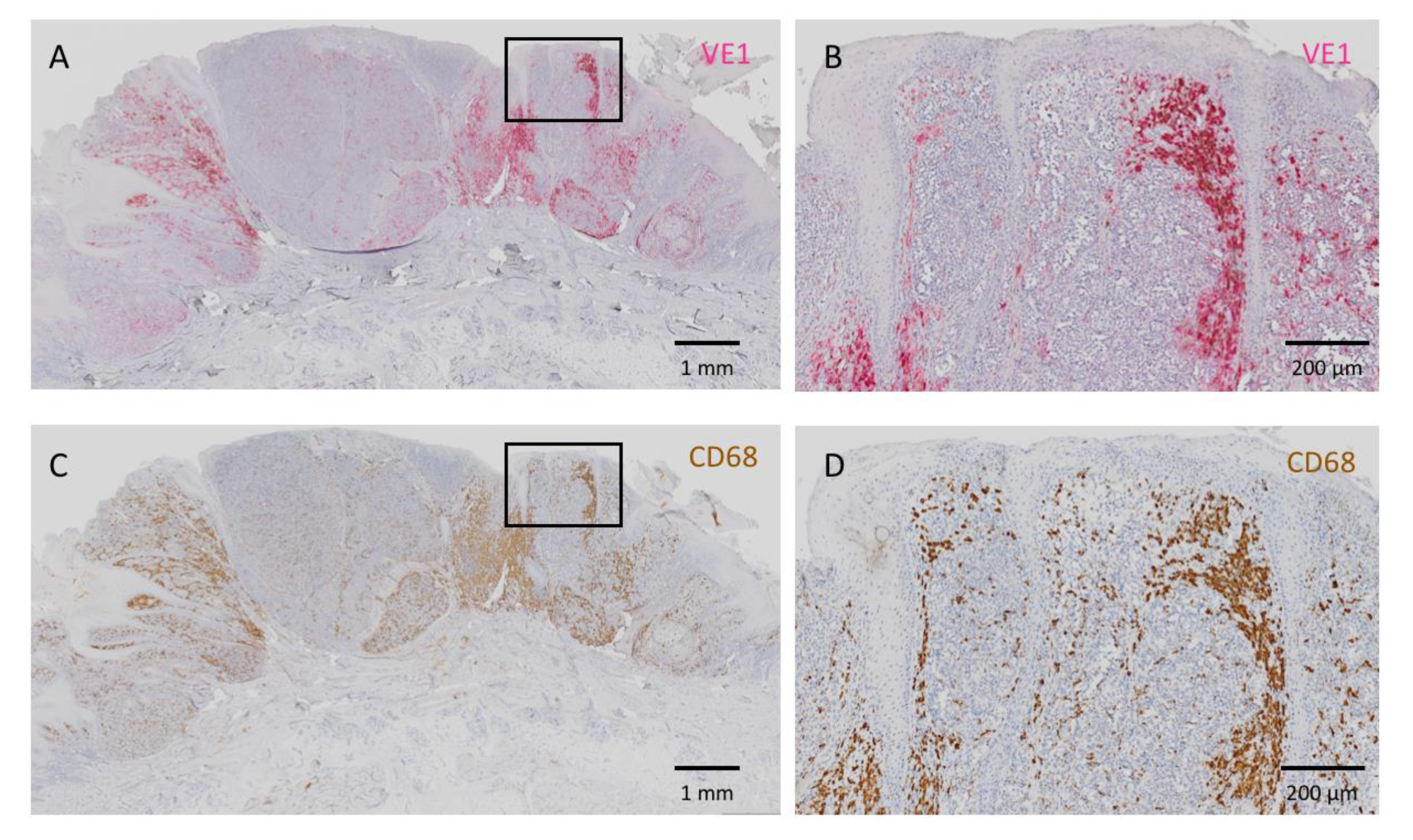
3.2. IHC of VE1
3.3. Consistency Between IHC and Real-Time PCR Regarding BRAF V600E Status in Acral Melanoma
3.4. Factors Associated with BRAF V600E Positivity
3.5. Comparison with Clinicopathological Factors between Heterogeneous and Homogeneous Acral Melanoma
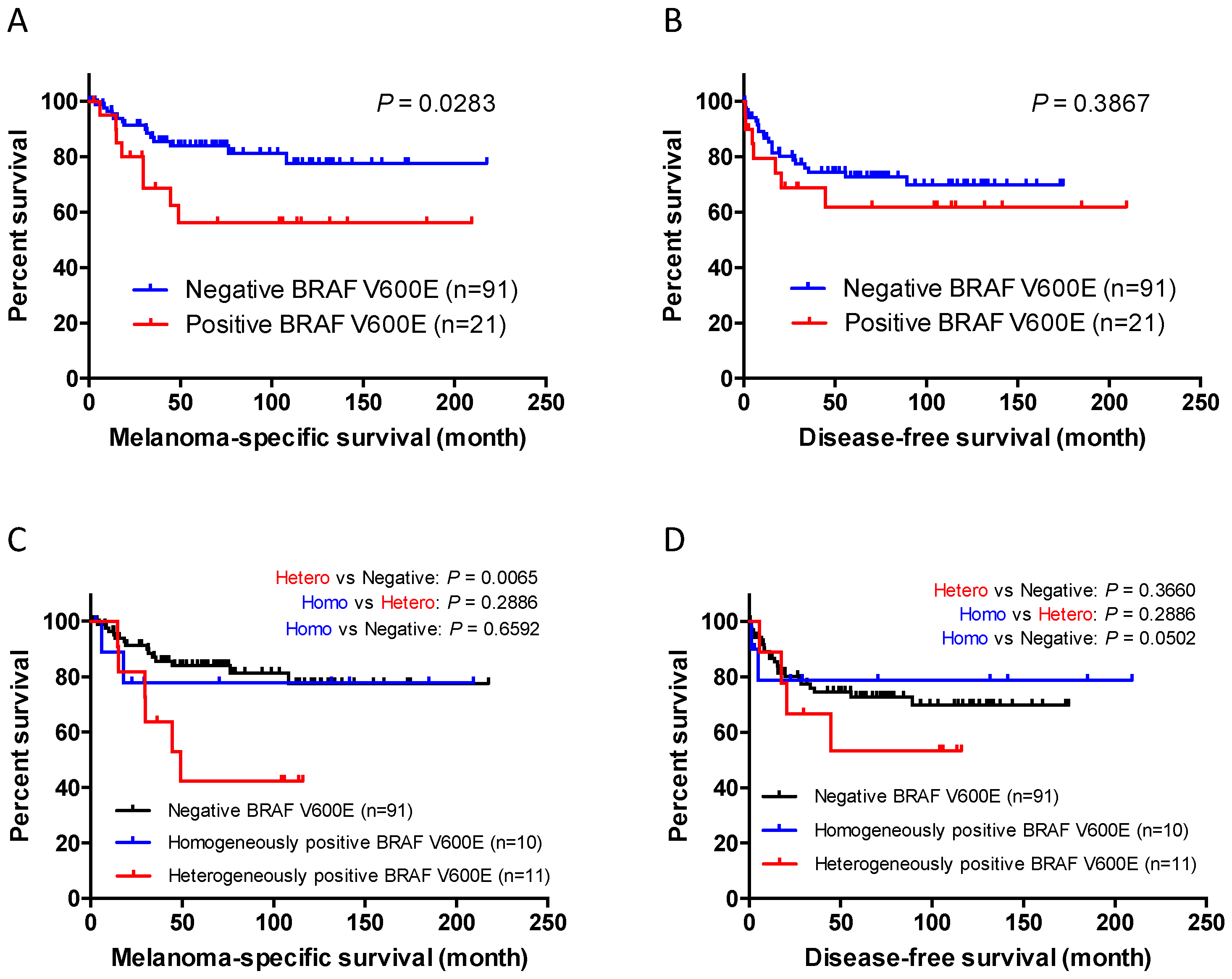
3.6. BRAF V600E Positivity is Linked to Worse Patient Survival in Acral Melanoma
3.7. Cox Multivariate Analysis for Patient Survival
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Curtin, J.A.; Fridlyand, J.; Kageshita, T.; Patel, H.N.; Busam, K.J.; Kutzner, H.; Cho, K.H.; Aiba, S.; Bröcker, E.B.; LeBoit, P.E.; et al. Distinct Sets of Genetic Alterations in Melanoma. N. Engl. J. Med. 2005, 353, 2135–2147. [Google Scholar] [CrossRef]
- Rabbie, R.; Ferguson, P.; Molina-Aguilar, C.; Adams, D.J.; Robles-Espinoza, C.D. Melanoma Subtypes: Genomic Profiles, Prognostic Molecular Markers and Therapeutic Possibilities. J. Pathol. 2019, 247, 539–551. [Google Scholar] [CrossRef]
- Wada-Ohno, M.; Ito, T.; Furue, M. Adjuvant Therapy for Melanoma. Curr. Treat. Opt. Oncol. 2019, 20, 63. [Google Scholar] [CrossRef]
- Furue, M.; Ito, T.; Wada, N.; Wada, M.; Kadono, T.; Uchi, H. Melanoma and Immune Checkpoint Inhibitors. Curr. Oncol. Rep. 2018, 20, 29. [Google Scholar] [CrossRef]
- Coit, D.G.; Thompson, J.A.; Albertini, M.R.; Barker, C.; Carson, W.E.; Contreras, C.P.; Daniels, G.A.; DiMaio, D.; Fields, R.C.; Fleming, M.D.; et al. Cutaneous Melanoma, Version 2.2019, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2019, 17, 367–402. [Google Scholar] [CrossRef] [Green Version]
- Wada, M.; Ito, T.; Tsuji, G.; Nakahara, T.; Hagihara, A.; Furue, M.; Uchi, H. Acral Lentiginous Melanoma versus Other Melanoma: A Single-center Analysis in Japan. J. Dermatol. 2017, 44, 932–938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, T.; Wada, M.; Nagae, K.; Nakano-Nakamura, M.; Nakahara, T.; Hagihara, A.; Furue, M.; Uchi, H. Acral Lentiginous Melanoma: Who Benefits from Sentinel Lymph Node Biopsy? J. Am. Acad. Dermatol. 2015, 72, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Wada, M.; Nagae, K.; Nakano-Nakamura, M.; Nakahara, T.; Hagihara, A.; Furue, M.; Uchi, H. Triple-marker PCR Assay of Sentinel Lymph Node as a Prognostic Factor in Melanoma. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 912–918. [Google Scholar] [CrossRef] [PubMed]
- Sakaizawa, K.; Ashida, A.; Uchiyama, A.; Ito, T.; Fujisawa, Y.; Ogata, D.; Matsushita, S.; Fujii, K.; Fukushima, S.; Shibayama, Y.; et al. Clinical Characteristics Associated with BRAF, NRAS and KIT Mutations in Japanese Melanoma Patients. J. Dermatol. Sci. 2015, 80, 33–37. [Google Scholar] [CrossRef]
- Minagawa, A.; Omodaka, T.; Okuyama, R. Melanomas and Mechanical Stress Points on the Plantar Surface of the Foot. N. Engl. J. Med. 2016, 374, 2404–2406. [Google Scholar] [CrossRef] [Green Version]
- Haugh, A.M.; Zhang, B.; Quan, V.L.; Garfield, E.M.; Bubley, J.A.; Kudalkar, E.; Verzi, A.E.; Walton, K.; VandenBoom, T.; Merkel, E.A.; et al. Distinct Patterns of Acral Melanoma Based on Site and Relative Sun Exposure. J. Investig. Dermatol. 2018, 138, 384–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moon, K.R.; Choi, Y.D.; Kim, J.M.; Jin, S.; Shin, M.H.; Shim, H.J.; Lee, J.B.; Yun, S.J. Genetic Alterations in Primary Acral Melanoma and Acral Melanocytic Nevus in Korea: Common Mutated Genes Show Distinct Cytomorphological Features. J. Investig. Dermatol. 2018, 138, 933–945. [Google Scholar] [CrossRef] [Green Version]
- Shim, J.H.; Shin, H.T.; Park, J.; Park, J.H.; Lee, J.H.; Yang, J.M.; Kim, D.H.; Jang, K.T.; Lee, D.Y. Mutational Profiling of Acral Melanomas in Korean Populations. Exp. Dermatol. 2017, 26, 883–888. [Google Scholar] [CrossRef] [PubMed]
- Siroy, A.E.; Boland, G.M.; Milton, D.R.; Roszik, J.; Frankian, S.; Malke, J.; Haydu, L.; Prieto, V.G.; Tetzlaff, M.; Ivan, D.; et al. Beyond BRAF(V600): Clinical Mutation Panel Testing by Next-generation Sequencing in Advanced Melanoma. J. Investig. Dermatol. 2015, 135, 508–515. [Google Scholar] [CrossRef] [Green Version]
- Sheen, Y.S.; Tan, K.T.; Tse, K.P.; Liao, Y.H.; Lin, M.H.; Chen, J.S.; Liau, J.Y.; Tseng, Y.J.; Lee, C.H.; Hong, C.H.; et al. Genetic Alterations in Primary Melanoma in Taiwan. Br. J. Dermatol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Kaku-Ito, Y.; Murata, M.; Ichiki, T.; Kuma, Y.; Tanaka, Y.; Ide, T.; Ohno, F.; Wada-Ohno, M.; Yamada, Y.; et al. Intra- and Inter-Tumor BRAF Heterogeneity in Acral Melanoma: An Immunohistochemical Analysis. Int. J. Mol. Sci. 2019, 20, 6191. [Google Scholar] [CrossRef] [Green Version]
- Ito, T.; Kohashi, K.; Yamada, Y.; Iwasaki, T.; Maekawa, A.; Kuda, M.; Hoshina, D.; Abe, R.; Furue, M.; Oda, Y. Prognostic Significance of Forkhead Box M1 (FOXM1) Expression and Antitumor Effect of FOXM1 Inhibition in Angiosarcoma. J. Cancer 2016, 7, 823–830. [Google Scholar] [CrossRef] [Green Version]
- Ito, T.; Kohashi, K.; Yamada, Y.; Maekawa, A.; Kuda, M.; Furue, M.; Oda, Y. Prognostic Significance of Forkhead Box M1 (FoxM1) Expression and Antitumour Effect of FoxM1 Inhibition in Melanoma. Histopathology 2016, 69, 63–71. [Google Scholar] [CrossRef]
- Ito, T.; Tsuji, G.; Ohno, F.; Uchi, H.; Nakahara, T.; Hashimoto-Hachiya, A.; Yoshida, Y.; Yamamoto, O.; Oda, Y.; Furue, M. Activation of the OVOL1-OVOL2 Axis in the Hair Bulb and in Pilomatricoma. Am. J. Pathol. 2016, 186, 1036–1043. [Google Scholar] [CrossRef] [Green Version]
- Ito, T.; Tsuji, G.; Ohno, F.; Nakahara, T.; Uchi, H.; Furue, M. Potential Role of the OVOL1-OVOL2 Axis and c-Myc in the Progression of Cutaneous Squamous Cell Carcinoma. Mod. Pathol. 2017, 30, 919–927. [Google Scholar] [CrossRef]
- Meacham, C.E.; Morrison, S.J. Tumour Heterogeneity and Cancer Cell Plasticity. Nature 2013, 501, 328–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yancovitz, M.; Litterman, A.; Yoon, J.; Ng, E.; Shapiro, R.L.; Berman, R.S.; Pavlick, A.C.; Darvishian, F.; Christos, P.; Mazumdar, M.; et al. Intra- and Inter-tumor Heterogeneity of BRAF(V600E) Mutations in Primary and Metastatic Melanoma. PLoS ONE 2012, 7, e29336. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Goto, Y.; Murata, H.; Sakaizawa, K.; Uchiyama, A.; Saida, T.; Takata, M. Polyclonality of BRAF Mutations in Primary Melanoma and the Selection of Mutant Alleles during Progression. Br. J. Cancer 2011, 104, 464–468. [Google Scholar] [CrossRef] [PubMed]
- Curry, J.L.; Torres-Cabala, C.A.; Tetzlaff, M.T.; Bowman, C.; Prieto, V.G. Molecular Platforms Utilized to Detect BRAF V600E Mutation in Melanoma. Semin. Cutan. Med. Surg. 2012, 31, 267–273. [Google Scholar] [CrossRef]
- Skorokhod, A.; Capper, D.; von Deimling, A.; Enk, A.; Helmbold, P. Detection of BRAF V600E Mutations in Skin Metastases of Malignant Melanoma by Monoclonal Antibody VE1. J. Am. Acad. Dermatol. 2012, 67, 488–491. [Google Scholar] [CrossRef]
- Capper, D.; Preusser, M.; Habel, A.; Sahm, F.; Ackermann, U.; Schindler, G.; Pusch, S.; Mechtersheimer, G.; Zentgraf, H.; von Deimling, A. Assessment of BRAF V600E Mutation Status by Immunohistochemistry with a Mutation-specific Monoclonal Antibody. Acta Neuropathol. 2011, 122, 11–19. [Google Scholar] [CrossRef]
- Boursault, L.; Haddad, V.; Vergier, B.; Cappellen, D.; Verdon, S.; Bellocq, J.P.; Jouary, T.; Merlio, J.P. Tumor Homogeneity between Primary and Metastatic Sites for BRAF Status in Metastatic Melanoma Determined by Immunohistochemical and Molecular Testing. PLoS ONE 2013, 8, e70826. [Google Scholar] [CrossRef]
- Verlinden, I.; van den Hurk, K.; Clarijs, R.; Willig, A.P.; Stallinga, C.M.; Roemen, G.M.; van den Oord, J.J.; zur Hausen, A.; Speel, E.J.; Winnepenninckx, V.J. BRAFV600E Immunopositive Melanomas Show Low Frequency of Heterogeneity and Association with Epithelioid Tumor Cells: A STROBE-compliant Article. Medicine (Baltimore) 2014, 93, e285. [Google Scholar] [CrossRef]
- Riveiro-Falkenbach, E.; Villanueva, C.A.; Garrido, M.C.; Ruano, Y.; García-Martín, R.M.; Godoy, E.; Ortiz-Romero, P.L.; Ríos-Martín, J.J.; Santos-Briz, A.; Rodríguez-Peralto, J.L. Intra- and Inter-tumoral Homogeneity of BRAF(V600E) Mutations in Melanoma Tumors. J. Investig. Dermatol. 2015, 135, 3078–3085. [Google Scholar] [CrossRef] [Green Version]
- Menzies, A.M.; Lum, T.; Wilmott, J.S.; Hyman, J.; Kefford, R.F.; Thompson, J.F.; O’Toole, S.; Long, G.V.; Scolyer, R.A. Intrapatient Homogeneity of BRAFV600E Expression in Melanoma. Am. J. Surg. Pathol. 2014, 38, 377–382. [Google Scholar] [CrossRef]
- Manfredi, L.; Meyer, N.; Tournier, E.; Grand, D.; Uro-Coste, E.; Rochaix, P.; Brousset, P.; Lamant, L. Highly Concordant Results between Immunohistochemistry and Molecular Testing of Mutated V600E BRAF in Primary and Metastatic Melanoma. Acta Derm. Venereol. 2016, 96, 630–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eriksson, H.; Zebary, A.; Vassilaki, I.; Omholt, K.; Ghaderi, M.; Hansson, J. BRAFV600E Protein Expression in Primary Cutaneous Malignant Melanomas and Paired Metastases. JAMA Dermatol. 2015, 151, 410–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thiel, A.; Moza, M.; Kytölä, S.; Orpana, A.; Jahkola, T.; Hernberg, M.; Virolainen, S.; Ristimäki, A. Prospective Immunohistochemical Analysis of BRAF V600E Mutation in Melanoma. Hum. Pathol. 2015, 46, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Safaee Ardekani, G.; Jafarnejad, S.M.; Tan, L.; Saeedi, A.; Li, G. The Prognostic Value of BRAF Mutation in Colorectal Cancer and Melanoma: A Systematic Review and Meta-analysis. PLoS ONE 2012, 7, e47054. [Google Scholar] [CrossRef] [Green Version]
- Mar, V.J.; Liu, W.; Devitt, B.; Wong, S.Q.; Dobrovic, A.; McArthur, G.A.; Wolfe, R.; Kelly, J.W. The Role of BRAF Mutations in Primary Melanoma Growth Rate and Survival. Br. J. Dermatol. 2015, 173, 76–82. [Google Scholar] [CrossRef]
- Wilmott, J.S.; Menzies, A.M.; Haydu, L.E.; Capper, D.; Preusser, M.; Zhang, Y.E.; Thompson, J.F.; Kefford, R.F.; von Deimling, A.; Scolyer, R.A.; et al. BRAF(V600E) Protein Expression and Outcome from BRAF Inhibitor Treatment in BRAF(V600E) Metastatic Melanoma. Br. J. Cancer 2013, 108, 924–931. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Number (%) | Parameters | Number (%) |
|---|---|---|---|
| Age in years | N category | ||
| Range (mean ± SD) | 16–88 (65.9 ± 15.3) | N0 | 84 (75.0) |
| Sex | N1 | 10 (8.9) | |
| Male | 50 (44.6) | N2 | 7 (6.3) |
| Female | 62 (55.4) | N3 | 9 (8.0) |
| Ethnicity | Unknown | 2 (1.8) | |
| Japanese | 112 (100.0) | M category | |
| Histopathological subtype | M0 | 105 (93.8) | |
| Acral lentiginous | 110 (98.2) | M1 | 7 (6.3) |
| Nodular | 2 (1.8) | VE1 staining pattern | |
| Primary tumor site | Positive | 21 (18.8) | |
| Palm | 15 (13.4) | Homogeneous | 10 (8.9) |
| Nail bed on hand | 17 (15.2) | Heterogeneous | 11 (9.8) |
| Sole | 68 (60.7) | Negative | 91 (81.3) |
| Nail bed on foot | 12 (10.7) | Detection of BRAF V600E | |
| Ulceration | IHC | 97 (86.6) | |
| Present | 43 (38.4) | IHC + real-time PCR | 15 (13.4) |
| Absent | 69 (61.6) | MSS in month | |
| T category | Range (mean ± SD) | 1–218 (65.9 ± 51.5) | |
| Tis | 29 (25.9) | DFS in month | |
| T1 | 23 (20.5) | Range (mean ± SD) | 0–209 (59.6 ± 52.8) |
| T2 | 10 (8.9) | ||
| T3 | 17 (15.2) | ||
| T4 | 33 (29.5) | ||
| Total | 112 (100) |
| Parameters | BRAF V600E | p Value | |
|---|---|---|---|
| Negative | Positive | ||
| Age in years | |||
| <70 | 48 | 13 | 0.4775 |
| ≥70 | 43 | 8 | |
| Sex | |||
| Male | 38 | 12 | 0.2299 |
| Female | 53 | 9 | |
| Primary tumor site | |||
| Palm | 11 | 4 | 0.1772 |
| Sole | 59 | 9 | |
| Nail bed | 21 | 8 | |
| Ulceration | |||
| Present | 35 | 8 | 1.0000 |
| Absent | 56 | 13 | |
| T category | |||
| Tis, T1, T2 | 57 | 5 | 0.0015 * |
| T3, T4 | 34 | 16 | |
| N category | |||
| N0 | 71 | 13 | 0.0938 |
| N1–3 | 18 | 8 | |
| (Unknown) | (2) | ||
| M category | |||
| M0 | 85 | 20 | 1.0000 |
| M1 | 6 | 1 | |
| Total | 91 | 21 | |
| Parameters | Positive BRAF V600E | p Value | |
|---|---|---|---|
| Homogeneous | Heterogeneous | ||
| Age in years | |||
| < 70 | 6 | 7 | 1.0000 |
| ≥ 70 | 4 | 4 | |
| Sex | |||
| Male | 5 | 7 | 0.6699 |
| Female | 5 | 4 | |
| Primary tumor site | |||
| Palm | 2 | 2 | 0.4830 |
| Sole | 3 | 6 | |
| Nail bed | 5 | 3 | |
| Ulceration | |||
| Present | 3 | 5 | 0.6594 |
| Absent | 7 | 6 | |
| T category | |||
| Tis, T1, T2 | 3 | 2 | 0.6391 |
| T3, T4 | 7 | 9 | |
| N category | |||
| N0 | 8 | 5 | 0.1827 |
| N1–3 | 2 | 6 | |
| M category | |||
| M0 | 10 | 10 | 1.0000 |
| M1 | 0 | 1 | |
| Total | 10 | 11 | |
| Variable | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 95% CI | p Value | |
| Age † | 1.05 | 1.02–1.10 | 0.0040 * | 1.06 | 1.02–1.18 | 0.0113 * |
| Male sex | 2.24 | 0.93–5.42 | 0.0723 | 2.06 | 0.78–5.46 | 0.1449 |
| Tumor site, non-nail bed | 2.77 | 0.81–9.46 | 0.1031 | |||
| Breslow thickness † | 1.05 | 1.02–1.10 | 0.0053 * | 1.13 | 0.96–1.33 | 0.1275 |
| Ulceration | 6.48 | 2.49–16.84 | 0.0001 * | 3.82 | 1.30–11.24 | 0.0148 * |
| LN metastasis | 4.14 | 1.69–10.18 | 0.0019 * | 1.06 | 0.37–3.01 | 0.9139 |
| BRAF V600E positivity | 2.54 | 1.06–6.05 | 0.0359 * | 1.93 | 0.67–5.51 | 0.2219 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ito, T.; Kaku-Ito, Y.; Murata, M.; Furue, K.; Shen, C.-H.; Oda, Y.; Furue, M. Immunohistochemical BRAF V600E Expression and Intratumor BRAF V600E Heterogeneity in Acral Melanoma: Implication in Melanoma-Specific Survival. J. Clin. Med. 2020, 9, 690. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9030690
Ito T, Kaku-Ito Y, Murata M, Furue K, Shen C-H, Oda Y, Furue M. Immunohistochemical BRAF V600E Expression and Intratumor BRAF V600E Heterogeneity in Acral Melanoma: Implication in Melanoma-Specific Survival. Journal of Clinical Medicine. 2020; 9(3):690. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9030690
Chicago/Turabian StyleIto, Takamichi, Yumiko Kaku-Ito, Maho Murata, Kazuhisa Furue, Che-Hung Shen, Yoshinao Oda, and Masutaka Furue. 2020. "Immunohistochemical BRAF V600E Expression and Intratumor BRAF V600E Heterogeneity in Acral Melanoma: Implication in Melanoma-Specific Survival" Journal of Clinical Medicine 9, no. 3: 690. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9030690